

Treatment Alternatives in Charcot Arthropathy of the Foot
Bom2Sv
Bom2Sv

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
December 2015<br />
10<br />
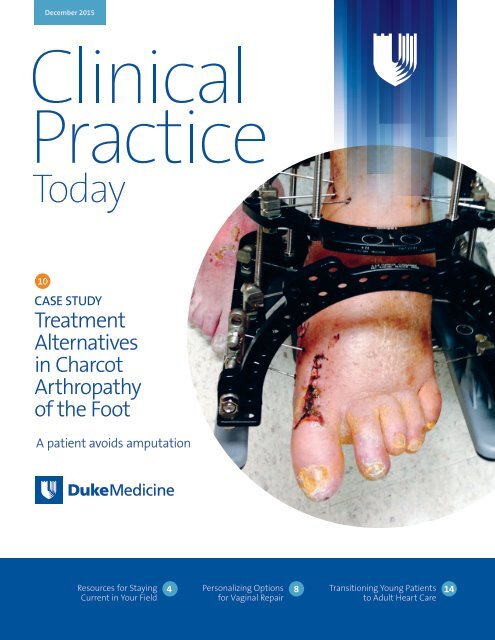
CASE STUDY<br />
<strong>Treatment</strong><br />
<strong>Alternatives</strong><br />
<strong>in</strong> <strong>Charcot</strong><br />
<strong>Arthropathy</strong><br />
<strong>of</strong> <strong>the</strong> <strong>Foot</strong><br />
A patient avoids amputation<br />
Resources for Stay<strong>in</strong>g<br />
Current <strong>in</strong> Your Field 4<br />
Personaliz<strong>in</strong>g Options<br />
for Vag<strong>in</strong>al Repair<br />
8<br />
Transition<strong>in</strong>g Young Patients<br />
to Adult Heart Care 14
Cl<strong>in</strong>ical Practice Today<br />
Duke Medic<strong>in</strong>e Market<strong>in</strong>g<br />
and Communications<br />
Editor<br />
Mary Jane Gore, MA<br />
Publisher<br />
Med-IQ<br />
Editorial Management<br />
Laura Rafferty<br />
Lisa R. R<strong>in</strong>ehart, MS, ELS<br />
Sherri Damlo<br />
Writers<br />
Karen Appold<br />
Frank Celia<br />
Meredith Lidard Kleeman<br />
Emily Paulsen<br />
Tim Pittman<br />
Shelly K. Schwartz<br />
About Duke Medic<strong>in</strong>e<br />
U.S. News & World Report consistently<br />
ranks Duke University Hospital <strong>in</strong><br />
its Honor Roll <strong>of</strong> top hospitals <strong>in</strong> <strong>the</strong><br />
United States.<br />
We strive to transform medic<strong>in</strong>e and<br />
health locally and globally through<br />
<strong>in</strong>novative scientific research, rapid<br />
translation <strong>of</strong> breakthrough discoveries,<br />
educat<strong>in</strong>g future cl<strong>in</strong>ical and scientific<br />
leaders, advocat<strong>in</strong>g and practic<strong>in</strong>g<br />
evidence-based medic<strong>in</strong>e to improve<br />
community health, and lead<strong>in</strong>g efforts<br />
to elim<strong>in</strong>ate health <strong>in</strong>equalities.<br />
To refer patients, call 844-790-2013.<br />
For more details on <strong>the</strong> services we<br />
<strong>of</strong>fer your patients, please visit<br />
DukeMedic<strong>in</strong>e.org.<br />
Duke University Hospital, Durham, NC<br />
Duke Regional Hospital, Durham, NC<br />
Duke Raleigh Hospital, Raleigh, NC<br />
Duke University, 3100 Tower Blvd., Suite 1008<br />
Durham, NC 27707-2575<br />
Materials may not be repr<strong>in</strong>ted without<br />
written consent from <strong>the</strong> publisher.<br />
If you wish to be removed from <strong>the</strong> mail<strong>in</strong>g<br />
list, please email <strong>in</strong>fo@med-iq.com or<br />
call 866-858-7434.<br />
©2015 Duke Medic<strong>in</strong>e. All rights reserved.<br />
<strong>in</strong> Cl<strong>in</strong>ical Practice Today<br />
4<br />
6<br />
7<br />
8<br />
9<br />
10<br />
12<br />
13<br />
14<br />
Resources for Stay<strong>in</strong>g Current <strong>in</strong> Your Field<br />
Review updates <strong>in</strong> your cl<strong>in</strong>ical area with <strong>the</strong>se easy tools<br />
Pediatric Bra<strong>in</strong> Tumor Surgery<br />
The most common types <strong>of</strong> pediatric tumors are those<br />
<strong>in</strong> <strong>the</strong> posterior fossa, such as gliomas, medulloblastomas,<br />
and ependymomas<br />
Four Strategies for Manag<strong>in</strong>g Patients<br />
Who Refuse Vacc<strong>in</strong>ations<br />
Consider follow<strong>in</strong>g <strong>the</strong>se approaches to encourage patients<br />
to vacc<strong>in</strong>ate <strong>the</strong>mselves and <strong>the</strong>ir children<br />
Personaliz<strong>in</strong>g Options for Vag<strong>in</strong>al Repair<br />
Prolapse can be surgically corrected with vag<strong>in</strong>al, m<strong>in</strong>imally<br />
<strong>in</strong>vasive, or abdom<strong>in</strong>al surgery<br />
Safeguard<strong>in</strong>g Medical Identities<br />
Keep your practice and your patients safe by implement<strong>in</strong>g<br />
a few basic precautions<br />
CASE STUDY<br />
<strong>Treatment</strong> <strong>Alternatives</strong> <strong>in</strong> <strong>Charcot</strong> <strong>Arthropathy</strong><br />
<strong>of</strong> <strong>the</strong> <strong>Foot</strong><br />
A patient avoids amputation<br />
Essential Tech Functions for Office-Based Doctors<br />
Th<strong>in</strong>k beyond electronic health records by us<strong>in</strong>g products<br />
that help fulfill <strong>the</strong> Triple Aim<br />
Lower<strong>in</strong>g HbA1C <strong>in</strong> a Patient With O<strong>the</strong>r<br />
Health Challenges<br />
Cl<strong>in</strong>icians should consider barriers to health care and<br />
psychosocial factors when manag<strong>in</strong>g patients with<br />
complex needs<br />
Transition<strong>in</strong>g Young Patients to Adult Heart Care<br />
Speak with pediatric patients with congenital heart disease<br />
even before <strong>the</strong>y enter <strong>the</strong>ir teens<br />
To learn more or<br />
to refer a patient,<br />
call 844-790-2013
News Briefs<br />
Life-Chang<strong>in</strong>g Dialysis<br />
Graft Reduces Patient<br />
Pa<strong>in</strong>, Saves Costs<br />
A life-chang<strong>in</strong>g arteriovenous graft developed at<br />
Duke could prevent pa<strong>in</strong> and bruis<strong>in</strong>g for dialysis<br />
patients and help prevent complications responsible<br />
for millions <strong>of</strong> dollars <strong>in</strong> annual health care costs.<br />
The device is progress<strong>in</strong>g toward commercial use.<br />
The Bullet Pro<strong>of</strong> graft <strong>in</strong>cludes 2 penetrationresistant<br />
chambers that prevent needles from<br />
damag<strong>in</strong>g <strong>the</strong> s<strong>of</strong>t tub<strong>in</strong>g used <strong>in</strong> dialysis.<br />
Standard dialysis grafts ensure a strong blood<br />
flow through <strong>the</strong> hollow tube or conduit, but<br />
dur<strong>in</strong>g dialysis, <strong>the</strong>y are vulnerable to needle<br />
pokes that accidentally push through both sides<br />
<strong>of</strong> <strong>the</strong> graft. These <strong>in</strong>advertent pokes create<br />
pa<strong>in</strong>ful <strong>in</strong>juries that can be expensive to repair.<br />
With support from Duke’s cl<strong>in</strong>ical translational<br />
fund<strong>in</strong>g programs, a team <strong>of</strong> researchers plans to<br />
release <strong>the</strong> medical device with<strong>in</strong> 1 year.<br />
ICDs Underused<br />
Among Older Patients<br />
After Heart Attack<br />
Research from Duke’s Sean D. Pokorney, MD, MBA,<br />
published <strong>in</strong> <strong>the</strong> June 23-30, 2015, JAMA issue,<br />
reported data regard<strong>in</strong>g concerns about <strong>the</strong> underuse<br />
<strong>of</strong> implantable cardioverter-defibrillators (ICDs) <strong>in</strong><br />
older patients who experienced a heart attack.<br />
Accord<strong>in</strong>g to <strong>the</strong> f<strong>in</strong>d<strong>in</strong>gs, among Medicare<br />
patients who experienced a heart attack from<br />
2007 to 2010, fewer than 1 <strong>in</strong> 10 eligible patients<br />
with low ejection fraction (a measure <strong>of</strong> how well<br />
<strong>the</strong> left ventricle <strong>of</strong> <strong>the</strong> heart pumps blood with<br />
each beat) received an ICD with<strong>in</strong> 1 year after <strong>the</strong><br />
heart attack, even though ICD implantation was<br />
associated with a lower risk <strong>of</strong> death at 2 years after<br />
<strong>the</strong> heart attack. (X-ray above shows an ICD.)<br />
Modified Poliovirus<br />
Be<strong>in</strong>g Tested Aga<strong>in</strong>st<br />
Incurable Prostate Cancer<br />
