Prevention of Exuberant Granulation Tissue and Neovascularization ...
Prevention of Exuberant Granulation Tissue and Neovascularization ...
Prevention of Exuberant Granulation Tissue and Neovascularization ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
LABORATORY SCIENCES<br />
<strong>Prevention</strong> <strong>of</strong> <strong>Exuberant</strong> <strong>Granulation</strong> <strong>Tissue</strong> <strong>and</strong><br />
<strong>Neovascularization</strong> in the Rat Cornea by Naltrexone<br />
Ian S. Zagon, MS, PhD; Matthew S. Klocek, MS; James W. Griffith, DVM; Joseph W. Sassani, MD, MHA;<br />
András M. Komáromy, DVM, PhD; Patricia J. McLaughlin, MS, DEd<br />
Objective: To determine whether topical application <strong>of</strong><br />
naltrexone prevents exuberant granulation tissue formation<br />
with neovascularization in diabetic rat corneas.<br />
Methods: Diabetes was induced with streptozotocin. A<br />
5-mm corneal abrasion at 9 or 11 weeks was treated topically<br />
for 7 days (4 times daily) with naltrexone or a sterile<br />
vehicle.<br />
Results: Within 2 to 5 days after reepithelialization, diabetic<br />
rats given the sterile vehicle had a 41% incidence<br />
<strong>of</strong> corneal lesions represented by exuberant granulation<br />
tissue with corneal neovascularization extending from the<br />
limbus. These lesions exhibited edema, cellular <strong>and</strong> vascular<br />
inflammation, <strong>and</strong> disruption <strong>of</strong> stromal lamella by<br />
fibrovascular tissue <strong>and</strong> calcium mineralization, but infection<br />
was not detected. No corneal lesions were re-<br />
Author Affiliations:<br />
Departments <strong>of</strong> Neural <strong>and</strong><br />
Behavioral Sciences (Drs Zagon<br />
<strong>and</strong> McLaughlin <strong>and</strong><br />
Mr Klocek), Comparative<br />
Medicine (Dr Griffith), <strong>and</strong><br />
Ophthalmology (Dr Sassani),<br />
The Milton S. Hershey Medical<br />
Center, Pennsylvania State<br />
University, Hershey; <strong>and</strong> the<br />
Department <strong>of</strong> Clinical Studies,<br />
School <strong>of</strong> Veterinary Medicine,<br />
University <strong>of</strong> Pennsylvania,<br />
Philadelphia (Dr Komáromy).<br />
CORNEAL NEOVASCULARIZAtion<br />
has been estimated to<br />
affect 1.4 million Americans<br />
annually. 1 Corneal<br />
neovascularization is associated<br />
with a wide variety <strong>of</strong> conditions,<br />
including contact lens wear, surgical<br />
<strong>and</strong> nonsurgical trauma, alkali <strong>and</strong><br />
other chemical burns, <strong>and</strong> infection. 1-3 Corneal<br />
neovascularization may be helpful in<br />
combating infections, assisting in corneal<br />
healing, <strong>and</strong> arresting autoimmune<br />
corneal melting. 3,4 Nevertheless, such vascularization<br />
can lead to corneal scarring,<br />
edema, lipid deposition, <strong>and</strong> inflammation<br />
that may significantly compromise<br />
corneal transparency <strong>and</strong> result in severe<br />
visual impairment, including blindness.<br />
1-3 The etiology <strong>of</strong> corneal neovascularization<br />
is unclear, though the association<br />
<strong>of</strong> stromal edema proximal to the<br />
limbus has been proposed as necessary to<br />
allow blood vessels into the usually compact<br />
stroma. 1-3,5 Treatment modalities<br />
include surgery, topical corticosteroids,<br />
angiostatic steroids, nonsteroidal antiinflammatory<br />
agents, <strong>and</strong> natural inhibi-<br />
corded in the diabetic group treated with naltrexone or<br />
the control group given the sterile vehicle. Diabetic rats<br />
with corneal lesions given the sterile vehicle reepithelialized<br />
more slowly than diabetic rats given the sterile vehicle<br />
without such lesions, but no difference in blood glucose<br />
levels were noted.<br />
Conclusions: Using a minimally invasive model in diabetic<br />
rats, topical naltrexone normalizes corneal wound<br />
healing <strong>and</strong> prevents neovascularization.<br />
Clinical Relevance: Direct application <strong>of</strong> naltrexone<br />
may serve as an important strategy for facilitating corneal<br />
healing <strong>and</strong> inhibiting corneal neovascularization.<br />
Arch Ophthalmol. 2008;126(4):501-506<br />
(REPRINTED) ARCH OPHTHALMOL / VOL 126 (NO. 4), APR 2008 WWW.ARCHOPHTHALMOL.COM<br />
501<br />
©2008 American Medical Association. All rights reserved.<br />
Downloaded From: http://173.193.11.201/ on 04/04/2013<br />
tors <strong>of</strong> angiogenesis. 1-3 However, treatments<br />
<strong>of</strong> ocular neovascularization may<br />
have limitations, such as recurrence, adverse<br />
effects, <strong>and</strong> patients being ineligible<br />
for therapy. 1 Thus, models <strong>of</strong> ocular<br />
neovascularization, as well as treatment<br />
regimens for corneal lesions with neovascularization,<br />
are needed.<br />
In previous investigations, we have reported<br />
that topical treatment with the opioid<br />
antagonist naltrexone facilitates corneal<br />
reepithelialization in healthy <strong>and</strong><br />
diabetic corneas. 6-9 Subsequent preliminary<br />
histological examination has revealed<br />
that a subset <strong>of</strong> reepithelialized<br />
poorly controlled diabetic rat corneas exhibit<br />
exuberant granulation tissue formation<br />
with stromal neovascularization.<br />
These observations have led to the present<br />
study, which examines the hypothesis<br />
that topical application <strong>of</strong> the opioid<br />
antagonist naltrexone prevents granulation<br />
tissue formation <strong>and</strong> accompanying<br />
neovascularization in a unique model <strong>of</strong><br />
delayed wound healing in rats with type<br />
1 diabetes.
