

A study of the pathology and pathogenesis of bronchiectasis.
A study of the pathology and pathogenesis of bronchiectasis.
A study of the pathology and pathogenesis of bronchiectasis.

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
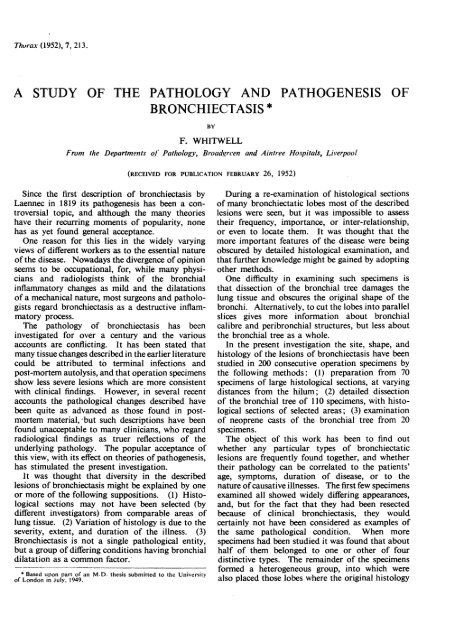
PATHOLOGY AND PATHOGENESIS OF BRONCHIECTASIS221cylindrical <strong>bronchiectasis</strong> <strong>of</strong><strong>the</strong> left lower lobe <strong>and</strong>lingula, with minimalchanges in <strong>the</strong> right middlelobe. Left lower lobectomywith removal <strong>of</strong> <strong>the</strong> lingulawas performed.Macroscopic Appearance<strong>of</strong> Specimen.-The lingula issmall <strong>and</strong> firm, <strong>and</strong> has a Jshiny, thin pleural covering.Sections show <strong>the</strong> bronchi eto be dilated, thickened,filled with pus, <strong>and</strong> surroundedby interstitial pneumonia.The microscopicappearance is similar to that<strong>of</strong> <strong>the</strong> posterior basal segment(q .v.). > v,t'-The lower lobe appearswell aerated, though <strong>the</strong>basal segments contain some .jfirm areas. The pleuralmembrane is normal: <strong>the</strong>reare enlarged hilar lymph 4-gl<strong>and</strong>s.Sections <strong>of</strong> <strong>the</strong> lobe (Fig.17) show more extensive"disease than in Case 464.There is marked thickening<strong>and</strong> dilatation <strong>of</strong> all branches<strong>of</strong> <strong>the</strong> posterior basal bronchus,<strong>and</strong> extensive pneumoniain this segment.Changes in <strong>the</strong> middle <strong>and</strong> 4santerior basal segments are<strong>of</strong> lesser severity, <strong>and</strong> are FIG. 17-Moderate follicularcomparable wi.dh those seenin <strong>the</strong> posterior basal segment <strong>of</strong> <strong>the</strong> previous case.No abnormality is to be seen in <strong>the</strong> more pigmentedapical segment.Microscopic Features.-The appearance <strong>of</strong> lesionsin <strong>the</strong> middle <strong>and</strong> anterior basal segments is similar tothat <strong>of</strong> <strong>the</strong> previous case.In <strong>the</strong> posterior basal bronchus <strong>the</strong>re is diffuse infiltration<strong>of</strong> chronic inflammatory cells in <strong>the</strong> sub-epi<strong>the</strong>lialtissues The ducts <strong>of</strong> mucous gl<strong>and</strong>s are funnelshapedinstead <strong>of</strong> being tubular, <strong>and</strong> lymph folliclessurround <strong>the</strong>ir mouths. Bronchial supporting structuresare normal except for loss <strong>of</strong> elastic tissue near <strong>the</strong>follicles.The branches <strong>of</strong> <strong>the</strong> posterior basal bronchus aredilated, thickened, <strong>and</strong> filled with pus.The epi<strong>the</strong>lium consists <strong>of</strong> ciliated columnar cells,with no areas <strong>of</strong> ulceration or squamous metaplasia.Inflammatory cells are pr<strong>of</strong>use in <strong>the</strong> oedematous walls;lymph follicles are numerous <strong>and</strong> <strong>of</strong>ten confluent.There is a more complete loss <strong>of</strong> bronchial supportingtissues than in <strong>the</strong> previous case, only isolated fragmentsremaining.p<strong>bronchiectasis</strong> <strong>of</strong> left lower lobe (Case 758). Iron haematoxylin <strong>and</strong>van Gieson.All bronchioles in <strong>the</strong> segment are diseased, most <strong>of</strong><strong>the</strong>m being partly occluded, while some appear almostobliterated. Epi<strong>the</strong>lial changes follow those in <strong>the</strong> previousspecimen, but <strong>the</strong> inflammatory reaction is moreextensive, lymph follicles are more numerous, <strong>and</strong> <strong>the</strong>reis almost total loss <strong>of</strong> muscle <strong>and</strong> elastic tissue.In some fields <strong>the</strong> zones <strong>of</strong> interstitial pneumoniaare so wide that <strong>the</strong>y form a confluent mass. As <strong>the</strong>reis little thickening <strong>of</strong> interlobular septa, <strong>the</strong> originallobular pattern is obliterated. No alveolar collapse ispresent.SEVERE FOLLICULAR BRONCHIECTASISCASE 497.