

An Overview on: Sublingual Route for Systemic Drug Delivery
An Overview on: Sublingual Route for Systemic Drug Delivery
An Overview on: Sublingual Route for Systemic Drug Delivery

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
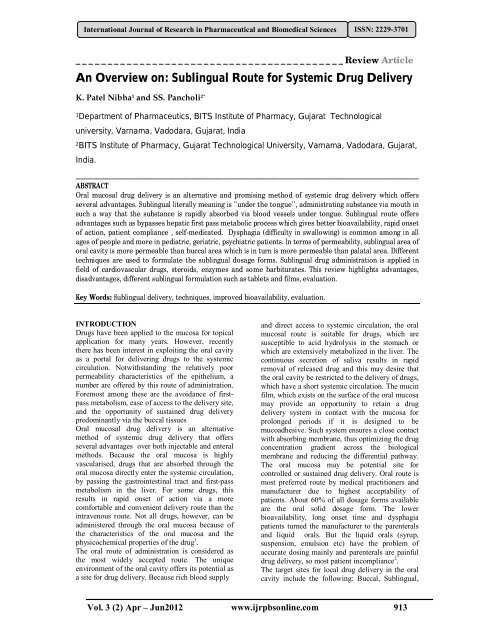
Internati<strong>on</strong>al Journal of Research in Pharmaceutical and Biomedical Sciences ISSN: 2229-3701can create problem in swallowing the food andpotential <strong>for</strong> food lodge in the throat increases.The absorpti<strong>on</strong> is transfer of the drug from its siteof administrati<strong>on</strong> into systemic circulati<strong>on</strong>, so itcan be said that absorpti<strong>on</strong> is directly proporti<strong>on</strong>allayer thickness. The absorpti<strong>on</strong> of the drug followsin this way <strong>Sublingual</strong> > Buccal > Gingival >Palatal. Due to high permeability and rich bloodsupply, the sublingual route can produce rapid<strong>on</strong>set of acti<strong>on</strong> so the drug with short deliveryperiod can be delivered and dose regimen isfrequent. The drug gets diluted in the saliva andfrom there the drug is adsorbed across the oralcavity.For example: Glyceryl nitrate-a potent cor<strong>on</strong>aryvasodilator which is used <strong>for</strong> rapid symptomaticrelief of angina. After administrati<strong>on</strong> its getspharmacologically active after 1-2 minutes. Oralspray was found to provide rapid relief ofsymptom with first class metabolism. The extent offirst class metabolism when compared to thesublingual spray decreased to 48% with sublingualtablets and 28% with the oral dose. Nitrate whichappears in the plasma c<strong>on</strong>centrati<strong>on</strong> can bemaintained <strong>for</strong> 24 hours when administratedsublingually 9 .The Mechanism of <strong>Sublingual</strong> Absorpti<strong>on</strong>The absorpti<strong>on</strong> potential of the buccal mucosa isinfluenced by the lipid solubility and there<strong>for</strong>e thepermeability of the soluti<strong>on</strong> (osmosis), thei<strong>on</strong>izati<strong>on</strong> (pH), and the molecular weight of thesubstances. For example, absorpti<strong>on</strong> of some drugsvia the buccal mucosa is shown to increase whencarrier pH is lowering (more acidic) and decreasewith a lowering of pH (more alkaline). The cells ofthe oral epithelium and epidermis are also capableof absorbing by endocytosis (the uptake of particlesby a cell as if by hollowly wrapping itself around it.These engulfed particles are usually too large todiffuse through its wall). It is unlikely that thismechanism is used across the entire stratifiedepithelium. It is also unlikely that active transportprocesses operate within the oral mucosa.However, it is believed that acidic stimulati<strong>on</strong> anduptake into the circulatory system.The mouth is lined with a mucous membranewhich is covered with squamous epithelium andc<strong>on</strong>tains mucous glands. The buccal mucosa issimilar to the sublingual mucosal tissue.The salivary glands c<strong>on</strong>sist of lobules of cellswhich secrete saliva through the salivary ducts intothe mouth. The three pairs of salivary glands arethe Parotid, the Sub mandibular and the <strong>Sublingual</strong>which lies <strong>on</strong> the floor of the mouth. The more acidthe taste the greater the stimulati<strong>on</strong> of salivaryoutput, serving also to avoid potential harm to acidsensitive tooth enamel by bathing the mouth incopious neutralizing fluid. With stimulati<strong>on</strong> ofsalivary secreti<strong>on</strong> oxygen is c<strong>on</strong>sumed andvasodilator substances are produced, and theglandular blood flow increases, due to increasedglandular metabolism.The sublingual artery travels <strong>for</strong>ward to thesublingual gland, it supplies the gland and branchesto the neighboring muscles and to the mucousmembranes of the mouth, t<strong>on</strong>gue and gums. Twosymmetrical branches travel behind the jaw b<strong>on</strong>eunder the t<strong>on</strong>gue to meet and join at its tip. <str<strong>on</strong>g>An</str<strong>on</strong>g>otherbranches meets and anastomoses with the submental branches of the facial artery. The sublingualartery system stems from the lingual artery – thebody’s main blood supply to the t<strong>on</strong>gue and thefloor of the mouth – which arises from the externalcarotid artery. The proximity with the internalcarotid artery allows fast access to its routesupplying the greater part of the cerebralhemisphere<strong>Drug</strong>s <strong>for</strong> sublingual administrati<strong>on</strong><strong>Sublingual</strong> drug administrati<strong>on</strong> is applied in thefield of cardiovascular drugs, steroids, somebarbiturates and enzymes. It has been a developingfield in the