Anti TRANSGLUTAMINASI IgG EIA WELL R REF - Radim S.p.A.
Anti TRANSGLUTAMINASI IgG EIA WELL R REF - Radim S.p.A.
Anti TRANSGLUTAMINASI IgG EIA WELL R REF - Radim S.p.A.

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Anti</strong> <strong>TRANSGLUTAMINASI</strong> <strong>IgG</strong><br />
R <strong>REF</strong> K10TG<br />
<strong>EIA</strong> <strong>WELL</strong><br />
Italiano p. 3<br />
English p. 12<br />
96<br />
M412 – Rev.1 – 04/2008 – Pag. 1/24
REAGENTI DEL KIT - KIT REAGENTS<br />
Reag. Quant. Stato fisico,<br />
Physical state<br />
MTP 1 x 96<br />
Pronti per l'uso<br />
Ready for use<br />
WASH 1 x 50 mL Conc.<br />
DIL 1 x 100 mL<br />
CAL 5 x 2 mL<br />
CONJ 1 x 14 mL<br />
CTR 2 x 2 mL<br />
TMB 2 x 15 mL<br />
STOP 1 x 14 mL<br />
Pronto per l'uso<br />
Ready for use<br />
Pronti per l'uso<br />
Ready for use<br />
Pronto per l'uso<br />
Ready for use<br />
Pronti per l'uso<br />
Ready for use<br />
Pronto per l'uso<br />
Ready for use<br />
Pronto per l'uso<br />
Ready for use<br />
"Le Istruzioni per l'uso tradotte nelle altre lingue di interesse sono consultabili sul sito<br />
Internet all'indirizzo www.radim.com".<br />
“The instructions for use available in the other languages of interest can be viewed on our<br />
website www.radim.com".<br />
“Οι οδηγίες χρήσης μεταφρασμένες στις άλλες ενδιαφερόμενες γλώσσες όπως επίσης στην<br />
ηλεκτρονική διεύθυνση www.radim.com".<br />
“In den anderen Sprachen von Interesse ist die Bedienungsanleitung kann auf der Website<br />
unter der Adresse www.radim.com konsultiertwerden”.<br />
"Le mode d’emploi dans les autres langues intéressées est consultable sur le site Internet à<br />
l'adresse www.radim.com”.<br />
“Las instrucciones de uso traducidas en los otros idiomas de interés se pueden consultar en<br />
nuestro sitio Internet www.radim.com”.<br />
"As instruções de uso traduzidas nos outros idiomas de interesse podem ser consultadas<br />
no nosso site Internet, ao endereço www.radim.com."<br />
K10TG - <strong>Anti</strong>-Transglutaminasi <strong>IgG</strong> <strong>EIA</strong> <strong>WELL</strong><br />
M412 – Rev.1 – 04/2008 – Pag. 2/24
DOSAGGIO IMMUNOENZIMATICO PER LA DETERMINAZIONE<br />
QUANTITATIVA DEGLI ANTICORPI <strong>IgG</strong> ANTI-<strong>TRANSGLUTAMINASI</strong><br />
TISSUTALE NEL SIERO O PLASMA UMANO.<br />
PER USO DIAGNOSTICO IN VITRO<br />
1. APPLICAZIONI CLINICHE<br />
La malattia celiaca è un’affezione cronica caratterizzata sul piano clinico da una<br />
gamma estremamente variabile di disturbi digestivi (malassorbimento intestinale,<br />
diarrea), da ritardo della crescita e a volte da dermatite erpetiforme.<br />
A livello anatomo-patologico, la malattia è accompagnata da atrofia dei villi della<br />
mucosa dell’intestino tenue, ipertrofia delle cripte ed ipercellularità della mucosa.<br />
Come conseguenza del malassorbimento intestinale possono manifestarsi stati di<br />
deplezione di fattori nutritivi, causa ad esempio di anemia, dovuta a carenza di<br />
acido folico e vitamina B12. Inoltre individui con celiachia da lungo tempo,<br />
presentano un rischio elevato di sviluppare il linfoma delle cellule T.<br />
La frequenza delle malattia celiaca in Italia ed in Europa è stata stimata essere<br />
pari a 1/200-1/300 su un’ampia casistica di popolazione pediatrica. Tale incidenza<br />
risulta essere più elevata nella sindrome di Down e nel diabete giovanile insulinodipendente.<br />
La malattia celiaca si instaura a seguito di una intolleranza, mediata<br />
da meccanismi immunologici, nei confronti di proteine di alcuni cereali. In<br />
particolare la gliadina, frazione proteica solubile in alcool del glutine, è<br />
considerata la principale responsabile della tossicità della farina di grano nei<br />
confronti della mucosa intestinale dei pazienti celiaci. Finora la determinazione di<br />
anticorpi <strong>IgG</strong> e IgA anti-gliadina (ELISA) e la determinazione delle IgA antiendomisio<br />
(IFA) sono state considerate i principali parametri sierologici per la<br />
diagnosi della malattia celiaca. Nel 1977, è stato descritto da DIETERICH<br />
l’enzima Transglutaminasi tissutale (TGA) come il principale auto-antigene<br />
endomisiale, utilizzante la gliadina come substrato, verso cui sono diretti gli<br />
anticorpi IgA anti-endomisio. Numerosi studi effettuati successivamente hanno<br />
confermato l’elevata coincidenza nei celiaci di anticorpi anti-transglutaminasi di<br />
classe IgA e <strong>IgG</strong>, determinate mediante tecniche ELISA e le IgA anti-endomisio<br />
determinate in immunofluorescenza.<br />
Il dosaggio degli anticorpi di classe <strong>IgG</strong> assume particolare rilevanza nei casi di<br />
ridotta presenza di IgA, come nei bambini al di sotto dei 4 anni e nei pazienti con<br />
deficit di IgA.<br />
2. PRINCIPIO DEL METODO<br />
Il presente kit è basato sul metodo immunoenzimatico (ELISA) ed utilizza come<br />
marcatore enzimatico la perossidasi. Durante la prima incubazione, gli<br />
autoanticorpi anti-Transglutaminasi della classe <strong>IgG</strong>, eventualmente presenti nel<br />
siero in esame, si legano alla Transglutaminasi (ricombinante umana da<br />
Baculovirus) adesa alla superficie dei pozzetti. Tramite lavaggio viene eliminato il<br />
materiale non legato; in una successiva incubazione gli anticorpi anti-<strong>IgG</strong> umane,<br />
coniugati alla perossidasi, reagiscono con il complesso precedentemente<br />
K10TG - <strong>Anti</strong>-Transglutaminasi <strong>IgG</strong> <strong>EIA</strong> <strong>WELL</strong><br />
M412 – Rev.1 – 04/2008 – Pag. 3/24
formatosi tra antigene ed anticorpo anti-Transglutaminasi. Dopo ulteriore<br />
lavaggio, viene aggiunta tetrametilbenzidina (TMB) incolore che, reagendo con la<br />
perossidasi presente, produce un composto colorato. La reazione di sviluppo del<br />
colore è bloccata con l'aggiunta di H2SO4 e l'intensità del colore, misurata<br />
mediante spettrofotometro a 450 nm, è direttamente proporzionale alla<br />
concentrazione di anticorpi <strong>IgG</strong> anti-Transglutaminasi presenti nei calibratori, nei<br />