-A 9-year-old girl, who had suffered froma productive cough since measles in early childhood,was admitted with an acute exacerbation <strong>of</strong> symptoms.She was dyspnoeic on slight exertion, showed fingerclubbing, <strong>and</strong> bronchograms revealed <strong>bronchiectasis</strong> <strong>of</strong><strong>the</strong> left lower lobe <strong>and</strong> lingula. Left lower lobectomywith excision <strong>of</strong> <strong>the</strong> lingula was performed.Microscopic Appearance <strong>of</strong> Specimen.-The lingulais small <strong>and</strong> firm, <strong>and</strong> shows gross <strong>bronchiectasis</strong> with
222F. WHITWELLt!.^FIG. 18-Severe follicular <strong>bronchiectasis</strong> <strong>of</strong> right lower lobe 2 cm. frcHaematoxylin <strong>and</strong> eosin.interstitial pneumonia <strong>and</strong> collapse. The microscopicfeatures do not differ from those at <strong>the</strong> base <strong>of</strong> <strong>the</strong>lower lobe.The lower lobe is quite bulky <strong>and</strong> firm, <strong>and</strong> hasenlarged hilar lymph gl<strong>and</strong>s. The pleural membrane isthickened over <strong>the</strong> base <strong>of</strong> <strong>the</strong> lob,, but normal at <strong>the</strong>apex, which is partly aerated.On section (Figs. 18 <strong>and</strong> 19) <strong>the</strong>re is mild <strong>bronchiectasis</strong>with some pneumonia in <strong>the</strong> partially aerated apicalsegment, while <strong>the</strong> basal segments all show gross <strong>bronchiectasis</strong>with pneumonia, collapse, <strong>and</strong> some fibrosis.It is mainly in <strong>the</strong> segmental bronchi <strong>and</strong> <strong>the</strong>ir first <strong>and</strong>second branchings that dilatation is seen: more peripheralbronchi look like narrow clefts in solid tissue.The disease is most severe in <strong>the</strong> lower parts <strong>of</strong> <strong>the</strong> basalsegments.Microscopic Features.-Though <strong>the</strong> gross appearanceis far removed from that <strong>of</strong> <strong>the</strong> previous two specimens<strong>the</strong>re are no qualitative differences in <strong>the</strong> histology.Changes in <strong>the</strong> apical segment are similar to thosedescribed in mild lesions <strong>of</strong> <strong>the</strong> previous cases. Thelesions in each basal segment are<strong>of</strong> equal severity.There is some dilatation but littlethickening <strong>of</strong> <strong>the</strong> basal segmentalbronchi, <strong>and</strong> while epi<strong>the</strong>lial liningsare normal, <strong>the</strong>re is diffuse inflammatoryinfiltration <strong>of</strong> sub-epi<strong>the</strong>lialtissues with some lymph follicleW. formation. Elastic tissue is extensivelydestroyed, but <strong>the</strong> loss <strong>of</strong>muscle is only slight <strong>and</strong> cartilagesare normal. Mucous gl<strong>and</strong>s aresmall <strong>and</strong> scanty; <strong>the</strong>y lie close to<strong>the</strong> bronchial epi<strong>the</strong>lium <strong>and</strong> havevery short ducts.The proximal branches are dilated<strong>and</strong> distorted, but more peripheralones are flattened. Their histologyis similar to that described incorresponding bronchi <strong>of</strong> <strong>the</strong>406,01 previous case.In some areas <strong>the</strong> lesions