administrati<strong>on</strong> of many vitamins andminerals which are found to be readily andthoroughly absorbed by this method. <strong>Sublingual</strong>lyabsorbed nutriti<strong>on</strong>, which avoids exposure to thegastric system and liver, means direct nutriti<strong>on</strong>albenefits, particularly important <strong>for</strong> sufferers ofgastro‐intestinal difficulties such as ulcers,hyperactive gut, coeliac disease, those withcompromised digesti<strong>on</strong>, the elderly and invalids –the nutriti<strong>on</strong>al benefit is independent ofgastro‐intestinal influences (10,11) . Examples of drugsadministered by this route include antianginal likenitrites and nitrates, anti hypertensive likenifedipine, analgesics like morphine andbr<strong>on</strong>chodilators like fenoterol. Certain steroids likeestradiol and peptides like oxytocin can also beadministered e.g. fentanyl citrate, apomorphine,prochlorperazine dimaleate {PRO}, and hydrazineHCl {HYD}.<strong>Sublingual</strong> <strong>for</strong>mulati<strong>on</strong><strong>Sublingual</strong> tabletsThey are to be placed under the t<strong>on</strong>gue and produceimmediate systemic effect by enabling the drugabsorbed directly through mucosal lining of themouth beneath the t<strong>on</strong>gue. The drug absorbed fromstomach goes to mesenteric circulati<strong>on</strong> whichc<strong>on</strong>nects to stomach via portal vein. Thusabsorpti<strong>on</strong> through oral cavity avoids first passmetabolism. The tablets are usually small and flat,compressed lightly to keep them soft. The tabletmust dissolve quickly allowing the API to beabsorbed quickly. It is designed to dissolve in smallquantity of saliva. After the tablet is placed in themouth below the t<strong>on</strong>gue, the patient should avoideating, drinking, smoking and possibly talking inVol. 3 (2) Apr – Jun2012 www.ijrpbs<strong>on</strong>line.com 915
Internati<strong>on</strong>al Journal of Research in Pharmaceutical and Biomedical Sciences ISSN: 2229-3701order to keep the tablet in place. Swallowing ofsaliva should also be avoided since the saliva mayc<strong>on</strong>tain dissolved drug. Bland excipients are usedto avoid salivary stimulati<strong>on</strong>. Various techniquescan be used to <strong>for</strong>mulate rapidly disintegrating ordissolving tablets. (12,13) Direct compressi<strong>on</strong> is <strong>on</strong>eof these techniques which require incorporati<strong>on</strong> ofa superdisintegrant into the <strong>for</strong>mulati<strong>on</strong>, or the useof highly water-soluble excipients to achieve fasttablet disintegrati<strong>on</strong>. Direct compressi<strong>on</strong> does notrequire the use of water or heat during the<strong>for</strong>mulati<strong>on</strong> procedure and is the ideal method <strong>for</strong>moisture and heat-labile medicati<strong>on</strong>s.a) Fast disintegrating sublingual tablets (FDT)FDT is defined as a solid dosage <strong>for</strong>m that c<strong>on</strong>tainsmedicinal substances and disintegrates rapidly(within few sec<strong>on</strong>ds) without water when kept <strong>on</strong>the t<strong>on</strong>gue. The drug is released, dissolved, ordispersed in the saliva, and then swallowed andabsorbed across the GIT (14) . FDTs also are alsocalled as Orodispersible tablet, mouth-dissolving,quick-dissolving, fast-melt, and freeze-driedwafers. Tablets that disintegrate or dissolve rapidlyin the patient’s mouth are c<strong>on</strong>venient <strong>for</strong> youngchildren, the elderly and patients with swallowingdifficulties and in situati<strong>on</strong>s where potable liquidsare not available. Direct compressi<strong>on</strong> is <strong>on</strong>e of thetechniques which require the incorporati<strong>on</strong> of asuperdisintegrant into the <strong>for</strong>mulati<strong>on</strong>, or the use ofhighly water soluble excipients to achieve fasttablet disintegrati<strong>on</strong>. Compared to c<strong>on</strong>venti<strong>on</strong>aldosage <strong>for</strong>m the drug dissoluti<strong>on</strong>, its absorpti<strong>on</strong> aswell as <strong>on</strong>set of clinical acti<strong>on</strong> and itsbioavailability may be significantly greater (15-17) .Though chewable tablets are available in themarket, they are not same as the new FDTs.Patients <strong>for</strong> whom chewing is difficult or painfulcan use these FDTs. It can be used easily in infantsand in children who have lost their primary teethand who do not have full use of their permanentteeth (18) .Recent market studies indicate that more than halfof the patients prefers FDTs than otherc<strong>on</strong>venti<strong>on</strong>al dosage <strong>for</strong>ms (19) and most patientswould ask their doctors <strong>for</strong> FDTs (70%), purchaseFDTs (70%), or prefer FDTs