Redetermination Form
Redetermination Form
Redetermination Form

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
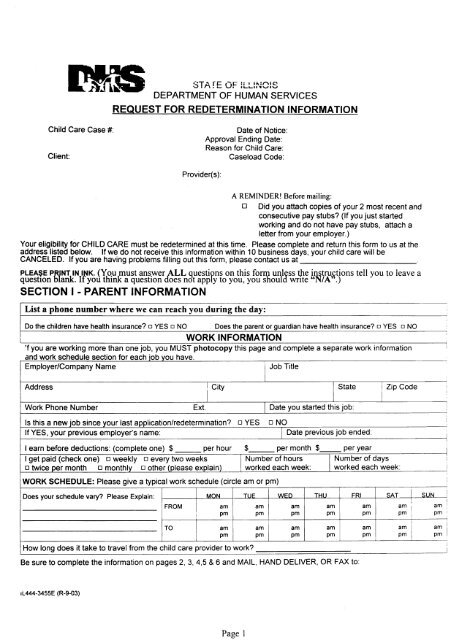
JDEPARTMENT OF HUMAN SERVICESREQUEST FOR REDETERMINATION INFORMATIONChild Care Case #:Client:Date of Notice:Approval Ending Date:Reason for Child Care:Caseload Code:Provider(s):A REMINDER! Before mailing:o Did you attach copies of your 2 most recent andconsecutive pay stubs? (If you just startedworking and do not have pay stubs, attach aletter from your employer.)Your eligibility for CHILD CARE must be redetermined at this time. Please complete and return this form to usat theaddress listed below. If we do not receive this information within 10 business days, your child care will beCANCELED. If you are having problems filling out this form, please contact us at_PLEA$E PRJankNTIN INK. (You must answer ALL questipns on this form unless the instructions tell you to leave aquestIon bl . If you think a question does not apply to you, you should write "N/A".)SECTION I - PARENT INFORMATIONList a phone number where we can reach you during the day:Do the children have health insurance? 0 YES 0 NO . Does the parent or guardian have health insurance? 0 YES 0 NOWORK INFORMATION'f you are working more than one job, you MUST photocopy this page and complete a separate work informationan d wor k sc hdl e u e secfIon f or eac hOb )0 you have,Employer/Company NameI Job TitleAddressWork Phone NumberIExt.I CityIs this a new job since your last application/redetermination?If YES, your previous employer's name:I earn before deductions: (complete one) $ per hourI get paid (check one) o weekly o every two weekso twice per month o monthly o other (please explain)WORK SCHEDULE: Please give a typical work schedule (circle am or pm)Does your schedule vary? Please Explain:FROMTOIII!IMONHow long does it take to travel from the child care provider to work?ampmampmDYESI State I Zip Code !iII Date you started this job:o NOI Date previous job ended:$ per month $ per year iI Number of hours I Number of days !worked each week: worked each week: ITUEampmWEDampmamampm I pmBe sure to complete the information on pages 2,3,4,5 & 6 and MAIL, HAND DELIVER, OR FAX to:THUampmampmFRISAT I SUNamam :pm ~~ I pm :am am Iam ipm pm I pm IItijIi!IIIIIL444-3455E (R-9-03)Page 1
Case Name:Are you c'urrently attending school, training or a T"NF..R~quired Activity?__NO (Go to Section II - Otner Parent/Stepparent info, bottom of this page) __Yes (Complete the Section below)TYPE OF EDUCATIONfTRAININGCURRENTLY ATTENDING:(Check one)SCHOOLITRAININGITANF-REQUIRED ACTIVITY INFORMATION__ 1) High School or GED __ 4) 2-Year College Degree__ 2) Other Below Post-Secondary __ 5) 4-Year College Degree(For example, ABE or ESL)__ 3) OccupationalNocationalType of Degree Being Earned--Do you already have a degree? 0 Yes 0 No If yes, list your degreesSchool NamefTraining Program Currently Attending IPhone Number IDate Started , Ending DateAddress City State Zip Codet-------------.-------------.J---------------.L....--------L--__--1 ,How long does it take to travel from the child care provider to school?_ISCHOOL SCHEDULE: Please complete the following schedule (circle am or pm)Does your schedule vary? PleaseIi I MON TUE I WED THU FRI SAT SUNExplain:i IIFROM am I am Iam am am am ampm I pm pm pm pm pm pmIam am am am am am amITOpm I pm pm pm pm pm pmi! ITANF CLIENTS: You MUST provide an Official Class Schedule (if you are in school) and one of the following. Check the one you have attachedo Responsibility and Service Plan (RSP) (<strong>Form</strong> 400 ) o Contracted Provider's Referral (<strong>Form</strong> 2151A)o IDHS Contract Report - Notification of Employment (<strong>Form</strong> 3085) 0 IDHS Referral (<strong>Form</strong> 2151)CLIENTS NOT RECEIVING TANF CASH ASSISTANCE: You MUST provide an Official Class Schedule and a copy of: (check all that apply)o Confirmation letter from training program0 Grade Report <strong>Form</strong>o Registration/Class information about internship, student teaching, practicumSECTION II - OTHER PARENTI STEPPARENT INFORMATIONIs the other parent or stepparent of any of the children living in your home?