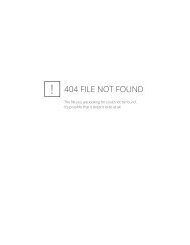
International AIDS Society–USATopics <strong>in</strong> HIV Medic<strong>in</strong>eTable 1. Characteristics <strong>of</strong> Antiretroviral <strong>Drug</strong>s Applicablefor <strong>The</strong>rapeutic <strong>Drug</strong> <strong>Monitor<strong>in</strong>g</strong>CriteriaAnalytical<strong>Drug</strong> assay is accurate, specific, precise,requires small sample volume, yieldsrapid results, and is <strong>in</strong>expensivePharmacok<strong>in</strong>eticPharmacok<strong>in</strong>etic data are availableSignificant <strong>in</strong>terpatient pharmacok<strong>in</strong>eticvariability existsPharmacologicPharmacologic effect is related to drugconcentration<strong>Drug</strong> has a narrow <strong>the</strong>rapeutic <strong>in</strong>dex<strong>Drug</strong> has constant pharmacologic effectover extended period <strong>of</strong> timeCl<strong>in</strong>icalCl<strong>in</strong>ical studies have documented <strong>the</strong><strong>the</strong>rapeutic and toxic ranges <strong>of</strong> <strong>the</strong> drugCriteria for TDM Use <strong>in</strong> Cl<strong>in</strong>ical Medic<strong>in</strong>e<strong>The</strong> required criteria for <strong>the</strong> use <strong>of</strong> TDM <strong>in</strong> cl<strong>in</strong>ical medic<strong>in</strong>ewere described by Spector and colleagues <strong>in</strong> 1988. 2 <strong>The</strong>se criteriaare reviewed below <strong>in</strong> <strong>the</strong> context <strong>of</strong> antiretroviral drugs andcharacteristics that make drugs candidates for TDM (Table 1).Analytical CriteriaEvaluation√ <strong>in</strong>dicates sufficient data are available for antiretroviral drugs tomeet <strong>the</strong> specified criterion; ± <strong>in</strong>dicates some data are available but<strong>the</strong> criterion has not been met. *Depends on <strong>the</strong> extent <strong>of</strong> viral<strong>in</strong>hibition. Adapted from Spector et al, Cl<strong>in</strong> Pharmacol <strong>The</strong>r, 1988.A drug assay is available with high specificity, small sample volume requirements,reasonable cost, and rapid turnaround time.Very sensitive and specific assays are available for all <strong>the</strong> protease<strong>in</strong>hibitors, nonnucleoside reverse transcriptase <strong>in</strong>hibitors(NNRTIs), and nucleoside reverse transcriptase <strong>in</strong>hibitors(nRTIs) us<strong>in</strong>g high-performance liquid chromatography withultraviolet (HPLC-UV) detection or liquid chromatography-massspectrometry/mass spectrometry (LC-MS/MS). However, nRTIsare more complex than protease <strong>in</strong>hibitors and NNRTIs s<strong>in</strong>ce<strong>the</strong>y circulate <strong>in</strong> <strong>the</strong> plasma as prodrugs and require <strong>in</strong>tracellularphosphorylation to <strong>the</strong> active triphosphate metabolite. As aresult, plasma concentrations <strong>of</strong> nRTIs may not always reflectactivity <strong>in</strong> <strong>the</strong> <strong>in</strong>tracellular compartment. A good example isdidanos<strong>in</strong>e, which has a very short plasma half-life but a long<strong>in</strong>tracellular half-life and duration <strong>of</strong> action. 