The Potential Role of Therapeutic Drug Monitoring in the Treatment ...
The Potential Role of Therapeutic Drug Monitoring in the Treatment ...
The Potential Role of Therapeutic Drug Monitoring in the Treatment ...
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
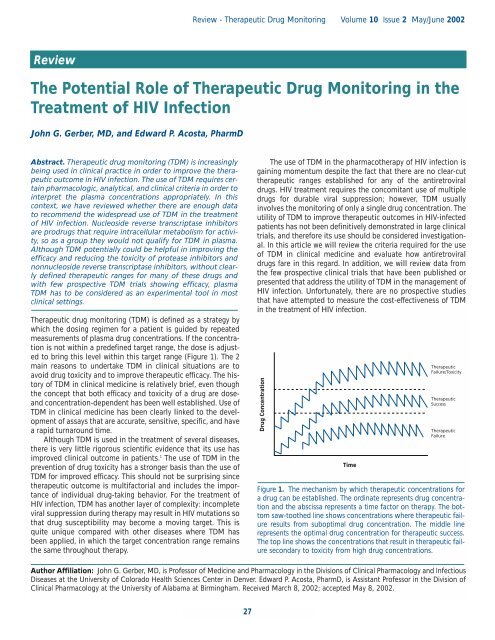
Review - <strong>The</strong>rapeutic <strong>Drug</strong> <strong>Monitor<strong>in</strong>g</strong> Volume 10 Issue 2 May/June 2002Review<strong>The</strong> <strong>Potential</strong> <strong>Role</strong> <strong>of</strong> <strong>The</strong>rapeutic <strong>Drug</strong> <strong>Monitor<strong>in</strong>g</strong> <strong>in</strong> <strong>the</strong><strong>Treatment</strong> <strong>of</strong> HIV InfectionJohn G. Gerber, MD, and Edward P. Acosta, PharmDAbstract. <strong>The</strong>rapeutic drug monitor<strong>in</strong>g (TDM) is <strong>in</strong>creas<strong>in</strong>glybe<strong>in</strong>g used <strong>in</strong> cl<strong>in</strong>ical practice <strong>in</strong> order to improve <strong>the</strong> <strong>the</strong>rapeuticoutcome <strong>in</strong> HIV <strong>in</strong>fection. <strong>The</strong> use <strong>of</strong> TDM requires certa<strong>in</strong>pharmacologic, analytical, and cl<strong>in</strong>ical criteria <strong>in</strong> order to<strong>in</strong>terpret <strong>the</strong> plasma concentrations appropriately. In thiscontext, we have reviewed whe<strong>the</strong>r <strong>the</strong>re are enough datato recommend <strong>the</strong> widespread use <strong>of</strong> TDM <strong>in</strong> <strong>the</strong> treatment<strong>of</strong> HIV <strong>in</strong>fection. Nucleoside reverse transcriptase <strong>in</strong>hibitorsare prodrugs that require <strong>in</strong>tracellular metabolism for activity,so as a group <strong>the</strong>y would not qualify for TDM <strong>in</strong> plasma.Although TDM potentially could be helpful <strong>in</strong> improv<strong>in</strong>g <strong>the</strong>efficacy and reduc<strong>in</strong>g <strong>the</strong> toxicity <strong>of</strong> protease <strong>in</strong>hibitors andnonnucleoside reverse transcriptase <strong>in</strong>hibitors, without clearlydef<strong>in</strong>ed <strong>the</strong>rapeutic ranges for many <strong>of</strong> <strong>the</strong>se drugs andwith few prospective TDM trials show<strong>in</strong>g efficacy, plasmaTDM has to be considered as an experimental tool <strong>in</strong> mostcl<strong>in</strong>ical sett<strong>in</strong>gs.<strong>The</strong>rapeutic drug monitor<strong>in</strong>g (TDM) is def<strong>in</strong>ed as a strategy bywhich <strong>the</strong> dos<strong>in</strong>g regimen for a patient is guided by repeatedmeasurements <strong>of</strong> plasma drug concentrations. If <strong>the</strong> concentrationis not with<strong>in</strong> a predef<strong>in</strong>ed target range, <strong>the</strong> dose is adjustedto br<strong>in</strong>g this level with<strong>in</strong> this target range (Figure 1). <strong>The</strong> 2ma<strong>in</strong> reasons to undertake TDM <strong>in</strong> cl<strong>in</strong>ical situations are toavoid drug toxicity and to improve <strong>the</strong>rapeutic efficacy. <strong>The</strong> history<strong>of</strong> TDM <strong>in</strong> cl<strong>in</strong>ical medic<strong>in</strong>e is relatively brief, even though<strong>the</strong> concept that both efficacy and toxicity <strong>of</strong> a drug are doseandconcentration-dependent has been well established. Use <strong>of</strong>TDM <strong>in</strong> cl<strong>in</strong>ical medic<strong>in</strong>e has been clearly l<strong>in</strong>ked to <strong>the</strong> development<strong>of</strong> assays that are accurate, sensitive, specific, and havea rapid turnaround time.Although TDM is used <strong>in</strong> <strong>the</strong> treatment <strong>of</strong> several diseases,<strong>the</strong>re is very little rigorous scientific evidence that its use hasimproved cl<strong>in</strong>ical outcome <strong>in</strong> patients. 1 <strong>The</strong> use <strong>of</strong> TDM <strong>in</strong> <strong>the</strong>prevention <strong>of</strong> drug toxicity has a stronger basis than <strong>the</strong> use <strong>of</strong>TDM for improved efficacy. This should not be surpris<strong>in</strong>g s<strong>in</strong>ce<strong>the</strong>rapeutic outcome is multifactorial and <strong>in</strong>cludes <strong>the</strong> importance<strong>of</strong> <strong>in</strong>dividual drug-tak<strong>in</strong>g behavior. For <strong>the</strong> treatment <strong>of</strong>HIV <strong>in</strong>fection, TDM has ano<strong>the</strong>r layer <strong>of</strong> complexity: <strong>in</strong>completeviral suppression dur<strong>in</strong>g <strong>the</strong>rapy may result <strong>in</strong> HIV mutations sothat drug susceptibility may become a mov<strong>in</strong>g target. This isquite unique compared with o<strong>the</strong>r diseases where TDM hasbeen applied, <strong>in</strong> which <strong>the</strong> target concentration range rema<strong>in</strong>s<strong>the</strong> same throughout <strong>the</strong>rapy.<strong>The</strong> use <strong>of</strong> TDM <strong>in</strong> <strong>the</strong> pharmaco<strong>the</strong>rapy <strong>of</strong> HIV <strong>in</strong>fection isga<strong>in</strong><strong>in</strong>g momentum despite <strong>the</strong> fact that <strong>the</strong>re are no clear-cut<strong>the</strong>rapeutic ranges established for any <strong>of</strong> <strong>the</strong> antiretroviraldrugs. HIV treatment requires <strong>the</strong> concomitant use <strong>of</strong> multipledrugs for durable viral suppression; however, TDM usually<strong>in</strong>volves <strong>the</strong> monitor<strong>in</strong>g <strong>of</strong> only a s<strong>in</strong>gle drug concentration. <strong>The</strong>utility <strong>of</strong> TDM to improve <strong>the</strong>rapeutic outcomes <strong>in</strong> HIV-<strong>in</strong>fectedpatients has not been def<strong>in</strong>itively demonstrated <strong>in</strong> large cl<strong>in</strong>icaltrials, and <strong>the</strong>refore its use should be considered <strong>in</strong>vestigational.In this article we will review <strong>the</strong> criteria required for <strong>the</strong> use<strong>of</strong> TDM <strong>in</strong> cl<strong>in</strong>ical medic<strong>in</strong>e and evaluate how antiretroviraldrugs fare <strong>in</strong> this regard. In addition, we will review data from<strong>the</strong> few prospective cl<strong>in</strong>ical trials that have been published orpresented that address <strong>the</strong> utility <strong>of</strong> TDM <strong>in</strong> <strong>the</strong> management <strong>of</strong>HIV <strong>in</strong>fection. Unfortunately, <strong>the</strong>re are no prospective studiesthat have attempted to measure <strong>the</strong> cost-effectiveness <strong>of</strong> TDM<strong>in</strong> <strong>the</strong> treatment <strong>of</strong> HIV <strong>in</strong>fection.<strong>Drug</strong> ConcentrationTime<strong>The</strong>rapeuticFailure/Toxicity<strong>The</strong>rapeuticSuccess<strong>The</strong>rapeuticFailureFigure 1. <strong>The</strong> mechanism by which <strong>the</strong>rapeutic concentrations fora drug can be established. <strong>The</strong> ord<strong>in</strong>ate represents drug concentrationand <strong>the</strong> abscissa represents a time factor on <strong>the</strong>rapy. <strong>The</strong> bottomsaw-too<strong>the</strong>d l<strong>in</strong>e shows concentrations where <strong>the</strong>rapeutic failureresults from suboptimal drug concentration. <strong>The</strong> middle l<strong>in</strong>erepresents <strong>the</strong> optimal drug concentration for <strong>the</strong>rapeutic success.<strong>The</strong> top l<strong>in</strong>e shows <strong>the</strong> concentrations that result <strong>in</strong> <strong>the</strong>rapeutic failuresecondary to toxicity from high drug concentrations.Author Affiliation: John G. Gerber, MD, is Pr<strong>of</strong>essor <strong>of</strong> Medic<strong>in</strong>e and Pharmacology <strong>in</strong> <strong>the</strong> Divisions <strong>of</strong> Cl<strong>in</strong>ical Pharmacology and InfectiousDiseases at <strong>the</strong> University <strong>of</strong> Colorado Health Sciences Center <strong>in</strong> Denver. Edward P. Acosta, PharmD, is Assistant Pr<strong>of</strong>essor <strong>in</strong> <strong>the</strong> Division <strong>of</strong>Cl<strong>in</strong>ical Pharmacology at <strong>the</strong> University <strong>of</strong> Alabama at Birm<strong>in</strong>gham. Received March 8, 2002; accepted May 8, 2002.27
International AIDS Society–USATopics <strong>in</strong> HIV Medic<strong>in</strong>eTable 1. Characteristics <strong>of</strong> Antiretroviral <strong>Drug</strong>s Applicablefor <strong>The</strong>rapeutic <strong>Drug</strong> <strong>Monitor<strong>in</strong>g</strong>CriteriaAnalytical<strong>Drug</strong> assay is accurate, specific, precise,requires small sample volume, yieldsrapid results, and is <strong>in</strong>expensivePharmacok<strong>in</strong>eticPharmacok<strong>in</strong>etic data are availableSignificant <strong>in</strong>terpatient pharmacok<strong>in</strong>eticvariability existsPharmacologicPharmacologic effect is related to drugconcentration<strong>Drug</strong> has a narrow <strong>the</strong>rapeutic <strong>in</strong>dex<strong>Drug</strong> has constant pharmacologic effectover extended period <strong>of</strong> timeCl<strong>in</strong>icalCl<strong>in</strong>ical studies have documented <strong>the</strong><strong>the</strong>rapeutic and toxic ranges <strong>of</strong> <strong>the</strong> drugCriteria for TDM Use <strong>in</strong> Cl<strong>in</strong>ical Medic<strong>in</strong>e<strong>The</strong> required criteria for <strong>the</strong> use <strong>of</strong> TDM <strong>in</strong> cl<strong>in</strong>ical medic<strong>in</strong>ewere described by Spector and colleagues <strong>in</strong> 1988. 2 <strong>The</strong>se criteriaare reviewed below <strong>in</strong> <strong>the</strong> context <strong>of</strong> antiretroviral drugs andcharacteristics that make drugs candidates for TDM (Table 1).Analytical CriteriaEvaluation√ <strong>in</strong>dicates sufficient data are available for antiretroviral drugs tomeet <strong>the</strong> specified criterion; ± <strong>in</strong>dicates some data are available but<strong>the</strong> criterion has not been met. *Depends on <strong>the</strong> extent <strong>of</strong> viral<strong>in</strong>hibition. Adapted from Spector et al, Cl<strong>in</strong> Pharmacol <strong>The</strong>r, 1988.A drug assay is available with high specificity, small sample volume requirements,reasonable cost, and rapid turnaround time.Very sensitive and specific assays are available for all <strong>the</strong> protease<strong>in</strong>hibitors, nonnucleoside reverse transcriptase <strong>in</strong>hibitors(NNRTIs), and nucleoside reverse transcriptase <strong>in</strong>hibitors(nRTIs) us<strong>in</strong>g high-performance liquid chromatography withultraviolet (HPLC-UV) detection or liquid chromatography-massspectrometry/mass spectrometry (LC-MS/MS). However, nRTIsare more complex than protease <strong>in</strong>hibitors and NNRTIs s<strong>in</strong>ce<strong>the</strong>y circulate <strong>in</strong> <strong>the</strong> plasma as prodrugs and require <strong>in</strong>tracellularphosphorylation to <strong>the</strong> active triphosphate metabolite. As aresult, plasma concentrations <strong>of</strong> nRTIs may not always reflectactivity <strong>in</strong> <strong>the</strong> <strong>in</strong>tracellular compartment. A good example isdidanos<strong>in</strong>e, which has a very short plasma half-life but a long<strong>in</strong>tracellular half-life and duration <strong>of</strong> action. 