than regular tablets orliquids (>80%) (20) . The US Food and <strong>Drug</strong>Administrati<strong>on</strong> Center <strong>for</strong> <strong>Drug</strong> Evaluati<strong>on</strong> andResearch (CDER) defines, in the „Orange Book ,an FDT as “a solid dosage <strong>for</strong>m c<strong>on</strong>tainingmedicinal substances, which disintegrates rapidlyin saliva, usually within a few sec<strong>on</strong>ds, whenplaced up<strong>on</strong> the t<strong>on</strong>gue” (21). The implicati<strong>on</strong> ofthese dosage <strong>for</strong>ms is emphasized by the term“Orodispersible Tablet”, by the EuropeanPharmacopoeia which defines it as a tablet that canbe placed in oral cavity where it disperses rapidlybe<strong>for</strong>e swallowing (22) . FDTs has been developed<strong>for</strong> numerous indicati<strong>on</strong>s ranging from migraines(in which quick <strong>on</strong>set of acti<strong>on</strong> is necessary) tomental illness (in which patient compliance isnecessary <strong>for</strong> treating chr<strong>on</strong>ic indicati<strong>on</strong>s such asmental depressi<strong>on</strong> and schizophrenia) (23) .b)Bioadhesive sublingual tabletsThe new sublingual tablet c<strong>on</strong>cept presented isbased <strong>on</strong> interactive mixtures c<strong>on</strong>sisting of a watersoluble carrier covered with fine drug particles anda bioadhesive comp<strong>on</strong>ent. With this approach, it ispossible to maintain rapid dissoluti<strong>on</strong> incombinati<strong>on</strong> with bioadhesive retenti<strong>on</strong> of the drugin the oral cavity. Bioadhesi<strong>on</strong> is usually defined asthe b<strong>on</strong>d <strong>for</strong>med between two biological surfacesor between a biological and a synthetic surface.Problem associated with sublingual tablet<strong>for</strong>mulati<strong>on</strong> is that there is always a risk that thepatient will swallow part of the dose be<strong>for</strong>e theactive substance has been released and absorbedlocally into systemic circulati<strong>on</strong>. this could resultsan unwanted prol<strong>on</strong>gati<strong>on</strong> of the pharmacologicaleffect. Additi<strong>on</strong> of a bioadhesive comp<strong>on</strong>ent is awell-known method of increasing the possibility ofa more site-specific release. However, this c<strong>on</strong>ceptis normally applied to n<strong>on</strong>-disintegrating tablets ordisc to achieve extended release of the activesubstance and, c<strong>on</strong>sequently, such a system will notbe suitable <strong>for</strong> a fast acting <strong>for</strong>mulati<strong>on</strong>. There<strong>for</strong>e,it would be of interest to study a disintegratingtablet which releases the drug quickly, but whichalso has bioadhesive properties which couldprevent the drug from being swallowed.Bioadhesi<strong>on</strong> mechanismsThe mucus layer is often involved in the adhesi<strong>on</strong>of a bioadhesive polymer and is present as either agel layer adhering to the mucosal surface or asoluti<strong>on</strong> or suspensi<strong>on</strong> of various substances. Themucus layer mainly c<strong>on</strong>sists of mucin glycoprotein,Vol. 3 (2) Apr – Jun2012 www.ijrpbs<strong>on</strong>line.com 916
Internati<strong>on</strong>al Journal of Research in Pharmaceutical and Biomedical Sciences ISSN: 2229-3701inorganic salts, proteins, lipids and water with thecompositi<strong>on</strong> varying depending <strong>on</strong> its source. Theelectr<strong>on</strong>ic theory involves an electr<strong>on</strong>ic transferbetween the two materials causing a double layerof electric charge, which results in attracti<strong>on</strong> <strong>for</strong>ces.The adsorpti<strong>on</strong> theory involves adhesi<strong>on</strong> betweenthe mucosa and the adhesive material by van derwaals interacti<strong>on</strong>, hydrogen b<strong>on</strong>ds and related<strong>for</strong>ces. The wetting theory involves interfacialtensi<strong>on</strong>s between the two materials. Penetrati<strong>on</strong> ofthe polymer chains into the mucus network andvice versa, causing a mechanical b<strong>on</strong>d, is referredto as the diffusi<strong>on</strong> theory. The importance of waterc<strong>on</strong>tent and movement of water into the adhesivematerial from the mucosa, i.e. dehydrati<strong>on</strong> of themucosa, has also been suggested as a mechanical<strong>for</strong> adhesi<strong>on</strong>.Measurement of bio-adhesive strengthBio-adhesi<strong>on</strong> strength of the tablets was measured<strong>on</strong> a modified physical balance. The method usedbovine cheek pouch as the method mucosal andIPB ph 6.6 as the moistening fluid. The surface ofthe mucosal membrane was first blotted with afilter paper and then moistened with 25/L 1 of