Potency and Tolerance of Calcitonin Stimulation with High Dose ...
Potency and Tolerance of Calcitonin Stimulation with High Dose ...
Potency and Tolerance of Calcitonin Stimulation with High Dose ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
J Clin Endocrin Metab. First published ahead <strong>of</strong> print June 2, 2009 as doi:10.1210/jc.2008-2403<br />
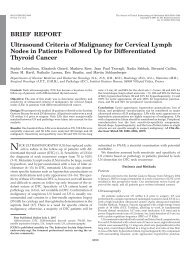
BRIEF REPORT<br />
<strong>Potency</strong> <strong>and</strong> <strong>Tolerance</strong> <strong>of</strong> <strong>Calcitonin</strong> <strong>Stimulation</strong> <strong>with</strong> <strong>High</strong> <strong>Dose</strong> Calcium versus<br />
Pentagastrin in Normal Adults<br />
Patricia Doyle, Christian Düren, Kai Nerlich, Frederik A. Verburg, Inge Grelle, Hanne Jahn,<br />
Martin Fassnacht 1 , Uwe Mäder 2 , Christoph Reiners <strong>and</strong> Markus Luster<br />
Department <strong>of</strong> Nuclear Medicine, 1 Dept. <strong>of</strong> Internal Medicine I, Endocrine <strong>and</strong> Diabetes Unit<br />
<strong>and</strong> 2 Comprehensive Cancer Center, University Hospital, University <strong>of</strong> Würzburg, Würzburg,<br />
Germany<br />
Abbreviated title: Calcium is a more potent than pentagastrin<br />
Key terms: human calcitonin, reference range, healthy adults, basal, stimulated, pentagastrin,<br />
calcium, medullary thyroid cancer<br />
Precis: <strong>High</strong>-dose calcium is a more potent <strong>and</strong> better-tolerated secretogogue <strong>of</strong> human<br />
calcitonin than is pentagastrin in young thyroid-healthy human subjects<br />
Word count excluding abstract, figure captions, <strong>and</strong> references: 1799<br />
Correspondence <strong>and</strong> reprint requests to:<br />
Christoph Reiners, MD, PhD<br />
Department <strong>of</strong> Nuclear Medicine, University <strong>of</strong> Würzburg<br />
Josef-Schneider-Strasse 2<br />
97080 Würzburg GERMANY<br />
+49-931-201-35868 (phone)<br />
+49-931-201-35247 (fax)<br />
reiners@nuklearmedizin.uni-wuerzburg.de<br />
Disclosure:<br />
P.D., C.D., K.N., F.A.V., I.G., H.J., M.F., U.M. <strong>and</strong> M.L. have nothing to declare.<br />
C.R. Received Grant support for Logistical <strong>and</strong> editorial assistance on this paper from<br />
Siemens Healthcare diagnostics GmbH<br />
Copyright (C) 2009 by The Endocrine Society<br />
1
Abstract<br />
Objective: 1. To Compare pentagastrin- <strong>and</strong> calcium-stimulated serum hCT levels for non-<br />
smoking healthy adults <strong>with</strong>out evidence <strong>of</strong> thyroid disorders 2. Determine reference ranges<br />
<strong>of</strong> basal <strong>and</strong> pentagastrin- <strong>and</strong> calcium-stimulated serum hCT levels.<br />
Design: Healthy volunteer study including <strong>with</strong>in-group <strong>and</strong> inter-group comparisons.<br />
Setting: Tertiary referral center.<br />
Subjects: Fifty healthy, non-smoking volunteers (25 female; ages 22 - 57 years) <strong>with</strong>out<br />
evidence <strong>of</strong> thyroid abnormality.<br />
Interventions: hCT measurement using a <strong>Calcitonin</strong> two-site automated chemiluminescent<br />
immunometric assay (the most common hCT assay in clinical practice) in serum samples<br />
obtained before <strong>and</strong> 2 min, 5 min, <strong>and</strong> 15 min after intravenous stimulation using<br />
pentagastrin, 0.5 µg/kg bodyweight, or calcium gluconate, 2.5 mg/kg.<br />
Main outcome measures: Reference ranges for basal, unstimulated <strong>and</strong> pentagastrin- or<br />
calcium-stimulated hCT; pentagastrin <strong>and</strong> calcium tolerability in healthy adults.<br />
Results: Ninety-fifth percentile basal hCT values did not differ between males <strong>and</strong> females<br />
(5.0 vs. 5.7 pg/mL). Ninety-fifth percentile maximal stimulated hCT values rose distinctly<br />
after pentagastrin (peak: men, 37.8 pg/mL; women, 26.2 pg/mL) <strong>and</strong> even more so after<br />
