GANGLIOGLIOMA (WHO I) GANGLIOGLIOMA (WHO I)
GANGLIOGLIOMA (WHO I) GANGLIOGLIOMA (WHO I)
GANGLIOGLIOMA (WHO I) GANGLIOGLIOMA (WHO I)

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
TUMORS OF THE CENTRAL<br />
NERVOUS SYSTEM: PART 3<br />
Arie Perry, M.D.<br />
Division of Neuropathology,<br />
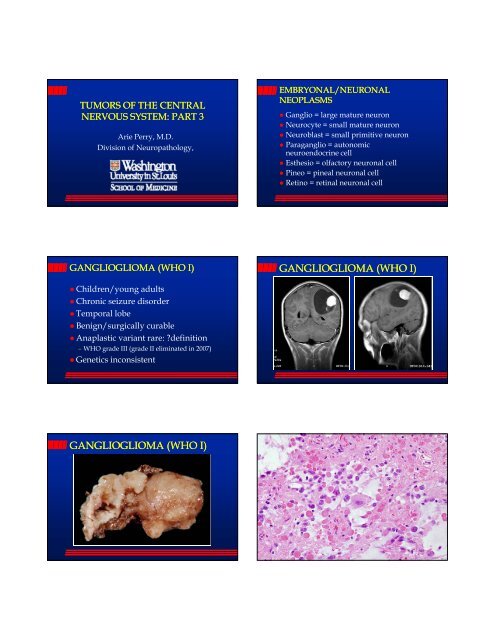
<strong>GANGLIOGLIOMA</strong> (<strong>WHO</strong> I)<br />
� Children/young adults<br />
� Chronic seizure disorder<br />
� Temporal lobe<br />
� Benign/surgically curable<br />
� Anaplastic variant rare: ?definition<br />
– <strong>WHO</strong> grade III (grade II eliminated in 2007)<br />
� Genetics inconsistent<br />
<strong>GANGLIOGLIOMA</strong> (<strong>WHO</strong> I)<br />
EMBRYONAL/NEURONAL<br />
NEOPLASMS<br />
� Ganglio = large mature neuron<br />
� Neurocyte = small mature neuron<br />
� Neuroblast = small primitive neuron<br />
� PParaganglio li = autonomic t i<br />
neuroendocrine cell<br />
� Esthesio = olfactory neuronal cell<br />
� Pineo = pineal neuronal cell<br />
� Retino = retinal neuronal cell<br />
<strong>GANGLIOGLIOMA</strong> (<strong>WHO</strong> I)
CG<br />
PASD<br />
SYN Neu-N<br />
CD34<br />
SPECIAL VARIANTS<br />
� Desmoplastic Infantile Ganglioglioma<br />
or Astrocytoma (DIG/DIA)<br />
� Dysplastic Gangliocytoma of<br />
Cerebellum (Lhermitte-Duclos<br />
Disease): Cowden Disease (PTEN)
DESMOPLASTIC INFANTILE<br />
<strong>GANGLIOGLIOMA</strong> (DIG) (<strong>WHO</strong> I)<br />
� Age
LHERMITTE<br />
LHERMITTE-DUCLOS DUCLOS DZ (<strong>WHO</strong> I)<br />
� Dysplastic gangliocytoma of cerebellum<br />
� Peak onset in third to fourth decade<br />
� Internal granular layer dysplasia/hypertrophy<br />
� Expanded foliar cortex, diminished white matter<br />
� Obstructive hydrocephalus/ataxia<br />
� Cowden disease/PTEN mutations in nearly all<br />
adults, but some exceptions in children<br />
� PTEN functions in neuronal migration,<br />
development and soma size (knockout mice)<br />
LHERMITTE<br />
LHERMITTE-DUCLOS DUCLOS DZ<br />
LHERMITTE<br />
LHERMITTE-DUCLOS DUCLOS DZ LHERMITTE<br />
LHERMITTE-DUCLOS DUCLOS DZ<br />
LHERMITTE<br />
LHERMITTE-DUCLOS DUCLOS DZ<br />
CENTRAL NEUROCYTOMA (<strong>WHO</strong> II)<br />
� Older children/Young adults<br />
� Lat. v./3 rd v./F. of Monro/S. pellucidum<br />
� Obstructive hydrocephalus<br />
�� Globular/calcified<br />
� Usually benign, but may recur (MIB-1>2%)<br />
� DDx: oligodendroglioma, ependymoma<br />
� Genetics inconsistent, but no 1p/19q losses
CENTRAL NEUROCYTOMA, <strong>WHO</strong> II<br />
EXTRAVENTRICULAR NEUROCYTOMA<br />
