Medical Certification for FMLA - Family Member
Medical Certification for FMLA - Family Member
Medical Certification for FMLA - Family Member
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
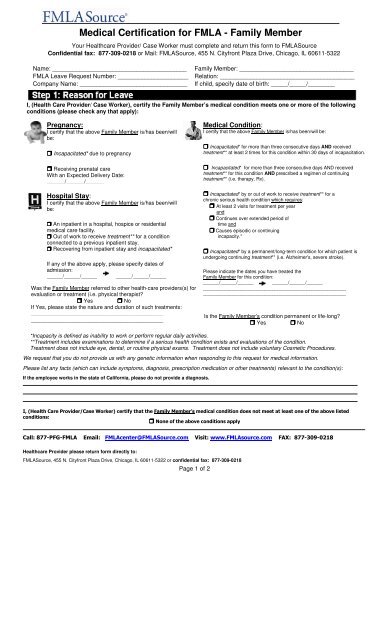
<strong>Medical</strong> <strong>Certification</strong> <strong>for</strong> <strong>FMLA</strong> - <strong>Family</strong> <strong>Member</strong>Your Healthcare Provider/ Case Worker must complete and return this <strong>for</strong>m to <strong>FMLA</strong>SourceConfidential fax: 877-309-0218 or Mail: <strong>FMLA</strong>Source, 455 N. Cityfront Plaza Drive, Chicago, IL 60611-5322Name: ________________________________________ <strong>Family</strong> <strong>Member</strong>: __________________________________<strong>FMLA</strong> Leave Request Number: _____________________ Relation: ________________________________________Company Name: ________________________________ If child, specify date of birth: _____/_____/________I, (Health Care Provider/ Case Worker), certify the <strong>Family</strong> <strong>Member</strong>’s medical condition meets one or more of the followingconditions (please check any that apply):Pregnancy:I certify that the above <strong>Family</strong> <strong>Member</strong> is/has been/willbe: Incapacitated* due to pregnancy Receiving prenatal careWith an Expected Delivery Date:______/______/______Hospital Stay:I certify that the above <strong>Family</strong> <strong>Member</strong> is/has been/willbe: An inpatient in a hospital, hospice or residentialmedical care facility. Out of work to receive treatment** <strong>for</strong> a conditionconnected to a previous inpatient stay. Recovering from inpatient stay and incapacitated*If any of the above apply, please specify dates ofadmission:______/______/______ ______/______/______Was the <strong>Family</strong> <strong>Member</strong> referred to other health-care providers(s) <strong>for</strong>evaluation or treatment (i.e. physical therapist? Yes NoIf Yes, please state the nature and duration of such treatments:________________________________________________________________________________________<strong>Medical</strong> Condition:I certify that the above <strong>Family</strong> <strong>Member</strong> is/has been/will be: Incapacitated* <strong>for</strong> more than three consecutive days AND receivedtreatment** at least 2 times <strong>for</strong> this condition within 30 days of incapacitation. Incapacitated* <strong>for</strong> more than three consecutive days AND receivedtreatment** <strong>for</strong> this condition AND prescribed a regimen of continuingtreatment** (i.e. therapy, Rx). Incapacitated* by or out of work to receive treatment** <strong>for</strong> achronic serious health condition which requires: At least 2 visits <strong>for</strong> treatment per yearand Continues over extended period oftime and Causes episodic or continuingincapacity.* Incapacitated* by a permanent/long-term condition <strong>for</strong> which patient isundergoing continuing treatment** (i.e. Alzheimer's, severe stroke).Please indicate the dates you have treated the<strong>Family</strong> <strong>Member</strong> <strong>for</strong> this condition:______/______/______ ______/______/__________________________________________________________________________________________________________________Is the <strong>Family</strong> <strong>Member</strong>'s condition permanent or life-long? Yes No*Incapacity is defined as inability to work or per<strong>for</strong>m regular daily activities.**Treatment includes examinations to determine if a serious health condition exists and evaluations of the condition.Treatment does not include eye, dental, or routine physical exams. Treatment does not include voluntary Cosmetic Procedures.We request that you do not provide us with any genetic in<strong>for</strong>mation when responding to this request <strong>for</strong> medical in<strong>for</strong>mation.Please list any facts (which can include symptoms, diagnosis, prescription medication or other treatments) relevant to the condition(s):If the employee works in the state of Cali<strong>for</strong>nia, please do not provide a diagnosis.I, (Health Care Provider/Case Worker) certify that the <strong>Family</strong> <strong>Member</strong>’s medical condition does not meet at least one of the above listedconditions: None of the above conditions applyCall: 877-PFG-<strong>FMLA</strong> Email: <strong>FMLA</strong>center@<strong>FMLA</strong>Source.com Visit: www.<strong>FMLA</strong>source.com FAX: 877-309-0218Healthcare Provider please return <strong>for</strong>m directly to:<strong>FMLA</strong>Source, 455 N. Cityfront Plaza Drive, Chicago, IL 60611-5322 or confidential fax: 877-309-0218Page 1 of 2
