GINA_WR_2006.qxp:GINA_WR_2006.qxp 7/20/07 4:11 PM Page *10EXECUTIVE SUMMARYMANAGING ASTHMA IN CHILDREN 5 YEARS AND YOUNGERINTRODUCTIONSince the first <strong>asthma</strong> guidelines were published morethan 30 years ago, there has been a trend towards producingunified guidelines that apply to all age groups. Thishas been prompted by the recognition that commonpathogenic <strong>and</strong> inflammatory mechanisms underlie all<strong>asthma</strong>, evidence-based literature on the efficacy of keycontroller <strong>and</strong> reliever medications, <strong>and</strong> an ef<strong>for</strong>t to unifytreatment approaches <strong>for</strong> <strong>asthma</strong> patients in different agecategories. This approach avoids repetition of details thatare common to all patients with <strong>asthma</strong>. There is relativelylittle age-specific data on <strong>management</strong> of <strong>asthma</strong> inchildren, <strong>and</strong> guidelines have tended to extrapolate fromevidence gained from adolescents <strong>and</strong> adults.This revision of the Global Strategy <strong>for</strong> AsthmaManagement <strong>and</strong> Prevention again provides a unified textas a source document. Each chapter contains separatesections containing details <strong>and</strong> <strong>management</strong> advice <strong>for</strong>specific age categories where these are consideredrelevant. These age groups include children 5 years <strong>and</strong>younger (sometimes called preschool age), children olderthan 5 years, adolescents, adults, <strong>and</strong> the elderly. Most ofthe differences between these age groups relate to naturalhistory <strong>and</strong> comorbidities, but there are also importantdifferences in the approach to diagnosis, measures <strong>for</strong>assessing severity <strong>and</strong> monitoring control, responses todifferent classes of medications, techniques <strong>for</strong> engagingwith the patient <strong>and</strong> his/her family in establishing <strong>and</strong>maintaining a treatment plan, <strong>and</strong> the psychosocialchallenges presented at different stages of life.Special challenges that must be taken into account inmanaging <strong>asthma</strong> in children in the first 5 years of lifeinclude difficulties with diagnosis, the efficacy <strong>and</strong> safety ofdrugs <strong>and</strong> drug delivery systems, <strong>and</strong> the lack of data onnew therapies. Patients in this age group are oftenmanaged by pediatricians who are routinely faced with awide variety of issues related to childhood diseases.There<strong>for</strong>e, <strong>for</strong> the convenience of readers this ExecutiveSummary extracts sections of the report that pertain todiagnosis <strong>and</strong> <strong>management</strong> of <strong>asthma</strong> in children 5 years<strong>and</strong> younger. These extracts may also be found in themain text, together with detailed discussion of otherrelevant background data on <strong>asthma</strong> in this age group‡.As emphasized throughout the report, <strong>for</strong> patients in allage groups with a confirmed diagnosis of <strong>asthma</strong>, the goalxof treatment should be to achieve <strong>and</strong> maintain control(see Figure 4.3-2) <strong>for</strong> prolonged periods, with due regardto the safety of treatment, potential <strong>for</strong> adverse effects,<strong>and</strong> the cost of treatment required to achieve this goal.DIAGNOSIS OF ASTHMA IN CHILDREN 5 YEARS ANDYOUNGERWheezing <strong>and</strong> diagnosis of <strong>asthma</strong>: Diagnosis of <strong>asthma</strong>in children 5 years <strong>and</strong> younger presents a particularlydifficult problem. This is because episodic wheezing <strong>and</strong>cough are also common in children who do not have<strong>asthma</strong>, particularly in those under age 3. Wheezing isusually associated with a viral respiratory illness—predominantly respiratory syncytial virus in childrenyounger than age 2, <strong>and</strong> other viruses in older preschoolchildren. Three categories of wheezing have beendescribed in children 5 years <strong>and</strong> younger:• Transient early wheezing, which is often outgrown inthe first 3 years. This is often associated withprematurity <strong>and</strong> parental smoking.• Persistent early-onset wheezing (be<strong>for</strong>e age 3). Thesechildren typically have recurrent episodes of wheezingassociated with acute viral respiratory infections, noevidence of atopy, <strong>and</strong> no family history of atopy.Their symptoms normally persist through school age<strong>and</strong> are still present at age 12 in a large proportion ofchildren. The cause of wheezing episodes is usuallyrespiratory syncytial virus in children younger than age 2,while other viruses predominate in children ages 2-5.• Late-onset wheezing/<strong>asthma</strong>. These children have<strong>asthma</strong> that often persists throughout childhood <strong>and</strong>into adult life. They typically have an atopicbackground, often with eczema, <strong>and</strong> airway pathologythat is characteristic of <strong>asthma</strong>.The following categories of symptoms are highlysuggestive of a diagnosis of <strong>asthma</strong>: frequent episodes ofwheeze (more than once a month), activity-induced coughor wheeze, nocturnal cough in periods without viralinfections, absence of seasonal variation in wheeze, <strong>and</strong>symptoms that persist after age 3. A simple clinical indexbased on the presence of a wheeze be<strong>for</strong>e the age of 3,<strong>and</strong> the presence of one major risk factor (parental historyof <strong>asthma</strong> or eczema) or two of three minor risk factors(eosinophilia, wheezing without colds, <strong>and</strong> allergic rhinitis)has been shown to predict the presence of <strong>asthma</strong> inlater childhood.‡ References <strong>and</strong> evidence levels are deleted from this extracted material but are provided in the main text.
