Human Resources Employee Information Form
Employee Information Form Human Resources
Employee Information Form Human Resources
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
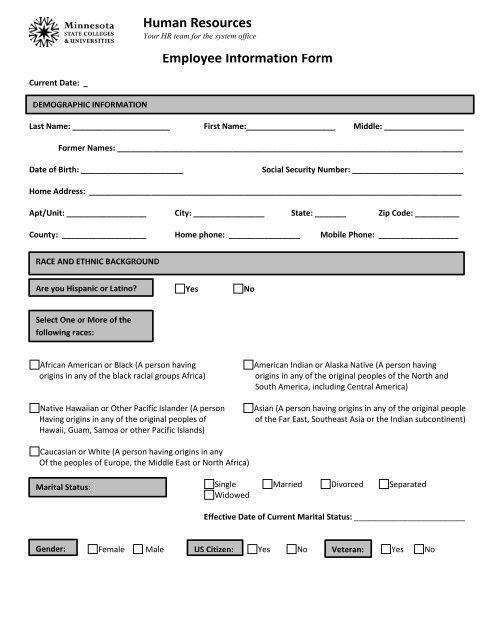
<strong>Human</strong> <strong>Resources</strong><br />
Your HR team for the system office<br />
<strong>Employee</strong> <strong>Information</strong> <strong>Form</strong><br />
Current Date: _<br />
DEMOGRAPHIC INFORMATION<br />
Last Name: ______________________ First Name:____________________ Middle: __________________<br />
<strong>Form</strong>er Names: ______________________________________________________________________________<br />
Date of Birth: _______________________<br />
Social Security Number: _________________________<br />
Home Address: ____________________________________________________________________________________<br />
Apt/Unit: __________________ City: ________________ State: _______ Zip Code: __________<br />
County: ___________________ Home phone: ________________ Mobile Phone: __________________<br />
RACE AND ETHNIC BACKGROUND<br />
Are you Hispanic or Latino?<br />
Yes<br />
No<br />
Select One or More of the<br />
following races:<br />
African American or Black (A person having<br />
origins in any of the black racial groups Africa)<br />
Native Hawaiian or Other Pacific Islander (A person<br />
Having origins in any of the original peoples of<br />
Hawaii, Guam, Samoa or other Pacific Islands)<br />
American Indian or Alaska Native (A person having<br />
origins in any of the original peoples of the North and<br />
South America, including Central America)<br />
Asian (A person having origins in any of the original people<br />
of the Far East, Southeast Asia or the Indian subcontinent)<br />
Caucasian or White (A person having origins in any<br />
Of the peoples of Europe, the Middle East or North Africa)<br />
Marital Status:<br />
Single Married Divorced Separated<br />
Widowed<br />
Effective Date of Current Marital Status: _________________________<br />
Gender: Female Male US Citizen: Yes No Veteran: Yes No
Disability Status: Yes No If yes, please provide a brief description<br />
A disability may be defined as:<br />
a) having a physical and/or mental impairment<br />
Which substantially limits one or more major<br />
Life activities;<br />
b) having a record of such impairment; or<br />
c) being regarded as having such an impairment.<br />
“Major life activities” means functions such as caring for one’s<br />
self, performing manual tasks, walking, seeing, hearing, speaking,<br />
breathing, learning and working.<br />
ADDITIONAL EMPLOYMENT INFORMATION<br />
Have you previously been employed by the State of Minnesota? Yes No<br />
If yes, please indicate which agency or agencies and dates of employment:<br />
If you were previously employed by the State of Minnesota, which retirement plan were you in? (i.e. MSRS, TRA, etc.)<br />
Educational Background (Report all earned degrees and provide copies of official transcript for each.)<br />
Institution #1:__________________ Institution #2: __________________ Institution #3: ___________________<br />
City & State: __________________ City & State: __________________ City & State: ___________________<br />
Degree: __________________ Degree: __________________ Degree: ___________________<br />
Date Rec’d: __________________ Date Rec’d: __________________ Date Rec’d: ___________________<br />
Emergency Contact <strong>Information</strong>:<br />
Name (1): ______________________________ Name (2): _______________________________<br />
Address: ______________________________ Address: _______________________________<br />
State/Province: ______________________________<br />
State Province: _______________________________<br />
Zip Code: ______________________________ Zip Code: _______________________________<br />
Home Phone: ______________________________ Home Phone: _______________________________<br />
Relationship: ______________________________ Relationship: _______________________________<br />
I hereby declare that the information provided on this form is true and accurate to the best of my knowledge.<br />
<strong>Employee</strong> Signature<br />
_________________________________________________