3 S<strong>in</strong>ce it has been√√√√±±*±very difficult to measure accurately <strong>the</strong> <strong>in</strong>tracellular concentrations<strong>of</strong> many nRTI triphosphates, nRTIs may not be good candidatesfor TDM and thus will not be <strong>in</strong>cluded <strong>in</strong> <strong>the</strong> discussion<strong>of</strong> <strong>the</strong> o<strong>the</strong>r criteria for TDM. <strong>The</strong> analytical criteria required forapplication <strong>of</strong> TDM is met by <strong>the</strong> protease <strong>in</strong>hibitors andNNRTIs; <strong>the</strong> cost and turnaround time criteria will likely be metas more laboratories undertake <strong>the</strong> analysis <strong>of</strong> <strong>the</strong>se drugs.Pharmacok<strong>in</strong>etic Criteria<strong>The</strong>re is significant <strong>in</strong>ter<strong>in</strong>dividual variability <strong>in</strong> pharmacok<strong>in</strong>etics, result<strong>in</strong>g<strong>in</strong> large variability <strong>in</strong> achieved plasma concentrations. Adequate pharmacok<strong>in</strong>eticdata concern<strong>in</strong>g <strong>the</strong> drug are available.Although a fixed dose is adm<strong>in</strong>istered to all adults tak<strong>in</strong>g protease<strong>in</strong>hibitors and NNRTIs, large variability <strong>in</strong> achieved plasmaconcentrations has been well documented for all <strong>the</strong> drugs<strong>in</strong> cl<strong>in</strong>ical use. 4-7 A number <strong>of</strong> pharmacok<strong>in</strong>etic studies havebeen conducted on currently available antiretroviral drugs asreviewed <strong>in</strong> a recent position paper on TDM. 8 All protease<strong>in</strong>hibitors have large <strong>in</strong>tersubject variability <strong>in</strong> achieved plasmaconcentration follow<strong>in</strong>g fixed-dose adm<strong>in</strong>istration (Figure 2).This variability becomes a concern when <strong>the</strong> achieved troughconcentration is below <strong>the</strong> concentration necessary for <strong>in</strong>hibition<strong>of</strong> viral replication, <strong>the</strong>reby creat<strong>in</strong>g <strong>the</strong> potential for <strong>the</strong>evolution <strong>of</strong> drug-resistant isolates. Adm<strong>in</strong>istration <strong>of</strong> ritonavirwith o<strong>the</strong>r protease <strong>in</strong>hibitors tends to reduce <strong>the</strong> pharmacok<strong>in</strong>eticvariability <strong>of</strong> <strong>the</strong> protease <strong>in</strong>hibitors, but <strong>the</strong> <strong>in</strong>tersubjectvariability still rema<strong>in</strong>s high. 9 Large <strong>in</strong>ter<strong>in</strong>dividual variability isalso present with achieved plasma concentrations <strong>of</strong> NNRTIs,yet it is unclear whe<strong>the</strong>r failure <strong>of</strong> NNRTI-based <strong>the</strong>rapy is dueto low plasma concentrations. Achieved plasma concentrationsfor nevirap<strong>in</strong>e are orders <strong>of</strong> magnitude higher than what isrequired for viral <strong>in</strong>hibition <strong>in</strong> vitro. 10 However, quasi specieswith high-level drug resistance circulate as m<strong>in</strong>ority stra<strong>in</strong>s, and<strong>the</strong>refore adequate exposure to concomitant nRTIs is likely crucial<strong>in</strong> ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g successful <strong>the</strong>rapy with most <strong>of</strong> <strong>the</strong> NNRTIs.Ind<strong>in</strong>avir Concentration (µM)201510500 1 2 3 4 5 6 7 8Time (hours)Figure 2. <strong>The</strong> extreme variability <strong>of</strong> <strong>the</strong> pharmacok<strong>in</strong>etics <strong>of</strong> a protease<strong>in</strong>hibitor (<strong>in</strong>d<strong>in</strong>avir) follow<strong>in</strong>g standard dos<strong>in</strong>g (800 mg q8h).Similar data show<strong>in</strong>g large <strong>in</strong>tersubject variability <strong>in</strong> pharmacok<strong>in</strong>eticsare available for o<strong>the</strong>r protease <strong>in</strong>hibitors. Adapted with permissionfrom Acosta et al, Pharmaco<strong>the</strong>rapy, 1999.28