calcium (peak: men, 131.1 pg/mL, women, 90.2 pg/mL). No hCT increase was detected in<br />
4/25 men <strong>and</strong> 12/25 women after pentagastrin versus 0/24 men <strong>and</strong> 2/18 women after<br />
calcium. Calcium was associated <strong>with</strong> fewer <strong>and</strong> less intense adverse effects than was<br />
pentagastrin.<br />
Conclusion: <strong>High</strong>-dose calcium is a more potent <strong>and</strong> better-tolerated hCT stimulator than is<br />
pentagastrin. The reference ranges for basal <strong>and</strong> stimulated hCT established via automated<br />
chemiluminescent assay were lower than those reported for other assays.<br />
2
Introduction<br />
Human calcitonin (hCT) is a tumor marker essential to the diagnosis <strong>and</strong> follow-up <strong>of</strong><br />
medullary thyroid cancer (MTC ) (1-4). Current European consensus recommends hCT<br />
measurement when initially evaluating thyroid nodules (5). If hCT is mildly elevated,<br />
European centers commonly perform a confirmatory test <strong>with</strong> intravenous pentagastrin<br />
stimulation (3, 6-8). A less popular alternative stimulation test uses a short intravenous<br />
calcium infusion (3, 6). <strong>Stimulation</strong> testing also may aid early risk stratification in patients<br />
<strong>with</strong> MTC (4).<br />
For reasons including the unavailability <strong>of</strong> pentagastrin in the US, the American<br />
Thyroid Association has not recommended routine hCT measurement (9). However, a recent<br />
U.S. cost-effectiveness study (10), though not <strong>with</strong>out flaws, provides data favoring such<br />
testing .<br />
Key to employing stimulated hCT measurement clinically are the reliability <strong>and</strong><br />
relevance to everyday practice <strong>of</strong> healthy adult reference values. Most published reference<br />
values for stimulation tests were obtained in small series not rigorously screened for thyroid<br />
abnormality (2, 6, 7, 11). Calcium stimulation was investigated in only a few studies (12)<br />
using disparate regimens, e.g., 10% calcium gluconate dosages <strong>of</strong> 2.0-2.5 mg/kg body weight,<br />
injection over 30 sec-5 min (3, 13-15).<br />
Indeed, hCT reference ranges generally were obtained <strong>with</strong> competitive<br />
radioimmunoassays <strong>and</strong> do not apply to automated non-competitive chemiluminescent<br />
immunometric assays.<br />
Differences in hCT measurement are evident even <strong>with</strong>in the radioimmunoassay<br />
class, emphasizing the need to re-evaluate reference ranges <strong>and</strong> cut-<strong>of</strong>f values for each assay<br />
individually (16).<br />
We therefore conducted this study to define the normal ranges on a commonly used<br />
chemiluminescent immunometric assay <strong>of</strong> serum hCT values in healthy adults before <strong>and</strong><br />
after pentagastrin or high-dose calcium stimulation,. We also sought to assess these<br />
secretagogues’ tolerability in such subjects..<br />
3
Subjects <strong>and</strong> Methods<br />
Study sample<br />
Table 1 summarizes study sample characteristics. The sample comprised 50 non-<br />
smoking, non-pregnant adult volunteers <strong>with</strong>out known chronic or serious acute illness or<br />
evident thyroid abnormality after screening described below. Subjects could not take<br />
prescription medication other than oral contraceptives (9/25 women). Any pre-study<br />
laboratory abnormality (potassium, sodium, calcium, creatinine, liver enzymes) resulted in<br />
exclusion. The University <strong>of</strong> Würzburg Ethics Committee approved the study; all subjects<br />
gave written informed consent.<br />
Screening for thyroid abnormalities<br />
Pre-study, all subjects underwent thyroid ultrasonography <strong>with</strong> a Sonoline Elegra<br />
system (Siemens, Erlangen, Germany) featuring a linear 7.5-MHz transducer. Thyroid<br />
