ESC Guidelines on the diagnosis and treatment of peripheral artery ...
ESC Guidelines on the diagnosis and treatment of peripheral artery ...
ESC Guidelines on the diagnosis and treatment of peripheral artery ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Page 26 <strong>of</strong> 56<br />
c<strong>on</strong>sidered. 243 However, even in this situati<strong>on</strong>, DUS can be an<br />
important aid in determining <strong>the</strong> most appropriate site <strong>of</strong> anastomosis<br />
by identificati<strong>on</strong> <strong>of</strong> <strong>the</strong> least calcified porti<strong>on</strong> <strong>of</strong> <strong>the</strong> vessel. 244<br />
Intravascular ultrasound has been proposed for plaque characterizati<strong>on</strong><br />
<strong>and</strong> after angioplasty, but its routine role in <strong>the</strong> clinical<br />
setting requires fur<strong>the</strong>r investigati<strong>on</strong>.<br />
4.5.2.4 Computed tomography angiography<br />
CTA using MDCT technology allows imaging with high resoluti<strong>on</strong>.<br />
Compared with DSA, <strong>the</strong> sensitivity <strong>and</strong> specificity for occlusi<strong>on</strong>s<br />
reported using <strong>the</strong> single-detector techniques already reached a<br />
high degree <strong>of</strong> accuracy. In a recent meta-analysis, <strong>the</strong> reported<br />
sensitivity <strong>and</strong> specificity <strong>of</strong> CTA to detect aortoiliac stenoses<br />
.50% were 96% <strong>and</strong> 98%, respectively. 245 The same study<br />
showed similar sensitivity (97%) <strong>and</strong> specificity (94%) for <strong>the</strong><br />
femoropopliteal regi<strong>on</strong>, comparable with those reported for <strong>the</strong><br />
below-knee arteries (sensitivity 95%, specificity 91%). 245<br />
The great advantage <strong>of</strong> CTA remains <strong>the</strong> visualizati<strong>on</strong> <strong>of</strong> calcificati<strong>on</strong>s,<br />
clips, stents, <strong>and</strong> bypasses. However, some artefacts may<br />
be present due to <strong>the</strong> ‘blooming effect’.<br />
4.5.2.5 Magnetic res<strong>on</strong>ance angiography<br />
MRA can n<strong>on</strong>-invasively visualize <strong>the</strong> lower limb arteries even in<br />
<strong>the</strong> most distal parts. The resoluti<strong>on</strong> <strong>of</strong> MRA using<br />
gadolinium-enhanced c<strong>on</strong>trast techniques reaches that <strong>of</strong> DSA. In<br />
comparis<strong>on</strong> with DSA, MRA has an excellent sensitivity (93–<br />
100%) <strong>and</strong> specificity (93–100%). 237,246 – 250 Owing to different<br />
techniques (2D <strong>and</strong> 3D, with or without gadolinium), <strong>the</strong> results<br />
are not as uniform as for CTA, <strong>and</strong> studies comparing MRA with<br />
CTA are not available. In direct comparis<strong>on</strong>, MRA has <strong>the</strong> greatest<br />
ability to replace diagnostic DSA in symptomatic patients to assist<br />
decisi<strong>on</strong> making, especially in <strong>the</strong> case <strong>of</strong> major allergies. There are<br />
also limitati<strong>on</strong>s for <strong>the</strong> use <strong>of</strong> MRA in <strong>the</strong> presence <strong>of</strong> pacemakers<br />
or metal implants (including stents), or in patients with claustrophobia.<br />
Gadolinium c<strong>on</strong>trast agents cannot be used in <strong>the</strong> case<br />
<strong>of</strong> severe renal failure (GFR ,30 mL/min per 1.73 m 2 ). Of note,<br />
MRA cannot visualize arterial calcificati<strong>on</strong>s, which may be a limitati<strong>on</strong><br />
for <strong>the</strong> selecti<strong>on</strong> <strong>of</strong> <strong>the</strong> anastomotic site for a surgical bypass.<br />
4.5.2.6 Digital subtracti<strong>on</strong> angiography<br />
For <strong>the</strong> aorta <strong>and</strong> <strong>peripheral</strong> arteries, retrograde transfemoral ca<strong>the</strong>terizati<strong>on</strong><br />
is usually used. Cross-over techniques allow <strong>the</strong> direct<br />
antegrade flow imaging from <strong>on</strong>e side to <strong>the</strong> o<strong>the</strong>r. If <strong>the</strong> femoral<br />
access is not possible, transradial or transbrachial approaches <strong>and</strong><br />
direct antegrade ca<strong>the</strong>terizati<strong>on</strong> are needed. C<strong>on</strong>sidered as <strong>the</strong><br />
gold st<strong>and</strong>ard for decades, DSA is now reserved for patients undergoing<br />
interventi<strong>on</strong>s, especially c<strong>on</strong>comitant to endovascular procedures.<br />
Indeed, <strong>the</strong> n<strong>on</strong>-invasive techniques provide satisfying<br />
imaging in almost all cases, with less radiati<strong>on</strong>, <strong>and</strong> avoiding complicati<strong>on</strong>s<br />
