Speech Intelligibility, Acceptability, and Communication-Related ...
Speech Intelligibility, Acceptability, and Communication-Related ...
Speech Intelligibility, Acceptability, and Communication-Related ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
ORIGINAL ARTICLE<br />
<strong>Speech</strong> <strong>Intelligibility</strong>, <strong>Acceptability</strong>, <strong>and</strong><br />
<strong>Communication</strong>-<strong>Related</strong> Quality of Life<br />
in Chinese Alaryngeal Speakers<br />
Ida K.-Y. Law, MPhil; Estella P.-M. Ma, PhD; Edwin M.-L. Yiu, PhD<br />
Objective: To investigate (1) speech intelligibility <strong>and</strong><br />
acceptability in using 4 different alaryngeal speech methods:<br />
esophageal (ES), electrolaryngeal (EL), pneumatic<br />
device (PD), <strong>and</strong> tracheosophageal (TE) speech; <strong>and</strong><br />
(2) communication-related quality of life (QOL) in the<br />
alaryngeal speakers who used these 4 alaryngeal speech<br />
methods.<br />
Design: Survey.<br />
Participants: Alaryngeal speakers who had undergone<br />
speech rehabilitation <strong>and</strong> were recruited from the<br />
New Voice Club of Hong Kong.<br />
Main Outcome Measures: <strong>Speech</strong> samples collected<br />
from 49 alaryngeal speakers were rated by 6 judges for<br />
speech intelligibility <strong>and</strong> acceptability. The speakers also<br />
completed a communication-related QOL question-<br />
Author Affiliations: Voice<br />
Research Laboratory, Division of<br />
<strong>Speech</strong> <strong>and</strong> Hearing Sciences,<br />
<strong>and</strong> Centre for <strong>Communication</strong><br />
Disorders, The University of<br />
Hong Kong, Hong Kong.<br />
TOTAL LARYNGECTOMY INvolves<br />
surgical removal of<br />
the whole larynx. 1 Following<br />
the surgical procedure,<br />
speech restoration<br />
can be achieved by different alaryngeal<br />
speech methods: electrolaryngeal (EL),<br />
pneumatic device (PD), esophageal (ES),<br />
<strong>and</strong> tracheosophageal (TE) speech. The<br />
speech production mechanisms of these<br />
alaryngeal speech methods are different.<br />
The EL, TE, <strong>and</strong> PD speech methods require<br />
separate devices for speech production;<br />
ES speech does not require external<br />
devices.<br />
Earlier studies 2-5 investigated speech intelligibility<br />
mostly of ES <strong>and</strong> EL speech.<br />
With the increasing popularity of TE <strong>and</strong><br />
PD speech, more recent studies have been<br />
able to provide data on these 4 currently<br />
available speech methods. Although there<br />
was 1 study 6 that reported no significant difference<br />
in the speech intelligibility across<br />
naire called the <strong>Communication</strong> Activity <strong>and</strong> Participation<br />
After Laryngectomy.<br />
Results: We found that the ES <strong>and</strong> EL speakers showed<br />
considerably poorer speech intelligibility <strong>and</strong> communication-related<br />
QOL. The PD speakers demonstrated notably<br />
better speech intelligibility <strong>and</strong> acceptability ratings.<br />
However, high intelligibility <strong>and</strong> acceptability do<br />
not necessarily mean better QOL. The TE speakers, who<br />
demonstrated only the second highest speech intelligibility<br />
<strong>and</strong> acceptability, showed the best functional QOL.<br />
Conclusion: In speech rehabilitation after laryngectomy,<br />
QOL <strong>and</strong> speech intelligibility <strong>and</strong> acceptability<br />
should be considered together to find a balance that is<br />
acceptable to the patient.<br />
Arch Otolaryngol Head Neck Surg. 2009;135(7):704-711<br />
different alaryngeal speech methods, information<br />
to date generally shows that both<br />
TE speech 7,8 <strong>and</strong> PD speech 9 (which is more<br />
commonly used in Asian countries) show<br />
relatively good speech intelligibility. Alaryngeal<br />
speech intelligibility has also been<br />
found to be different across different age<br />
groups of listeners. 10 It has been shown that<br />
younger listeners are more proficient at underst<strong>and</strong>ing<br />
alaryngeal speech than older<br />
listeners. 10 Therefore, it is important to consider<br />
the age factor of the listeners in any<br />
alaryngeal speech intelligibility study.<br />
With its lexical tone feature, Chinese<br />
language adds another dimension to the<br />
study of alaryngeal speech intelligibility.<br />
Cantonese, a dialect of Chinese, is a tone<br />
language with 6 contrastive lexical tones,<br />
which means words that have the same<br />
sounds but only differ in pitch contour to<br />
signify different meanings. Cantonesespeaking<br />
alaryngeal speakers may face<br />
difficulties in producing various pitch<br />
(REPRINTED) ARCH OTOLARYNGOL HEAD NECK SURG/ VOL 135 (NO. 7), JULY 2009 WWW.ARCHOTO.COM<br />
704<br />
©2009 American Medical Association. All rights reserved.<br />
Downloaded From: http://173.193.11.201/ on 03/26/2013
Table 1. Sex Distribution <strong>and</strong> Postoperation Time<br />
levels. Because pitch variations are essential to convey<br />
different lexical meanings of Cantonese words, such difficulties<br />
would affect speech intelligibility. A number of<br />
studies 11-14 of the Cantonese-speaking alaryngeal population<br />
focused on the speech intelligibility of different alaryngeal<br />
speech, with particular attention to lexical tone<br />
production. In the study by Yiu et al, 14 ES speakers demonstrated<br />
the highest speech intelligibility, but TE <strong>and</strong><br />
PD speakers were more efficient in conveying lexical tones.<br />
Similarly, Ching et al 11 found that PD speakers showed<br />
the highest lexical tone intelligibility. A study by Ng et<br />
al 12 also found PD speakers to be able to produce better<br />
pitch variations, <strong>and</strong> hence better lexical tone production,<br />
than those using other types of alaryngeal speech<br />
methods, although there was no notable difference in the<br />
overall speech intelligibility among the 4 different alaryngeal<br />
speech types.<br />
<strong>Speech</strong> impairments following laryngectomy, including<br />
lower speech intelligibility <strong>and</strong> poorer lexical tone production,<br />
