

Neurology New Patient Welcome Packet - Mount Sinai Hospital
Neurology New Patient Welcome Packet - Mount Sinai Hospital
Neurology New Patient Welcome Packet - Mount Sinai Hospital
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
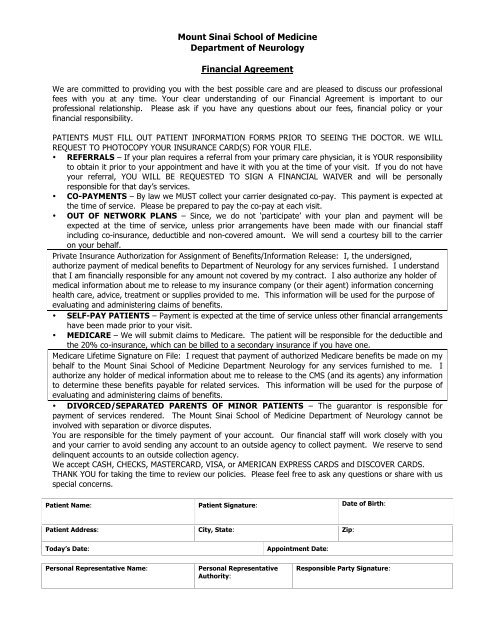
<strong>Mount</strong> <strong>Sinai</strong> School of MedicineDepartment of <strong>Neurology</strong>Financial AgreementWe are committed to providing you with the best possible care and are pleased to discuss our professionalfees with you at any time. Your clear understanding of our Financial Agreement is important to ourprofessional relationship. Please ask if you have any questions about our fees, financial policy or yourfinancial responsibility.PATIENTS MUST FILL OUT PATIENT INFORMATION FORMS PRIOR TO SEEING THE DOCTOR. WE WILLREQUEST TO PHOTOCOPY YOUR INSURANCE CARD(S) FOR YOUR FILE.• REFERRALS – If your plan requires a referral from your primary care physician, it is YOUR responsibilityto obtain it prior to your appointment and have it with you at the time of your visit. If you do not haveyour referral, YOU WILL BE REQUESTED TO SIGN A FINANCIAL WAIVER and will be personallyresponsible for that day’s services.• CO-PAYMENTS – By law we MUST collect your carrier designated co-pay. This payment is expected atthe time of service. Please be prepared to pay the co-pay at each visit.• OUT OF NETWORK PLANS – Since, we do not ‘participate’ with your plan and payment will beexpected at the time of service, unless prior arrangements have been made with our financial staffincluding co-insurance, deductible and non-covered amount. We will send a courtesy bill to the carrieron your behalf.Private Insurance Authorization for Assignment of Benefits/Information Release: I, the undersigned,authorize payment of medical benefits to Department of <strong>Neurology</strong> for any services furnished. I understandthat I am financially responsible for any amount not covered by my contract. I also authorize any holder ofmedical information about me to release to my insurance company (or their agent) information concerninghealth care, advice, treatment or supplies provided to me. This information will be used for the purpose ofevaluating and administering claims of benefits.• SELF-PAY PATIENTS – Payment is expected at the time of service unless other financial arrangementshave been made prior to your visit.• MEDICARE – We will submit claims to Medicare. The patient will be responsible for the deductible andthe 20% co-insurance, which can be billed to a secondary insurance if you have one.Medicare Lifetime Signature on File: I request that payment of authorized Medicare benefits be made on mybehalf to the <strong>Mount</strong> <strong>Sinai</strong> School of Medicine Department <strong>Neurology</strong> for any services furnished to me. Iauthorize any holder of medical information about me to release to the CMS (and its agents) any informationto determine these benefits payable for related services. This information will be used for the purpose ofevaluating and administering claims of benefits.• DIVORCED/SEPARATED PARENTS OF MINOR PATIENTS – The guarantor is responsible forpayment of services rendered. The <strong>Mount</strong> <strong>Sinai</strong> School of Medicine Department of <strong>Neurology</strong> cannot beinvolved with separation or divorce disputes.You are responsible for the timely payment of your account. Our financial staff will work closely with youand your carrier to avoid sending any account to an outside agency to collect payment. We reserve to senddelinquent accounts to an outside collection agency.We accept CASH, CHECKS, MASTERCARD, VISA, or AMERICAN EXPRESS CARDS and DISCOVER CARDS.THANK YOU for taking the time to review our policies. Please feel free to ask any questions or share with usspecial concerns.<strong>Patient</strong> Name: <strong>Patient</strong> Signature: Date of Birth:<strong>Patient</strong> Address: City, State: Zip:Today’s Date:Appointment Date:Personal Representative Name:Personal RepresentativeAuthority:Responsible Party Signature:
![December 2, 2012 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/51092274/1/190x245/december-2-2012-pdf-mount-sinai-hospital.jpg?quality=85)
![January 21, 2013 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/50916550/1/190x245/january-21-2013-pdf-mount-sinai-hospital.jpg?quality=85)
![February 3, 2013 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/50584982/1/190x245/february-3-2013-pdf-mount-sinai-hospital.jpg?quality=85)
![March 18, 2012 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/50462098/1/190x245/march-18-2012-pdf-mount-sinai-hospital.jpg?quality=85)

![Partners Program Guide [PDF] - Mount Sinai Hospital](https://img.yumpu.com/49411954/1/190x245/partners-program-guide-pdf-mount-sinai-hospital.jpg?quality=85)

![March 19 - April 1, 2012 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/48990923/1/190x245/march-19-april-1-2012-pdf-mount-sinai-hospital.jpg?quality=85)
![PGY-1 Residency Application [PDF] - Mount Sinai Hospital](https://img.yumpu.com/48577701/1/190x245/pgy-1-residency-application-pdf-mount-sinai-hospital.jpg?quality=85)


