CO â Vergiftung und Rauchgasintoxikation - Druckkammerzentrum ...
CO â Vergiftung und Rauchgasintoxikation - Druckkammerzentrum ...
CO â Vergiftung und Rauchgasintoxikation - Druckkammerzentrum ...

Sie wollen auch ein ePaper? Erhöhen Sie die Reichweite Ihrer Titel.
YUMPU macht aus Druck-PDFs automatisch weboptimierte ePaper, die Google liebt.
Pressure (atm abs)<br />
Pressure (atm abs)<br />
Pressure (atm abs)<br />
Pressure (atm abs)<br />
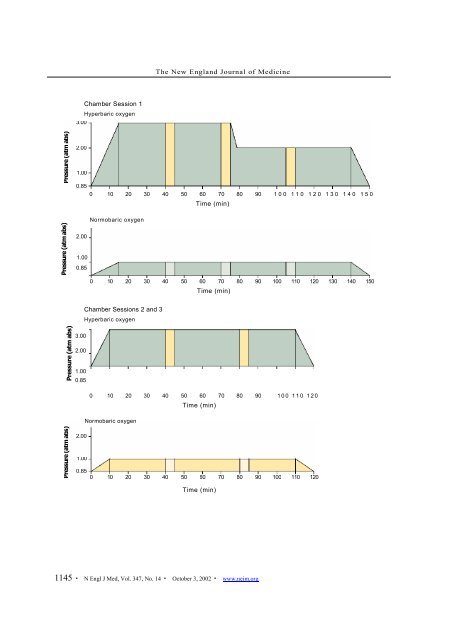
3.00<br />
2.00<br />
1.00<br />
The New England Journal of Medicine<br />
0.85<br />
0 10 20 30 40 50 60 70 80 90 1 0 0 1 1 0 1 2 0 1 3 0 1 4 0 1 5 0<br />
2.00<br />
1.00<br />
0.85<br />
3.00<br />
2.00<br />
1.00<br />
0.85<br />
2.00<br />
1.00<br />
Chamber Session 1<br />
Hyperbaric oxygen<br />
Normobaric oxygen<br />
Normobaric oxygen<br />
Time (min)<br />
0 10 20 30 40 50 60 70 80 90 100 110 120 130 140 150<br />
Chamber Sessions 2 and 3<br />
Hyperbaric oxygen<br />
Time (min)<br />
0 10 20 30 40 50 60 70 80 90 1 0 0 1 1 0 1 2 0<br />
Time (min)<br />
0.85<br />
0 10 20 30 40 50 60 70 80 90 100 110 120<br />
Time (min)<br />
1145 · N Engl J Med, Vol. 347, No. 14 · October 3, 2002 · www.nejm.org