<strong>of</strong> body armor, uniform and clothing, but little else. They mayeven be considered an added resource for extra ammunition, asthey can carry heavier loads than the operators who must moveat lightning speed in tight confines. Whether these medics shouldbe armed is a matter for the individual departments, and may bedetermined by pre-existing policies, and, in some cases, state law.Having at least one sidearm for each medic, however, would likelyresult in the lives <strong>of</strong> police, medics and innocent victims beingsaved at some point.2The next level <strong>of</strong> advancement in training and ability is increasedtactical awareness and understanding for all fire/rescue and EMS personnel. Although these individualsdon’t need the expertise <strong>of</strong> the tactical medics, they must be aware<strong>of</strong> what tactics patrol <strong>of</strong>ficers employ when entering a building,clearing and securing areas, handling hostages and woundedsuspects, withdrawing under fire, and working in small teams.This will greatly enhance the ability <strong>of</strong> the two groups to operatetogether in active shooter situations, particularly in those jurisdictionswhere it’s likely patrol will arrive ahead <strong>of</strong> SWAT. Thesemedical pr<strong>of</strong>essionals will not require extreme tactical knowledge,but they will need sufficient knowledge to ensure they canget their medical expertise to where it’s needed, while under fire,and without interfering with those engaged in combat. These pr<strong>of</strong>essionalscan also receive all <strong>of</strong> the training they need <strong>from</strong> thevery departments they will be assisting.3And finally, just as the medics must be trained in combattactics by the police, the police must also be trained in superiorfirst aid by the medics. Police must be better at renderingaid to their law enforcement comrades, themselves and thevictims. In a battle environment where police can expect to suffercasualties at the rate <strong>of</strong> one cop for every five terrorists shot (as theRussian special forces do), in addition to dozens (and even hundreds)<strong>of</strong> dead and dying victims, medics assigned to police willbe overwhelmed. At Norris Hall, there were two tactical medicswho would have had to treat 55 people if the police had not beensufficiently trained.To develop this evolution in training does not require largebudgets for equipment or six-figure DHS grants. What it doesrequire, however, is the willingness to train, and a desire to bebetter than we are now. In advancing the skill level in the twocritical areas <strong>of</strong> tactics and medicine-under-fire, we can, onceagain, turn to the model <strong>of</strong> the Army Special Forces, in which thefirst duty <strong>of</strong> each specialist is to teach his expert skill set to all <strong>of</strong>the other members <strong>of</strong> the team, so that any one team member canstep in and do another’s job if that person is wounded or killed.Police <strong>of</strong>ficers, paramedics, EMS personnel and firefighterscan ill afford a different attitude in the battles America is yet t<strong>of</strong>ight on her own soil. While some advances in equipment will behelpful, the real requirements are dedication, discipline and awillingness to commit time and effort.For these reasons, both North American Rescue Inc. (NAR)and the Archangel Group Ltd. have been working to prepareAmerica’s warriors to be able to do just that: kill and rescue. Since9/11, Archangel has trained thousands <strong>of</strong> police, soldiers, andstate and federal agents in unprecedented and innovative waysto conduct these battles against a committed, well-prepared anddeadly enemy.At the same time, NAR has been workingwith the most elite Special Operations soldiersand sailors who are conducting operations inour overseas combat zones to provide the mostadvanced, efficacious casualty care and extractiontechniques for combat at home—techniquesthat represent an enormous evolutionin casualty care <strong>from</strong> early conventional firstaid and CPR.Together, these organizations have forged aset <strong>of</strong> common skills that have joint tactical andmedical applications. No police <strong>of</strong>ficer, SWAToperator, firefighter or paramedic can be withoutthis skill set. New, and inexpensive, evacuationand medical equipment is now availablethat every police <strong>of</strong>ficer, soldier, medic, EMSpr<strong>of</strong>essional and firefighter can benefit <strong>from</strong>.Cutting-edge training in TCCC is nowavailable to everyone. No longer is this equipmentand training limited only to our elitemilitary Special Operations Forces. Nor canwe afford for it to be, because police <strong>of</strong>ficers,paramedics and firefighters are the ones wewill be turning to when this enemy returns.The enemy has promised us the deaths <strong>of</strong>millions <strong>of</strong> American citizens—including ourown children—before this war is over. Theonly way to prevent them <strong>from</strong> reaching thatgoal is our ability to kill them and rescue andresuscitate our own; for our enemy will allowus no other solution.John Giduck is a senior consultant with the ArchangelGroup (www.antiterrorconsultants.org), an agencythat provides training to U.S. law enforcement,government agencies and military. He has a lawdegree and a master’s degree in Russian studies, andhas worked with several Russian special forces units.He authored Terror at Beslan and co-authoredthe newly released The Green Beret in You:Living with Total Commitment to Family,Career, Sports and Life. Currently he’s finishinga doctoral dissertation on the global expansion <strong>of</strong>radical Islam. Giduck has reported no conflicts <strong>of</strong>interest related to the sponsor <strong>of</strong> this supplement,North American Rescue.Editor’s Note: The author’s book, Terror atBeslan: A Russian Tragedy with <strong>Lessons</strong>for America’s Schools, provides a detailedaccount <strong>of</strong> the events at the Beslan school siege.Learn more at:www.antiterrorconsultants.org/terror_beslan.htm.References:1. Giduck J: Terror At Beslan: A Russian Tragedywith <strong>Lessons</strong> for America’s Schools. ArchangelPublishing Group Inc.: Golden, Colorado, 2005.2. Ahlers MM: “Agency says 7,000 sites at ‘high risk’<strong>of</strong> terrorist attack.” CNN.com News Report, June21, 2008.10 War on TraumaJournal <strong>of</strong> Emergency Medical Services
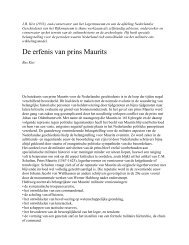
Photo <strong>of</strong>fice <strong>of</strong> medical history/Surgeon GeneralWWIIWWIPhoto <strong>of</strong>fice <strong>of</strong> medical history/Surgeon General“It is appropriate that experienceduring unavoidable ‘epidemics <strong>of</strong>trauma’ be exploited in improvingour national capability to providebetter surgical and medical care forour citizens. ”Spurgeon Neel,Colonel, Medical Corps, U.S. Army 1Though EMS as medical treatment <strong>of</strong> apatient prior to and during transportationto the hospital may have roots datingback centuries, it is only since Napoleon’sEuropean campaigns that we can draw a directline <strong>from</strong> his system for moving combat casualtiesto today’s EMS. Napoleon’s physician,Dominique-Jean Larrey, developed a systemspecifically for transportation <strong>of</strong> battle casualties(the “flying” ambulance), which was introducedinto the U.S. Army during the Civil War.Photo APVietnamIraq &AfghanistanPhoto courtesy SSG Fredrick GoldackerBy Daved van Stralen, MDIn the trench warfare <strong>of</strong> WWI, the U.S. Armyassigned nonphysicians to the trenches for treatment<strong>of</strong> casualties. In WWII, these first aid menentered combat, becoming the corpsmen andcombat medics in service today.During WWII, the Army also introducedair transport <strong>of</strong> the injured; this developmentwas followed by helicopter transport directly<strong>from</strong> the scene <strong>of</strong> injury to the hospital in theKorean <strong>Conflict</strong> and the Vietnam War. Asalluded to in Col. Neel’s 1968 statement, each<strong>of</strong> these advances in prehospital care came<strong>from</strong> the epidemic <strong>of</strong> trauma that occursduring military combat.Elsevier Public Safety War on Trauma 11