3 S<strong>in</strong>ce it has been√√√√±±*±very difficult to measure accurately <strong>the</strong> <strong>in</strong>tracellular concentrations<strong>of</strong> many nRTI triphosphates, nRTIs may not be good candidatesfor TDM and thus will not be <strong>in</strong>cluded <strong>in</strong> <strong>the</strong> discussion<strong>of</strong> <strong>the</strong> o<strong>the</strong>r criteria for TDM. <strong>The</strong> analytical criteria required forapplication <strong>of</strong> TDM is met by <strong>the</strong> protease <strong>in</strong>hibitors andNNRTIs; <strong>the</strong> cost and turnaround time criteria will likely be metas more laboratories undertake <strong>the</strong> analysis <strong>of</strong> <strong>the</strong>se drugs.Pharmacok<strong>in</strong>etic Criteria<strong>The</strong>re is significant <strong>in</strong>ter<strong>in</strong>dividual variability <strong>in</strong> pharmacok<strong>in</strong>etics, result<strong>in</strong>g<strong>in</strong> large variability <strong>in</strong> achieved plasma concentrations. Adequate pharmacok<strong>in</strong>eticdata concern<strong>in</strong>g <strong>the</strong> drug are available.Although a fixed dose is adm<strong>in</strong>istered to all adults tak<strong>in</strong>g protease<strong>in</strong>hibitors and NNRTIs, large variability <strong>in</strong> achieved plasmaconcentrations has been well documented for all <strong>the</strong> drugs<strong>in</strong> cl<strong>in</strong>ical use. 4-7 A number <strong>of</strong> pharmacok<strong>in</strong>etic studies havebeen conducted on currently available antiretroviral drugs asreviewed <strong>in</strong> a recent position paper on TDM. 8 All protease<strong>in</strong>hibitors have large <strong>in</strong>tersubject variability <strong>in</strong> achieved plasmaconcentration follow<strong>in</strong>g fixed-dose adm<strong>in</strong>istration (Figure 2).This variability becomes a concern when <strong>the</strong> achieved troughconcentration is below <strong>the</strong> concentration necessary for <strong>in</strong>hibition<strong>of</strong> viral replication, <strong>the</strong>reby creat<strong>in</strong>g <strong>the</strong> potential for <strong>the</strong>evolution <strong>of</strong> drug-resistant isolates. Adm<strong>in</strong>istration <strong>of</strong> ritonavirwith o<strong>the</strong>r protease <strong>in</strong>hibitors tends to reduce <strong>the</strong> pharmacok<strong>in</strong>eticvariability <strong>of</strong> <strong>the</strong> protease <strong>in</strong>hibitors, but <strong>the</strong> <strong>in</strong>tersubjectvariability still rema<strong>in</strong>s high. 9 Large <strong>in</strong>ter<strong>in</strong>dividual variability isalso present with achieved plasma concentrations <strong>of</strong> NNRTIs,yet it is unclear whe<strong>the</strong>r failure <strong>of</strong> NNRTI-based <strong>the</strong>rapy is dueto low plasma concentrations. Achieved plasma concentrationsfor nevirap<strong>in</strong>e are orders <strong>of</strong> magnitude higher than what isrequired for viral <strong>in</strong>hibition <strong>in</strong> vitro. 10 However, quasi specieswith high-level drug resistance circulate as m<strong>in</strong>ority stra<strong>in</strong>s, and<strong>the</strong>refore adequate exposure to concomitant nRTIs is likely crucial<strong>in</strong> ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g successful <strong>the</strong>rapy with most <strong>of</strong> <strong>the</strong> NNRTIs.Ind<strong>in</strong>avir Concentration (µM)201510500 1 2 3 4 5 6 7 8Time (hours)Figure 2. <strong>The</strong> extreme variability <strong>of</strong> <strong>the</strong> pharmacok<strong>in</strong>etics <strong>of</strong> a protease<strong>in</strong>hibitor (<strong>in</strong>d<strong>in</strong>avir) follow<strong>in</strong>g standard dos<strong>in</strong>g (800 mg q8h).Similar data show<strong>in</strong>g large <strong>in</strong>tersubject variability <strong>in</strong> pharmacok<strong>in</strong>eticsare available for o<strong>the</strong>r protease <strong>in</strong>hibitors. Adapted with permissionfrom Acosta et al, Pharmaco<strong>the</strong>rapy, 1999.28
Review - <strong>The</strong>rapeutic <strong>Drug</strong> <strong>Monitor<strong>in</strong>g</strong> Volume 10 Issue 2 May/June 2002<strong>The</strong>re are many reasons beh<strong>in</strong>d pharmacok<strong>in</strong>etic variability<strong>of</strong> <strong>the</strong>se lipophilic drugs. <strong>The</strong>re is undoubtedly variability <strong>in</strong>drug solubilization and absorption from <strong>the</strong> <strong>in</strong>test<strong>in</strong>al tract.Multidrug-resistant prote<strong>in</strong>s such as P-glycoprote<strong>in</strong> likelyimpede <strong>the</strong> bioavailability <strong>of</strong> protease <strong>in</strong>hibitors. In addition,<strong>the</strong> large variability <strong>of</strong> CYP3A expression <strong>in</strong> <strong>the</strong> small <strong>in</strong>test<strong>in</strong>eand <strong>the</strong> liver can result <strong>in</strong> significant variability <strong>in</strong> <strong>the</strong> drug'sbioavailability and systemic clearance. Based upon <strong>the</strong> large<strong>in</strong>tersubject pharmacok<strong>in</strong>etic variability <strong>of</strong> protease <strong>in</strong>hibitorsand NNRTIs and <strong>the</strong> sufficient data available on <strong>the</strong>ir pharmacok<strong>in</strong>eticpr<strong>of</strong>iles, both drug classes qualify for TDM.Pharmacologic CriteriaPharmacologic effect is proportional to <strong>the</strong> plasma drug concentration. Anarrow range exists between <strong>the</strong> efficacious and toxic concentrations. A constantpharmacologic effect over an extended period <strong>of</strong> time exists.Higher plasma concentrations <strong>of</strong> protease <strong>in</strong>hibitors haveresulted <strong>in</strong> a greater HIV-1 RNA response dur<strong>in</strong>g <strong>in</strong>itial doserang<strong>in</strong>gstudies as well as <strong>in</strong> cl<strong>in</strong>ical trials. This is not surpris<strong>in</strong>gs<strong>in</strong>ce <strong>the</strong> basic tenet <strong>of</strong> pharmacology is that a concentrationresponserelationship exists with all cl<strong>in</strong>ically active drugs.Under certa<strong>in</strong> circumstances, however, this relationship may notalways hold true. One is <strong>the</strong> presence <strong>of</strong> active metabolites thatcan contribute to <strong>the</strong> overall <strong>the</strong>rapeutic activity <strong>of</strong> <strong>the</strong> drug. Of<strong>the</strong> available protease <strong>in</strong>hibitors and NNRTIs, only nelf<strong>in</strong>avir isassociated with a measurable active metabolite <strong>in</strong> <strong>the</strong> plasma. 