__ NO (Go to Section III - Family Information, on page 4) __ YES (Complete the following section)Is the other parent or stepparent working? 0 YES 0 NOIs the other parent or stepparent attending school? 0 YES 0 NOIf the other parent/stepparent is not working or in a school/training program, please explain why he/she cannot carefor the children?Other Parent/Stepparent Last Name M.1. First NameSocial Security Number (Optional)Date of BirthMonth: Day: Year:Phone NumberFOR OFFICE USE:! REASON FOR CHILDCARE1) Work/On-the-job Training for TANF and Non-TANF2) TANF EducationlTraining Activity or Teen Parent in HighSchooi/GED3) TANF Work & EducationlTraining Activity or Teen Parent Work &High School GED4) Non-TANF Education & TrainingPage 2
Page 4SECTION I!! - F=AMILY IttffiRM.~I!ONCase Name:~A~ILY SIZE means the applicant (you); the biologicai. step or adoptive parent of any of the applicant's chiidren who~Ive In your home; and your biological or adoptive cnildren under age 21 living in your home. You may also choose to. Include other persons in the home who are related to you by blood or law if they rely on you for more than 500/0 of theirtpport.._What is your family size?How many adults are in ~our family?How many children are in your family?__ How many chi dren are receiving child care? __Co~plete the information below for each child for whom you are seeking child care payments. If needed, attach anadditional paQe.DATEU.S.SOCIALWARD OFFIRST NAME LAST NAME OF M/FETHNICCITIZENSECURITYORIGIN*NUMBERTHE STATEBIRTHYES/NO··(Optional)YES/NO !I:II i• For each child's ETHNIC ORIGIN. list all numbers below that apply: ~Required for Federal Reporting)1 - White 2 - Black or African American 3 - Hispanic or Latino ( ersons declarin~ Hispanic ethnicity should also listtheir race. If you list "3" for a child, also list their race. for example, "3, 1", u3, 2" or "3, I).4 - Asian 5 - American Indian or Alaskan Native 6 - Native Hawaiian or Pacific Islanderu** If NO " . IS entered for U.S. CITIZEN, wnte allen registration number and attach copy of documentation.List all other family members counted in family size: (If more space is needed, please follow this format on a separate sheet of paper)iIFIRST NAMEILAST NAMEDATE OFBIRTHRELATIONSH IPTO APPLICANTSOCIAL SECURITYNUMBER (Optional)IIi 1 IIiI:ISection IV -INCOME INFORMATIONI! Enter the MONTHLY income in each box for all adults age 19 and over counted in family size. If the income does not apply, write UN/A".I IITYPE OF INCOMEiI1. Gross Emr-Ioyment Income: (including tips) from pay stubs before deductions.. Enter any sel -em~loyment income below.i Attach copies of most recent and consecutive pay stubs for each person.$CLIENTOTHER FAMILYMEMBERS$:! 2. Self-Employment Income $ $: 3. Child Support ReceivedI C .: 4. TANF ash ASSistance5. Other Federal Cash Income: For example, Social Security payments and ra.ilroad benefits.I 6. Other Monthly Income: For example. interest income, royalties. pensions. annuities, alimony,ongoing monthly adoption assistance, unemployment compensation, DCFS payments, veteran'spension, survivor's benefits, and permanent disability payments.SUBTOTAL (add lines 1-6)MINUS: Child Support Paid by Applicant's FamilyTOTALL MONTHLY INCOMEI ~ousing Cash Assistance Including Vouchers With S~CifiC Cash Value::For Federal reporting, does not count when totaling onthly Family Income)1 FOR OFFICE USE: PARENT CO-PAYMENTI$$$$$$$$$$$$.__ .$$$ .