volume in mL was calculated using the algorithm, 0.5 x length x width x depth. Additionally,<br />
subjects underwent free T3, free T4, <strong>and</strong> TSH measurement using IMMULITE ® 2000<br />
automated chemiluminescent assays (Siemens Healthcare Diagnostics GmbH, Eschborn,<br />
Germany). Thyroperoxidase <strong>and</strong> thyroglobulin autoantibody titers were determined using<br />
enzyme immunoassays (Varelisa, Phadia GmbH, Freiburg, Germany).<br />
Basal <strong>and</strong> Stimulated hCT testing<br />
We averaged basal hCT measurements taken in the initial examination <strong>and</strong> before<br />
each stimulation test. After pentagastrin stimulation, there was a wash-out period <strong>of</strong> at least<br />
6 months before the calcium stimulation described below. Eight subjects (1 man, 7 women)<br />
missed that calcium stimulation because they became pregnant (n = 1) or left our region (n =<br />
7).<br />
Pentagastrin (Pentagastrin Injection BP, Cambridge Laboratories, Wallsend, UK) was<br />
administered as an intravenous injection <strong>of</strong> 0.5 µg/kg body weight over 10 sec <strong>and</strong> calcium<br />
gluconate (Calcium Braun 10%, Braun Melsungen AG, Melsungen, Germany) as an<br />
intravenous injection <strong>of</strong> 2.5 mg/kg at 10 mL/min. All subjects fasted ≥ 4 hr before<br />
stimulation.<br />
4
Serum hCT Assay<br />
Blood samples were taken via in-dwelling intravenous cannula immediately before<br />
<strong>and</strong> 2 min, 5 min, <strong>and</strong> 15 min after the intravenous pentagastrin or calcium injection.<br />
Samples were placed in ice-water to prevent hCT degradation <strong>and</strong> transferred to the in-house<br />
laboratory <strong>with</strong>in 30 min <strong>of</strong> being drawn for centrifugation after clotting was complete. Serum<br />
samples were assayed for calcitonin using the IMMULITE ® 2000 <strong>Calcitonin</strong> automated<br />
chemiluminescent system (Siemens Healthcare Diagnostics GmbH, Eschborn, Germany), a<br />
solid-phase, enzyme–labeled, two-site immunometric assay. The assay received regulatory<br />
approval based on data showing an analytical sensitivity <strong>of</strong> 2 pg/ml. Subsequent testing by the<br />
manufacturer has shown an analytical sensitivity <strong>of</strong> 0.34 pg/ml <strong>and</strong> a functional sensitivity <strong>of</strong><br />
0.7 pg/ml. Analytical sensitivity is defined as a concentration two st<strong>and</strong>ard deviations (SDs)<br />
above the mean counts/sec <strong>of</strong> the zero calibrator, i.e., the 97.5 th percentile. Functional<br />
sensitivity is defined as the lowest analyte level <strong>with</strong> an inter-assay coefficient <strong>of</strong> variation<br />
(CV)
high percentage <strong>of</strong> women (80%) but not men (32%) had very low basal hCT concentrations<br />
(
calcium-stimulated hCT levels were strongly correlated (Figure 1C, Spearmans’ rho = 0.758,<br />
P < 0.001). Analysis <strong>of</strong> variance revealed that sex significantly influenced the magnitude <strong>of</strong><br />
the stimulated hCT levels (P =0.008), but age, weight, height, body mass index <strong>and</strong> thyroid<br />
volume did not.<br />
Tolerability <strong>of</strong> stimulation agents<br />
Clinical side effects also are reported in Table 1. Due to a perception <strong>of</strong> more<br />
unpleasant adverse effects <strong>of</strong> pentagastrin than <strong>of</strong> calcium, all subjects receiving both (n = 42)<br />
declared a preference for the latter.<br />
Discussion<br />
Because <strong>of</strong> its relatively large sample size, rigorous exclusion <strong>of</strong> evidence <strong>of</strong> thyroid<br />
abnormality, <strong>and</strong> inclusion <strong>of</strong> calcium stimulation testing, the present study provides the most<br />
reliable <strong>and</strong> clinically relevant reference values for basal <strong>and</strong> stimulated serum hCT<br />
