The Use of Diathermy Scissors in Parotid Gland Surgery
The Use of Diathermy Scissors in Parotid Gland Surgery
The Use of Diathermy Scissors in Parotid Gland Surgery

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>The</strong> <strong>Use</strong> <strong>of</strong> <strong>Diathermy</strong> <strong>Scissors</strong><br />
<strong>in</strong> <strong>Parotid</strong> <strong>Gland</strong> <strong>Surgery</strong><br />
Juergen O. Ussmueller, MD; Michael Jaehne, MD; Bjoern-Georg Neumann, MD<br />
Objective: To evaluate the benefits, as well as the possible<br />
complications, <strong>of</strong> the use <strong>of</strong> diathermy scissors <strong>in</strong><br />
parotid gland surgery.<br />
Design: Prospective study <strong>of</strong> the surgical procedures <strong>of</strong><br />
the diathermy scissors and a retrospective comparison<br />
with a conventionally treated control group concern<strong>in</strong>g<br />
cut-closure time.<br />
Sett<strong>in</strong>g: Tertiary care referral academic center.<br />
Patients: Prospective exam<strong>in</strong>ation <strong>of</strong> 30 unselected patients<br />
undergo<strong>in</strong>g superficial (n=23) or subtotal/total<br />
(n=10) parotidectomies performed with diathermy scissors.<br />
Indications were benign tumors (n=18), malignant<br />
tumors (n=12), and cystic lesions (n=3). In a control<br />
group (n=50), 36 superficial and 21 subtotal/total<br />
parotidectomies were performed.<br />
Results: <strong>The</strong> use <strong>of</strong> diathermy scissors reduces the need<br />
to frequently change dissect<strong>in</strong>g and coagulat<strong>in</strong>g surgical<br />
<strong>in</strong>struments. <strong>The</strong> scissors reduce <strong>in</strong>traoperative bleed<strong>in</strong>g<br />
and therefore improve visualization and orientation<br />
From the Department <strong>of</strong><br />
Otorh<strong>in</strong>olaryngology–Head and<br />
Neck <strong>Surgery</strong>, University<br />
Hospital Eppendorf, Hamburg,<br />
Germany. <strong>The</strong> authors have no<br />
relevant f<strong>in</strong>ancial <strong>in</strong>terest <strong>in</strong><br />
this article.<br />
ORIGINAL ARTICLE<br />
THE BASIC GOAL OF PAROTID<br />
gland surgery is the cont<strong>in</strong>uous<br />
preparation and<br />
strict preservation <strong>of</strong> the facial<br />
nerve dur<strong>in</strong>g en bloc resection<br />
<strong>of</strong> a tumor along with surround<strong>in</strong>g<br />
tissue; therefore, the tissue ly<strong>in</strong>g<br />
superficial to the facial nerve is dissected<br />
microscopically. Microscopic dissection,<br />
however, may lead to multilocular m<strong>in</strong>or<br />
bleed<strong>in</strong>gs, which <strong>in</strong> turn may obscure visualization<br />
<strong>of</strong> the course <strong>of</strong> the nerve and<br />
require frequent replacement <strong>of</strong> the operat<strong>in</strong>g<br />
tools for dissection and coagulation,<br />
lead<strong>in</strong>g to prolonged surgery.<br />
In a prospective study, we exam<strong>in</strong>ed<br />
the benefits <strong>of</strong>, as well as the complications<br />
that can result from, the use <strong>of</strong> diathermy<br />
scissors to determ<strong>in</strong>e whether<br />
they are a suitable tool for parotid gland<br />
surgery.<br />
<strong>in</strong> the surgical field. Postoperative bleed<strong>in</strong>g or seroma and<br />
Frey syndrome were not observed. In 1 case, a salivary<br />
fistula was present for 3 weeks. Three cases <strong>of</strong> transient<br />
facial weakness occurred, all <strong>of</strong> which completely resolved<br />
by 6 months after surgery. In the control group,<br />
the cut-closure time ranged from 50 to 120 m<strong>in</strong>utes (average,<br />
87.6 m<strong>in</strong>utes) dur<strong>in</strong>g superficial parotidectomy;<br />
it ranged from 80 to 160 m<strong>in</strong>utes (average, 130.0 m<strong>in</strong>utes)<br />
dur<strong>in</strong>g subtotal and total parotidectomy. In comparison,<br />
<strong>in</strong> the study group, the average time ga<strong>in</strong> was<br />