IPBpH 6.6. the weight in grams is required to detachthe tablets from the mucosal surface gave themeasure of bio-adhesive strength.c) Lipid matrix sublingual tabletsSuch tablets are <strong>for</strong>mulated using advances insublingual and liposomal technology to create adosage <strong>for</strong>m that offers a faster and more completeabsorpti<strong>on</strong> than traditi<strong>on</strong>al oral routes ofadministrati<strong>on</strong>. The lipid matrix sublingual tablet isa bioavailable, quick, c<strong>on</strong>venient and c<strong>on</strong>sistentdosage <strong>for</strong>m <strong>for</strong> many neutraceuticals that are oftentaken orally.For e.g., Glutathi<strong>on</strong>e MB12(methylcobalamin)melat<strong>on</strong>in.d) <strong>Sublingual</strong> vitamin tabletVitamin D i.e. cholecalciferol is a natural precursorof calcium regulating horm<strong>on</strong>e calcitriol. VitaminD is thus used in hypocalcaemia/hyperparathyroidism. Because of its incompleteabsorpti<strong>on</strong> from GI tract, local intestinaldegradati<strong>on</strong> and hepatic metabolism, it is givensublingually.2)Thin film drug deliveryThin film drug delivery is a process of deliveringdrugs of the systemic circulati<strong>on</strong> via thin film thatdissolves when in c<strong>on</strong>tact with liquid, oftenreferred to a dissolving films or strips and dissolvewithin 1 min when placed in the mouth withoutdrinking or chewing.Such dissolving film or strip are typically designed<strong>for</strong> oral administrati<strong>on</strong>, with the user placing thestrip <strong>on</strong> or under the t<strong>on</strong>gue or al<strong>on</strong>g the inside ofthe cheek. Thin film’s ability to dissolve rapidlywithout the need <strong>for</strong> water provides an alternativeto patients with swallowing disorders and topatients suffering from nausea, such as thosepatients receiving chemotherapy.The first developed fast-dissolving dosage <strong>for</strong>mc<strong>on</strong>sisted in tablet <strong>for</strong>m, and the rapiddisintegrating properties were obtained through aspecial process or <strong>for</strong>mulati<strong>on</strong> modificati<strong>on</strong>s 24 .More recently, fast-dissolving films are gaininginterest as an alternative to fast-dissolving tablets todefinitely eliminate patients’ fear of chocking andovercome patent impediments. Fast-dissolvingfilms are generally c<strong>on</strong>stituted of plasticizedhydrocolloids. Problems are caused by foamingduring the film <strong>for</strong>mati<strong>on</strong> due to the heating of thematerial or solvent evaporati<strong>on</strong>, the flaking duringthe slitting and the cracking in the cutting phase.The films should be stable to moisture, facilitatethe handling, have to be flexible and exhibit asuitable tensile stress and do not stick to thepackaging materials and fingers.Film can be prepared by five method: 1) Solventcasting. 2)Semisolid casting. 3)Hot melt extrusi<strong>on</strong>.4)Solid dispersi<strong>on</strong> extrusi<strong>on</strong>. 5) Rolling.1) Solvent casting methodFilm is <strong>for</strong>mulated using the solvent castingmethod, whereby the water-soluble ingredients aredissolved to <strong>for</strong>m a clear viscous soluti<strong>on</strong>. The APIand other agents are dissolved in smaller amountsof the soluti<strong>on</strong> and combined with the bulk. Thismixture is then added to the aqueous viscoussoluti<strong>on</strong>. The entrapped air is removed by vacuum.The resulting soluti<strong>on</strong> is cast as a film and allowedto dry, which is then cut into pieces of the desiredsize. 252)Semisolid castingSoluti<strong>on</strong> of water soluble film <strong>for</strong>ming polymer ismixed with soluti<strong>on</strong> of acid insoluble polymerwhich <strong>for</strong>ms homogenous viscous soluti<strong>on</strong>. Theratio should be 1:4. For e.g. cellulose acetatephthalate, cellulose acetate butyrate. It is thens<strong>on</strong>icated which is coated <strong>on</strong> n<strong>on</strong>-treated castingfilm.3)Hot Melt Extrusi<strong>on</strong>In present method the mass is prepared first underthe c<strong>on</strong>trol of temperature and steering speed.Afterwards, the film is coated and dried in a dryingtunnel, <strong>on</strong>ce again the temperature, air circulati<strong>on</strong>and line speed are c<strong>on</strong>trolled. Then follows aslitting and in the last step the films are punched,pouched and sealed. 264)Solid Dispersi<strong>on</strong> Extrusi<strong>on</strong>Solid dispersi<strong>on</strong>s are prepared by immisciblecomp<strong>on</strong>ents and drug. Finally the solid dispersi<strong>on</strong>sare shaped in to films by means of dies.5)RollingSoluti<strong>on</strong> or suspensi<strong>on</strong> drug is rolled <strong>on</strong> the carrier.The solvent is mainly water and mixture of waterVol. 3 (2) Apr – Jun2012 www.ijrpbs<strong>on</strong>line.com 917