concentrations in healthy adults obtained to date via automated chemiluminescent assay. Our<br />
reference range for basal hCT agrees <strong>with</strong> Leboulleux et al.’s description <strong>of</strong> “normal” adult<br />
circulating hCT levels as
versa. Similar findings in healthy subjects were noted by Gharib et al. (14), who used a<br />
different calcium infusion regimen (2mg/kg over 5 min) than ours <strong>and</strong> injected pentagastrin as<br />
a bolus. However, in that study, pentagastrin provided more potent stimulation than did<br />
calcium in a 12-person subgroup <strong>of</strong> thyroidectomized MTC patients (14). Additionally,<br />
Costante et al. reported that a 30-second infusion <strong>of</strong> calcium gluconate, 2.5 mg/kg, was<br />
equally effective as pentagastrin in identifying patients <strong>with</strong> C-cell hyperplasia or MTC (3).<br />
Therefore the impact <strong>of</strong> the calcium regimen <strong>and</strong> the comparative efficacy <strong>of</strong> the two agents<br />
in clinical practice remain unclear. Additional trials investigating hCT levels in patients <strong>with</strong><br />
thyroid abnormalities, such as multinodular goiter <strong>and</strong> autoimmune thyroiditis, <strong>and</strong> MTC<br />
patients are necessary to resolve these issues <strong>and</strong> define appropriate cut-<strong>of</strong>f values for disease.<br />
In line <strong>with</strong> previous observations, virtually all subjects reported greater transient<br />
discomfort <strong>of</strong> varying intensity after pentagastrin than after calcium (3, 17, 18).<br />
This study had several limitations. Since all subjects underwent pentagastrin<br />
stimulation before calcium stimulation, a sequencing effect was possible; however, the<br />
months-long wash-out between stimulation tests renders this unlikely. The wash-out’s length,<br />
however, may have contributed to the loss to follow-up <strong>of</strong> an appreciable portion (16%) <strong>of</strong><br />
subjects, which may have introduced bias into the comparison <strong>of</strong> the stimulation agents.<br />
Additionally, the study included no elderly subjects or MTC patients.<br />
Conclusions<br />
In healthy young to middle-aged adults, calcium seems to be a more potent <strong>and</strong><br />
better-tolerated hCT stimulator than is pentagastrin. The reference ranges for basal <strong>and</strong><br />
stimulated hCT for healthy adults established via automated chemiluminescent assay were<br />
lower than those reported for other assays. Gender-based cut-<strong>of</strong>fs may be unnecessary for<br />
unstimulated, but necessary for stimulated hCT testing.<br />
Acknowledgements<br />
We thank Petra Völcker, Werner Kühnel <strong>and</strong> Robert Marlowe for their assistance.<br />
8
References<br />
1. Hahm JR, Lee MS, Min YK, Lee MK, Kim KW, Nam SJ, Yang JH, Chung JH<br />
2001 Routine measurement <strong>of</strong> serum calcitonin is useful for early detection <strong>of</strong><br />
medullary thyroid carcinoma in patients <strong>with</strong> nodular thyroid diseases. Thyroid<br />
11:73-80<br />
2. Elisei R, Bottici V, Luchetti F, Di Coscio G, Romei C, Grasso L, Miccoli P,<br />
Iacconi P, Basolo F, Pinchera A, Pacini F 2004 Impact <strong>of</strong> routine measurement <strong>of</strong><br />
serum calcitonin on the diagnosis <strong>and</strong> outcome <strong>of</strong> medullary thyroid cancer:<br />
experience in 10,864 patients <strong>with</strong> nodular thyroid disorders. J Clin Endocrinol Metab<br />
89:163-8<br />
3. Costante G, Meringolo D, Durante C, Bianchi D, Nocera M, Tumino S, Crocetti<br />
U, Attard M, Maranghi M, Torlontano M, Filetti S 2007 Predictive value <strong>of</strong> serum<br />
calcitonin levels for preoperative diagnosis <strong>of</strong> medullary thyroid carcinoma in a<br />
cohort <strong>of</strong> 5817 consecutive patients <strong>with</strong> thyroid nodules. J Clin Endocrinol Metab<br />