Tumors with neurocytic<br />
features also occur outside the<br />
ventricular system:<br />
Cerebral hemispheres<br />
Cerebellar liponeurocytoma<br />
(now <strong>WHO</strong> grade II)<br />
Spine<br />
Generally circumscribed rather<br />
than infiltrative<br />
SYN Neu-N<br />
GFAP MIB-1<br />
EXTRAVENTRICULAR NEUROCYTOMA<br />
GFAP positive cells<br />
Ganglion cells
PINEAL PARENCHYMAL TUMORS<br />
� Pineocytoma, <strong>WHO</strong> grade I<br />
– Identical to neurocytomas (pineocytic rosettes)<br />
� PPT, Int. Differentiation, <strong>WHO</strong> grades II-III<br />
– No rosettes, mitotic activity, NF+ = gr. II?<br />
– High MI (Ki-67) and no NF+ = gr. III?<br />
� Pineoblastoma, <strong>WHO</strong> grade IV<br />
PINEOCYTOMA, <strong>WHO</strong> GRADE I<br />
PPT, INT. DIFF., <strong>WHO</strong> GRADE II EMBRYONAL CNS TUMORS<br />
MEDULLOBLASTOMA/PNET (<strong>WHO</strong> IV)<br />
� Children/young adults<br />
� Aggressive natural history<br />
� CSF seeding (“icing” and drop mets)<br />
�� 5-year 5 year survival: 60-80% 60 80% with therapy<br />
� Radiation may save patient’s life, but is harmful<br />
to the developing CNS<br />
� Favorable and unfavorable variants<br />
� Histogenesis: EGL or SEGM of 4th ventricle<br />
� Medulloblastoma<br />
– Classic<br />
– Desmoplastic<br />
– Extensively Nodular<br />
– L Large cell/Anaplastic<br />
ll/A l ti<br />
– Medullo with myogenic<br />
differentiation<br />
– Medullo with melanotic<br />
differentiation<br />
� Pineoblastoma<br />
� CNS PNET<br />
– Neuroblastoma<br />
– Ganglioneuroblastoma<br />
– Ependymoblastoma<br />
– Medulloepithelioma<br />
� Atypical teratoid /<br />
Rhabdoid tumor
DESMOPLASTIC MEDULLOBLASTOMA<br />
Reticulin SYN<br />
MIB-1
ANAPLASTIC MEDULLOBLASTOMA<br />
Pre-Op Post-Op 2 weeks Post-Op
MEDULLOBLASTOMA GENETICS<br />
� Genetics<br />
– isochromosome 17q (50%)<br />
p<br />
q<br />
p<br />
q<br />
BAF-47<br />
CEP17<br />
17q11.2<br />
CEP8<br />
c-myc
EXTENSIVELY NODULAR MEDULLO
Primitive Neoplasms<br />
S-PNET Medullo pPNET/ES AT/RT<br />
Neuronal ± glial Neuronal ± glial Limited neuronal Polyphenotypic<br />
phenotype phenotype phenotype (EMA, SMA,<br />
O13 (CD99) (CD99)- O13 (CD99) (CD99)- O13 (CD99)+ (CD99) VIM, O13)<br />
?-14q, -19q i(17q) t(11;22)<br />
EWS-FLI-1<br />
35% 5-year<br />
survival<br />
70% 5-year<br />
survival<br />
AT/RT, <strong>WHO</strong> IV<br />
40% 5-year<br />
survival<br />
-22q<br />
INI-1 mutations<br />
BCL2<br />
NF2<br />
BAF-47<br />
VIM<br />
SMA<br />
DURAL EWS-PNET<br />
EWS PNET<br />
EMA<br />
BCL2<br />
NF2
CD99<br />
PAS PASD<br />
EWS-BA EWS-FLI1