ESC Guidelines on the diagnosis and treatment of peripheral artery ...
ESC Guidelines on the diagnosis and treatment of peripheral artery ...
ESC Guidelines on the diagnosis and treatment of peripheral artery ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Page 24 <strong>of</strong> 56<br />
In more severe cases pain is present at rest, in <strong>the</strong> supine positi<strong>on</strong><br />
(F<strong>on</strong>taine stage III; Ru<strong>the</strong>rford grade II). Rest pain is localized more<br />
<strong>of</strong>ten in <strong>the</strong> foot <strong>and</strong> should be distinguished from muscle cramping<br />
or arthritis. Patients <strong>of</strong>ten complain <strong>of</strong> permanent coldness in <strong>the</strong><br />
feet. Ulcers <strong>and</strong> gangrene (F<strong>on</strong>taine stage IV; Ru<strong>the</strong>rford grade III)<br />
indicate severe ischaemia <strong>and</strong> begin mostly at <strong>the</strong> level <strong>of</strong> toes <strong>and</strong><br />
<strong>the</strong> distal part <strong>of</strong> <strong>the</strong> limb. Arterial ulcers are, in most cases, extremely<br />
painful; <strong>the</strong>y are frequently sec<strong>on</strong>dary to local trauma, even<br />
minor, <strong>and</strong> should be distinguished from venous ulcers. When pain<br />
is absent, <strong>peripheral</strong> neuropathy should be c<strong>on</strong>sidered. Ulcers are<br />
<strong>of</strong>ten complicated by local infecti<strong>on</strong> <strong>and</strong> inflammati<strong>on</strong>.<br />
Critical limb ischaemia is <strong>the</strong> most severe clinical manifestati<strong>on</strong><br />
<strong>of</strong> LEAD, defined as <strong>the</strong> presence <strong>of</strong> ischaemic rest pain, <strong>and</strong><br />
Table 5 Clinical staging <strong>of</strong> LEAD<br />
F<strong>on</strong>taine<br />
classificati<strong>on</strong><br />
Ru<strong>the</strong>rford classificati<strong>on</strong><br />
Stage Symptoms Grade Category Symptoms<br />
I Asymptomatic 0 0 Asymptomatic<br />
II<br />
III<br />
IV<br />
Intermittent<br />
claudicati<strong>on</strong><br />
Ischaemic<br />
rest pain<br />
Ulcerati<strong>on</strong> or<br />
gangrene<br />
LEAD ¼ lower extremity <strong>artery</strong> disease.<br />
I 1<br />
I 2<br />
I 3<br />
II 4<br />
III 5<br />
III 6<br />
Mild<br />
claudicati<strong>on</strong><br />
Moderate<br />
claudicati<strong>on</strong><br />
Severe<br />
claudicati<strong>on</strong><br />
Ischaemic<br />
rest pain<br />
Minor tissue<br />
loss<br />
Major tissue<br />
loss<br />
<str<strong>on</strong>g>ESC</str<strong>on</strong>g> <str<strong>on</strong>g>Guidelines</str<strong>on</strong>g><br />
ischaemic lesi<strong>on</strong>s or gangrene objectively attributable to arterial<br />
occlusive disease.<br />
4.5.1.2 Clinical examinati<strong>on</strong><br />
Clinical examinati<strong>on</strong> can be quite informative both for screening<br />
<strong>and</strong> for <strong>diagnosis</strong>. Patients should be relaxed <strong>and</strong> acclimatized to<br />
<strong>the</strong> room temperature. Inspecti<strong>on</strong> may show pallor in more<br />