16 m<strong>in</strong>utes dur<strong>in</strong>g superficial parotidectomy when diathermy<br />
scissors were used, a statiscally significant difference<br />
(P=.03). Dur<strong>in</strong>g subtotal and total parotidectomy<br />
with diathermy scissors, the average time ga<strong>in</strong> was<br />
19.3 m<strong>in</strong>utes and was statistically not significant (P=.23).<br />
Conclusions: <strong>The</strong> results <strong>of</strong> the present study show that<br />
diathermy scissors are very well suited for most <strong>of</strong> the<br />
surgical steps <strong>in</strong> parotid gland surgery. <strong>The</strong>y provide an<br />
elegant, safe, and fast surgical procedure, especially <strong>in</strong><br />
the hands <strong>of</strong> an experienced surgeon.<br />
Arch Otolaryngol Head Neck Surg. 2004;130:187-189<br />
(REPRINTED) ARCH OTOLARYNGOL HEAD NECK SURG/ VOL 130, FEB 2004 WWW.ARCHOTO.COM<br />
187<br />
©2004 American Medical Association. All rights reserved.<br />
Downloaded From: http://173.193.11.201/ on 03/21/2013<br />
METHODS<br />
In a prospective study <strong>in</strong>volv<strong>in</strong>g 30 patients,<br />
23 superficial parotidectomies, 9 subtotal parotidectomies,<br />
and 1 total parotidectomy were<br />
performed with diathermy scissors. <strong>The</strong> ma<strong>in</strong><br />
<strong>in</strong>dications for surgery <strong>in</strong>cluded benign and<br />
malignant tumors (pleomorphic adenoma,<br />
Warth<strong>in</strong> tumor, oncocytoma, ac<strong>in</strong>ic cell carc<strong>in</strong>oma,<br />
mucoepidermoid carc<strong>in</strong>oma, carc<strong>in</strong>osarcoma,<br />
malignant lymphoma, and metastasis)<br />
as well as cystic lesions (cystic lymphoid<br />
hyperplasia <strong>in</strong> AIDS and salivary duct cyst). In<br />
4 cases, exposure <strong>of</strong> the facial nerve was required<br />
dur<strong>in</strong>g excision <strong>of</strong> cutaneous malignancies<br />
(malignant melanoma and Merkel cell<br />
carc<strong>in</strong>oma). <strong>Diathermy</strong> scissors were used to<br />
perform a total <strong>of</strong> 37 operations, 4 <strong>of</strong> which<br />
were surgical revisions.<br />
<strong>The</strong> standard procedure consisted <strong>of</strong> microscopic<br />
identification <strong>of</strong> the facial nerve stem<br />
<strong>in</strong> the stylomastoid fossa, followed by anterograde<br />
preparation <strong>of</strong> the facial nerve fan. <strong>The</strong>
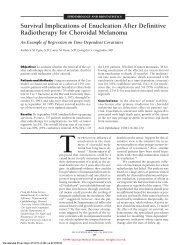
Figure 1. Superficial parotidectomy performed with diathermy scissors,<br />
<strong>in</strong>traoperative view. Simultaneous dissection <strong>of</strong> the parotid gland<br />
parenchyma ly<strong>in</strong>g superficial to the facial nerve (arrow <strong>in</strong>dicates bifurcation<br />
<strong>of</strong> the facial nerve trunk).<br />
Figure 2. Superficial parotidectomy performed with diathermy scissors,<br />
<strong>in</strong>traoperative view. Dissected parenchyma <strong>of</strong> the superficial parotid lobe<br />
show<strong>in</strong>g no bleed<strong>in</strong>g.<br />
use <strong>of</strong> the microscope made identification and preparation <strong>of</strong><br />
the nerve branches safer and easier. After the nerve stem was<br />
def<strong>in</strong>itively identified, the diathermy scissors were used almost<br />
cont<strong>in</strong>uously, for preparation, conventional cutt<strong>in</strong>g, conventional<br />
bipolar coagulation, and simultaneous cutt<strong>in</strong>g and<br />
bipolar coagulation. <strong>The</strong> bipolar <strong>in</strong>tensity sett<strong>in</strong>g was 50 W.<br />
Additional <strong>in</strong>traoperative facial nerve monitor<strong>in</strong>g was conducted<br />
<strong>in</strong> cases <strong>in</strong>volv<strong>in</strong>g revision surgery and resection <strong>of</strong> malignant<br />
sk<strong>in</strong> tumors <strong>of</strong> the cheek.<br />
After surgery, the entire range <strong>of</strong> complications, especially<br />
hemorrhage, hematoma, seroma, salivary fistula, Frey syndrome,<br />
and facial nerve paralysis, was exam<strong>in</strong>ed. Postoperative<br />
