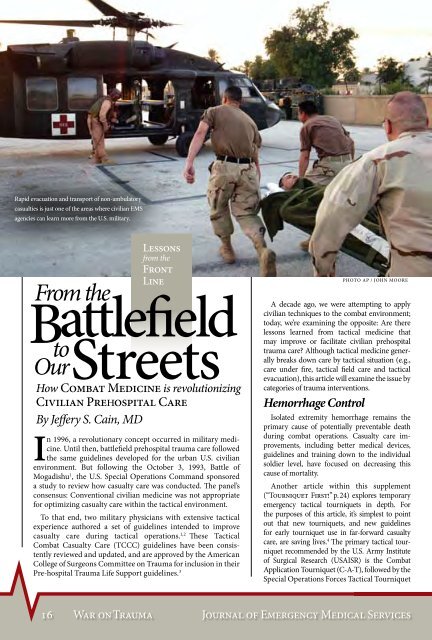
Rapid evacuation and transport <strong>of</strong> non-ambulatorycasualties is just one <strong>of</strong> the areas where civilian EMSagencies can learn more <strong>from</strong> the U.S. military.Photo AP / John MooreBy Jeffery S. Cain, MDIn 1996, a revolutionary concept occurred in military medicine.Until then, battlefield prehospital trauma care followedthe same guidelines developed for the urban U.S. civilianenvironment. But following the October 3, 1993, Battle <strong>of</strong>Mogadishu 1 , the U.S. Special Operations Command sponsoreda study to review how casualty care was conducted. The panel’sconsensus: Conventional civilian medicine was not appropriatefor optimizing casualty care within the tactical environment.To that end, two military physicians with extensive tacticalexperience authored a set <strong>of</strong> guidelines intended to improvecasualty care during tactical operations. 1,2 These TacticalCombat Casualty Care (TCCC) guidelines have been consistentlyreviewed and updated, and are approved by the AmericanCollege <strong>of</strong> Surgeons Committee on Trauma for inclusion in theirPre-hospital Trauma Life Support guidelines. 3A decade ago, we were attempting to applycivilian techniques to the combat environment;today, we’re examining the opposite: Are therelessons learned <strong>from</strong> tactical medicine thatmay improve or facilitate civilian prehospitaltrauma care? Although tactical medicine generallybreaks down care by tactical situation (e.g.,care under fire, tactical field care and tacticalevacuation), this article will examine the issue bycategories <strong>of</strong> trauma interventions.Hemorrhage ControlIsolated extremity hemorrhage remains theprimary cause <strong>of</strong> potentially preventable deathduring combat operations. Casualty care improvements,including better medical devices,guidelines and training down to the individualsoldier level, have focused on decreasing thiscause <strong>of</strong> mortality.Another article within this supplement(“Tourniquet First!” p.24) explores temporaryemergency tactical tourniquets in depth. Forthe purposes <strong>of</strong> this article, it’s simplest to pointout that new tourniquets, and new guidelinesfor early tourniquet use in far-forward casualtycare, are saving lives. 4 The primary tactical tourniquetrecommended by the U.S. Army Institute<strong>of</strong> Surgical Research (USAISR) is the CombatApplication Tourniquet (C-A-T), followed by theSpecial Operations Forces Tactical Tourniquet16 War on TraumaJournal <strong>of</strong> Emergency Medical Services
Delphi®EMTEmergency& MedicalPneumaticTourniquetC-A-T® CombatApplication Tourniquet®(SOF-TT). The Delphi Emergency & MedicalTourniquet (EMT) is the primary pneumatictourniquet used with fixed surgical facilitiesand unit aid stations. 5,6,7Compression bandages are widely usedthroughout the military. Several new commercialproducts represent a significant improvementover older, non-compression style bandages.These newer devices all incorporate a non-adherentbandage in the form <strong>of</strong> an elastic wrap tail.Sequential wrapping <strong>of</strong> the elastic tail generatesa compressive force that, when combined withgauze packing, creates an extremely efficient andeffective pressure bandage. TheEmergency Bandage by First CareProducts was the first <strong>of</strong> thesemodern compression bandages togain widespread acceptance.The Emergency Trauma Dressingby North American Rescue(NAR) represents a significantdesign improvement over olderdevices. 8 This elastic compressionwrap is a tighter weave and generatesgreater compressive force.The wrap’s “Quick Grip” feature(Velcro® enclosures equally spacedalong the wrap) prevents the entirewrap <strong>from</strong> unrolling prematurelyif the wrap is accidentally droppedduring application.Certain wound locations—such as the proximalextremities,axilla, groin, torsoand neck—makeit difficult to controlhemorrhage with directpressure and compressiondressings; tourniquets are alsoineffective in many <strong>of</strong> these areas.Researchers have developed severalnew tools and clinical guidelines to address thiscritical issue. Over the past few years, a number <strong>of</strong>hemostatic agents, in both bandage and powderform, have been developed that actually arrest lifethreateningarterial hemorrhage. 9,10,11The most recent research conducted by both the Army and Navyresearch centers compared more than 10 types <strong>of</strong> hemostatic agentsfor controlling arterial hemorrhage in animal models. One granularproduct (WoundStat, manufactured by Trauma Cure) was found to havea 100% survival rate for subjects with wounds that would otherwisebe fatal. Another product, an improved gauze impregnated with akaolin substance (Combat Gauze, manufactured by Z-Medica), demonstratedgreater than 80% efficacy in independent lab presentationsto the research committee. This product is actually a pro-coagulant thatpromotes blood clotting.These newer hemostatic agents are proving to be both more effectiveand less expensive than those previously approved by the TCCCcommittee. In clinical trials, WoundStat showed the highestclinical efficacy, yet it is a granular-based product,which is problematic to adequatelyapply during tactical operations.Combat Gauze showed the nexthighest efficacy. Both were superiorto the benchmark HemCon andQuikClot. Celox, a granular chitosan-basedagent, also outperformedboth HemCon and QuikClot inboth USAIR and Naval Research LabStudies. Note: This data was taken <strong>from</strong>the “Comparative Testing and Analysis<strong>of</strong> New Hemostatic Agents in LethalInjury Models” presentation, which providespre-published data <strong>from</strong> the NavyResearch Lab and the Army Institute<strong>of</strong> Surgical Research to the TCCCcommittee.ETDCompressionBandageHowever, Celox didn’t performas well as WoundStat or CombatGauze. It’s a lighter weight powderthan WoundStat, which makes applicationto arterial hemorrhage injurydifficult.Based upon the results <strong>of</strong> thesestudies and input <strong>from</strong> combat medicsregarding device preferences, the TCCCcommittee revised its recommendations. Thenewest guideline change is to utilize CombatGauze as the primary hemostatic agent, withWoundStat as the backup or when thewound characteristics are moreamenable to a granular agent.Hemostatic Agents:Combat GauzeWoundStatElsevier Public Safety War on Trauma 17