

Gastrojejunostomy: a simple method of
Gastrojejunostomy: a simple method of
Gastrojejunostomy: a simple method of

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Annals <strong>of</strong> the Royal College <strong>of</strong> Surgeons <strong>of</strong> England (1986) vol. 68<br />
<strong>Gastrojejunostomy</strong>: a <strong>simple</strong> <strong>method</strong> <strong>of</strong><br />
treatment <strong>of</strong> gastric volvulus<br />
A G FARKAS NlB BS<br />
Senior House Officer<br />
L R CELESTIN FRCS<br />
Consultant Surgeon<br />
Department <strong>of</strong> General Surgery, Frenchay Hospital, Bristol<br />
Key words: GASTROE{INTEROSTOMY; STOMACH, VOlNVIULUS; SURGERY<br />
Summary<br />
Ten patients treated for gastric volvulus over eleven years are reviewed.<br />
Nine were treated successfully by gastrojejunostomy. The '1)<br />
advantages <strong>of</strong> this <strong>simple</strong> procedure are discussed. Changes occurring<br />
in the position <strong>of</strong> the pylorus may predispose to this condition.<br />
Introduction<br />
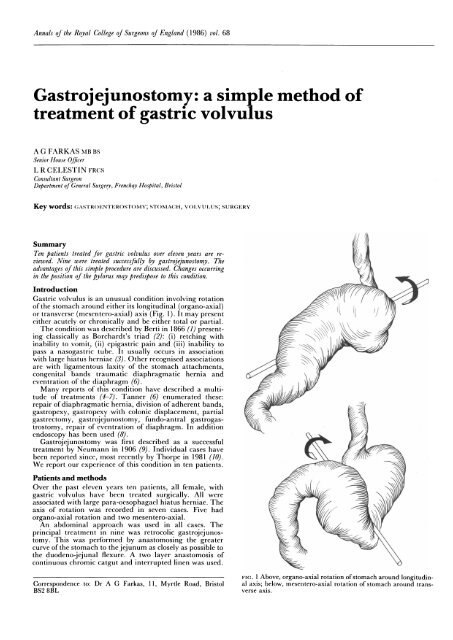
Gastric volvulus is an unusual condition involving rotation<br />
<strong>of</strong> the stomach around either its longitudinal (organo-axial)<br />
or transverse (mesentcro-axial) axis (Fig. 1). It may present<br />
cither acutely or chronically and be either total or partial.<br />
The condition was described by Berti in 1866 (1) present-<br />
to<br />
ing classically as Borchardt's triad (2): (i) retching with<br />
inability to vomit,Borchardtgstriad (2) (ii) etchinability to<br />
pass a nasogastric tube. It usually occurs in association<br />
with large hiatus herniae (3). Other recognised associations<br />
are with ligamentous laxity <strong>of</strong> the stomach attachments,<br />
congenital bands traumatic diaphragmatic hernia and<br />
eventration <strong>of</strong> the diaphragm (6).<br />
Many reports <strong>of</strong> this condition have described a multitude<br />
<strong>of</strong> treatments (4-7). Tanner (6) enumerated these:<br />
repair <strong>of</strong> diaphragmatic hernia, division <strong>of</strong> adherent bands,<br />
gastropexy, gastropexy with colonic displacement, partial<br />
gastrectomy, gastrojcjunostomy, fundo-antral gastrogastrostomy,<br />
repair <strong>of</strong> eventration <strong>of</strong> diaphragm. In addition<br />
endoscopy has been used (8).<br />
<strong>Gastrojejunostomy</strong> was first described as a successful A<br />
treatment by Neumann in 1906 (9). Individual cases have<br />
been reported since, most recently by Thorpe in 1981 (10).<br />
We report our experience <strong>of</strong> this condition in ten patients.<br />
Patients and <strong>method</strong>s<br />
Over the past eleven years ten patients, all female, with<br />
gastric volvulus have been treated surgically. All were<br />
associated with large para-oesophagael hiatus herniae. The<br />
axis <strong>of</strong> rotation was recorded in seven cases. Five had<br />
organo-axial rotation and two mesentero-axial.<br />
An abdominal approach was used in all cases. The<br />
principal treatment in nine was retrocolic gastrojejunostomy.<br />
This was performed by anastomosing the greater<br />
curve <strong>of</strong> the stomach to the jejunum as closely as possible to<br />
the duodeno-jejunal flexure. A two layer anastomosis <strong>of</strong><br />
continuous chromic catgut and interrupted linen was used.<br />
F IG. I Above, organo-axial rotation <strong>of</strong> stomach around longitudin-<br />
Correspondence to: Dr A G Farkas, 11, Myrtle Road, Bristol al axis; below, mesentero-axial rotation <strong>of</strong> stomach around trans-<br />
BS2 8BL verse axis.