Mean Weight, g<br />
Mean Glucose Level, mg/dL<br />
600<br />
500<br />
400<br />
300<br />
200<br />
100<br />
0<br />
600<br />
500<br />
400<br />
300<br />
200<br />
100<br />
0<br />
A Control<br />
Diabetic<br />
B<br />
0<br />
Control<br />
Diabetic<br />
0<br />
∗<br />
2 4 6 8<br />
∗<br />
METHODS<br />
∗ ∗ ∗<br />
1 4 8<br />
Time, wk<br />
Figure 1. Body weights (A) <strong>and</strong> glucose levels (B) <strong>of</strong> rats rendered diabetic<br />
with streptozotocin (n=65) <strong>and</strong> untreated animals receiving citrate buffer<br />
(controls [n=26]). Body weight was recorded at the time <strong>of</strong> streptozotocin<br />
injection (week 0) <strong>and</strong> every 2 weeks thereafter. Blood glucose levels were<br />
recorded 1, 4, <strong>and</strong> 8 weeks after administration <strong>of</strong> streptozotocin. To convert<br />
glucose to mmol/L, multiply by 0.0555. *Indicates significantly different<br />
from control rats at P.001; error bars, st<strong>and</strong>ard error <strong>of</strong> the mean.<br />
ANIMALS AND INDUCTION OF DIABETES<br />
We obtained male Sprague-Dawley rats (weight, approximately<br />
175 g) from Charles River Laboratories (Wilmington,<br />
Massachusetts) <strong>and</strong> housed them under st<strong>and</strong>ard laboratory conditions.<br />
All investigations conformed to the regulations <strong>of</strong> the<br />
Association for Research in Vision <strong>and</strong> Ophthalmology <strong>and</strong> the<br />
National Institutes <strong>of</strong> Health <strong>and</strong> the guidelines <strong>of</strong> the Institutional<br />
Animal Care <strong>and</strong> Use Committee <strong>of</strong> the College <strong>of</strong> Medicine<br />
at Pennsylvania State University.<br />
Type 1 diabetes was induced according to Havel et al 10 <strong>and</strong><br />
Ahrén et al. 11 An intraperitoneal injection <strong>of</strong> 40 mg <strong>of</strong> streptozotocin<br />
(Sigma-Aldrich Corp, St Louis, Missouri) per kilogram<br />
<strong>of</strong> body weight in 0.5 mol/L <strong>of</strong> ice-cold citrate buffer (pH<br />
4.5) was administered. A second dose <strong>of</strong> streptozotocin (40 mg/<br />
kg) was injected 24 hours later. This regimen produced insulindeficient<br />
diabetes in 100% <strong>of</strong> the animals within 48 to 72 hours;<br />
this group consisted <strong>of</strong> 65 rats. Animals not receiving streptozotocin<br />
that were injected with citrate buffer served as the control<br />
group; this group consisted <strong>of</strong> 26 rats.<br />
Blood glucose levels were monitored from the tail vein using<br />
a True Track Smart System Glucometer (Home Diagnostics Inc,<br />
Ft Lauderdale, Florida) immediately before administering streptozotocin<br />
<strong>and</strong> at 1, 4, <strong>and</strong> 8 weeks after streptozotocin administration.<br />
A glucose level <strong>of</strong> 400 mg/dL [to convert to mmol/L,<br />
multiply by 0.0555] was considered the minimum level compatible<br />
with a stable nontoxic diabetic state. 12<br />
∗<br />
∗<br />
CORNEAL ABRASIONS<br />
The procedures for epithelial debridement <strong>and</strong> observation <strong>of</strong><br />
repair followed those reported earlier. 6-8 In brief, animals were<br />
anesthetized with a mixture <strong>of</strong> ketamine (70 mg/kg), xylazine<br />
(7 mg/kg), <strong>and</strong> acepromazine (10 mg/kg). Eyes were examined<br />
under a dissecting microscope. If judged to be disease free,<br />
a 5 mm–diameter circle was outlined in the center <strong>of</strong> the cornea<br />
with a disposable dermatological skin punch (Acuderm,<br />
Ft Lauderdale, Florida). The encircled corneal epithelium was<br />
removed with a No. 15 Bard-Parker scalpel blade. Care was taken<br />
not to injure the underlying basement membrane <strong>and</strong> subjacent<br />
corneal tissue. 6 Epithelial defects were created between 7:30<br />
<strong>and</strong> 8:30 AM or 4 <strong>and</strong> 5 PM; we chose these times because previous<br />
studies showed no differences in the labeling index between<br />
morning <strong>and</strong> afternoon. 6 Any animal that experienced<br />
bleeding in the course <strong>of</strong> mechanical abrasion was not included<br />
in the study. Only 1 eye was abraded at a time in each<br />
animal. The right eye was abraded on the ninth week following<br />
injection <strong>of</strong> streptozotocin. Two weeks later, following closure<br />
<strong>of</strong> the initial epithelial defect, the left eye was abraded.<br />
TOPICAL ADMINISTRATION OF NALTREXONE<br />
Naltrexone (Sigma-Aldrich) was prepared at concentrations <strong>of</strong><br />
10 −4 or 10 −5 M in a moxifloxacin hydrochloride ophthalmic<br />
solution (Vigamox; Alcon Inc, Ft Worth, Texas). Compounds<br />
