Estudo da fratura do planalto tibial através da tomografia ...
Estudo da fratura do planalto tibial através da tomografia ...
Estudo da fratura do planalto tibial através da tomografia ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
ESTUDO DA FRATURA DO PLANALTO TIBIAL ATRAVÉS DA TOMOGRAFIA COMPUTADORIZADA<br />
<strong>Estu<strong>do</strong></strong> <strong>da</strong> <strong>fratura</strong> <strong>do</strong> <strong>planalto</strong> <strong>tibial</strong><br />
através <strong>da</strong> <strong>tomografia</strong> computa<strong>do</strong>riza<strong>da</strong> *<br />
NARCISO ALVES FAUSTINO JÚNIOR 1 , RICARDO DE SOUZA ANDRADE 1 , CONSTANTINO JORGE CALAPODOPULOS 2<br />
RESUMO<br />
No perío<strong>do</strong> entre maio de 1995 e julho de 1997, 21 pacientes<br />
porta<strong>do</strong>res de <strong>fratura</strong> <strong>do</strong> <strong>planalto</strong> <strong>tibial</strong> foram submeti<strong>do</strong>s<br />
a radiografias simples <strong>do</strong> joelho e à <strong>tomografia</strong><br />
axial computa<strong>do</strong>riza<strong>da</strong>. Este exame mostrou-se eficiente<br />
para a caracterização <strong>da</strong> <strong>fratura</strong>, indicação <strong>do</strong> tratamento<br />
e planejamento operatório.<br />
Unitermos – Fratura <strong>do</strong> <strong>planalto</strong> <strong>tibial</strong>; <strong>planalto</strong> <strong>da</strong> tíbia; <strong>tomografia</strong><br />
computa<strong>do</strong>riza<strong>da</strong><br />
SUMMARY<br />
Study of the <strong>tibial</strong> plateau using computerized tomography<br />
From May 1995 to July 1997, 21 patients with fractures<br />
on the <strong>tibial</strong> plateau were submitted to simple knee X-rays<br />
and axial computerized tomographies. This exam proved to<br />
be efficient in the characterization of the fracture, indication<br />
of the treatment, and surgical planning.<br />
detalhe anatômico pode subestimar uma depressão articular<br />
anterior ou central e exagerar a depressão posterior (1,4,6,7) .<br />
A indicação <strong>do</strong> tratamento operatório <strong>do</strong> <strong>planalto</strong> <strong>tibial</strong><br />
baseia-se na depressão articular maior que 5mm (5,8) , nas condições<br />
gerais <strong>do</strong> paciente, na deman<strong>da</strong> funcional e, sobretu<strong>do</strong>,<br />
no tipo de <strong>fratura</strong> (1,2,7) .<br />
O objetivo deste trabalho foi verificar a importância <strong>da</strong><br />
<strong>tomografia</strong> computa<strong>do</strong>riza<strong>da</strong> em <strong>fratura</strong>s <strong>do</strong> <strong>planalto</strong> <strong>da</strong> tíbia.<br />
CASUÍSTICA E MÉTODOS<br />
Foram estu<strong>da</strong><strong>do</strong>s 21 pacientes com <strong>fratura</strong> <strong>do</strong> <strong>planalto</strong> <strong>tibial</strong>.<br />
Quatorze (66,7%) eram homens e 7 (33,3%), mulheres,<br />
