PROTOCOLS
New Front Cover.indd - pgpic.com
New Front Cover.indd - pgpic.com

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
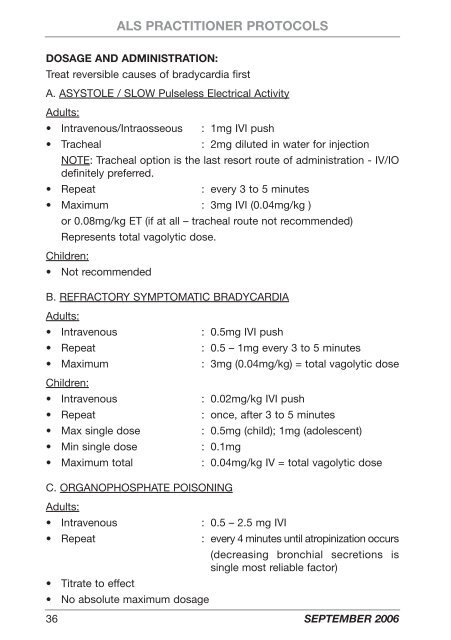
ALS PRACTITIONER <strong>PROTOCOLS</strong>DOSAGE AND ADMINISTRATION:Treat reversible causes of bradycardia firstA. ASYSTOLE / SLOW Pulseless Electrical ActivityAdults:• Intravenous/Intraosseous : 1mg IVI push• Tracheal: 2mg diluted in water for injectionNOTE: Tracheal option is the last resort route of administration - IV/IOdefinitely preferred.• Repeat: every 3 to 5 minutes• Maximum : 3mg IVI (0.04mg/kg )or 0.08mg/kg ET (if at all – tracheal route not recommended)Represents total vagolytic dose.Children:• Not recommendedB. REFRACTORY SYMPTOMATIC BRADYCARDIAAdults:• Intravenous• Repeat• MaximumChildren:• Intravenous• Repeat• Max single dose• Min single dose• Maximum total: 0.5mg IVI push: 0.5 – 1mg every 3 to 5 minutes: 3mg (0.04mg/kg) = total vagolytic dose: 0.02mg/kg IVI push: once, after 3 to 5 minutes: 0.5mg (child); 1mg (adolescent): 0.1mg: 0.04mg/kg IV = total vagolytic doseC. ORGANOPHOSPHATE POISONINGAdults:• Intravenous: 0.5 – 2.5 mg IVI• Repeat: every 4 minutes until atropinization occurs(decreasing bronchial secretions issingle most reliable factor)• Titrate to effect• No absolute maximum dosage36 SEPTEMBER 2006