can have an impact on the alaryngeal speaker’s<br />
communication abilities. The extent to which speech intelligibility<br />
in different speech methods has an impact on<br />
quality of life (QOL) is largely unknown. Clements et al 15<br />
investigated ES, EL, <strong>and</strong> TE speakers’ satisfaction with their<br />
speech quality, communication abilities, interaction with<br />
others, <strong>and</strong> general QOL. They found TE speakers to be<br />
notably more satisfied with their speech method <strong>and</strong> to<br />
have better speech quality than ES <strong>and</strong> EL speakers. Nevertheless,<br />
no important difference was found in the level<br />
of satisfaction with QOL across the 3 alaryngeal speech<br />
groups. In general, their participants 15 reported low selfperceived<br />
ratings on their abilities to communicate over<br />
the telephone, high levels of limitation in communicating<br />
with others, <strong>and</strong> low levels of satisfaction with QOL.<br />
However, the small number of communication activities<br />
investigated in their study would not be adequate to assess<br />
the communication of the alaryngeal speaker population.Moreover,noPDspeakerswereincludedinthestudy<br />
because PD is not a commonly used speaking method in<br />
Western countries.<br />
In Hong Kong, most patients who have undergone laryngectomy<br />
are seen in public hospitals. The TE option<br />
is usually discussed with the patients before the surgery.<br />
Individuals who are not suitable for the TE option<br />
are all given the other 3 alaryngeal speech options. Most<br />
patients voluntarily choose the EL speech as their immediate<br />
means for communication after surgery. The other<br />
2 options, ES <strong>and</strong> PD, are also tried by patients during<br />
rehabilitation follow-up sessions.<br />
The present study compared the speech intelligibility<br />
<strong>and</strong> acceptability among 4 currently available alaryngeal<br />
Participants, No. Months After Laryngectomy, No.<br />
Alaryngeal <strong>Speech</strong> Mode<br />
Female Male Total Mean (SD) Range<br />
Esophageal 0 7 7 120.43 (51.23) 24-194<br />
Electrolarynx 0 14 14 62.79 (62.41) 6-190<br />
Tracheosophageal 1 12 13 70.92 (51.23) 20-181<br />
Pneumatic device 3 12 15 82.53 (60.44) 7-192<br />
speech modes, namely, EL, ES, TE, <strong>and</strong> PD speech using<br />
2 distinct age groups of listeners (25-33 years vs 60-65<br />
years). The study also compared the communicationrelated<br />
QOL among speakers of these 4 alaryngeal speech<br />
modes. The information on the speech intelligibility, acceptability,<br />
<strong>and</strong> QOL in different Chinese alaryngeal<br />
speech methods would provide health care workers <strong>and</strong><br />
alaryngeal speakers an opportunity to make informed decisions<br />
as to the selection of a more suitable alaryngeal<br />
speech method. Although the PD method is not popular<br />
in Western societies, the information provided herein will<br />
serve to show that it can be a useful option for alaryngeal<br />
speakers whose mother tongue is one of those tonal<br />
languages.<br />
METHODS<br />
PARTICIPANTS<br />
Fifty-six native Cantonese-speaking alaryngeal speakers recruited<br />
from the New Voice Club of Hong Kong participated<br />
in the present study. All these participants had stopped attending<br />
the regular speech therapy clinics provided by the hospitals,<br />
<strong>and</strong> therefore it can be assumed that they all had achieved<br />
their maximum ability in acquiring the new speaking methods.<br />
Each participant was given a hearing screening test at octave<br />
frequencies ranging from 250 to 8 kHz at a 20-dB hearing<br />
level (HL). Seven participants were excluded from the study<br />
owing to other medication complications or having failed the<br />
hearing screening test. Therefore, only data from 49 alaryngeal<br />
speakers, ranging in age from 40 to 77 years (mean[SD]<br />
age, 65.37 [8.77] years) <strong>and</strong> with a postoperative period ranging<br />
from 6 to 194 months (mean [SD] duration, 79.22 [58.76]<br />
months) were included in the final analysis. Table 1 shows<br />
the sex distribution <strong>and</strong> postoperation time across the 4 alaryngeal<br />
speech method groups. All of the EL speakers used the<br />
neck-type EL devices, <strong>and</strong> all of the TE speakers were fitted with<br />
the Blom-Singer (InHealth Technologies, Carpinteria, California)<br />
valve using digital occlusion. The seemingly low proportion<br />
of female alaryngeal speakers indeed reflected the distribution<br />
of sex in the alaryngeal-speaking population in Hong<br />
Kong. Kruskal-Wallis 1-way analysis of variance (ANOVA) revealed<br />
no significant differences in the length of postoperation<br />
period (P=.27), age (P=.12), <strong>and</strong> education level (P=.20)<br />
among the 4 alaryngeal speech method groups.<br />
PROCEDURES<br />
Perceptual Evaluations of <strong>Speech</strong><br />
<strong>Intelligibility</strong> <strong>and</strong> <strong>Acceptability</strong><br />
<strong>Speech</strong> Material. The Cantonese Sentence <strong>Intelligibility</strong> Test<br />
(CSIT) 16 was used to assess the speech intelligibility of the par-<br />
(REPRINTED) ARCH OTOLARYNGOL HEAD NECK SURG/ VOL 135 (NO. 7), JULY 2009 WWW.ARCHOTO.COM<br />
705<br />
©2009 American Medical Association. All rights reserved.<br />
Downloaded From: http://173.193.11.201/ on 03/26/2013
ticipants at sentence level. The CSIT was developed from the<br />
Assessment of <strong>Intelligibility</strong> of Dysarthric <strong>Speech</strong> (AIDS). 17 In<br />
the CSIT, 16 there are a total of 1100 daily Chinese (Cantonese)<br />
sentences (100 sentences, each with 5-15 words, for each sentence<br />
length set), which make up the master pool. These sentences<br />
do not contain quotations, reduplication, parentheses,<br />
proper names, or numbers larger than 10. For each speaker, a<br />
unique set of 22 sentences was r<strong>and</strong>omly selected within the<br />
master pool, with a sentence length that varied from 5 to 15<br />
words. Two sentences were selected for each sentence length,<br />
<strong>and</strong> they were all printed out on a single sheet of A4 paper<br />