Internati<strong>on</strong>al Journal of Research in Pharmaceutical and Biomedical Sciences ISSN: 2229-3701and alcohol. The film is dried <strong>on</strong> the rollers andgives desired shape and size 27 .Evaluati<strong>on</strong>Hardness and thicknessThe test is d<strong>on</strong>e as per the standard methods. Thehardness of three randomly selected tablets fromeach <strong>for</strong>mulati<strong>on</strong> is determined by placing eachtablet diag<strong>on</strong>ally between the two plungers of tablethardness tester (with the nozzle) and applyingpressure until the tablet broke down into two partscompletely and the reading <strong>on</strong> the scale is noteddown (28) .The thickness of three randomly selectedtablets from each <strong>for</strong>mulati<strong>on</strong> is determined in mmusing a vernier caliper (Pico India). The averagevalues is calculated 28 .<strong>Drug</strong> C<strong>on</strong>tentRandomly ten tablets are selected from<strong>for</strong>mulati<strong>on</strong>, finely powdered and powderequivalent mg of drug is accurately weighed andtransferred to 100 ml volumetric flasks c<strong>on</strong>tainingsoluti<strong>on</strong> of desired pH. The flask is shaken to mixthe c<strong>on</strong>tents thoroughly. The volume is made up tothe mark with soluti<strong>on</strong> and filtered. One ml of thefiltrate is suitably diluted and drug c<strong>on</strong>tent isestimated using a double beam UV-visiblespectrophotometer. This procedure is repeatedthrice and the average value is calculated.Wetting time (WT)It is useful <strong>for</strong> quality c<strong>on</strong>trol and providessupportive evaluati<strong>on</strong> of these sublingual tablets.Unlike the disintegrati<strong>on</strong> test, the wetting test usesminimal water, which may be more representativeof the quantity of moisture available sublingually.Using this test, the time required <strong>for</strong> moisture topenetrate the tablet completely is measured andpossibly represents the time required to releasedrug in the presence of minute volumes of salivaThe tablet was placed above absorbent paper fittedinto a petri dish. After the paper is thoroughlywetted with distilled water, excess water iscompletely drained out of the dish. The timerequired <strong>for</strong> the water to diffuse from the wettedabsorbent paper throughout the entire tablet is thenrecorded using a stopwatch 28Disintegrati<strong>on</strong> testA relatively simple method with rigorousc<strong>on</strong>diti<strong>on</strong>s is developed. Each individual tablet isdropped into 10‐ml glass test tube (1.5‐cmdiameter) c<strong>on</strong>taining 2ml distilled water, and thetime required <strong>for</strong> complete tablet disintegrati<strong>on</strong> isobserved visually and recorded using a stopwatch.The visual inspecti<strong>on</strong> is enhanced by gentlyrotating the test tube at a 45 0 angle, withoutagitati<strong>on</strong>, to distribute any tablet particles thatmight mask any remaining undisintegrated porti<strong>on</strong>of the tablets. In the USP disintegrati<strong>on</strong> test <strong>for</strong>sublingual tablets, the disintegrati<strong>on</strong> apparatus <strong>for</strong>oral tablets is used without the covering plasticdisks, 29 and 2 minutes is specified as the acceptabletime limit <strong>for</strong> tablet disintegrati<strong>on</strong> [29]. .Water absorpti<strong>on</strong> ratioA piece of tissue paper folded twice is placed in asmall Petri dish C<strong>on</strong>taining 6 ml of water. A tabletis put <strong>on</strong> the tissue paper and allowed to completelywet. The wetted tablet is then weighted. Waterabsorpti<strong>on</strong> ratio, R was determined using followingequati<strong>on</strong> 28 .R = 100 × Wa –Wb/Wawhere, Wa = Weight of tablet after waterabsorpti<strong>on</strong>Wb = Weight of tablet be<strong>for</strong>e water absorpti<strong>on</strong>.In vitro disintegrating testDisintegrati<strong>on</strong> times <strong>for</strong> sublingual tablets isdetermined using USP tablet disintegrati<strong>on</strong>apparatus with desired medium. The volume ofmedium was 900 ml and temp was 37± 2 °C. Thetime in sec<strong>on</strong>ds taken <strong>for</strong> complete disintegrati<strong>on</strong>of the tablets with no palatable mass remaining inthe apparatus is measured 28 .In vitro dissoluti<strong>on</strong> testIn-vitro release rate of sublingual tablets will becarried out using United State Pharmacopoeia(USP) XXIV dissoluti<strong>on</strong> testing apparatus (Paddlemethod). A aliquot sample of the soluti<strong>on</strong> iswithdrawn from the dissoluti<strong>on</strong> apparatus. Thesamples are