Design and Usability of a Home Telerehabilitation System to Train ...
Design and Usability of a Home Telerehabilitation System to Train ...
Design and Usability of a Home Telerehabilitation System to Train ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Design</strong> <strong>and</strong> <strong>Usability</strong> <strong>of</strong> a <strong>Home</strong> <strong>Telerehabilitation</strong> <strong>System</strong> <strong>to</strong> <strong>Train</strong><br />
H<strong>and</strong> Recovery Following Stroke<br />
William K. Durfee 1 , Samantha A. Weinstein 1 , James R. Carey 2 , Ela Bhatt 2 , <strong>and</strong> Ashima<br />
Nagpal 2<br />
1 2<br />
Department <strong>of</strong> Mechanical Engineering, Program in Physical Therapy, University <strong>of</strong><br />
Minnesota, Minneapolis USA<br />
Submitted <strong>to</strong> the Journal <strong>of</strong> Biomechanical Engineering (ASME), April 2006<br />
Address Correspondence <strong>to</strong>:<br />
William Durfee<br />
University <strong>of</strong> Minnesota<br />
111 Church ST S.E.<br />
Minneapolis, MN 55455<br />
tel: 612-625-0099<br />
email: wkdurfee@umn.edu<br />
Track-JBiomechEng.doc Page 1 <strong>of</strong> 31
ABSTRACT<br />
Current theories <strong>of</strong> stroke rehabilitation point <strong>to</strong>wards paradigms <strong>of</strong> intense, concentrated use<br />
<strong>of</strong> the afflicted limb as a means for mo<strong>to</strong>r program reorganization <strong>and</strong> partial function<br />
res<strong>to</strong>ration. Track<strong>Train</strong> is a home system for stroke rehabilitation that trains recovery <strong>of</strong> h<strong>and</strong><br />
function by a treatment <strong>of</strong> concentrated movement. A wearable goniometer measured finger<br />
<strong>and</strong> wrist motions in both h<strong>and</strong>s. An interface box transmitted sensor measurements in real-<br />
time <strong>to</strong> a lap<strong>to</strong>p computer. Stroke patients used joint motion <strong>to</strong> control the screen cursor in a<br />
one-dimensional tracking task for several hours a day over the course <strong>of</strong> 10 <strong>to</strong> 14 days <strong>to</strong><br />
complete a treatment <strong>of</strong> 1800 tracking trials. A tele-moni<strong>to</strong>ring component enabled a therapist<br />
<strong>to</strong> check in with the patient by video phone <strong>to</strong> moni<strong>to</strong>r progress, motivate the patient <strong>and</strong><br />
upload tracking data <strong>to</strong> a central file server. The system was designed for use at home by<br />
patients with no computer skills. Track<strong>Train</strong> was placed in the homes <strong>of</strong> 24 subjects with<br />
chronic stroke <strong>and</strong> impaired finger motion, ranging from two <strong>to</strong> 305 miles away from the<br />
clinic, plus one that was a distance <strong>of</strong> 1,057 miles. Fifteen subjects installed the system at<br />
home themselves after instruction in the clinic, nine required a home visit <strong>to</strong> install. Three<br />
required follow-up visits <strong>to</strong> fix equipment. A post treatment telephone survey was conducted<br />
<strong>to</strong> assess ease <strong>of</strong> use <strong>and</strong> most responded that the system was easy <strong>to</strong> use. Functional<br />
improvements were seen in the subjects enrolled in the formal treatment study, although the<br />
treatment period was <strong>to</strong> short <strong>to</strong> trigger cortical reorganization. We conclude that Track<strong>Train</strong><br />
is feasible for home use <strong>and</strong> that tracking training has promise as a treatment paradigm.<br />
Track-JBiomechEng.doc Page 2 <strong>of</strong> 31
1 INTRODUCTION<br />
Stroke is a major health problem. According <strong>to</strong> the American Heart Association (2005), in the<br />
United States, approximately 700,000 people suffer a first or recurrent stroke each year <strong>and</strong><br />
stroke is the third leading cause <strong>of</strong> death after heart disease <strong>and</strong> cancer. On average, every 45<br />
seconds, someone in the U.S. has a stroke. Stroke is the leading cause <strong>of</strong> serious, long-term<br />
disability. About 4.7 million stroke survivors are alive <strong>to</strong>day, <strong>and</strong> this number is increasing<br />
because <strong>of</strong> improved acute care. In 1999, more than 1.1 million adults reported difficulty with<br />
functional limitations resulting from stroke. The direct <strong>and</strong> indirect cost <strong>of</strong> stroke in 2005 was<br />
$56.8 billion.<br />
A common stroke disability is partial or complete paralysis <strong>of</strong> a limb, which leads <strong>to</strong><br />
impairment <strong>of</strong> basic functional skills in 75% <strong>of</strong> people with stroke (Jorgensen et al., 1999).<br />
One <strong>of</strong> the most debilitating limb impairment is paralysis <strong>of</strong> the h<strong>and</strong> (Hummelsheim et al.,<br />
1997; Nudo <strong>and</strong> Friel, 1999). Often, the individual will be able <strong>to</strong> close the fingers in<strong>to</strong> a fist,<br />
which is part <strong>of</strong> the characteristic spastic flexion synergy, but is unable <strong>to</strong> open the fingers<br />
because <strong>of</strong> extremely weak finger extensor muscles <strong>and</strong> spastic <strong>to</strong>ne in the antagonistic flexor<br />
muscles. As a result, the person cannot manipulate objects dexterously, which impairs<br />
feeding, dressing, h<strong>and</strong>writing, <strong>and</strong> occupational skills.<br />
Recent scientific findings fundamental <strong>to</strong> mo<strong>to</strong>r learning <strong>and</strong> neuroplasticity have challenged<br />
the traditional paradigms for mo<strong>to</strong>r rehabilitation following stroke. Functional loss in stroke<br />
occurs not only from cells that have died but also from reduced excitability in neurons that<br />
have survived the infarct (Feeney <strong>and</strong> Baron, 1986; Chu et al., 2002). The significance for<br />
rehabilitation is that there may be viable neurons available for recruitment in the stroke<br />
Track-JBiomechEng.doc Page 3 <strong>of</strong> 31
hemisphere, leading <strong>to</strong> the search for potent mechanisms that promote the res<strong>to</strong>ration <strong>of</strong><br />
voluntary recruitment <strong>of</strong> suppressed neurons. The literature is clear that movement retraining<br />
for stroke rehabilitation must be intense <strong>and</strong> must be prolonged <strong>and</strong> the patient must engage<br />
the task repeatedly <strong>and</strong> independently (Schmidt, 1988, Winstein et al., 1994). Importantly,<br />
self-improvement does not stem directly from the therapist coaching <strong>and</strong> guiding the activity;<br />
rather, improvement is thought <strong>to</strong> stem from internal information processing by the subject<br />
with consolidation <strong>of</strong> all the cues inherent <strong>to</strong> the task leading <strong>to</strong> a refined mo<strong>to</strong>r output<br />
(Winstein et al., 1994). Thus, subjects must be given opportunities <strong>to</strong> train themselves. The<br />
guiding <strong>and</strong> coaching efforts by therapists may be helpful in the short run but in the long run<br />
it will be the subject’s own information processing, including failed efforts, that will lead <strong>to</strong><br />
the cellular <strong>and</strong> molecular changes that stimulate mo<strong>to</strong>r learning/relearning <strong>and</strong> a fuller<br />
recovery.<br />
One example <strong>of</strong> modern therapy that is based on mo<strong>to</strong>r learning principles is constraint-<br />
induced movement therapy. CIMT forces the patient <strong>to</strong> use the paretic limb while the healthy<br />
limb is restrained <strong>and</strong> was designed <strong>to</strong> overcome learned nonuse <strong>of</strong> the impaired limb (Taub,<br />
1980). Clinical studies have shown CIMT <strong>to</strong> be effective for patients who start with some<br />
residual range-<strong>of</strong>-motion (Liepert et al., 2000; Page et al., 2004; Ploughman <strong>and</strong> Corbett,<br />
2004, Taub et al., 1993; Taub et al., 1999). CIMT requires massed practice (practice time is<br />
greater than rest time) for 6-7 hours daily for two weeks with continual therapist supervision<br />
(Taub, 2000).<br />
Forced-use such as CIMT, however, may not be the most potent behavioral stimulus for<br />
neuroplastic change. Forced-learning may be even more effective. This is a pivotal question<br />
in rehabilitation as it dictates the type <strong>of</strong> tasks <strong>and</strong> level <strong>of</strong> cognitive engagement that<br />
Track-JBiomechEng.doc Page 4 <strong>of</strong> 31
therapists select for training in subjects with stroke. Repetitive execution <strong>of</strong> simple mo<strong>to</strong>r<br />
tasks may not be as effective in re-training mo<strong>to</strong>r skills as complex mo<strong>to</strong>r tasks that involve<br />
in-depth cognitive processing (Carey et al., 2005). A joint-movement tracking training system<br />
<strong>to</strong> promote recovery <strong>of</strong> movement control in stroke was applied <strong>to</strong> the h<strong>and</strong> <strong>of</strong> subjects with<br />