were given as a single drop using the commercial applicator<br />
bottle to the central cornea <strong>of</strong> the injured eye, with the lower<br />
eyelid held away from the eye to avoid overflow. Eye drops were<br />
administered to unanesthetized animals at 7:30 AM, 10:30 AM,<br />
1:30 PM, <strong>and</strong> 4:30 PM for 7 consecutive days. Diabetic rats were<br />
r<strong>and</strong>omly assigned to receive either naltrexone or a vehicle,<br />
whereas control animals received only the vehicle.<br />
SLITLAMP OBSERVATIONS OF THE CORNEA<br />
All animals were examined with a h<strong>and</strong>held slitlamp microscope<br />
to document overall corneal morphology <strong>and</strong> pathology,<br />
particularly the progression <strong>of</strong> corneal lesions. Corneas<br />
were observed with the slitlamp every day after debridement<br />
for the first 7 days <strong>and</strong> every other day for 3 weeks. Rats were<br />
placed in an is<strong>of</strong>lurane chamber for 60 seconds, <strong>and</strong> evaluation<br />
with the slitlamp was conducted before <strong>and</strong> after dilation<br />
<strong>of</strong> each eye. Corneal lesions were graded subjectively as grade<br />
1, 2, or 3 depending on whether they covered no more than<br />
25%, 50%, or 75%, respectively, <strong>of</strong> the corneal surface area.<br />
PHOTOGRAPHY<br />
Animals were anesthetized in a Plexiglas chamber attached to<br />
an is<strong>of</strong>lurane vaporizer, <strong>and</strong> the residual epithelial defect was<br />
stained with topical fluorescein. Rat eyes were viewed using a<br />
dissecting microscope with a tungsten light source <strong>and</strong> a gelatin<br />
Wratten No. 47 filter <strong>and</strong> photographed with a chargecoupled<br />
device camera at 1.5 magnification. Photographs were<br />
taken immediately after epithelial debridement (0 hours) <strong>and</strong><br />
16, 24, 32, <strong>and</strong> 40 hours later. No animal was photographed at<br />
intervals shorter than 12 hours to prevent disruption <strong>of</strong> the healing<br />
process. The area <strong>of</strong> defect was determined using Optimas<br />
s<strong>of</strong>tware (Meyer Instruments Inc, Houston, Texas) <strong>and</strong> was calculated<br />
as the percentage <strong>of</strong> the original epithelial defect.<br />
HISTOLOGY<br />
Animals were euthanized at 2, 3, 4, or 21 days following debridement<br />
by a lethal intraperitoneal injection <strong>of</strong> 100 mg/kg sodium<br />
(REPRINTED) ARCH OPHTHALMOL / VOL 126 (NO. 4), APR 2008 WWW.ARCHOPHTHALMOL.COM<br />
502<br />
©2008 American Medical Association. All rights reserved.<br />
Downloaded From: http://173.193.11.201/ on 04/04/2013
A B C D<br />
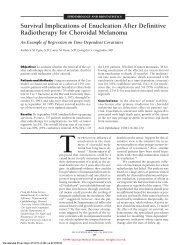
Figure 2. Photographs <strong>of</strong> corneas from control (A) <strong>and</strong> diabetic (B-D) rats treated topically with a sterile vehicle. Corneal lesions were divided into grades 1, 2, <strong>and</strong><br />
3, indicating lesions that covered no more than 25% (B), 50% (C), or 75% (D), respectively, <strong>of</strong> the corneal surface area.<br />
pentobarbital; eyes were enucleated <strong>and</strong> placed in formalin for<br />
24 hours <strong>and</strong> prepared for paraffin embedding. Vertical sections<br />
(8 µm) that included the corneal surface, limbus, <strong>and</strong> conjunctiva<br />
were processed using hematoxylin-eosin, Masson trichrome,<br />
Brown-Hopps, or von Kossa staining protocols.<br />
STATISTICAL ANALYSIS<br />
Body weights <strong>and</strong> glucose measurements were analyzed using<br />
the 2-tailed t test. The area <strong>of</strong> residual defect was analyzed each<br />
time using 1-way analysis <strong>of</strong> variance, with subsequent analysis<br />
by the Newman-Keuls test. The incidence <strong>of</strong> corneal lesions<br />
was analyzed using the 2 test.<br />
RESULTS<br />
INDUCTION OF DIABETES<br />
All rats weighed a mean (SE) <strong>of</strong> 174 (2) g at the time <strong>of</strong><br />
streptozotocin injections (Figure 1A). Control rats gained<br />
approximately 301 g during the 8 weeks. Rats in the diabetic<br />
group were comparable in body weight with control<br />
animals until 2 weeks after injection <strong>of</strong> streptozotocin.<br />
At this time, the diabetic group had a 15% reduction<br />
(P.001) in body weight relative to the control animals.<br />
Diabetic rats weighed significantly less (approximately<br />
25%-35%) than control rats beginning week 4 <strong>and</strong><br />
throughout the study.<br />
Mean (SE) baseline glucose readings were 139 (8)<br />
mg/dL for all rats, <strong>and</strong> these values were consistent in<br />
the control group throughout the study (Figure 1B). Rats<br />