Duke’s success <strong>in</strong> early cl<strong>in</strong>ical trials us<strong>in</strong>g modified<br />
poliovirus to treat a deadly form <strong>of</strong> bra<strong>in</strong> cancer may<br />
lead to new applications for <strong>the</strong> virus <strong>in</strong> <strong>the</strong> battle<br />
aga<strong>in</strong>st <strong>in</strong>curable metastatic prostate cancer.<br />
An <strong>in</strong>terdiscipl<strong>in</strong>ary team applied <strong>the</strong> new <strong>the</strong>rapy,<br />
known as PVSRIPO, to late-stage prostate cancer.<br />
PVSRIPO has been modified and managed with <strong>the</strong><br />
addition <strong>of</strong> rh<strong>in</strong>ovirus. The eng<strong>in</strong>eered virus specifically<br />
targets and destroys tumor cells while leav<strong>in</strong>g<br />
healthy cells unsca<strong>the</strong>d. Animal test<strong>in</strong>g is underway<br />
<strong>in</strong> mice. Smita Nair, PhD, a pr<strong>in</strong>cipal <strong>in</strong>vestigator and<br />
cancer immuno<strong>the</strong>rapy researcher <strong>in</strong> Duke’s Surgery<br />
Department, is work<strong>in</strong>g to apply <strong>the</strong> modified virus<br />
to non–central nervous system challenges.<br />
Daniel J. George, MD, a medical oncologist, says<br />
physicians are focused on f<strong>in</strong>d<strong>in</strong>g new <strong>the</strong>rapies<br />
that can extend lives and attack prostate cancer.<br />
December 2015<br />
Cl<strong>in</strong>icalPracticeToday.com<br />
3
Resources for<br />
Stay<strong>in</strong>g Current<br />
<strong>in</strong> Your Field<br />
By Shelly K. Schwartz<br />
Review updates <strong>in</strong> your cl<strong>in</strong>ical area with <strong>the</strong>se easy tools<br />
It began like any o<strong>the</strong>r journal club meet<strong>in</strong>g.<br />
Anes<strong>the</strong>siology residents were ga<strong>the</strong>red <strong>in</strong> a<br />
Duke University School <strong>of</strong> Medic<strong>in</strong>e classroom<br />
to review <strong>the</strong> latest medical literature from <strong>the</strong>ir<br />
specialty—evidence-based research that might<br />
move <strong>the</strong> needle on treatment protocols and<br />
patient outcomes. As <strong>the</strong> discussion on aspir<strong>in</strong> use<br />
<strong>in</strong> patients undergo<strong>in</strong>g noncardiac surgery got<br />
underway, moderator Ankeet Udani, MD, began<br />
read<strong>in</strong>g aloud comments from thought leaders<br />
across <strong>the</strong> globe who had weighed <strong>in</strong> remotely via<br />
Twitter. Sporadically, he also read relevant tweets<br />
from cl<strong>in</strong>icians outside <strong>of</strong> <strong>the</strong> Duke University<br />
system who were participat<strong>in</strong>g <strong>in</strong> real time. “We<br />
were look<strong>in</strong>g for a way to augment <strong>the</strong> current<br />
classroom format us<strong>in</strong>g social media and realized<br />
that most medical students and residents are already<br />
us<strong>in</strong>g Twitter,” says Udani, an assistant pr<strong>of</strong>essor<br />
<strong>of</strong> anes<strong>the</strong>siology and co-creator <strong>of</strong> <strong>the</strong> Duke<br />
Anes<strong>the</strong>siology Twitter Journal Club with colleague<br />
Jeff Taekman, MD. “We wanted to provide a broad<br />
perspective for our residents <strong>of</strong> what people are<br />
do<strong>in</strong>g <strong>in</strong> our field around <strong>the</strong> world.”<br />
Topics for <strong>the</strong> quarterly journal club, drawn from<br />
recent studies and journal articles, get posted to<br />
Twitter 1 week before <strong>the</strong> <strong>in</strong>-person meet<strong>in</strong>gs,<br />
Udani expla<strong>in</strong>s, <strong>in</strong>vit<strong>in</strong>g cl<strong>in</strong>icians, academics, and<br />
experts to contribute. The <strong>in</strong>put <strong>the</strong>y provide and<br />
<strong>the</strong> onl<strong>in</strong>e comments sent <strong>in</strong> dur<strong>in</strong>g classroom<br />
discussions are later organized and posted onl<strong>in</strong>e,<br />
which sets <strong>the</strong> Duke Anes<strong>the</strong>siology Twitter<br />
Journal Club apart. “Ours is not <strong>the</strong> first onl<strong>in</strong>e<br />
journal club, but we are unique because we<br />
moderate <strong>the</strong> onl<strong>in</strong>e Twitter feed and curate <strong>the</strong><br />
entire discussion to create an everlast<strong>in</strong>g resource<br />
for all anes<strong>the</strong>siologists,” says Udani.<br />
Social media is among <strong>the</strong> many tools that<br />
cl<strong>in</strong>icians are us<strong>in</strong>g to keep current <strong>in</strong> <strong>the</strong>ir field,<br />
a matter <strong>of</strong> critical importance to patient safety<br />
and <strong>the</strong> quality <strong>of</strong> care. In a 2014 survey by onl<strong>in</strong>e<br />
medical network Doximity, 98% <strong>of</strong> physicians<br />
reported that read<strong>in</strong>g medical literature was ei<strong>the</strong>r<br />
“important” or “very important” to <strong>the</strong>ir practice,<br />
and 16% believed that stay<strong>in</strong>g current directly<br />
helped save <strong>the</strong> life <strong>of</strong> a patient <strong>in</strong> <strong>the</strong> last year.<br />
But read<strong>in</strong>g every published article is nei<strong>the</strong>r practical<br />
nor possible. Moreover, not all are relevant<br />
to every specialty; <strong>in</strong> addition, some lack scientific<br />
validity and still o<strong>the</strong>rs are ta<strong>in</strong>ted by bias. To<br />
keep <strong>the</strong>ir knowledge base fresh, physicians must<br />
become adept at separat<strong>in</strong>g <strong>the</strong> wheat from<br />
4 Cl<strong>in</strong>ical Practice Today from Duke Medic<strong>in</strong>e
<strong>the</strong> chaff or rely on resources that vet scientific<br />
literature on <strong>the</strong>ir behalf.<br />
Pr<strong>of</strong>essional Groups<br />
A good start<strong>in</strong>g po<strong>in</strong>t is <strong>the</strong> medical guidel<strong>in</strong>es<br />
from reputable pr<strong>of</strong>essional organizations, which<br />
provide cl<strong>in</strong>ical recommendations regard<strong>in</strong>g<br />
<strong>the</strong> diagnosis, management, and treatment <strong>of</strong><br />
diseases, says Bernard Sklar, MD, a family physician<br />
and Webmaster for CMElist.com. “Most doctors<br />
are guided by <strong>the</strong>ir pr<strong>of</strong>essional organizations, each<br />
<strong>of</strong> which have <strong>the</strong>ir own set <strong>of</strong> competencies that<br />
<strong>the</strong>y th<strong>in</strong>k doctors need to be updated on,” he says.<br />
RSS Feeds<br />
Most pr<strong>of</strong>essional organizations also <strong>of</strong>fer a<br />
subscription-based RSS feed, enabl<strong>in</strong>g cl<strong>in</strong>icians to<br />
automatically download relevant articles to <strong>the</strong>ir<br />
computers. Many peer-reviewed medical journals<br />
<strong>of</strong>fer <strong>the</strong> same service, <strong>in</strong>clud<strong>in</strong>g <strong>the</strong> British<br />
Medical Journal. RSS feeds appear as a series <strong>of</strong><br />
headl<strong>in</strong>es and summaries, enabl<strong>in</strong>g doctors to<br />
quickly locate content that matters to <strong>the</strong>m.<br />
Review Organizations<br />
To answer specific cl<strong>in</strong>ical questions related to<br />
patient care, <strong>the</strong> American College <strong>of</strong> Physicians<br />
suggests that doctors beg<strong>in</strong> <strong>the</strong>ir literature<br />
