NEWS(winter '05).indd - Douglass Hanly Moir Pathology
NEWS(winter '05).indd - Douglass Hanly Moir Pathology
NEWS(winter '05).indd - Douglass Hanly Moir Pathology

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Doctors’ NewsletterWinterPage 2EditorialDr Colin GoldschmidtPages 3-4Interpretation ofLiver Function TestsDr Grahame CaldwellPages 5-6Viral HepatitisDr Ian ChambersPage 7Haematological Changesin Liver DiseaseDr Debbie ClarkPage 8Latest NewsNew Mesothelin TestAnswers to Quiz
EditorialMaking Sense of<strong>Pathology</strong> InformationDr Colin GoldschmidtChief Executive OfficerIt is my pleasure to introduce this latest edition of theDoctors’ Newsletter. Our theme for this issue is the liver,as tests of liver function are one of our most frequentlyrequested profiles, and primary liver disease is ofincreasing prominence in Australia. The articles offered inthis Newsletter cover biochemical, microbiological, andhaematological aspects of liver disease and we hope thatyou will find them useful in your daily clinical work.Various estimates suggest that medical knowledge doublesevery five years or less. Such a rapid pace constantlychallenges all of us, and underpins a need to try to makesense of the sea of information we face on a daily basis.How can we help, as far as pathology is concerned? In ourPractice, we believe it is worthwhile putting considerablethought and effort into providing interpretive guidance onresults we generate.Interpretive comments mean effective communication,not just more facts or numbers. For this reason we try,wherever possible, to add such comments in the formof accompanying text or interpretive algorithm. Thesecomments, although often pre-prepared, are added toindividual results by a pathologist or senior scientist inresponse to the available information. Where a patient’sprofile is difficult to interpret, or may suggest that urgentaction is required, we may phone you directly to discussthe results.We are fortunate to have a large team of pathologists at<strong>Douglass</strong> <strong>Hanly</strong> <strong>Moir</strong> and Barratt & Smith <strong>Pathology</strong>, andtheir expertise covers the entire spectrum of pathologytesting. With the increasing complexity of currently availablepathology tests, the need for sub-specialised pathologistsis essential and here too, we are fortunate to have thisin-depth expertise amongst our pathologist group. As partof our commitment to continuous improvement, we ensurethat our advice takes account of the most up-to-dateinformation on any given test.I am frequently asked why I believe that <strong>Douglass</strong> <strong>Hanly</strong><strong>Moir</strong> and Barratt & Smith <strong>Pathology</strong> is different from otherpathology groups. Even though I might not be entirelyneutral in my view on this subject, I do have a list of“value-added” features which I believe differentiate us fromour competitors. However, I always come back to ouroutstanding pathologist group as the major differentiatingfeature. Whether by virtue of interpretive comment ortelephone consultation, our super-specialised pathologistsprovide current, educated and practical advice whichwe hope allows you to make better sense of the resultsissued. They are the dynamic link between your practiceand the increasingly complex world of pathology testingand, judging by the number of calls our pathologists receiveeach day from referring doctors, their input appears to bemuch appreciated. So, please feel free to make use of this“differentiated” service – and phone a <strong>Douglass</strong> <strong>Hanly</strong> <strong>Moir</strong>or Barratt & Smith pathologist today!Finally, it remains for me to extend to you my warmestwishes and to thank you most sincerely for yourongoing support.With my warmest regards,Dr Colin GoldschmidtM.B.B.Ch., F.R.C.P.A., F.A.I.C.D.Chief Executive Officer<strong>Douglass</strong> <strong>Hanly</strong> <strong>Moir</strong> <strong>Pathology</strong>Barratt & Smith <strong>Pathology</strong>2