92:450-5<br />
4. Machens A, Hauptmann S, Dralle H 2008 Medullary thyroid cancer responsiveness<br />
to pentagastrin stimulation: an early surrogate parameter <strong>of</strong> tumor dissemination? J<br />
Clin Endocrinol Metab 93:2234-8<br />
5. Pacini F, Schlumberger M, Dralle H, Elisei R, Smit JW, Wiersinga W 2006<br />
European consensus for the management <strong>of</strong> patients <strong>with</strong> differentiated thyroid<br />
carcinoma <strong>of</strong> the follicular epithelium. Eur J Endocrinol 154:787-803<br />
6. Demers LM, Spencer CA 2003 Laboratory medicine practice guidelines: laboratory<br />
support for the diagnosis <strong>and</strong> monitoring <strong>of</strong> thyroid disease. Clin Endocrinol (Oxf)<br />
58:138-40<br />
7. Karanikas G, Moameni A, Poetzi C, Zettinig G, Kaserer K, Bieglmayer C,<br />
Niederle B, Dudczak R, Pirich C 2004 Frequency <strong>and</strong> relevance <strong>of</strong> elevated<br />
calcitonin levels in patients <strong>with</strong> neoplastic <strong>and</strong> nonneoplastic thyroid disease <strong>and</strong> in<br />
healthy subjects. J Clin Endocrinol Metab 89:515-9<br />
8. Vierhapper H, Niederle B, Bieglmayer C, Kaserer K, Baumgartner-Parzer S<br />
2005 Early diagnosis <strong>and</strong> curative therapy <strong>of</strong> medullary thyroid carcinoma by routine<br />
measurement <strong>of</strong> serum calcitonin in patients <strong>with</strong> thyroid disorders. Thyroid 15:1267-<br />
72<br />
9. Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, M<strong>and</strong>el SJ,<br />
Mazzaferri EL, McIver B, Sherman SI, Tuttle RM 2006 Management guidelines<br />
for patients <strong>with</strong> thyroid nodules <strong>and</strong> differentiated thyroid cancer. Thyroid 16:109-42<br />
10. Cheung K, Roman SA, Wang TS, Walker HD, Sosa JA 2008 <strong>Calcitonin</strong><br />
measurement in the evaluation <strong>of</strong> thyroid nodules in the United States: a costeffectiveness<br />
<strong>and</strong> decision analysis. J Clin Endocrinol Metab 93:2173-80<br />
11. Wion-Barbot N, Schuffenecker I, Niccoli P, Conte-Devolx B, Lecomte P,<br />
Houdent C, Bigorgne JC, Modigliani E 1997 Results <strong>of</strong> the calcitonin stimulation<br />
test in normal volunteers compared <strong>with</strong> genetically unaffected members <strong>of</strong> MEN 2A<br />
<strong>and</strong> familial medullary thyroid carcinoma families. Ann Endocrinol (Paris) 58:302-8<br />
12. Hodak SP, Burman KD 2004 The calcitonin conundrum--is it time for routine<br />
measurement <strong>of</strong> serum calcitonin in patients <strong>with</strong> thyroid nodules? J Clin Endocrinol<br />
Metab 89:511-4<br />
13. Wells SA, Jr., Baylin SB, Linehan WM, Farrell RE, Cox EB, Cooper CW 1978<br />
Provocative agents <strong>and</strong> the diagnosis <strong>of</strong> medullary carcinoma <strong>of</strong> the thyroid gl<strong>and</strong>.<br />
Ann Surg 188:139-41<br />
14. Gharib H, Kao PC, Heath H, 3rd 1987 Determination <strong>of</strong> silica-purified plasma<br />
calcitonin for the detection <strong>and</strong> management <strong>of</strong> medullary thyroid carcinoma:<br />
comparison <strong>of</strong> two provocative tests. Mayo Clin Proc 62:373-8<br />
15. Gimm O, Sutter T, Dralle H 2001 Diagnosis <strong>and</strong> therapy <strong>of</strong> sporadic <strong>and</strong> familial<br />
9
medullary thyroid carcinoma. J Cancer Res Clin Oncol 127:156-65<br />
16. Bieglmayer C, Vierhapper H, Dudczak R, Niederle B 2007 Measurement <strong>of</strong><br />
calcitonin by immunoassay analyzers. Clin Chem Lab Med 45:662-6<br />
17. Leboulleux S, Baudin E, Travagli JP, Schlumberger M 2004 Medullary thyroid<br />
carcinoma. Clin Endocrinol (Oxf) 61:299-310<br />
18. Vitale G, Ciccarelli A, Caraglia M, Galderisi M, Rossi R, Del Prete S,<br />
Abbruzzese A, Lupoli G 2002 Comparison <strong>of</strong> two provocative tests for calcitonin in<br />