receiving streptozotocin became hyperglycemic within<br />
5 days <strong>and</strong> had glucose levels greater than 450 mg/dL<br />
throughout the duration <strong>of</strong> experimentation.<br />
SLITLAMP OBSERVATIONS OF THE CORNEA<br />
Within 2 to 5 days after reepithelialization, 41% <strong>of</strong> the<br />
29 diabetic animals receiving the sterile vehicle exhibited<br />
corneas with exuberant granulation tissue <strong>and</strong> blood<br />
vessels extending from the limbus to the corneal lesion<br />
(Figure 2). No additional diabetic animals receiving the<br />
sterile vehicle exhibited corneal lesions after this period.<br />
However, those animals with corneal lesions <strong>of</strong>ten<br />
had changes in severity <strong>of</strong> this complication (Table).<br />
None <strong>of</strong> the animals in the control group receiving the<br />
sterile vehicle or in the diabetic group receiving either<br />
10 −4 or 10 −5 M <strong>of</strong> naltrexone presented with corneal lesions<br />
during the study. The incidence <strong>of</strong> corneal lesions<br />
in the diabetic rats receiving the sterile vehicle differed<br />
significantly (P.001) from those recorded for the control<br />
group receiving the sterile vehicle <strong>and</strong> diabetic group<br />
receiving naltrexone.<br />
HISTOLOGY<br />
2 mm<br />
Table. Severity <strong>of</strong> Corneal Lesions With <strong>Neovascularization</strong><br />
in Diabetic Rats Given a Sterile Vehicle<br />
Corneal Lesion<br />
Severitya No. <strong>of</strong> Rats<br />
Week 1 Week 2 Week 3<br />
Grade 1 7 2 2<br />
Grade 2 5 4 4<br />
Grade 3 0 6 6<br />
a Corneal lesions were graded as 1, 2, <strong>and</strong> 3, depending on whether the<br />
lesion covered no more than 25%, 50%, or 75% <strong>of</strong> the corneal surface area,<br />
respectively.<br />
Examination <strong>of</strong> the corneas <strong>of</strong> rats in all groups revealed<br />
a complete epithelial layer by 2 to 3 days after debridement.<br />
However, within 4 to 7 days after mechanical abrasion,<br />
animals in the diabetic group receiving the sterile vehicle<br />
were identified with corneal lesions, segmented<br />
leukocytes in clefts in some areas <strong>of</strong> the stroma, <strong>and</strong> numerous<br />
spindle cell nuclei <strong>and</strong> melanin pigment. Edema<br />
in the stroma was observed in these animals. Rats in the<br />
diabetic group receiving the sterile vehicle that had corneal<br />
lesions exhibited capillaries containing red blood cells<br />
in the stroma, particularly at the margins <strong>of</strong> the cornea.<br />
Moreover, in some <strong>of</strong> these specimens, the epithelial layer<br />
appeared to be detached from the corneal surface.<br />
Histological examination <strong>of</strong> sections <strong>of</strong> corneas collected<br />
3 weeks after debridement from diabetic rats receiving<br />
the sterile vehicle were characterized by cellular<br />
<strong>and</strong> vascular indications <strong>of</strong> inflammation <strong>and</strong> edema<br />
(Figure 3). Focal necrosis <strong>and</strong> loss <strong>of</strong> surface epithelium<br />
with segmented leukocytes <strong>and</strong> macrophages were<br />
visible within the subjacent stroma. The inflammatory<br />
cells <strong>and</strong> capillary proliferation disrupted the normally<br />
transparent lamellar pattern <strong>of</strong> collagen within the stroma<br />
(Figure 3F). There was focal degeneration <strong>and</strong> mineralization<br />
<strong>of</strong> the subepithelial basement membrane that was<br />
confirmed positive for calcium with the von Kossa stain<br />
(data not shown). Examination <strong>of</strong> sections stained with<br />
the Brown-Hopps tissue gram stain revealed an absence<br />
(REPRINTED) ARCH OPHTHALMOL / VOL 126 (NO. 4), APR 2008 WWW.ARCHOPHTHALMOL.COM<br />
503<br />
©2008 American Medical Association. All rights reserved.<br />
Downloaded From: http://173.193.11.201/ on 04/04/2013
Ep<br />
St<br />
En<br />
A B<br />
50 µm<br />
C D<br />
E F<br />
Ep<br />
BV<br />
Figure 3. Photomicrographs <strong>of</strong> sections <strong>of</strong> the central cornea taken 21 days<br />
after wounding from rats in the control group receiving a sterile vehicle<br />
(A <strong>and</strong> B), in the diabetic group receiving naltrexone (C <strong>and</strong> D), <strong>and</strong> in the<br />
diabetic group receiving a sterile vehicle that had corneal lesions (E <strong>and</strong> F).<br />
Sections were stained with hematoxylin-eosin (A, C, <strong>and</strong> E) or Masson<br />
trichrome (B, D, <strong>and</strong> F). Note the detached epithelium (Ep), calcified<br />
basement membrane (*), loss <strong>of</strong> lamella, <strong>and</strong> granulation tissue with the<br />
