CPL registration form
CPL registration form
CPL registration form
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
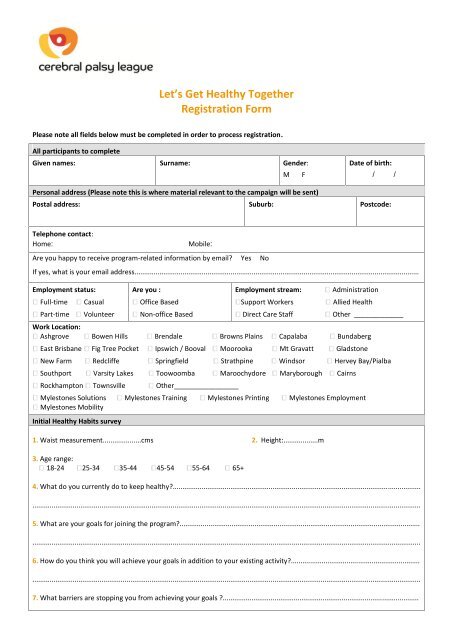
Let’s Get Healthy TogetherRegistration FormPlease note all fields below must be completed in order to process <strong>registration</strong>.All participants to completeGiven names: Surname: Gender:M FDate of birth:/ /Personal address (Please note this is where material relevant to the campaign will be sent)Postal address: Suburb: Postcode:Telephone contact:Home:Mobile:Are you happy to receive program-related in<strong>form</strong>ation by email? Yes NoIf yes, what is your email address....................................................................................................................................................Employment status:Full-timePart-timeCasualVolunteerAre you :Office BasedNon-office BasedEmployment stream:Support WorkersDirect Care StaffAdministrationAllied HealthOther _____________Work Location:Ashgrove Bowen Hills Brendale Browns Plains Capalaba BundabergEast Brisbane Fig Tree Pocket Ipswich / Booval Moorooka Mt Gravatt GladstoneNew Farm Redcliffe Springfield Strathpine Windsor Hervey Bay/PialbaSouthport Varsity Lakes Toowoomba Maroochydore Maryborough CairnsRockhampton Townsville Other_________________Mylestones Solutions Mylestones Training Mylestones Printing Mylestones EmploymentMylestones MobilityInitial Healthy Habits survey1. Waist measurement....................cms 2. Height:..................m3. Age range:18-24 25-34 35-44 45-54 55-64 65+4. What do you currently do to keep healthy?...........................................................................................................................................................................................................................................................................................................................................5. What are your goals for joining the program?.......................................................................................................................................................................................................................................................................................................................................6. How do you think you will achieve your goals in addition to your existing activity?.............................................................................................................................................................................................................................................................................7. What barriers are stopping you from achieving your goals ?......................................................................................................
(continued from page 1).........................................................................................................................................................................................................8. How will you overcome these barriers?...............................................................................................................................................................................................................................................................................................................................................9. I am interested in getting involved in group activities within the workplace Yes No10. I would like to be part of the 10,000 steps workplace challenge Yes NoIf you have internet access, please join 10,000 steps workplace challenge at this web address:http://www.10000steps.org.au/index/workplaces/ Please select ‘an individual participating in a challenge’.If you do not have internet, you can register as an off line applicant. Please Fiona Finn on 07 3358 8016 or Rose De Maria on07 3358 8019 for assistance.Diet:11. I currently consume the recommended 2 fruit, 5 veg per day eating routine? daily 2-3 times/weekonce/week neverTerms of participation1. I understand that exercise may be a risk to my physical health and safety if not done properly. I further understand that itis <strong>CPL</strong>’s recommendation that I consult a physician prior to engaging in any exercise program or activity, or undertaking anyfood or diet program, whether or not such program is recommended by <strong>CPL</strong>. I understand that neither <strong>CPL</strong> nor the adviceof any member of <strong>CPL</strong> personnel is a substitute for medical advice.2. I understand I need to become knowledgeable about the risks involved and assume personal responsibility for my actionsand exercise my own judgement as to the difficulty and my ability to safely protect myself from the inherent risksassociated with any activities I undertake.3. I agree to participate in mid-program and post-program surveys, contributing feedback and de-identified statistics towardsthe program evaluation.4. I agree to join the Qld Government Get Healthy program to access the in<strong>form</strong>ation and coaching service (13 43 25 84).Confidentiality1. Participant <strong>registration</strong> is a confidential process; however <strong>registration</strong> details will need to be viewed by certain <strong>CPL</strong> staff forreview purposes and program evaluation.2. In<strong>form</strong>ation collected will be used for evaluation, but will be collated in a de-identified <strong>form</strong> for statistical purposes toreport to Work Health & Safety Qld and assist in refining the offers and direction of the program.3. Names and contact details will be given to local champions so that registered staff can be provided with offers anddirection of the programParticipant acknowledgementI acknowledge that I have read, understood and agree to the above terms and wish to register for the program.Signature.......................................................................................Date.....................................................................................Please return completed <strong>form</strong> to:Email: hrhealthsafetygroup@cplqld.org.au or rdemaria@cplqld.org.auFax: Rose De Maria (07) 3358 8164