Cancer Reform Strategy - NHS Cancer Screening Programmes
Cancer Reform Strategy - NHS Cancer Screening Programmes
Cancer Reform Strategy - NHS Cancer Screening Programmes
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
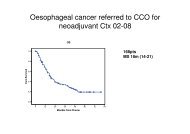
90 CANCER REFORM STRATEGYnot offered the chance to be treated in clinicaltrials. Implementation of the ImprovingOutcomes Guidance on Children & YoungPeople with <strong>Cancer</strong> should ensure that children& young people, are treated in centres where acomplete portfolio of relevant trials is supported.6.34 Children and younger people who developcancer will have very different needs and it willbe important that care for them is provided inan age appropriate setting. For teenagers andyoung adults with cancer, it is estimated that70% are not treated in a setting appropriate fortheir age. Implementation of the Children andYoung People’s Improving Outcomes Guidance(IOG) will therefore require provision of asufficient number of dedicated age appropriateservices to ensure that every network has aservice to refer to. More than one service maybe needed in high density populations. Goodcommissioners will ensure that services are ageappropriate for the population they serve.Gender and cancer6.35 Some cancers are gender specific (such asprostate and testicular for men, ovary anduterus for women) and others affect one genderfar more than the other (such as breast cancer).However, for the ten commonest cancers whichaffect both men and women age standardisedmortality rates are in every case higher in men.6.36 The reasons for the differences in mortalityrates between men and women are not fullyunderstood. In some cancers, such as lungcancer and oesophageal cancer, differences insmoking prevalence play a large part. In someother cancers, it may be due to laterpresentation by men. In melanoma for example,the incidence is higher in women, possiblybecause of the greater over exposure tosunlight, but death rates are higher in men,perhaps due to presentation at a moreadvanced stage.6.37 In 2006, a symposium organised by theMen’s Health Forum and chaired by the National<strong>Cancer</strong> Director discussed the issues aroundcancer and gender. The event highlighted thatthere are still many cancer types for which thereason for higher incidence and mortality in menis not known and that this higher incidence maybe the result of unidentified risk factors orgeneral biological predisposition. 40 It is clear thatmore research is needed if we are to fullyunderstand how gender impacts on cancer.6.38 The Symposium also highlighted that therange of settings in which men are offeredadvice, information and routine health checksshould be expanded from traditional primaryand secondary care settings, for example intothe workplace.Figure 11: Age standardised mortality per 100,000 populationMenWomenLung 55.8 28.4Colorectal 24.0 14.7Oesophagus 13.0 5.1Stomach 10.9 4.3Pancreas 9.6 7.3Bladder 9.1 3.0Non-Hodgkin’s Lymphoma 7.5 4.7Leukaemia 6.8 4.3Kidney 6.1 2.3Melanoma 2.7 1.9