stroke (Carey et al., 2002) <strong>and</strong> <strong>to</strong> the ankle in a single-subject research design (Carey et al.,<br />
2004) with favorable results. Unlike CIMT, tracking training emphasizes mo<strong>to</strong>r learning<br />
principles espoused by Schmidt (1991) that minimize guidance <strong>and</strong> involvement by a<br />
therapist, thereby potentially saving treatment cost.<br />
Conventional physical therapy for rehabilitation requires extensive interaction with a<br />
therapist, <strong>of</strong>ten for hours a day. These labor intensive efforts are costly <strong>and</strong> contribute <strong>to</strong> the<br />
staggering financial impact <strong>of</strong> stroke. Consequently, practitioners <strong>and</strong> administra<strong>to</strong>rs are<br />
challenged <strong>to</strong> find alternative methods <strong>to</strong> deliver quality health care at reasonable cost. One<br />
example <strong>of</strong> cost containment in stroke rehabilitation is home-based rehabilitation. Evidence<br />
has shown that early discharge from acute hospital care followed by home-based<br />
rehabilitation, involving pr<strong>of</strong>essionals visiting the home, reduced costs while preserving<br />
treatment outcomes that were equivalent <strong>to</strong> conventional rehabilitation methods (Young <strong>and</strong><br />
Forster, 1992, Widen Holmqvist et al., 1998, Beech et al., 1999, Anderson et al., 2000). With<br />
home-based treatment, patients can receive treatment at an intensity (hours per day) that is<br />
appropriate <strong>to</strong> their state <strong>of</strong> recovery rather than directed by health insurance policy, which<br />
may be <strong>to</strong>o much early on or <strong>to</strong>o little later on. Conventionally, rehabilitation for people with<br />
stroke is restricted <strong>to</strong> the first 6-12 months following the stroke, however, current research<br />
indicates that further recovery is possible with rehabilitation years after stroke (Kraft et al.,<br />
1992, Kunkel et al., 1999, Liepert et al., 2000a, Carey et al., 2002, Luft et al., 2004). With<br />
Track-JBiomechEng.doc Page 5 <strong>of</strong> 31
home-based treatment, the amount <strong>of</strong> time devoted <strong>to</strong> rehabilitation is only restricted by the<br />
patient’s level <strong>of</strong> commitment <strong>and</strong> not by the cost <strong>of</strong> a therapist.<br />
Interest in technology driven, home-based stroke movement therapies is evidenced by the<br />
emergence <strong>of</strong> pilot projects such as JavaTherapy, a web application that uses st<strong>and</strong>ard input<br />
devices such as force controlled joysticks (Reinkensmeyer et al., 2002), <strong>and</strong> UniTherapy, a<br />
telerehabilitation platform for computer-assisted movitvating rehabilitation that supports force<br />
feedback training with st<strong>and</strong>ard <strong>and</strong> cus<strong>to</strong>m PC input devices (Feng & Winters, 2005).<br />
Robot-aided neurorehabilitation is another emerging technology based treatment for stroke.<br />
Grounded or wearable powered manipula<strong>to</strong>rs assist or guide the paralyzed limb through a<br />
desired motion in much the same manner as a classic h<strong>and</strong>s-on physical therapy treatment.<br />
Upper limb devices include the MIT Manus (Krebs et al., 1998; Fasoli et al., 2003; Fasoli et<br />
al., 2004), Ketic Muscles’ H<strong>and</strong> Men<strong>to</strong>r (Koeneman et al., 2004). Lower limb devices include<br />
the Locomat by Hocoma (Colombo et al., 2000) among many others. Preliminary results have<br />
shown that upper <strong>and</strong> lower limb robot therapy can be effective. Unlike the Track<strong>Train</strong><br />
system described here, robots can be expensive <strong>and</strong> must be carefully designed <strong>to</strong> be safe<br />
before being considered for home use.<br />
Our group conducted a pilot study that used a finger movement tracking program where<br />
subjects with stroke received 18-20 one-hour rehabilitation training sessions using their<br />
paretic index finger <strong>to</strong> track target waveforms displayed on a computer screen under variable<br />
conditions (Carey et al., 2002). The subjects came <strong>to</strong> the clinic for treatment sessions with a<br />
physical therapist supervising. Pre <strong>and</strong> post training treatment functional magnetic resonance<br />
imaging (fMRI) was used <strong>to</strong> determine which parts <strong>of</strong> the brain were activated when the<br />
subject was performing the finger tracking activity. The results showed improved ability <strong>to</strong><br />
Track-JBiomechEng.doc Page 6 <strong>of</strong> 31
grasp <strong>and</strong> release small objects, <strong>and</strong> a change in cortical activation from predominantly<br />
ipsilateral control (non-stroke hemisphere active) <strong>to</strong> contralateral control (stroke hemisphere<br />
active) during movement <strong>of</strong> the paretic finger. The difficulty with the pilot study was that<br />
subjects were required <strong>to</strong> come <strong>to</strong> the clinic for training sessions. This was not only<br />
inconvenient, but physically difficult <strong>and</strong> time dem<strong>and</strong>ing <strong>of</strong> the subjects. Further, in-clinic<br />
training sessions could last no more than 60 minutes while current massed practice<br />
rehabilitation theory points <strong>to</strong> the benefit <strong>of</strong> longer training sessions.<br />
In light <strong>of</strong> the promising results <strong>of</strong> the pilot study, our group has developed Track<strong>Train</strong>, a<br />
system that enables tracking training sessions in the subjects’ homes without a therapist<br />
present. With home-based training the subject only has <strong>to</strong> come <strong>to</strong> the clinic for pre <strong>and</strong> post-<br />
treatment evaluations. Track<strong>Train</strong> attracted more subjects <strong>to</strong> the study than clinic-based<br />
training because many eligible subjects are not interested in coming <strong>to</strong> the clinic daily, or live<br />
<strong>to</strong>o far from the clinic for convenient daily travel. In addition, if home-based therapy proves<br />
<strong>to</strong> be effective than it could lead <strong>to</strong> new clinical treatment paradigms <strong>to</strong> serve larger numbers<br />
<strong>of</strong> patients with stroke at a lower cost.<br />
The main requirements driving the design <strong>of</strong> Track<strong>Train</strong> were first <strong>to</strong> create a system that<br />
required the patient <strong>to</strong> move his or her h<strong>and</strong> <strong>and</strong> wrist in a tracking task that required<br />
concentration <strong>to</strong> accomplish mo<strong>to</strong>r relearning, <strong>and</strong> second <strong>to</strong> create an easy-<strong>to</strong>-use system that<br />
could be operated au<strong>to</strong>nomously at home without requiring technical expertise. In addition,<br />
the system needed a telecommunication mechanism for periodic real time interaction with a<br />
remote physical therapist <strong>to</strong> moni<strong>to</strong>r, assist, <strong>and</strong> motivate the patient’s progress. The basics <strong>of</strong><br />
the tracking task were established in the pilot study. Thus the challenge in this project was <strong>to</strong><br />
design system that allowed patients <strong>to</strong> train at home without a therapist present.<br />
Track-JBiomechEng.doc Page 7 <strong>of</strong> 31
2 SYSTEM DESCRIPTION<br />
2.1 Overview<br />
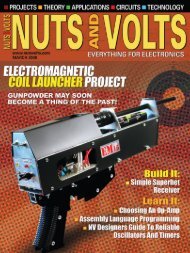
The Track<strong>Train</strong> home tracking system has two cus<strong>to</strong>m bilateral electrogoniometers that sense<br />
wrist <strong>and</strong> finger flexion <strong>and</strong> extension motions, a microcontroller-based interface box, a<br />
lap<strong>to</strong>p computer with tracking s<strong>of</strong>tware, a cell phone, a web cam, <strong>and</strong> a l<strong>and</strong> line telephone<br />
switch box (Figure 1). The system is designed for self installation in the patient’s home, or for<br />
installation by the therapist. While the system has many individual components, it is still<br />
relatively compact <strong>and</strong> fits easily on a desk<strong>to</strong>p or table without being an overly obtrusive<br />
presence in the patient’s home.<br />
2.2 H<strong>and</strong> Sensors<br />
<br />
The h<strong>and</strong> sensor has three platforms connected by rotating links, all made <strong>of</strong> polycarbonate.<br />
The sensor measures flexion <strong>and</strong> extension <strong>of</strong> the wrist <strong>and</strong> first MCP joints (Figure 2). The<br />
links form two four-bar mechanisms that transfer finger <strong>and</strong> wrist joint motion <strong>to</strong> two 0.5<br />
inch, 1.0K potentiometers (ETI <strong>System</strong>s, SP12S-1K) located on the platforms. This design<br />
was chosen over potentiometers axially aligned with the joint because it afforded higher<br />
<strong>to</strong>lerance <strong>to</strong> placement location. Because the linkage straddles the joint, the two platforms at<br />
either end need only be on opposite sides <strong>of</strong> the joint <strong>and</strong> do not require precise placement.<br />
This is particularly important for a sensor that was designed <strong>to</strong> be self-donned by the patient.<br />
