l(CK-MB), and troponin. TotalCK levels are elevated inpatients with CRF, but CK-MB levels are not; thus, elevationin CK-MB levels is dueto myocardial injury. Elevationof troponin levels withouta corresponding elevationin total CK levels has beenshown to reflect enzymeelimination kinetics due torenal failure or cross-reactivityof the troponin I assaywith noncardiac antigens.Therefore, any enzyme elevationsare not diagnostic in andof themselves. The diagnosisof postoperative MI shouldbe made based on a combinationof clinical, laboratory,and ECG evidence. The preoperativeuse of beta-blockertherapy (eg, atenolol) may bebeneficial, though at the riskof developing or worseninghyperkalemia.Patients already on dialysis-Forpatients already ondialysis, dialysis adequacy,preoperative dialysis needs,postoperative dialysis timing,and dosage requirements forall medications should be determined.Patients on hemodialysisusually require preoperativedialysis within 24hours before surgery to reducethe risk of volume overload,hyperkalemia, and excessivebleeding. Patients withperitoneal dialysis who areundergoing abdominal surgeryshould be switched tohemodialysis until woundhealing is complete. Peritonealdialysis should be continuedfor those undergoingnon-abdominal surgery.lPatients who already havea renal transplant -Because of complicated druginteractions and immunosuppressivedosing, monitoring,and adjustment, a nephrologistwith specializedknowledge of renal transplantationshould be involvedin the preoperative evaluationof patients with CRF whohave received kidney transplantation.Cyclosporine ortacrolimus taken by renaltransplant recipients for immunosuppressionare metabolizedby the cytochromeP-450 system in the liver andthus interact with a wide varietyof agents. Diltiazem,hepatic 3-methylglutaryl coenzymeA reductase inhibitors,macrolides, and antifungaldrugs inhibit the system,elevate drug levels, and canprecipitate nephrotoxicity.Others, such a scarbamazepine,barbiturates, and theophylline,induce the hepaticenzyme system, reduce druglevels, and can precipitate rejection.Drug levels must bemonitored in this setting.Intravenouscy closp-orine ortacrolimus should be given atone-third the oral dose untilthe patient is able to tolerateoral medications. A thoroughpre-operative evaluation ofthe patient is mandatory toassess the functions of thedifferent systems. Both generaland regional anaesthetictechniques can be used, dependingupon the functionalstatus.References1. Wolfe RA, Ashby VB, MilfordEL, et al: Comparison ofmortality in all patients ondialysis, patients on dialysiswaiting transplantation, andrecipients of the firstcadaveric transplant. N EnglJ Med 341: 1725-1730, 1999.2. Gaston RS, Alveranga DY,Becker BN, et al: Kidney andpancreas transplantation. AmJ Transplant 3 (Supp 4): 64-77, 2003.3. Legendre C, Saltiel C, KriesH, Grunfeld J-P. Hypertensionin kidney transplantation.Klin Wochenschr 1989;67: 919-22.4. Gunnarsson R, Lofmark R,Norlander R, et al. Acutemyocardial infarction in renaltransplant recipients: incidenceand prognosis. EurHeart J 1984; 5: 218-21.5. Hambley H, Mufti GH.Erythropoietin: an old friendrevisited. Br Med J 1990; 300:621-2.6. Goldfarb S, Cox M, Suiger I,Goldbert M. Acutehyperkalaemia induced byhyperglycaemia; hormonalmechanisms. Ann Intern Med1976; 84: 426-32.7. Vandam LD, Harrison JH,Murray JE, et al: Anaestheticaspects of renal homotransplantationin man. Anesthesiology23: 783-92, 1962.8. Linke CL, Merin RG: Aregional anaesthetic approach56Journal of Postgraduate Medical Education, Training & ResearchVol. II, No. 5, September-October 2007
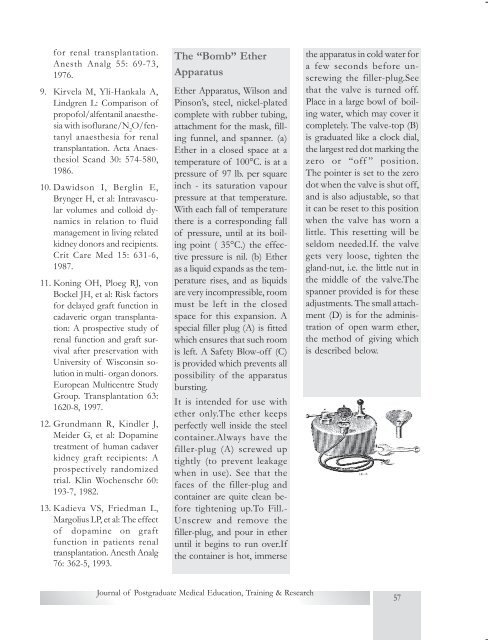
for renal transplantation.Anesth Analg 55: 69-73,1976.9. Kirvela M, Yli-Hankala A,Lindgren L: Comparison ofpropofol/alfentanil anaesthesiawith isoflurane/N 2O/fentanylanaesthesia for renaltransplantation. Acta AnaesthesiolScand 30: 574-580,1986.10. Dawidson I, Berglin E,Brynger H, et al: Intravascularvolumes and colloid dynamicsin relation to fluidmanagement in living relatedkidney donors and recipients.Crit Care Med 15: 631-6,1987.11. Koning OH, Ploeg RJ, vonBockel JH, et al: Risk factorsfor delayed graft function incadaveric organ transplantation:A prospective study ofrenal function and graft survivalafter preservation withUniversity of Wisconsin solutionin multi- organ donors.European Multicentre StudyGroup. Transplantation 63:1620-8, 1997.12. Grundmann R, Kindler J,Meider G, et al: Dopaminetreatment of human cadaverkidney graft recipients: Aprospectively randomizedtrial. Klin Wochenschr 60:193-7, 1982.13. Kadieva VS, Friedman L,Margolius LP, et al: The effectof dopamine on graftfunction in patients renaltransplantation. Anesth Analg76: 362-5, 