severe cases, sometimes at leg elevati<strong>on</strong>. Pulse palpati<strong>on</strong> is very<br />
informative for screening purposes <strong>and</strong> should be d<strong>on</strong>e systematically.<br />
Pulse aboliti<strong>on</strong> is a specific ra<strong>the</strong>r than a sensitive clinical sign.<br />
Auscultati<strong>on</strong> <strong>of</strong> bruits over <strong>the</strong> femoral <strong>artery</strong> at <strong>the</strong> groin <strong>and</strong><br />
more distally is also suggestive, but poorly sensitive. The value <strong>of</strong><br />
<strong>the</strong> clinical findings in patients with LEAD can be str<strong>on</strong>gly improved<br />
by measuring <strong>the</strong> ABI. The blue toe syndrome is characterized by a<br />
sudden cyanotic discolourati<strong>on</strong> <strong>of</strong> <strong>on</strong>e or more toes; it is usually<br />
due to embolic a<strong>the</strong>rosclerotic debris from <strong>the</strong> proximal arteries.<br />
4.5.2 Diagnostic tests<br />
4.5.2.1 Ankle–brachial index<br />
The primary n<strong>on</strong>-invasive test for <strong>the</strong> <strong>diagnosis</strong> <strong>of</strong> LEAD is <strong>the</strong> ABI.<br />
In healthy pers<strong>on</strong>s, <strong>the</strong> ABI is .1.0. Usually an ABI ,0.90 is used<br />
to define LEAD. The actual sensitivity <strong>and</strong> specificity have been<br />
estimated, respectively, at 79% <strong>and</strong> 96%. 226 For <strong>diagnosis</strong> in<br />
primary care, an ABI ,0.8 or <strong>the</strong> mean <strong>of</strong> three ABIs ,0.90<br />
had a positive predictive value <strong>of</strong> ≥95%; an ABI .1.10 or <strong>the</strong><br />
mean <strong>of</strong> three ABIs .1.00 had a negative predictive value <strong>of</strong><br />
≥99%. 227 The level <strong>of</strong> ABI also correlates with LEAD severity,<br />
with high risk <strong>of</strong> amputati<strong>on</strong> when <strong>the</strong> ABI is ,0.50. An ABI<br />
change .0.15 is generally required to c<strong>on</strong>sider worsening <strong>of</strong><br />
limb perfusi<strong>on</strong> over time, or improving after revascularizati<strong>on</strong>. 228<br />
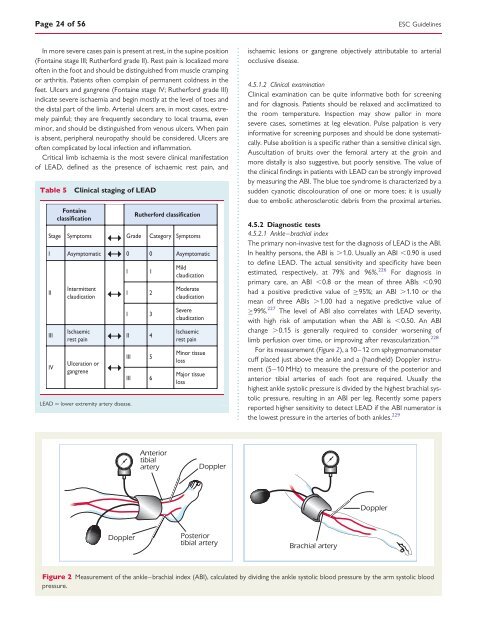
For its measurement (Figure 2), a 10–12 cm sphygmomanometer<br />
cuff placed just above <strong>the</strong> ankle <strong>and</strong> a (h<strong>and</strong>held) Doppler instrument<br />
(5–10 MHz) to measure <strong>the</strong> pressure <strong>of</strong> <strong>the</strong> posterior <strong>and</strong><br />
anterior tibial arteries <strong>of</strong> each foot are required. Usually <strong>the</strong><br />
highest ankle systolic pressure is divided by <strong>the</strong> highest brachial systolic<br />
pressure, resulting in an ABI per leg. Recently some papers<br />
reported higher sensitivity to detect LEAD if <strong>the</strong> ABI numerator is<br />
<strong>the</strong> lowest pressure in <strong>the</strong> arteries <strong>of</strong> both ankles. 229<br />
Figure 2 Measurement <strong>of</strong> <strong>the</strong> ankle–brachial index (ABI), calculated by dividing <strong>the</strong> ankle systolic blood pressure by <strong>the</strong> arm systolic blood<br />
pressure.