controlli e nei campioni in esame.<br />
3. REAGENTI CONTENUTI NEL KIT: PREPARAZIONE E STABILITA'<br />
− I reagenti sono sufficienti per 96 pozzetti.<br />
− Il kit deve essere conservato a 2-8°C.<br />
− La data di scadenza di ciascun reagente è indicata sulla rispettiva etichetta.<br />
− Una volta aperto il kit è stabile 1 mese a 2-8°C.<br />
3.1 Reagenti Specifici<br />
• MTP Micropiastra Sensibilizzata: 1 micropiastra da 96 pozzetti, separabili<br />
singolarmente, sensibilizzati con Transglutaminasi ricombinante umana da<br />
Baculovirus. I pozzetti non utilizzati devono essere conservati a 2°-8°C nella<br />
custodia di alluminio accuratamente sigillata.<br />
• CAL Calibratori: 5 flaconi contenenti <strong>IgG</strong> anti-Transglutaminasi in matrice<br />
sierica, alle seguenti concentrazioni: 0, 7, 25, 50 e 100 U/mL. Conservante:<br />
NaN3 (
4.1 Dosaggio Manuale<br />
− Micropipette automatiche a puntali intercambiabili a volume variabile.<br />
− Agitatore per micropiastre, regolabile a 1200 rpm.<br />
− Cilindri graduati per la diluizione dei reattivi.<br />
− Pompa aspirante oppure apparecchiatura automatica per il lavaggio delle<br />
micropiastre.<br />
− Spettrofotometro di precisione per micropiastre, con possibilità di misura in<br />
assorbanza nell'intervallo 0-3.0 A ad una lunghezza d'onda di 450 e 405 nm.<br />
− Carta millimetrata.<br />
− H2O distillata.<br />
4.2 Dosaggio Automatico<br />
− Il dispositivo può essere utilizzato con strumentazione automatica di kit ELISA<br />
su micropiastra.<br />
− Si garantisce l’applicabilità su strumentazione RADIM e/o SEAC<br />
− Qualora si utilizzi strumentazione automatica di altri fornitori, è responsabilità<br />
dell’utilizzatore assicurarsi che il kit sia stato opportunamente validato.<br />
5. AVVERTENZE E PRECAUZIONI<br />
Per ottenere risultati corretti e riproducibili, è necessario osservare le<br />
seguenti norme:<br />
− Non mescolare i reagenti specifici (vedi 3.1) di lotti differenti.<br />
− E’ possibile utilizzare reagenti comuni (vedi 3.2) di lotti differenti.<br />
− Non usare i reagenti dopo la data di scadenza.<br />
− Non esporre i reattivi e i campioni a calore intenso o a forti sorgenti di<br />
inquinamento.<br />
− Usare vetreria perfettamente pulita ed esente da contaminazioni di ioni<br />
metallici o sostanze ossidanti.<br />
− Usare acqua distillata o deionizzata, conservata in recipienti perfettamente<br />
puliti.<br />
− Evitare accuratamente contaminazioni tra campioni; a tal fine è consigliabile<br />
usare pipette con puntali monouso per ogni campione e per ogni reattivo.<br />
− Non modificare in alcun modo il Procedimento Operativo di esecuzione del<br />
test. Eventuale non rispetto di:<br />
• sequenza e quantità nell’aggiunta dei reattivi<br />
• tempi e temperatura di incubazione<br />
può dare luogo a risultati clinici errati.<br />
− Ricostituire gli eventuali reagenti liofili secondo le modalità descritte sulle<br />
etichette. Eventuale utilizzo di reattivi o volumi non idonei, può provocare<br />
l’ottenimento di dati clinici non attendibili.<br />
− In caso di procedura manuale è importante l’utilizzo di pipette calibrate e<br />
possedere un’adeguata manualità tecnica. In particolare è essenziale una<br />
K10TG - <strong>Anti</strong>-Transglutaminasi <strong>IgG</strong> <strong>EIA</strong> <strong>WELL</strong><br />
M412 – Rev.1 – 04/2008 – Pag. 5/24
uona precisione nella preparazione e dispensazione dei reattivi. E’<br />
necessario un adeguato piano di manutenzione (pulizia e calibrazione) di tale<br />
strumentazione.<br />
− Assicurarsi che la pompa di aspirazione oppure l’apparecchiatura automatica<br />
per il lavaggio delle micropiastre sia perfettamente funzionante. Un lavaggio<br />
non accurato delle micropiastre può dare luogo a misclassificazione dei<br />
campioni. E’ necessario un adeguato piano di manutenzione di tale<br />
strumentazione.<br />
− Assicurarsi che lo spettrofotometro per micropiastre sia perfettamente<br />
funzionante. L’utilizzo di uno spettrofotometro non calibrato o con filtri non<br />
puliti, può comportare un errore nella lettura dei campioni, con conseguente<br />
possibile misclassificazione degli stessi. E’ necessario un adeguato piano di<br />
manutenzione (pulizia e calibrazione) di tale strumentazione.<br />
− Assicurarsi che la stufa termostatata (se necessaria) sia perfettamente<br />
funzionante. L’incubazione a temperature diverse da 37±2°C può dare luogo a<br />
perdita di sensibilità e/o a denaturazione biologica dei materiali (reattivi e/o<br />
campioni). E’ necessario un adeguato piano di manutenzione di tale<br />
strumentazione e un controllo periodico della temperatura registrata.<br />
− Assicurarsi che l’agitatore per micropiastre (se necessario) sia perfettamente<br />
funzionante. L’agitazione in condizione diverse dall’atteso può dare luogo a<br />
misclassificazione dei campioni . E’ necessario un adeguato piano di<br />
manutenzione di tale strumentazione.<br />
− Assicurarsi che la strumentazione utilizzata per la conservazione dei campioni<br />
e/o del dispositivo sia perfettamente funzionante. La conservazione a<br />
temperature diverse dall’atteso, può dare luogo a denaturazione biologica dei<br />
materiali (reattivi e/o campioni). E’ necessario un adeguato piano di<br />
manutenzione di tale strumentazione e un controllo periodico della<br />
temperatura registrata.<br />
− Utilizzare un adeguato metodo per la corretta identificazione dei campioni.<br />
Possibili conseguenze possono essere sia la perdita di specificità del<br />
dispositivo che risultati analitici errati.<br />
Per evitare contaminazioni personali ed ambientali, è necessario osservare<br />
le seguenti norme di sicurezza:<br />
− Utilizzare guanti monouso durante la manipolazione di materiale<br />
potenzialmente infetto e durante il dosaggio.<br />
− Non pipettare i reagenti con la bocca.<br />
− Non fumare, mangiare, bere o applicare cosmetici durante l'esecuzione del<br />
dosaggio.<br />