108 A G Farkas and L R Celestin<br />
TABLE I. Details <strong>of</strong> the ten patients treated.<br />
Age<br />
Case Sex Presentation Treatment Outcome<br />
1 82F Pain and <strong>Gastrojejunostomy</strong> Symptoms relieved<br />
vomiting Repair <strong>of</strong> hiatus Alive<br />
2 68F Vomiting Total gastrectomy Died <strong>of</strong> anastomotic<br />
dehiscence<br />
3 82F Pain and <strong>Gastrojejunostomy</strong> Well until unrelated<br />
vomiting death 2 years<br />
4 69F Pain and <strong>Gastrojejunostomy</strong> Well until died <strong>of</strong><br />
vomiting Repair <strong>of</strong> hiatus carcinoma <strong>of</strong> stomach<br />
4 years<br />
5 81F Haematemesis <strong>Gastrojejunostomy</strong> Symptoms relieved<br />
Excision gastric Died <strong>of</strong> adhesive<br />
ulcer obstruction 2 months<br />
6 83F Pain and <strong>Gastrojejunostomy</strong> Well until unrelated<br />
vomiting death 3 months<br />
7 75F Pain <strong>Gastrojejunostomy</strong> Symptoms relieved<br />
Repair <strong>of</strong> hiatus Alive<br />
8 81F Haematemesis <strong>Gastrojejunostomy</strong> Symptoms relieved<br />
Repair <strong>of</strong> hiatus Alive<br />
9 58F Haematemesis <strong>Gastrojejunostomy</strong> Symptoms relieved<br />
Splenectomy Alive<br />
10 68F Dysphagia <strong>Gastrojejunostomy</strong> Symptoms relieved<br />
Repair oesophageal Alive<br />
tear<br />
The hiatus was repaired in four cases using interrupted<br />
nylon sutures.<br />
In case 2 difficult mobilization <strong>of</strong> the stomach resulted in<br />
gastric perforation necessitating thoraco-abdominal gastrectomy.<br />
In case 5 a bleeding gastric ulcer was excised. In<br />
case 9 splenectomy was carried out and in case 10 an<br />
oesophageal tear repaired following difficulties in mobilising<br />
the stomach.<br />
Results<br />
The ten cases are summarised in Table I. All nine patients<br />
treated by gastrojejunostomy had relief <strong>of</strong> symptoms following<br />
surgery and are either alive or have died from unrelated<br />
causes. The only perioperative mortality among all patients<br />
FIG. 2 Radiograph <strong>of</strong> organo-axial rotation.<br />
was in case 2 following total gastrectomy. Case 5 died<br />
following a laparotomy for adhesions two months after<br />
gastrojejunostomy and excision <strong>of</strong> gastric ulcer; case 6 died<br />
<strong>of</strong> unrelated causes 3 months after surgery.<br />
We have not encountered any recurrence <strong>of</strong> symptoms in<br />
this group <strong>of</strong> patients.<br />
Discussion<br />
The significance <strong>of</strong> the axis about which the stomach<br />
rotates has been discussed extensively (7, 11). The pylorus is<br />
normally situated to the right <strong>of</strong> the midline at the level <strong>of</strong><br />
the first lumbar intervertebral space. In volvulus the pylorus,<br />
as found at surgery, is in the midline at the level <strong>of</strong> the<br />
body <strong>of</strong> LI (Figs. 2 and 3). In para-oesophageal herniation<br />
FiG. 3 Diagram <strong>of</strong> radiograph in Fig. 2 showing movement <strong>of</strong><br />
greater curve A to A' and lesser curve B to B'. Pylorus P moves<br />
upwards and to the midline P'.