Interpretation of Liver Function Testsand secreted into the bile and thence the gut. Conjugatedbilirubin is water soluble and appears in the urine. In excess,it is responsible for the dark discolouration of the urine inobstructive jaundice.In the normal physiological state, serum bilirubin ispredominantly unconjugated. If there is haemolysis,ineffective erythropoiesis, or resorption of a haematoma,unconjugated (“indirect”) bilirubin will rise. Conjugated(“direct”) hyperbilirubinaemia occurs in parenchymal liverdisease and as a result of intrahepatic or extrahepaticobstruction to bile flow.Doctors frequently face the need to interpret abnormalitiesin Liver Function Tests (LFT), as these are among the mostfrequently requested pathology investigations. The problemis compounded by the fact that the apparent severity of theabnormalities does not necessarily reflect the extent of theunderlying liver disease.Some patients, for example, with advanced parenchymalcell loss have only mildly abnormal LFT results. On the otherhand, abnormalities in the LFT group such as elevation inenzyme levels may result from disease remote from the liver.This is particularly a problem where a ‘liver’ enzyme also ispresent in other tissues of the body.This article will briefly discuss the seven tests shown belowthat are normally performed in response to a request for LFT.Three recent examples from our laboratory of abnormal LFTresults illustrating the various patterns of disease also areincluded.Protein is used in conjunction with albumin to estimateglobulin levels and falls within the LFT group. This, however,will not be discussed, as the significance of globulin valueshas already been considered in a previous newsletter article.Liver Function Tests (excluding Total Protein & Globulins)BilirubinAlkaline Phosphatase (ALP)Gamma-Glutamyltransferase (GGT)Lactate Dehydrogenase (LD)Aspartate Transaminase (AST)Alanine Transaminase (ALT)AlbuminBilirubinDr Grahame CaldwellDirector - BiochemistryBilirubin is formed from the physiological lysis of red bloodcells. As unconjugated bilirubin, it is transported to theliver loosely bound to albumin. Unconjugated bilirubin isinsoluble in water and therefore does not appear in theurine. Within the liver it is conjugated to bilirubin glucuronideBilirubin levels rise in a wide variety of liver disorders. Belowis a list of common causes of an isolated rise in bilirubinlevels.Some causes of an isolated elevated bilirubin:• Haemolysis• Ineffective erythropoiesis (eg megaloblastic anaemia)• Resorption of haematoma• Drugs (eg rifampicin)• Genetic metabolic defects (eg Gilbert’s syndrome)Alkaline PhosphataseAlkaline phosphatase originates from two main sources:liver and bone. It is also present in other tissues includingplacenta, leukocytes, intestine, and kidney. A first stepin determining the cause of a raised ALP is to identifythe source of the enzyme. This may be apparent fromthe clinical assessment and investigations including theremaining LFT results. However, if necessary, isoenzymestudies may be used to determine the tissue source.Raised hepatic ALP is characteristically associated withcholestasis.Common causes of raised ALP:• Pregnancy• Normal bone growth (children and adolescents)• Bile duct obstruction (eg stones, malignancy)• Drug-induced cholestasis• Metastatic liver disease• Primary biliary cirrhosis• Sclerosing cholangitis• Bone diseaseGamma-GlutamyltransferaseGamma-glutamyltransferase (GGT) is present in all cellsexcept skeletal muscle. In most cases, however, abnormallevels of this enzyme tend to be specific for the liver. Theprimary source of GGT is from biliary epithelial cells andperiportal hepatocytes. GGT is useful as a sensitive markerfor hepatobiliary status; raised serum levels are caused byenzyme induction and cholestasis.Common causes of a raised GGT:• Alcohol• Drugs (eg anticonvulsants)• Biliary obstruction• Hepatitis• Non-alcoholic fatty liver3