replaced with fresh dissoluti<strong>on</strong>medium of same quantity. The samples are filteredthrough Whatman filter paper No 40 and analyzedin UV spectrophotometer. The percentage drugrelease is calculated using an equati<strong>on</strong> obtainedfrom the calibrati<strong>on</strong> curve 30 .Test <strong>for</strong> filmTensile StrengthTensile strength is the maximum stress applied to apoint at which the film specimen breaks 31 . It iscalculated by the applied load at rupture divided bythe cross-secti<strong>on</strong>al area of the film as given below:Tensile strength = Load at failure × 100Film thickness × film widthPercent El<strong>on</strong>gati<strong>on</strong>A film sample stretches when stress is applied andit is referred to as strain. Strain is basically thede<strong>for</strong>mati<strong>on</strong> of film divided by original dimensi<strong>on</strong>of the sample. El<strong>on</strong>gati<strong>on</strong> of film increases as theplasticizer c<strong>on</strong>tent increases.Vol. 3 (2) Apr – Jun2012 www.ijrpbs<strong>on</strong>line.com 918
Internati<strong>on</strong>al Journal of Research in Pharmaceutical and Biomedical Sciences ISSN: 2229-3701Percent El<strong>on</strong>gati<strong>on</strong>-L * 100Lowhere,L = Increase in length of filmLo = Initial length of film.Young's ModulusYoung's modulus or elastic modulus is the measureof stiffness of film. It is represented as the ratio ofapplied stress over strain in the regi<strong>on</strong> of elasticde<strong>for</strong>mati<strong>on</strong> as follows:Young's Modulus = Slope * 100Film thickness *Cross-head speedFolding EnduranceFolding endurance is determined by drying processrepeated folding of the film at the same place tillthe breaks. The number of times the film is foldedwithout dry breaking is computed as the foldingendurance value 32 .ThicknessThe thickness of the polymer films was measuredby using screw gauge. The thickness of each stripat six different areas was determined and standarddeviati<strong>on</strong> was calculated 33In vitro disintegrati<strong>on</strong> timeIn vitro disintegrati<strong>on</strong> time is determined visuallyin a glass dish of 25ml distilled water with swirlingevery 10 sec. The disintegrati<strong>on</strong> time is the timewhen the film starts to break or disintegrates. Thedisintegrati<strong>on</strong> time of prepared films was measuredin triplicate 34 .Uni<strong>for</strong>mity of drug c<strong>on</strong>tentThe film of area 1x1 cm2 was cut and dissolved in6.8 phosphate buffer soluti<strong>on</strong> and made up to 100mL in a volumetric flask. Then 1 mL waswithdrawn from the soluti<strong>on</strong> and diluted to 10mL.The absorbance of the soluti<strong>on</strong> was taken at 276nm and c<strong>on</strong>centrati<strong>on</strong> was calculated. By correctingdiluti<strong>on</strong> factor, the drug c<strong>on</strong>tent was calculated.The test was per<strong>for</strong>med in triplicate 35 .In-vitro dissoluti<strong>on</strong> studiesDissoluti<strong>on</strong> study was carried out in USP paddletype apparatus using 300 mL of stimulated salivaryfluid (pH 6.8) as a dissoluti<strong>on</strong> medium at 50 rpm.Temperature of the dissoluti<strong>on</strong> medium wasmaintained at 37±0.5ºC. Samples of 5ml werewithdrawn at every 4 minute interval, filtered(through 0.45µ) and replaced with 5ml of freshdissoluti<strong>on</strong> medium. The samples were suitablydiluted and estimated spectrophotometrically at 276nm by using ELICO-164 double beam UV-Visiblespectrophotometer. The dissoluti<strong>on</strong> experimentswere c<strong>on</strong>ducted in triplicate. Dissoluti<strong>on</strong> rate wasstudied <strong>for</strong> all designed <strong>for</strong>mulati<strong>on</strong>s anddissoluti<strong>on</strong> parameters were calculated.CONCLUSION<strong>Sublingual</strong> drug delivery have been used <strong>for</strong><strong>for</strong>mulati<strong>on</strong> of many drugs with view point of rapiddrug release and quick <strong>on</strong>set of acti<strong>on</strong>. <strong>Sublingual</strong>products were developed to overcome the difficultyin swallowing c<strong>on</strong>venti<strong>on</strong>al tablet, am<strong>on</strong>g pediatric,geriatric and psychiatric patients with dysphagia.The target populati<strong>on</strong> has expanded to those whowant c<strong>on</strong>venient dosing without water anywhere,anytime. The potential <strong>for</strong> such dosage <strong>for</strong>ms ispromising because str<strong>on</strong>g market acceptance andpatient demand. Peak blood levels of most productsadministered sublingually are achieved within10‐15 minutes, which is generally much faster thanwhen those same drugs are ingested orally.<strong>Sublingual</strong> absorpti<strong>on</strong> is efficient. The percent ofeach dose absorbed is generally higher than thatachieved by means of oral ingesti<strong>on</strong>. Various typesof sublingual dosage <strong>for</strong>ms are available in marketlike tablets, films and sprays.Vol. 3 (2) Apr – Jun2012 www.ijrpbs<strong>on</strong>line.com 919