inclusion <strong>of</strong> small caliber blood vessels (BV) in the diabetic animals given a<br />
sterile vehicle (E <strong>and</strong> F). En indicates endothelium; St, stroma.<br />
<strong>of</strong> bacteria associated with the corneal lesions. Animals<br />
in the control group receiving the sterile vehicle, as well<br />
as rats in the diabetic group receiving naltrexone at concentrations<br />
<strong>of</strong> 10 −4 <strong>and</strong> 10 −5 M, did not exhibit any histological<br />
abnormalities.<br />
CORNEAL REEPITHELIALIZATION<br />
The 5-mm trephine demarcated the entire corneal region<br />
<strong>of</strong> the rat eye but did not encroach on the limbus<br />
or conjunctiva (Figure 4A). Wound healing occurred<br />
in a manner consistent with previous studies in healthy<br />
rats, rabbits, <strong>and</strong> humans as well as in diabetic rats. 9,13,14<br />
The initial area <strong>of</strong> the abrasion ranged from 19.3 mm 2 to<br />
25.6 mm 2 <strong>and</strong> corresponded to corneal injuries <strong>of</strong> 4.9 to<br />
5.7 mm in diameter. No differences in the size <strong>of</strong> the initial<br />
abrasions were noted between groups.<br />
Diabetic animals (with or without corneal lesions) receiving<br />
the sterile vehicle had corneal epithelial defect<br />
measurements that indicated a significant retardation from<br />
the control group receiving the sterile vehicle at 32<br />
(P.05) <strong>and</strong> 40 (P.001) hours <strong>and</strong> from the diabetic<br />
groups given 10 −4 Mor10 −5 M naltrexone treatment at<br />
A<br />
Mean Epithelial Defect, %<br />
16 h<br />
24 h<br />
32 h<br />
40 h<br />
B<br />
100<br />
75<br />
50<br />
25<br />
0<br />
DB SV (CL)<br />
∗<br />
†<br />
∗<br />
Initial Wound<br />
DB SV (No CL) DB NTX Control SV<br />
16 (P.05), 24 (P.001), 32 (P.01), <strong>and</strong> 40 (P.001)<br />
hours (data not shown). The diabetic animals receiving<br />
the sterile vehicle that had corneal lesions had greater<br />
epithelial defects than diabetic rats receiving the sterile<br />
vehicle without corneal lesions at 16 <strong>and</strong> 40 hours<br />
(Figure 4). Diabetic animals receiving naltrexone at concentrations<br />
<strong>of</strong> either 10 −4 Mor10 −5 M did not differ from<br />
each other in corneal reepithelialization at any time (data<br />
were collapsed for comparison). However, the diabetic<br />
‡<br />
§<br />
II<br />
0 16 24 32 40<br />
Time, h<br />
<br />
DB SV (CL)<br />
DB SV (No CL)<br />
DB NTX<br />
Control SV<br />
‡<br />
‡ ‡<br />
# #<br />
Figure 4. A, Representative photographs <strong>of</strong> rat eyes stained with fluorescein<br />
immediately (0 hours) <strong>and</strong> at 16, 24, 32, or 40 hours following a 5-mm<br />
corneal abrasion. Diabetic (DB) animals were topically treated with a sterile<br />
vehicle (SV) <strong>and</strong> the photographs are subdivided into animals that exhibited<br />
corneal lesions (CL) <strong>and</strong> those that did not (No CL) as well as DB corneas<br />
treated topically with 10 −4 M <strong>of</strong> naltrexone (NTX). Photographs <strong>of</strong> corneas<br />
from control rats receiving an SV are included. Corneal abrasions were<br />
created 9 weeks after injection <strong>of</strong> streptozotocin. Original magnification<br />
1.5. B, Residual epithelial defects after formation <strong>of</strong> a 5-mm mechanical<br />
abrasion. Significantly different from the DB SV (CL) group at P.05 (*),<br />
P.01 (†), or P.001 (‡). Significantly different from the DB SV (No CL)<br />
group at P.05 (), P.01 (§), or P.001 (#). Significantly different from<br />
control SV group at P.001 ( ). Error bars indicate st<strong>and</strong>ard error <strong>of</strong> the<br />
mean.<br />
(REPRINTED) ARCH OPHTHALMOL / VOL 126 (NO. 4), APR 2008 WWW.ARCHOPHTHALMOL.COM<br />
504<br />
©2008 American Medical Association. All rights reserved.<br />
Downloaded From: http://173.193.11.201/ on 04/04/2013
animals receiving naltrexone had smaller defects than control<br />
animals receiving the sterile vehicle at 24 hours but<br />
were comparable at 16, 32, <strong>and</strong> 40 hours.<br />
BLOOD GLUCOSE LEVELS<br />
In the diabetic group receiving the sterile vehicle, blood<br />
glucose levels in animals exhibiting corneal lesions did<br />
not differ from glucose levels in rats without corneal lesions<br />
at 1, 4, <strong>and</strong> 8 weeks. Specifically, mean (SE) blood<br />
glucose levels were 564 (18) mg/dL for 12 diabetic rats<br />
receiving the sterile vehicle that exhibited corneal lesions<br />
<strong>and</strong> 524 (19) mg/dL for 17 diabetic rats receiving<br />
the sterile vehicle that had no corneal lesions.<br />
COMMENT<br />