11<strong>The</strong> hydroxylated metabolite is designated as M-8 and is generatedby nelf<strong>in</strong>avir's oxidation by CYP2C19. 12 M-8 and nelf<strong>in</strong>avirhave equipotent <strong>in</strong> vitro activity aga<strong>in</strong>st HIV. At this po<strong>in</strong>t, it isunclear to what extent <strong>the</strong> M-8 metabolite contributes to <strong>the</strong>overall antiretroviral activity after nelf<strong>in</strong>avir adm<strong>in</strong>istration. It islikely that M-8 plasma b<strong>in</strong>d<strong>in</strong>g is significantly less than nelf<strong>in</strong>avirplasma b<strong>in</strong>d<strong>in</strong>g, so that <strong>the</strong> fraction <strong>of</strong> <strong>the</strong> drug that equilibrates<strong>in</strong>tracellularly may be higher for M-8 than for nelf<strong>in</strong>avir.More research is required s<strong>in</strong>ce <strong>in</strong> cl<strong>in</strong>ical use nelf<strong>in</strong>avir appearsto be more effective than what would be predicted from its plasmaconcentration alone.Prote<strong>in</strong> b<strong>in</strong>d<strong>in</strong>g is ano<strong>the</strong>r factor <strong>in</strong>fluenc<strong>in</strong>g <strong>the</strong> concentration-responserelationship for protease <strong>in</strong>hibitors becausechanges <strong>in</strong> overall b<strong>in</strong>d<strong>in</strong>g <strong>of</strong> <strong>the</strong>se drugs could affect <strong>the</strong> waytotal drug concentrations are <strong>in</strong>terpreted. HIV replication occurswith<strong>in</strong> cells, and protease <strong>in</strong>hibitors have to reach <strong>the</strong>ir <strong>in</strong>tracellulartarget for activity. At equilibrium, <strong>the</strong> unbound concentration<strong>of</strong> a drug <strong>in</strong> plasma should be equivalent to <strong>the</strong> unboundconcentration <strong>in</strong> <strong>the</strong> cell as long as <strong>the</strong>re are no energy-dependentpumps that can transport drugs aga<strong>in</strong>st a concentrationgradient. <strong>The</strong> importance <strong>of</strong> <strong>the</strong> unbound concentration <strong>of</strong> adrug for activity was clearly demonstrated by <strong>the</strong> lack <strong>of</strong> cl<strong>in</strong>icalactivity <strong>of</strong> <strong>the</strong> protease <strong>in</strong>hibitor SC-52151. 13 Because <strong>of</strong> its highdegree <strong>of</strong> prote<strong>in</strong> b<strong>in</strong>d<strong>in</strong>g, <strong>the</strong> drug showed no activity despiteachiev<strong>in</strong>g seem<strong>in</strong>gly adequate plasma concentration based on<strong>in</strong> vitro anti-HIV activity.Protease <strong>in</strong>hibitors are organic bases that are mostly bound<strong>in</strong> plasma to α 1 -acid glycoprote<strong>in</strong>s (AAGs), which are acutephasereactants whose concentrations <strong>in</strong>crease under conditions<strong>of</strong> <strong>in</strong>fection and acute <strong>in</strong>flammation. 14 <strong>The</strong> extent <strong>of</strong> prote<strong>in</strong>b<strong>in</strong>d<strong>in</strong>g <strong>of</strong> protease <strong>in</strong>hibitors is dependent upon <strong>the</strong> concentration<strong>of</strong> AAGs. 15 Higher concentrations <strong>of</strong> AAGs result <strong>in</strong><strong>in</strong>creased prote<strong>in</strong> b<strong>in</strong>d<strong>in</strong>g <strong>of</strong> protease <strong>in</strong>hibitors. Changes <strong>in</strong>prote<strong>in</strong> b<strong>in</strong>d<strong>in</strong>g for drugs like <strong>in</strong>d<strong>in</strong>avir, which is only 60% plasmabound, will not greatly affect plasma-unbound concentrationsand antiretroviral activity. In contrast, changes <strong>in</strong> prote<strong>in</strong>b<strong>in</strong>d<strong>in</strong>g for highly prote<strong>in</strong>-bound drugs, such as nelf<strong>in</strong>avir andlop<strong>in</strong>avir, will significantly alter <strong>the</strong>ir activity at an equivalentplasma concentration. Thus when total plasma concentration <strong>of</strong>a highly prote<strong>in</strong>-bound drug is <strong>in</strong>terpreted, <strong>the</strong> same concentrationwith variable prote<strong>in</strong> b<strong>in</strong>d<strong>in</strong>g may not translate <strong>in</strong>to equivalentantiretroviral activity. None<strong>the</strong>less, <strong>the</strong>re is some evidencethat <strong>the</strong> pharmacologic effect <strong>of</strong> protease <strong>in</strong>hibitors is proportionalto <strong>the</strong> plasma concentration <strong>in</strong> drug-naive subjects. 16<strong>The</strong> treatment <strong>of</strong> HIV <strong>in</strong>fection requires multiple drugs fordurable efficacy. For NNRTIs, <strong>the</strong> concentration-response relationshipis less firmly established, but data with efavirenz<strong>in</strong>creas<strong>in</strong>gly po<strong>in</strong>t <strong>in</strong> that direction. 7 It is presently unclear ifconcomitant use <strong>of</strong> all <strong>the</strong> nRTIs will result <strong>in</strong> an equivalentantiretroviral efficacy at a specific protease <strong>in</strong>hibitor or NNRTIconcentration. It is this high level <strong>of</strong> pharmacologic complexity<strong>in</strong> <strong>the</strong> treatment <strong>of</strong> HIV <strong>in</strong>fection that makes <strong>the</strong> relationshipbetween plasma concentration <strong>of</strong> protease <strong>in</strong>hibitors andantiretroviral response difficult to predict.