search with a resource such as PubMed, a free<br />
onl<strong>in</strong>e search eng<strong>in</strong>e from <strong>the</strong> US National Library<br />
<strong>of</strong> Medic<strong>in</strong>e that acts as a database for <strong>the</strong><br />
most important abstracts and journal citations<br />
published <strong>in</strong> MEDLINE. The PubMed search tool<br />
allows users to create filters that help weed out<br />
irrelevant content. For example, <strong>the</strong> systematicreviews<br />
filter displays citations for systematic<br />
reviews, meta-analyses, reviews <strong>of</strong> cl<strong>in</strong>ical trials,<br />
guidel<strong>in</strong>es, and o<strong>the</strong>r reviews.<br />
Mobile Health<br />
Mobile apps also help br<strong>in</strong>g <strong>the</strong> current body <strong>of</strong><br />
medical knowledge <strong>in</strong>to <strong>the</strong> exam<strong>in</strong>ation room.<br />
Two <strong>of</strong> <strong>the</strong> most widely used apps are DynaMed<br />
and UpToDate®—evidence-based, cl<strong>in</strong>ical decisionsupport<br />
resources that <strong>in</strong>tegrate f<strong>in</strong>d<strong>in</strong>gs from<br />
research studies. Docph<strong>in</strong> and Read by QxMD<br />
also provide access to medical literature from a<br />
wide range <strong>of</strong> journals. In addition, groups like<br />
Cochrane Library <strong>of</strong>fer a collection <strong>of</strong> high-quality,<br />
<strong>in</strong>dependent evidence to <strong>in</strong>form health care<br />
decision mak<strong>in</strong>g. Many medical organizations<br />
enable specialists to download cl<strong>in</strong>ical guidel<strong>in</strong>es,<br />
white papers, and best-practice statements to<br />
<strong>the</strong>ir personal devices.<br />
Modern Medic<strong>in</strong>e<br />
Facebook, Twitter, and Google+ <strong>of</strong>fer yet ano<strong>the</strong>r<br />
platform for keep<strong>in</strong>g current, as sites like Cochrane<br />
Library become active on social media. Blogs,<br />
<strong>in</strong>clud<strong>in</strong>g those from PLoS One, can also shed new<br />
light on evidence-based <strong>the</strong>rapies. In addition,<br />
audio podcasts from <strong>in</strong>fluential medical journals<br />
and medical schools, <strong>in</strong>clud<strong>in</strong>g <strong>the</strong> New England<br />
Journal <strong>of</strong> Medic<strong>in</strong>e and Johns Hopk<strong>in</strong>s Medic<strong>in</strong>e,<br />
can help keep practic<strong>in</strong>g physicians <strong>in</strong>formed<br />
about current medical news while deliver<strong>in</strong>g <strong>the</strong><br />
added benefit <strong>of</strong> expert op<strong>in</strong>ion.<br />
Whatever tools physicians use to help keep pace<br />
with <strong>in</strong>novation, <strong>the</strong>y must always evaluate <strong>the</strong><br />
literature with a critical eye, says Brian Alper, MD,<br />
MSPH, a family physician and founder <strong>of</strong> DynaMed.<br />
Threats to validity abound—some due to bias<br />
and some due to error. “It’s complicated how<br />
many different factors can bias our science,” says<br />
Alper. “You have to look at <strong>the</strong> details <strong>of</strong> how <strong>the</strong><br />
research came toge<strong>the</strong>r.”<br />
The best resources are timely, trusted, and<br />
capable <strong>of</strong> condens<strong>in</strong>g <strong>the</strong> complete body <strong>of</strong><br />
medical literature <strong>in</strong>to summaries that are useful<br />
to physicians at <strong>the</strong> po<strong>in</strong>t <strong>of</strong> care. “Health care<br />
pr<strong>of</strong>essionals need <strong>the</strong> best <strong>in</strong>formation available<br />
to help guide <strong>the</strong>ir practice, and <strong>the</strong> <strong>in</strong>formation<br />
keeps chang<strong>in</strong>g,” says Alper.<br />
December 2015<br />
Cl<strong>in</strong>icalPracticeToday.com<br />
5
Pediatric Bra<strong>in</strong><br />
Tumor Surgery<br />
Although pediatric neurosurgeons assess and<br />
treat a wider variety <strong>of</strong> conditions than <strong>the</strong>ir<br />
colleagues who treat adult patients, specialized<br />
centers for pediatric tumors and sp<strong>in</strong>e conditions<br />
<strong>of</strong>fer specific programs for some patients.<br />
Eric Thompson, MD, a Duke pediatric neurosurgeon<br />
and tumor specialist, leads <strong>the</strong> Duke<br />
University Medical Center multidiscipl<strong>in</strong>ary<br />
pediatric bra<strong>in</strong> tumor board composed <strong>of</strong><br />
neurosurgeons, neuro-oncologists, radiation<br />
oncologists, neuroradiologists, neuropathologists,<br />
and tra<strong>in</strong>ees from those fields. The board<br />
discusses cases and reaches a consensus on treatment<br />
plans for <strong>the</strong> most challeng<strong>in</strong>g tumor cases.<br />
The most common types <strong>of</strong> tumors treated <strong>in</strong><br />
children are those <strong>in</strong> <strong>the</strong> posterior fossa, <strong>in</strong>clud<strong>in</strong>g<br />
gliomas, medulloblastomas, and ependymomas.<br />
Metastases, although fairly rare, occur <strong>in</strong> up to 5%<br />
<strong>of</strong> children with solid tumors.<br />
Larger centers <strong>of</strong>ten <strong>of</strong>fer <strong>the</strong> advantage <strong>of</strong><br />
cutt<strong>in</strong>g-edge technology as well as cl<strong>in</strong>ical expertise.<br />
Intraoperative magnetic resonance imag<strong>in</strong>g<br />
(MRI) is frequently used at Duke to facilitate <strong>the</strong><br />
maximal safe removal <strong>of</strong> bra<strong>in</strong> tumors. Ano<strong>the</strong>r<br />
significant advantage is <strong>the</strong> ability to enroll<br />
children <strong>in</strong> cl<strong>in</strong>ical trials, especially patients whose<br />
cancer has progressed. Duke is a member <strong>of</strong> both<br />
<strong>the</strong> Pediatric Bra<strong>in</strong> Tumor Consortium and <strong>the</strong><br />
Children’s Oncology Group.<br />
When to Refer<br />
Parents most commonly ask pediatric neurosurgeons<br />
<strong>the</strong> follow<strong>in</strong>g 2 questions:<br />
• Is <strong>the</strong> child’s head an abnormal shape?<br />
• Is <strong>the</strong> child’s head too large?<br />
The answers to <strong>the</strong>se questions suggest when<br />
referral to specialists might be prudent. If a child’s<br />
head is flat <strong>in</strong> <strong>the</strong> back and <strong>the</strong> head is clearly not<br />
gett<strong>in</strong>g rounder after several months <strong>of</strong> prohibit<strong>in</strong>g<br />
<strong>the</strong> child from lay<strong>in</strong>g on his or her back, <strong>the</strong>n<br />
it is time to refer to a pediatric neurosurgeon.<br />
Regard<strong>in</strong>g head size, <strong>the</strong>re is usually not cause for<br />
alarm unless <strong>the</strong> head has begun to grow at an<br />
accelerated rate. “If a child’s skull size is cross<strong>in</strong>g<br />
multiple percentiles, that would be a good time to<br />
refer,” Thompson says.<br />
Duke welcomes <strong>the</strong> opportunity to work closely with<br />
community physicians to treat pediatric patients with<br />
bra<strong>in</strong> and sp<strong>in</strong>e tumors, craniosynostosis, vascular<br />
disease, epilepsy, sp<strong>in</strong>a bifida, hydrocephalus, and<br />
spasticity. To learn more or to refer, call 844-790-2013.<br />
(T2-weighted MRI reveals a medulloblastoma.)<br />
6 Cl<strong>in</strong>ical Practice Today from Duke Medic<strong>in</strong>e
Four Strategies for Manag<strong>in</strong>g<br />
Patients Who Refuse Vacc<strong>in</strong>ations<br />