The links are designed <strong>to</strong> rotate relative <strong>to</strong> one another in the plane <strong>of</strong> the platforms which<br />
allows the sensor <strong>to</strong> fit multiple h<strong>and</strong>s as the angle between the axis <strong>of</strong> the wrist <strong>and</strong> the axis<br />
<strong>of</strong> the forefinger differs between people. The sensor dimensions were determined by sampling<br />
Track-JBiomechEng.doc Page 8 <strong>of</strong> 31
male <strong>and</strong> female h<strong>and</strong>s <strong>and</strong> consulting anthropometric data (Tilley, 2001). The relation<br />
between the joint angle <strong>and</strong> potentiometer angle is sufficiently linear over the typical range <strong>of</strong><br />
motions seen that a linearization algorithm was not incorporated in<strong>to</strong> the s<strong>of</strong>tware. The sensor<br />
had small green LEDs on the two proximal platforms which flashed as a cue <strong>to</strong> the subject for<br />
which joint was active.<br />
<br />
The patient must don <strong>and</strong> d<strong>of</strong>f the sensor independently. The platforms balance on <strong>to</strong>p <strong>of</strong> the<br />
arm with relative stability. Hence, most <strong>of</strong> the difficulty in this task is associated with<br />
fastening <strong>and</strong> adjusting the straps. Two slap bracelets (fabric covered, metal strips that lie flat<br />
when bent in one direction <strong>and</strong> self-assemble in<strong>to</strong> a circle when a small amount <strong>of</strong> pressure is<br />
applied in the opposite direction) were used for anchoring the proximal sensor platform <strong>to</strong> the<br />
forearm. A Velcro strap with a D-ring at one end was used <strong>to</strong> anchor the h<strong>and</strong> platform. The<br />
patient slides his h<strong>and</strong> in<strong>to</strong> the looped strap <strong>and</strong> then pulls it back around on itself <strong>to</strong> tighten<br />
<strong>and</strong> secure the Velcro. The finger strap is flexible fabric ring that the patient slides his finger<br />
in<strong>to</strong>. A spring loaded clip is used <strong>to</strong> pull up the slack in the ring <strong>and</strong> secure it at the correct<br />
diameter. Because the clip is difficult <strong>to</strong> operate with limited dexterity <strong>and</strong> strength, the ring<br />
size is adjusted by the therapist at the initial fitting session. Because the finger is conical, the<br />
patient can don the sensor by sliding his forefinger in<strong>to</strong> the ring until it is snug. The links can<br />
be used as h<strong>and</strong>les for device removal.<br />
2.3 Interface box<br />
The sensor interface box converts the potentiometer reading in<strong>to</strong> a digital signal that is<br />
transmitted <strong>to</strong> the computer through its serial port. The interface box contains analog signal<br />
Track-JBiomechEng.doc Page 9 <strong>of</strong> 31
conditioning circuitry including programmable gain <strong>and</strong> <strong>of</strong>fset, a 20 Hz, two-pole low pass<br />
filter, <strong>and</strong> a programmable multiplexer that selects which channel <strong>to</strong> digitize (Figure 3).<br />
Signals are digitized at 100 Hz with a 10-bit analog-<strong>to</strong>-digital converter. S<strong>of</strong>tware on a<br />
PIC16F873 microcontroller controls the peripherals, creates the real-time sampling loop, <strong>and</strong><br />
sends the signal <strong>to</strong> the PC serial port. The host program running on the PC communicates<br />
with the microcontroller <strong>to</strong> enable <strong>and</strong> inhibit sampling, <strong>and</strong> <strong>to</strong> set current channel, gain <strong>and</strong><br />
<strong>of</strong>fset. A four stage running average filter implemented on the PC performed additional<br />
smoothing <strong>of</strong> the sampled signal.<br />
<br />
The sensor interface box has a large red but<strong>to</strong>n on the <strong>to</strong>p cover, a small black but<strong>to</strong>n on the<br />
back, <strong>and</strong> two color coded jacks for the left <strong>and</strong> right h<strong>and</strong> sensor cables on the front . The red<br />
but<strong>to</strong>n is the only control the user needs <strong>to</strong> operate the program. Through prompts on the<br />
computer display, the red but<strong>to</strong>n is used <strong>to</strong> start the treatment, pause the treatment, calibrate<br />
the h<strong>and</strong> sensors, <strong>and</strong> end the treatment. The black but<strong>to</strong>n is used for unusual circumstances <strong>to</strong><br />
abort the program <strong>and</strong> immediately shutdown the computer.<br />
2.4 Computer<br />
The system control unit is a Dell Latitude D600 lap<strong>to</strong>p computer running the Windows XP.<br />
The computer is treated as an appliance with the patient never having <strong>to</strong> use the keyboard or<br />
mouse. The lap<strong>to</strong>p mouse was not connected <strong>and</strong> the keyboard was covered with a screen.<br />
The keyboard <strong>and</strong> mouse were not used for several reasons. Keys are close <strong>to</strong>gether which<br />
increases the likelihood that a patient with limited dexterity might press the wrong key. Using<br />
a mouse requires fine mo<strong>to</strong>r control which is lacking in the users, <strong>and</strong> also requires familiarity<br />
Track-JBiomechEng.doc Page 10 <strong>of</strong> 31
with computers. Access <strong>to</strong> the keyboard <strong>and</strong> mouse could afford technologically savvy<br />
patients a means <strong>of</strong> getting in<strong>to</strong> the inner workings <strong>of</strong> the system, which is not desired. The<br />
red but<strong>to</strong>n on the interface box <strong>and</strong> the lap<strong>to</strong>p’s power but<strong>to</strong>n were the only two controls<br />
needed by the subject <strong>to</strong> operate the system. On power-up the computer immediately boots<br />
in<strong>to</strong> the tracking program <strong>and</strong> from there, all interaction by the user was done with the single<br />
red but<strong>to</strong>n on the interface box.<br />
2.5 S<strong>of</strong>tware<br />
The tracking application on the PC was created using Micros<strong>of</strong>t Visual Basic 6.0. On power-<br />
up, the PC au<strong>to</strong>matically started the application. With both sensors mounted, the subject went<br />
through a prompted calibration sequence with the display instructing the subject <strong>to</strong> open <strong>and</strong><br />
close their h<strong>and</strong> <strong>and</strong> flex <strong>and</strong> extend their wrist as far as possible which au<strong>to</strong>matically<br />
communicated the subject’s active range <strong>of</strong> motion <strong>to</strong> the application (Figure 4). The red<br />
but<strong>to</strong>n was pressed <strong>to</strong> sequence through the joints. If the measured range <strong>of</strong> motion was less<br />
than a threshold, it was likely that the sensor had been misapplied <strong>and</strong> the subject was advised<br />
through on-screen instructions <strong>to</strong> telephone the therapist for advice. The sensors must be<br />
calibrated each time the program is started as there is no guarantee that the sensor was placed<br />
on the h<strong>and</strong> the same way each time. At the completion <strong>of</strong> calibration, the subject pushed the<br />
red but<strong>to</strong>n <strong>to</strong> commence the day’s therapeutic tracking training session.<br />
<br />
The first screen <strong>of</strong> a trial contained four key pieces <strong>of</strong> information for the subject (Figure 4).<br />
At the <strong>to</strong>p <strong>of</strong> the screen, the number <strong>of</strong> blocks left in the session <strong>and</strong> the number <strong>of</strong> trials left<br />
in the block are shown. Instructions on how <strong>to</strong> pause the program by pressing the red but<strong>to</strong>n<br />
Track-JBiomechEng.doc Page 11 <strong>of</strong> 31
are given in the center <strong>of</strong> the screen. Text <strong>and</strong> pic<strong>to</strong>rial indica<strong>to</strong>rs <strong>of</strong> the h<strong>and</strong>, joint, <strong>and</strong> arm<br />
position <strong>to</strong> be used for the next tracking task are shown at the bot<strong>to</strong>m <strong>of</strong> the screen. There<br />
were two LEDs on the h<strong>and</strong> sensors, one located at the wrist <strong>and</strong> the other at the finger. The<br />
LED on the h<strong>and</strong> <strong>and</strong> joint <strong>to</strong> be used in the next trial blinked throughout the first <strong>and</strong> second<br />
trial screens indicating which joint would be used for the next tracking trial. A countdown<br />
clock displayed the time remaining <strong>to</strong> the start <strong>of</strong> the next tracking task.<br />
The second screen in the trial sequence was the tracking task (Figure 5). At the start <strong>of</strong> the<br />
trial, a green ball was displayed on the far left <strong>of</strong> the box with the joint motion controlling the<br />
vertical motion <strong>of</strong> the ball. The patient had one second at the start <strong>of</strong> the trial <strong>to</strong> move the ball<br />
up <strong>and</strong> down <strong>to</strong> get a feel for the range <strong>of</strong> motion through which he would be working. After<br />
