<strong>Summary</strong> <strong>of</strong> <strong>the</strong> <strong>Gross</strong> <strong>Anatomy</strong> <strong>of</strong> <strong>the</strong> <strong>Extraocular</strong> <strong>Muscles</strong> 45FIGURE 3–8. Tenon’s space shown by injection with Indiaink. (Modified from Charpy A: <strong>Muscles</strong> et capsulede Tenon. In Poirier P, Charpy A, eds: Traité d’anatomiehumaine, new ed, vol 5/2. Paris, Masson, 1912, p 539.)not clearly delineated; it is thin and more or lesscontinuous with <strong>the</strong> meshwork <strong>of</strong> <strong>the</strong> orbital fat.If <strong>the</strong> globe is enucleated, one can see <strong>the</strong>anterior orifice <strong>of</strong> Tenon’s capsule, <strong>the</strong> borders <strong>of</strong>which were attached to <strong>the</strong> sclera before enucleation;<strong>the</strong> posterior orifice, which is fused with<strong>the</strong> sheaths <strong>of</strong> <strong>the</strong> optic nerve; and <strong>the</strong> smoothinner surface with <strong>the</strong> slits <strong>of</strong> entry for <strong>the</strong> extraocularmuscles. The openings for <strong>the</strong> vortex veinsare small and not readily visualized (Fig. 3–9).Muscle Sheaths and TheirExtensionsThe extrinsic ocular muscles pierce Tenon’s capsule,enter <strong>the</strong> subcapsular space, and insert into<strong>the</strong> sclera. Therefore, one can distinguish an extracapsularand an intracapsular portion <strong>of</strong> eachmuscle.In <strong>the</strong>ir extracapsular portions, <strong>the</strong> extrinsic eyemuscles are enveloped by a muscle sheath. Thissheath is a reflection <strong>of</strong> Tenon’s capsule and runsbackward from <strong>the</strong> entrance <strong>of</strong> <strong>the</strong> muscles into<strong>the</strong> subcapsular space for a distance <strong>of</strong> 10 to 12mm. At <strong>the</strong> lower aspect <strong>of</strong> <strong>the</strong> entrance, Tenon’scapsule is reduplicated. At <strong>the</strong> upper aspect, itcontinues forward as a single membrane (Fig.3–10). The muscle sheaths <strong>of</strong> <strong>the</strong> four rectus musclesare connected by a formation known as <strong>the</strong>intermuscular membrane, which closely relates<strong>the</strong>se muscles to each o<strong>the</strong>r (Fig. 3–11). In addition,<strong>the</strong>re are numerous extensions from all <strong>the</strong>sheaths <strong>of</strong> <strong>the</strong> extraocular muscles, which form anintricate system <strong>of</strong> fibrous attachments interconnecting<strong>the</strong> muscles, attaching <strong>the</strong>m to <strong>the</strong> orbit,supporting <strong>the</strong> globe, and checking <strong>the</strong> ocularmovements. These will now be described in <strong>the</strong>iressential features.The fascial sheath <strong>of</strong> <strong>the</strong> superior rectus muscleclosely adheres in its anterior external surface to<strong>the</strong> undersurface <strong>of</strong> <strong>the</strong> sheath <strong>of</strong> <strong>the</strong> levator muscle<strong>of</strong> <strong>the</strong> upper lid. In front <strong>of</strong> <strong>the</strong> equator <strong>the</strong>sheath <strong>of</strong> <strong>the</strong> superior rectus muscle also sends aseparate extension obliquely forward that widensand ends on <strong>the</strong> lower surface <strong>of</strong> <strong>the</strong> levator muscle.The fusion <strong>of</strong> <strong>the</strong> two muscles accounts for<strong>the</strong> cooperation <strong>of</strong> upper lid and globe in elevation<strong>of</strong> <strong>the</strong> eye, a fact that must be kept in mind whensurgical procedures on <strong>the</strong> superior rectus muscleare being considered.The fascial sheath <strong>of</strong> <strong>the</strong> inferior rectus muscledivides anteriorly into two layers: an upper one,which becomes part <strong>of</strong> Tenon’s capsule, and aFIGURE 3–9. Anterior and posteriororifice <strong>of</strong> Tenon’s capsule shownafter enucleation <strong>of</strong> <strong>the</strong> globe. (Modifiedfrom Charpy A: <strong>Muscles</strong> et capsulede Tenon. In Poirier P, Charpy A,eds: Traité d’anatomie humaine, newed, vol 5/2. Paris, Masson, 1912, p539.)