(2129-cm) in a 22-point font size.<br />
Recording Procedures. Recording of speech samples took place<br />
in a quiet room located at the New Voice Club of Hong Kong<br />
with the background noise level kept below 45 dB (Aweighted)<br />
(hereinafter dBA) as measured by a sound level meter.<br />
All the speech samples were recorded using a Sony<br />
MZ-R909 Mini-Disc Digital recorder (Tokyo, Japan) with a Shure<br />
SM48 dynamic microphone (Niles, Illinois) held 10 cm away<br />
from the center of the speaker’s mouth. Each speaker was given<br />
a brief practice period to become familiar with the speech materials,<br />
recording instructions, <strong>and</strong> procedures before the actual<br />
recording. To ensure that the quality of the recorded speech<br />
samples was representative of the speaker’s daily communication<br />
speech, a r<strong>and</strong>omly selected sample from the recordings<br />
of each participant was played back to that individual. They<br />
were asked to judge if the recorded speech sample was representative<br />
of the quality of their daily communication speech.<br />
If the played-back sample was judged to be not representative<br />
by the individual speaker, the recording procedure was repeated<br />
until a representative sample was recorded.<br />
In the recording of the sentences from the CSIT, 16 the sentence<br />
list to be read was placed in front of each individual. The<br />
participants were instructed to read each of the 22 sentences<br />
as clearly as possible. The order of sentences to be recorded<br />
was r<strong>and</strong>omized to avoid any possible order effect. Also, to avoid<br />
any reading errors owing to misreading of words, the following<br />
procedures were used. First, the investigator (I.K.-Y.L.)<br />
would indicate to the speaker each sentence to be read by pointing<br />
to the respective sentence. The speaker was asked to read<br />
the indicated sentence together with the investigator once. Then<br />
the investigator read the sentence aloud alone once, followed<br />
by the speaker, who read the sentence aloud alone once. This<br />
final attempt by the speaker was recorded. If any obvious reading<br />
error was noted in the recording, that sentence would be<br />
recorded again.<br />
Listeners. Six native Cantonese-speaking adults served as judges<br />
to transcribe <strong>and</strong> rate the speech samples. Three of them were<br />
25 to 33 years old (younger judge group), <strong>and</strong> 3 others were<br />
60 to 65 years old (older judge group). They were asked to transcribe<br />
<strong>and</strong> provide perceptual ratings of speech impairment for<br />
all the speech samples. All judges had no prior exposure to individuals<br />
who had undergone a laryngectomy <strong>and</strong> were alaryngeal<br />
speakers. They were not aware of the content of the<br />
speech materials used in the study before the listening tasks.<br />
All of them passed a hearing screening test at a threshold level<br />
of 20-dB HL at each octave frequency (250-8000 Hz).<br />
Listening Tasks<br />
A Sony CMT-JST MD high-fidelity sound system was used to<br />
play all the recorded speech samples to each individual judge<br />
with the speakers at a distance of 2 m in a quiet room (with a<br />
background noise level 45 dBA as measured by a sound level<br />
meter). The intensity level of the playback was adjusted by in-<br />
dividual judges to a comfortable level. The order of the alaryngeal<br />
speakers <strong>and</strong> the recorded sentences of each speaker was<br />
played back at a r<strong>and</strong>omized order across listeners to avoid any<br />
possible order effect.<br />
Each of the 6 judges scored each alaryngeal speaker individually.<br />
They were asked to judge speech samples of the CSIT first.<br />
They were instructed to orthographically transcribe the 22 sentences<br />
<strong>and</strong> rate the severity of speech impairment of each speaker<br />
based on the speech samples on an 11-point (0-10) equalappearing<br />
interval (EAI) scale with 0 corresponding to no speech<br />
impairment <strong>and</strong> 10 corresponding to very severe speech impairment.<br />
In the orthographic transcription task, the judges were first<br />
asked to listen to all 22 sentences together once <strong>and</strong> then listen<br />
to each of the sentences a second time, pausing between 2 sentences<br />
whenever necessary, to transcribe each sentence word by<br />
word on the score sheets. The guideline suggested by Yorkston<br />
<strong>and</strong> Beukelman 17 was followed; that is, judges were not allowed<br />
to listen to each sentence more than 2 times <strong>and</strong> were encouraged<br />
to guess at words that were not completely understood.<br />
Each judge was required to repeat these tasks for 40 r<strong>and</strong>omly<br />
selected speaker sample sets (ie, 80% of the total number<br />
of speaker sample sets) 2 weeks after their first listening<br />
task. This procedure was to establish the intrajudge reliability.<br />
The interjudge reliability was established by correlating the<br />
intelligibility scores transcribed by an individual judge with the<br />
other 2 judges within the younger <strong>and</strong> older judge groups.<br />
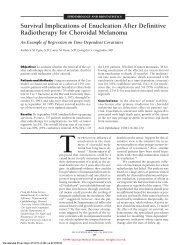
<strong>Communication</strong>-<strong>Related</strong> QOL<br />
Each participant also completed the <strong>Communication</strong> Activity <strong>and</strong><br />
Participation After Laryngectomy 18 (CAPAL) questionnaire<br />
(Figure) to evaluate the extent of communication-related QOL<br />
deterioration in alaryngeal speakers. This profile was developed<br />
using the International Classification of Functioning, Disability,<br />
<strong>and</strong> Health (ICF) framework, 19 which evaluates the communication-related<br />
QOL in individuals who have undergone laryngectomy<br />
<strong>and</strong> experienced 3 levels of disablement, namely, speech<br />
impairment, communication activity limitation, <strong>and</strong> communication<br />
participation restriction. The CAPAL 18 has been shown to<br />
be a valid <strong>and</strong> reliable tool. In short, content validity was established<br />
using focus groups composed of alaryngeal speakers (n=15),<br />
their relatives (n=24), <strong>and</strong> speech therapists (n=10). They were<br />