the one second delay, a beep sounded <strong>and</strong> the ball began <strong>to</strong> move horizontally across the<br />
screen at a fixed rate determined by the waveform duration. The task <strong>of</strong> the subject was <strong>to</strong><br />
move the green ball follow the blue target by moving the specified joint up <strong>and</strong> down. The<br />
ball left a red trail for visual feedback <strong>to</strong> the patient. When the ball reached the right end <strong>of</strong><br />
the box, a double beep indicated the end <strong>of</strong> the trial. The third trial screen showed a <strong>to</strong>tal<br />
tracking score <strong>to</strong> indicate the subject's performance (Figure 5).<br />
<br />
Eleven tracking performance scores (Carey, 1990; Schmidt <strong>and</strong> Lee, 2005) were computed<br />
<strong>and</strong> s<strong>to</strong>red for each trial. The scores <strong>and</strong> associated computation algorithms are shown in<br />
Table 1. The subject is shown 1000*AI during the rest period after each trial as their<br />
performance score on the trial. The score ranges from a large negative number if the tracking<br />
is anti-phase <strong>to</strong> 1000 for perfect tracking.<br />
Track-JBiomechEng.doc Page 12 <strong>of</strong> 31
Following some trials, the screen also displayed text providing au<strong>to</strong>mated feedback on<br />
performance. The feedback alerted the subject <strong>to</strong> areas <strong>of</strong> weak performance, such as wrist or<br />
finger extension, or alerted the subject <strong>to</strong> excessive or insufficient frequency <strong>of</strong> movement.<br />
The feedback was generated based on the 11 tracking performance metrics that were<br />
calculated after every trial. This more descriptive information is known as “knowledge <strong>of</strong><br />
performance” (KP). KP feedback was shown <strong>to</strong> subjects in a faded schedule after certain<br />
blocks <strong>of</strong> trials being shown every third block on day one <strong>and</strong> gradually declining <strong>to</strong> every<br />
20th block by day 10. The purpose <strong>of</strong> the faded feedback is <strong>to</strong> reduce reliance on external<br />
guidance <strong>and</strong> instead promote internal error-detection capability (Schmidt, 1991). The KP<br />
information, when it appeared, was based only on the immediately preceding trial <strong>and</strong> was<br />
always complemented with an encouraging comment <strong>to</strong> motivate continuing effort. An<br />
example is, "You are not reaching the <strong>to</strong>ps <strong>of</strong> the upper blue waves. Try <strong>to</strong> reach higher <strong>and</strong><br />
<strong>to</strong>uch the peaks," <strong>and</strong> "Mrs. Jones, your performance is great! Keep it up!"<br />
The treatment plan was 180 tracking trials per day for 10 days, a <strong>to</strong>tal treatment <strong>of</strong> 1800 trials.<br />
The trials were organized in<strong>to</strong> 60 blocks with three identical trials per block. The blocks were<br />
r<strong>and</strong>omly selected from a set <strong>of</strong> 100 test conditions which varied in target wave shape,<br />
frequency, amplitude, duration, joint used, h<strong>and</strong> used, h<strong>and</strong> posture <strong>and</strong> visual feedback<br />
(Table 2). The variations were needed <strong>to</strong> keep the patient concentrated on the task. The paretic<br />
h<strong>and</strong> was used for 90% <strong>of</strong> the blocks <strong>and</strong> the nonparetic h<strong>and</strong> for 10%. Tracking with the<br />
nonparetic h<strong>and</strong> was included <strong>to</strong> take advantage <strong>of</strong> cross education. Cross education is the<br />
principle <strong>of</strong> training in which effort unilaterally has beneficial effects bilaterally (Greenough<br />
Track-JBiomechEng.doc Page 13 <strong>of</strong> 31
et al., 1985; Imamizu et al., 1998; Shields et al., 1999). H<strong>and</strong> posture (palm up/down), where<br />
for the up case, cursor movement is opposite the joint movement, was included <strong>to</strong> case greater<br />
complexity <strong>and</strong> depth <strong>of</strong> cognitive processing for the task (Carey et al., 1994, 1995, 1998). In<br />
some blocks, the ball <strong>and</strong> red trail were replaced by a vertical hairline cursor that sweeps<br />
across <strong>to</strong> show timing but provides no visual feedback on joint location. Every trial was<br />
followed by a rest period <strong>of</strong> the same duration <strong>of</strong> the preceding trial, constituting distributed,<br />
rather than massed, practice (Dail, 2004; Lee, 1989).<br />
<br />
Once the training session started, other than tracking, the only action required by the subject<br />
was <strong>to</strong> press the red but<strong>to</strong>n whenever a pause was desired. If the subject did not press the<br />
pause, the computer continued until all 180 trials were done that day. Most subjects choose <strong>to</strong><br />
pause periodically. If the pause was less than five minutes, pressing the red but<strong>to</strong>n <strong>to</strong> resume<br />
brought the subject immediately back <strong>to</strong> the previous training point. For longer pauses, the<br />
program assumed the subject had removed the sensors <strong>and</strong> pressing the red but<strong>to</strong>n <strong>to</strong> resume<br />
went back <strong>to</strong> the calibration screen. The application informed the subject when the day’s<br />
session was complete <strong>and</strong> au<strong>to</strong>matically shut down the computer. The au<strong>to</strong>matic shutdown<br />
regulated the rate <strong>of</strong> rehabilitation <strong>to</strong> the prescribed regimen <strong>of</strong> one session per day. The<br />
application had additional branch points <strong>to</strong> detect <strong>and</strong> exit gracefully if the sensor was still<br />
(meaning the subject may have left the room), the sensor was disconnected from the interface<br />
box, the computer was shut down, or power was removed from the sensor box.<br />
2.6 Telecommunication<br />
Track-JBiomechEng.doc Page 14 <strong>of</strong> 31
Telecommunication <strong>to</strong>ok place between therapist <strong>and</strong> patient every few days. The periodic,<br />
real-time, face-<strong>to</strong>-face interaction with a therapist was for moni<strong>to</strong>ring, motivating <strong>and</strong><br />
assistance, <strong>and</strong> is essential for patient compliance with the rigorous pro<strong>to</strong>col. We assumed<br />
every subject had a l<strong>and</strong>-line telephone <strong>and</strong> cellular phone coverage, but not broad-b<strong>and</strong><br />
internet. Based on pilot work, we assumed that high quality audio was essential for<br />
meaningful communication, but low quality video was adequate. Voice communication was<br />
by cell phone (TracPhone). Two-way video <strong>and</strong> data transmission was by web cameras<br />
(Logitech QuickCam 4000) <strong>and</strong> dial-up internet access, resulting in low quality (color,<br />
128x96, 3 frames per sec) video imaging.<br />
To initiate a tele-session, the therapist called the subject on the cell phone (after first alerting<br />
the subject with a l<strong>and</strong>line phone call as the subject is not used <strong>to</strong> answering the cell phone).<br />
The cell phone was set for au<strong>to</strong>-answer on any but<strong>to</strong>n push so that mo<strong>to</strong>r-impaired subjects<br />
did not have <strong>to</strong> manipulate small but<strong>to</strong>ns. A cell phone speaker phone accessory was used so<br />
that the subject could communicate h<strong>and</strong>s free. The therapist instructed the subject <strong>to</strong> flip the<br />
switch on the telephone interface box, which connected the l<strong>and</strong> line <strong>to</strong> the PC modem, then<br />
power up the computer. On boot up, the PC au<strong>to</strong>matically detected the dial <strong>to</strong>ne, dialed the<br />
ISP, connected <strong>to</strong> the host computer, <strong>and</strong> from there the therapist could download trial data<br />
<strong>and</strong> remotely start the web cam. After connecting, the subject could see the therapist’s face<br />
on the computer display, <strong>and</strong> the therapist could see the subject or could ask the subject <strong>to</strong><br />
hold his or her h<strong>and</strong> in front <strong>of</strong> the camera <strong>to</strong> see whether the electrogoniometer was attached<br />
properly. During the communication the therapist answered questions <strong>and</strong> provided helpful<br />
comments <strong>and</strong> motivation. At the end, the therapist could remotely shut down the subject's<br />
computer. The session ended with the therapist instructing the subject <strong>to</strong> <strong>to</strong>ggle the switch<br />
Track-JBiomechEng.doc Page 15 <strong>of</strong> 31
setting on the telephone interface box so that the next time the subject computer powered up,<br />
it would boot in<strong>to</strong> tracking treatment mode.<br />
3 EVALUATION STUDY<br />
3.1 OBJECTIVES<br />
The tracking training evaluation study had two objectives. First, <strong>to</strong> determine if home-based,<br />
self-administered tracking training with only occasional teleconferencing with a remote<br />