aresimilar to those in severely affectedparts <strong>of</strong> previous specimens (Fig. 20).Sometimes, particularly near <strong>the</strong>4. i~; diaphragmatic surface <strong>of</strong> <strong>the</strong> lobe,it is impossible to define <strong>the</strong> outerwalls <strong>of</strong> air passages, or to distinguishbronchi from bronchioles.Granulation tissue in <strong>the</strong> bronchial<strong>and</strong> bronchiolar walls merges with<strong>the</strong> confluent interstitial pneumoniaforming a granulomatous mass,which contains epi<strong>the</strong>lium-linedclefts <strong>and</strong> patches <strong>of</strong> collapse.There are so many lymph folliclesthroughout this granulomatous tissueom hilum (Case 497). that <strong>the</strong> pulmonary lobules resemblelymph gl<strong>and</strong>s. No bronchial supportingtissues survive; thickened interlobular septa,however, help to identify <strong>the</strong> original outline <strong>of</strong> lobules.The close relationship <strong>of</strong> thickened branches <strong>of</strong> <strong>the</strong>pulmonary artery to <strong>the</strong> epi<strong>the</strong>lium-lined clefts suggeststhat <strong>the</strong> latter were originally bronchi <strong>and</strong> bronchioles,<strong>and</strong> unlikely to be re-epi<strong>the</strong>lialized pulmonary excavations.THE PATHOLOGY OFFOLLICULAR BRONCHIECTASISThese examples demonstrate that lesions mayrange from a relatively minor <strong>and</strong> inconspicuousfocus in one bronchopulmonary segment <strong>of</strong> ano<strong>the</strong>rwise normal lobe, to formation <strong>of</strong> a more orless solid lobe which bears little resemblance to<strong>the</strong> normal.In this investigation over a third <strong>of</strong> <strong>the</strong> specimensshowed features similar to <strong>the</strong> illustrated examples,with <strong>the</strong>ir typical microscopic lesions, <strong>the</strong> mostconstant <strong>and</strong> characteristic <strong>of</strong> which were <strong>the</strong> forma-
PATHOLOGY AND PATHOGENESIS OF BRONCHIECTASIS223tion <strong>of</strong> lymph follicles <strong>and</strong> interstitialpneumonia.LYMPH FOLLICLE FORMATIONSeverely diseased bronchi <strong>and</strong> bronchiolescontain many lymph follicles<strong>and</strong> nodes within <strong>the</strong>ir thickenedwalls, but, although this lymphoidtissue is extremely prominent, itforms only part <strong>of</strong> an extensivemural inflammation. At this stage <strong>of</strong> 5*<strong>the</strong> disease <strong>the</strong>re is widespread destruction<strong>of</strong> bronchial elastic tissue,muscle, cartilage, <strong>and</strong> mucous gl<strong>and</strong>s.From <strong>the</strong> examination <strong>of</strong> manyspecimens it appears that elastic tissueis <strong>the</strong> first <strong>of</strong> <strong>the</strong> supporting tissuesto be destroyed in <strong>bronchiectasis</strong>,muscle is <strong>the</strong> next to suffer, <strong>and</strong> cartilagesurvives <strong>the</strong> longest. Mucousgl<strong>and</strong>s are also destroyed, survivingfor about as long as cartilage. It isthought that once any <strong>of</strong> <strong>the</strong>se FIG. 19.-Same lobe as in Fig. 18, 5specialized tissues has been destroyedit cannot regenerate.In areas <strong>of</strong> very mild <strong>bronchiectasis</strong> <strong>the</strong>only abnormalities in <strong>the</strong> bronchial tree aresub-epi<strong>the</strong>lial accumulations <strong>of</strong> lymph follicles<strong>and</strong> nodes, <strong>and</strong> some oedema. Diffuseinflammation is not present <strong>and</strong> both muscle =<strong>and</strong> cartilage appear normal; special stains,however, show that <strong>the</strong>re is destruction <strong>of</strong>elastic tissue near <strong>the</strong> lymph follicles (Fig.16). It is considered that this loss <strong>of</strong> elastictissue is a fundamental lesion in follicular<strong>bronchiectasis</strong>, for once part <strong>of</strong> <strong>the</strong> bronchialtree has been damaged in this manner it ispermanently weakened <strong>and</strong> incapable <strong>of</strong>overcoming secondary infections.Apart from <strong>the</strong>ir destructive influence onelastic tissue, <strong>the</strong> lymph follicles, merelybecause <strong>of</strong> <strong>the</strong>ir size, distort <strong>the</strong> affectedbronchial tree. Sub-epi<strong>the</strong>lial follicles projectinto <strong>the</strong> lumina causing partial obstruction,while intramural follicles enlargebronchial walls, compressing <strong>the</strong> openings F<strong>of</strong> peripheral branches <strong>of</strong> <strong>the</strong> bronchialtreeSimilarwhichbutenter <strong>the</strong>morediseasedsevere effectsbronchi.are seen in t<strong>the</strong> bronchioles, where complete occlusion ; .4is <strong>of</strong>ten produced.Lymph follicles <strong>and</strong> nodes are present innormal lungs; Miller (1947) <strong>and</strong> Engel(1947) agree that lymphoid tissue occursat points <strong>of</strong> bifurcation <strong>of</strong> bronchi <strong>and</strong>' FIG. 20.- Follicular broncl- .- - WI .1.cm. from hilum.-hiectasis. Haematoxylin <strong>and</strong> eosin x 10.
224F. WHITWELLbronchioles, <strong>and</strong> between bronchioles <strong>and</strong> branches<strong>of</strong> pulmonary arteries which accomp.any <strong>the</strong>m. A<strong>study</strong> <strong>of</strong> normal lung segments has confirmed this,<strong>and</strong> has shown that this lymphoid tissue is outside<strong>the</strong> bronchial tree, where no alteration <strong>of</strong> elastictissue is to be seen.Abnormal lymphoid accumulations in <strong>the</strong> lungare sometimes seen in o<strong>the</strong>r forms <strong>of</strong> <strong>bronchiectasis</strong>,around chronic lung abscesses, <strong>and</strong> in tuberculosis.In <strong>the</strong>se conditions <strong>the</strong> number <strong>of</strong> follicles is muchsmaller <strong>and</strong> <strong>the</strong>y are mostly situated outside <strong>the</strong>bronchial tree, but local destructive changes dooccur near <strong>the</strong> occasional ones found in <strong>the</strong> bronchi.Many authors (Robinson, 1933; Ogilvie, 1941;Allison, Gordon, <strong>and</strong> Zinnernann, 1943) havementioned <strong>the</strong> presence <strong>of</strong> <strong>the</strong>se bronchial lymphfollicles in <strong>bronchiectasis</strong>, but <strong>the</strong>ir significance hasnot been studied, <strong>and</strong> only Engel (1947) has noted<strong>the</strong> associated loss <strong>of</strong> elastic tissue. He has calledthis condition " nodal bronchitis <strong>and</strong> bronchiolitis"<strong>and</strong> has described thickened collapsed bronchi <strong>and</strong>bronchioles where <strong>the</strong> walls contained lymphnodules but no diffuse cellular infiltration. Amarked loss <strong>of</strong> elastic tissue occurred near <strong>the</strong>JK3&NORMALEARLY CHANGA.9 ,LATE CHANGESLOBLFIG. 21.