com i<strong>da</strong>de média de 46 anos (variação: 16-74). O joelho direito<br />
foi afeta<strong>do</strong> em 8 (38%) pacientes e o esquer<strong>do</strong> em 13<br />
(62%).<br />
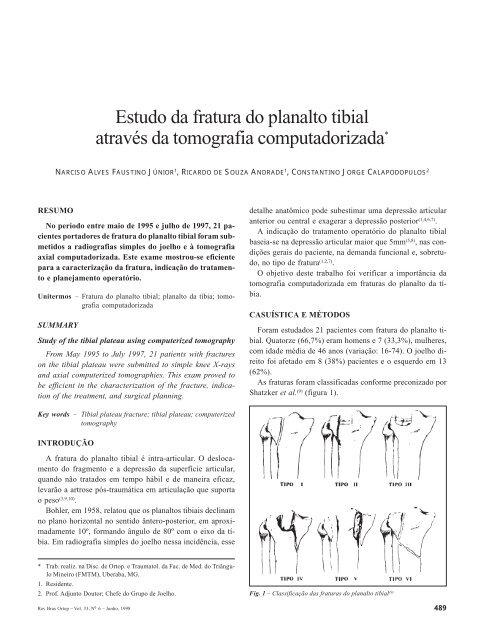
As <strong>fratura</strong>s foram classifica<strong>da</strong>s conforme preconiza<strong>do</strong> por<br />
Shatzker et al. (9) (figura 1).<br />
Key words – Tibial plateau fracture; <strong>tibial</strong> plateau; computerized<br />
tomography<br />
INTRODUÇÃO<br />
A <strong>fratura</strong> <strong>do</strong> <strong>planalto</strong> <strong>tibial</strong> é intra-articular. O deslocamento<br />
<strong>do</strong> fragmento e a depressão <strong>da</strong> superfície articular,<br />
quan<strong>do</strong> não trata<strong>do</strong>s em tempo hábil e de maneira eficaz,<br />
levarão a artrose pós-traumática em articulação que suporta<br />
o peso (3,9,10) .<br />
Bohler, em 1958, relatou que os <strong>planalto</strong>s tibiais declinam<br />
no plano horizontal no senti<strong>do</strong> ântero-posterior, em aproxima<strong>da</strong>mente<br />
10º, forman<strong>do</strong> ângulo de 80º com o eixo <strong>da</strong> tíbia.<br />
Em radiografia simples <strong>do</strong> joelho nessa incidência, esse<br />
* Trab. realiz. na Disc. de Ortop. e Traumatol. <strong>da</strong> Fac. de Med. <strong>do</strong> Triângulo<br />
Mineiro (FMTM), Uberaba, MG.<br />
1. Residente.<br />
2. Prof. Adjunto Doutor; Chefe <strong>do</strong> Grupo de Joelho.<br />
Fig. 1 – Classificação <strong>da</strong>s <strong>fratura</strong>s <strong>do</strong> <strong>planalto</strong> <strong>tibial</strong> (9)<br />
Rev Bras Ortop _ Vol. 33, Nº 6 – Junho, 1998 489
N.A. FAUSTINO JR., R.S. ANDRADE & C.J. CALAPODOPULOS<br />
TABELA 1<br />
Características gerais <strong>do</strong>s pacientes submeti<strong>do</strong>s<br />
à <strong>tomografia</strong> axial computa<strong>do</strong>riza<strong>da</strong> quanto<br />
a i<strong>da</strong>de, sexo, la<strong>do</strong> e <strong>planalto</strong> acometi<strong>do</strong><br />
Caso Paciente I<strong>da</strong>de Sexo La<strong>do</strong> Planalto<br />
(anos)<br />
Fig. 2 – Diagrama<br />
<strong>da</strong> elaboração <strong>da</strong><br />
<strong>tomografia</strong> axial<br />
computa<strong>do</strong>riza<strong>da</strong>:<br />
1) Secção <strong>da</strong><br />
superfície <strong>do</strong>s<br />
côndilos femorais;<br />
2) Corte <strong>da</strong> base<br />
<strong>da</strong> espinha <strong>tibial</strong><br />
ou <strong>planalto</strong> não<br />
<strong>fratura</strong><strong>do</strong>.<br />
To<strong>do</strong>s os pacientes foram submeti<strong>do</strong>s a radiografias em<br />
ântero-posterior e em perfil e à <strong>tomografia</strong> axial computa<strong>do</strong>riza<strong>da</strong><br />
com o aparelho Shimadzu SCT 3.000T, que fornece<br />
cortes axiais e não permite os biplanares sagitais e coronais.<br />