asked to finalize the appropriate items to be included in the final<br />
version. Construct validity was established by comparing CAPAL<br />
results with 2 validated self-administered questionnaires: the Chinese<br />
version of the Medical Outcomes Study 36-item Short-<br />
Form Instrument 20 <strong>and</strong> the Chinese-Cantonese version of the Hospital<br />
Anxiety <strong>and</strong> Depression Scale 21 using Pearson r correlation<br />
coefficients. Significant correlations that varied from 0.26 to 0.6<br />
were found between the CAPAL <strong>and</strong> the other 2 questionnaires<br />
(P.05 for all comparisons). The internal consistency showed a<br />
Cronbach coefficient of 0.98 <strong>and</strong> a test-retest reliability of 0.84.<br />
Responses to each item were collected using an 11-point (0-<br />
10) EAI scale. Respondents were asked to put a cross on the<br />
point that best represented their response, with 0 corresponding<br />
to never <strong>and</strong> 10 corresponding to always.<br />
DATA ANALYSIS<br />
Calculation of <strong>Speech</strong> <strong>Intelligibility</strong> <strong>and</strong><br />
<strong>Acceptability</strong> Scores<br />
The speech intelligibility score was obtained by dividing the<br />
number of correctly transcribed words by the total number of<br />
words (220). For each individual speaker, a total of 6 speech<br />
intelligibility scores were obtained, 3 from the younger judge<br />
group <strong>and</strong> another 3 from the older judge group. The mean<br />
(REPRINTED) ARCH OTOLARYNGOL HEAD NECK SURG/ VOL 135 (NO. 7), JULY 2009 WWW.ARCHOTO.COM<br />
706<br />
©2009 American Medical Association. All rights reserved.<br />
Downloaded From: http://173.193.11.201/ on 03/26/2013
Self-perceived Ratings of <strong>Speech</strong> Impairment<br />
1. How severe do you think is your speech impairment?<br />
Daily <strong>Communication</strong><br />
2. How often does someone you are familiar with (eg, spouse/family members) ask<br />
you to repeat in face-to-face conversation because of not underst<strong>and</strong>ing your<br />
speech?<br />
3. How often have you avoided talking to someone you are familiar with<br />
(eg, spouse/family members) face-to-face because of your speech impairment?<br />
4. How often does someone who has regular contact with you (eg, relatives/ friends)<br />
ask you to repeat in face-to-face conversation because of not underst<strong>and</strong>ing your<br />
speech?<br />
5. How often have you avoided talking to someone who has regular contact with you<br />
(eg, relatives/friends) face-to-face because of your speech impairment?<br />
6. How often do strangers ask you to repeat in face-to-face conversation because of<br />
not underst<strong>and</strong>ing your speech (eg, ordering in a restaurant)?<br />
7. How often have you avoided talking to strangers face-to-face because of your<br />
speech impairment (eg, ordering in a restaurant)?<br />
8. How often does someone you are familiar with (eg, spouse/family members) ask<br />
you to repeat in telephone conversation because of not underst<strong>and</strong>ing your speech?<br />
9. How often have you avoided talking to someone you are familiar with<br />
(eg, spouse/family members) on phone because of your speech impairment?<br />
10. How often does someone who has regular contact with you (eg, relatives/friends)<br />
ask you to repeat in telephone conversation because of not underst<strong>and</strong>ing your<br />
speech?<br />
11. How often have you avoided talking to someone who has regular contact with you<br />
(eg, relatives/friends) on phone because of your speech impairment?<br />
12. How often do strangers ask you to repeat in telephone conversation because of not<br />
underst<strong>and</strong>ing your speech (eg, government service hotlines)?<br />
13. How often have you avoided talking to strangers on phone because of your speech<br />
impairment (eg, government service hotlines)?<br />
14. How often does your speech impairment affect you talking in noisy environment<br />
(eg, in a Chinese restaurant)?<br />
15. Have you avoided talking in noisy environment because of your speech impairment<br />
(eg, in a Chinese restaurant)?<br />
16. How often does your speech impairment affect you talking in quiet environment<br />
(eg, in the library)?<br />
17. How often have you avoided talking in quiet environment because of your speech<br />
impairment (eg, in the library)?<br />
18. How often does your speech impairment affect you talking in groups?<br />
19. How often have you avoided talking in groups because of your speech impairment?<br />
20. How often does your speech impairment affect you to express your emotions<br />
verbally?<br />
21. How often have you avoided expressing your emotions verbally because of your<br />
speech impairment?<br />
Figure. <strong>Communication</strong> Activity <strong>and</strong> Participation After Laryngectomy questionnaire. 18<br />
speech intelligibility scores given to each speaker by both the<br />
younger judges <strong>and</strong> the older judges were compared.<br />
Calculation of the CAPAL Scores<br />
The item scores were computed to obtain the following section<br />
scores:<br />
1. Self-perceived speech impairment score (1 item, maximum<br />
score=10)<br />
2. Daily communication section score (20 items, maximum<br />
score=200)<br />
3. Social communication section score (6 items, maximum<br />
score=60)<br />
4. Job section score (4 items, maximum score=40)<br />
5. Emotion section score (14 items, maximum score=140)<br />
6. Total CAPAL score (the sum of the 5 section scores)<br />
(maximum score=450)<br />
Within each section of the daily communication, social communication,<br />
<strong>and</strong> job sections, items were organized in pairs;<br />
the first item addressed activity limitation, <strong>and</strong> the second item<br />
addressed participation restriction. Therefore, 2 additional scores<br />
were computed for each of these 3 sections:<br />
Social <strong>Communication</strong><br />
22. How often does your speech impairment affect you making new friends?<br />
23. How often have you avoided making new friends because of your speech<br />
impairment?<br />
24. How often does your speech impairment affect you talking in your usual leisure<br />