<strong>The</strong> <strong>the</strong>rapeutic ranges for protease <strong>in</strong>hibitors and NNRTIsare difficult to evaluate because most drugs cannot be pushedto maximally tolerated doses. <strong>The</strong>re are both absorption andtolerability limitations for <strong>the</strong>se agents. It is likely that mostdrugs used <strong>in</strong> <strong>the</strong> treatment <strong>of</strong> HIV <strong>in</strong>fection have a narrowrange between <strong>the</strong> tolerated dose and <strong>the</strong> systemic concentrationrequired for durable suppression. Gatti and colleaguesclearly demonstrated that adverse effects <strong>of</strong> ritonavir are correlatedto both peak and trough concentrations. 17 <strong>The</strong> tolerability<strong>of</strong> ritonavir is dose dependent and most patients do not tolerate<strong>the</strong> usual dose necessary for durable antiretroviral efficacy,600 mg twice daily. Consequently, ritonavir is used ma<strong>in</strong>ly as ametabolic <strong>in</strong>hibitor <strong>of</strong> o<strong>the</strong>r protease <strong>in</strong>hibitors at a lower andbetter-tolerated dose.For nelf<strong>in</strong>avir, for which most <strong>of</strong> <strong>the</strong> toxicity is gastro<strong>in</strong>test<strong>in</strong>al,<strong>the</strong>re is no relationship between plasma concentration and<strong>the</strong> development <strong>of</strong> diarrhea. 18 Nephrotoxicity caused by <strong>in</strong>d<strong>in</strong>avirhas been related to a peak plasma concentration (C max )above 10 µg/mL. 19 S<strong>in</strong>ce <strong>in</strong>d<strong>in</strong>avir has a very short plasma halflife,a large amount <strong>of</strong> drug has to be adm<strong>in</strong>istered to ma<strong>in</strong>ta<strong>in</strong>adequate trough concentrations (C trough ). As a result, <strong>the</strong>peak/trough ratio for <strong>in</strong>d<strong>in</strong>avir is <strong>the</strong> highest among <strong>the</strong> protease<strong>in</strong>hibitors. <strong>The</strong> high C max <strong>of</strong> <strong>in</strong>d<strong>in</strong>avir can be manipulatedby us<strong>in</strong>g lower <strong>in</strong>d<strong>in</strong>avir doses with low-dose ritonavir to prolong<strong>the</strong> drug's plasma half-life. 20For NNRTIs, central nervous system (CNS) toxicity associatedwith efavirenz has been shown to be related to plasma concentration,and <strong>the</strong> concentration necessary for maximal activityis not far from <strong>the</strong> concentration that results <strong>in</strong> CNS toxicity. 7<strong>The</strong> presence or evolution <strong>of</strong> resistant viral stra<strong>in</strong>s willdeterm<strong>in</strong>e whe<strong>the</strong>r antiretroviral drugs exhibit a constant pharmacologiceffect over an extended period <strong>of</strong> time. <strong>The</strong> HIVreverse transcriptase gene does not conta<strong>in</strong> a “pro<strong>of</strong>read<strong>in</strong>g”mechanism, and as long as <strong>the</strong> virus is replicat<strong>in</strong>g, it can generatemutations that confer reduced susceptibility to antiretroviraldrugs. If viral replication is conta<strong>in</strong>ed, a constant pharmaco-29
International AIDS Society–USA Topics <strong>in</strong> HIV Medic<strong>in</strong>elogic effect over an extended period <strong>of</strong> time does <strong>in</strong>deed occurfor both <strong>the</strong> protease <strong>in</strong>hibitors and <strong>the</strong> NNRTIs. If mutated andphenotypically less susceptible viral stra<strong>in</strong>s evolve dur<strong>in</strong>g <strong>the</strong>rapy,<strong>the</strong> pharmacologic effect is not constant over even a shortperiod <strong>of</strong> time. Higher concentrations <strong>of</strong> drugs may need to beachieved to control viral replication to <strong>the</strong> same extent as dur<strong>in</strong>g<strong>in</strong>itial <strong>the</strong>rapy.Based on <strong>the</strong>se pharmacologic criteria, <strong>the</strong> applicability <strong>of</strong>TDM to antiretroviral drugs is variable. S<strong>in</strong>ce treatment <strong>of</strong> HIV<strong>in</strong>fection requires <strong>the</strong> concomitant use <strong>of</strong> multiple drugs, monitor<strong>in</strong>gonly a s<strong>in</strong>gle drug (eg, a protease <strong>in</strong>hibitor or NNRTI)may not be appropriate. Both <strong>the</strong> <strong>the</strong>rapeutic efficacy and <strong>the</strong>toxicity <strong>of</strong> protease <strong>in</strong>hibitors and NNRTIs may demonstratesynergy, antagonism, or additive effects when comb<strong>in</strong>ed with<strong>the</strong> various nRTIs or each o<strong>the</strong>r. <strong>The</strong> presence <strong>of</strong> basel<strong>in</strong>e m<strong>in</strong>oritydrug-resistant mutations and <strong>the</strong> evolution <strong>of</strong> drug resistanceover time can make <strong>the</strong> concentration necessary forantiretroviral efficacy a mov<strong>in</strong>g target.Cl<strong>in</strong>ical CriteriaCl<strong>in</strong>ical studies exist that def<strong>in</strong>e <strong>the</strong> <strong>the</strong>rapeutic and toxic ranges <strong>of</strong> <strong>the</strong> drug.A <strong>the</strong>rapeutic range has not been formally def<strong>in</strong>ed for all drugs<strong>in</strong> cl<strong>in</strong>ical use for HIV, but concentration-response data areavailable for most <strong>of</strong> <strong>the</strong> protease <strong>in</strong>hibitors and NNRTIs. Oneproblem is <strong>the</strong> uncerta<strong>in</strong>ty as to which pharmacok<strong>in</strong>etic parameterbest def<strong>in</strong>es <strong>the</strong> <strong>the</strong>rapeutic and toxic exposures <strong>of</strong> <strong>the</strong>drugs. <strong>The</strong> C trough is usually monitored to determ<strong>in</strong>e adequatedrug exposure because it is <strong>the</strong> easiest to collect for both <strong>the</strong>patient and <strong>the</strong> <strong>in</strong>vestigator; however, this parameter requiresan accurate recall <strong>of</strong> when <strong>the</strong> last dose <strong>of</strong> <strong>the</strong> drug was