Durante esse exame foram realiza<strong>do</strong>s <strong>do</strong>is cortes: um ao<br />
nível <strong>da</strong> superfície <strong>do</strong>s côndilos femorais e o outro, na base<br />
<strong>da</strong> espinha <strong>tibial</strong> <strong>do</strong> <strong>planalto</strong> não <strong>fratura</strong><strong>do</strong>. Esses parâmetros<br />
serviram de referência para cálculo <strong>da</strong> depressão <strong>do</strong> <strong>planalto</strong><br />
<strong>fratura</strong><strong>do</strong>. Se ambos os <strong>planalto</strong>s estivessem <strong>fratura</strong><strong>do</strong>s, a linha<br />
referencial era a superfície <strong>do</strong>s côndilos femorais, sen<strong>do</strong><br />
o espaço articular normal de 5mm. Para esse cálculo, os cortes<br />
axiais foram de 2mm de espessura a ca<strong>da</strong> 2mm no senti<strong>do</strong><br />
distal (figuras 2 e 3).<br />
As características gerais <strong>do</strong>s pacientes encontram-se na<br />
tabela 1.<br />
RESULTADOS<br />
Das 21 <strong>fratura</strong>s, o <strong>planalto</strong> lateral foi acometi<strong>do</strong> em 16<br />
(76,2%), o medial em 2 (9,5%) e ambos em 3 (14,3%) (tabela<br />
1).<br />
A <strong>tomografia</strong> axial computa<strong>do</strong>riza<strong>da</strong> em 18 (85,7%) <strong>fratura</strong>s<br />
evidenciou maior depressão <strong>da</strong> superfície articular em<br />
relação ao estu<strong>do</strong> radiológico. Em 1 (4,8%) não houve diferença,<br />
em 2 (9,5%) não foi possível aferir devi<strong>do</strong> à má quali<strong>da</strong>de<br />
<strong>da</strong>s radiografias (tabela 2).<br />
1 IAF 49 F Direito L<br />
2 OPM 45 F Direito L<br />
3 VFS 44 M Esquer<strong>do</strong> L/M<br />
4 MAM 52 F Esquer<strong>do</strong> M<br />
5 NR 74 M Esquer<strong>do</strong> L<br />
6 ASJ 36 M Esquer<strong>do</strong> L<br />
7 CAGD 41 M Esquer<strong>do</strong> L<br />
8 ECS 69 M Esquer<strong>do</strong> L<br />
9 ZBF 70 F Esquer<strong>do</strong> L<br />
10 ARS 16 F Esquer<strong>do</strong> L<br />
11 MDB 37 F Esquer<strong>do</strong> L/M<br />
12 EA 64 F Direito L<br />
13 SJB 24 M Esquer<strong>do</strong> L<br />
14 EO 28 M Esquer<strong>do</strong> L<br />
15 GAM 31 M Direito L<br />
16 JVM 47 M Direito L<br />
17 SFA 48 M Direito L<br />
18 JDT 34 M Esquer<strong>do</strong> L<br />
19 GSS 55 M Direito M<br />
20 JBS 41 M Esquer<strong>do</strong> L/M<br />
21 GLS 57 M Direito M<br />
L = Planalto lateral; M = Planalto medial<br />
TABELA 2<br />
Classificação e comparação <strong>da</strong>s aferições <strong>da</strong> depressão articular<br />
Tipo de <strong>fratura</strong><br />
Depressão (mm)<br />
Caso Paciente Radiografias CT Radiografias CT<br />
1 IAF VI VI 9 10<br />
2 OPM II II 0 06<br />
3 VFS VI VI 8 (L)/0 (M) 10 (L)/2 (M)<br />
4 MAM IV IV 2 06<br />
5 NR V V – 08<br />
6 ASJ II II 3 06<br />
7 CAGD II II 4 06<br />
8 ECS VI VI 2 02<br />
9 ZBF II II 3 04<br />