medullary thyroid carcinoma: omeprazole vs pentagastrin. Clin Chem 48:1505-10<br />
19. d'Herbomez M, Caron P, Bauters C, Cao CD, Schlienger JL, Sapin R, Baldet L,<br />
Carnaille B, Wemeau JL 2007 Reference range <strong>of</strong> serum calcitonin levels in<br />
humans: influence <strong>of</strong> calcitonin assays, sex, age, <strong>and</strong> cigarette smoking. Eur J<br />
Endocrinol 157:749-55<br />
20. Guyetant S, Rousselet MC, Durigon M, Chappard D, Franc B, Guerin O, Saint-<br />
Andre JP 1997 Sex-related C cell hyperplasia in the normal human thyroid: a<br />
quantitative autopsy study. J Clin Endocrinol Metab 82:42-7<br />
10
Tables<br />
Table 1. Subject characteristics at study entry <strong>and</strong> clinical side effects <strong>of</strong> pentagastrin <strong>and</strong><br />
calcium. FT3, free triiodothyronine; FT4, free thyroxine; SD, st<strong>and</strong>ard deviation;<br />
TSH, thyroid-stimulating hormone<br />
Characteristic Value<br />
Females, n (%) 25 (50%)<br />
Age, yr, mean ± SD (range) 33.1 ± 9.7 (23 - 57)<br />
Body mass index, kg/m², mean ± SD (range) 22.8 ± 3.0 (18.1- 33.1)<br />
Thyroid volume by ultrasound, mL, mean ± SD<br />
(normal range)<br />
11.0 ± 5.0 (5.0 - 24.0)<br />
TSH, mIU/L, mean ± SD (normal range) 1.6 ± 0.6 (0.3 - 4.0)<br />
FT3, pmol/mL, mean ± SD (normal range) 4.4 ± 0.7 (2.7 - 7.6)<br />
FT4, pmol/mL, mean ± SD (normal range) 17.6 ± 2.1 (11.0 – 23.0)<br />
Thyroperoxidase autoantibody titers, mean<br />
(normal range)<br />
Thyroglobulin autoantibody titers, mean (normal<br />
range)<br />
7.0 (0 - 100)<br />
20.6 (0 – 100)<br />
Calcium, mmol/L, mean ± SD (normal range) 2.4 ± 0.1 (2.0 - 2.7)<br />
Pentagastrin side effects (N = 50), incidence, %<br />
Retro/Substernal tightness / abdominal cramping<br />
Extremity paresthesia<br />
Feeling <strong>of</strong> warmth<br />
Dizziness<br />
Nausea, urge to micturate, salty metallic taste<br />
Pentagastrin side effect duration<br />
94%<br />
74%<br />
30%<br />
12%<br />
a few subjects each<br />
1-2 min<br />
11
Calcium side effects (n = 42), incidence, %<br />
Temporary flushing, feeling <strong>of</strong> warmth<br />
Facial paresthesia, altered gustatory sensation<br />
98%<br />
20%<br />
Calcium side effects duration up to 15 min<br />
12
Figure Legends<br />
Figure 1. Serum calcitonin values in male versus female healthy adults at baseline (Panels A<br />
<strong>and</strong> B), after pentagastrin stimulation (Panel A) (n = 50) or after calcium stimulation (Panel<br />
B) (n = 42). The central box represents the values from the lower to upper quartile (25th to<br />
75th percentile). The middle line represents the median. The vertical line extends from the<br />
minimum to the maximum values, excluding outlier <strong>and</strong> far outlier values, which are<br />
displayed as separate points. Outlier values are defined as being larger than the upper quartile<br />
plus 1.5 times the interquartile range; far outlier values are defined as being larger than the<br />
upper quartile plus 3 times the interquartile range. Panel C represents the relationship between<br />
the maximum pentagastrin- <strong>and</strong> calcium-stimulated hCT levels (Spearmans’ rho = 0.758, P <<br />
0.001).<br />
13
<strong>Calcitonin</strong> (pg/ml)<br />
A) Pentagastrin stimulation ― 95th percentile maximal stimulated hCT values (2 min*):<br />
60<br />
50<br />
40<br />
30<br />
20<br />
10<br />
0<br />
in men 37.8 pg/ml; in women 26.2 pg/ml<br />
m f m f m f m f<br />
basal 2 min * 5 min * 15 min *<br />
* after pentagastrin-injection
<strong>Calcitonin</strong> (pg/ml)<br />
B) Calcium stimulation ― 95th percentile maximal stimulated hCT values (2 min*):<br />
260<br />
240<br />
220<br />
200<br />
180<br />
160<br />
140<br />
120<br />
100<br />
80<br />
60<br />
40<br />
20<br />
0<br />
in men 131.1 pg/ml (95.4 pg/ml); in women 90.2 pg/ml<br />
m f m f m f m f<br />
basal 2 min * 5 min * 15 min *<br />
* after calcium-injection
C) Maximum calcium- vs. pentagastrin-stimulated hCT-levels