Our study reveals that more than 40% <strong>of</strong> rats with poorly<br />
controlled diabetes <strong>and</strong> corneal abrasions exhibit exuberant<br />
granulation tissue formation with neovascularization<br />
as determined by slitlamp microscopy <strong>and</strong> confirmed<br />
with histopathology. This abnormality following<br />
reepithelialization <strong>of</strong> the cornea, with indications at the<br />
histological level, was recorded as early as 2 days after<br />
debridement. These complications involved inflammation,<br />
edema, mineralization, <strong>and</strong> neovascularization but<br />
did not appear to include an infectious process.<br />
Our data show that these complications following corneal<br />
epithelial repair can be completely prevented by topical<br />
treatment with either 10 −4 or 10 −5 M <strong>of</strong> naltrexone.<br />
Interestingly, diabetic animals with corneal lesions were<br />
found to be correlated with significantly slower rates <strong>of</strong><br />
reepithelialization than those detected in diabetic rats<br />
without corneal lesions. These results would suggest that<br />
the appearance <strong>of</strong> granulation tissue with neovascularization<br />
may be related to an increased susceptibility for<br />
damage in these diabetic corneas brought on by delays<br />
in repair <strong>of</strong> injury. In this regard, it is well known that<br />
there is an irregular thickening <strong>and</strong> multilamination <strong>of</strong><br />
the epithelial basement membrane in diabetic humans<br />
<strong>and</strong> animals. 13,15 It may be conjectured that the subset <strong>of</strong><br />
diabetic animals displaying more exaggerated delays in<br />
reepithelialization than others have a problem with the<br />
integrity <strong>of</strong> the basement membrane. However, we did<br />
find that the blood glucose levels in both groups were<br />
similar; so it can be concluded that the magnitude <strong>of</strong> hyperglycemia<br />
was not an issue in this regard. Presumably,<br />
the exuberant granulation tissue disrupts the repaired<br />
corneal epithelium as the excessive granulation<br />
tissue protrudes above the level <strong>of</strong> the surrounding epithelium.<br />
Given the edema in the stroma <strong>and</strong> the appearance<br />
<strong>of</strong> new blood vessels from the limbus, our observations<br />
support the hypothesis <strong>of</strong> Cogan, 5 that stromal<br />
edema occurring near the limbus may be necessary to allow<br />
blood vessels into the corneal stroma. Thus, for the<br />
first time, we have defined a model for a pathologic response<br />
to complications in reepithelialization that involve<br />
exuberant granulation tissue formation <strong>and</strong> neovascularization.<br />
Moreover, we have demonstrated a<br />
treatment modality using naltrexone that aborts this<br />
process.<br />
The mechanism(s) concerning naltrexone’s capacity<br />
to attenuate neovascularization in the repair <strong>of</strong> the abraded<br />
cornea <strong>of</strong> diabetic rats is unclear. One possibility is that<br />
naltrexone directly diminishes the proliferation <strong>of</strong> these<br />
blood vessels. However, it is known that 5 µg <strong>of</strong> naltrexone<br />
placed on a methylcellulose disc stimulates angiogenesis<br />
(blood vessel number <strong>and</strong> length) compared with<br />
controls given vehicles in a chick chorioallantoic membrane<br />
preparation. 16,17 Moreover, naltrexone at a dosage<br />
that induced a continuous opioid receptor blockade (ie,<br />
30 mg/kg daily) has been reported to elevate DNA synthesis<br />
in the intima <strong>and</strong> media <strong>and</strong> to increase intimal<br />
thickness <strong>and</strong> reduce luminal area in the carotid artery<br />
that was denuded with balloon catheterization in comparison<br />
with vehicle-exposed control rats. 18 These data<br />
are consistent with findings that sustained opioid receptor<br />
blockade with naltrexone or other opioid antagonists<br />
results in enhanced DNA synthesis in tissues undergoing<br />
development, cellular renewal, or repair as well<br />
as in neoplasia. 19 Thus, the evidence does not appear to<br />
support the hypothesis that naltrexone has a direct inhibitory<br />
effect on neovascularization. Another possible<br />
mechanism regarding naltrexone treatment <strong>and</strong> diminished<br />
neovascularization is based on the observation that<br />
the cornea <strong>of</strong> the diabetic rats receiving the sterile vehicle<br />
heals slower than that in the control group receiving<br />
the sterile vehicle. 6,7 In the current study, when the<br />
diabetic group receiving the sterile vehicle is subdivided<br />