therapist is feasible, <strong>and</strong> second whether tracking training was more beneficial for cortical<br />
reorganization <strong>and</strong> improved mo<strong>to</strong>r control than movement training. While both questions<br />
were examined in the study, this paper is concerned with the first objective. A companion<br />
paper (Carey et al., 2006) contains the complete results for the second objective.<br />
3.2 METHODS<br />
The tracking training system was placed in the homes <strong>of</strong> 24 subjects ranging from 2 <strong>to</strong> 307<br />
miles from the University (median = 18 miles), plus one 1057 miles away. Subject inclusion<br />
criteria were post-stroke duration <strong>of</strong> at least 12 months; satisfac<strong>to</strong>ry corrected vision <strong>to</strong> detect<br />
the position <strong>of</strong> a cursor on the computer screen as being slightly above, below or exactly on a<br />
target line; <strong>and</strong> at least 10 degrees <strong>of</strong> active extension-flexion movement at the index finger<br />
metacarpophalangeal (MP) joint <strong>of</strong> the paretic h<strong>and</strong>. All subjects had sufficient cognition <strong>to</strong><br />
perform the training <strong>and</strong> testing with Mini-Mental State Examination (Folstein, 1975) scores<br />
<strong>of</strong> 25 or higher except for one subject with a score <strong>of</strong> 21, who was still deemed appropriate <strong>to</strong><br />
participate. Exclusion criteria were indwelling metals or medical implants incompatible with<br />
functional magnetic resonance imaging (fMRI), pregnancy <strong>and</strong> claustrophobia. The mean age<br />
(± SD) <strong>of</strong> the subjects was 66.7 ± 9.6 years. The mean stroke duration (time from stroke onset<br />
Track-JBiomechEng.doc Page 16 <strong>of</strong> 31
<strong>to</strong> entrance in<strong>to</strong> study) was 39.1 ± 24.8 months. The study was approved by the University <strong>of</strong><br />
Minnesota IRB.<br />
Twenty <strong>of</strong> the 24 subjects were in the controlled training study with 10 in the tracking training<br />
group <strong>and</strong> 10 in the movement group. Subjects in the movement group performed the same<br />
number <strong>of</strong> movement trials, as directed by the computer display, but neither target waveform<br />
nor response line was displayed <strong>and</strong> thus the subject was not required <strong>to</strong> problem-solve nor<br />
concentrate <strong>to</strong> perform the task.<br />
During the pre-treatment evaluation session at the University, subjects were trained in use <strong>of</strong><br />
the equipment, <strong>and</strong> watched a video clip that showed the steps for setting up the equipment at<br />
home. The video was s<strong>to</strong>red on the tracking lap<strong>to</strong>p for later review at home. The subject <strong>and</strong><br />
family member practiced the equipment setup <strong>and</strong> performed six tracking trials under<br />
supervision <strong>of</strong> the therapist. The subject was then sent home with the equipment. Subjects<br />
completed the 1800 trials in 10 <strong>to</strong> 14 days. The therapist communicated with the subject about<br />
5 times using the teleconferencing system. The therapist was also available by pager.<br />
Pre <strong>and</strong> post treatment evaluations included Box <strong>and</strong> Block (Mathiowetz, 1985), Jebsen-<br />
Taylor H<strong>and</strong> Function (Jebsen, 1969), finger range <strong>of</strong> motion, finger movement tracking<br />
accuracy, <strong>and</strong> fMRI voxel count, intensity <strong>and</strong> laterality index. The fMRI measures were<br />
included <strong>to</strong> evaluate cortical reorganization. Details <strong>of</strong> these evaluations are in Carey et al.<br />
(2006). A telephone usability survey was conducted following the completion <strong>of</strong> the<br />
treatment. The survey contained six questions with a five point Likert response scale.<br />
Track-JBiomechEng.doc Page 17 <strong>of</strong> 31
3.3 USABILITY RESULTS<br />
Fifteen <strong>of</strong> the 24 subjects were able <strong>to</strong> install the system by themselves while nine required a<br />
home visit for installation. An additional four home visits were required <strong>to</strong> correct a computer<br />
or equipment malfunction or equipment. One subject dropped out because they were unable <strong>to</strong><br />
independently don <strong>and</strong> d<strong>of</strong>f the sensor <strong>and</strong> had no companion <strong>to</strong> help. Teleconferencing<br />
sessions were conducted with 22 <strong>of</strong> 24 subjects. All 20 subjects in the controlled study<br />
completed the 1800 trial treatment. Nineteen <strong>of</strong> the 24 subjects completed the usability survey<br />
whose results are shown in Table 3. Two <strong>of</strong> the 19 had no teleconferencing sessions <strong>and</strong> did<br />
not answer Question 6.<br />
<br />
Off those subjects completing the usability survey, all agreed they "unders<strong>to</strong>od how <strong>to</strong> use the<br />
system" <strong>and</strong> that "the computer was easy <strong>to</strong> use." Fourteen could independently don <strong>and</strong> d<strong>of</strong>f<br />
the sensors. Fifteen did not feel the system interfered with their daily routine, 15 saw the<br />
au<strong>to</strong>mated feedback as being useful <strong>and</strong> 16 found the teleconferencing sessions easy <strong>to</strong><br />
manage. In self reported comments associated with the survey, almost all <strong>of</strong> the subjects<br />
commented on the convenience <strong>of</strong> being able <strong>to</strong> work on the treatment at their leisure, fitting<br />
it around their normal daily routine. About one quarter <strong>of</strong> the subjects had difficulty donning<br />
<strong>and</strong> d<strong>of</strong>fing the sensors by themselves, which was probably correlated <strong>to</strong> severity <strong>of</strong> the<br />
stroke. The most consistent complaint was putting on the electrogoniometers independently,<br />
particularly using the paretic h<strong>and</strong> <strong>to</strong> apply the electrogoniometer <strong>to</strong> the nonparetic h<strong>and</strong>,<br />
which <strong>to</strong>ok some subjects 10-15 minutes or more.<br />
Track-JBiomechEng.doc Page 18 <strong>of</strong> 31
3.4 TREATMENT RESULTS<br />
Complete information on treatment results are in the companion paper (Carey et al., 2006)<br />
<strong>and</strong> only a summary is presented here. The Track group showed improvement in Box <strong>and</strong><br />
Block, Jebsen Taylor, finger range <strong>of</strong> motion <strong>and</strong> finger tracking while the Move group<br />
showed improvements only in Box <strong>and</strong> Block <strong>and</strong> Jebsen Taylor. Unlike our earlier clinic<br />
based finger tracking training project that demonstrated brain reorganization (Carey, 2002),<br />
the fMRI data in this study showed no significant evidence <strong>of</strong> brain reorganization for either<br />
group.<br />
4 DISCUSSION<br />
The subjects were <strong>to</strong>lerant <strong>of</strong> the Track<strong>Train</strong> system. The concern that elderly people<br />
unaccus<strong>to</strong>med <strong>to</strong> complications <strong>of</strong> electronic technology might drop out <strong>of</strong> the study did not<br />
materialize. The subjects simply needed <strong>to</strong> be gently trained in the system operation <strong>and</strong> be<br />
reassured that help was only a phone call away. Subjects who were hesitant at first became<br />
excited by the challenge <strong>to</strong> continually do better. The evaluation project confirmed that an<br />
easy-<strong>to</strong>-use, simple user interface, coupled with an initial instruction session is essential for<br />
successful home use.<br />
The h<strong>and</strong> sensor could be improved <strong>to</strong> make it easier <strong>to</strong> don <strong>and</strong> d<strong>of</strong>f. Next generation sensors<br />
should be wireless <strong>to</strong> eliminate cable interference, should not have the linkage bars above the<br />
wrist, <strong>and</strong> should have a simplified attachment process. Because <strong>of</strong> the theoretical value <strong>of</strong><br />
cross-education (Greenough, 1985; Imamizu , 1998; Shields, 1999; Luft, 2004), the training<br />
effort with the nonparetic h<strong>and</strong> should be retained, increasing the challenge for a usable<br />
sensor design.<br />
Track-JBiomechEng.doc Page 19 <strong>of</strong> 31
The current system takes up most <strong>of</strong> a desk when all the cables, boxes <strong>and</strong> communications<br />
equipment is placed. Future systems must be compact <strong>and</strong> even simpler <strong>to</strong> set up. In<br />
particular, the number <strong>of</strong> connections must be reduced by either combining system<br />
components in<strong>to</strong> a single appliance, or mounting components on a single board or in a single<br />
package. Ideally, the subject should only have <strong>to</strong> plug in<strong>to</strong> a power outlet <strong>and</strong> connect <strong>to</strong> the<br />
telephone or broadb<strong>and</strong>.<br />
Periodic therapist contact was essential for reassuring <strong>and</strong> motivating patients <strong>to</strong> complete the<br />