Viral HepatitisHepatitis is most commonly characterised by elevationsof ALT and AST to a degree disproportionately greaterthan any elevations in GGT and ALP which may alsobe present. While viral infection is a common causeof hepatitis, other causes must be considered in theappropriate context. These include alcohol and other drugs,autoimmune pathology and non-viral infectious causes suchas leptospirosis and Q fever.The main viral agents causing hepatitis include thespecifically hepatotropic agents Hepatitis A to E,but also EBV, CMV and sundry other viruses which arecirculating in the community. While the latter group maycommonly cause biochemical hepatitis, this tends to bean incidental finding and is rarely clinically significant. Themorbidity and mortality associated with infection withHepatitis A to E, however, is of huge clinical and economicimportance worldwide.Hepatitis A Virus (HAV)Dr Ian ChambersDirector - MicrobiologyHAV infection is spread person-to-person by theorofaecal route, or by ingestion of contaminated food orwater. It is highly contagious and spreads rapidly betweenindividuals in prolonged close contact. The decliningincidence of infection in developed countries, but continuingendemicity in developing parts of the world, makes HAV,and vaccination against it, important issues for travellersoverseas.HAV produces an acutehepatitis with a meanincubation of around 30days. In children under6 years infection isusually sub-clinical.There is no chroniccarrier state andimmunity afterinfection islife-long.Hepatitis B Virus (HBV)HBV is a global health problem, with an estimated350 million HBV carriers worldwide. More than 500,000deaths each year are attributable to the chronic sequelae ofHBV such as cirrhosis and hepatocellular carcinoma.It is transmitted by cutaneous and mucosal exposureto infectious blood or body fluids, making sexualcontact and needle-sharing the main identifiable routes oftransmission in countries such as Australia.HBsAg is the hallmark of HBV infection. It appears 2-7weeks before the onset of symptoms and most patientswho recover from HBV infection clear HBsAg within 6months. Persistence beyond this time implies chronicinfection, which occurs in approximately 10% of infectedadults.HBeAg is a marker of active viral replication, andits persistence in a chronic carrier of HBV indicates highinfectivity and a greater likelihood of progression tochronic liver disease. However, the HBV pre-coremutant, being unable to synthesize HBeAg, is associatedwith ongoing viral replication and liver damage withoutdetectable HBeAg.Hepatitis C Virus (HCV)HCV is spread by parenteralroutes, most commonly (in Australia)by the sharing of contaminatedneedles. However, in more than 40% ofcases no recent or readily identifiable riskfactor can be identified. Liver disease causedby HCV is now the leading reason for livertransplantation in Australia.There is a high rate of subclinical infectionwith HCV. Only about 15-25% of cases of acuteinfection result in the development of jaundice. Thosethat do are less likely to progress to chronic diseasewhich is seen in 50-70% of those infected.The presence of antibody to HCV does not distinguishbetween past or current infection. Nucleic aciddetection by PCR is used to assess disease activityand for pre- and post-treatment evaluation.Hepatitis D Virus (HDV)HDV is a defective virus, whichcan only infect thosewho are co-infected with HBV. Its geographicdistribution includes the Amazon basin, central Africa,the Mediterranean basin and the Middle East. HDVmay cause a benign, acute hepatitis or lead tofulminant liver failure. In the chronic setting, patientsmay be asymptomatic carriers or may progressmore rapidly to cirrhosis and hepatocellularcarcinoma. While uncommon in Australia, itshould be suspected in patients with chronicHBV who develop an acute hepatitis or have rapidprogression of their liver disease.5