Review - <strong>The</strong>rapeutic <strong>Drug</strong> <strong>Monitor<strong>in</strong>g</strong> Volume 10 Issue 2 May/June 2002<strong>The</strong>re are many reasons beh<strong>in</strong>d pharmacok<strong>in</strong>etic variability<strong>of</strong> <strong>the</strong>se lipophilic drugs. <strong>The</strong>re is undoubtedly variability <strong>in</strong>drug solubilization and absorption from <strong>the</strong> <strong>in</strong>test<strong>in</strong>al tract.Multidrug-resistant prote<strong>in</strong>s such as P-glycoprote<strong>in</strong> likelyimpede <strong>the</strong> bioavailability <strong>of</strong> protease <strong>in</strong>hibitors. In addition,<strong>the</strong> large variability <strong>of</strong> CYP3A expression <strong>in</strong> <strong>the</strong> small <strong>in</strong>test<strong>in</strong>eand <strong>the</strong> liver can result <strong>in</strong> significant variability <strong>in</strong> <strong>the</strong> drug'sbioavailability and systemic clearance. Based upon <strong>the</strong> large<strong>in</strong>tersubject pharmacok<strong>in</strong>etic variability <strong>of</strong> protease <strong>in</strong>hibitorsand NNRTIs and <strong>the</strong> sufficient data available on <strong>the</strong>ir pharmacok<strong>in</strong>eticpr<strong>of</strong>iles, both drug classes qualify for TDM.Pharmacologic CriteriaPharmacologic effect is proportional to <strong>the</strong> plasma drug concentration. Anarrow range exists between <strong>the</strong> efficacious and toxic concentrations. A constantpharmacologic effect over an extended period <strong>of</strong> time exists.Higher plasma concentrations <strong>of</strong> protease <strong>in</strong>hibitors haveresulted <strong>in</strong> a greater HIV-1 RNA response dur<strong>in</strong>g <strong>in</strong>itial doserang<strong>in</strong>gstudies as well as <strong>in</strong> cl<strong>in</strong>ical trials. This is not surpris<strong>in</strong>gs<strong>in</strong>ce <strong>the</strong> basic tenet <strong>of</strong> pharmacology is that a concentrationresponserelationship exists with all cl<strong>in</strong>ically active drugs.Under certa<strong>in</strong> circumstances, however, this relationship may notalways hold true. One is <strong>the</strong> presence <strong>of</strong> active metabolites thatcan contribute to <strong>the</strong> overall <strong>the</strong>rapeutic activity <strong>of</strong> <strong>the</strong> drug. Of<strong>the</strong> available protease <strong>in</strong>hibitors and NNRTIs, only nelf<strong>in</strong>avir isassociated with a measurable active metabolite <strong>in</strong> <strong>the</strong> plasma. 11<strong>The</strong> hydroxylated metabolite is designated as M-8 and is generatedby nelf<strong>in</strong>avir's oxidation by CYP2C19. 12 M-8 and nelf<strong>in</strong>avirhave equipotent <strong>in</strong> vitro activity aga<strong>in</strong>st HIV. At this po<strong>in</strong>t, it isunclear to what extent <strong>the</strong> M-8 metabolite contributes to <strong>the</strong>overall antiretroviral activity after nelf<strong>in</strong>avir adm<strong>in</strong>istration. It islikely that M-8 plasma b<strong>in</strong>d<strong>in</strong>g is significantly less than nelf<strong>in</strong>avirplasma b<strong>in</strong>d<strong>in</strong>g, so that <strong>the</strong> fraction <strong>of</strong> <strong>the</strong> drug that equilibrates<strong>in</strong>tracellularly may be higher for M-8 than for nelf<strong>in</strong>avir.More research is required s<strong>in</strong>ce <strong>in</strong> cl<strong>in</strong>ical use nelf<strong>in</strong>avir appearsto be more effective than what would be predicted from its plasmaconcentration alone.Prote<strong>in</strong> b<strong>in</strong>d<strong>in</strong>g is ano<strong>the</strong>r factor <strong>in</strong>fluenc<strong>in</strong>g <strong>the</strong> concentration-responserelationship