Approximation and contact of the maxillary central incisor roots with the incisive canal after maximum retraction with temporary anchorage devices_ Report of 2 patients
artigos ortodontia
artigos ortodontia

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Chung, Choi, <strong>and</strong> Kim 497<br />
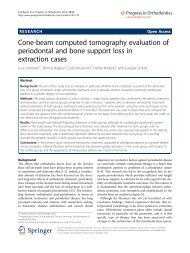
Fig 4. CBCT images <strong>of</strong> <strong>the</strong> <strong>maxillary</strong> arch <strong>and</strong> <strong>the</strong> <strong>central</strong> <strong>incisor</strong>s <strong>after</strong> <strong>maximum</strong> <strong>retraction</strong>: A, axial<br />
<strong>and</strong> B, coronal sections show that <strong>the</strong> right <strong>central</strong> <strong>incisor</strong> root is in <strong>contact</strong> <strong>with</strong> <strong>the</strong> <strong>incisive</strong> <strong>canal</strong>;<br />
C, sagittal sections <strong>of</strong> <strong>the</strong> right <strong>central</strong> <strong>incisor</strong> slice passing <strong>the</strong> <strong>incisive</strong> <strong>canal</strong>; D, ano<strong>the</strong>r slice slightly<br />
distal passing <strong>the</strong> tooth axis; E, sagittal section <strong>of</strong> <strong>the</strong> left <strong>central</strong> <strong>incisor</strong> slice passing <strong>the</strong> <strong>incisive</strong> <strong>canal</strong>;<br />
F, ano<strong>the</strong>r slice slightly distal passing <strong>the</strong> tooth axis. The arrows indicate <strong>the</strong> <strong>incisive</strong> <strong>canal</strong>.<br />
DISCUSSION<br />
The proximity <strong>of</strong> <strong>the</strong> <strong>maxillary</strong> <strong>incisor</strong> <strong>roots</strong> to <strong>the</strong><br />
<strong>incisive</strong> <strong>canal</strong> or <strong>the</strong> possibility <strong>of</strong> approximation or invasion<br />
<strong>of</strong> <strong>the</strong> tooth <strong>roots</strong> into <strong>the</strong> <strong>incisive</strong> <strong>canal</strong> <strong>after</strong> anterior<br />
<strong>retraction</strong> has not been closely evaluated in <strong>the</strong><br />
orthodontic literature. The lack <strong>of</strong> information is<br />
possibly because <strong>the</strong> <strong>incisive</strong> <strong>canal</strong> is a midsagittal structure<br />
positioned between <strong>the</strong> <strong>roots</strong>, <strong>and</strong> its dimension or<br />
morphology is not clearly defined by conventional<br />
2-dimensional radiographs. However, <strong>with</strong> <strong>the</strong> help <strong>of</strong><br />
3D imaging, <strong>the</strong> <strong>incisive</strong> <strong>canal</strong> was noted as an anatomic<br />
structure that may be associated <strong>with</strong> orthodontically<br />
induced inflammatory root resorption <strong>of</strong> <strong>the</strong> <strong>maxillary</strong><br />
<strong>central</strong> <strong>incisor</strong>s during <strong>maximum</strong> <strong>retraction</strong>.<br />
The <strong>maxillary</strong> <strong>central</strong> <strong>incisor</strong>s are most frequently<br />
involved in orthodontically induced inflammatory root<br />
resorption, which is reportedly associated <strong>with</strong> patientrelated<br />
risk factors such as genetic influence, root<br />
morphology, root proximity to <strong>the</strong> cortical bone, alveolar<br />
bone density, <strong>and</strong> type <strong>of</strong> malocclusion, <strong>and</strong> <strong>with</strong> orthodontic<br />
treatment-related risk factors such as treatment<br />
duration, magnitude <strong>of</strong> force, <strong>and</strong> amount <strong>of</strong> apical<br />
root movement. 14,15 Although force levels about 150 g<br />
<strong>of</strong> force were used for en-masse <strong>retraction</strong> in our<br />
<strong>patients</strong>, it is possible that <strong>the</strong> apparent root resorption<br />
was mainly related to <strong>the</strong> large amounts <strong>of</strong> anterior<br />
<strong>retraction</strong> <strong>and</strong> root movement to maintain anterior<br />
torque.<br />
However, in patient 1, <strong>the</strong> differences in <strong>the</strong> levels <strong>of</strong><br />
root resorption between <strong>the</strong> right <strong>and</strong> left <strong>central</strong> <strong>incisor</strong>s<br />
were quite evident <strong>with</strong> distinct morphologic features,<br />
whereas <strong>the</strong> patient-related <strong>and</strong> treatment-related<br />
American Journal <strong>of</strong> Orthodontics <strong>and</strong> Dent<strong>of</strong>acial Orthopedics September 2015 Vol 148 Issue 3