Internati<strong>on</strong>al Journal of Research in Pharmaceutical and Biomedical Sciences ISSN: 2229-3701Table 1:Superdisintegrant Commercially available Mechanism0f acti<strong>on</strong>Cross linkedCelluloseCrosscarmellose®Ac-Di-Sol®,Nymce ZSX®Primellose®,Solutab®,Vivasol®, L-HPCCross linked PVP Crosspovid<strong>on</strong>e M®Kollid<strong>on</strong>®Polyplasd<strong>on</strong>e®Crosslinked starchCrosslinked alginicAcidExplotab®Primogel®Alginic acid NFSwells 4-8 foldsin < 10sec<strong>on</strong>ds.Swelling andwicking bothSwells very littleand returnsto original sizeaftercompressi<strong>on</strong> butact bycapillary acti<strong>on</strong>Swells 7-12 foldsin < 30sec<strong>on</strong>ds.Rapid swelling inaqueousmedium orwicking acti<strong>on</strong>Special commentSwells in twodimensi<strong>on</strong>s.Directcompressi<strong>on</strong>or Granulati<strong>on</strong>Starchfree.Waterinsoluble andsp<strong>on</strong>gy innature so getporous tabletSwells in threedimensi<strong>on</strong>sand highlevel serve assustain releasematrixPromotedisintegrati<strong>on</strong>in both dryor wetgranulati<strong>on</strong>.Table 2: Marketed Products of <strong>Sublingual</strong> TabletBrand Name Catergory SrengthAbstral Fentanyl Citrate Opioid <str<strong>on</strong>g>An</str<strong>on</strong>g>algesic50, 100, 200, 300, 400, 600,800 µgSubutex Buprenorphine Opioid <str<strong>on</strong>g>An</str<strong>on</strong>g>algesic 2 and 8mgAvitan Lorazepam <str<strong>on</strong>g>An</str<strong>on</strong>g>tianxiety 1, 2 mgEdular Zolpidem tartrate Sedatives/ Hypnotics 5, 10 mgIsordil Isosorbide dinitrate Vasodilators 2.5, 5 10mgSubox<strong>on</strong>e BuprenorphinehydrochlorideNarcotic + Opioid antag<strong>on</strong>ist 2/0.5, 8/2 mgNitrostat Nitroglycerine <str<strong>on</strong>g>An</str<strong>on</strong>g>tianginal 0.3 mg , 0.4 mg , or 0.6 mgFig. 1:Vol. 3 (2) Apr – Jun2012 www.ijrpbs<strong>on</strong>line.com 920
Internati<strong>on</strong>al Journal of Research in Pharmaceutical and Biomedical Sciences ISSN: 2229-3701Fig. 2: Diagram of sublingualgland and sublingual arteryFig. 3: Thin Film <strong>Drug</strong> <strong>Delivery</strong>REFERENCES1. Zhang H, Zhang J, Streisand JB. OralMucosal <strong>Drug</strong> <strong>Delivery</strong>: ClinicalPharmacokinetics and TherapeuticApplicati<strong>on</strong>s. Clin Pharmaco 2002:41(20):661-680.2. A Short Review <strong>on</strong> “A Novel Approach inOral Fast Dissolving <strong>Drug</strong> <strong>Delivery</strong>Vol. 3 (2) Apr – Jun2012 www.ijrpbs<strong>on</strong>line.com 921
Internati<strong>on</strong>al Journal of Research in Pharmaceutical and Biomedical Sciences ISSN: 2229-3701System and Their Patents”M.D. NehalSiddiqui, Garima Garg and PramodKumar Sharma, Advance in biologicalReaserch 5 (6): 291-203, 20113. <strong>Sublingual</strong> mucosa as a route <strong>for</strong> systemicdrug delivery,neha narang1*, jyotisharma, Internati<strong>on</strong>al Journal of Pharmacyand Pharmaceutical Sciences,Vol 3, Suppl2, 2011.4. Birudaraj R, Berner B, Shen S. Buccalpermeati<strong>on</strong> of buspir<strong>on</strong>e: Mechanisticstudies <strong>on</strong> transport pathways. J Pharm Sci2005; 94: 70-785. Ishikawa T, Koizumi N, Mukai B,Utoguchi N, Fujii M, Matsumoto M et al.,Pharmacokinetics of acetaminophen fromrapidly disintegrating compressed tabletprepared using microcrystalline cellulose(PH-M-06) and spherical sugar granules.Chem Pharm Bull (Tokyo) 2001; 49: 230-232.6. Price TM, Blauer KL, Hansen M,Stanczyk F, Lobo R, Bates GW. Singledosepharmacokinetics of sublingualversus oral administrati<strong>on</strong> of micr<strong>on</strong>ized17 beta-estradiol. Obstet Gynecol. 1997;89: 340-345.7. Kurosaki Y, Takatori T, Nishimura H,Nakayama T, Kimura T . Regi<strong>on</strong>alvariati<strong>on</strong> in oral mucosal drug absorpti<strong>on</strong>permeability and degree of keratinizati<strong>on</strong>in hamster oral cavity. Pharm Res 1991; 8:1297‐1301.8. Ghosh TK, Chatterjee DJ, Pfister WR.Quick dissolving oral dosage <strong>for</strong>ms:Scientific and regulatory c<strong>on</strong>siderati<strong>on</strong>sfrom a clinical pharmacology andbiopharmaceutical perspective. In: GhoshTK and Pfister WR (Eds). <strong>Drug</strong> <strong>Delivery</strong>to the Oral Cavity Molecules to Market.NY, USA: CRC Press, 2005: 337‐356.9. Richman MD, Fox D, Shangraw RF.Preparati<strong>on</strong> and stability of glyceryltrinitrate sublingual tablets prepared bydirect compressi<strong>on</strong>. J Pharm Sci 1965;54(3): 447‐451.10. Boer D et al. <strong>Drug</strong> absorpti<strong>on</strong> bysublingual and rectal routes. British J<str<strong>on</strong>g>An</str<strong>on</strong>g>aesthesia 1984; 56: 69‐82.11. Al‐Ghananeem AM, Malkawi AH, CrooksPA. Effect of pH <strong>on</strong> <strong>Sublingual</strong>Absorpti<strong>on</strong> of Oxycod<strong>on</strong>e Hydrochloride.AAPS PharmSciTech 2006; 7(1): Article23.12. Allen LV. Rapid-dissolve technology: aninterview with Loyd V.Allen. Int J PharmTechnol. 