Your Healthcare Provider/ Case Worker must complete and return this <strong>for</strong>m to <strong>FMLA</strong>SourceConfidential fax: 877-309-0218 or Mail: <strong>FMLA</strong>Source, 455 N. Cityfront Plaza Drive, Chicago, IL 60611-5322Name: _____________________________________<strong>FMLA</strong> Leave Request Number: _________________<strong>Family</strong> <strong>Member</strong>: _____________________________________Company Name: ____________________________________When completing this section, keep in mind that your patient’s need <strong>for</strong> care by the employee seeking leave mayinclude assistance with basic medical, hygienic, nutritional, safety or transportation needs, or the provision of physicalor psychological care.Continuous:I certify that the above <strong>Family</strong> <strong>Member</strong> will require care by theemployee <strong>for</strong> a single continuous period due to his/her medicalcondition including time <strong>for</strong> treatment and recovery:(A) Begin date: ____/____/____ End date:____/____/____(Estimate dates if unknown)Explain the care needed <strong>for</strong> the <strong>Family</strong> <strong>Member</strong> by the Employee andwhy such care is medically necessary:Reduced Schedule:I certify that the above employee will need to work the following parttime/reduced-hoursschedule to care <strong>for</strong> the <strong>Family</strong> <strong>Member</strong>Intermittent/Episodic:I certify that the above <strong>Family</strong> <strong>Member</strong> will require intermittent/episodiccare by the employee <strong>for</strong> the condition as follows:(A) Begin date: ____/____/____ End date:____/____/____(Estimate dates if unknown)(B) Treatments/scheduled appointments: Frequency = ____# per week month year Duration = ____# hour(s) or ____days(s) per treatment(s)Please ESTIMATE treatment schedule (if any) including pre-scheduledappointments, the time required <strong>for</strong> each appointment (including anyrecovery period):(A) Begin date: ____/____/____ End date:____/____/____(Estimate dates if unknown)(B) If the schedule is fixed, please indicate hours/days per week theemployee can work:Sun. Mon. Tue. Wed. Thu. Fri. Sat.(C) Based on the patients medical history & your knowledge of themedical condition, please indicate the frequency AND duration ofepisodes of incapacitation (e.g. 3 times per 2 months lasting 1-2 days): Frequency = ____# time(s) per ____week(s) or ____ month(s) Duration = ____# hour(s) or ____days(s) per episode(s)(C) If the schedule varies weekly, please indicate the number of hoursper day and the number of days per week the employee is able towork:_____ Hours/Day _____ Days/WeekExplain the care needed <strong>for</strong> the <strong>Family</strong> <strong>Member</strong> by the Employee andwhy such care is medically necessary:(D) Does the <strong>Family</strong> <strong>Member</strong> need care during these episodes?Yes NoExplain the care needed <strong>for</strong> the <strong>Family</strong> <strong>Member</strong> by the Employee andwhy such care is medically necessary:Healthcare Provider / Case Worker must sign and return <strong>for</strong>m directly to <strong>FMLA</strong>Source.Signature Date Date Revised InitialPrint Name Phone FaxType of PracticeStreet Address City StateZipCall: 877-PFG-<strong>FMLA</strong> Email: <strong>FMLA</strong>center@<strong>FMLA</strong>Source.com Visit: www.<strong>FMLA</strong>source.com FAX: 877-309-0218Healthcare Provider please return <strong>for</strong>m directly to:<strong>FMLA</strong>Source, 455 N. Cityfront Plaza Drive, Chicago, IL 60611-5322 or confidential fax: 877-309-0218Page 2 of 2