pro<strong>to</strong>col. Visual contact by video proved important for two reasons. First, the visual presence<br />
<strong>of</strong> the therapist <strong>of</strong>ten provided sufficient motivation for the patient <strong>to</strong> continue the treatment.<br />
Second, if the patient was having difficulties with the sensor, the therapist could see the<br />
problem <strong>and</strong> provide a solution. Future systems would benefit from a pan-tilt-zoom camera<br />
that could be remotely controlled by the therapist. The teleconferencing technology used in<br />
this project demonstrated that while high quality audio is essential, low quality video is<br />
acceptable. Broadb<strong>and</strong> connections are preferable <strong>to</strong> increase the quality <strong>of</strong> the video <strong>and</strong><br />
simplify the process <strong>of</strong> au<strong>to</strong>matically downloading tracking data <strong>to</strong> a central database each<br />
night. While the penetration <strong>of</strong> cable <strong>and</strong> DSL broadb<strong>and</strong> <strong>to</strong> remote areas is still lagging, the<br />
recent rise <strong>of</strong> wireless broadb<strong>and</strong> access through cellular phone networks promises broadb<strong>and</strong><br />
coverage <strong>to</strong> most areas.<br />
The controlled study showed that tracking training had a positive effect on finger range <strong>of</strong><br />
motion, finger tracking, <strong>and</strong> functional h<strong>and</strong> dexterity, demonstrating the potential for clinical<br />
efficacy. We suspect that the two weeks <strong>of</strong> training was <strong>to</strong>o short <strong>to</strong> differentiate between the<br />
Track <strong>and</strong> Move groups <strong>and</strong> <strong>to</strong>o short <strong>to</strong> show the brain reorganization that was evident in our<br />
earlier study. Future studies will spread the treatment over a longer time period.<br />
Track-JBiomechEng.doc Page 20 <strong>of</strong> 31
One might argue that training by tracking waveforms on the screen is boring <strong>and</strong> instead that<br />
joint motion should drive a video game. There are at least three reasons for not taking the<br />
video game approach. First, it is not clear what video game would be motivating for hours at a<br />
time <strong>to</strong> elderly subjects with stroke. While teens can become addicted <strong>to</strong> a single video game<br />
or <strong>to</strong> a category <strong>of</strong> video games, motivation drivers have not been studied for our target<br />
population. Thus, choosing any one or any collection <strong>of</strong> video games may not solve the<br />
motivation problem. Second, controlling a video game does not permit control over<br />
amplitude, frequency <strong>and</strong> type <strong>of</strong> movement. With structured waveforms, Track<strong>Train</strong> can<br />
provide targets at several frequencies <strong>and</strong> specific amplitudes scaled <strong>to</strong> the patient’s active<br />
range <strong>of</strong> motion, <strong>and</strong> vary parameters in predetermined or adaptive paradigms as needed for<br />
treatment. Third, in this study patients were sufficiently motivated by target tracking <strong>to</strong><br />
complete long, daily sessions <strong>of</strong> treatment.<br />
5 CONCLUSION<br />
The study demonstrated the technical feasibility <strong>of</strong> a home based tracking training system for<br />
mo<strong>to</strong>r rehabilitation following stroke. <strong>Home</strong>-based treatment using Track<strong>Train</strong> resulted in<br />
functional improvements similar <strong>to</strong> those seen for the equivalent clinic-based system <strong>and</strong><br />
subjects indicated that they preferred the home system for its convenience. The ability <strong>of</strong><br />
subjects <strong>to</strong> successfully complete a treatment plan showed that elderly patients can underst<strong>and</strong><br />
<strong>and</strong> use the system without continual supervision intended. Improvements are needed <strong>to</strong><br />
eliminate the sensor wires <strong>and</strong> <strong>to</strong> simplify telecommunication. Future treatment must be<br />
spread out for longer than two weeks for significant cortical reorganization.<br />
Track-JBiomechEng.doc Page 21 <strong>of</strong> 31
ACKNOWLEDGMENTS<br />
This work was supported by the National Institute on Disability <strong>and</strong> Rehabilitation Research<br />
(U.S. Department <strong>of</strong> Education #H133G020145-04) <strong>and</strong> the National Institutes <strong>of</strong> Health<br />
(National Center for Research Resources #M01-RR00400 <strong>and</strong> Biomedical Technology<br />
Research Resources #P41-R008079).<br />
Track-JBiomechEng.doc Page 22 <strong>of</strong> 31
REFERENCES<br />
AHA (2005) Heart <strong>and</strong> Stroke Statistics, 2005 Update. American Heart Association.<br />
Anderson C, Rubenach S, Mhurchu CN, Clark M, Spencer C, Winsor A (2000) <strong>Home</strong> or<br />
hospital for stroke rehabilitation? results <strong>of</strong> a r<strong>and</strong>omized controlled trial : I: health<br />
outcomes at 6 months. Stroke 31:1024-1031.<br />
Beech R, Rudd AG, Tilling K, Wolfe CD (1999) Economic consequences <strong>of</strong> early inpatient<br />
discharge <strong>to</strong> community-based rehabilitation for stroke in an inner-London teaching<br />
hospital. Stroke 30:729-735.<br />
Black JE, Isaacs KR, Anderson BJ, Alcantara AA, Greenough WT (1990) Learning causes<br />
synap<strong>to</strong>genesis, whereas mo<strong>to</strong>r activity causes angiogenesis, in cerebellar cortex <strong>of</strong><br />
adult rats. Proceedings <strong>of</strong> the National Academy <strong>of</strong> Sciences <strong>of</strong> the United States <strong>of</strong><br />
America 87:5568-5572.<br />
Bohannon R, Smith M (1987) Interrater reliability <strong>of</strong> a modified Ashworth scale <strong>of</strong> muscle<br />
spasticity. Phys Ther 67:206.<br />
Brennan DM, Georgeadis AC, Baron CR, Barker LM (2004) The effect <strong>of</strong> videoconferencebased<br />
telerehabilitation on s<strong>to</strong>ry retelling performance by brain-injured subjects <strong>and</strong> its<br />
implications for remote speech-language therapy. Telemedicine Journal & E-Health<br />
10:147-154.<br />
Carey J, Baxter T, Di Fabio R (1998) Tracking control in the nonparetic h<strong>and</strong> <strong>of</strong> subjects with<br />
stroke. Arch Phys Med Rehabil 79:435-441.<br />
Carey JR (1990) Manual Stretch: Effect on Finger Movement Control <strong>and</strong> Force Control in<br />
Stroke Subjects with Spastic Extrinsic Finger Flexor Muscles. Arch Phys Med Rehabil<br />
71:888-894.<br />
Carey JR, Patterson RP, Hollenstein PJ (1988) Sensitivity <strong>and</strong> reliability <strong>of</strong> force tracking <strong>and</strong><br />
joint-movement tracking scores in healthy subjects. Phys Ther 68:1087-1091.<br />
Carey JR, Bhatt E, Nagpal A (2005) Neuroplasticity Promoted by Task Complexity. Exercise<br />
<strong>and</strong> Sport Science Review 33:24-31.<br />
Carey JR, Anderson KM, Kimberley TJ, Lewis SM, Auerbach EJ, Ugurbil K (2004) fMRI<br />
analysis <strong>of</strong> ankle movement tracking training in subject with stroke. Exp Brain Res<br />
154:281-290.<br />
Carey JR, Kimberley TJ, Lewis SM, Auerbach E, Dorsey L, Rundquist P, Ugurbil K (2002)<br />
Analysis <strong>of</strong> fMRI <strong>and</strong> Finger Tracking <strong>Train</strong>ing in Subjects with Chronic Stroke. Brain<br />
125:773-788.<br />
Carey J, Durfee W, Bhatt E, Nagpal A, Weinstein S, Anderson K, Lewis S (2006), Tracking<br />
vs. movement <strong>Telerehabilitation</strong> training <strong>to</strong> change h<strong>and</strong> function <strong>and</strong> brain<br />
reorganization in stroke, Submitted <strong>to</strong> Neurorehabilitation <strong>and</strong> Neural Repair.<br />
Cauraugh J, Light K, Kim S, Thigpen M, Behrman A (2000) Chronic mo<strong>to</strong>r dysfunction after<br />
stroke: recovering wrist <strong>and</strong> finger extension by electromyography-triggered<br />
neuromuscular stimulation. Stroke 31:1360-1364.<br />
Chae J, Yang G, Park BK, Labatia I (2002) Muscle weakness <strong>and</strong> cocontraction in upper<br />
limb hemiparesis: relationship <strong>to</strong> mo<strong>to</strong>r impairment <strong>and</strong> physical disability.<br />
Neurorehabilitation & Neural Repair 16:241-248.<br />
Chauhan N, Zhao Z, Barber P, Buchan A (2003) Lessons in experimental ischemia for<br />
clinical stroke medicine. Curr Opin Neurology 16:65-71.<br />
Chen R, Yung D, Li JY (2003) Organization <strong>of</strong> ipsilateral excita<strong>to</strong>ry <strong>and</strong> inhibi<strong>to</strong>ry pathways in<br />
the human mo<strong>to</strong>r cortex. Journal <strong>of</strong> Neurophysiology 89:1256-1264.<br />
Chu WJ, Mason GF, Pan JW, Hethering<strong>to</strong>n HP, Liu HG, San Pedro EC, Mountz JM (2002)<br />
Regional cerebral blood flow <strong>and</strong> magnetic resonance spectroscopic imaging findings in<br />
diaschisis from stroke. Stroke 33:1243-1248.<br />
Colombo G, Joerg M, Schreier R, Dietz V. (2000) Treadmill training <strong>of</strong> paraplegic patients<br />
using a robotic orthosis. Journal <strong>of</strong> Rehabilitation Research <strong>and</strong> Development, 37(6):693-<br />
700.<br />
Track-JBiomechEng.doc Page 23 <strong>of</strong> 31