for protease <strong>in</strong>hibitors becausechanges <strong>in</strong> overall b<strong>in</strong>d<strong>in</strong>g <strong>of</strong> <strong>the</strong>se drugs could affect <strong>the</strong> waytotal drug concentrations are <strong>in</strong>terpreted. HIV replication occurswith<strong>in</strong> cells, and protease <strong>in</strong>hibitors have to reach <strong>the</strong>ir <strong>in</strong>tracellulartarget for activity. At equilibrium, <strong>the</strong> unbound concentration<strong>of</strong> a drug <strong>in</strong> plasma should be equivalent to <strong>the</strong> unboundconcentration <strong>in</strong> <strong>the</strong> cell as long as <strong>the</strong>re are no energy-dependentpumps that can transport drugs aga<strong>in</strong>st a concentrationgradient. <strong>The</strong> importance <strong>of</strong> <strong>the</strong> unbound concentration <strong>of</strong> adrug for activity was clearly demonstrated by <strong>the</strong> lack <strong>of</strong> cl<strong>in</strong>icalactivity <strong>of</strong> <strong>the</strong> protease <strong>in</strong>hibitor SC-52151. 13 Because <strong>of</strong> its highdegree <strong>of</strong> prote<strong>in</strong> b<strong>in</strong>d<strong>in</strong>g, <strong>the</strong> drug showed no activity despiteachiev<strong>in</strong>g seem<strong>in</strong>gly adequate plasma concentration based on<strong>in</strong> vitro anti-HIV activity.Protease <strong>in</strong>hibitors are organic bases that are mostly bound<strong>in</strong> plasma to α 1 -acid glycoprote<strong>in</strong>s (AAGs), which are acutephasereactants whose concentrations <strong>in</strong>crease under conditions<strong>of</strong> <strong>in</strong>fection and acute <strong>in</strong>flammation. 14 <strong>The</strong> extent <strong>of</strong> prote<strong>in</strong>b<strong>in</strong>d<strong>in</strong>g <strong>of</strong> protease <strong>in</strong>hibitors is dependent upon <strong>the</strong> concentration<strong>of</strong> AAGs. 15 Higher concentrations <strong>of</strong> AAGs result <strong>in</strong><strong>in</strong>creased prote<strong>in</strong> b<strong>in</strong>d<strong>in</strong>g <strong>of</strong> protease <strong>in</strong>hibitors. Changes <strong>in</strong>prote<strong>in</strong> b<strong>in</strong>d<strong>in</strong>g for drugs like <strong>in</strong>d<strong>in</strong>avir, which is only 60% plasmabound, will not greatly affect plasma-unbound concentrationsand antiretroviral activity. In contrast, changes <strong>in</strong> prote<strong>in</strong>b<strong>in</strong>d<strong>in</strong>g for highly prote<strong>in</strong>-bound drugs, such as nelf<strong>in</strong>avir andlop<strong>in</strong>avir, will significantly alter <strong>the</strong>ir activity at an equivalentplasma concentration. Thus when total plasma concentration <strong>of</strong>a highly prote<strong>in</strong>-bound drug is <strong>in</strong>terpreted, <strong>the</strong> same concentrationwith variable prote<strong>in</strong> b<strong>in</strong>d<strong>in</strong>g may not translate <strong>in</strong>to equivalentantiretroviral activity. None<strong>the</strong>less, <strong>the</strong>re is some evidencethat <strong>the</strong> pharmacologic effect <strong>of</strong> protease <strong>in</strong>hibitors is proportionalto <strong>the</strong> plasma concentration <strong>in</strong> drug-naive subjects. 16<strong>The</strong> treatment <strong>of</strong> HIV <strong>in</strong>fection requires multiple drugs fordurable efficacy. For NNRTIs, <strong>the</strong> concentration-response relationshipis less firmly established, but data with efavirenz<strong>in</strong>creas<strong>in</strong>gly po<strong>in</strong>t <strong>in</strong> that direction. 