Primary health care: now more than ever - World Health Organization
Primary health care: now more than ever - World Health Organization
Primary health care: now more than ever - World Health Organization

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
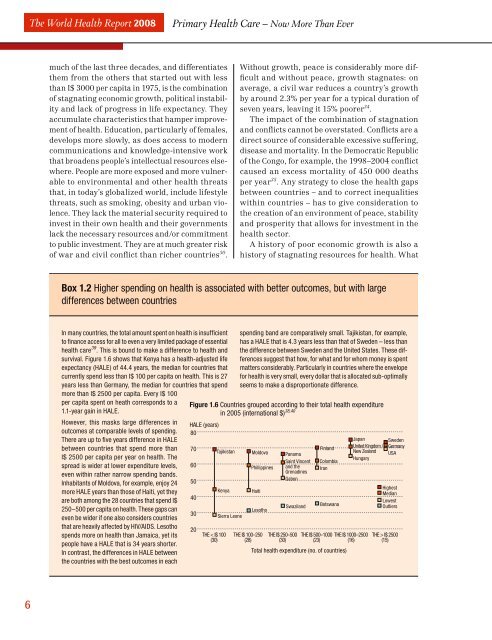
The <strong>World</strong> <strong>Health</strong> Report 2008<strong>Primary</strong> <strong>Health</strong> Care – Now More Than Evermuch of the last three decades, and differentiatesthem from the others that started out with less<strong>than</strong> I$ 3000 per capita in 1975, is the combinationof stagnating economic growth, political instabilityand lack of progress in life expectancy. Theyaccumulate characteristics that hamper improvementof <strong>health</strong>. Education, particularly of females,develops <strong>more</strong> slowly, as does access to moderncommunications and k<strong>now</strong>ledge-intensive workthat broadens people’s intellectual resources elsewhere.People are <strong>more</strong> exposed and <strong>more</strong> vulnerableto environmental and other <strong>health</strong> threatsthat, in today’s globalized world, include lifestylethreats, such as smoking, obesity and urban violence.They lack the material security required toinvest in their own <strong>health</strong> and their governmentslack the necessary resources and/or commitmentto public investment. They are at much greater riskof war and civil conflict <strong>than</strong> richer countries 30 .Without growth, peace is considerably <strong>more</strong> difficultand without peace, growth stagnates: onaverage, a civil war reduces a country’s growthby around 2.3% per year for a typical duration ofseven years, leaving it 15% poorer 34 .The impact of the combination of stagnationand conflicts cannot be overstated. Conflicts are adirect source of considerable excessive suffering,disease and mortality. In the Democratic Republicof the Congo, for example, the 1998–2004 conflictcaused an excess mortality of 450 000 deathsper year 35 . Any strategy to close the <strong>health</strong> gapsbetween countries – and to correct inequalitieswithin countries – has to give consideration tothe creation of an environment of peace, stabilityand prosperity that allows for investment in the<strong>health</strong> sector.A history of poor economic growth is also ahistory of stagnating resources for <strong>health</strong>. WhatBox 1.2 Higher spending on <strong>health</strong> is associated with better outcomes, but with largedifferences between countriesIn many countries, the total amount spent on <strong>health</strong> is insuffi cientto fi nance access for all to even a very limited package of essential<strong>health</strong> <strong>care</strong> 39 . This is bound to make a difference to <strong>health</strong> andsurvival. Figure 1.6 shows that Kenya has a <strong>health</strong>-adjusted lifeexpectancy (HALE) of 44.4 years, the median for countries thatcurrently spend less <strong>than</strong> I$ 100 per capita on <strong>health</strong>. This is 27years less <strong>than</strong> Germany, the median for countries that spend<strong>more</strong> <strong>than</strong> I$ 2500 per capita. Every I$ 100per capita spent on heath corresponds to a1.1-year gain in HALE.How<strong>ever</strong>, this masks large differences inoutcomes at comparable levels of spending.There are up to fi ve years difference in HALEbetween countries that spend <strong>more</strong> <strong>than</strong>I$ 2500 per capita per year on <strong>health</strong>. Thespread is wider at lower expenditure levels,even within rather narrow spending bands.Inhabitants of Moldova, for example, enjoy 24<strong>more</strong> HALE years <strong>than</strong> those of Haiti, yet theyare both among the 28 countries that spend I$250–500 per capita on <strong>health</strong>. These gaps caneven be wider if one also considers countriesthat are heavily affected by HIV/AIDS. Lesothospends <strong>more</strong> on <strong>health</strong> <strong>than</strong> Jamaica, yet itspeople have a HALE that is 34 years shorter.In contrast, the differences in HALE betweenthe countries with the best outcomes in eachspending band are comparatively small. Tajikistan, for example,has a HALE that is 4.3 years less <strong>than</strong> that of Sweden – less <strong>than</strong>the difference between Sweden and the United States. These differencessuggest that how, for what and for whom money is spentmatters considerably. Particularly in countries where the envelopefor <strong>health</strong> is very small, <strong>ever</strong>y dollar that is allocated sub-optimallyseems to make a disproportionate difference.Figure 1.6 Countries grouped according to their total <strong>health</strong> expenditurein 2005 (international $) 38,40HALE (years)80706050403020TajikistanKenyaTHE < I$ 100(30)Sierra LeoneMoldovaPhillippinesHaitiLesothoTHE I$ 100–250(28)PanamaSaint Vincentand theGrenadinesGabonSwazilandTHE I$ 250–500(30)FinlandColombiaIranBotswanaTHE I$ 500–1000(23)Total <strong>health</strong> expenditure (no. of countries)Japan SwedenUnited Kingdom / GermanyNew Zealand USAHungaryTHE I$ 1000–2500(16)HighestMedianLowestOutliersTHE > I$ 2500(15)6