Cramer S, Nelles G, Benson R, Kaplan J, Parker R, Kwong K, Kennedy D, Finklestein S,<br />
Rosen B (1997) A functional MRI study <strong>of</strong> subjects recovered from hemiparetic stroke.<br />
Stroke 28:2518-2527.<br />
Dail TK, Christina RW (2004), Distribution <strong>of</strong> practice <strong>and</strong> metacognition in learning <strong>and</strong> longterm<br />
retention <strong>of</strong> a discrete mo<strong>to</strong>r task. Research Quarterly for Exercise & Sport,<br />
75(2):148-155.<br />
Desrosiers J, Bravo G, Hebert R, Dutil E, Mercier L (1994) Validation <strong>of</strong> the Box <strong>and</strong> Block<br />
Test as a measure <strong>of</strong> dexterity <strong>of</strong> elderly people: reliability, validity, <strong>and</strong> norms studies.<br />
Archives <strong>of</strong> Physical Medicine & Rehabilitation 75:751-755.<br />
Durfee, W., Weinstein S, Carey J, Bhatt E, Nagpal A (2005), <strong>Home</strong> stroke telerehabilitation<br />
system <strong>to</strong> train recovery <strong>of</strong> h<strong>and</strong> function. Proceedings <strong>of</strong> the 2005 IEEE 9th International<br />
Conference on Rehabilitation Robotics, pp. 353-356.<br />
S. Fasoli, H. I. Krebs, J. Stein, W. R. Frontera, <strong>and</strong> N. Hogan, (2003) Effects <strong>of</strong> robotic<br />
therapy on mo<strong>to</strong>r impairment <strong>and</strong> recovery in chronic stroke, Archives <strong>of</strong> Physical<br />
Medicine <strong>and</strong> Rehabilitation, 84:477-482<br />
S. Fasoli, H. I. Krebs, J. Stein, W. R. Frontera, R. Hughes, <strong>and</strong> N.Hogan, (2004) Robotic<br />
therapy for chronic mo<strong>to</strong>r impairments after stroke: follow-up results, Archives <strong>of</strong> Physical<br />
Medicine <strong>and</strong> Rehabilitation, 85:1106-1111.<br />
Feeney DM, Baron JC (1986) Diaschisis. Stroke 17:817-830.<br />
Feigin V, Lawes C, Bennett D, Anderson C (2003) Stroke epidemiology: a review <strong>of</strong><br />
population-based studies <strong>of</strong> incidence, prevalence, <strong>and</strong> case-fatality in the late 20th<br />
century. Neurology 2:43-53.<br />
Feng, X, Winters, J, (2005) UniTherapy: A computer-assisted motivating neurorehabilitation<br />
platform for teleassessment <strong>and</strong> remote therapy, Proceedings <strong>of</strong> the 2005 IEEE 9th<br />
International Conference <strong>of</strong> Rehabilitation Robotics, 349-352.<br />
Folstein M, Folstein S, McHugh P (1975) "Mini-mental state:" A practical method for grading<br />
the cognitive state <strong>of</strong> patients for the clinician. J Psychiat Res 12:189-198.<br />
Gomez-Pinilla F, So V, Kesslak JP (1998) Spatial learning <strong>and</strong> physical activity contribute <strong>to</strong><br />
the induction <strong>of</strong> fibroblast growth fac<strong>to</strong>r: neural substrates for increased cognition<br />
associated with exercise. Neuroscience 85:53-61.<br />
Greenough W, Larson J, Withers G (1985) Effects <strong>of</strong> unilateral <strong>and</strong> bilateral training in a<br />
reaching task on dendritic branching <strong>of</strong> neurons in the rat mo<strong>to</strong>r-sensory forelimb cortex.<br />
Behavioral <strong>and</strong> Neural Biology 44:301-314.<br />
ICORR (2005), Proceedings <strong>of</strong> the 2005 IEEE 9th International Conference on Rehabilitation<br />
Robotics, June, 2005, Chicago, IL, USA.<br />
Imamizu H, Uno Y, Kawa<strong>to</strong> M (1998) Adaptive internal model <strong>of</strong> intrinsic kinematics involved<br />
in learning an aiming task. J Exp Psychol Hum Percept Perform 24:812-829.<br />
Jebsen RH, Taylor N, Trieschmann RB, Trotter MJ, Howard LA (1969) An objective <strong>and</strong><br />
st<strong>and</strong>ardized test <strong>of</strong> h<strong>and</strong> function. Arch Phys Med Rehabil 50:311-319.<br />
Jorgensen HS, Nakayama H, Raaschou HO, Olsen TS (1999) Stroke. Neurologic <strong>and</strong><br />
functional recovery the Copenhagen Stroke Study.887-906.<br />
Kane RL, Chen Q, Finch M, Blewett L, Burns R, Moskowitz M (2000) The optimal outcomes<br />
<strong>of</strong> post-hospital care under medicare. Health Services Research 35:615-661.<br />
Kimberley TJ, Lewis SM, Auerbach EJ, Dorsey LL, Lojovich JM, Carey JR (2004) Electrical<br />
Stimulation driving functional improvements <strong>and</strong> cortical changes in subjects with stroke.<br />
Exp Brain Res 154:450-460.<br />
Kleim JA, Barbay S, Cooper NR, Hogg TM, Reidel CN, Remple MS, Nudo RJ (2002) Mo<strong>to</strong>r<br />
learning-dependent synap<strong>to</strong>genesis is localized <strong>to</strong> functionally reorganized mo<strong>to</strong>r cortex.<br />
Neurobiology <strong>of</strong> Learning <strong>and</strong> Memory 77:63-77.<br />
Klintsova AY, Dickson E, Yoshida R, Greenough WT (2004) Altered expression <strong>of</strong> BDNF <strong>and</strong><br />
its high-affinity recep<strong>to</strong>r TrkB in response <strong>to</strong> complex mo<strong>to</strong>r learning <strong>and</strong> moderate<br />
exercise. Brain Research 1028:92-104.<br />
Track-JBiomechEng.doc Page 24 <strong>of</strong> 31
Koeneman, E.J., R.S. Schultz, S.L. Wolf, D.E. Herring, J.B. Koeneman. (2004) A Pneumatic<br />
Muscle H<strong>and</strong> Therapy Device. in Proceedings <strong>of</strong> the 26th Annual International<br />
Conference <strong>of</strong> the IEEE EMBS.<br />
Kopp B, Kunkel A, Flor H, Platz T, Rose U, Mauritz KH, Gresser K, McCulloch KL, Taub E<br />
(1997) The Arm Mo<strong>to</strong>r Ability Test: reliability, validity, <strong>and</strong> sensitivity <strong>to</strong> change <strong>of</strong> an<br />
instrument for assessing disabilities in activities <strong>of</strong> daily living. Archives <strong>of</strong> Physical<br />
Medicine & Rehabilitation 78:615-620.<br />
Kramer AM, Kowalsky JC, Lin M, Grigsby J, Hughes R, Steiner JF (2000) Outcome <strong>and</strong><br />
utilization differences for older persons with stroke in HMO <strong>and</strong> fee-for-service<br />
systems.[see comment]. Journal <strong>of</strong> the American Geriatrics Society 48:726-734.<br />
Krebs, H.I., N. Hogan, M.L. Aisen, <strong>and</strong> B.T. Volpe, (1998)Robot Aided Neuro-rehabilitation,<br />
IEEE Transactions on Rehabilitation Engineering, 6:75-87.<br />
Lee TD, Genovese ED (1989). Distribution <strong>of</strong> practice in mo<strong>to</strong>r skill acquisition: different<br />
effects for discrete <strong>and</strong> continuous tasks. Research Quarterly for Exercise & Sport,<br />
60(1):59-65.<br />
Liepert J, Bauder H, Miltner WHR, Taub E, Weiller C (2000) Treatment-Induced Cortical<br />
Reorganization After Stroke in Humans. Stroke 31:1210-1216.<br />
Lu B (2004) Acute <strong>and</strong> long-term synaptic modulation by neurotrophins. Progress in Brain<br />
Research 146:137-150.<br />
Luft AR, McCombe-Waller S, Whitall J, Forrester LW, Macko R, Sorkin JD, Schulz JB,<br />
Goldberg AP, Hanley DF (2004) Repetitive bilateral arm training <strong>and</strong> mo<strong>to</strong>r cortex<br />
activation in chronic stroke - A r<strong>and</strong>omized controlled trial. Jama-Journal <strong>of</strong> the American<br />
Medical Association 292:1853-1861.<br />
Magill RA, Hall KG (1990) A review <strong>of</strong> the contextual interference effect in mo<strong>to</strong>r skill<br />
acquisition. Human Movement Science 9:241-289.<br />
Mathiowetz V, Voll<strong>and</strong> G, Kashman N, Weber K (1985) Adult norms for the Box <strong>and</strong> Block<br />
Test <strong>of</strong> manual dexterity. Am J Occup Ther 39:386-391.<br />
Miltner WH, Bauder H, Sommer M, Dettmers C, Taub E (1999) Effects <strong>of</strong> constraint-induced<br />
movement therapy on patients with chronic mo<strong>to</strong>r deficits after stroke: a replication.<br />
Stroke 30:586-592.<br />
Muellbacher W, Richards C, Ziemann U, Wittenberg G, Weltz D, Boroojerdi B, Cohen L,<br />
Hallett M (2002) Improving H<strong>and</strong> Function in Chronic Stroke. Arch Neurol 59:1278-1282.<br />
Murase N, Duque J, Mazzocchio R, Cohen LG (2004) Influence <strong>of</strong> interhemispheric<br />
interactions on mo<strong>to</strong>r function in chronic stroke. Annals <strong>of</strong> Neurology 55:400-409.<br />
Nagpal A, (2005) Finger tracking training versus movement training during brain<br />
reorganization <strong>and</strong> functional improvements in home-based stroke rehabilitation,<br />
Presented at American Physical Therapy Association III STEP Conference: Linking<br />
Movement Science <strong>and</strong> Intervention, July 2005, Salt Lake City.<br />
NIH (2004) Wearable Robots Help with Stroke Rehabilitation, Retrieved June 28, 2005, from<br />
http://www.nibib.nih.gov/eAdvances/121504.htm.<br />
Nudo R, Milliken G (1996) Reorganization <strong>of</strong> movement representations in primary mo<strong>to</strong>r<br />
cortex following focal ischemic infarcts in adult squirrel monkeys. J Neurophys 75:5:2144-<br />
2149.<br />
Nudo R, Friel K (1999) Cortical plasticity after stroke: Implications for rehabilitation. Rev<br />
Neurol (Paris) 155:713-717.<br />
Nudo R, Milliken G, Jenkins W, Merzenich M (1996a) Use-dependent alterations <strong>of</strong><br />
movement representations in primary mo<strong>to</strong>r cortex <strong>of</strong> adult squirrel monkeys. J Neurosci<br />
16(2):785-807.<br />
Nudo R, Wise B, SiFuentes F, Milliken G (1996b) Neural substrates for the effects <strong>of</strong><br />