follow-up lasted for 12 months. Assessment <strong>of</strong> concomitant nerve<br />
impulses (caused by the scissors) and the possible adverse impact<br />
<strong>of</strong> facial nerve monitor<strong>in</strong>g were <strong>of</strong> special <strong>in</strong>terest. Required<br />
time for surgical preparation was exam<strong>in</strong>ed retrospectively by comparison<br />
<strong>of</strong> the average cut-closure time <strong>in</strong> the study group with<br />
that <strong>in</strong> a control group <strong>of</strong> 50 patients who were conventionally<br />
treated. <strong>The</strong> control group underwent 36 superficial and 21 subtotal/total<br />
parotidectomies <strong>in</strong> the same surgical manner but without<br />
the use <strong>of</strong> the diathermy scissors. Cases <strong>in</strong>volv<strong>in</strong>g revision<br />
surgery and preparation <strong>of</strong> the facial nerve <strong>in</strong> sk<strong>in</strong> malignancies<br />
were excluded. <strong>The</strong> <strong>in</strong>dications for surgery were almost the same<br />
<strong>in</strong> both groups. <strong>The</strong> follow-up time was the same (12 months).<br />
All operations were performed by the same surgeon, with<br />
the patients under general anesthesia and normal conditions<br />
<strong>of</strong> blood pressure (110-130 mm Hg systolic). <strong>The</strong> statistical significance<br />
<strong>of</strong> cut-closure time differences was calculated by normality<br />
(Kolmogorov-Smirnov) and t tests.<br />
No. <strong>of</strong> Operations<br />
12<br />
10<br />
8<br />
6<br />
4<br />
2<br />
0<br />
Superficial <strong>Parotid</strong>ectomy<br />
40 60 80 100 120 140 160<br />
Cut-Closure Time, m<strong>in</strong><br />
RESULTS<br />
<strong>Diathermy</strong> scissors are very well suited for most <strong>of</strong> the<br />
surgical steps <strong>in</strong> parotid gland surgery. However, some<br />
practice is needed for proper use <strong>of</strong> this tool. Both arterial<br />
and venous bleeders are safely coagulated, result<strong>in</strong>g<br />
<strong>in</strong> a major reduction <strong>of</strong> <strong>in</strong>traoperative bleed<strong>in</strong>g. Coagulation<br />
<strong>of</strong> arterial and venous vessels with a diameter <strong>of</strong> 2<br />
to 3 mm can ideally be performed before cutt<strong>in</strong>g, with<br />
the tips <strong>of</strong> the scissors slightly open. This step, <strong>in</strong> turn,<br />
reduces the frequency with which <strong>in</strong>struments need to<br />
be changed. Simultaneous cutt<strong>in</strong>g and coagulation also<br />
reduces <strong>in</strong>traoperative bleed<strong>in</strong>g. <strong>The</strong>refore, the use <strong>of</strong> the<br />
diathermy scissors improves the view <strong>in</strong> the surgical field,<br />
especially visualization <strong>of</strong> the facial nerve branches<br />
(Figure 1 and Figure 2).<br />
COMPLICATIONS<br />
<strong>The</strong>re was no evidence <strong>of</strong> postoperative bleed<strong>in</strong>g, hemorrhage,<br />
or seroma. In 1 case, after superficial parotidectomy<br />
for pleomorphic adenoma, a salivary fistula was present<br />
for 3 weeks. With<strong>in</strong> the 12-month follow-up period,<br />
we did not observe any cases <strong>of</strong> Frey syndrome. Transient<br />
facial nerve paralysis occurred <strong>in</strong> 3 <strong>of</strong> 37 cases: 2<br />
cases with isolated <strong>in</strong>ferior trunk weakness and 1 case<br />
with a complete peripheral facial paresis. All 3 cases completely<br />
resolved by 6 months after surgery. <strong>The</strong> quality<br />
<strong>of</strong> facial nerve monitor<strong>in</strong>g was not impaired by diathermy<br />
scissors. Muscle contractions were sometimes observed<br />
with the use <strong>of</strong> the diathermy scissors, similar to<br />
electrocautery.<br />
CUT-CLOSURE TIME<br />
<strong>Diathermy</strong><br />
<strong>Scissors</strong> Group<br />
Control Group<br />
Figure 3. Cut-closure time <strong>of</strong> superficial parotidectomy performed with and<br />
without diathermy scissors.<br />