− Le soluzioni di Cromogeno e Reagente Bloccante vanno manipolate con<br />
cautela. Evitare il contatto con la pelle, gli occhi e le mucose. In caso di<br />
incidente lavare abbondantemente con acqua.<br />
− I materiali di origine umana utilizzati nella preparazione del presente kit sono<br />
stati saggiati per la presenza di HBsAg, anti-HIV e anti-HCV e sono risultati<br />
ripetutamente negativi. Comunque nessun test attualmente disponibile<br />
garantisce l'assenza degli agenti virali responsabili della sindrome da<br />
K10TG - <strong>Anti</strong>-Transglutaminasi <strong>IgG</strong> <strong>EIA</strong> <strong>WELL</strong><br />
M412 – Rev.1 – 04/2008 – Pag. 6/24
immunodeficienza acquisita, dell'epatite B ed epatite C. Tutti i reagenti<br />
contenenti materiale biologico e tutti i campioni di siero umano devono essere<br />
considerati potenzialmente infettivi.<br />
− Evitare la produzione di schizzi e la formazione di aerosol; qualora ciò si<br />
verificasse ripulire accuratamente con ipoclorito di sodio ad una<br />
concentrazione del 3%. Il mezzo adoperato per la pulizia deve essere trattato<br />
come residuo potenzialmente infetto ed eliminato secondo le modalità<br />
opportune.<br />
− La sodio azide contenuta come conservante in alcuni reagenti, può reagire con<br />
il piombo ed il rame delle tubature formando azidi di metallo altamente<br />
esplosive. Per evitare l formazione e l'accumulo di tali composti far scorrere<br />
abbondante acqua sui reagenti eliminati.<br />
− Ai sensi del D.L. italiano n. 22 del 05.02.97, che fa riferimento alle direttive<br />
CEE (91/156/CEE, 91/689/CEE, 94/62/CEE) tutti i rifiuti provenienti da<br />
lavorazioni manuali e/o in automatico sono classificati rifiuti speciali pericolosi<br />
con codice di classificazione CER 180103; devono quindi essere eliminati<br />
affidandoli a ditte autorizzate al ritiro ed allo smaltimento.<br />
6. RACCOLTA E PREPARAZIONE DEI CAMPIONI<br />
Il dosaggio è effettuato su siero e plasma umano. Campioni fortemente lipemici o<br />
emolizzati possono alterare i risultati. La presenza di filamenti di fibrina può<br />
interferire nel dosaggio; assicurarsi pertanto che i campioni siano perfettamente<br />
limpidi prima di dosarli. I campioni possono essere conservati per un periodo non<br />
superiore ad una settimana se correttamente mantenuti a 2-8°C, a - 20°C per<br />
tempi più lunghi. Si consiglia di non congelare e scongelare ripetutamente i<br />
campioni.<br />
Prima dell'uso, diluire i campioni 1:100 con il Diluente dei Campioni (es. 10 µL di<br />
campione + 990 µL di diluente).<br />
7. PROCEDIMENTO OPERATIVO *<br />
− Attendere che i reagenti ed i campioni raggiungano la temperatura ambiente.<br />
− Agitare i campioni per inversione prima dell'uso.<br />
7.1 Preparare i pozzetti per: Bianco, Calibratori, Sieri di Controllo e Campioni.<br />
7.2 Dispensare 100 µL di Calibratori, Sieri di Controllo e Campioni<br />
precedentemente diluiti, nei rispettivi pozzetti.<br />
N.B.: i Calibratori ed i Sieri di Controllo non devono essere diluiti.<br />
7.3 Dispensare 100 µL di Diluente Campioni diluito nel pozzetto del Bianco.<br />
7.4 Incubare per 60±5 minuti in agitazione a 1200 rpm a temperatura<br />
ambiente (18-25°C), coprendo la micropiastra con il copripiastra adesivo<br />
fornito nel kit.<br />
7.5 Effettuare 4 lavaggi con un volume di 350 µL per pozzetto, impiegando la<br />
Soluzione di Lavaggio diluita. Aspirare accuratamente il liquido da tutti i<br />
pozzetti.<br />
K10TG - <strong>Anti</strong>-Transglutaminasi <strong>IgG</strong> <strong>EIA</strong> <strong>WELL</strong><br />
M412 – Rev.1 – 04/2008 – Pag. 7/24
7.6 Dispensare 100 µL di Coniugato Enzimatico in tutti i pozzetti.<br />
7.7 Incubare per 30±2 minuti in agitazione a 1200 rpm a temperatura<br />
ambiente (18-25°C), coprendo la micropiastra con il copripiastra adesivo<br />
fornito nel kit.<br />
7.8 Lavare i pozzetti come al punto 7.5.<br />
7.9 Dispensare 100 µL di Cromogeno in tutti i pozzetti.<br />
7.10 Incubare per 10 minuti in agitazione a 1200 rpm a temperatura ambiente<br />
(18-25°C), al riparo dalla luce.<br />
7.11 Dispensare 100 µL di Reagente Bloccante in tutti i pozzetti.<br />
7.12 Leggere la densità ottica delle soluzioni a 450 nm in uno spettrofotometro<br />
preferibilmente bicromatico con lunghezza d'onda di riferimento a 620 nm<br />
(azzerando lo strumento con il Bianco). Nel caso di estinzione in overflow,<br />
utilizzare la lettura spettrofotometrica a 405 nm. La lettura deve essere<br />
effettuata entro 15 minuti dal termine del dosaggio.<br />
* Qualora si utilizzasse nel procedimento operativo uno strumento automatico per<br />
micropiastre RADIM e/o SEAC, far riferimento al relativo manuale.<br />
8. SCHEMA DEL DOSAGGIO: vedi p. 22<br />
9. CALCOLO DEI RISULTATI *<br />
Disegnare la curva su carta millimetrata, riportando sull'asse delle ascisse le<br />
concentrazioni dei calibratori e su quello delle ordinate l'assorbanza ottenuta per<br />
ciascun calibratore. Interpolando sulla curva di calibrazione le assorbanze relative<br />
ai sieri di controllo e a ciascun campione, si otterranno le corrispondenti<br />
concentrazioni di <strong>IgG</strong> anti-Transglutaminasi, espresse in U/mL.<br />
* Nel caso si utilizzi uno strumento automatico per micropiastre RADIM e/o SEAC,<br />
la lettura spettrofotometrica è eseguita automaticamente a 3 lunghezze d'onda:<br />
450, 405 e 620 nm, permettendo l'ampliamento del range di lettura.<br />
9.1 Esempio di Calcolo<br />
I valori sotto riportati debbono essere considerati unicamente un esempio e non<br />
devono essere utilizzati in luogo dei dati sperimentali.<br />
Descrizione Assorbanza 450 nm <strong>IgG</strong><br />
anti-<br />
Transglutaminasi<br />
Calibratore 0 U/mL 0.003<br />
Calibratore 7 U/mL 0.565<br />
Calibratore 25 U/mL 1.640<br />
K10TG - <strong>Anti</strong>-Transglutaminasi <strong>IgG</strong> <strong>EIA</strong> <strong>WELL</strong><br />
M412 – Rev.1 – 04/2008 – Pag. 8/24
Calibratore 50 U/mL 3.150<br />
Calibratore 100 U/ml 5.350<br />