By Meredith Lidard Kleeman<br />
Thanks to immunizations, <strong>the</strong> United States has very low rates <strong>of</strong> vacc<strong>in</strong>e-preventable diseases such as<br />
measles, mumps, and polio, accord<strong>in</strong>g to <strong>the</strong> Centers for Disease Control and Prevention (CDC). Yet, despite<br />
<strong>the</strong> success rates <strong>of</strong> immunizations, some patients refuse to vacc<strong>in</strong>ate <strong>the</strong>mselves and <strong>the</strong>ir children.<br />
Understand<strong>in</strong>g your patients’ objections is <strong>the</strong> first step <strong>in</strong> try<strong>in</strong>g to encourage <strong>the</strong>m to get vacc<strong>in</strong>ated, says<br />
Robert Werg<strong>in</strong>, MD, board chair <strong>of</strong> <strong>the</strong> American Academy <strong>of</strong> Family Physicians. Werg<strong>in</strong> shares his strategies<br />
for respond<strong>in</strong>g to common patient concerns.<br />
1<br />
Emphasize safety. Many <strong>of</strong> <strong>the</strong> patients <strong>in</strong><br />
his practice are concerned about vacc<strong>in</strong>e<br />
safety, Werg<strong>in</strong> says. They may have heard<br />
about <strong>the</strong> <strong>in</strong>famous article l<strong>in</strong>k<strong>in</strong>g autism<br />
to <strong>the</strong> measles, mumps, and rubella (MMR)<br />
vacc<strong>in</strong>e. Physicians can address this concern by<br />
<strong>in</strong>form<strong>in</strong>g patients that <strong>the</strong>re is clear pro<strong>of</strong> that<br />
<strong>the</strong> MMR vacc<strong>in</strong>e does not cause autism and<br />
lett<strong>in</strong>g <strong>the</strong>m know that <strong>the</strong> antivacc<strong>in</strong>e study<br />
has s<strong>in</strong>ce been discredited. Werg<strong>in</strong> also advises<br />
physicians to expla<strong>in</strong> that, although vacc<strong>in</strong>es are<br />
associated with some risks, <strong>the</strong>y are extremely<br />
low. He tells his patients that <strong>the</strong> risks are about<br />
<strong>the</strong> same as be<strong>in</strong>g struck by lightn<strong>in</strong>g.<br />
Expla<strong>in</strong> herd immunity. Most people,<br />
2 <strong>in</strong>clud<strong>in</strong>g many medical pr<strong>of</strong>essionals, have<br />
never experienced polio, measles, or mumps<br />
firsthand. This lack <strong>of</strong> first-hand knowledge can<br />
make patients believe that <strong>the</strong>se diseases are no<br />
longer a threat. Rem<strong>in</strong>d patients that because<br />
<strong>of</strong> herd immunity, as long as everyone around<br />
<strong>the</strong>m cont<strong>in</strong>ues to get vacc<strong>in</strong>ated, <strong>the</strong> threat <strong>of</strong><br />
contract<strong>in</strong>g those diseases rema<strong>in</strong>s low; however,<br />
if enough members <strong>of</strong> a community do not get<br />
immunized, those diseases could reemerge.<br />
3<br />
Practice “cheerful persistence.” Werg<strong>in</strong><br />
talks to his patients about vacc<strong>in</strong>es at<br />
every visit and beg<strong>in</strong>s <strong>the</strong> conversation about<br />
immunizations as early as possible, start<strong>in</strong>g<br />
with prenatal and well-baby checkups. “I have<br />
a group <strong>of</strong> patients who have a lot <strong>of</strong> concerns,<br />
but sometimes with my ‘cheerful persistence’<br />
technique, <strong>the</strong>ir kids will get immunized, but it<br />
may be a little late,” he says.<br />
4<br />
Def<strong>in</strong>e your practice’s policies. Some<br />
pediatric practices strictly adhere to <strong>the</strong><br />
CDC-recommended immunization schedule<br />
to motivate patients to get vacc<strong>in</strong>ated, whereas<br />
o<strong>the</strong>r practices are will<strong>in</strong>g to alter <strong>the</strong> schedule<br />
for patients with concerns. As <strong>the</strong> only doctor<br />
<strong>in</strong> his rural community, Werg<strong>in</strong> wants to<br />
rema<strong>in</strong> a trusted resource for his patients.<br />
“I try to adhere to <strong>the</strong> CDC guidel<strong>in</strong>es, but,<br />
personally, I choose to keep foster<strong>in</strong>g <strong>the</strong><br />
[doctor-patient] relationship…and keep<br />
prodd<strong>in</strong>g gently toward gett<strong>in</strong>g <strong>the</strong> vacc<strong>in</strong>es,”<br />
he says. “But each practice has to decide<br />
how <strong>the</strong>y’ll handle those issues.”<br />
December 2015 Cl<strong>in</strong>icalPracticeToday.com 7
Personaliz<strong>in</strong>g<br />
Options for<br />
Vag<strong>in</strong>al Repair<br />
A married 65-year-old woman with 2 adult<br />
children called her primary care physician because<br />
she had noticed a concern<strong>in</strong>g bulge near <strong>the</strong><br />
open<strong>in</strong>g <strong>of</strong> her vag<strong>in</strong>a. At a Duke Primary Care<br />
cl<strong>in</strong>ic, she described someth<strong>in</strong>g bulg<strong>in</strong>g from her<br />
vag<strong>in</strong>a that seemed to grow <strong>in</strong> size after stra<strong>in</strong><strong>in</strong>g<br />
to have a bowel movement on a day she had<br />
gardened for hours. The doctor <strong>in</strong>formed her that<br />
<strong>the</strong> condition was vag<strong>in</strong>al prolapse.<br />
She was referred to Duke Urogynecology for an<br />
evaluation <strong>of</strong> pelvic organ prolapse. The patient<br />
said she now had to push <strong>the</strong> bulge <strong>in</strong>side daily.<br />
An o<strong>the</strong>rwise healthy, active woman, she was not<br />
experienc<strong>in</strong>g pa<strong>in</strong> but felt <strong>in</strong>complete bladder<br />
empty<strong>in</strong>g and hesitancy when void<strong>in</strong>g.<br />
Amie Kawasaki, MD, <strong>the</strong> treat<strong>in</strong>g urogynecologist<br />
at Duke, discovered that <strong>the</strong> anterior vag<strong>in</strong>al<br />
wall support<strong>in</strong>g <strong>the</strong> bladder as well as <strong>the</strong> uterus<br />
had prolapsed beyond <strong>the</strong> open<strong>in</strong>g <strong>of</strong> her vag<strong>in</strong>a.<br />
After measurements, <strong>the</strong> patient was diagnosed<br />
with stage 3 uterovag<strong>in</strong>al and anterior vag<strong>in</strong>al<br />
prolapse. Several nonsurgical and surgical<br />
treatment options were discussed.<br />
“Some prolapse is very mild and can be observed<br />
and treated with physical <strong>the</strong>rapy, but more<br />
significant prolapse can ei<strong>the</strong>r be managed with<br />
a silicone pessary or with surgery,” Kawasaki says.<br />
Prolapse can be surgically corrected with vag<strong>in</strong>al,<br />
m<strong>in</strong>imally <strong>in</strong>vasive (laparoscopic and/or roboticassisted),<br />
or abdom<strong>in</strong>al surgery. Some surgical procedures<br />
are performed with native tissue, whereas<br />
o<strong>the</strong>rs <strong>in</strong>corporate syn<strong>the</strong>tic mesh material.<br />
Aware <strong>of</strong> all options, <strong>the</strong> patient wanted <strong>the</strong><br />
longest-last<strong>in</strong>g repair so that she could resume<br />
garden<strong>in</strong>g and o<strong>the</strong>r activities for years to come.<br />
The urogynecologist performed robotic-assisted<br />
laparoscopic hysterectomy with mesh sacrocolpopexy.<br />
The <strong>in</strong>dication for this procedure is<br />
advanced vag<strong>in</strong>al prolapse <strong>in</strong>volv<strong>in</strong>g <strong>the</strong> uterus, or<br />
