

Neurology New Patient Welcome Packet - Mount Sinai Hospital
Neurology New Patient Welcome Packet - Mount Sinai Hospital
Neurology New Patient Welcome Packet - Mount Sinai Hospital
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
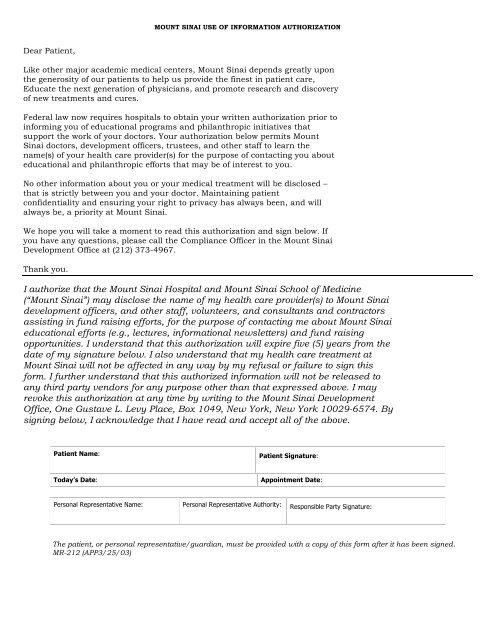
MOUNT SINAI USE OF INFORMATION AUTHORIZATIONDear <strong>Patient</strong>,Like other major academic medical centers, <strong>Mount</strong> <strong>Sinai</strong> depends greatly uponthe generosity of our patients to help us provide the finest in patient care,Educate the next generation of physicians, and promote research and discoveryof new treatments and cures.Federal law now requires hospitals to obtain your written authorization prior toinforming you of educational programs and philanthropic initiatives thatsupport the work of your doctors. Your authorization below permits <strong>Mount</strong><strong>Sinai</strong> doctors, development officers, trustees, and other staff to learn thename(s) of your health care provider(s) for the purpose of contacting you abouteducational and philanthropic efforts that may be of interest to you.No other information about you or your medical treatment will be disclosed –that is strictly between you and your doctor. Maintaining patientconfidentiality and ensuring your right to privacy has always been, and willalways be, a priority at <strong>Mount</strong> <strong>Sinai</strong>.We hope you will take a moment to read this authorization and sign below. Ifyou have any questions, please call the Compliance Officer in the <strong>Mount</strong> <strong>Sinai</strong>Development Office at (212) 373-4967.Thank you.I authorize that the <strong>Mount</strong> <strong>Sinai</strong> <strong>Hospital</strong> and <strong>Mount</strong> <strong>Sinai</strong> School of Medicine(“<strong>Mount</strong> <strong>Sinai</strong>”) may disclose the name of my health care provider(s) to <strong>Mount</strong> <strong>Sinai</strong>development officers, and other staff, volunteers, and consultants and contractorsassisting in fund raising efforts, for the purpose of contacting me about <strong>Mount</strong> <strong>Sinai</strong>educational efforts (e.g., lectures, informational newsletters) and fund raisingopportunities. I understand that this authorization will expire five (5) years from thedate of my signature below. I also understand that my health care treatment at<strong>Mount</strong> <strong>Sinai</strong> will not be affected in any way by my refusal or failure to sign thisform. I further understand that this authorized information will not be released toany third party vendors for any purpose other than that expressed above. I mayrevoke this authorization at any time by writing to the <strong>Mount</strong> <strong>Sinai</strong> DevelopmentOffice, One Gustave L. Levy Place, Box 1049, <strong>New</strong> York, <strong>New</strong> York 10029-6574. Bysigning below, I acknowledge that I have read and accept all of the above.<strong>Patient</strong> Name:<strong>Patient</strong> Signature:Today’s Date:Appointment Date:Personal Representative Name: Personal Representative Authority: Responsible Party Signature:The patient, or personal representative/guardian, must be provided with a copy of this form after it has been signed.MR-212 (APP3/25/03)
![December 2, 2012 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/51092274/1/190x245/december-2-2012-pdf-mount-sinai-hospital.jpg?quality=85)
![January 21, 2013 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/50916550/1/190x245/january-21-2013-pdf-mount-sinai-hospital.jpg?quality=85)
![February 3, 2013 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/50584982/1/190x245/february-3-2013-pdf-mount-sinai-hospital.jpg?quality=85)
![March 18, 2012 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/50462098/1/190x245/march-18-2012-pdf-mount-sinai-hospital.jpg?quality=85)

![Partners Program Guide [PDF] - Mount Sinai Hospital](https://img.yumpu.com/49411954/1/190x245/partners-program-guide-pdf-mount-sinai-hospital.jpg?quality=85)

![March 19 - April 1, 2012 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/48990923/1/190x245/march-19-april-1-2012-pdf-mount-sinai-hospital.jpg?quality=85)
![PGY-1 Residency Application [PDF] - Mount Sinai Hospital](https://img.yumpu.com/48577701/1/190x245/pgy-1-residency-application-pdf-mount-sinai-hospital.jpg?quality=85)