Siero Controllo Negativo 0.250 3.1 U/ml<br />
Siero Controllo Positivo 1.900 29.3 U/ml<br />
Campione 1 0.151 1.8 U/mL<br />
Campione 2 2.800 44.2 U/mL<br />
Interpolando sulla curva di calibrazione, i campioni dosati risultano avere<br />
rispettivamente un titolo di <strong>IgG</strong> anti-Tranglutaminasi di 1.80 e 44.2 U/mL.<br />
9.2 Criteri di Accettazione<br />
Prima di procedere al calcolo dei risultati verificare che le dosi dei controlli<br />
rientrino nei range riportati sul Certificato di Controllo Qualità allegato al kit.<br />
Se i valori ottenuti non rispecchiano quelli attesi, è necessario ripetere il dosaggio.<br />
9.3 Interpretazione dei Risultati<br />
I sieri di soggetti non celiaci presentano valori di <strong>IgG</strong> anti-Transglutaminasi<br />
inferiori a 7 U/ml. I campioni con valori di <strong>IgG</strong> compresi tra 5-7 U/ml sono da<br />
considerare di dubbia interpretazione e devono essere dosati nuovamente per<br />
conferma.<br />
Valori normali: ≤ 5 U/ml<br />
Zona grigia: 5-7 U/ml<br />
Valori patologici: ≥ 7 U/ml<br />
10. CARATTERISTICHE METODOLOGICHE<br />
10.1 Specificità Clinica<br />
La specificità clinica del metodo è stata valutata su un campione rappresentativo<br />
di soggetti non celiaci, risultando pari a 100%.<br />
10.2 Sensibilità Clinica<br />
La sensibilità clinica del metodo è stata valutata su un campione rappresentativo<br />
di soggetti positivi agli anticorpi <strong>IgG</strong> anti-transglutaminasi, risultando pari a 95%.<br />
10.3 Specificità Analitica<br />
Il presente metodo analitico non ha mostrato interferenze con sieri positivi a<br />
patologie autoimmuni sistemiche .<br />
10.4 Sensibilità Analitica<br />
La sensibilità analitica del metodo è definita come minima dose significativamente<br />
distinguibile dal calibratore zero. E’ stata valutata dispensando 10 replicati del<br />
calibratore zero e leggendo la media delle D.O.+2 D.S. sulla curva di calibrazione.<br />
La sensibilità analitica è risultata pari a 0.24 U/ml.<br />
10.5 Precisione<br />
K10TG - <strong>Anti</strong>-Transglutaminasi <strong>IgG</strong> <strong>EIA</strong> <strong>WELL</strong><br />
M412 – Rev.1 – 04/2008 – Pag. 9/24
La precisione é stata valutata misurando la variabilità intra-saggio ed inter-saggio<br />
su 3 sieri a differenti concentrazioni di <strong>IgG</strong> anti-Tranglutaminasi.<br />
Intra-saggio<br />
Inter-saggio<br />
Sieri Media<br />
(U/ml)<br />
D.S. C.V. Replicati<br />
A1 14.7 1.1 7.5% 10<br />
A2 33.2 1.7 5.0% 10<br />
A3 39.2 2.3 5.9% 10<br />
Sieri Media<br />
(U/ml)<br />
D.S. C.V. Dosaggio<br />
A1 7.2 0.6 7.9% 12<br />
A2 12 0.9 7.8% 12<br />
A3 31.3 1.9 6.2% 12<br />
10.6 Accuratezza<br />
L’accuratezza è stata valutata effettuando prove di Parallelismo e Recupero.<br />
Si è ritenuto indispensabile effettuare le prove su un numero vasto di campioni<br />
considerando sia la variabilità che l’eterogeneità degli anticorpi di classe G<br />
presente nei sieri come fattori che influenzano la risposta e la concordanza tra<br />
atteso e misurato.<br />
Test di Parallelismo<br />
La prova di parallelismo è stata effettuata considerando due sieri a<br />
concentrazione nota di anticorpi <strong>IgG</strong> anti-transglutaminasi diluiti nello Zero<br />
standard.<br />
Atteso Misurato %<br />
S1 78.0<br />
1:2 39.0 43.7 112<br />
1:4 19.5 24.2 124<br />
1:8 9.8 13.1 133<br />
Atteso Misurato %<br />
S2 44.1<br />
1:2 22.0 28.4 129<br />
1:4 11.0 14.9 135<br />
1:8 5.5 6.3 114<br />
K10TG - <strong>Anti</strong>-Transglutaminasi <strong>IgG</strong> <strong>EIA</strong> <strong>WELL</strong><br />
M412 – Rev.1 – 04/2008 – Pag. 10/24
Test di Recupero<br />
Il test di Recupero è stato allestito considerando due sieri a concentrazione nota<br />
diluiti secondo un rapporto 1:2 con i punti della curva standard.<br />
Atteso Misurato %<br />
S1 25.0<br />
‘+7U (1/2) 16.0 18.0 112<br />
‘+25U (1/2) 25 24.8 99<br />
‘+50U (1/2) 37.5 41.1 109<br />
Atteso Misurato %<br />
S2 7.0<br />
‘+7U (1/2) 7.0 7.5 106<br />
‘+25U (1/2) 16 21.1 132<br />
‘+50U (1/2) 28.5 37.5 131<br />
11. LIMITI DEL DOSAGGIO<br />
Come per qualsiasi procedura analitica la diagnosi di un paziente non può essere<br />
fatta in base al risultato di un singolo dosaggio.<br />
I risultati ottenuti da questo metodo immunoenzimatico contribuiscono alla<br />
diagnosi ma non ne costituiscono l’unico elemento nella pratica clinica.<br />
12. LEGENDA SIMBOLI: vedi p. 20<br />
ENZYME IMMUNOASSAY FOR QUANTITATIVE DETECTION OF TISSUE<br />
TRANSGLUTAMINASE IgA ANTIBODIES IN HUMAN SERUM OR PLASMA.<br />
1. CLINICAL APPLICATIONS<br />
FOR IN VITRO DIAGNOSTIC USE ONLY<br />
K10TG - <strong>Anti</strong>-Transglutaminasi <strong>IgG</strong> <strong>EIA</strong> <strong>WELL</strong><br />
M412 – Rev.1 – 04/2008 – Pag. 11/24
The celiac disease is a chronic pathology, characterized by several<br />
gastroenterological disorders (intestinal malabsorption, diarrhea), as well as<br />
growth retardation and dermatitis herpetiformis.<br />
Anatomically speaking, celiac disease is accompanied by villous atrophy of the<br />
small bowel mucosa, hypertrophic crypts and also excessive amounts of mucosal<br />
cells. The intestinal malabsorption can lead to depauperation of nutrient factors,<br />
as anemia caused by deficiency of folic acid and vitamin B12. Moroever subjects<br />
with celiac disease for long time have a high risk to develop the cell T lymphoma.<br />
In Italy and in Europe the celiac disease frequency is 1/200-1/300, estimated on<br />
wide casuistry of paediatric population. This incidence is higher in the Down<br />
syndrome and in the juvenile-onset diabetes. The celiac disease is an intolerance<br />
to some cereal proteins, mediated by immunological mechanisms. Particularly the<br />
gliadin, which is an alcohol soluble proteic fraction of gluten, is the main<br />
responsable for the wheatmeal toxicity in gluten/sensitive subjects. Up to now the<br />
main diagnosis of celiac disease was obteined by quantitative testing of both antigliadin<br />