vag<strong>in</strong>al vault <strong>in</strong> <strong>the</strong> case <strong>of</strong> a prior hysterectomy.<br />
Afterward, <strong>the</strong> patient was comfortable and ate a<br />
regular d<strong>in</strong>ner <strong>in</strong> <strong>the</strong> hospital. Six weeks later, she<br />
returned to all <strong>of</strong> her typical activities.<br />
Duke Urogynecology specializes <strong>in</strong> treat<strong>in</strong>g<br />
vag<strong>in</strong>al prolapse, bladder control problems, and<br />
bowel leakage. Duke’s team <strong>of</strong> doctors, nurses,<br />
and physical <strong>the</strong>rapists works with patients to<br />
f<strong>in</strong>d <strong>the</strong> right nonsurgical and surgical solutions<br />
for <strong>the</strong>ir activity level.<br />
To refer, call 844-790-2013. (Image above shows<br />
robotic-assisted laparoscopic hysterectomy.)<br />
8 Cl<strong>in</strong>ical Practice Today from Duke Medic<strong>in</strong>e
Safeguard<strong>in</strong>g<br />
Medical Identities<br />
By Frank Celia<br />
Cyber crim<strong>in</strong>als are now turn<strong>in</strong>g <strong>the</strong>ir sights on<br />
<strong>the</strong> less-protected area <strong>of</strong> medical data, experts<br />
say. Accord<strong>in</strong>g to <strong>the</strong> research firm Ponemon<br />
Institute, medical identity <strong>the</strong>ft affected 1.4<br />
million people <strong>in</strong> 2009 and 2.3 million <strong>in</strong> 2014.<br />
Rick Kam, CIPP/US president and co-founder <strong>of</strong> ID<br />
Experts, which designs security s<strong>of</strong>tware, says,<br />
“One reason to take this seriously is that it can<br />
be a threat to <strong>the</strong> cont<strong>in</strong>ued operation <strong>of</strong> your<br />
bus<strong>in</strong>ess.” To discourage identity <strong>the</strong>ft, consider<br />
follow<strong>in</strong>g some basic precautions.<br />
Know your weaknesses. Earlier this year, several<br />
large health care organizations fell victim to data<br />
breaches. The most common po<strong>in</strong>t <strong>of</strong> <strong>in</strong>gress?<br />
Email. Always use a secure email system, especially<br />
if patients communicate with your practice<br />
this way. (ProtonMail, Tutanota, and Lavaboom<br />
are examples <strong>of</strong> secure email providers.)<br />
Encryption is <strong>the</strong> key to digital security, says Kam.<br />
Almost all digital devices <strong>of</strong>fer encryption for free<br />
or as a built-<strong>in</strong> function. “As soon as you pull <strong>the</strong><br />
device out <strong>of</strong> <strong>the</strong> box, make sure <strong>the</strong> encryption is<br />
on,” he says. “That’s about as complex as it needs<br />
to get.”<br />
Ano<strong>the</strong>r po<strong>in</strong>t <strong>of</strong> weakness: <strong>the</strong> telephone.<br />
Thieves may pose as health care pr<strong>of</strong>essionals<br />
seek<strong>in</strong>g patient <strong>in</strong>formation over <strong>the</strong> phone.<br />
With access to just 1 patient’s data, Medicare<br />
or <strong>in</strong>surers can be bilked <strong>of</strong> thousands <strong>of</strong> dollars.<br />
When unknown cl<strong>in</strong>icians call, take <strong>the</strong>ir contact<br />
<strong>in</strong>formation and <strong>of</strong>fer to call <strong>the</strong>m back. Then, check<br />
<strong>the</strong>ir geographic location aga<strong>in</strong>st <strong>the</strong> patient’s.<br />
Staff tra<strong>in</strong><strong>in</strong>g. Every practice needs a written<br />
data security policy. Topics should <strong>in</strong>clude procedures<br />
for transport<strong>in</strong>g data <strong>of</strong>fsite and us<strong>in</strong>g<br />
mobile devices, protocols for depart<strong>in</strong>g staff (eg,<br />
chang<strong>in</strong>g passwords), and parameters on personal<br />
device use (eg, surf<strong>in</strong>g <strong>the</strong> Internet). At least<br />
1 staff member should be <strong>in</strong> charge <strong>of</strong> implement<strong>in</strong>g<br />
and cont<strong>in</strong>ually updat<strong>in</strong>g this policy.<br />
Additionally, make sure that staff members can<br />
recognize <strong>the</strong> hallmarks <strong>of</strong> “phish<strong>in</strong>g” emails<br />
(ie, ones designed to <strong>in</strong>fect systems with malware<br />
or viruses). Just open<strong>in</strong>g such an email can <strong>in</strong>fect<br />
an entire system.<br />
Paperwork. Never sign referrals for unknown<br />
patients. Because payers are sometimes <strong>the</strong> first<br />
to detect discrepancies, keep enrollment <strong>in</strong>formation<br />
updated. Make sure to promptly <strong>in</strong>form<br />
payers when open<strong>in</strong>g, clos<strong>in</strong>g, mov<strong>in</strong>g, or separat<strong>in</strong>g<br />
from a practice. Lastly, compare remittance<br />
notices with patient records whenever possible.<br />
December 2015<br />
Cl<strong>in</strong>icalPracticeToday.com<br />
9
CASE STUDY<br />
<strong>Treatment</strong><br />
<strong>Alternatives</strong><br />
<strong>in</strong> <strong>Charcot</strong><br />
<strong>Arthropathy</strong><br />
<strong>of</strong> <strong>the</strong> <strong>Foot</strong><br />
Early postoperative phase with foot stabilized<br />
<strong>in</strong> th<strong>in</strong>-wire frame construct.<br />
A patient avoids amputation<br />
A 72-year-old man with type 2 diabetes mellitus<br />
was referred to Duke Medic<strong>in</strong>e <strong>in</strong> October 2014<br />
for treatment <strong>of</strong> <strong>Charcot</strong> arthropathy <strong>of</strong> <strong>the</strong> foot,<br />
a sequela <strong>of</strong> diabetes. Although his blood glucose<br />
levels had been well controlled for 5 to 6 years,<br />
he developed numbness, pa<strong>in</strong>, and peripheral<br />
neuropathy <strong>in</strong> both feet.<br />
In October 2014, he was referred to a local<br />
orthopaedic surgeon who diagnosed <strong>Charcot</strong><br />
arthropathy <strong>of</strong> <strong>the</strong> midfoot based on radiographic<br />
f<strong>in</strong>d<strong>in</strong>gs. Due to severe arthropathy, osteomyelitis,<br />
and sk<strong>in</strong> ulceration, <strong>the</strong> patient was <strong>of</strong>fered<br />
below-<strong>the</strong>-knee amputation or referral for a<br />
second op<strong>in</strong>ion.<br />
“<strong>Charcot</strong> arthropathy is an uncommon complication<br />
<strong>in</strong> patients with long-stand<strong>in</strong>g diabetes<br />
and peripheral neuropathy,” says Beatrice Hong,<br />
MD, a diabetologist at Duke, who did not treat<br />
<strong>the</strong> patient. “The presentation is variable, <strong>in</strong>itially<br />
with warmth and swell<strong>in</strong>g that progresses <strong>in</strong>to a<br />
characteristic collapse <strong>of</strong> <strong>the</strong> arch <strong>of</strong> <strong>the</strong> midfoot,<br />
result<strong>in</strong>g <strong>in</strong> bony prom<strong>in</strong>ences.”<br />
One month earlier, <strong>the</strong> patient had noticed<br />
redness and swell<strong>in</strong>g <strong>in</strong> his left foot and was<br />
treated for presumptive cellulitis. Fragmentation<br />
went unnoticed on radiographs. He cont<strong>in</strong>ued<br />
walk<strong>in</strong>g on <strong>the</strong> foot and developed a sk<strong>in</strong> ulcer<br />
on <strong>the</strong> lateral plantar aspect. Subsequently, he<br />
received local debridement and more antibiotics.<br />
If it is diagnosed before destructive changes <strong>of</strong><br />
<strong>the</strong> bone/jo<strong>in</strong>t take place, <strong>Charcot</strong> arthropathy<br />
can <strong>of</strong>ten be managed with cast<strong>in</strong>g, <strong>of</strong>fload<strong>in</strong>g<br />
