ESC Guidelines on the diagnosis and treatment of peripheral artery ...
ESC Guidelines on the diagnosis and treatment of peripheral artery ...
ESC Guidelines on the diagnosis and treatment of peripheral artery ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Page 14 <strong>of</strong> 56<br />
4.1.1.4.1 Asymptomatic carotid <strong>artery</strong> disease<br />
4.1.1.4.1.1 Surgery<br />
A total <strong>of</strong> 5233 patients with asymptomatic carotid <strong>artery</strong><br />
disease were enrolled in r<strong>and</strong>omized multicentre trials comparing<br />
CEA with medical management. 53,54,66,81 After 4657 patientyears<br />
<strong>of</strong> follow-up, <strong>the</strong> r<strong>and</strong>omized Asymptomatic Carotid<br />
A<strong>the</strong>rosclerosis Study (ACAS) estimated <strong>the</strong> 30-m<strong>on</strong>th risk <strong>of</strong><br />
ipsilateral stroke in <strong>the</strong> case <strong>of</strong> carotid <strong>artery</strong> stenosis .60%<br />
at 5.1% for patients who underwent CEA in additi<strong>on</strong> to best<br />
medical <strong>the</strong>rapy (at that time) vs. 11.0% for those with best<br />
medical <strong>the</strong>rapy al<strong>on</strong>e. 53 The Asymptomatic Carotid Surgery<br />
Trial (ACST) r<strong>and</strong>omized 3120 asymptomatic patients to ei<strong>the</strong>r<br />
immediate CEA or indefinite deferral <strong>of</strong> CEA. 54 The 5-year risks<br />
were 6.4% vs. 11.8% for all strokes (absolute risk reducti<strong>on</strong><br />
5.4%, P ¼ 0.0001), 3.5% vs. 6.1% for fatal or disabling stroke<br />
(absolute risk reducti<strong>on</strong> 2.6%, P ¼ 0.004), <strong>and</strong> 2.1% vs. 4.2% for<br />
fatal strokes (absolute risk reducti<strong>on</strong> 2.1%, P ¼ 0.006), respectively.<br />
Combining perioperative events <strong>and</strong> strokes, net risks<br />
were 6.9% vs. 10.9% at 5 years (gain 4.1%, 2.0–6.2) <strong>and</strong> 13.4%<br />
vs. 17.9% at 10 years (gain 4.6%, 1.2–7.9). 66 Medicati<strong>on</strong> was<br />
similar in both groups; throughout <strong>the</strong> study, most patients were<br />
<strong>on</strong> antithrombotic <strong>and</strong> antihypertensive <strong>the</strong>rapy. Net benefits<br />
were significant irrespective <strong>of</strong> <strong>the</strong> use <strong>of</strong> lipid-lowering <strong>the</strong>rapy,<br />
for men <strong>and</strong> women under <strong>the</strong> age <strong>of</strong> 75 years at entry. In <strong>the</strong><br />
three trials, <strong>the</strong> benefit was greater in men than in women, but<br />
<strong>the</strong> number <strong>of</strong> women enrolled was low.<br />
It can be c<strong>on</strong>cluded that CEA is beneficial in asymptomatic<br />
patients (especially men) between 40 <strong>and</strong> 75 years <strong>of</strong> age with<br />
.60% stenosis, if <strong>the</strong>ir life expectancy is .5 years <strong>and</strong> operative<br />
mortality ,3%. 66,70 – 77,79,81 However, <strong>the</strong> absolute benefit <strong>of</strong><br />
revascularizati<strong>on</strong> in terms <strong>of</strong> stroke preventi<strong>on</strong> is small (1–2%<br />
per year), <strong>and</strong> those trials were performed prior to extensive<br />
use <strong>of</strong> statins. Therefore, <strong>the</strong> benefit <strong>of</strong> revascularizati<strong>on</strong> <strong>on</strong> top<br />
<strong>of</strong> optimal medical management should be reassessed.<br />
4.1.1.4.1.2 Endovascular <strong>the</strong>rapy<br />
The results <strong>of</strong> eight CAS registries enrolling .1000 patients<br />
have been published recently (Table 3). 82 The registries included<br />
.20 000 patients at high surgical risk, mainly asymptomatic. Pre<strong>and</strong><br />
post-procedure neurological assessment <strong>and</strong> blinded event adjudicati<strong>on</strong><br />
were required in most studies. Overall, <strong>the</strong> studies dem<strong>on</strong>strated<br />
that death <strong>and</strong> stroke rates with CAS are in <strong>the</strong> range<br />