<strong>IgG</strong> and IgA antibodies (ELISA) and of anti-endomysium IgA antibodies<br />
(IFA). In 1977, DIETERICH described the tissue Transglutaminase enzyme (TGA)<br />
as the main endomysial auto-antigen. As substrate this enzyme uses the gliadin,<br />
which represents the target of anti-endomysium IgA antibodies. Subsequent<br />
several studies have confirmed the high correlation between the antitransglutaminase<br />
IgA antibodies, performed by ELISA methods, and the antiendomysium<br />
IgA antibodies, performed by IFA methods.<br />
<strong>Anti</strong>-Transglutaminase <strong>IgG</strong> antibodies test has significance in case of a reduce<br />
presence of IgA such as in children under 4 years old and IgA deficit desease<br />
2. PRINCIPLE OF THE ASSAY<br />
This kit is based upon an enzyme immunoassay method (ELISA), where<br />
horseradish peroxidase is used as enzyme tracer. During the first incubation, the<br />
sample anti-Transglutaminase <strong>IgG</strong> antibodies, if any, are bound to the<br />
Transglutaminase (human recombinant from Baculovirus) coated wells. A wash<br />
cycle eliminates unbound material. In the incubation that follows, a second<br />
antibody (conjugated with horseradish peroxidase) will bind to the<br />
Transglutaminase-antigen-antibody complex. After a further wash cycle the<br />
colorless tetramethylbenzidine (TMB) is added to the wells, where it yields a<br />
colored compound, by reacting with the peroxidase enzyme. Color development<br />
will be stopped by adding H2SO4.The color intensity, measured in a<br />
spectrophotemeter at 450 nm, will thus be directly proportional to the antitransglutaminase<br />
<strong>IgG</strong> antibody concentration in calibrators, control sera and<br />
samples.<br />
3. REAGENTS PROVIDED WITH THE KIT> PREPARATION AND STABILITY<br />
− The reagents are sufficient for 96 wells.<br />
− Store the kit at 2-8°C.<br />
− The expiry date of each reagent is shown on the vial label.<br />
K10TG - <strong>Anti</strong>-Transglutaminasi <strong>IgG</strong> <strong>EIA</strong> <strong>WELL</strong><br />
M412 – Rev.1 – 04/2008 – Pag. 12/24
− Once opened the kit is stable at 2-8°C for 1 month.<br />
3.1 Specific Reagents<br />
• MTP Coated Microplate: 1 microplate for 96 breakable wells, coated with<br />
human recombinant Transglutaminase from Baculovirus. Keep unused wells at<br />
2-8°C in the provided plastic bag and accurately sealed.<br />
• CAL Calibrators: 5 vials containing anti-Transglutaminase <strong>IgG</strong> in serum<br />
matrix, at the following concentrations: 0, 7, 25, 50 and 100 U/mL.<br />
Preservative: NaN3 (
− This test can be used with automatic instrument for ELISA kits on microplate.<br />
− We guarantee its applications on RADIM and/or SEAC automatic instruments.<br />
− While using a non RADIM or SEAC automatic instrument for microplate, it is<br />
under end user responsibility, to make sure that it was appropriately tested for<br />
ELISA kits.<br />
5. WARNINGS AND PRECAUTIONS<br />
In order to obtain correct and reproducible results, the following rules must<br />
be observed:<br />
− Do not mix specific reagents (see 3.1) from different lots.<br />
− It is possible to mix common reagents (see 3.2) from different lots.<br />
− Do not use reagents beyond their expiry date.<br />
− Do not store or leave reagents and samples at high temperatures or areas of<br />
possible contamination.<br />
− Use thoroughly clean glassware, free from metal ion contamination or oxidizing<br />
substances.<br />
− Use distilled or deionized water, stored in perfectly clean containers.<br />
− Carefully avoid any contamination among samples; for this purpose,<br />
disposable tips should be used for each sample and reagent.<br />
− Do not modify in any way the "Assay Procedure". If you not respect:<br />
• exact incubation times and quantities adding the reagents<br />
• incubation times and temperature<br />
may cause incorrect clinical results.<br />
− Reconstitute lyophilized reagents, if present, as described on the relative<br />
labels. Any deviation in reagent use or wrong volumes, may affect the reliability<br />
of results obtained.<br />
− In case of manual procedure, it is important to use calibrated pipettes and<br />
have appropriate technical manuals. Primary importance is a good precision<br />
preparing and dispensing the reagents. Ensure that all the equipment used is<br />
in perfect working order, has been correctly calibrated and is regularly<br />
maintained.<br />
− Ensure that the aspiration pump or automated well washing device is in perfect<br />
working order. Inadequate rinsing of wells may cause an incorrect samples<br />
classifications. Ensure that all the equipment used is in perfect working order.<br />
− Ensure that the microplate spectrophotometer is in perfect working order. The<br />
use of a not calibrated spectrophotometer or not clean filters may cause a<br />
wrong reading samples with consequent incorrect samples classifications.<br />
Ensure that all the equipment used is in perfect working order.<br />
− Ensure that the dry heater (if necessary) is in perfect working order. The<br />
incubation temperature different from 37±2°C may cause a sensitivity losses<br />
and/or biological denaturation (samples and/or reagents). Ensure that the<br />
equipment used is in perfect working order and periodically check the recorded<br />
temperature.<br />
K10TG - <strong>Anti</strong>-Transglutaminasi <strong>IgG</strong> <strong>EIA</strong> <strong>WELL</strong><br />
M412 – Rev.1 – 04/2008 – Pag. 14/24
− Ensure that the microplate shaker (if necessary) is in perfect working order.<br />
Incorrect agitation may cause wrong samples classifications. Ensure that the<br />
equipment used is in perfect working order.<br />
− Ensure that all the equipment used for samples storage and/or the system is in<br />
perfect working order. The storage at different suggested temperature may<br />
cause biological material denaturation (samples and/or reagents). Ensure that<br />
the equipment used is in perfect working order and periodically check the<br />