migration <strong>of</strong> the stomach into the chest is a factor leading to<br />
movement <strong>of</strong> the pylorus and duodenum across the midline.<br />
We suggest that though herniation is the aetiological factor,<br />
migration <strong>of</strong> the pylorus may predispose to volvulus, as it<br />
only occurs when the distance between cardia and pylorus<br />
is such as to allow abnormal mobility <strong>of</strong> the stomach.<br />
The aim <strong>of</strong> surgical correction is relief <strong>of</strong> symptoms and<br />
prevention <strong>of</strong> recurrence. The average age in our series was<br />
74: any procedure in this elderly population should be as<br />
<strong>simple</strong> as possible. The diaphragmatic hiatus was repaired<br />
in cases when it was readily accessible but was felt to be <strong>of</strong><br />
secondary importance and not to warrant more extensive<br />
surgery. Symptoms <strong>of</strong> reflux oesophagitis are rare, due to an<br />
increased oesophago-gastric angle (6). <strong>Gastrojejunostomy</strong><br />
at the fixed point <strong>of</strong> the duodeno-jejunal juction tethers the<br />
untwisted stomach in the abdomen and prevents recurrent<br />
volvulus. This procedure carries the further advantage <strong>of</strong><br />
preventing the not infrequent migration <strong>of</strong> the transverse<br />
colon into the chest anterior to the stomach. Fixation by<br />
anastomosis does not break down as may happen in <strong>simple</strong><br />
gastropexy (6).<br />
<strong>Gastrojejunostomy</strong> is a <strong>simple</strong> and effective treatment for<br />
gastric volvulus. Morbidity and mortality in this series has<br />
been associated with extensive gastric mobilization or the<br />
performance <strong>of</strong> surgical procedures in addition to gastrojejunostomy.<br />
We suggest that these should be avoided when<br />
possible.<br />
Notes on books<br />
Atlas <strong>of</strong> Human Anatomy by J A Gosling, P F Harris, J R<br />
Humpherson, I Whitmore and P L T Wilan. Illustrated.<br />
1985. Gower Medical Publishing Limited, London. £19.50.<br />
Originating from the Manchester University Department <strong>of</strong> Anatomy<br />
this folio volume comprises high quality colour photographs<br />
<strong>of</strong> cadaver dissections accompanied by a coloured line diagram <strong>of</strong><br />
the photograph fully labelled. A succinct text accompanies the<br />
illustrations.<br />
The photographs are <strong>of</strong> outstanding quality and there can be<br />
few students <strong>of</strong> anatomy who will fail to enjoy studying this<br />
vilume. It complements existing texts and should have a ready sale<br />
in view <strong>of</strong> the remarkably low price.<br />
Radiation Protection in Hospitals by Richard F Mould.<br />
201 pages, illustrated. 1985. Adam Hilger, Bristol. £19.50.<br />
Personnel in the Departments <strong>of</strong> Nuclear Medicine, Diagnostic<br />
Radiology and Radiotherapy ali need to know the principles and<br />
importance <strong>of</strong> radiation protection. This book tells all. It has<br />
evolved over many years <strong>of</strong> lecturing on the topic <strong>of</strong> radiation<br />
protection to a wide spectrum <strong>of</strong> hospital staff and is written in a<br />
most readable style. Numerous illustrations, including the judicious<br />
use <strong>of</strong> cartoons, enliven the pages.<br />
Head and Neck Cancer edited by Robert E Wittes. 350<br />
pages, illustrated. 1985. John Wiley, Chichester. £37.50.<br />
Selected areas <strong>of</strong> current interest in head and neck cancer comprise<br />
this volume. Epidemiology, staging, treatment and prevention,<br />
cells in culture and <strong>method</strong>ology are the headings <strong>of</strong> the five<br />
sections covered. Particularly emphasised is the increasing use <strong>of</strong><br />
combined modality treatment. Fully referenced and handsomely<br />
produced.<br />
Congenital Heart Surgery: Current Techniques and<br />