-Development <strong>of</strong> bronchiolar lesions <strong>and</strong> secondary lobular cfollicular <strong>bronchiectasis</strong>.rSESnodules, <strong>and</strong> this was noted too <strong>of</strong>ten for it to befortuitous. Engel commented that he was unableto decide whe<strong>the</strong>r this lesion was caused by avirus. an unusual infection, or some o<strong>the</strong>r influence.INTERSTITIAL PNEUMONIAInterstitial pneumonia is to be seen in o<strong>the</strong>rpulmonary conditions, but it is a constant feature<strong>of</strong> follicular <strong>bronchiectasis</strong>. The pneumonia isfound in <strong>the</strong> parenchyma around affected bronchioles,<strong>and</strong> its extent is dependent upon <strong>the</strong>severity <strong>of</strong> <strong>the</strong> <strong>bronchiectasis</strong>.In normal lung tissue <strong>the</strong> respiratory part <strong>of</strong> <strong>the</strong>organ appears in section as a lace-work <strong>of</strong> largespaces separated from one ano<strong>the</strong>r by thin-walledsepta (Maximow <strong>and</strong> Bloom, 1942). These fineinter-alveolar septa contain capillaries, elasticfibres, <strong>and</strong> a fine reticulum <strong>of</strong> connective tissue;<strong>and</strong> in normal parenchyma such interstitial tissuesare inconspicuous.In interstitial pneumonia, however, <strong>the</strong> peribronchiolar<strong>and</strong> inter-alveolar connective tissues areoedematous, <strong>and</strong> contain infiltrations <strong>of</strong> plasmacells, mononuclears, <strong>and</strong> lymphocytes, toge<strong>the</strong>rwith occasional lymph follicles, dilatedcapillaries <strong>and</strong> lymphatics. The vastincrease in bulk <strong>of</strong> interstitial tissues isassociated with a reduction in volume<strong>of</strong> <strong>the</strong> alveoli, <strong>and</strong> an alteration <strong>of</strong> <strong>the</strong>irlining cells.Cells lining normal alveoli are/- inconspicuous, but in interstitialpneumonia <strong>the</strong> alveoli are lined byan epi<strong>the</strong>lium <strong>of</strong> small cuboidal cells.The origini <strong>of</strong> this epi<strong>the</strong>lium is obscure;some think it is a down-growth <strong>of</strong>bronchiolar epi<strong>the</strong>lium, o<strong>the</strong>rs regardDv. it as a metaplasia <strong>of</strong> cells normallyfound lining alveoli, while Watts <strong>and</strong>___2fistMcDonald (1948) think that both <strong>the</strong>se',4RX, processes occur.In mild bronchiolar lesions only thosealveoli actually in contact with <strong>the</strong>bronchiolar walls appear to have undergonethis epi<strong>the</strong>lialization; in fact,in many instances only parts <strong>of</strong> <strong>the</strong>sealveoli are affected. As <strong>the</strong>se alteredalveoli are <strong>of</strong>ten only found in <strong>the</strong>periphery <strong>of</strong> pulmonary lobules, itseems unlikely that <strong>the</strong> lining cells area bronchiolar down-growth, <strong>and</strong> moreULE probable that local metaplasia hasoccurred as a result <strong>of</strong> interstitial insollapeinflammation.
PA THOLOG Y AND PA THOGENESIS OF BRONCHIECTASIS225CLINICAL FEATURES OF IFOLLICULAR BRONCHIECTASISThe ages <strong>of</strong> all <strong>the</strong> patients were obtained from<strong>the</strong> register, but only two-thirds <strong>of</strong> <strong>the</strong> case-recordswere available for analysis.The age distribution <strong>of</strong> all <strong>the</strong> cases <strong>of</strong> follicular<strong>bronchiectasis</strong> is shown in Fig. 4. O<strong>the</strong>r detailswere obtained from <strong>the</strong> 28 case-records, <strong>and</strong> are asfollows:Under 6 yrs.6-8 yrs. .9-1l yrs. ..12-14 yrs. .15-17 yrs. .18-20 yrs. .Over 20 yrs.IUnder 3 yrs.3-6 yrs. . .7-9 yrs. ..10-13 yrs. . .14-18 yrs. . .Over 18 yrs.AGE AT OPERATIONAGE AT ONSFT OF SYMPTOMS1 patient9 patients84 ,4 ,,2 ,0 -1 5 patients7 ,,2 ,,2 ,,2 ,,0 ,,PRE-OPERATIVE DIURATION OF SYMPTOMSUnder 1 yr. 0 patients1-3 yrs. . 7 ,,4-5 yrs. . 