

Neurology New Patient Welcome Packet - Mount Sinai Hospital
Neurology New Patient Welcome Packet - Mount Sinai Hospital
Neurology New Patient Welcome Packet - Mount Sinai Hospital
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
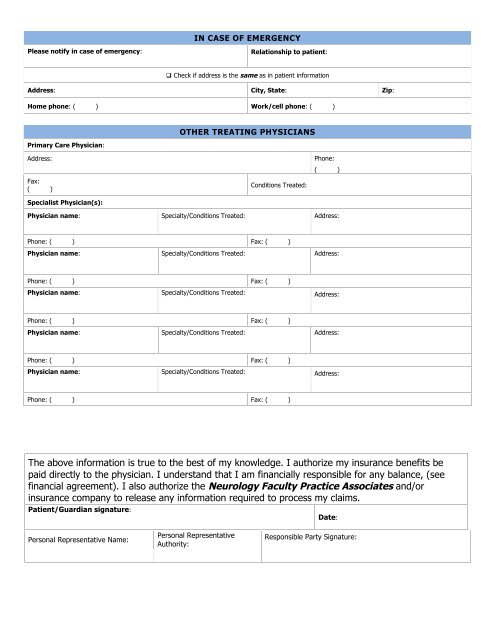
IN CASE OF EMERGENCYPlease notify in case of emergency:Relationship to patient: Check if address is the same as in patient informationAddress: City, State: Zip:Home phone: ( ) Work/cell phone: ( )Primary Care Physician:OTHER TREATING PHYSICIANSAddress:Fax:( )Specialist Physician(s):Conditions Treated:Phone:( )Physician name: Specialty/Conditions Treated: Address:Phone: ( ) Fax: ( )Physician name: Specialty/Conditions Treated: Address:Phone: ( ) Fax: ( )Physician name:Specialty/Conditions Treated:Address:Phone: ( ) Fax: ( )Physician name: Specialty/Conditions Treated: Address:Phone: ( ) Fax: ( )Physician name:Specialty/Conditions Treated:Address:Phone: ( ) Fax: ( )The above information is true to the best of my knowledge. I authorize my insurance benefits bepaid directly to the physician. I understand that I am financially responsible for any balance, (seefinancial agreement). I also authorize the <strong>Neurology</strong> Faculty Practice Associates and/orinsurance company to release any information required to process my claims.<strong>Patient</strong>/Guardian signature:Date:Personal Representative Name:Personal RepresentativeAuthority:Responsible Party Signature:
![December 2, 2012 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/51092274/1/190x245/december-2-2012-pdf-mount-sinai-hospital.jpg?quality=85)
![January 21, 2013 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/50916550/1/190x245/january-21-2013-pdf-mount-sinai-hospital.jpg?quality=85)
![February 3, 2013 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/50584982/1/190x245/february-3-2013-pdf-mount-sinai-hospital.jpg?quality=85)
![March 18, 2012 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/50462098/1/190x245/march-18-2012-pdf-mount-sinai-hospital.jpg?quality=85)

![Partners Program Guide [PDF] - Mount Sinai Hospital](https://img.yumpu.com/49411954/1/190x245/partners-program-guide-pdf-mount-sinai-hospital.jpg?quality=85)

![March 19 - April 1, 2012 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/48990923/1/190x245/march-19-april-1-2012-pdf-mount-sinai-hospital.jpg?quality=85)
![PGY-1 Residency Application [PDF] - Mount Sinai Hospital](https://img.yumpu.com/48577701/1/190x245/pgy-1-residency-application-pdf-mount-sinai-hospital.jpg?quality=85)