2003; 7: 449-450.13. Fu Y, Yang S, Je<strong>on</strong>g SH, Kimura S, ParkK. Orally fast disintegrating tablets:developments, technologies, taste-makingand clinical studies. Crit Rev Ther <strong>Drug</strong>Carrier Syst. 2004; 21: 433-476.14. European Directorate <strong>for</strong> quality ofMedicines. Pharmaeuropa. 1998; 10(4):547. http://www.pheur.org. Accessed 6February 2007.15. Sreenivas SA, Dandagi PM, Gadad AP,Godbloe AM, Hiremath SP,Mastiholimath VS. Orodispersible tablets:New-fangled drug delivery systems – Areview. Indian J Pharm Educ Res, 2005;39(4): 177-181.16. Seager H. <strong>Drug</strong>-delivery products andZydis Fastdissolving dosage <strong>for</strong>m. JPharm Pharmacol, 1998; 50: 375-382.17. Bradoo R, Shahani S, Deewan B,Sudarshan S. Fast dissolving drug deliverysystem. J Am Med Assoc India, 2001; 4(10): 27-31.18. Mizumoto T, Masuda Y, Takeshi Y, EstuoY, Katsuhide T. Formulati<strong>on</strong> design of anovel fastdisintegrating tablet. Int JPharm, 2005; 306(1- 2): 83–90.19. Deepak K. Orally disintegrating tablets.Tablets and Capsules, 2004; 7: 30-35.20. Brown D. Orally disintegrating tablets:Taste over speed. <strong>Drug</strong> Deliv Tech, 2001;3(6): 58-61.21. US Food and <strong>Drug</strong> Administrati<strong>on</strong>, CDERData Standards Manual. 2003.http://www.fda.gov/cder/dsm/DRG/drg00201.htm. Accessed 6February 2007.22. European Directorate <strong>for</strong> quality ofMedicines. Pharmaeuropa. 1998; 10(4):547. http://www.pheur.org. Accessed 6February 2007.23. Ghosh TK, Chatterjee DJ, Pfister WR.Quick dissolving oral dosage <strong>for</strong>ms:Scientific and regulatory c<strong>on</strong>siderati<strong>on</strong>sfrom a clinical pharmacology andbiopharmaceutical perspective. In: GhoshTK and Pfister WR (Eds). <strong>Drug</strong> <strong>Delivery</strong>to the Oral Cavity: Molecules to Market.NY, USA: CRC Press, 2005, pp 337-356.24. G. Sandri, M.C. B<strong>on</strong>fer<strong>on</strong>i, F. Ferrari, S.Rossi, C. Caramella, Differentiatingfactors between oral fast-dissolvingtechnologies, Am. J. <strong>Drug</strong> Deliv. 4 (4)(2006) 249–262.25. Mahesh A., Nalini shastri andMSdanandam,2010. Development films oftaste of Levocetrizine Dihydrochloride <strong>for</strong>oral use Current DRud <strong>Delivery</strong>, 7(1):21-2726. Cilurzo, F., I.E. Cup<strong>on</strong>e, P. Minghetti, F.Selmin, .L. M<strong>on</strong>tanari, 2008. Fastdissolving films made of maltodextrins.European J. Pharmaceutics andBiopharmaceutics. 70: 895-900.Vol. 3 (2) Apr – Jun2012 www.ijrpbs<strong>on</strong>line.com 922
Internati<strong>on</strong>al Journal of Research in Pharmaceutical and Biomedical Sciences ISSN: 2229-370127. Frey, 2006. Film Strips andPharmaceuticals.PharmaceuticalManufacturing and Packaging Sourcer,pp: 92-93.28. Lachman L, Liberman A and King JL.Tablets: The theory and practice ofindustrial pharmacy,(3rdediti<strong>on</strong>),Varghesepublishing house.1987:296-300.29. Sunada H, Y<strong>on</strong>ezawa Y, Danjo K, OtsukaA, Iida K.Preparati<strong>on</strong> and evaluati<strong>on</strong> of acompressed tablet rapidly disintegrating inthe oral cavity. Chem Pharm Bull(Tokyo)1996; 44: 2121‐212730. Edmund J. Preparati<strong>on</strong>, characterizati<strong>on</strong>and scale of ketoc<strong>on</strong>azole with enhanceddissoluti<strong>on</strong> and bioavailability. <strong>Drug</strong> DevInd Pharm 2007;33:755-765.31. Felt<strong>on</strong> L., P. O'D<strong>on</strong>nell and J. McGinity,Mechanical properties of polymeric filmsprepared from aqueous dispersi<strong>on</strong>s, in:Aqueous polymeric coatings <strong>for</strong>pharmaceutical dosage <strong>for</strong>m, 3rd editi<strong>on</strong>,J. McGinity, L.Felt<strong>on</strong>(Eds), Vol. 176,DRugs and the Pharmaceutical Sci,pp:108.32. Shinde, A.J., K.C. Garala and H.N. More,2008. Development and characterizati<strong>on</strong>of transdermal therapeutics system oftramadol hydrochloride, Asian J.Pharmaceutics. 4: 265-269.33. A Robert Neurath, Nathan Strick andYun-Yao Li. BMC Infectious Diseases2003; 3:27.34. Renuka Mishra, Avani Amin.Pharmaceutical Technology. Feb 2, 2009;33(2):48-56.35. Prashant M, satturwar S, Fulzele V andavinash K. dorle. AAPSPharmscitech.2005;6(4):48-53.Vol. 3 (2) Apr – Jun2012 www.ijrpbs<strong>on</strong>line.com 923













