Ankle Arthrodesis Using Ring External Fixation - Orthofix.com
Ankle Arthrodesis Using Ring External Fixation - Orthofix.com
Ankle Arthrodesis Using Ring External Fixation - Orthofix.com

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
FIGURE 3. <strong>External</strong> fixation alone does not create<br />
fusion; proper joint preparation is necessary.<br />
count with differential and blood cultures. Consideration<br />
may be given to a MRI or a <strong>com</strong>bination technetium bone<br />
scan/indium-labeled white blood cells scan to confirm/<br />
evaluate the extent of infection, keeping in mind that<br />
peripheral vascular disease and antibiotics will interfere<br />
with the effectiveness of these studies. To obtain useful<br />
intraoperative cultures, antibiotics should be stopped at<br />
least 3 days before surgery. Planning should include the<br />
potential for a staged procedure. Irrigation and debridement,<br />
hardware removal, and possible antibiotic bead<br />
placement should be planned as the first stage. If the ankle<br />
is determined to be unstable at that time, the external<br />
fixator should be placed for support. In a second stage, the<br />
antibiotic beads can be removed, the ankle again debrided,<br />
and <strong>com</strong>pression may be applied through the ankle if there<br />
is no evidence of persistent infection. Alternatively, the<br />
FIGURE 4. Ideal position for arthrodesis: neutral sagittal<br />
plane (plantigrade foot), slight hindfoot valgus, tibial shaft<br />
axis aligned with the second metatarsal, and no anterior<br />
talar translation within the ankle mortise. This is particularly<br />
important if a prebuilt frame is applied.<br />
152<br />
Special Focus: Easley et al<br />
plan can be for a single-stage procedure if the surgeon is<br />
satisfied that all of the infected tissue has been removed.<br />
| TECHNIQUE<br />
Techniques in Foot and <strong>Ankle</strong> Surgery<br />
A proximal regional anesthetic typically suffices for<br />
ankle arthrodesis using external fixation. Tourniquet use<br />
is generally limited to the approach for tibiotalar joint<br />
preparation. <strong>External</strong> fixation in itself cannot create a<br />
fusion; proper joint preparation is essential. Therefore,<br />
if there is any concern for the perfusion of either the<br />
tibial plafond or (more likely) the talar dome, then the<br />
tourniquet must be released before wound closure to confirm<br />
bleeding at the arthrodesis site. There is no need for<br />
tourniquet use during application of the external fixator.<br />
The patient is positioned supine, often with a support<br />
under the hip of the operated leg. The goal is to orient the<br />
lower leg directly perpendicular to the operating room<br />
table/floor to facilitate proper placement of the external<br />
fixator. A sterile proximal calf support (Bbump^) (Fig.2)<br />
should be created to suspend the lower leg during<br />
external fixator placement.<br />
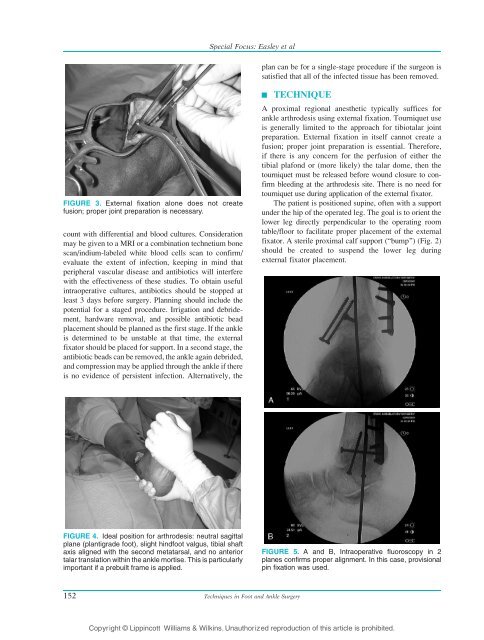
FIGURE 5. A and B, Intraoperative fluoroscopy in 2<br />
planes confirms proper alignment. In this case, provisional<br />
pin fixation was used.<br />
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.