into those with <strong>and</strong> without corneal lesions, those<br />
with corneal lesions exhibited even more retarded reepithelialization<br />
than those without corneal lesions. This finding<br />
suggests that the pace <strong>of</strong> repair <strong>of</strong> corneal defects is<br />
more highly associated with the appearance <strong>of</strong> neovascularization,<br />
with a greater risk <strong>of</strong> neovascularization in<br />
animals with the slowest rates <strong>of</strong> reepithelization. This<br />
hypothesis is consonant with the observation that diabetic<br />
animals exposed to topical naltrexone have an accelerated<br />
rate <strong>of</strong> corneal wound healing comparable with<br />
that <strong>of</strong> the control animals receiving sterile vehicles, <strong>and</strong><br />
these diabetic rats receiving naltrexone did not display<br />
neovascularization. Thus, it could be conjectured that the<br />
mechanisms for the promotion <strong>of</strong> neovascularization in<br />
the cornea <strong>of</strong> diabetic animals may be factors <strong>and</strong> events<br />
occurring in the extended period <strong>of</strong> reepithelialization.<br />
If this is the case, then a test <strong>of</strong> this hypothesis would be<br />
an examination <strong>of</strong> the repercussions <strong>of</strong> a drug- or mechanical-induced<br />
retardation in corneal repair in diabetic<br />
rats, which would be predicted to increase the incidence<br />
<strong>of</strong> neovascularization. Finally, it is known that<br />
naltrexone treatment restores corneal sensitivity in diabetic<br />
rats. 7 In this manner, it may optimize the homeostatic<br />
milieu <strong>and</strong> thereby facilitate healing by reestablishing<br />
the blink reflex <strong>and</strong> tear production.<br />
The complications following corneal reepithelialization<br />
in rats we documented has not been reported in humans.<br />
One factor that may contribute to the development<br />
<strong>of</strong> the corneal lesions we observed is the severity in degree<br />
<strong>and</strong> duration <strong>of</strong> hyperglycemia (blood glucose levels in these<br />
rats were routinely 450 mg/dL for 8 weeks). Moreover,<br />
humans have a Bowman membrane that is absent in<br />
rats. If a corneal abrasion in a rat can be equated to a superficial<br />
corneal ulcer in humans, the lack <strong>of</strong> this ana-<br />
(REPRINTED) ARCH OPHTHALMOL / VOL 126 (NO. 4), APR 2008 WWW.ARCHOPHTHALMOL.COM<br />
505<br />
©2008 American Medical Association. All rights reserved.<br />
Downloaded From: http://173.193.11.201/ on 04/04/2013
tomic barrier (ie, the Bowman membrane) in the rat could<br />
make their corneas more susceptible to inflammatory mediators<br />
accompanying reepithelialization. Further contributing<br />
to the complications following corneal epithelial repair<br />
in these poorly controlled diabetic animals may be the<br />
presence <strong>of</strong> decreased corneal sensitivity that we have previously<br />
reported, which can be remedied by topical treatment<br />
with naltrexone. 14 Decreased corneal sensitivity would<br />
be expected to decrease tear production <strong>and</strong>/or blink reflex,<br />
thereby subjecting the newly repaired cornea to an adverse<br />
environment.<br />
The healthy human cornea is free from blood vessels,<br />
but neovascularization is a common clinical problem<br />
seen as a response to chronic hypoxia or various inflammatory<br />
stimuli, such as bacterial keratitis, alkali burns,<br />
<strong>and</strong> graft rejection. 1-3 The severity <strong>of</strong> clinical disorders<br />
involving corneal neovascularization, which, untreated,<br />
may lead to pronounced visual impairment, emphasizes<br />
the importance <strong>of</strong> broadening our base <strong>of</strong> knowledge<br />
in this field. That the model we describe is occurring<br />
on the ocular surface makes these lesions very accessible<br />
for defining related structural, biochemical, <strong>and</strong><br />
physiological events, particularly neovascularization. Additionally,<br />
such a model provides the unique opportunity<br />
to delineate the effect <strong>of</strong> various treatment regimens.<br />
Therefore, for the first time, we have characterized<br />
a unique model <strong>of</strong> exuberant granulation tissue with neovascularization<br />
that accompanies complications <strong>of</strong> corneal<br />
reepithelialization that can be tested for toxicity <strong>and</strong><br />
efficacy <strong>of</strong> therapeutic modalities.<br />
Submitted for Publication: May 22, 2007; final revision<br />
received July 17, 2007; accepted July 18, 2007.<br />
Correspondence: Ian S. Zagon, MS, PhD, Department <strong>of</strong><br />