Page 5/ SECT!ON V - CHILO"CARE AR.RANGEMENTSCase Name:I - -LIST THE CHILDREN CARED FOR BY EACH PROVIDER If your children go to school, pre-K, or Head Startduring the day, list only the hours that they are with the child care provider. For school age children, list only the)urs that they are in Child Care. (This is not a Provider Change <strong>Form</strong>.)Is one of your providers an approved Head StartlPre-Kcollaboration?#1 Provider Name:~iICHILD'S NAME AGE MON TUE WED THU FRI SAT SUN Provider'sCurrentDaily RateIi #2 Provider Name:!CHILD'S NAMEIIi iIIIIIi #3 Provider Name:CHILD'S NAMEI,iiiI[I!IFROMIampmampmampmampmampmampmampmI II TOtam Ipm iampmampmampmampmampmampmj FROM am am am am am am ampmI Ipm pm pm pm pm pmTO ampmampmampmampmampmampmampmFROMIampmampm IampmampmampmampmampmIIITO am am ~ am am am ampm i pm pm pm pm pm pmIIIFROMIIampmampmampmampmampmampmampmIIIiIiiiI!iIIIAGE iIII TO am I am am am am am amIiI pm pm pmI IiIIIf yes, Collaborator's Name:How long is the program? 0 9mo 0 12mo 0 other_pm pm pm pmI MON 1 TUE WED THU FRI SAT SUNiIiFROM ampm Ii ampmampmampmampmampmampmTO am 1 am am am am am amIFROMI!TOiIIIpm I pm pm pm pm pm pmampm I am am am am am ampm pm pm pm pm pmIampm IiampmampmampmampmampmampmFROM am ! am am am am am am1 pm i pm pm I pm pm pm pm! TOiampm IiI I FROM ampmIIIIiIiAGE!! TOiIIFROMTOFROMTOi FROMiTOIIIampmMONampmampmampmampmampm~~1iIII1IlTUEampmampmampmampmampmampmampmampmampmampmampmampmWEDampmampmampmampmampmampmampmampmampmTHUampmampmampmampmampmampmampmampmampmFRIampmampmampmampmampmampmampmampmampmSATampmampmampmampmampmampmampmampmampmSUNampmampmampmampmampmampmPCovider'surr~ntDally atePCovider'SDal~rrffty ateIiIIII:iI!
Lase Name:SECT!ON VI - CLIFNT CERTIFICATIONAfter reading each of the following statements, I certify that:I understand that I am responsible for paying a share of my child care costs (parent co-payment) to myprovider and that failure to do so may result in the loss of my child care provider.• I understand that my eligibility will be redetermined every 6 months or as needed.The child(ren) is/are current on all immunizations and verification is on file with the provider.• A review of each facility/home has been completed and I agree that it is a safe environment.• I have given written notification to each provider if I want anyone other than myself to pick up the child(ren).• An emergency phone number and written consent for medical care and for dispensing prescriptionmedication has been given to each provider.The name of the family physician is on file with each provider.I am responsible for the selection of the child care providers for my child(ren).• I will report any change in child care arrangements or employment within 5 days. Failure to report changesin a timely manner may result in pay back of overpayments and/or loss of child care benefits.• I understand that I must be working or attending an IDHS approved education, training, or other workrelated activity in order to be eligible to receive child care benefits.I understand the information provided will be checked using State databases, and if inconsistencies arediscovered, the processing of my redetermination may be delayed or denied.All of the statements listed above are true.I :The information provided about my case is true, correct and complete.I understand that I am not required to provide my Social Security Number and that if I deliberately providean incorrect or fictitious Social Security Number I may be prosecuted for fraud.The information provided will be disclosed only for administrative purposes and that I may be required toverify the information that I have provided.I understand that I have the right to appeal and to have a fair hearing of a grievance.I understand that giving false information or failure to provide correct information can result in pay back ofoverpayments and/or referral for prosecution for fraUd.I My signature is my consent and authorization for information to be released to the Department of Human1 Services or its agents that may establish my eligibility or my continued eligibility for the Child Care Program.I Client's Signature:Date:-------IiPage 6