recorded temperature.<br />
− Utilise a suitable method for the correct identification of patient samples.<br />
Incorrect identification may cause a specificity losses of the system and wrong<br />
clinical results.<br />
In order to avoid personal and environmental contamination, the following<br />
precautions must be observed:<br />
− Use disposable gloves while handling potentially infectious material and while<br />
performing the assay.<br />
− Do not pipette reagents by mouth.<br />
− Do not smoke, eat, drink or apply cosmetics during the assay.<br />
− Chromogen and Blocking Reagent should be handled with care. Avoid contact<br />
with skin, eyes and mucous membranes. In case of accident rinse thoroughly<br />
with running water.<br />
− All material of human origin used for the preparation of this kit tested negative<br />
for HBsAg, anti-HIV and anti-HCV. Since no test at present can guarantee<br />
complete absence of these viruses, all samples and reagents containing<br />
biological material used for the assay must be considered potentially<br />
infectious.<br />
− Avoid splashing and aerosol formation; in such cases, carefully wash with a<br />
3% sodium hypochlorite solution. Any such cleaning material must be treated<br />
as potentially infectious and disposed of accordingly.<br />
− Some reagents contain sodium azide as preservative; to prevent build-up of<br />
explosive metal azides in lead and copper plumbing, reagents should be<br />
discarded by flushing the drain with large amounts of water.<br />
− According to Italian decree D.L. no. 22 dated 05.02.97, in compliance with<br />
EEC directives (91/156/EEC, 91/689/EEC, 94/62/EEC), all waste products<br />
originating from either manual and/or automated processing are classified as<br />
hazardous special waste material (European classification code180103). As<br />
such, they must be eliminated by delegating to special enterprises, qualified for<br />
waste collection and disposal.<br />
6. SPECIMEN COLLECTION AND PREPARATION<br />
The assay can be performed in serum or plasma samples. Highly lipemic or<br />
hemolyzed samples may affect the results. The presence of fibrin filaments could<br />
interfere with the assay; make sure that samples are always perfectly clear before<br />
testing. Keep samples properly stored at 2-8°C for 1 week; for longer periods it is<br />
K10TG - <strong>Anti</strong>-Transglutaminasi <strong>IgG</strong> <strong>EIA</strong> <strong>WELL</strong><br />
M412 – Rev.1 – 04/2008 – Pag. 15/24
advisable to freeze samples at -20°C. Repeated freezing and thawing of samples<br />
should be avoided.<br />
Before use, dilute samples 1:100 with Sample Diluent (example: 10 µL sample +<br />
990 µL Sample Diluent).<br />
7. ASSAY PROCEDURE *<br />
− Allow reagents and samples to warm up at room temperature.<br />
− Mix samples by inversion before use.<br />
7.1 Prepare the wells for: Blank, Calibrators, Controls and Samples.<br />
7.2 Pipette 100 µL of Calibrators, Controls and diluted Samples into the<br />
corresponding wells.<br />
Note: Calibrators and Controls must not be diluted.<br />
7.3 Pipette 100 µL of Sample Diluent into the Blank well.<br />
7.4 Cover the microplate with adhesive sheet (supplied with the kit) and<br />
incubate for 60±5 minutes at 1200 rpm at room temperature (18-25°C).<br />
7.5 Wash the wells 4 times with 350 µL of diluted Washing Solution. Aspirate all<br />
liquid from the wells.<br />
7.6 Add 100 µL of Enzyme Conjugate into all wells.<br />
7.7 Cover the microplate with adhesive sheet (supplied with the kit) and<br />
incubate for 30±2 minutes at 1200 rpm at room temperature (18-25°C).<br />
7.8 Wash the wells as described in point 7.5.<br />
7.9 Pipette 100 µL of Chromogen into all wells.<br />
7.10 Incubate the wells for 10 minutes at 1200 rpm at room temperature (18-<br />
25°C). Avoid direct light exposure.<br />
7.11 Pipette 100 µL of Blocking Reagent into all wells.<br />
7.12 Read the absorbance of the wells with a preferably bichromatic<br />
spectrophotometer at 450 nm, with reference wavelength at 620 nm (setting<br />
the instrument at zero with the Blank well). In case of overflow absorbance<br />
values, read at 405 nm. Reading must be completed within 15 minutes from<br />
the end of the assay.<br />
* While using for the procedure a RADIM and/or SEAC automatic instrument for<br />
microplates, refer to its relative manual.<br />
8. ASSAY SCHEME: see p. 22<br />
9. CALCULATION OF RESULTS *<br />
Draw a calibration curve on millimetric graph-paper, by plotting the calibrator<br />
concentrations (x-axis) against their relative absorbances (y-axis). Corresponding<br />
anti-Transglutaminase <strong>IgG</strong> concentrations in U/mL are obtained by interpolating<br />
the absorbances of each sample on the calibration curve.<br />
K10TG - <strong>Anti</strong>-Transglutaminasi <strong>IgG</strong> <strong>EIA</strong> <strong>WELL</strong><br />
M412 – Rev.1 – 04/2008 – Pag. 16/24
* While using a RADIM and/or SEAC automatic instrument for microplates, the<br />
spectrophotometric reading will be performed automatically at 3 different<br />
wavelengths: 450, 405 and 620 nm, thereby allowing a wider curve range.<br />
9.1 Calculation Example<br />
The following values must be considered as an example and should not be used<br />
in place of experimental data.<br />
Description Absorbance 450 nm <strong>Anti</strong>-<br />
Transglutaminase<br />
<strong>IgG</strong><br />
Calibrator 0 U/mL 0.003<br />
Calibrator 7 U/mL 0.565<br />
Calibrator 25 U/mL 1.640<br />
Calibrator 50 U/mL 3.150<br />
Calibrator 100 U/ml 5.350<br />
Negative Control Serum 0.250 3.1 U/ml<br />
Positive Control Serum 1.900 29.3 U/ml<br />
Sample 1 0.151 1.8 U/mL<br />
Sample 2 2.800 44.2 U/mL<br />
By interpolation, the tested sample will have an anti-Transglutaminase <strong>IgG</strong> titer of<br />
1.80 and 44.2 U/mL.<br />
9.2 Validation Criteria<br />
Before proceeding in calculating the results, make sure the control concentrations<br />