Viral HepatitisHepatitis E Virus (HEV)HEV is an enterically-transmitted virus which isendemic to the Indian subcontinent and southeast andcentral Asia. While several epidemics have been reportedfrom China and India, the Australian experience is ofsporadic cases, mainly in returning travellers. Indigenouscases, however, have been reported from the NorthernTerritory.HEV does not cause chronic liver disease, butinfection in pregnant women is associated withfulminant liver failure in approximately 25% of cases.Hepatitis Viruses Beyond A to EApproximately 15% of hepatitis infections remainunexplained, and causes continue to be sought.Hepatitis F virus (HFV) was initially identified as a possiblehepatitis virus but there is insufficient evidence tocorroborate this and the identity of HFV is in doubt.Hepatitis G Virus (HGV, also called GB virus) wasinitially cloned from the plasma of a surgeon with acutehepatitis and is closely related to HCV. It is found amongblood donors and can be transmitted by transfusion butdoes not appear to be associated with hepatitis – nordoes it worsen the course of concurrent HCV infection.Tests for HGV are not currently available.Non-Hepatotropic Viruses and the LiverMany acute viral infections may cause transaminaseelevation, but only a minority manifest as a clinicallyapparent hepatitis. The most frequently encountered of thisgroup are Epstein-Barr virus and Cytomegalovirus, butothers include Parvovirus B19, Herpes simplex, Dengue,Enterovirus and HIV.Requesting Hepatitis TestingOrdering the appropriate hepatitis tests is confusingbecause there are so many different serological markers,especially for Hepatitis B. In addition, Medicare restrictionsadd another layer of complexity when deciding whichtests can be performed. The table provided is a guide tothe tests which are relevant in the most common clinicalsettings and their interpretation.Confusion can be minimized by either specifying theindividual markers by name or, if making a general requestfor “Hepatitis serology”, specifying the clinical context ofthe request e.g. “? immunity Hep A and B” or “? acutehepatitis”.Serological Markers For Hepatitis A, B, CInterpretation of Hepatitis SerologyHBcAbHAV IgM HAV IgG HBsAg anti-HBsIgM TotalHBeAg anti-HBe HBV PCR anti-HCV HCV PCR Interpretation+ – Acute Hepatitis A+ or – + Past Hepatitis A+ – + + + – + Acute Hepatitis B+ – – + – + – Hepatitis B carrier (“low-infectivity”)+ – + or – + + – + Hepatitis B carrier (“high-infectivity”)+ – – + – – + Hepatitis B carrier (pre-core mutant)– + – + – + – Past, resolved Hepatitis B– + – – – – – Successful Hepatitis B vaccination+ or – + Acute Hepatitis C+ + Chronic Hepatitis C+ – Resolved Hepatitis CKEY: Ab = antibody Ag = antigen HBV PCR - no medicare item yetFor any enquiries, please contact Dr Ian Chambers on (02) 98 555 3306
Haematological Changes in Liver DiseaseThe Full Blood CountIn chronic liver disease a number of changes occur in thefull blood count and film; sometimes these findings may bethe first indication of liver dysfunction.Haemoglobin LevelDr Debbie ClarkHaematologistAs in any chronic disease, the haemoglobin level mayfall, especially in patients with advanced liver disease.Macrocytosis is a common finding. Target cells aresometimes present (see Figure 1), although when presentin large numbers, suggest obstructive jaundice orhaemoglobinopathy.Blood loss, for example from bleeding varices, maycontribute to the anaemia. Dietary folate deficiency iscommon in patients with underlying alcohol abuse andalcohol itself may suppress haemopoiesis or causesideroblastic change in the marrow. Occasionally,haemolysis may occur in patients with liver disorders.Interestingly, viral hepatitis may rarely be followed byaplastic anaemia.Coagulation AbnormalitiesA bleeding tendency is common in patients with chronicand severe liver disease and multiple haemostaticabnormalities may be present. This may cause difficultieswhere liver biopsy is required or may contribute to bleedingfrom varices.Liver parenchymal cells are responsible for production ofmost coagulation factors. In addition, biliary obstructionresulting in impaired absorption of Vitamin K can lead tofurther decreased synthesis of factors II, VII, IX and X.Coagulation tests such as the PT (prothrombin time) andAPTT (activated partial thromboplastin time) are frequentlyprolonged in these circumstances.The prothrombin time is a particularly useful indicator ofimpaired liver function (in advanced cases); unlike thetraditional biochemical ‘liver function’ tests which