braces, custom shoes, and orthotic devices.<br />
However, when <strong>the</strong> bones and jo<strong>in</strong>ts have become<br />
unstable, fragmented, and malaligned with<br />
compromised sk<strong>in</strong> and s<strong>of</strong>t tissue, surgery is<br />
typically necessary. Reconstructive surgery might<br />
be a viable option to avoid amputation.<br />
In <strong>Charcot</strong> arthropathy <strong>of</strong> <strong>the</strong> foot, <strong>the</strong> goal <strong>of</strong><br />
surgical <strong>in</strong>tervention is to realign and stabilize <strong>the</strong><br />
foot with osteotomies, arthrodesis, and <strong>in</strong>ternal<br />
and/or external fixation. Unfortunately, <strong>the</strong> foot<br />
cannot always be salvaged, and amputation may<br />
be necessary for some patients. Many factors<br />
10 Cl<strong>in</strong>ical Practice Today from Duke Medic<strong>in</strong>e
can <strong>in</strong>fluence patient outcomes, <strong>in</strong>clud<strong>in</strong>g loss<br />
<strong>of</strong> protective sensation <strong>in</strong> <strong>the</strong> lower extremities,<br />
obesity, poor bone and s<strong>of</strong>t-tissue quality, peripheral<br />
arterial disease, and immunosuppression.<br />
At Duke Orthopaedics, <strong>the</strong> patient met with<br />
foot and ankle specialist Karl Schweitzer, MD, to<br />
discuss possible treatment options.<br />
“In a normal foot, <strong>the</strong> <strong>in</strong>nervation to <strong>the</strong> jo<strong>in</strong>ts keeps<br />
us from putt<strong>in</strong>g too much pressure on our feet, but<br />
<strong>in</strong> patients with peripheral neuropathy, that protective<br />
sensation is dim<strong>in</strong>ished or absent,” he expla<strong>in</strong>s.<br />
This particular patient was <strong>in</strong> <strong>the</strong> fragmentation/<br />
dissolution stage <strong>of</strong> <strong>Charcot</strong> arthropathy. “Many<br />
<strong>of</strong> <strong>the</strong>se folks get missed because, cl<strong>in</strong>ically, it<br />
looks like an <strong>in</strong>fection and x-rays are not obta<strong>in</strong>ed<br />
or considered,” Schweitzer surmises.<br />
Schweitzer <strong>of</strong>fered reconstructive surgery as an<br />
alternative to amputation. “I told him that if he<br />
was on board, we could try to salvage his foot,”<br />
Schweitzer says. The patient agreed, and <strong>the</strong><br />
procedure took place <strong>in</strong> November 2014.<br />
weeks, Schweitzer added a rocker attachment<br />
on <strong>the</strong> bottom <strong>of</strong> <strong>the</strong> frame so that <strong>the</strong> patient<br />
could walk on it, thus ga<strong>in</strong><strong>in</strong>g some mobility and<br />
<strong>in</strong>dependence.<br />
At 3.5 months, computed tomography revealed<br />
that <strong>the</strong> foot had healed and that no residual<br />
osteomyelitis was present. Schweitzer removed<br />
<strong>the</strong> frame and transitioned <strong>the</strong> patient to a<br />
fracture boot and <strong>the</strong>n, f<strong>in</strong>ally, to a custom<br />
diabetic shoe.<br />
“Now he’s ulcer free, and, more importantly, he<br />
still has his foot,” Schweitzer adds.<br />
Schweitzer stresses <strong>the</strong> importance <strong>of</strong> a multidiscipl<strong>in</strong>ary<br />
approach. “Surgery is only one<br />
component. It takes <strong>in</strong>fectious disease and<br />
hospitalist medic<strong>in</strong>e specialists, along with<br />
physical <strong>the</strong>rapy, nurs<strong>in</strong>g, and nutrition services,<br />
to appropriately care for <strong>the</strong>se patients,” notes<br />
Schweitzer.<br />
Osteotomies were performed to help realign<br />
<strong>the</strong> patient’s foot and prepare <strong>the</strong> bone surfaces<br />
for fusion. Ra<strong>the</strong>r than us<strong>in</strong>g <strong>in</strong>ternal fixation,<br />
which can be a site for <strong>in</strong>fection, Schweitzer<br />
applied an Ilizarov frame, a specialized form <strong>of</strong><br />
external fixation that is stronger than conventional<br />
external fixation systems. Th<strong>in</strong> metal wires were<br />
positioned <strong>in</strong> <strong>the</strong> bone at po<strong>in</strong>ts along <strong>the</strong> foot,<br />
ankle, and lower leg and <strong>the</strong>n attached to a frame<br />
<strong>of</strong> alum<strong>in</strong>um r<strong>in</strong>gs and sta<strong>in</strong>less steel rods.<br />
Schweitzer says <strong>the</strong> wires are tensioned with<strong>in</strong><br />
<strong>the</strong> frame. “It is so strong,” he expla<strong>in</strong>s, “that we<br />
allow <strong>the</strong> patients to weight bear <strong>in</strong> <strong>the</strong> frame.”<br />
The patient wore <strong>the</strong> apparatus for 3 to 4<br />
months, which is how long it takes to achieve<br />
adequate stabilization. However, after 4 to 6<br />
Preoperative photograph <strong>of</strong> patient’s foot reveal<strong>in</strong>g<br />
deep plantar foot ulceration that probes to<br />
bone (left).<br />
Healed s<strong>of</strong>t-tissue envelope, <strong>in</strong>clud<strong>in</strong>g prior plantar<br />
foot ulceration area, follow<strong>in</strong>g frame removal (right).<br />
December 2015<br />
Cl<strong>in</strong>icalPracticeToday.com<br />
11
Essential Tech<br />
Functions for Office-<br />
Based Doctors<br />
By Emily Paulsen<br />
As electronic health record (EHR) adoption<br />
among <strong>of</strong>fice-based physicians cont<strong>in</strong>ues to<br />
climb, an EHR alone may not be enough to meet<br />
<strong>the</strong> needs <strong>of</strong> health care pr<strong>of</strong>essionals and <strong>the</strong>ir<br />
patients. In response to Medicare’s goal <strong>of</strong> ty<strong>in</strong>g<br />
50% <strong>of</strong> payments to quality or value by 2018,<br />
medical <strong>of</strong>fices may need to expand <strong>the</strong>ir<br />
capabilities <strong>in</strong> several areas that an EHR may<br />
not adequately address.<br />
“EHRs were orig<strong>in</strong>ally built to capture charges<br />
and for bill<strong>in</strong>g; <strong>the</strong>y don’t necessarily improve<br />
<strong>the</strong> quality <strong>of</strong> care or workflow for physicians,”<br />
says Neil Versel, health <strong>in</strong>formation technology<br />
reporter for MedCityNews.<br />
Newer products—especially those designed for<br />
small ambulatory practices—have added more<br />
cl<strong>in</strong>ical features, says Andrey Ostrovsky, MD, CEO<br />
<strong>of</strong> Care at Hand, a population health management<br />
system, and co-author <strong>of</strong> <strong>the</strong> 2014 Institute<br />
for Healthcare Improvement report, A Framework<br />
for Select<strong>in</strong>g Digital Health Technology. But, he<br />
adds, medical <strong>of</strong>fices should not expect one<br />
product to do it all. Instead, he suggests start<strong>in</strong>g<br />
with <strong>the</strong> essential functions required to fulfill <strong>the</strong><br />
Triple Aim (improv<strong>in</strong>g <strong>the</strong> patient experience <strong>of</strong><br />
care and population health while reduc<strong>in</strong>g<br />
<strong>the</strong> cost <strong>of</strong> care) and <strong>the</strong>n look<strong>in</strong>g for <strong>the</strong> best<br />
products to fulfill those functions, which <strong>in</strong>clude:<br />
• Population health management. As reimbursement<br />
becomes <strong>in</strong>creas<strong>in</strong>gly tied to prevention<br />
and avoid<strong>in</strong>g unnecessary hospitalizations,<br />
medical <strong>of</strong>fices need functions that can identify<br />