Dur<strong>in</strong>g superficial parotidectomy procedures (n=23), the<br />
cut-closure time ranged from 50 to 120 m<strong>in</strong>utes, with<br />
an average <strong>of</strong> 87.6 m<strong>in</strong>utes (Figure 3). Dur<strong>in</strong>g subtotal<br />
and total parotidectomy procedures (n=10), it ranged<br />
from 80 to 160 m<strong>in</strong>utes, with an average <strong>of</strong> 130.0 m<strong>in</strong>utes<br />
(Figure 4). In comparison, <strong>in</strong> the control group<br />
these figures were 60 to 140 m<strong>in</strong>utes (average, 103.6 m<strong>in</strong>utes)<br />
for superficial parotidectomy and 80 to 230 m<strong>in</strong>-<br />
(REPRINTED) ARCH OTOLARYNGOL HEAD NECK SURG/ VOL 130, FEB 2004 WWW.ARCHOTO.COM<br />
188<br />
©2004 American Medical Association. All rights reserved.<br />
Downloaded From: http://173.193.11.201/ on 03/21/2013
utes (average, 149.3 m<strong>in</strong>utes) for subtotal and total parotidectomy<br />
(Figures 3 and 4). <strong>The</strong>refore, with the use<br />
<strong>of</strong> diathermy scissors, we saw a statistically significant<br />
average time ga<strong>in</strong> <strong>of</strong> 16.0 m<strong>in</strong>utes (15.4%) (P=.03) dur<strong>in</strong>g<br />
superficial parotidectomy procedures. Dur<strong>in</strong>g subtotal<br />
and total parotidectomy procedures, the average time<br />
ga<strong>in</strong> was 19.3 m<strong>in</strong>utes (12.9%); it was not statistically<br />
significant, however, because <strong>of</strong> the small number <strong>of</strong><br />
operations.<br />
COMMENT<br />
With the development <strong>of</strong> and advances <strong>in</strong> new and alternative<br />
surgical dissection techniques (eg, lasercutt<strong>in</strong>g<br />
technologies, ultrasound scalpel, water-jet dissection,<br />
and others), a decision has to be made as to which<br />
one <strong>of</strong> these tools is best used for the large spectrum <strong>of</strong><br />
surgical procedures. 1 Additional technical support and<br />
the acquisition <strong>of</strong> new practical skills to properly use these<br />
tools are also frequently required.<br />
In contrast, the diathermy scissors represent a simple<br />
extension <strong>of</strong> the application <strong>of</strong> dissection scissors but with<br />
additional hemostatic capability. <strong>The</strong>re are numerous publications<br />
concern<strong>in</strong>g the application <strong>of</strong> diathermy and<br />
bipolar scissors <strong>in</strong> different surgical procedures (eg, colectomy,<br />
circumcision, laparoscopic cholecystectomy,<br />
vag<strong>in</strong>al and abdom<strong>in</strong>al hysterectomy, and elevation <strong>of</strong> the<br />
radial forearm fasciocutaneous free flap). Baggish and<br />
Tucker 2 conclude that bipolar scissors provide significant<br />
safety advantages and performance that is equal to<br />
or better than monopolar scissors when used for laparascopic<br />
surgery. In head and neck surgery, bipolar scissors<br />
have already been used for (pediatric) adenoidectomy,<br />
tonsillectomy, punctate diathermy <strong>of</strong> the s<strong>of</strong>t palate<br />
<strong>in</strong> the surgical treatment <strong>of</strong> snor<strong>in</strong>g, reduction <strong>of</strong> the nasal<br />
turb<strong>in</strong>ates, and excision <strong>of</strong> thyroid cancer 3 ; they have<br />
also proved useful <strong>in</strong> facial plastic surgery. 4 Wax et al 5<br />
compared scalpel and bipolar scissors <strong>in</strong> the elevation <strong>of</strong><br />
radial forearm fasciocutaneous free flaps. <strong>The</strong>y found that<br />
the total mean time <strong>of</strong> flap elevation and blood loss were<br />
reduced significantly <strong>in</strong> the bipolar scissors group, whereas<br />
the complications were equivalent. 5 To our knowledge,<br />
the present study is the first one to evaluate the use <strong>of</strong><br />
diathermy scissors <strong>in</strong> parotid gland surgery.<br />
<strong>The</strong> facial nerve is more likely to be <strong>in</strong>jured dur<strong>in</strong>g<br />
parotidectomy than dur<strong>in</strong>g any other procedure <strong>in</strong> head<br />