10 ARS II II 2 04<br />
11 MDB V V 3 (L)/0 (M) 4 (L)/2 (M)<br />
12 EA II II 6 08<br />
13 SJB I II 0 08<br />
14 EO VI VI 4 04<br />
15 GAM III III 7 10<br />
16 JVM II II 5 08<br />
17 SFA II II – 06<br />
18 JDT VI VI 8 10<br />
19 GSS VI VI 181 20<br />
20 JBS V V 3 (L)/0 (M) 6 (L)/2 (M)<br />
21 GLS IV IV 3 06<br />
490 Rev Bras Ortop _ Vol. 33, Nº 6 – Junho, 1998
ESTUDO DA FRATURA DO PLANALTO TIBIAL ATRAVÉS DA TOMOGRAFIA COMPUTADORIZADA<br />
Fig. 3 – A) Tomografia axial computa<strong>do</strong>riza<strong>da</strong>, visão panorâmica (diagrama) <strong>da</strong> elaboração <strong>do</strong>s cortes<br />
axiais. B) Secção <strong>da</strong> base <strong>da</strong> espinha <strong>tibial</strong>: a área escura no <strong>planalto</strong> lateral indica o local e a extensão <strong>da</strong><br />
depressão articular. C) Corte <strong>da</strong> superfície <strong>da</strong> depressão articular, área circular branca. D) Secção distal:<br />
nota-se a extensão <strong>do</strong> traço <strong>da</strong> <strong>fratura</strong> de anterior para posterior sem cominuição.<br />
Em 1 (4,8%) a classificação <strong>do</strong> tipo de <strong>fratura</strong>, após a avaliação<br />
com <strong>tomografia</strong> computa<strong>do</strong>riza<strong>da</strong>, alterou-se, <strong>do</strong> tipo<br />
I para o tipo II de Shatzker.<br />
Dos 19 pacientes, em 11 (58%) a <strong>tomografia</strong> computa<strong>do</strong>riza<strong>da</strong><br />
evidenciou maior fragmentação, quan<strong>do</strong> compara<strong>da</strong><br />
com as radiografias, e em 8 (42%) não houve alterações (tabela<br />
3).<br />
DISCUSSÃO<br />
As <strong>fratura</strong>s <strong>do</strong> <strong>planalto</strong> <strong>tibial</strong> constituem 1% <strong>da</strong>s <strong>fratura</strong>s<br />
<strong>do</strong> esqueleto e em 8% nos pacientes i<strong>do</strong>sos, com varia<strong>da</strong>s<br />
configurações <strong>da</strong> topografia anatômica. Comprometem o <strong>planalto</strong><br />
medial em 10 a 23%, o lateral de 55 a 79% e ambos de<br />
TABELA 3<br />
Cominuição <strong>da</strong> <strong>fratura</strong><br />
Radiografia<br />
CT<br />
Nenhuma 06 03<br />
Leve 05 03<br />
Modera<strong>da</strong> 06 06<br />
Grave 02 07<br />
Total 19 19<br />
Obs.: Consideraram-se os seguintes critérios de comunuição:<br />
Nenhuma = 1 traço fraturário<br />
Leve = 2 traços fraturários<br />
Modera<strong>da</strong> = 3-4 traços fraturários<br />
Grave = > 5 traços fraturários<br />
Rev Bras Ortop _ Vol. 33, Nº 6 – Junho, 1998 491
N.A. FAUSTINO JR., R.S. ANDRADE & C.J. CALAPODOPULOS<br />
11 a 31% (9,10) . Em nosso estu<strong>do</strong>, o <strong>planalto</strong> <strong>tibial</strong> estava <strong>fratura</strong><strong>do</strong><br />
em 2 (9,5%) casos, o lateral em 16 (76,2%) e ambos<br />
em 3 (14,3%).<br />
Embora a <strong>tomografia</strong> axial computa<strong>do</strong>riza<strong>da</strong> tenha demonstra<strong>do</strong><br />