expected in current recommendati<strong>on</strong>s for CEA even in patients at<br />
high surgical risk, <strong>and</strong> that CAS results tend to improve over time.<br />
So far, <strong>the</strong> r<strong>and</strong>omized evidence for CAS in asymptomatic<br />
patients is limited. While no study has compared endovascular<br />
<strong>treatment</strong> with medical <strong>the</strong>rapy, two trials (SAPPHIRE <strong>and</strong><br />
CREST) comparing CAS vs. CEA have also enrolled asymptomatic<br />
patients (for details see Secti<strong>on</strong> 4.1.1.4.2.2).<br />
4.1.1.4.2 Symptomatic carotid <strong>artery</strong> disease<br />
It should be emphasized that neurological assessment <strong>and</strong> appropriate<br />
<strong>treatment</strong> should be proposed as so<strong>on</strong> as possible after <strong>the</strong> index<br />
event. At a very minimum patients need to be seen <strong>and</strong> treated<br />
within 2 weeks, with important benefit <strong>of</strong> instituting medical <strong>treatment</strong><br />
88 <strong>and</strong> performing revascularizati<strong>on</strong> as so<strong>on</strong> as possible after<br />
<strong>the</strong> <strong>on</strong>set <strong>of</strong> symptoms. 89,90<br />
4.1.1.4.2.1 Surgery<br />
Pooled data from <strong>the</strong> NASCET, <strong>the</strong> European Carotid Surgery<br />
Trial (ECST), <strong>and</strong> <strong>the</strong> Veterans Affairs Trial included .35 000<br />
patient-years <strong>of</strong> follow-up in patients (28% women) with symptomatic<br />
disease. 50,51,91,92 CEA increased <strong>the</strong> 5-year risk <strong>of</strong> ipsilateral<br />
ischaemic stroke over medical <strong>the</strong>rapy al<strong>on</strong>e in patients with<br />
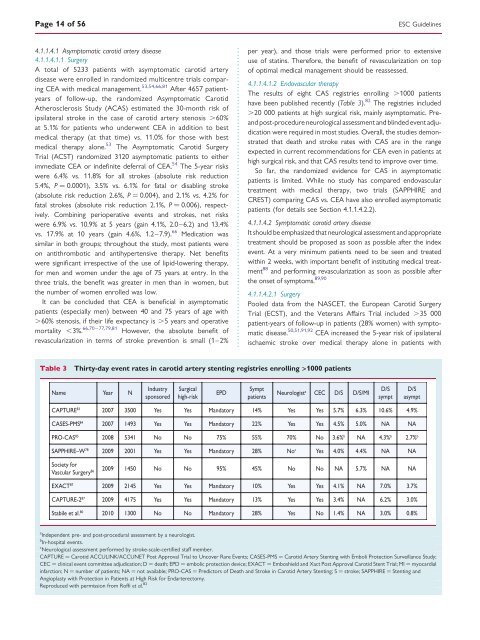
Table 3 Thirty-day event rates in carotid <strong>artery</strong> stenting registries enrolling >1000 patients<br />
Name Year N<br />
Industry<br />
sp<strong>on</strong>sored<br />
Surgical<br />
high-risk<br />
EPD<br />
Sympt<br />
patients<br />
Neurologist a CEC D/S D/S/MI<br />
CAPTURE 83 2007 3500 Yes Yes M<strong>and</strong>atory 14% Yes Yes 5.7% 6.3% 10.6% 4.9%<br />
CASES-PMS 84 2007 1493 Yes Yes M<strong>and</strong>atory 22% Yes Yes 4.5% 5.0% NA NA<br />
PRO-CAS 85 2008 5341 No No 75% 55% 70% No 3.6% b NA 4.3% b 2.7% b<br />
SAPPHIRE–W 78 2009 2001 Yes Yes M<strong>and</strong>atory 28% No c Yes 4.0% 4.4% NA NA<br />
Society for<br />
Vascular Surgery 86 2009 1450 No No 95% 45% No No NA 5.7% NA NA<br />
EXACT 87 2009 2145 Yes Yes M<strong>and</strong>atory 10% Yes Yes 4.1% NA 7.0% 3.7%<br />
CAPTURE-2 87 2009 4175 Yes Yes M<strong>and</strong>atory 13% Yes Yes 3.4% NA 6.2% 3.0%<br />
Stabile et al. 80 2010 1300 No No M<strong>and</strong>atory 28% Yes No 1.4% NA 3.0% 0.8%<br />
a<br />
Independent pre- <strong>and</strong> post-procedural assessment by a neurologist.<br />
b<br />
In-hospital events.<br />
c<br />
Neurological assessment performed by stroke-scale-certified staff member.<br />
CAPTURE ¼ Carotid ACCULINK/ACCUNET Post Approval Trial to Uncover Rare Events; CASES-PMS ¼ Carotid Artery Stenting with Emboli Protecti<strong>on</strong> Surveillance Study;<br />
CEC ¼ clinical event committee adjudicati<strong>on</strong>; D ¼ death; EPD ¼ embolic protecti<strong>on</strong> device; EXACT ¼ Emboshield <strong>and</strong> Xact Post Approval Carotid Stent Trial; MI ¼ myocardial<br />
infarcti<strong>on</strong>; N ¼ number <strong>of</strong> patients; NA ¼ not available; PRO-CAS ¼ Predictors <strong>of</strong> Death <strong>and</strong> Stroke in Carotid Artery Stenting; S ¼ stroke; SAPPHIRE ¼ Stenting <strong>and</strong><br />
Angioplasty with Protecti<strong>on</strong> in Patients at High Risk for Endarterectomy.<br />
Reproduced with permissi<strong>on</strong> from R<strong>of</strong>fi et al. 82<br />
D/S<br />
sympt<br />
<str<strong>on</strong>g>ESC</str<strong>on</strong>g> <str<strong>on</strong>g>Guidelines</str<strong>on</strong>g><br />
D/S<br />
asympt