How to Enforce Employment Rights Under the Americans with ...
How to Enforce Employment Rights Under the Americans with ...
How to Enforce Employment Rights Under the Americans with ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
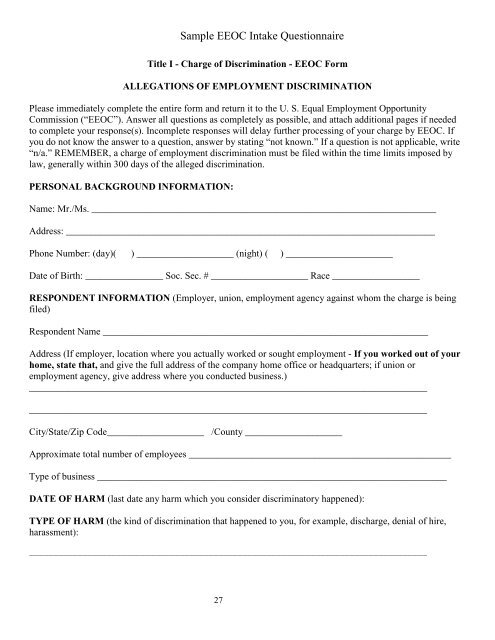
Sample EEOC Intake QuestionnaireTitle I - Charge of Discrimination - EEOC FormALLEGATIONS OF EMPLOYMENT DISCRIMINATIONPlease immediately complete <strong>the</strong> entire form and return it <strong>to</strong> <strong>the</strong> U. S. Equal <strong>Employment</strong> OpportunityCommission (“EEOC”). Answer all questions as completely as possible, and attach additional pages if needed<strong>to</strong> complete your response(s). Incomplete responses will delay fur<strong>the</strong>r processing of your charge by EEOC. Ifyou do not know <strong>the</strong> answer <strong>to</strong> a question, answer by stating “not known.” If a question is not applicable, write“n/a.” REMEMBER, a charge of employment discrimination must be filed <strong>with</strong>in <strong>the</strong> time limits imposed bylaw, generally <strong>with</strong>in 300 days of <strong>the</strong> alleged discrimination.PERSONAL BACKGROUND INFORMATION:Name: Mr./Ms. _______________________________________________________________________Address: ____________________________________________________________________________Phone Number: (day)( ) ____________________ (night) ( ) ______________________Date of Birth: ________________ Soc. Sec. # ____________________ Race __________________RESPONDENT INFORMATION (Employer, union, employment agency against whom <strong>the</strong> charge is beingfiled)Respondent Name ___________________________________________________________________Address (If employer, location where you actually worked or sought employment - If you worked out of yourhome, state that, and give <strong>the</strong> full address of <strong>the</strong> company home office or headquarters; if union oremployment agency, give address where you conducted business.)____________________________________________________________________________________________________________________________________________________________________City/State/Zip Code____________________ /County ____________________Approximate <strong>to</strong>tal number of employees ______________________________________________________Type of business ________________________________________________________________________DATE OF HARM (last date any harm which you consider discrimina<strong>to</strong>ry happened):TYPE OF HARM (<strong>the</strong> kind of discrimination that happened <strong>to</strong> you, for example, discharge, denial of hire,harassment):__________________________________________________________________________________27