maiores valores de depressão articular em 18 (85,7%)<br />
pacientes, a classificação <strong>da</strong> <strong>fratura</strong> foi altera<strong>da</strong>, em um caso,<br />
<strong>do</strong> tipo I para o tipo II de Shatzker.<br />
O aparelho de <strong>tomografia</strong> utiliza<strong>do</strong> não realizou os cortes<br />
biplanares sagitais e coronais, não aferin<strong>do</strong> o deslocamento<br />
<strong>da</strong> <strong>fratura</strong>; entretanto, permitiu verificar a cominuição e a<br />
localização <strong>da</strong> <strong>fratura</strong>, caracterizan<strong>do</strong> a topografia <strong>da</strong> lesão.<br />
Concluímos que a <strong>tomografia</strong> axial computa<strong>do</strong>riza<strong>da</strong> é de<br />
grande valor na avaliação <strong>da</strong> <strong>fratura</strong> <strong>do</strong> <strong>planalto</strong> <strong>tibial</strong>, fornecen<strong>do</strong><br />
identificação níti<strong>da</strong> <strong>do</strong>s fragmentos, grau de cominuição<br />
e a depressão articular, proporcionan<strong>do</strong> maiores detalhes<br />
quan<strong>do</strong> compara<strong>da</strong> com as radiografias convencionais.<br />
REFERÊNCIAS<br />
1. Dias, J.J., Stirling, A.J., Finlay, D.B. et al: Computerized axial tomography<br />
for <strong>tibial</strong> plateau fractures. J Bone Joint Surg [Br] 69: 84-88, 1987.<br />
2. Elstrom, J., Pankovich, A.M., Sassoon, H. et al: The use of tomography<br />
in the assessment of fractures of the <strong>tibial</strong> plateau. J Bone Joint Surg<br />
[Am] 58: 551-555, 1976.<br />
3. Hohl, M.: Tibial condylar fractures long term follow-up. Tex Med 70:<br />
46-56, 1974.<br />
4. Kode, L., Leberman, J.M., Motta, A. et al: Evaluation of <strong>tibial</strong> plateau<br />
fractures: efficacy of MR imaging compared with CT. AJR Am J Roentgenol<br />
163: 141-147, 1994.<br />
5. McEreny, K.W., Wilson, A.J., Pilgram, T.K. et al: Fractures of the <strong>tibial</strong><br />
plateau: value of spiral CT coronal plane reconstructions for detecting<br />
displacement in vitro. AJR Am J Roentgenol 163: 117-181, 1994.<br />
6. Newber, A.H. & Greenstein, R.: Radiographic evaluation of <strong>tibial</strong> plateau<br />
fractures. Radiology 126: 319-323, 1978.<br />
7. Raffi, M., Firooznia, H., Golimbu, C. et al: Computed tomography of<br />
<strong>tibial</strong> plateau fractures. AJR Am J Roentgenol 142: 1181-1186, 1984.<br />
8. Roberts, J.: Fractures of the condyles of the tibia. J Bone Joint Surg<br />
[Am] 50: 1505-1521, 1968.<br />
9. Schatzker, J., McBroom, R. & Bruce, D.: The <strong>tibial</strong> plateau fracture. The<br />
Toronto Experience 1968, 1975. Clin Orthop 138: 94-104, 1979.<br />
10. Tscherne, H. & Lobenhoffer, P.: Tibial plateau fractures. Management<br />
and expected results. Clin Orthop 262: 87-100, 1993.<br />
492 Rev Bras Ortop _ Vol. 33, Nº 6 – Junho, 1998