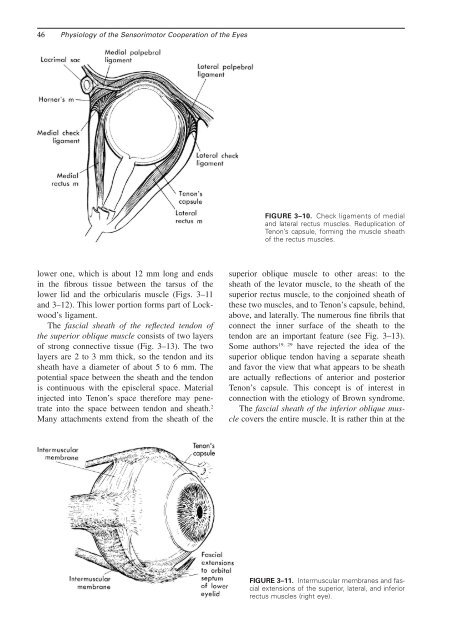
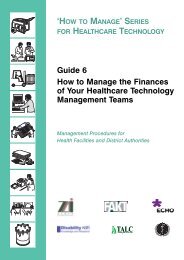
46 Physiology <strong>of</strong> <strong>the</strong> Sensorimotor Cooperation <strong>of</strong> <strong>the</strong> EyesFIGURE 3–10. Check ligaments <strong>of</strong> medialand lateral rectus muscles. Reduplication <strong>of</strong>Tenon’s capsule, forming <strong>the</strong> muscle sheath<strong>of</strong> <strong>the</strong> rectus muscles.lower one, which is about 12 mm long and endsin <strong>the</strong> fibrous tissue between <strong>the</strong> tarsus <strong>of</strong> <strong>the</strong>lower lid and <strong>the</strong> orbicularis muscle (Figs. 3–11and 3–12). This lower portion forms part <strong>of</strong> Lockwood’sligament.The fascial sheath <strong>of</strong> <strong>the</strong> reflected tendon <strong>of</strong><strong>the</strong> superior oblique muscle consists <strong>of</strong> two layers<strong>of</strong> strong connective tissue (Fig. 3–13). The twolayers are 2 to 3 mm thick, so <strong>the</strong> tendon and itssheath have a diameter <strong>of</strong> about 5 to 6 mm. Thepotential space between <strong>the</strong> sheath and <strong>the</strong> tendonis continuous with <strong>the</strong> episcleral space. Materialinjected into Tenon’s space <strong>the</strong>refore may penetrateinto <strong>the</strong> space between tendon and sheath. 2Many attachments extend from <strong>the</strong> sheath <strong>of</strong> <strong>the</strong>superior oblique muscle to o<strong>the</strong>r areas: to <strong>the</strong>sheath <strong>of</strong> <strong>the</strong> levator muscle, to <strong>the</strong> sheath <strong>of</strong> <strong>the</strong>superior rectus muscle, to <strong>the</strong> conjoined sheath <strong>of</strong><strong>the</strong>se two muscles, and to Tenon’s capsule, behind,above, and laterally. The numerous fine fibrils thatconnect <strong>the</strong> inner surface <strong>of</strong> <strong>the</strong> sheath to <strong>the</strong>tendon are an important feature (see Fig. 3–13).19, 29Some authors have rejected <strong>the</strong> idea <strong>of</strong> <strong>the</strong>superior oblique tendon having a separate sheathand favor <strong>the</strong> view that what appears to be sheathare actually reflections <strong>of</strong> anterior and posteriorTenon’s capsule. This concept is <strong>of</strong> interest inconnection with <strong>the</strong> etiology <strong>of</strong> Brown syndrome.The fascial sheath <strong>of</strong> <strong>the</strong> inferior oblique musclecovers <strong>the</strong> entire muscle. It is ra<strong>the</strong>r thin at <strong>the</strong>FIGURE 3–11. Intermuscular membranes and fascialextensions <strong>of</strong> <strong>the</strong> superior, lateral, and inferiorrectus muscles (right eye).