Neural <strong>and</strong> Behavioral Sciences, Mail Code H109, The<br />
M. S. Hershey Medical Center, 500 University Dr, Room<br />
C3729, Hershey, PA 17033 (isz1@psu.edu).<br />
Financial Disclosure: None reported.<br />
Funding/Support: This study was supported in part by<br />
grants EY16666 <strong>and</strong> K12 EY015398 from the National<br />
Institutes <strong>of</strong> Health.<br />
From the Archives <strong>of</strong> the Archives<br />
Now World War II has thrust on the United States leadership<br />
in ophthalmology, as in all other branches <strong>of</strong> medicine.<br />
At present this is a stimulus to the progress <strong>of</strong> ophthalmology<br />
here. It is to be hoped that, in spite <strong>of</strong> political<br />
obstacles which many <strong>of</strong> us fear we foresee in the near<br />
future, this accelerated progress will continue without<br />
interruption.<br />
Reference: Verhoeff FH. American ophthalmology<br />
during the past century. Arch Ophthalmol. 1948;39:464.<br />
REFERENCES<br />
1. Lee P, Wang CC, Adamis AP. Ocular neovascularization: an epidemiological review.<br />
Surv Ophthalmol. 1998;43(3):245-269.<br />
2. Chang JH, Gabison EE, Kato T, Azar DT. Corneal neovascularization. Opin<br />
Ophthalmol. 2001;12(4):242-249.<br />
3. Carmichael TR. Corneal angiogenesis. In: Tombran-Tink J, Barnstable CJ, eds.<br />
Ocular Angiogenesis. Totowa, NJ: Humana Press; 2006:45-71.<br />
4. Dana MR, Streilein JW. Loss <strong>and</strong> restoration <strong>of</strong> immune privilege in eyes with<br />
corneal neovascularization. Invest Ophthalmol Vis Sci. 1996;37(12):2485-2494.<br />
5. Cogan DG. Vascularization <strong>of</strong> the cornea: its experimental induction by small lesions<br />
<strong>and</strong> a new theory <strong>of</strong> its pathogenesis. Arch Ophthalmol. 1949;41:406-416.<br />
6. Zagon IS, Jenkins JB, Sassani JW, et al. Naltrexone, an opioid antagonist, facilitates<br />
reepithelialization <strong>of</strong> the cornea in diabetic rat. Diabetes. 2002;51(10):<br />
3055-3062.<br />
7. Klocek MS, Sassani JW, McLaughlin PJ, Zagon IS. Topically applied naltrexone<br />
restores corneal reepithelialization in diabetic rats. J Ocul Pharmacol Ther. 2007;<br />
23(2):89-102.<br />
8. Zagon IS, Sassani JW, McLaughlin PJ. Re-epithelialization <strong>of</strong> the rat cornea is accelerated<br />
by blockade <strong>of</strong> opioid receptors. Brain Res. 1998;798(1-2):254-260.<br />
9. Zagon IS, Sassani JW, McLaughlin PJ. Re-epithelialization <strong>of</strong> the human cornea<br />
is regulated by endogenous opioids. Invest Ophthalmol Vis Sci. 2000;41(1):<br />
73-81.<br />
10. Havel PJ, Hahn TM, Sindelar DK, et al. Effects <strong>of</strong> streptozotocin-induced diabetes<br />
<strong>and</strong> insulin treatment on the hypothalamic melanocortin system <strong>and</strong> muscle<br />
uncoupling protein 3 expression in rats. Diabetes. 2000;49(2):244-252.<br />
11. Ahrén B, Stern JS, Gingerich RL, Curry DL, Havel PJ. Glucagon secretory responses<br />
to hypoglycemia, adrenaline, <strong>and</strong> carbachol in streptozotocin diabetic<br />
rats. Acta Physiol Sc<strong>and</strong>. 1995;155(2):215-221.<br />
12. Nakamura M, Sato N, Chikama T-I, Hasegawa Y, Nishida T. Fibronectin facilitates<br />
corneal epithelial wound healing in diabetic rats. Exp Eye Res. 1997;64<br />
(3):355-359.<br />
13. Rehany U, Ishii Y, Lahav M, Rumelt S. Ultrastructural changes in corneas <strong>of</strong> diabetic<br />
patients. Cornea. 2000;19(4):534-538.<br />
14. Zagon IS, Klocek MS, Sassani JW, Mauger DT, McLaughlin PJ. Corneal safety<br />
<strong>of</strong> topically applied naltrexone. J Ocul Pharmacol Ther. 2006;22(5):377-387.<br />
15. Taylor HR, Kimsey RA. Corneal epithelial basement membrane changes in diabetes.<br />
Invest Ophthalmol Vis Sci. 1981;20(4):548-553.<br />
16. Blebea J, Mazo JE, Kihara TK, et al. Opioid growth factor modulates angiogenesis.<br />
J Vasc Surg. 2000;32(2):364-373.<br />
17. Blebea J, Vu J-H, Assadnia S, McLaughlin PJ, Atnip RG, Zagon IS. Differential<br />
effects <strong>of</strong> vascular growth factors on arterial <strong>and</strong> venous angiogenesis. J Vasc<br />
Surg. 2002;35(3):532-538.<br />
18. Zagon IS, Essis FM, Verderame MF, Healy DA, Atnip RG, McLaughlin PJ. Opioid<br />
growth factor inhibits intimal hyperplasia in balloon-injured rat carotid artery.<br />
J Vasc Surg. 2003;37(3):636-643.<br />
19. Zagon IS, Verderame MF, McLaughlin PJ. The biology <strong>of</strong> the opioid growth factor<br />
receptor (OGFr). Brain Res Res. 2002;38(3):351-376.<br />
(REPRINTED) ARCH OPHTHALMOL / VOL 126 (NO. 4), APR 2008 WWW.ARCHOPHTHALMOL.COM<br />
506<br />
©2008 American Medical Association. All rights reserved.<br />
Downloaded From: http://173.193.11.201/ on 04/04/2013