activities (eg, playing mahjong, hiking, playing chess)?<br />
25. How often have you avoided talking in your usual leisure activities because of your<br />
speech impairment?<br />
26. How often does your speech impairment affect you talking in social gatherings<br />
(eg, gatherings with friends <strong>and</strong> ex-colleagues)?<br />
27. How often have you avoided talking in social gatherings because of your speech<br />
impairment?<br />
Job<br />
28. Does the speech impairment affect your working performance?<br />
29. How often have you thought of quitting/changing your job because of your speech<br />
impairment?<br />
30. Does the speech impairment increase your stress at work?<br />
31. How often have you avoided working because of your speech impairment?<br />
Emotion<br />
32. Do you feel embarrassed when you are talking to someone you are familiar with<br />
(eg, spouse/family members)?<br />
33. Do you feel embarrassed when you are talking to someone who has regular contact<br />
with you (eg, relatives/friends)?<br />
34. Do you feel embarrassed when you are talking to strangers?<br />
35. Do you feel upset when you are talking to someone you are familiar with<br />
(eg, spouse/family members)?<br />
36. Do you feel upset when you are talking to someone who has regular contact with you<br />
(eg, relatives/friends)?<br />
37. Do you feel upset when you are talking to strangers?<br />
38. Do you feel tense when you are talking to someone you are familiar with<br />
(eg, spouse/family members)?<br />
39. Do you feel tense when you are talking to someone who has regular contact with you<br />
(eg, relatives/friends)?<br />
40. Do you feel tense when you are talking to strangers?<br />
41. Do you feel low self-esteem when you are talking to someone you are familiar with<br />
(eg, spouse/family members)?<br />
42. Do you feel low self-esteem when you are talking to someone who has regular<br />
contact with you (eg, relatives/friends)?<br />
43. Do you feel low self-esteem when you are talking to strangers?<br />
44. Does your speech impairment affect your self-image (how you think of yourself)?<br />
45. Does your speech impairment affect your communication-related characteristics?<br />
1. <strong>Communication</strong> activity limitation (CAL) scores: the sum<br />
of scores from the first items of the paired questions within each<br />
section. The sum of CAL scores from the 3 sections resulted in<br />
the total CAL.<br />
2. <strong>Communication</strong> participation restriction (CPR) scores:<br />
sum of scores from the second items of the paired questions<br />
within each section. The sum of CPR scores from the 3 sections<br />
resulted in the total CPR.<br />
RESULTS<br />
PERCEPTUAL RATINGS<br />
OF SPEECH IMPAIRMENTS<br />
Table 2 lists the perceptual ratings of alaryngeal speakers’<br />
speech impairment by the 2 groups of judges. The<br />
mean ratings from younger <strong>and</strong> older judges were 7.1 <strong>and</strong><br />
5.3 (maximum score=10), respectively, which are significantly<br />
different (df, 96; t, 5.25; P.001), indicating<br />
that older judges perceived the alaryngeal speech to be<br />
less severe than younger judges.<br />
(REPRINTED) ARCH OTOLARYNGOL HEAD NECK SURG/ VOL 135 (NO. 7), JULY 2009 WWW.ARCHOTO.COM<br />
707<br />
©2009 American Medical Association. All rights reserved.<br />
Downloaded From: http://173.193.11.201/ on 03/26/2013
Table 2. Perceptual Ratings of Alaryngeal Speakers a<br />
Group<br />
ES EL TE PD<br />
F3,45<br />
Younger judges 8.43 (0.98) 7.5 (0.86) 7.62 (0.87) 4.73 (1.03) 37.52b Older judges 7.14 (0.69) 4.5 (1.10) 6.38 (0.77) 3.20 (1.08) 39.14b There were also significant differences in the perceptual<br />
ratings between the different alaryngeal<br />
speaker groups within the younger <strong>and</strong> the older<br />
judge groups (1-way ANOVA: F3,45=37.52 [younger<br />
judges]; F 3,45=39.14 [older judges]; P.001 for both<br />
comparisons). Post hoc Scheffe tests revealed that the<br />
PD speaker group received significantly lower severity<br />
impairment ratings than the other groups of speakers<br />
(P.001 for all comparisons) from both the younger<br />
<strong>and</strong> the older judges.<br />
SPEECH INTELLIGIBILITY SCORES OF THE<br />
CANTONESE SENTENCE INTELLIGIBILITY TEST<br />
Table 3 lists the speech intelligibility scores of the<br />
CSIT 16 obtained by different speech groups. For both<br />
the younger <strong>and</strong> the older judges, there were significant<br />
differences in the CSIT scores among the alaryngeal<br />
speaker groups (1-way ANOVA: F3,45=38.54 [younger<br />
judges]; F3,45=36.00 [older judges]; P.001 for both<br />
comparisons). Post hoc comparison using Scheffe tests<br />
revealed that the PD speaker group received the highest<br />
CSIT score compared with the other groups of alaryngeal<br />
speakers (P.001 for all comparisons) from both<br />
group of judges.<br />
In the orthographic transcription tasks of the CSIT,<br />
reliability was assessed by Pearson r correlation coefficients.<br />
The intrajudge reliability of the older judge group<br />
was 0.74 (P=.001), <strong>and</strong> the interjudge reliability ranged<br />
from 0.64 to 0.72 (P=.001). For the younger judge group,<br />
the intrajudge reliability was 0.86 (P=.001), <strong>and</strong> the interjudge<br />
reliability ranged from 0.78 to 0.84 (P=.001).<br />
When comparing the speech intelligibility scores obtained<br />
from the younger judges <strong>and</strong> the older judges, the<br />
younger judges demonstrated a significantly higher score<br />
than the older judges (df, 96; t, 5.25; P.001).<br />
Perceptual Rating According to Alaryngeal <strong>Speech</strong> Mode<br />
Abbreviations: EL, electrolarynx; ES, esophageal; PD, pneumatic device; TE, tracheosophageal.<br />
aThe ratings, given as means (SDs) were made on an 11-point equal-appearing interval scale, with 0 indicating no speech impairment <strong>and</strong> 10, severe speech<br />
impairment.<br />
bP.001. Table 3. Cantonese Sentence <strong>Intelligibility</strong> Test Scores of Alaryngeal Speakers a<br />
Score According to Alaryngeal <strong>Speech</strong> Mode<br />
Group<br />
ES EL TE PD<br />
F3,45<br />