adm<strong>in</strong>istered.Calculat<strong>in</strong>g an accurate area-under-<strong>the</strong>-curve valuewould require obta<strong>in</strong><strong>in</strong>g specimens over an extended period <strong>of</strong>time, which is unrealistic <strong>in</strong> a busy cl<strong>in</strong>ical sett<strong>in</strong>g. Logically,C trough should def<strong>in</strong>e <strong>the</strong> lowest drug concentration dur<strong>in</strong>g adosage <strong>in</strong>terval and thus def<strong>in</strong>e <strong>the</strong> m<strong>in</strong>imum effective concentration<strong>of</strong> <strong>the</strong> drug, but this has not been prospectively validatedfor any <strong>of</strong> <strong>the</strong> antiretroviral drugs.In terms <strong>of</strong> toxicity, <strong>the</strong> trough and <strong>the</strong> peak drug concentrationseach may play an important role. For example, C max maybest approximate <strong>the</strong> risk <strong>of</strong> <strong>in</strong>d<strong>in</strong>avir-<strong>in</strong>duced nephrotoxicity, 19but o<strong>the</strong>r toxicities such as sk<strong>in</strong> and nail abnormalities may berelated to total drug exposure. Marzol<strong>in</strong>i and colleaguesattempted to def<strong>in</strong>e <strong>the</strong> <strong>the</strong>rapeutic range <strong>of</strong> efavirenz by retrospectivelycorrelat<strong>in</strong>g CNS toxicity with plasma concentrations<strong>in</strong> a small group <strong>of</strong> subjects, some <strong>of</strong> whom were experienc<strong>in</strong>gvirologic failure. 7 Although this may be one way to def<strong>in</strong>e <strong>the</strong><strong>the</strong>rapeutic ranges for drugs, prospective studies that validate<strong>the</strong>se drug concentrations with observations <strong>of</strong> efficacy and toxicitywould certa<strong>in</strong>ly streng<strong>the</strong>n <strong>the</strong> argument for TDM.In drug-naive subjects, <strong>the</strong> C trough necessary for cont<strong>in</strong>uedviral suppression has been def<strong>in</strong>ed best for <strong>in</strong>d<strong>in</strong>avir. This concentrationis approximately 100 ng/mL, which is close to <strong>the</strong>prote<strong>in</strong>-b<strong>in</strong>d<strong>in</strong>g-corrected 95% <strong>in</strong>hibitory concentration for <strong>in</strong>d<strong>in</strong>avir<strong>in</strong> vitro. 16 However, <strong>the</strong> determ<strong>in</strong>ation <strong>of</strong> <strong>the</strong> C trough necessaryfor durable virologic suppression is made <strong>in</strong> <strong>the</strong> presence<strong>of</strong> concomitant nRTIs, and whe<strong>the</strong>r all <strong>of</strong> <strong>the</strong> nRTIs <strong>in</strong>teract with<strong>the</strong> protease <strong>in</strong>hibitors at <strong>the</strong> same potency <strong>in</strong> vivo has not beenstudied. Abacavir, for example, which is a much more potentantiretroviral drug than stavud<strong>in</strong>e, may quantitatively contributeto successful <strong>the</strong>rapy more than stavud<strong>in</strong>e when usedconcomitantly with protease <strong>in</strong>hibitors. 21,22Prospective Cl<strong>in</strong>ical Trials<strong>The</strong>re are only a few prospective studies that have exam<strong>in</strong>ed <strong>the</strong>utility <strong>of</strong> TDM <strong>in</strong> <strong>the</strong> treatment <strong>of</strong> HIV. ATHENA was a prospectivetrial <strong>of</strong> TDM <strong>in</strong> which analyses <strong>of</strong> a subgroup <strong>of</strong> patients on<strong>in</strong>d<strong>in</strong>avir or nelf<strong>in</strong>avir were performed. 23 N<strong>in</strong>ety-two treatmentnaivepatients were randomized to receive nelf<strong>in</strong>avir 1250 mgtwice daily us<strong>in</strong>g TDM or no TDM. A concentration ratio (CR)was used to assess drug exposure and make dos<strong>in</strong>g modifications<strong>in</strong> <strong>the</strong> TDM group. A measured drug level (drawn at anytime follow<strong>in</strong>g an unobserved dose) was compared with a populationaverage concentration-time curve. A ratio <strong>of</strong> 1 meant <strong>the</strong>patient’s concentration was <strong>the</strong> same as <strong>the</strong> population averageon that occasion. If <strong>the</strong> first nelf<strong>in</strong>avir CR was less than 0.9, tak<strong>in</strong>g<strong>the</strong> drug with food was discussed with <strong>the</strong> patient. If <strong>the</strong>subsequent CR rema<strong>in</strong>ed less than 0.9, <strong>the</strong> dose was <strong>in</strong>creasedto 1500 mg twice daily, and low-dose ritonavir was added if <strong>the</strong>third CR was low. <strong>The</strong> average turnaround time for <strong>the</strong> assayresults was 4 weeks.By <strong>in</strong>tent-to-treat (ITT) analysis, <strong>the</strong> proportions <strong>of</strong> patientsachiev<strong>in</strong>g plasma HIV-1 RNA levels below 500 copies/mL at 1year were 81% and 59% <strong>in</strong> <strong>the</strong> TDM and no-TDM groups, respectively(P=.03). <strong>The</strong> authors suggested that <strong>the</strong>se results reflecteddifferences <strong>in</strong> drug efficacy because <strong>the</strong> ma<strong>in</strong> reason for drugdiscont<strong>in</strong>uation <strong>in</strong> <strong>the</strong> no-TDM group was virologic failure,which was more frequent for <strong>the</strong> no-TDM group.