are included within the values described on the Quality Control sheet.<br />
If the values obtained are not as expected, it will be necessary to repeat the<br />
assay.<br />
9.3 Interpretation of Results<br />
Subjects samples without celiac disease show anti-Transglutaminase <strong>IgG</strong> levels<br />
below 7 U/ml. The samples with <strong>IgG</strong> levels included in the range 5-7 U/ml should<br />
be considered border line and should be repeated to confirm the results.<br />
Normal values: ≤ 5 U/ml<br />
Border line: 5-7 U/ml<br />
Pathological<br />
values:<br />
≥ 7 U/ml<br />
10. PERFORMANCES OF THE ASSAY<br />
10.1 Clinical Specificity<br />
K10TG - <strong>Anti</strong>-Transglutaminasi <strong>IgG</strong> <strong>EIA</strong> <strong>WELL</strong><br />
M412 – Rev.1 – 04/2008 – Pag. 17/24
The clinical specificity of the method was evaluated on a representative group of<br />
patients diagnosed as free from coelic disease. The result is 100%.<br />
10.2 Clinical Sensitivity<br />
The clinical sensitivity of the method was evaluated on a representative group of<br />
individuals suffering from coelic disease. The result is 95%.<br />
10.3 Analytical Specificity<br />
This analitycal method shows no interferences with patients positive for<br />
autoimmune disease.<br />
10.4 Analytical Sensitivity<br />
The analytical sensitivity is expressed as the minimal dose showing a significant<br />
difference from the zero calibrator. It has been checked by pipetting 10 replicates<br />
of zero calibrator and reading O.D. mean value + 2 S.D. upon the calibration<br />
curve. This dose is 0.24 U/mL.<br />
10.5 Precision<br />
Precision has been evaluated determining the repeatability and the reproducibility<br />
of the assay (intra- and inter-assay variability), on 3 sera at different anti-<br />
Transglutaminase <strong>IgG</strong> concentrations.<br />
Repeability (Intra-assay)<br />
Serum Mean<br />
(U/ml)<br />
S.D. C.V. Replicates<br />
A1 14.7 1.1 7.5% 10<br />
A2 33.2 1.7 5.0% 10<br />
A3 39.2 2.3 5.9% 10<br />
Reproducibility (Inter-assay)<br />
Serum Mean<br />
(U/ml)<br />
S.D. C.V. Assay<br />
A1 7.2 0.6 7.9% 12<br />
A2 12 0.9 7.8% 12<br />
A3 31.3 1.9 6.2% 12<br />
10.6 Accuracy<br />
Accuracy of the method has been checked by the recovery and parallelism tests.<br />
Recovery test<br />
Two sera at known concentration of <strong>IgG</strong> were diluted 1:2 with the calibrators and<br />
tested<br />
Expected Measured %<br />
S1 25.0<br />
‘+7U(1/2) 16.0 18.0 112<br />
K10TG - <strong>Anti</strong>-Transglutaminasi <strong>IgG</strong> <strong>EIA</strong> <strong>WELL</strong><br />
M412 – Rev.1 – 04/2008 – Pag. 18/24
‘+25(1/2) 25 24.8 99<br />
‘+50(1/2) 37.5 41.1 109<br />
Expected Measured %<br />
S2 7.0<br />
‘+7U(1/2) 7.0 7.5 106<br />
‘+25(1/2) 16 21.1 132<br />
‘+50(1/2) 28.5 37.5 131<br />
Parallelism test<br />
Two sera with high <strong>IgG</strong> content were tested at different dilutions with the Zero<br />
standard:<br />
Expected Measured %<br />
S1 78.0<br />
1:2 39.0 43.7 112<br />
1:4 19.5 24.2 124<br />
1:8 9.8 13.1 133<br />
Expected Measured %<br />
S2 44.1<br />
1:2 22.0 28.4 129<br />
1:4 11.0 14.9 135<br />
1:8 5.5 6.3 114<br />
11. LIMITATION OF THE PROCEDURE<br />
As with all diagnostic tests, a definite clinical diagnosis should not be based<br />
on the results of a single test, but should only be made by the physician after<br />
all clinical and laboratory findings have been evaluated<br />
12. SYMBOLS LEGEND: see p. 20<br />
K10TG - <strong>Anti</strong>-Transglutaminasi <strong>IgG</strong> <strong>EIA</strong> <strong>WELL</strong><br />
M412 – Rev.1 – 04/2008 – Pag. 19/24
SIMBOLI, SYMBOLS, SYMBOLES, SÍMBOLOS, SÍMBOLOS, SYMBOLE,<br />
ΣΥΜΒΟΛΑ, SYMBOLIT, SYMBOLER<br />
EN 980 - EDMA<br />
<strong>REF</strong> Codice di riferimento o di ordine / reference or order code / Référence<br />
ou numéro de commande / referencia o número de pedido / referência<br />
ou número da encomenda / Referenz oder Bestellnummer / κωδικός<br />
προϊόντος ή παραγγελίας / Refarans veye sipariş numarsı / referenční<br />
nebo objednací číslo<br />
LOT Lotto / lot / Lot / lote / lote / charge / παρτίδα / parti / šarže<br />
IVD<br />
Data di scadenza / expiry date / date d’expiration / Fecha de<br />
caducidad / Data de vencimento / Verfallsdatum / Ηµεροµηνία λήξης /<br />
Son kullanma targhi / datum expirace<br />
Per uso diagnostico in-vitro / For in-vitro diagnostic use / Pour<br />
diagnostic in-vitro / Para uso diagnóstico In-vitro / aplicação do<br />
diagnóstico In-vitro / Für den Gebrauch in der IN-VITRO-DIAGNOSTIK<br />
/ για in vitro διαγνωστική χρήση / in –vitro diagnostik kullanım / pro<br />
použití in-vitro<br />
Marcatura CE secondo le direttive IVD 98/79/CE / CE marking<br />
according to IVD guidelines 98/79/EC / marquage CE conforme aux<br />
directives IVD 98/79/EC / marcado CE según directiva de IVD<br />
98/79/CE / marcação-CE segundo a directriz-IVD 98/79/CE / CE-<br />
Markierung bei Erfüllung der IVD Richtlinie 98/79/EG / Σηµανση CE<br />
βάσει κοινοτικής οδηγίας IVD 98/79/EC / 98/79/EC IVD tüzüğüne göre<br />
CE işareti / CE označení dle IVD 98/79/EU<br />
Conservare a 2-8°C / keep at 2-8°C / conserver à 2-8°C / Conservar a<br />
2-8°C / conservar a 2-8°C / Lagerung bei 2-8°C / φύλαξη στους 2-8°C<br />
/ 2-8°C da saklayınız / skladovat při 2-8°C<br />
Fabbricante / Manufacturer / Fabriquant / produzido por / Fabricante /<br />
produkt der / κατασκευάζεται από / tarafından üretilmiştir / výrobce<br />
Rischio biologico / Biohazard / Risque Biologique / Riesgo Biológico /<br />
Risco Biológico / Bιολογικός κίνδυνος / Riziko tehlike biyolojik/<br />
Biologicky nebezpečné<br />
Consultare la metodica operativa / consult instructions for use /<br />
consulter le mode opératoire / consultar las instrucciones de uso /<br />
consultar as instruções de uso / Schauen Sie die Arbeitsanleitung an /<br />
συμβουλευτείτε τις οδηγίες χρήσης / kullanımda başvurulacak bilgiler /<br />
Sledujte návod k použití<br />
K10TG - <strong>Anti</strong>-Transglutaminasi <strong>IgG</strong> <strong>EIA</strong> <strong>WELL</strong><br />