inherent to <strong>the</strong> arterial puncture, reported in ,1% <strong>of</strong> cases.<br />
4.5.2.7 O<strong>the</strong>r tests<br />
Several o<strong>the</strong>r n<strong>on</strong>-invasive tests can be used routinely, ei<strong>the</strong>r to<br />
localize <strong>the</strong> lesi<strong>on</strong>s or to evaluate <strong>the</strong>ir effect <strong>on</strong> limb perfusi<strong>on</strong>:<br />
segmental pressure measurements <strong>and</strong> pulse volume recordings,<br />
251<br />
(laser) Doppler flowmetry, transcutaneous oxygen<br />
pressure assessment (TCPO2), <strong>and</strong> venous occlusi<strong>on</strong> plethysmography<br />
before <strong>and</strong> during reactive hyperaemia. 252<br />
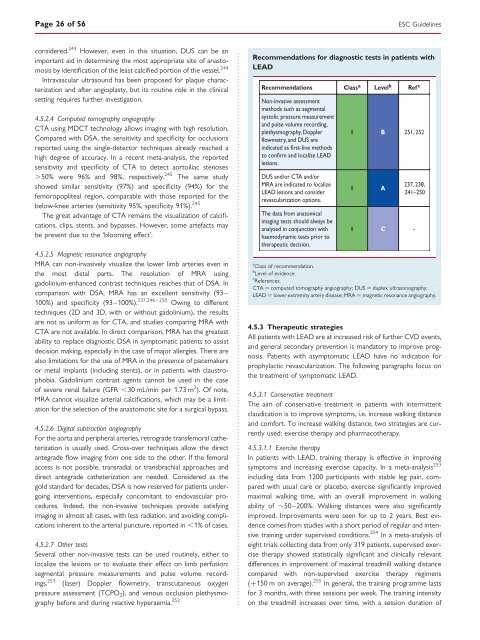
Recommendati<strong>on</strong>s for diagnostic tests in patients with<br />
LEAD<br />
Recommendati<strong>on</strong>s Class a Level b Ref c<br />
N<strong>on</strong>-invasive assessment<br />
methods such as segmental<br />
systolic pressure measurement<br />
<strong>and</strong> pulse volume recording,<br />
plethysmography, Doppler<br />
flowmetry, <strong>and</strong> DUS are<br />
indicated as first-line methods<br />
to c<strong>on</strong>firm <strong>and</strong> localize LEAD<br />
lesi<strong>on</strong>s.<br />
DUS <strong>and</strong>/or CTA <strong>and</strong>/or<br />
MRA are indicated to localize<br />
LEAD lesi<strong>on</strong>s <strong>and</strong> c<strong>on</strong>sider<br />
revascularizati<strong>on</strong> opti<strong>on</strong>s.<br />
The data from anatomical<br />
imaging tests should always be<br />
analysed in c<strong>on</strong>juncti<strong>on</strong> with<br />
haemodynamic tests prior to<br />
<strong>the</strong>rapeutic decisi<strong>on</strong>.<br />
I B 251, 252<br />
I A<br />
237, 238,<br />
241–250<br />
I C -<br />
<str<strong>on</strong>g>ESC</str<strong>on</strong>g> <str<strong>on</strong>g>Guidelines</str<strong>on</strong>g><br />
a<br />
Class <strong>of</strong> recommendati<strong>on</strong>.<br />
b<br />
Level <strong>of</strong> evidence.<br />
c<br />
References.<br />
CTA ¼ computed tomography angiography; DUS ¼ duplex ultras<strong>on</strong>ography;<br />
LEAD ¼ lower extremity <strong>artery</strong> disease; MRA ¼ magnetic res<strong>on</strong>ance angiography.<br />
4.5.3 Therapeutic strategies<br />
All patients with LEAD are at increased risk <strong>of</strong> fur<strong>the</strong>r CVD events,<br />
<strong>and</strong> general sec<strong>on</strong>dary preventi<strong>on</strong> is m<strong>and</strong>atory to improve prognosis.<br />
Patients with asymptomatic LEAD have no indicati<strong>on</strong> for<br />
prophylactic revascularizati<strong>on</strong>. The following paragraphs focus <strong>on</strong><br />
<strong>the</strong> <strong>treatment</strong> <strong>of</strong> symptomatic LEAD.<br />
4.5.3.1 C<strong>on</strong>servative <strong>treatment</strong><br />
The aim <strong>of</strong> c<strong>on</strong>servative <strong>treatment</strong> in patients with intermittent<br />
claudicati<strong>on</strong> is to improve symptoms, i.e. increase walking distance<br />
<strong>and</strong> comfort. To increase walking distance, two strategies are currently<br />
used: exercise <strong>the</strong>rapy <strong>and</strong> pharmaco<strong>the</strong>rapy.<br />
4.5.3.1.1 Exercise <strong>the</strong>rapy<br />
In patients with LEAD, training <strong>the</strong>rapy is effective in improving<br />
symptoms <strong>and</strong> increasing exercise capacity. In a meta-analysis 253<br />
including data from 1200 participants with stable leg pain, compared<br />
with usual care or placebo, exercise significantly improved<br />
maximal walking time, with an overall improvement in walking<br />
ability <strong>of</strong> ≏50–200%. Walking distances were also significantly<br />
improved. Improvements were seen for up to 2 years. Best evidence<br />
comes from studies with a short period <strong>of</strong> regular <strong>and</strong> intensive<br />
training under supervised c<strong>on</strong>diti<strong>on</strong>s. 254 In a meta-analysis <strong>of</strong><br />
eight trials collecting data from <strong>on</strong>ly 319 patients, supervised exercise<br />
<strong>the</strong>rapy showed statistically significant <strong>and</strong> clinically relevant<br />
differences in improvement <strong>of</strong> maximal treadmill walking distance<br />
compared with n<strong>on</strong>-supervised exercise <strong>the</strong>rapy regimens<br />
(+150 m <strong>on</strong> average). 255 In general, <strong>the</strong> training programme lasts<br />
for 3 m<strong>on</strong>ths, with three sessi<strong>on</strong>s per week. The training intensity<br />
<strong>on</strong> <strong>the</strong> treadmill increases over time, with a sessi<strong>on</strong> durati<strong>on</strong> <strong>of</strong>