Younger judges 59.73 (7.97) 77.3 (7.01) 61.5 (6.82) 91.2 (4.80) 38.54b Older judges 56.9 (6.30) 62.0 (8.90) 59.1 (11.11) 79.7 (7.40) 36.00b Abbreviations: EL, electrolarynx; ES, esophageal; PD, pneumatic device; TE, tracheosophageal.<br />
a Maximum speech intelligibility score=100. Data are given as means (SDs).<br />
b P.001.<br />
PERCEIVED COMMUNICATION-RELATED QOL<br />
AFTER LARYNGECTOMY<br />
Table 4 lists the 5 section scores <strong>and</strong> total CAPAL scores<br />
in the different alaryngeal speech groups. It should be<br />
noted that in the analysis, data in the job section were<br />
excluded because only 5% of the total participants (3 of<br />
63) responded to the job section. Most of the participants<br />
were either retired or unemployed at the time of<br />
testing. Results of 1-way ANOVA revealed significant differences<br />
in the daily communication section score<br />
(P=.006), emotion section score (P=.04), <strong>and</strong> the total<br />
CAPAL score (P=.01). Electrolaryngeal speech scored the<br />
highest, whereas TE speech scored the lowest in the 4<br />
speaker groups for these 3 scores. Post hoc Scheffe tests<br />
of these 3 scores further indicated that differences between<br />
EL <strong>and</strong> TE speech were statistically significant (daily<br />
communication section score, P=.02; emotion section<br />
score, P=.04; total CAPAL score, P=.02).<br />
Table 5 lists the CAL scores of different speech groups.<br />
Results of 1-way ANOVA revealed significant differences<br />
in daily communication (P.01) <strong>and</strong> total score<br />
(P.01) among different alaryngeal speaker groups. Electrolaryngeal<br />
speech scored the highest, whereas TE speech<br />
scored the lowest among the 4 speaker groups. Post hoc<br />
Scheffe tests of these 3 scores further indicated that differences<br />
between EL <strong>and</strong> TE speech were statistically significant<br />
(P.01).<br />
Table 6 lists the CPR scores. Significant differences<br />
were found with daily communication (P.01) <strong>and</strong> total<br />
scores (P.01) among the 4 alaryngeal speaker groups.<br />
Electrolaryngeal speech scored the highest, whereas PD<br />
speech scored the lowest among the 4 speaker groups.<br />
Post hoc Scheffe tests of these 3 scores further showed<br />
that differences between EL <strong>and</strong> PD speech were statistically<br />
significant (P.01).<br />
(REPRINTED) ARCH OTOLARYNGOL HEAD NECK SURG/ VOL 135 (NO. 7), JULY 2009 WWW.ARCHOTO.COM<br />
708<br />
©2009 American Medical Association. All rights reserved.<br />
Downloaded From: http://173.193.11.201/ on 03/26/2013
Table 4. <strong>Communication</strong> Activity <strong>and</strong> Participation After Laryngectomy (CAPAL) Questionnaire Scores of Alaryngeal Speakers a<br />
Questionnaire Section<br />
ES EL TE PD<br />
F3,45<br />
Self-perceived speech impairment, max score=10 2.00 (2.24) 2.93 (2.70) 2.08 (1.32) 2.93 (2.52) 0.59<br />
Daily communication, max score=200 59.00 (32.92) 81.86 (45.63) 37.31 (33.31) 42.00 (22.23) 4.68b Social communication, max score=60 23.14 (13.45) 24.14 (17.97) 10.46 (16.52) 18.67 (18.62) 1.61<br />
Job, max score=40 NAc 17.00 (5.66) 10.00c NAc NAd Emotion, max score=140 23.00 (24.69) 38.36 (28.17) 11.85 (17.81) 29.20 (18.87) 3.27e Total, max score=450 107.14 (67.78) 164.29 (83.87) 72.70 (57.71) 92.80 (54.22) 3.98b COMMENT<br />
SPEECH INTELLIGIBILITY AND ACCEPTABILITY<br />
OF ALARYNGEAL SPEECH MODES<br />
One of our objectives was to compare the speech intelligibility<br />
<strong>and</strong> acceptability among different alaryngeal<br />
speaker groups. Results revealed that PD speakers had<br />
the highest speech intelligibility <strong>and</strong> acceptability scores<br />
compared with those using the other 3 alaryngeal<br />
speech methods. This finding is consistent with that<br />
reported from studies 11,14 on lexical tone production<br />
among Cantonese-speaking alaryngeal speakers. Ching<br />
Score According to Alaryngeal <strong>Speech</strong> Mode<br />
Abbreviations: EL, electrolarynx; ES, esophageal; max, maximum; NA, not available; PD, pneumatic device; TE, tracheosophageal.<br />
a Data are given as means (SDs) except where indicated.<br />
b P.01.<br />
c There is no st<strong>and</strong>ard deviation for this score.<br />
d Analysis of variance result for the job score was not available owing to the limited number of participants.<br />
e P.05.<br />
Table 5. <strong>Communication</strong> Activity Limitation (CAL) Scores of Alaryngeal Speakers a<br />
Score According to Alaryngeal <strong>Speech</strong> Mode<br />
Questionnaire Section<br />
ES EL TE PD<br />
F3,45<br />
Daily communication, max score=100 31.86 (17.78) 40.71 (22.99) 17.69 (12.11) 23.27 (10.91) 5.04b Social communication, max score=30 11.71 (6.85) 12.07 (9.08) 5.23 (8.26) 11.67 (9.78) 1.79<br />
Job, max score=20 NAc 12.00 (1.41) 5.00c NAc NAd Total, max score=150 43.57 (24.54) 64.78 (28.39) 27.92 (18.66) 34.93 (17.83) 4.35b Abbreviations: EL, electrolarynx; ES, esophageal; max, maximum; NA, not available; PD, pneumatic device; TE, tracheosophageal.<br />
a Data are given as means (SDs) execpt where indicated.<br />
b P.01.<br />
c There is no st<strong>and</strong>ard deviation for this score.<br />
d Analysis of variance result for the job section score was not available owing to the limited number of participants.<br />
Table 6. <strong>Communication</strong> Participation Restriction Scores of Alaryngeal Speakers a<br />
Score According to Alaryngeal <strong>Speech</strong> Mode<br />
Questionnaire Section<br />
ES EL TE PD<br />
F3,45<br />
Daily communication, max score=100 27.14 (16.00) 41.14 (22.42) 20.62 (24.23) 18.73 (13.99) 3.48b Social communication, max score=30 11.43 (6.75) 12.07 (9.03) 5.23 (8.34) 7.00 (9.58) 1.78<br />
Job, max score=20 NAc 5.00 (7.07) 5.00c NAc NAd Total, max score=150 38.57 (22.59) 58.21 (32.02) 30.85 (33.99) 25.73 (20.16) 3.00b Abbreviations: EL, electrolarynx; ES, esophageal; max, maximum; NA, not available; PD, pneumatic device; TE, tracheosophageal.<br />
a Data are given as means (SDs) except where indicated.<br />
b P.05.<br />
c There is no st<strong>and</strong>ard deviation for this score.<br />
d Analysis of variance result for job section score was not available owing to the limited number of participants.<br />
et al 11 found that PD speakers had the highest lexical<br />
tone intelligibility, whereas Yiu et al 14 also showed that<br />