and neck surgery, with far-reach<strong>in</strong>g functional and cosmetic<br />
consequences. It is the complex topography <strong>of</strong> parotid<br />
gland disease, with tumors <strong>of</strong>ten neighbor<strong>in</strong>g the<br />
facial nerve, as well as the anatomy <strong>of</strong> the nerve itself,<br />
with its sometimes extremely th<strong>in</strong> branches, that contributes<br />
to the risk <strong>of</strong> <strong>in</strong>jury dur<strong>in</strong>g surgery. At the same<br />
time, the well-perfused gland parenchyma makes surgical<br />
dissection difficult. Depend<strong>in</strong>g on these factors, and<br />
on the surgeon’s experience, significant differences may<br />
occur <strong>in</strong> regard to the required surgical time as well as<br />
to postoperative complications. Judg<strong>in</strong>g from our expe-<br />
No. <strong>of</strong> Operations<br />
5<br />
4<br />
3<br />
2<br />
1<br />
Subtotal/Total <strong>Parotid</strong>ectomy<br />
0 60 80 100 120 140 160 180 200 220 240<br />
Cut-Closure Time, m<strong>in</strong><br />
rience, the diathermy scissors <strong>of</strong>fer substantial support<br />
for the surgeon <strong>in</strong> parotid gland surgery.<br />
CONCLUSIONS<br />
<strong>The</strong> use <strong>of</strong> diathermy scissors <strong>in</strong> parotid gland surgery<br />
not only will reduce the previously frequent need to<br />
change dissect<strong>in</strong>g and coagulat<strong>in</strong>g <strong>in</strong>struments, it also will<br />
result <strong>in</strong> a very elegant, safe, and fast surgical procedure,<br />
especially <strong>in</strong> the hands <strong>of</strong> an experienced surgeon.<br />
With proper application, the scissors can facilitate dissection,<br />
reduce <strong>in</strong>traoperative bleed<strong>in</strong>g, and therefore improve<br />
visualization <strong>of</strong> the surgical field.<br />
Submitted for publication January 8, 2003; f<strong>in</strong>al revision<br />
received May 7, 2003; accepted June 25, 2003.<br />
This study was presented <strong>in</strong> part at the First International<br />
Congress on Salivary <strong>Gland</strong> Diseases; January 27,<br />
2002; Geneva, Switzerland.<br />
Correspond<strong>in</strong>g author and repr<strong>in</strong>ts: Jürgen Ußmüller,<br />
MD, Kl<strong>in</strong>ik und Polikl<strong>in</strong>ik für Hals-Nasen-Ohren–<br />
Heilkunde, Universitätskl<strong>in</strong>ikum Hamburg-Eppendorf, Mart<strong>in</strong>istraße<br />
52, D-20246 Hamburg, Germany (e-mail:<br />
ussmueller@uke.uni-hamburg.de).<br />
REFERENCES<br />
<strong>Diathermy</strong><br />
<strong>Scissors</strong> Group<br />
Control Group<br />
Figure 4. Cut-closure time <strong>of</strong> subtotal/total parotidectomy performed with<br />
and without diathermy scissors.<br />
1. Siegert R, Magritz R, Jurk V. Water-jet dissection <strong>in</strong> parotid surgery: <strong>in</strong>itial cl<strong>in</strong>ical<br />
results. Laryngorh<strong>in</strong>ootologie. 2000;79:780-784.<br />
2. Baggish MS, Tucker RD. Tissue actions <strong>of</strong> bipolar scissors compared with monopolar<br />
devices. Fertil Steril. 1995;63:422-426.<br />
3. Raut V, Bhat N, K<strong>in</strong>sella J, Toner JG, S<strong>in</strong>nathuray AR, Stevenson M. Bipolar scissors<br />
versus cold dissection tonsillectomy: a prospective, randomized, multiunit<br />
study. Laryngoscope. 2001;111:2178-2182.<br />
4. W<strong>in</strong>slow CP, Burke A, Bartels S, Cook TA, Wax MK. Bipolar scissors <strong>in</strong> facial<br />
plastic surgery. Arch Facial Plast Surg. 2000;2:209-212.<br />
5. Wax MK, W<strong>in</strong>slow C, Desyatnikowa S, Andersen PE, Cohen JI. A prospective comparison<br />
<strong>of</strong> scalpel versus bipolar scissors <strong>in</strong> the elevation <strong>of</strong> radial forearm fasciocutaneous<br />
free flaps. Laryngoscope. 2001;111:568-571.<br />
(REPRINTED) ARCH OTOLARYNGOL HEAD NECK SURG/ VOL 130, FEB 2004 WWW.ARCHOTO.COM<br />
189<br />
©2004 American Medical Association. All rights reserved.<br />
Downloaded From: http://173.193.11.201/ on 03/21/2013