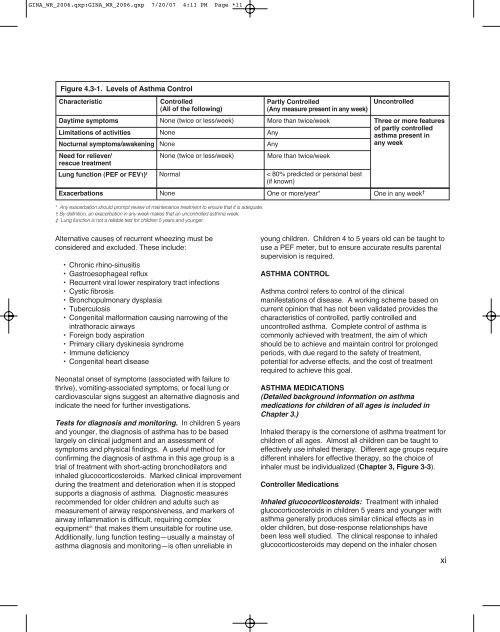
GINA_WR_2006.qxp:GINA_WR_2006.qxp 7/20/07 4:11 PM Page *11Figure 4.3-1. Levels of Asthma ControlCharacteristicControlled(All of the following)Partly Controlled(Any measure present in any week)UncontrolledDaytime symptoms None (twice or less/week) More than twice/week Three or more featuresLimitations of activities None Anyof partly controlled<strong>asthma</strong> present inNocturnal symptoms/awakening None Anyany weekNeed <strong>for</strong> reliever/rescue treatmentNone (twice or less/week)More than twice/weekLung function (PEF or FEV1) ‡ Normal < 80% predicted or personal best(if known)Exacerbations None One or more/year* One in any week †* Any exacerbation should prompt review of maintenance treatment to ensure that it is adequate.† By definition, an exacerbation in any week makes that an uncontrolled <strong>asthma</strong> week.‡ Lung function is not a reliable test <strong>for</strong> children 5 years <strong>and</strong> younger.Alternative causes of recurrent wheezing must beconsidered <strong>and</strong> excluded. These include:• Chronic rhino-sinusitis• Gastroesophageal reflux• Recurrent viral lower respiratory tract infections• Cystic fibrosis• Bronchopulmonary dysplasia• Tuberculosis• Congenital mal<strong>for</strong>mation causing narrowing of theintrathoracic airways• Foreign body aspiration• Primary ciliary dyskinesia syndrome• Immune deficiency• Congenital heart diseaseNeonatal onset of symptoms (associated with failure tothrive), vomiting-associated symptoms, or focal lung orcardiovascular signs suggest an alternative diagnosis <strong>and</strong>indicate the need <strong>for</strong> further investigations.Tests <strong>for</strong> diagnosis <strong>and</strong> monitoring. In children 5 years<strong>and</strong> younger, the diagnosis of <strong>asthma</strong> has to be basedlargely on clinical judgment <strong>and</strong> an assessment ofsymptoms <strong>and</strong> physical findings. A useful method <strong>for</strong>confirming the diagnosis of <strong>asthma</strong> in this age group is atrial of treatment with short-acting bronchodilators <strong>and</strong>inhaled glucocorticosteroids. Marked clinical improvementduring the treatment <strong>and</strong> deterioration when it is stoppedsupports a diagnosis of <strong>asthma</strong>. Diagnostic measuresrecommended <strong>for</strong> older children <strong>and</strong> adults such asmeasurement of airway responsiveness, <strong>and</strong> markers ofairway inflammation is difficult, requiring complexequipment 41 that makes them unsuitable <strong>for</strong> routine use.Additionally, lung function testing—usually a mainstay of<strong>asthma</strong> diagnosis <strong>and</strong> monitoring—is often unreliable inyoung children. Children 4 to 5 years old can be taught touse a PEF meter, but to ensure accurate results parentalsupervision is required.ASTHMA CONTROLAsthma control refers to control of the clinicalmanifestations of disease. A working scheme based oncurrent opinion that has not been validated provides thecharacteristics of controlled, partly controlled <strong>and</strong>uncontrolled <strong>asthma</strong>. Complete control of <strong>asthma</strong> iscommonly achieved with treatment, the aim of whichshould be to achieve <strong>and</strong> maintain control <strong>for</strong> prolongedperiods, with due regard to the safety of treatment,potential <strong>for</strong> adverse effects, <strong>and</strong> the cost of treatmentrequired to achieve this goal.ASTHMA MEDICATIONS(Detailed background in<strong>for</strong>mation on <strong>asthma</strong>medications <strong>for</strong> children of all ages is included inChapter 3.)Inhaled therapy is the cornerstone of <strong>asthma</strong> treatment <strong>for</strong>children of all ages. Almost all children can be taught toeffectively use inhaled therapy. Different age groups requiredifferent inhalers <strong>for</strong> effective therapy, so the choice ofinhaler must be individualized (Chapter 3, Figure 3-3).Controller MedicationsInhaled glucocorticosteroids: Treatment with inhaledglucocorticosteroids in children 5 years <strong>and</strong> younger with<strong>asthma</strong> generally produces similar clinical effects as inolder children, but dose-response relationships havebeen less well studied. The clinical response to inhaledglucocorticosteroids may depend on the inhaler chosenxi