both PD <strong>and</strong> TE speakers were more efficient in conveying<br />
lexical tone. The present findings provide further<br />
support to the contention that lexical tone production<br />
is critical in determining the speech intelligibility<br />
of Cantonese-speaking alaryngeal speakers.<br />
In comparing the speech intelligibility scores of<br />
CSIT 16 obtained from Cantonese alaryngeal speakers in<br />
the present study with the scores obtained from other<br />
nontonal language studies using the AIDS, 17 the<br />
Cantonese-speaking alaryngeal speakers as a whole<br />
seemed to show relatively lower speech intelligibility.<br />
(REPRINTED) ARCH OTOLARYNGOL HEAD NECK SURG/ VOL 135 (NO. 7), JULY 2009 WWW.ARCHOTO.COM<br />
709<br />
©2009 American Medical Association. All rights reserved.<br />
Downloaded From: http://173.193.11.201/ on 03/26/2013
Bridges 6 reported a mean sentence intelligibility score of<br />
87.69% for English-speaking TE speakers <strong>and</strong> 81.71%<br />
for the ES speakers with naïve listeners. A higher intelligibility<br />
score (97.4%) was reported by McAuliffe et al 22<br />
with a group of TE speakers. One possible explanation<br />
for the discrepancy between the Cantonese- <strong>and</strong><br />
English-speaking alaryngeal speakers might have been<br />
the nature of the lexical tone in Cantonese. Cantonese<br />
alaryngeal speakers would have to control the lexical<br />
tone variations in order to convey the verbal messages<br />
effectively. With an inability or difficulty in producing<br />
the lexical tone in some alaryngeal speech, the intelligibility<br />
would thus be lower. In fact, it has been reported<br />
that different alaryngeal speech methods are different in<br />
conveying lexical tones. 11,14<br />
Interestingly, younger listeners tended to underst<strong>and</strong><br />
alaryngeal speech relatively better but with a lower<br />
acceptability toward it. The present findings are similar<br />
to those reported by Clark, 10 who found that age of the<br />
listeners has a potential influence on the acceptability <strong>and</strong><br />
underst<strong>and</strong>ing of alaryngeal speech.<br />
COMMUNICATION-RELATED QOL<br />
OF ALARYNGEAL SPEECH MODES<br />
Another objective of this study was to compare the communication-related<br />
QOL among speakers of the 4 alaryngeal<br />
speech modes. Although the PD speakers received the<br />
best speech intelligibility ratings, they did not perceive themselves<br />
as having the best communication-related QOL, as<br />
revealed by the CAPAL scores. The present results reveal<br />
that alaryngeal speakers who used TE speech methods received<br />
the lowest CAPAL scores (ie, the best communication-related<br />
QOL), followed by the PD speech. However,<br />
such differences between TE <strong>and</strong> PD speech were not statistically<br />
significant (P.05). The use of an external visible<br />
device in the PD speech method may have made it cosmetically<br />
less favorable than TE speech mode. Such a factor<br />
may have further imposed on the patient’s self-perception<br />
of communication efficiency, hence resulting in relatively<br />
poorer QOL. The present findings support the findings of<br />
the QOL studies, which used the ICF 19 framework. According<br />
to the ICF, 19 an impairment does not necessarily<br />
result in similar fashion of activity limitation <strong>and</strong> participation<br />
restriction. Therefore, causal relationship among the<br />
3 levels should not be assumed. In fact, it has been advocated<br />
that speech impairment in alaryngeal speakers does<br />
not necessarily reflect the extent of communication activity<br />
limitation <strong>and</strong> participation restriction. 23 This is borne<br />
out by our findings.<br />
CONCLUSION<br />
Findings from the present study shed light on the<br />
management of the communication-related QOL in<br />
alaryngeal speakers in general, although the data were<br />
obtained from the Chinese population. On the one<br />
h<strong>and</strong>, this study found that listeners of different ages<br />
had a considerable difference in their abilities in<br />
underst<strong>and</strong>ing <strong>and</strong> accepting alaryngeal speech. The<br />
younger the listeners, the easier it was for them to<br />
underst<strong>and</strong> alaryngeal speech, but they had a lower<br />
level of acceptability toward it. On the other h<strong>and</strong>, the<br />
older the listeners, the more difficult it was for them<br />
to underst<strong>and</strong> alaryngeal speech, but they had a better<br />
level of acceptability toward it. This finding highlights<br />
the need to consider the ages of the alaryngeal speaker’s<br />
significant others, relatives, <strong>and</strong> friends. In the<br />
clinical study of laryngectomy, the age of the listeners<br />
or judges in rating alaryngeal speech should be taken<br />
into consideration.<br />
Moreover, in postlaryngectomy speech rehabilitation,<br />
the choice of different alaryngeal speech methods<br />
for new alaryngeal speakers should be based on empirical<br />
data. The present results indicate that ES speakers<br />
present with the poorest speech proficiency, <strong>and</strong> EL<br />
speakers perceive the poorest communication-related<br />
QOL. Although PD speech, which is more popular in<br />
the Chinese-speaking community, seems to be superior<br />
owing to its higher speech intelligibility in Chinese <strong>and</strong><br />
listeners’ acceptability ratings, TE speech reveals relatively<br />
better overall communication-related QOL than<br />
PD speech. Therefore, both TE <strong>and</strong> PD speech have<br />
their own advantages in the Chinese population. Considering<br />
that the ultimate goal in postlaryngectomy speech<br />
rehabilitation is to enhance an alaryngeal speaker’s QOL, 23<br />
we contend that TE speech achieves an overall more favorableoutcome<strong>and</strong>QOLforChinesealaryngealspeakers.We<br />
also argue that this conclusion—TE speech achieves a<br />
better outcome—can be applied equally well to Western<br />
communities.<br />
Submitted for Publication: January 27, 2008; final<br />
revision received May 12, 2008; accepted May 23,<br />
2008.<br />
Correspondence: Edwin M.-L. Yiu, PhD, Voice Research<br />