M412 – Rev.1 – 04/2008 – Pag. 20/24
96<br />
RDATE<br />
RCNS<br />
H2O<br />
Sufficiente per 96 test / sufficient for 96 tests / suffisant pour 96<br />
déterminations / suficiente para 96 determinaciones / Componentes<br />
para 96 testes / genügend für 96 Tests / επαρκεί για 96 τεστ / 96 test<br />
için yeterli / dostačující pro 96 testů<br />
Data di Riferimento / Reference date / Date de référence / Fecha de<br />
referencia / Data de refêrencia / Referenzdatum / ημερομηνία<br />
βαθμονόμησης / Referans Targhi / referenční datum<br />
Ricostituire con / reconstitute with / reconstituer avec / reconstituir con<br />
/ reconstituir com / rekonstituiren mit / ανασυστάται με / ile karıştırma /<br />
rekonstituovat<br />
Acqua distillata o deionizzata / deionized or distilled water / eau<br />
deionisée ou distillée / agua destilada o desionizada / água destilada<br />
ou deionizada / Deionisiertes oder Destilliertes Wasser / απιονισμένο -<br />
απεσταγμένο νερό / deiyonize veya distile su / deionizovaná nebo<br />
destilovaná voda<br />
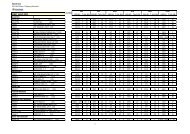
SCHEMA DEL DOSAGGIO-ASSAY SCHEME<br />
K10TG - <strong>Anti</strong>-Transglutaminasi <strong>IgG</strong> <strong>EIA</strong> <strong>WELL</strong><br />
M412 – Rev.1 – 04/2008 – Pag. 21/24
Prediluizione del campione, Sample predilution: 1/100.<br />
Pozzetti<br />
Wells<br />
Bianco,<br />
Blank<br />
CAL<br />
(1-5)<br />
CTR Campioni,<br />
Samples<br />
Reag<br />
CAL --- 100 µL --- ---<br />
CTR --- --- 100 µL ---<br />
Campioni, Samples --- --- --- 100 µL<br />
DIL 100 µL --- --- ---<br />
− Incubare, Incubate: T.A./R.T. 60±5 min. 1200 rpm<br />
− Aspirare e lavare, Aspirate and wash: 4 x 350 µL.<br />
CONJ 100 µL 100 µL 100 µL 100 µL<br />
− Incubare, Incubate: T.A./R.T. 30±2 min. 1200 rpm<br />
− Aspirare e lavare, Aspirate and wash: 4 x 350 µL.<br />
TMB 100 µL 100 µL 100 µL 100 µL<br />
− Incubare, Incubate: T.A./R.T. 10 min. 1200 rpm<br />
STOP 100 µL 100 µL 100 µL 100 µL<br />
− Leggere, Read: 450-405 nm.<br />
K10TG - <strong>Anti</strong>-Transglutaminasi <strong>IgG</strong> <strong>EIA</strong> <strong>WELL</strong><br />
M412 – Rev.1 – 04/2008 – Pag. 22/24
BIBLIOGRAFIA-<strong>REF</strong>ERENCES<br />
1 - Dieterich W., Laag E., Schöpper H., Volta U., Ferguson A., Gillet H., Riecken E.O.,<br />
Schuppan D. (1998). Autoantibodies to Tissue Transglutaminase as Predictor of<br />
Coeliac Disease. Gastroenterology, 115: 1317-1321.<br />
2 - Sulkanen S., Halttunen T., Laurila K., Kohlo K.L., Korponay-Szabò I.R., Sarnesto<br />
A., Savilahti E., Collin P., Mäki M. (1998). Tissue Transglutaminase Autoantibody<br />
Enzyme-Linked Immunoadsorbent Assay in Detecting Coeliac Disease.<br />
Gastroenterology, 115: 1322-1328.<br />
3 - Dieterich W., Ehnis T., Bauer M., Donner P., Volta U., Riecken O., Schuppan D.<br />
(1997). Identification of tissue transglutaminase as the autoantigen of celiac<br />
disease. Nature Medicine, 3: 797-801.<br />
4 - Maki M. (1997). Tissue Transglutaminase as the autoantigen of coeliac disease.<br />
Gut, 41: 565-566.<br />
5 - Sollid L.M., Molberg Ø., McAdam S., Lundin K.E.A. (1997). Autoantibodies in celiac<br />
disease: tissue transglutaminase-guilt by association?. Gut, 41: 851-852.<br />
6 - Salmaso C., Ocmant A., Pesce G., Altrinetti V., Montagna P., Descalzi D., Martini<br />
S., Bagnasco M., Mascara F. (2001). Comparison of ELISA for tissue<br />
transglutaminase autoantibodies with antiendomysium antibodies in pediatric and<br />
adult patients with celiac disease. Allergy, 56: 544-547.<br />
7 - Carroccio A., Vitale G., Di Prima L., Chifari N., Napoli S., La Russa C., Gulotta G.,<br />
Averna M.R., Montalto G., Mansueto S., Notarbartolo A. (2002). Comparison of<br />
<strong>Anti</strong>-Transglutaminase ELISAs and an <strong>Anti</strong>-Endomysial <strong>Anti</strong>body Assay in the<br />
Diagnosis od Celiac Disease: A Prospective Study. Clinical Chemistry, 48 (9):<br />
1546-1550.<br />
8 - Van Wijk M.A.M., van der Lei J., Mosseveld M., Bohenen A.M., van Bemmel J.H.<br />
(2002). Compliance of General Practitioners with a Guideline-based Decision<br />
Support System for Ordering Blood Tests. Clinical Chemistry, 48 (1): 55-60.<br />
9 - Kocna P., Vanìčkovà Z., Perušičovà J., Dvořàk M. (2002). Tissue<br />
Transglutaminase-Serology Markers for Celiac Disease. Clin. Chem. Lab. Med., 40<br />
(5): 485-492.<br />
10 - Hansson T., Dahlbom I., Rogberg S., Dannaeus A., Höpfl P., Gut H., Kraaz W.,<br />
Klareskog L. (2002). Recombinant Human Tissue Transglutaminase for Diagnosis<br />
and Follow-Up of Childhood Coeliac Disease. Pediatric Research, 51 (6): 700-705.<br />
11 - F. Cataldo, D. Lio, V. Marino, A. Picarelli, A. Ventura, GR Corazza (2000). <strong>IgG</strong><br />
antiendomysium and <strong>IgG</strong> anti-tissue-transglutaminase antibodies in coeliac patients<br />
with selective IgA deficiency. Gut 2000; 47:366-369<br />
12 - V. Kumar, M. Jarzabek-Chorzelska e al. (2002). Coeliac disease and<br />
Immunoglobulin A deficiency: how effective are the serologicals methods of<br />
diagnosis? Clinical and diagnostic laboratory Immunology, Nov. 2002, pag. 1295-<br />
1300<br />
13 - T. Hansson, I. Dahlbom e al. (2002). Recombinant human tissue transglutaminase<br />
for diagnosis and follow-up of chikdhood coeliac disease. Pediatric research vol.<br />
51, n°6, 2002<br />
14 - I R Korponay-Szabo, I. Dahlbom e al. (2003). Elevation of <strong>IgG</strong> antibodies against<br />
tissue transglutaminase as a diagnostic tool for coeliac disease in selective IgA<br />
deficiency. Gut 2003, 52: 1567-1571.<br />
K10TG - <strong>Anti</strong>-Transglutaminasi <strong>IgG</strong> <strong>EIA</strong> <strong>WELL</strong><br />
M412 – Rev.1 – 04/2008 – Pag. 23/24
RADIM S.p.A. - Via del Mare, 125 - 00040 Pomezia (Roma) Italia<br />
Tel.: +39 06 91.249.1 - Fax: +39 06 91.249.443<br />
National Order Entry: +39 06 91.249.702<br />
Export Department: +39 06 91.249.701<br />
Customer Care: +39 06 91.249.700<br />
info@radim.com - www.radim.com