7 It is presently unclear ifconcomitant use <strong>of</strong> all <strong>the</strong> nRTIs will result <strong>in</strong> an equivalentantiretroviral efficacy at a specific protease <strong>in</strong>hibitor or NNRTIconcentration. It is this high level <strong>of</strong> pharmacologic complexity<strong>in</strong> <strong>the</strong> treatment <strong>of</strong> HIV <strong>in</strong>fection that makes <strong>the</strong> relationshipbetween plasma concentration <strong>of</strong> protease <strong>in</strong>hibitors andantiretroviral response difficult to predict.<strong>The</strong> <strong>the</strong>rapeutic ranges for protease <strong>in</strong>hibitors and NNRTIsare difficult to evaluate because most drugs cannot be pushedto maximally tolerated doses. <strong>The</strong>re are both absorption andtolerability limitations for <strong>the</strong>se agents. It is likely that mostdrugs used <strong>in</strong> <strong>the</strong> treatment <strong>of</strong> HIV <strong>in</strong>fection have a narrowrange between <strong>the</strong> tolerated dose and <strong>the</strong> systemic concentrationrequired for durable suppression. Gatti and colleaguesclearly demonstrated that adverse effects <strong>of</strong> ritonavir are correlatedto both peak and trough concentrations. 17 <strong>The</strong> tolerability<strong>of</strong> ritonavir is dose dependent and most patients do not tolerate<strong>the</strong> usual dose necessary for durable antiretroviral efficacy,600 mg twice daily. Consequently, ritonavir is used ma<strong>in</strong>ly as ametabolic <strong>in</strong>hibitor <strong>of</strong> o<strong>the</strong>r protease <strong>in</strong>hibitors at a lower andbetter-tolerated dose.For nelf<strong>in</strong>avir, for which most <strong>of</strong> <strong>the</strong> toxicity is gastro<strong>in</strong>test<strong>in</strong>al,<strong>the</strong>re is no relationship between plasma concentration and<strong>the</strong> development <strong>of</strong> diarrhea. 18 Nephrotoxicity caused by <strong>in</strong>d<strong>in</strong>avirhas been related to a peak plasma concentration (C max )above 10 µg/mL. 19 S<strong>in</strong>ce <strong>in</strong>d<strong>in</strong>avir has a very short plasma halflife,a large amount <strong>of</strong> drug has to be adm<strong>in</strong>istered to ma<strong>in</strong>ta<strong>in</strong>adequate trough concentrations (C trough ). As a result, <strong>the</strong>peak/trough ratio for <strong>in</strong>d<strong>in</strong>avir is <strong>the</strong> highest among <strong>the</strong> protease<strong>in</strong>hibitors. <strong>The</strong> high C max <strong>of</strong> <strong>in</strong>d<strong>in</strong>avir can be manipulatedby us<strong>in</strong>g lower <strong>in</strong>d<strong>in</strong>avir doses with low-dose ritonavir to prolong<strong>the</strong> drug's plasma half-life. 20For NNRTIs, central nervous system (CNS) toxicity associatedwith efavirenz has been shown to be related to plasma concentration,and <strong>the</strong> concentration necessary for maximal activityis not far from <strong>the</strong> concentration that results <strong>in</strong> CNS toxicity. 7<strong>The</strong> presence or evolution <strong>of</strong> resistant viral stra<strong>in</strong>s willdeterm<strong>in</strong>e whe<strong>the</strong>r antiretroviral drugs exhibit a constant pharmacologiceffect over an extended period <strong>of</strong> time. <strong>The</strong> HIVreverse transcriptase gene does not conta<strong>in</strong> a “pro<strong>of</strong>read<strong>in</strong>g”mechanism, and as long as <strong>the</strong> virus is replicat<strong>in</strong>g, it can generatemutations that confer reduced susceptibility to antiretroviraldrugs. If viral replication is conta<strong>in</strong>ed, a constant pharmaco-29