patients who might be at risk <strong>of</strong> disease, relapse,<br />
or readmission.<br />
• Care management/coord<strong>in</strong>ation. Members <strong>of</strong><br />
<strong>the</strong> care team must work toge<strong>the</strong>r to ensure<br />
that patients have a care plan that <strong>in</strong>corporates<br />
evidence-based disease guidel<strong>in</strong>es.<br />
• Patient engagement. Effective and efficient<br />
care <strong>in</strong>volves <strong>the</strong> patient through patient<br />
portals and o<strong>the</strong>r patient-fac<strong>in</strong>g technology.<br />
For example, medical <strong>of</strong>fices may save time and<br />
obta<strong>in</strong> a more detailed medical history with<br />
technology that allows patients to enter data<br />
<strong>the</strong>mselves, Versel says.<br />
• Quality measurement/improvement. Quality<br />
measurement and improvement help ensure<br />
that care teams are work<strong>in</strong>g effectively.<br />
Unfortunately, Ostrovsky po<strong>in</strong>ts out, few products<br />
have been developed for this function.<br />
• Integration and <strong>in</strong>teroperability. Most importantly,<br />
<strong>the</strong> systems should be able to share<br />
<strong>in</strong>formation. “Patients and providers need to<br />
very seamlessly and securely be able to access<br />
<strong>the</strong> technology,” says Ostrovsky, <strong>the</strong>reby<br />
allow<strong>in</strong>g cl<strong>in</strong>icians to focus on effective care<br />
ra<strong>the</strong>r than navigat<strong>in</strong>g <strong>the</strong> technology.<br />
12 Cl<strong>in</strong>ical Practice Today from Duke Medic<strong>in</strong>e
Lower<strong>in</strong>g HbA1C <strong>in</strong><br />
a Patient With O<strong>the</strong>r<br />
Health Challenges<br />
In February 2014, a 51-year-old woman who<br />
had been liv<strong>in</strong>g with type 2 diabetes mellitus<br />
for 21 years was referred to Duke Medic<strong>in</strong>e’s<br />
Endocr<strong>in</strong>ology, Metabolism, and Nutrition division<br />
by her primary care physician.<br />
Her hemoglob<strong>in</strong> A1C (HbA1C) had been 14% for at<br />
least 2 years and had not been below 9% s<strong>in</strong>ce 2010.<br />
The patient was on a basal-bolus <strong>in</strong>sul<strong>in</strong> regimen,<br />
but she reported difficulty adher<strong>in</strong>g to <strong>the</strong><br />
treatment plan.<br />
Her body mass <strong>in</strong>dex (BMI) was 33 kg/m 2 , and she<br />
had diabetes-associated complications: stage 3<br />
chronic kidney disease, gastroparesis, and neuropathy<br />
<strong>in</strong> her feet. She also had hepatic steatosis,<br />
hypertension, hyperlipidemia, chronic pa<strong>in</strong>, and<br />
fibromyalgia. Leonor Cors<strong>in</strong>o, MD, learned that<br />
<strong>the</strong> patient also had bipolar affective disorder.<br />
“It’s critical to ask <strong>the</strong> patient about barriers to<br />
health care and to assess psychosocial factors,”<br />
Cors<strong>in</strong>o notes. The biggest challenges <strong>in</strong> this case<br />
were pa<strong>in</strong> and bipolar disorder.<br />
Cors<strong>in</strong>o discussed with <strong>the</strong> patient that her<br />
mental health probably played a role <strong>in</strong> glucose<br />
control and slightly adjusted <strong>the</strong> <strong>in</strong>sul<strong>in</strong> doses,<br />
prescrib<strong>in</strong>g 130 units <strong>of</strong> <strong>in</strong>sul<strong>in</strong> glarg<strong>in</strong>e at<br />
bedtime and 40 units <strong>of</strong> rapid-act<strong>in</strong>g <strong>in</strong>sul<strong>in</strong><br />
aspart at meals. The <strong>in</strong>sul<strong>in</strong> glarg<strong>in</strong>e was<br />
prescribed as 2 <strong>in</strong>jections <strong>of</strong> 65 units. The patient<br />
took no o<strong>the</strong>r antihyperglycemic medications,<br />
such as metform<strong>in</strong>, because <strong>of</strong> dim<strong>in</strong>ished<br />
kidney function. To manage obesity, she was<br />
prescribed lorcaser<strong>in</strong>.<br />
Cors<strong>in</strong>o sends patients “with mental health<br />
issues that could affect <strong>in</strong>formation process<strong>in</strong>g<br />
for <strong>in</strong>dividual diabetes education,” she says.<br />
The patient had been prescribed pregabal<strong>in</strong>,<br />
duloxet<strong>in</strong>e, and gabapent<strong>in</strong> for <strong>the</strong> management<br />
<strong>of</strong> neuropathy and chronic pa<strong>in</strong> without success,<br />
so Cors<strong>in</strong>o also referred her for a neurology<br />
consultation and contacted <strong>the</strong> patient’s mental<br />
health care cl<strong>in</strong>ician to discuss her proposed goals.<br />
The patient had 4 follow-up visits <strong>in</strong> <strong>the</strong> first year—<br />
a step that Cors<strong>in</strong>o considers crucial for success<br />
with patients who have complex needs. By August<br />
2014, <strong>the</strong> patient’s HbA1C had decreased to 7.8%,<br />
her lowest value s<strong>in</strong>ce at least 2009. Her fast<strong>in</strong>g<br />
and mealtime blood glucose levels were mostly<br />
at goal, and she had very few read<strong>in</strong>gs above<br />
180 mg/dL after eat<strong>in</strong>g. Her BMI had decreased<br />
to 31 kg/m 2 . To refer, call 844-790-2013. (Image<br />
shows a blood glucose meter.)<br />
December 2015<br />
Cl<strong>in</strong>icalPracticeToday.com<br />
13
Transition<strong>in</strong>g<br />
Young Patients to<br />
Adult Heart Care<br />
Pediatric patients with congenital heart disease<br />
generally receive <strong>the</strong> care <strong>the</strong>y need to thrive<br />
throughout childhood, but, as <strong>the</strong>y make <strong>the</strong><br />
transition to adult care, several challenges<br />
should be considered to keep care cont<strong>in</strong>uous<br />
and tailored to adult needs.<br />
Patients, caregivers, and physicians need awareness<br />
about <strong>the</strong> special needs <strong>of</strong> this transitional<br />
group <strong>of</strong> patients. Richard Krasuski, MD, who<br />
heads <strong>the</strong> Duke Adult Congenital Heart Disease<br />
Program, says that almost all patients with<br />
congenital heart disease are at risk <strong>of</strong> develop<strong>in</strong>g<br />
3 common problems: heart failure, rhythm<br />
disorders, and pulmonary hypertension.<br />
If heart failure develops, medications or pacemak<strong>in</strong>g<br />
devices can be used to help <strong>the</strong> heart<br />
pump more effectively. Sometimes, a patient<br />
simply needs a repair on a leaky heart valve or<br />
a surgical patch on a hole <strong>in</strong> <strong>the</strong> heart that was<br />
placed decades earlier. These procedures can be<br />
done with surgery or <strong>in</strong> <strong>the</strong> ca<strong>the</strong>terization laboratory.<br />
If <strong>the</strong> disease is too advanced, some patients<br />
may need a heart or even heart-lung transplant.<br />
Rhythm disturbances can orig<strong>in</strong>ate <strong>in</strong> <strong>the</strong> upper<br />
heart chambers (atria) or lower heart chambers<br />
(ventricles). Although patients <strong>of</strong>ten view atrial<br />
rhythm disorders as just a nuisance, <strong>the</strong>y can<br />
<strong>in</strong>terfere with well-be<strong>in</strong>g and <strong>in</strong>crease <strong>the</strong> risk <strong>of</strong><br />
stroke. A ventricular arrhythmia, however, could<br />
lead to more severe problems, <strong>in</strong>clud<strong>in</strong>g sudden<br />
death. If ventricular arrhythmia is diagnosed,<br />
patients need immediate medical attention.<br />
Krasuski says that rhythm disturbances can be<br />