Laboratory, Division of <strong>Speech</strong> <strong>and</strong> Hearing Sciences,<br />
University of Hong Kong, 5/F Prince Philip Dental<br />
Hospital, 34 Hospital Rd, Hong Kong (eyiu@hku<br />
.hk).<br />
Author Contributions: All of the authors had full access<br />
to all the data in the study <strong>and</strong> take full responsibility<br />
for the integrity of the data <strong>and</strong> the accuracy of the<br />
data analysis. Study concept <strong>and</strong> design: Law <strong>and</strong> Yiu. Acquisition<br />
of data: Law. Analysis <strong>and</strong> interpretation of data:<br />
Law <strong>and</strong> Ma. Drafting of the manuscript: Law <strong>and</strong> Ma. Critical<br />
revision of the manuscript for important intellectual content:<br />
Yiu. Statistical analysis: Ma. Obtained funding: Yiu.<br />
Administrative, technical, <strong>and</strong> material support: Law. Study<br />
supervision: Law <strong>and</strong> Yiu.<br />
Financial Disclosure: None reported.<br />
Funding/Support: This study was supported in part by<br />
a grant from the Voice Research Laboratory, University<br />
of Hong Kong (Ms Law).<br />
Additional Contributions: The New Voice Club of Hong<br />
Kong assisted with participant recruitment.<br />
REFERENCES<br />
1. Doyle PC. Foundations of Voice <strong>and</strong> <strong>Speech</strong> Rehabilitation Following Laryngeal<br />
Cancer. San Diego, CA: Singular Publishing; 1994.<br />
2. Shames GH, Font J, Matthews J. Factors related to speech proficiency of the<br />
laryngectomized. J <strong>Speech</strong> Hear Disord. 1963;28:273-287.<br />
(REPRINTED) ARCH OTOLARYNGOL HEAD NECK SURG/ VOL 135 (NO. 7), JULY 2009 WWW.ARCHOTO.COM<br />
710<br />
©2009 American Medical Association. All rights reserved.<br />
Downloaded From: http://173.193.11.201/ on 03/26/2013
3. Bennett S, Weinberg B. <strong>Acceptability</strong> ratings of normal, esophageal, <strong>and</strong> artificial<br />
larynx speech. J <strong>Speech</strong> Hear Res. 1973;16(4):608-615.<br />
4. Hyman M. An experimental study of artificial-larynx <strong>and</strong> esophageal speech.<br />
J <strong>Speech</strong> Hear Disord. 1955;20(3):291-299.<br />
5. McCroskey RL, Mulligan M. The relative intelligibility of esophageal speech <strong>and</strong><br />
artificial-larynx speech. J <strong>Speech</strong> Hear Disord. 1963;28:37-41.<br />
6. Bridges A. <strong>Acceptability</strong> ratings <strong>and</strong> intelligibility scores of alaryngeal speakers<br />
by three listeners groups. Br J Disord Commun. 1991;26(3):325-335.<br />
7. Max L, De Bruyn W, Steurs W. <strong>Intelligibility</strong> of oesophageal <strong>and</strong> tracheosophageal<br />
speech: preliminary observations. Eur J Disord Commun. 1997;32(4):<br />
429-440.<br />
8. Robbins J, Fisher H, Blom E, Singer M. A comparative acoustic study of normal,<br />
esophageal <strong>and</strong> tracheosophageal speech production. J <strong>Speech</strong> Hear Disord. 1984;<br />
49(2):202-210.<br />
9. Clark JG, Stemple JC. Assessment of three modes of alaryngeal speech with a<br />
synthetic sentence identification (SSI) task in varying message-to-competition<br />
ratios. J <strong>Speech</strong> Hear Res. 1982;25(3):333-338.<br />
10. Clark JG. Alaryngeal speech intelligibility <strong>and</strong> the older listener. J <strong>Speech</strong> Hear<br />
Disord. 1985;50(1):60-65.<br />
11. Ching TY, Williams R, Hasselt A. <strong>Communication</strong> of lexical tones in Cantonese<br />
alaryngeal speech. J <strong>Speech</strong> Hear Res. 1994;37(3):557-563.<br />
12. Ng ML, Kwok IC-L, Chow WS-F. <strong>Speech</strong> performance of adult Cantonesespeaking<br />
laryngectomees using different types of alaryngeal phonation. J Voice.<br />
1997;11(3):338-344.<br />
13. Wong SH, Cheung CC, Yuen AP, Ho WK, Wei WI. Assessment of tracheosophageal<br />
speech in a tonal language: a prospective study. Arch Otolaryngol Head Neck<br />
Surg. 1997;123(1):88-92.<br />
14. Yiu EM-L, Van Hasselt CA, Williams SR, Woo JK-S. <strong>Speech</strong> intelligibility in tone<br />
language (Chinese) laryngectomy speakers. Eur J Disord Commun. 1994;29<br />
(4):339-347.<br />
15. Clements KS, Rassekh CH, Seikaly H, Hokanson JA, Calhoun KH. <strong>Communication</strong><br />
after laryngectomy: an assessment of patient satisfaction. Arch Otolaryngol<br />
Head Neck Surg. 1997;123(5):493-496.<br />
16. Lo A. <strong>Intelligibility</strong> <strong>and</strong> <strong>Acceptability</strong> Measures of Cantonese Dysarthric <strong>Speech</strong><br />
[BSc dissertation]. University of Hong Kong; 1999.<br />
17. Yorkston KM, Beukelman DR. Assessment of <strong>Intelligibility</strong> of Dysarthric <strong>Speech</strong>.<br />
Tigard, OR: CC Publications Inc; 1981.<br />
18. Law IK-Y. <strong>Communication</strong> Activity <strong>and</strong> Participation After Laryngectomy [MPhil<br />
dissertation]. University of Hong Kong; 2005.<br />
19. World Health Organization. International Classification of Functioning, Disability<br />
<strong>and</strong> Health (ICF). Geneva, Switzerl<strong>and</strong>: World Health Organization; 2001.<br />
20. Lam CL-K, G<strong>and</strong>ek B, Ren XS, Chan MS. Tests of scaling assumptions <strong>and</strong> construct<br />
validity of the Chinese (HK) version of the SF-36 Health Survey. J Clin<br />
Epidemiol. 1998;51(11):1139-1147.<br />
21. Leung CM, Wing YK, Kwong PK, Lo A, Shum K. Validation of the Chinese-<br />
Cantonese version of the Hospital Anxiety <strong>and</strong> Depression Scale <strong>and</strong> comparison<br />
with the Hamilton Rating Scale of Depression. Acta Psychiatr Sc<strong>and</strong>. 1999;<br />
100(6):456-461.<br />
22. McAuliffe MJ, Ward EC, Bassett L, Perkins K. Functional speech outcomes after<br />
laryngectomy <strong>and</strong> pharyngolaryngectomy. Arch Otolaryngol Head Neck Surg. 2000;<br />
126(6):705-709.<br />
23. Eadie TL. The ICF: a proposed framework for comprehensive rehabilitation of<br />
individuals who use alaryngeal speech. Am J <strong>Speech</strong> Lang Pathol. 2003;12<br />
(2):189-197.<br />
(REPRINTED) ARCH OTOLARYNGOL HEAD NECK SURG/ VOL 135 (NO. 7), JULY 2009 WWW.ARCHOTO.COM<br />
711<br />
©2009 American Medical Association. All rights reserved.<br />
Downloaded From: http://173.193.11.201/ on 03/26/2013