rehabilitative training on mo<strong>to</strong>r recovery after ischemic infarct. Science 272:1791-1794.<br />
Oldfield R (1971) The assessment <strong>and</strong> analysis <strong>of</strong> h<strong>and</strong>edness: the Edinburgh inven<strong>to</strong>ry.<br />
Neuropsychologia 9(1):97-113.<br />
Track-JBiomechEng.doc Page 25 <strong>of</strong> 31
Page SJ, Sis<strong>to</strong> S, Levine P, McGrath RE (2004) Efficacy <strong>of</strong> modified constraint-induced<br />
movement therapy in chronic stroke: a single-blinded r<strong>and</strong>omized controlled trial. Arch<br />
Phys Med Rehabil 85:14-18.<br />
Pascual-Leone A, Grafman J, Hallett M (1994) Modulation <strong>of</strong> cortical mo<strong>to</strong>r output maps<br />
during development <strong>of</strong> implicit <strong>and</strong> explicit knowledge. Science 263:1287-1289.<br />
Pascual-Leone A, Nguyen KT, Cohen AD, Brasil-Ne<strong>to</strong> J, Cammarota A, Hallett M (1995)<br />
Modulation <strong>of</strong> muscle responses evoked by transcranial magnetic stimulation during the<br />
acquisition <strong>of</strong> new fine mo<strong>to</strong>r skills. J Neurophysiol 74:1037-1045.<br />
Piron L, Tonin P, Atzori AM, Zanotti E, Massaro C, Trivello E, Dam M (2002) Virtual<br />
environment system for mo<strong>to</strong>r tele-rehabilitation. Studies in Health Technology &<br />
Informatics 85:355-361.<br />
Ploughman M, Corbett D (2004) Can forced-use therapy be clinically applied after stroke? An<br />
explora<strong>to</strong>ry r<strong>and</strong>omized controlled trial.1417-1423.<br />
Reinkensmeyer DJ, Pang CT, Nessler JA, Painter CC (2002) Web-based telerehabilitation<br />
for the upper extremity after stroke. IEEE Transactions on Neural <strong>System</strong>s &<br />
Rehabilitation Engineering 10:102-108.<br />
Schmidt RA, Lee T (2005), Mo<strong>to</strong>r Control <strong>and</strong> Learning-A Behaviorial Emphasis, 4th ed.,<br />
Human Kinetics,<br />
Schmidt RA (1991) Frequent augmented feedback can degrade learning: Evidence <strong>and</strong><br />
interpretations. In: Tu<strong>to</strong>rials in mo<strong>to</strong>r neuroscience (Requin J, Stelmach G, eds), pp 59-<br />
75. Dordrecht, The Netherl<strong>and</strong>s: Kluwer Academic Publishers.<br />
Seitz RJ, Schlaug G, Kleinschmidt A, Knorr U, Nebeling B, Wirrwar A, Steinmetz H, Benecke<br />
R, H.J. F (1994) Remote depressions <strong>of</strong> cerebral metabolism in hemiparetic stroke:<br />
Topography <strong>and</strong> relation <strong>to</strong> mo<strong>to</strong>r <strong>and</strong> soma<strong>to</strong>sensory functions. Human Brain Mapping<br />
1:81-100.<br />
Shea JB, Zimney ST (1983) Context effects in memory <strong>and</strong> learning movement information.<br />
In R.A. Magill (Ed.). Amsterdam: North-Holl<strong>and</strong>.<br />
Shields RK, Leo KC, Messaros AJ, Somers VK (1999) Effects <strong>of</strong> repetitive h<strong>and</strong>grip training<br />
on endurance, specificity, <strong>and</strong> cross-education. Physical Therapy 79:467-475.<br />
Stern EB (1992) Stability <strong>of</strong> the Jebsen-Taylor H<strong>and</strong> Function Test across three test<br />
sessions. American Journal <strong>of</strong> Occupational Therapy 46:647-649.<br />
Taub E (1980) Soma<strong>to</strong>sensory deafferentation research with monkeys: Implications for<br />
rehabilitation medicine. In: Behavioral psychology in rehabilitation medicine: Clinical<br />
applications. (Ince L, ed), pp 371-401. New York: Williams & Wilkins.<br />
Taub E, Miller NE, Novack TA, Cook EWI, Fleming WC, Nepomuceno CS (1993) Technique<br />
<strong>to</strong> improve chronic mo<strong>to</strong>r deficit after stroke. Arch Phys Med Rehabil 74:347-354.<br />
Taub, E, Uswatte, G., & Pidikiti, R. (1999). Constraint-Induced Movement Therapy: A new<br />
family <strong>of</strong> techniques with broad application <strong>to</strong> physical rehabilitation—a clinical review. J.<br />
Rehab. Res. Devel., 36, 237-251.<br />
Taub, E, Uswatte, G. (2000). Constraint-Induced Movement Therapy <strong>and</strong> massed practice.<br />
Stroke, 31:983-c.<br />
Tilley A (2001), The Measure <strong>of</strong> Man <strong>and</strong> Woman: Human Fac<strong>to</strong>rs in <strong>Design</strong>, Wiley.<br />
Von Monakow C (1969) Diaschisis (1914 article translated by G. Harris). In: In: Brain <strong>and</strong><br />
Behavior I: Mood States <strong>and</strong> Mind. (Pribram KHe, ed), pp 27-36. Baltimore: Penguin.<br />
Weinstein S (2004), Guidelines for the <strong>Design</strong> <strong>of</strong> <strong>Home</strong> Telemedicine <strong>System</strong>s, MS Thesis,<br />
Department <strong>of</strong> Mechanical Engineering, University <strong>of</strong> Minnesota.<br />
Widen Holmqvist L, von Koch L, Kostulas V, Holm M, Widsell G, Tegler H, Johansson K,<br />
Almazan J, de Pedro-Cuesta J (1998) A r<strong>and</strong>omized controlled trial <strong>of</strong> rehabilitation at<br />
home after stroke in southwest S<strong>to</strong>ckholm.[see comment]. Stroke 29:591-597.<br />
Will B, Galani R, Kelche C, Rosenzweig MR (2004) Recovery from brain injury in animals:<br />
relative efficacy <strong>of</strong> environmental enrichment, physical exercise or formal training (1990-<br />
2002). Progress in Neurobiology 72:167-182.<br />
Winters JM (2004) A telehomecare model for optimizing rehabilitation outcomes.<br />
Telemedicine Journal & E-Health 10:200-212.<br />
Track-JBiomechEng.doc Page 26 <strong>of</strong> 31
Witte OW, S<strong>to</strong>ll G (1997) Delayed <strong>and</strong> remote effects <strong>of</strong> focal cortical infarctions: secondary<br />
damage <strong>and</strong> reactive plasticity. Advances in Neurology 73:207-227.<br />
Wulf G, Shea CH (2002) Principles derived from the study <strong>of</strong> simple skills do not generalize<br />
<strong>to</strong> complex skill learning. Psychonomic Bulletin & Review 9:185-211.<br />
Young JB, Forster A (1992) The Bradford community stroke trial: results at six months. BMJ<br />
304:1085-1089.<br />
Track-JBiomechEng.doc Page 27 <strong>of</strong> 31
Figure 1: Track<strong>Train</strong> home tracking system.<br />
Figure 2: H<strong>and</strong> sensor.<br />
Track-JBiomechEng.doc Page 28 <strong>of</strong> 31
LEFT<br />
SENSOR<br />
RIGHT<br />
SENSOR<br />
9V<br />
WALL<br />
SUPPLY<br />
Figure 3: Interface box.<br />
MCP6S26<br />
MUX<br />
MCP41100<br />
OFFSET<br />
5V<br />
VREG<br />
PWR<br />
2-POLE<br />
20 HZ<br />
FILTER<br />
Figure 4: Calibration (left) <strong>and</strong> pre-trial (right) screens.<br />
Figure 5: Tracking (left) <strong>and</strong> post-trial feedback (right) screens.<br />
Track-JBiomechEng.doc Page 29 <strong>of</strong> 31<br />
PIC16F873<br />
CONTROLLER<br />
MAX233<br />
LEVEL<br />
SHIFT<br />
BUTTO<br />
COMM<br />
PORT<br />
HOST PC
Table 1: Performance scores<br />
T = target trajec<strong>to</strong>ry, X = response trajec<strong>to</strong>ry, N = number <strong>of</strong> data points in record<br />
Metric <strong>and</strong> Name Computation Algorithm Interpretation<br />
E = Total Error = RMS Error<br />
1 / 2<br />
⎛ 1<br />
2 ⎞<br />
⎜ ∑( X i − Ti<br />
) ⎟<br />
⎝ N<br />
⎠<br />
RMS error between response <strong>and</strong><br />
target.<br />
CE = Constant Error = Average<br />
Error<br />
1<br />
∑( X i − Ti<br />
)<br />
N<br />
Average error between response<br />
<strong>and</strong> target. Reveals bias above or<br />
below target.<br />
VE = Variable Error = St<strong>and</strong>ard<br />
Deviation<br />
1/<br />
2<br />
⎛ 1<br />
2 ⎞<br />
⎜ ∑(<br />
X i − Ti<br />
− CE)<br />
⎟<br />
⎝ N<br />
⎠<br />
St<strong>and</strong>ard deviation <strong>of</strong> the<br />
response about the bias. Measure<br />
the spread <strong>of</strong> the response.<br />
CE/VE CE / VE<br />
>1 for response far from target<br />
but consistent, 0 means response lags target.<br />
Fade (First half RMS)/(Last half RMS) > 1 means response getting<br />
smaller as trial proceeds.<br />
Frequency (Zero crossings <strong>of</strong><br />
Large score means subject has<br />
response)/(Zero crossings <strong>of</strong><br />
target)<br />
tremor.<br />
Track-JBiomechEng.doc Page 30 <strong>of</strong> 31
Table 2: Tracking block conditions<br />
Parameter Units Conditions<br />
Wave Shape n/a triangle, left-saw, right-saw, square, pseudo-r<strong>and</strong>om<br />
Frequency Hz 0.2, 0.4, 0.8<br />
Duration Sec 5, 10, 15, 20<br />
Range % <strong>of</strong> ROM 0-50, 30-70, 50-100, 0-125<br />
Joint n/a wrist, finger<br />
Side n/a paretic, nonparetic<br />
Posture n/a pronated, supinated, mid<br />
Visual Feedback n/a on, <strong>of</strong>f<br />
Table 3: <strong>Usability</strong> survey results<br />
Questions N<br />
Track-JBiomechEng.doc Page 31 <strong>of</strong> 31<br />
Strongly<br />
Disagree Disagree<br />
No<br />
Opinion<br />
Agree<br />
Strongly<br />
Agree<br />
1. I unders<strong>to</strong>od how <strong>to</strong> use the system 19 9 10<br />
2. The computer was easy <strong>to</strong> use 19 9 10<br />
3. I was able <strong>to</strong> put on <strong>and</strong> take <strong>of</strong>f the h<strong>and</strong><br />
sensors by myself without problems<br />
19 1 4 10 4<br />
4. The physical system setup in my home<br />
interfered with my daily routine<br />
5. The scores <strong>and</strong> comments I received after<br />
each trial helped me<br />
6. It was easy for me <strong>to</strong> communicate with<br />
the therapist during a tele-session<br />
19 9 6 4<br />
19 3 1 14 1<br />
17 1 10 6