areoccasionally normal in advanced disease, it is a true testof the functional ability of the liver. Note that the INR, a testbased on the prothrombin time, was designed for testingof warfarin-induced coagulopathy, rather than that of liverdisease.Factor V and fibrinogen may also be reduced, and afunctional impairment of fibrinogen (dysfibrinogenaemia)is found in many patients. Impaired removal of activatedclotting factors and increased fibrinolytic activity may alsobe present.Figure 1White Cells and PlateletsIn longstanding liver disease mild to moderate leucopenia,including neutropenia, is often seen. Less commonly,acute liver damage or infiltration may be associated with aneutrophil leukocytosis.The platelet count is commonly reduced in patients withcirrhosis; although hypersplenism, immune mediateddestruction, and erythropoietin deficiency may beresponsible for these changes, the exact mechanismremains uncertain.Perpherial blood film showing macrocytosis and target cellsFor any enquiries, please contactDr Debbie Clark on (02) 98 555 4727
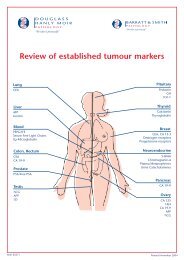
Latest News - New Mesothelin TestPleural mesotheliomaMesothelin TestOur practice is now able to offer Mesothelin (MESOMARK) testing formalignant mesothelioma.At present, we do not believe this assay has clinical utility for the generalscreening of patients at risk of malignant mesothelioma, but it will be usefulfor monitoring patients with a histological diagnosis of mesothelioma.You also may consider this test in patients at high risk of malignantmesothelioma, when diagnostic procedures have failed to confirm thediagnosis. Because of the difficulties in interpreting and managing patientswith low or intermediate levels of Mesothelin, we believe that the test isbetter restricted to a relevant clinical specialist setting.Since the test has become available only recently, we are keen tomonitor its performance and for this reason, we would appreciate allrelevant clinical data including information regarding patientfollow-up.The Mesothelin assay, at present, is performed weekly in ourlaboratory and the fee is $95 (excluding GST) per test. There is noMedicare rebate currently available for this assay.If you have any enquiries regarding this test,please do not hesitate to contact eitherDr Grahame Caldwell or Dr Karl Baumgarton (02) 98 555 312.Mesothelioma in a pleural aspirateAnswers to Quiz - Doctors’ Newsletter Autumn 2005In our last issue, we showed three cases from our records and asked for the most likely diagnosis. Here are theanswers:Question 1:This was a 13 year old girl presenting with lethargy, abdominal discomfort, jaundice and splenomegaly. The bilirubinand LD were elevated and the blood film showed spherocytes and increased polychromasia, findings consistent withspherocytic haemolysis.Diagnosis: hereditary spherocytosis.Question 2:This was a 28 year old man returning from an extended holiday in India, with fever, nausea, jaundice and hepatomegaly.Both AST and ALT were greater than 10,000U/L and the blood film showed atypical lymphocytes suggesting viralinfection.Diagnosis: viral hepatitis (Serology was positive for Hepatitis A).Question 3:This was a 78 year old man with weight loss, who had had a total gastrectomy three years previously. Significantfindings were a marked elevation of LD (in this case, a result of malignancy), and elevation of the alkaline phosphataseand gamma-glutamyltransferase (both biliary tract enzymes). The CT scan of the liver showed hepatic metastases.Diagnosis: metastatic carcinoma in the liver originating from a gastric carcinoma.DOUGLASS HANLY MOIR PATHOLOGY • ABN 80 003 332 858A subsidiary of SONIC HEALTHCARE LIMITEDBARRATT & SMITH PATHOLOGYA trading name of DOUGLASS HANLY MOIR PATHOLOGY PTY LTD • ABN 80 003 332 858A subsidiary of SONIC HEALTHCARE LIMITED95 EPPING ROAD • MACQUARIE PARK • NSW 2113 • AUSTRALIATEL 98 555 222 • FAX 9878 5077MAIL ADDRESS • LOCKED BAG 145 • NORTH RYDE • NSW 1670 • AUSTRALIA31 LAWSON STREET • PENRITH • NSW 2750 • AUSTRALIATEL 4734 6500 • FAX 4732 2503MAIL ADDRESS • PO BOX 443 • PENRITH • NSW 2751 • AUSTRALIA