Controversies edited by Anthony L Moulton. 347 pages,<br />
illustrated. Butterworths, London. £95.00.<br />
Forty-two authors from 8 different countries describe their<br />
approaches to 7 different congenital heart defects. With more than<br />
500 illustrations and many tables the different surgical approaches<br />
are detailed together with extinwive references to the literature.<br />
A <strong>simple</strong> <strong>method</strong> <strong>of</strong> treatment <strong>of</strong> gastric volvulus 109<br />
References<br />
I Berti A. Singalore attortigliamento dele'es<strong>of</strong>ago col duodeno<br />
seguita rapida morte. Gazz Med Ital Prov Veneti 1866;9:139.<br />
2 Borchardt M. Zun Pathalogie and Therapie des Magenvolvulus.<br />
Arch Klin Chir 1904;74:243.<br />
3 Vernhet J, Carabalona JP, Carabalona P. Les volvulus intrathoraciques<br />
de l'estomac au cours des hernies hiatales.<br />
Chirurgie 1980; 106:756-4.<br />
4 Dalgard BJ. Volvulus <strong>of</strong> the stomach. Acta Chir Scanda<br />
1952; 103:131-53.<br />
5 Buchanan J. Volvulus <strong>of</strong> the stomach. Br J Surg 1932;18:99-<br />
112.<br />
6 Tanner NC. Chronic and recurrent volvulus <strong>of</strong> the stomach.<br />
Am J Surg 1968; 115:505-15.<br />
7 Wastell C, Ellis H. Volvulus <strong>of</strong> the stomach. Br J Surg<br />
1971 ;58:557-62.<br />
8 Patel NM. Endoscopic correction chronic gastric volvulus.<br />
Gastrointest Endosc 1983;29:63.<br />
9 Neumann. Uber den Volvulus des Magens. Dtsch Z Chir<br />
1906;85: 136-50.<br />
10 Thorpe JAC. Chronic gastric volvulus-aetiology and treatment.<br />
BrJ Clin Pract 1981;35:161-2.<br />
11 Carter R, Brewer LA, Hinshaw DB. Acute gastric volvulus.<br />
AmJ Surg 1980;140:99-106.<br />
12 Askew AR. Treatment <strong>of</strong> acute and chronic gastric volvulus.<br />
Ann R Coll Surg Eng 1978;60:326-8.<br />
Manual on the AO/ASIF Tubular External Fixator by<br />
G Hierholzer, Th Ruedi, M Allgower and J Schatzker. 100<br />
pages, illustrated. Springer-Verlag, Berlin. DM 86.<br />
This is a specialized book for orthopaedic surgeons. It outlines the<br />
principal features <strong>of</strong> the tubular system <strong>of</strong> external fixation which<br />
was developed by the Working Group for Osteosynthesis <strong>of</strong> the<br />
AO/ASIF. It is copiously illustrated and handsomely produced on<br />
high quality paper.<br />
Surgical Endoscopy edited by Thomas L Dent, William E<br />
Strodel, Jeremiah G Turcotte and Mary L. Harper. 536<br />
pages, illustrated. 1985. Year Book Medical Publishers,<br />
Chicago. £57.<br />
Diagnostic and therapeutic endoscopy <strong>of</strong> the gastrointestinal tract<br />
and biliary tree, together with bronchoscopy, arthroscopy, cystoscopy<br />
and laparoscopy are covered in this concentrated text. Thirty<br />
three chapters comprise essays presented at a postgraduate symposium<br />
held in May 1985 in Michigan. Topical, readable and<br />
recommended.<br />
Surgical Care II by Robert E Condon and Jerome De<br />
Cosse. 431 pages, illustrated. 1985. Lea and Febiger, Philadelphia.<br />
$71.<br />
Applied surgical physiology is emphasised throughout this wideranging<br />
volume which covers such diverse subjects as gastrointestinal<br />
motility, massive intestinal resection, cerebrovascular disorders,<br />
the pathology <strong>of</strong> sepsis and wound healing. The volume is<br />
intended as a reference text for students as well as the practising<br />
surgeon. Each <strong>of</strong> the twenty one chapters is well referenced and<br />
the book is attractively produced on art paper.<br />
1985 Year Book <strong>of</strong> Plastic and Reconstructive Surgery<br />
edited by FrederickJ McCoy. 320 pages, illustrated. 1985.<br />
Year Book Medical Publishers, Chicago. £49.50.<br />
This is the sixteenth annual volume <strong>of</strong> a well-known series. It<br />
abstracts important articles published during the last few months<br />
and adds substantive editorial comments. Required reading for all<br />
plastic surgeons.