<strong>The</strong> ATHENA study also exam<strong>in</strong>ed <strong>the</strong> effect <strong>of</strong> TDM <strong>in</strong> subjectsreceiv<strong>in</strong>g <strong>in</strong>d<strong>in</strong>avir 800 mg 3 times a day, <strong>in</strong>d<strong>in</strong>avir 800 mgwith 100 mg ritonavir twice daily, or <strong>in</strong>d<strong>in</strong>avir plus ritonavir at400 mg each twice daily. <strong>The</strong> acceptable CR for <strong>in</strong>d<strong>in</strong>avir wasdef<strong>in</strong>ed as 0.75 to 2.0. This analysis showed more favorable outcomes<strong>in</strong> <strong>the</strong> group randomized to TDM. By ITT analysis, 75%and 48% <strong>of</strong> subjects had plasma HIV-1 RNA levels below 500copies/mL <strong>in</strong> <strong>the</strong> TDM and no-TDM arms, respectively, at 1 year.This difference was secondary to toxicity, s<strong>in</strong>ce <strong>the</strong>re were veryfew virologic failures and far fewer subjects <strong>in</strong> <strong>the</strong> TDM armdropped out <strong>of</strong> <strong>the</strong> study for toxicity reasons than those <strong>in</strong> <strong>the</strong>no-TDM arm. <strong>The</strong>se data suggest that TDM may be potentiallyuseful <strong>in</strong> <strong>the</strong> management <strong>of</strong> antiretroviral <strong>the</strong>rapy for both efficacyand toxicity reasons. Although <strong>the</strong>se substudies <strong>of</strong> <strong>the</strong>ATHENA trial had positive results, concerns rema<strong>in</strong> regard<strong>in</strong>g<strong>the</strong> statistical power <strong>of</strong> <strong>the</strong> study to detect differences betweengroups and whe<strong>the</strong>r cl<strong>in</strong>icians truly followed dose change recommendations.PharmAdapt was a prospective study compar<strong>in</strong>g <strong>the</strong> use <strong>of</strong>TDM versus no TDM <strong>in</strong> treatment-experienced patients <strong>in</strong> whom<strong>the</strong>rapy failed. 24,25 A total <strong>of</strong> 257 subjects enrolled <strong>in</strong> this study,but <strong>the</strong> presented data were limited to 180 subjects receiv<strong>in</strong>gprotease <strong>in</strong>hibitor-conta<strong>in</strong><strong>in</strong>g regimens. N<strong>in</strong>ety-six subjectswere <strong>in</strong> <strong>the</strong> control group and 84 subjects were <strong>in</strong> <strong>the</strong> TDMgroup. All subjects had genotypic resistance test<strong>in</strong>g prior to randomization,and drug <strong>the</strong>rapy was determ<strong>in</strong>ed on <strong>the</strong> basis <strong>of</strong><strong>the</strong>se results. <strong>The</strong> TDM group had a dose modification at week8 based on week 4 trough concentrations. <strong>The</strong> targeted protease30
International AIDS Society–USA Topics <strong>in</strong> HIV Medic<strong>in</strong>eIn <strong>the</strong> treatment <strong>of</strong> drug-experienced subjects who havedrug-resistant virus, determ<strong>in</strong><strong>in</strong>g a prote<strong>in</strong>-corrected IC 50 maybe useful. Apply<strong>in</strong>g TDM to <strong>the</strong>n achieve a concentration several-foldabove that IC 50 would seem reasonable. Evaluation <strong>of</strong> <strong>the</strong><strong>in</strong>hibitory quotient (IQ), <strong>in</strong> which <strong>the</strong> phenotypic sensitivity <strong>of</strong><strong>the</strong> virus to <strong>the</strong> drug and <strong>the</strong> plasma concentration <strong>of</strong> <strong>the</strong> drugdeterm<strong>in</strong>e <strong>the</strong> IQ, is be<strong>in</strong>g studied <strong>in</strong> cl<strong>in</strong>ical trials. Welldesignedand adequately powered prospective studies need tobe performed before IQ can be generally recommended for cl<strong>in</strong>icalpractice.<strong>The</strong> important message about TDM is that it may ultimatelyprove useful, but at this time <strong>the</strong>re are not enough data to recommendits use outside <strong>of</strong> very specific circumstances. TDMshould currently be viewed as an <strong>in</strong>vestigational tool to exploremeans <strong>of</strong> improv<strong>in</strong>g <strong>the</strong>rapeutic outcome and reduc<strong>in</strong>g toxicities<strong>in</strong> <strong>the</strong> treatment <strong>of</strong> HIV <strong>in</strong>fection.F<strong>in</strong>ancial Disclosure: Dr Gerber has served as a consultant to Agouron, Merck, RocheDiagnostics, and Roche Pharma. Dr Acosta has served as a consultant to Bristol-MyersSquibb, Merck, and Roche.References1. Schumacher GE, Barr JT. Economic and outcome issues for <strong>the</strong>rapeuticdrug monitor<strong>in</strong>g <strong>in</strong> medic<strong>in</strong>e. <strong>The</strong>r <strong>Drug</strong> Monit. 1998;20:539-542.2. Spector R, Park GD, Johnson GF, Vesell ES. <strong>The</strong>rapeutic drug monitor<strong>in</strong>g.Cl<strong>in</strong> Pharmacol <strong>The</strong>r. 1988;43:345-353.3. Morse GD, Shelton MJ, O'Donnell AM. Comparative pharmacok<strong>in</strong>etics <strong>of</strong>antiviral nucleoside analogues. Cl<strong>in</strong> Pharmacok<strong>in</strong>et. 1993;24:101-123.4. Acosta EP, Henry K, Baken L, Page LM, Fletcher CV. Ind<strong>in</strong>avir concentrationsand antiviral effect. Pharmaco<strong>the</strong>rapy. 1999;19:708-712.5. Baede-van Dijk PA, Hugen PW, Verweij-van Wissen CP, Koopmans PP,Burger DM, Hekster YA. Analysis <strong>of</strong> variation <strong>in</strong> plasma concentrations <strong>of</strong>nelf<strong>in</strong>avir and its active metabolite M8 <strong>in</strong> HIV-positive patients. AIDS.2001;15:991-998.6. Zhou XJ, She<strong>in</strong>er LB, D'Aquila RT, et al. Population pharmacok<strong>in</strong>etics <strong>of</strong>nevirap<strong>in</strong>e, zidovud<strong>in</strong>e, and didanos<strong>in</strong>e <strong>in</strong> human immunodeficiency virus<strong>in</strong>fectedpatients. <strong>The</strong> National Institute <strong>of</strong> Allergy and Infectious DiseasesAIDS Cl<strong>in</strong>ical Trials Group Protocol 241 Investigators. Antimicrob AgentsChemo<strong>the</strong>r. 1999;43:121-128.7. Marzol<strong>in</strong>i C, Telenti A, Decosterd LA, Greub G, Biollaz J, Bucl<strong>in</strong> T. Efavirenzplasma levels can predict treatment failure and central nervous system sideeffects <strong>in</strong> HIV-1-<strong>in</strong>fected patients. AIDS. 2001;15:71-75.8. Acosta EP, Gerber JG. Position paper on <strong>the</strong>rapeutic drug monitor<strong>in</strong>g <strong>of</strong>antiretroviral agents. AIDS Res Hum Retroviruses. In Press.9. Burger DM, Hugen PW, Aarnoutse RE, et al. A retrospective, cohort-basedsurvey <strong>of</strong> patients us<strong>in</strong>g twice-daily <strong>in</strong>d<strong>in</strong>avir + ritonavir comb<strong>in</strong>ations:pharmacok<strong>in</strong>etics, safety, and efficacy. J Acquir Immune Defic Syndr.2001;26:218-224.10. Havlir D, Cheeseman SH, McLaughl<strong>in</strong> M, et al. High-dose nevirap<strong>in</strong>e:safety, pharmacok<strong>in</strong>etics, and antiviral effect <strong>in</strong> patients with humanimmunodeficiency virus <strong>in</strong>fection. J Infect Dis. 1995;171:537-545.11. Zhang KE, Wu E, Patick AK, et al. Circulat<strong>in</strong>g metabolites <strong>of</strong> <strong>the</strong> humanimmunodeficiency virus protease <strong>in</strong>hibitor nelf<strong>in</strong>avir <strong>in</strong> humans: structuralidentification, levels <strong>in</strong> plasma, and antiviral activities. Antimicrob AgentsChemo<strong>the</strong>r. 2001;45:1086-1093.12. Lillibridge JH, Lee CA, Pithavala YK. <strong>The</strong> role <strong>of</strong> CYP2C19 <strong>in</strong> <strong>the</strong> formation<strong>of</strong> nelf<strong>in</strong>avir hydroxyl-t-butylamide (M8): <strong>in</strong> vitro/<strong>in</strong> vivo correlation.[Abstract 109.] 5th International ISSX Meet<strong>in</strong>g. October 25-29, 1998; Cairns,Australia.13. Fischl MA, Richman DD, Flexner C, et al. Phase I/II study <strong>of</strong> <strong>the</strong> toxicity,pharmacok<strong>in</strong>etics, and activity <strong>of</strong> <strong>the</strong> HIV protease <strong>in</strong>hibitor SC-52151. JAcquir Immune Defic Syndr Hum Retrovirol. 1997;15:28-34.14. Israili ZH, Dayton PG. Human alpha-1-glycoprote<strong>in</strong> and its <strong>in</strong>teractionswith drugs. <strong>Drug</strong> Metab Rev. 2001;33:161-235.15. Zhang XQ, Schooley RT, Gerber JG. <strong>The</strong> effect <strong>of</strong> <strong>in</strong>creas<strong>in</strong>g alpha1-acidglycoprote<strong>in</strong> concentration on <strong>the</strong> antiviral efficacy <strong>of</strong> human immunodeficiencyvirus protease <strong>in</strong>hibitors. J Infect Dis. 1999;180:1833-1837.16. Acosta EP, Havlir DV, Richman DD, et al. Pharmacodynamics (PD) <strong>of</strong><strong>in</strong>d<strong>in</strong>avir (IDV) <strong>in</strong> protease-naive HIV-<strong>in</strong>fected patients receiv<strong>in</strong>g ZDV and3TC. [Abstract 455.] 7th Conference on Retroviruses and OpportunisticInfections. January 30-February 2, 2000; San Francisco, Calif.17. Gatti G, Di Biagio A, Casazza R, et al. <strong>The</strong> relationship between ritonavirplasma levels and side-effects: implications for <strong>the</strong>rapeutic drug monitor<strong>in</strong>g.AIDS. 1999;13:2083-2089.18. Hsyu PH, Flexner C, Chu A, Petersen C. Correlation <strong>of</strong> efficacy, nelf<strong>in</strong>avirpharmacok<strong>in</strong>etics and diarrhea <strong>in</strong> treatment-naive HIV positive patientsreceiv<strong>in</strong>g nelf<strong>in</strong>avir, zidovud<strong>in</strong>e and lamivud<strong>in</strong>e. [Abstract 1735.] 41stInterscience Conference on Antimicrobial Agents and Chemo<strong>the</strong>rapy.December 16-19, 2001; Chicago, Ill.19. Dieleman JP, Gyssens IC, van der Ende ME, de Marie S, Burger DM.Urological compla<strong>in</strong>ts <strong>in</strong> relation to <strong>in</strong>d<strong>in</strong>avir plasma concentrations <strong>in</strong> HIV<strong>in</strong>fectedpatients. AIDS. 1999;13:473-478.20. Hsu A, Granneman GR, Cao G, et al. Pharmacok<strong>in</strong>etic <strong>in</strong>teractionbetween ritonavir and <strong>in</strong>d<strong>in</strong>avir <strong>in</strong> healthy volunteers. Antimicrob AgentsChemo<strong>the</strong>r. 1998;42:2784-2791.21. Saag MS, Sonnerborg A, Torres RA, et al. Antiretroviral effect and safety<strong>of</strong> abacavir and abacavir <strong>in</strong> comb<strong>in</strong>ation with zidovud<strong>in</strong>e <strong>in</strong> HIV-<strong>in</strong>fectedadults. AIDS. 1998;12:F202-F209.22. Kuritzkes DR, Marschner I, Johnson VA, et al. Lamivud<strong>in</strong>e <strong>in</strong> comb<strong>in</strong>ationwith zidovud<strong>in</strong>e, stavud<strong>in</strong>e, or didanos<strong>in</strong>e <strong>in</strong> patients with HIV-1 <strong>in</strong>fection.A randomized, double-bl<strong>in</strong>d, placebo-controlled trial. National Institute <strong>of</strong>Allergy and Infectious Disease AIDS Cl<strong>in</strong>ical Trials Group Protocol 306Investigators. AIDS. 1999;13:685-694.23. Burger DM, Hugen PWH, Droste J, Huitema ADR. <strong>The</strong>rapeutic drug monitor<strong>in</strong>g<strong>of</strong> nelf<strong>in</strong>avir 1250 mg bid <strong>in</strong> treatment naive patients improves <strong>the</strong>rapeuticoutcome after 1 year: results from ATHENA. [Abstract 6.26.] 2ndInternational Workshop on Cl<strong>in</strong>ical Pharmacology <strong>of</strong> HIV <strong>The</strong>rapy. April 2-4,2001; Noordwijk, Ne<strong>the</strong>rlands.24. Clevenbergh P, Durant J, Garraffo R, et al. Usefulness <strong>of</strong> protease<strong>in</strong>hibitor <strong>the</strong>rapeutic drug monitor<strong>in</strong>g? PharmAdapt: a prospective multicentricrandomized controlled trial: 12 weeks results. [Abstract 260B.] 8thConference on Retroviruses and Opportunistic Infections. February 4-8,2001; Chicago, Ill.25. Clevenbergh P, Garraffo R, Durant J, et al. Long term efficacy <strong>of</strong> protease<strong>in</strong>hibitor plasma drug levels monitor<strong>in</strong>g (PI TDM): PharmAdapt W 32 results.[Abstract 1730.] 41st Interscience Conference on Antimicrobial Agents andChemo<strong>the</strong>rapy. December 16-19, 2001; Chicago, Ill.26. Fletcher CV, Anderson PL, Kakuda TN, et al. Concentration-controlledcompared with conventional antiretroviral <strong>the</strong>rapy for HIV <strong>in</strong>fection. AIDS.2002;16:551-560.27. Fischl M, Castro J, Monroig R, et al. Impact <strong>of</strong> directly observed <strong>the</strong>rapylong-term outcomes <strong>in</strong> HIV cl<strong>in</strong>ical trials. [Abstract 528.] 8th Conference onRetroviruses and Opportunistic Infections. February 4-8, 2001; Chicago, Ill.32