a sign <strong>of</strong> blood flow problems, such as blockage<br />
<strong>in</strong> arteries or leaky valves. “Each patient with a<br />
rhythm disturbance needs a careful look at <strong>the</strong>ir<br />
<strong>in</strong>ternal plumb<strong>in</strong>g,” he says. “It may not be <strong>the</strong><br />
heart’s rhythm that is <strong>the</strong> primary problem.”<br />
The third potential problem to watch out for<br />
is pulmonary hypertension, an elevation <strong>of</strong><br />
pressure <strong>in</strong> <strong>the</strong> blood vessels <strong>of</strong> <strong>the</strong> lung. “This<br />
can be due to a back-up <strong>in</strong> blood flow from <strong>the</strong><br />
pump<strong>in</strong>g chamber to <strong>the</strong> body (so-called pulmonary<br />
venous hypertension),” Krasuski says. “It can<br />
be related to leaky or narrowed heart valves or a<br />
weakened heart muscle.”<br />
If <strong>the</strong> primary issue is an abnormality <strong>in</strong> <strong>the</strong><br />
lung vessels <strong>the</strong>mselves, <strong>the</strong>n it is referred to as<br />
pulmonary arterial hypertension. This is <strong>of</strong>ten<br />
<strong>the</strong> result <strong>of</strong> abnormal communications (shunts)<br />
<strong>in</strong> <strong>the</strong> heart and can even occur long after <strong>the</strong>y<br />
have been successfully repaired. Pulmonary<br />
arterial hypertension can be treated with medications,<br />
ca<strong>the</strong>ter procedures, or surgery.<br />
14 Cl<strong>in</strong>ical Practice Today from Duke Medic<strong>in</strong>e
At Duke, some patients with complex congenital<br />
heart disease may be treated with a hybrid<br />
procedure <strong>in</strong>volv<strong>in</strong>g both a cardiac surgeon and<br />
a cardiologist.<br />
Cont<strong>in</strong>u<strong>in</strong>g <strong>in</strong> Adult Care<br />
Transition<strong>in</strong>g patients <strong>in</strong>to adult care as <strong>the</strong>y<br />
leave <strong>the</strong>ir teens is not always easy. “We can<br />
do remarkable th<strong>in</strong>gs to treat congenital heart<br />
patients as <strong>the</strong>y age, but first <strong>the</strong>y have to<br />
consult with a doctor and be evaluated and learn<br />
exactly what needs to be done,” Krasuski says.<br />
“And that is a big part <strong>of</strong> <strong>the</strong> problem.”<br />
For example, many patients are lost to follow-up<br />
as <strong>the</strong>y fall <strong>of</strong>f <strong>of</strong> <strong>the</strong>ir parents’ health <strong>in</strong>surance.<br />
“Ano<strong>the</strong>r reason is that teens naturally chafe<br />
aga<strong>in</strong>st authority, and this can <strong>in</strong>clude neglect<strong>in</strong>g<br />
<strong>the</strong>ir commitment to health care,” Krasuski says.<br />
“In o<strong>the</strong>r countries, <strong>in</strong>clud<strong>in</strong>g Canada, <strong>the</strong>re is<br />
better monitor<strong>in</strong>g and preparation—this lapse<br />
doesn’t happen as <strong>of</strong>ten.”<br />
Krasuski expla<strong>in</strong>s, “Young<br />
adults may let <strong>the</strong>ir appo<strong>in</strong>tments<br />
or medications lapse or<br />
may avoid mak<strong>in</strong>g <strong>the</strong> transition<br />
to heart specialists who<br />
work with and understand<br />
<strong>the</strong> problems <strong>of</strong> ag<strong>in</strong>g hearts.”<br />
Some patients may delay<br />
until <strong>the</strong>y are <strong>in</strong> <strong>the</strong>ir 20s and<br />
30s to see a new physician. The doctor may not<br />
be a specialist <strong>in</strong> congenital heart disease and,<br />
<strong>the</strong>refore, may be unfamiliar with <strong>the</strong>ir heart<br />
issues and <strong>the</strong> details <strong>of</strong> prior surgeries. Lack<br />
<strong>of</strong> communication with <strong>the</strong>ir previous doctors<br />
may also exist. “Patients end up unsatisfied and<br />
<strong>of</strong>ten return to <strong>the</strong> comfort <strong>of</strong> see<strong>in</strong>g <strong>the</strong>ir earlier<br />
expert, a pediatrician or primary care physician,”<br />
Krasuski notes.<br />
Education Is Key<br />
Some patients with<br />
congenital heart<br />
disease may wait<br />
until <strong>the</strong>y are <strong>in</strong> <strong>the</strong>ir<br />
20s and 30s to see a<br />
new physician.<br />
Krasuski, who established an adult congenital<br />
heart program at <strong>the</strong> Cleveland Cl<strong>in</strong>ic before<br />
com<strong>in</strong>g to Duke, says it is best to beg<strong>in</strong> talk<strong>in</strong>g<br />
about <strong>the</strong> transition period even before children<br />
enter <strong>the</strong>ir teens.<br />
“The stakes may be higher than patients and<br />
families know,” Krasuski says. “Because <strong>of</strong> <strong>the</strong><br />
potential dangers, every patient should have<br />
a well-<strong>in</strong>formed primary care physician if <strong>the</strong>y<br />
don’t have a local cardiologist who understands<br />
<strong>the</strong>ir case. They may not be able to travel 5 hours<br />
if <strong>the</strong>y are hav<strong>in</strong>g emergent problems. We’re<br />
fortunate at Duke that we can air transport<br />
patients here when <strong>the</strong> need arises.”<br />
Ano<strong>the</strong>r reason for eas<strong>in</strong>g <strong>the</strong> transition is a<br />
predisposition to adult diseases earlier <strong>in</strong> life.<br />
Some people with congenital heart disease<br />
may not know that <strong>the</strong>y have a higher risk<br />
than <strong>the</strong> general population<br />
<strong>of</strong> develop<strong>in</strong>g high blood<br />
pressure or coronary artery<br />
disease, Krasuski notes. O<strong>the</strong>r<br />
problems can <strong>the</strong>n develop,<br />
<strong>in</strong>clud<strong>in</strong>g liver disease,<br />
diabetes, varicose ve<strong>in</strong>s, and<br />
peripheral artery disease.<br />
“It’s best to have an adult<br />
congenital heart expert l<strong>in</strong>ed<br />
up,” says Krasuski, particularly one who understands<br />
all levels <strong>of</strong> congenital heart disease,<br />
from mild to severe cases, categorized per <strong>the</strong><br />
2008 guidel<strong>in</strong>es from <strong>the</strong> American College <strong>of</strong><br />
Cardiology and <strong>the</strong> American Heart Association.<br />
To learn more or refer a patient, call 844-790-2013.<br />
(Image on previous page depicts a hole <strong>in</strong> <strong>the</strong> heart,<br />
which is a congenital defect.)<br />
December 2015<br />
Cl<strong>in</strong>icalPracticeToday.com<br />
15
Duke Medic<strong>in</strong>e<br />
DUMC 3687<br />
Durham, NC 27710<br />
844-790-2013<br />
Non-pr<strong>of</strong>it Org.<br />
U.S. Postage<br />
PAID<br />
Durham, NC<br />
Permit No. 60<br />
Look<strong>in</strong>g for more practice management tips,<br />
compell<strong>in</strong>g case studies, and <strong>in</strong>teractive image<br />
quizzes—free with a simple click?<br />
Don’t miss out on complimentary access to <strong>the</strong><br />
onl<strong>in</strong>e edition <strong>of</strong> Cl<strong>in</strong>ical Practice Today!<br />
Confirm your free access by simply visit<strong>in</strong>g Cl<strong>in</strong>icalPracticeToday.com to<br />
start receiv<strong>in</strong>g <strong>the</strong> latest scientific research and breakthrough discoveries<br />
from your colleagues at Duke Medic<strong>in</strong>e.<br />
To confirm your subscription, visit Cl<strong>in</strong>icalPracticeToday.com.<br />
Subscribe<br />
Today!<br />
Questions? Call (toll-free)<br />
866-858-7434 or email<br />
<strong>in</strong>fo@med-iq.com.