1993.The “Bomb” EtherApparatusEther Apparatus, Wilson andPinson’s, steel, nickel-platedcomplete with rubber tubing,attachment for the mask, fillingfunnel, and spanner. (a)Ether in a closed space at atemperature of 100°C. is at apressure of 97 lb. per squareinch - its saturation vapourpressure at that temperature.With each fall of temperaturethere is a corresponding fallof pressure, until at its boilingpoint ( 35°C.) the effectivepressure is nil. (b) Etheras a liquid expands as the temperaturerises, and as liquidsare very incompressible, roommust be left in the closedspace for this expansion. Aspecial filler plug (A) is fittedwhich ensures that such roomis left. A Safety Blow-off (C)is provided which prevents allpossibility of the apparatusbursting.It is intended for use withether only.The ether keepsperfectly well inside the steelcontainer.Always have thefiller-plug (A) screwed uptightly (to prevent leakagewhen in use). See that thefaces of the filler-plug andcontainer are quite clean beforetightening up.To Fill.-Unscrew and remove thefiller-plug, and pour in etheruntil it begins to run over.Ifthe container is hot, immersethe apparatus in cold water fora few seconds before unscrewingthe filler-plug.Seethat the valve is turned off.Place in a large bowl of boilingwater, which may cover itcompletely. The valve-top (B)is graduated like a clock dial,the largest red dot marking thezero or “off ” position.The pointer is set to the zerodot when the valve is shut off,and is also adjustable, so thatit can be reset to this positionwhen the valve has worn alittle. This resetting will beseldom needed.If. the valvegets very loose, tighten thegland-nut, i.e. the little nut inthe middle of the valve.Thespanner provided is for theseadjustments. The small attachment(D) is for the administrationof open warm ether,the method of giving whichis described below.Journal of Postgraduate Medical Education, Training & Research57
- Page 1:
Global Phenomenon of e-healthP.S. S
- Page 4 and 5:
Basic Life SupportRavinder Kumar Ba
- Page 6 and 7: age 5 . AHA recommends abdominalthr
- Page 8 and 9: ficult when bleeding is brisk, andi
- Page 10 and 11: orrhage, a non-bleeding visiblevess
- Page 12 and 13: structures visualized with nakedeye
- Page 14 and 15: LSCS is taken, patient shouldbe kep
- Page 16 and 17: in amniotic fluid), nor due to apre
- Page 18 and 19: l Reduction in induction-deliveryin
- Page 20 and 21: to the blood pressure changes.l Hyp
- Page 22 and 23: incidence of side-effects andPONV.
- Page 24 and 25: 2. Nasal injectionThe same needle i
- Page 26 and 27: injected. It blocks sensation fromt
- Page 28 and 29: Intraocular tumorsIn children, reti
- Page 30 and 31: A fast of six to eight hours forsol
- Page 32 and 33: lControl ventilation should beiniti
- Page 34 and 35: 6ReviewArticleAnaesthesia for Nonca
- Page 36 and 37: immunosuppression, andpreoperative
- Page 38 and 39: and the most frequent andimportant
- Page 40 and 41: ppressive drugs or chronic heartfai
- Page 42 and 43: 7ReviewArticleAnticoagulants and An
- Page 44 and 45: The dose of heparin varies withthe
- Page 46 and 47: and has a half -life of 24-48 hours
- Page 48 and 49: llPatients receiving heparin forgre
- Page 50 and 51: (5%). For patients with mitralprost
- Page 52 and 53: Cardiovascularl Hypertension- Over
- Page 54 and 55: elaxants, and provides goodpost-ope
- Page 58 and 59: 9ReviewArticleObesity and Anesthesi
- Page 60 and 61: yet to be validated and should be u
- Page 62 and 63: prior to induction followed byPEEP
- Page 64 and 65: Anesthetic Implications-Thepreferre
- Page 66 and 67: Excretion of catecholamines and the
- Page 68 and 69: 3. Tsioufis CP, Stefanadis CI,Touto
- Page 70 and 71: Diagnosisl Edrophonium (Tensilontes
- Page 72 and 73: erases may increase the needfor non
- Page 74 and 75: 2. Drachman DB. Myastheniagravis. N
- Page 76 and 77: ecommended to control psychoticsymp
- Page 78 and 79: espiratory complications due tothe
- Page 80 and 81: pain and a sensation of fullnessin
- Page 82 and 83: gastrointestinal stromaltumors: rec
- Page 84 and 85: 13Many new supraglotticairway devic
- Page 86 and 87: to the cuff size of the originalLMA
- Page 88 and 89: LMAs with valves that do notcontain
- Page 90 and 91: geal mask airway in paralyzed,anest
- Page 92 and 93: Foregger Midget) and diffusionof su
- Page 94 and 95: cause serious problems. Longersurge
- Page 96 and 97: positioning accuracy for CTguided s
- Page 98 and 99: decreases with increased optodesepa
- Page 100 and 101: observed that SJO 2of 50% ingeneral
- Page 102 and 103: ibility of cerebral circulatory arr
- Page 104 and 105: investigation and suggests thatesta
- Page 106:
14. Kiening ML, Unterberg AW,Bard T