76-10yrs... 1011 5Iyrs. 2Over 15 yrs. 2NATURE OF ILLNESS AT ONSET OF SYMPTOMSMeasles <strong>and</strong>!or whooping-cough13 patientsPrimary bronchopneumonia ..6Insidious onset ..7Tonsillectomy ..1 patientCrush injury <strong>of</strong> chest ..I ,,PresentDoubtfulAbsentNot notedPresentDoubtfulAbsentNot notedFINGER CLUBBINGPARANASAL SINUS INFECTIONS10 patients410 420 patients43I patientThe severity <strong>and</strong> extent <strong>of</strong> <strong>the</strong> disease appearedto be unrelated to <strong>the</strong> nature or severity <strong>of</strong> <strong>the</strong>initial illness, or to <strong>the</strong> duration <strong>of</strong> <strong>the</strong> symptoms.Patients with finger clubbing did not have <strong>the</strong>more extensive or severe pulmonary lesions; <strong>the</strong>rewas also no correlation between finger clubbing<strong>and</strong> duration <strong>of</strong> symptoms.There was obvious correlation between <strong>the</strong>nature <strong>of</strong> <strong>the</strong> patients' sputa <strong>and</strong> <strong>the</strong> degree <strong>of</strong>inflammation in <strong>the</strong> bronchi.PATHOGENESIS OF FOLLICULAR BRONCHIECTASISThe main lesions occur in smaller bronchi,bronchioles, <strong>and</strong> in alveoli, while minor secondarychanges take place in <strong>the</strong> larger bronchi. The moresevere <strong>the</strong> involvement <strong>of</strong> <strong>the</strong> lobe, <strong>the</strong> moreproximally does each <strong>of</strong> <strong>the</strong>se processes extend, withobliteration <strong>of</strong> <strong>the</strong> distal bronchial tree. Secondarychanges in <strong>the</strong> larger bronchi include <strong>the</strong> destruction<strong>of</strong> supporting tissues around <strong>the</strong> mucous gl<strong>and</strong>ducts, which <strong>the</strong>n enlarge <strong>and</strong> form part <strong>of</strong> <strong>the</strong>bronchial wall.Small bronchi <strong>and</strong> bronchioles are affectedsimilarly; only <strong>the</strong> bronchiolar changes will bedescribed as <strong>the</strong>se are more closely associated with<strong>the</strong> parenchymal disease. By <strong>study</strong>ing lesions <strong>of</strong>different severity it is possible to visualize <strong>the</strong>evolution <strong>of</strong> <strong>the</strong> advanced condition (Fig. 21).The early changes consist <strong>of</strong> thickening <strong>of</strong>bronchiolar walls due to oedema <strong>and</strong> lymph follicleformation, with destruction <strong>of</strong> elastic tissue near<strong>the</strong> follicles. These bronchioles are usually ra<strong>the</strong>rflattened, <strong>and</strong> are surrounded by narrow rims <strong>of</strong>interstitial inflammation.More advanced lesions show a greater number <strong>of</strong>follicles <strong>and</strong> a diffuse mural bronchiolitis, withdestruction <strong>of</strong> all elastic tissue <strong>and</strong> most <strong>of</strong> <strong>the</strong>muscle. The bronchiolar lumina are reduced <strong>and</strong><strong>of</strong>ten appear stellate on cross-section. Interstitialinflammation involves wider areas <strong>of</strong> <strong>the</strong> parenchyma,<strong>and</strong> <strong>the</strong>re is fibrosis around branches <strong>of</strong> <strong>the</strong>pulmonary arteries. Often <strong>the</strong> interlobular septa<strong>and</strong> pleural membrane are thickened. ~FAlveol,ar collapse has been seen only in specimenswhere <strong>the</strong>re was thickening <strong>of</strong> interlobular septa<strong>and</strong> pleural membrane. Microscopically this collapseis <strong>of</strong> <strong>the</strong> type produced by compression, <strong>and</strong>its distribution is lobular.The cause <strong>of</strong> <strong>the</strong> alveolar collapse can be foundin <strong>the</strong> lobules (Fig. 21). Thickened interlobularsepta <strong>and</strong> pleural membrane keep <strong>the</strong> outline <strong>of</strong> alobule rigid, but as <strong>the</strong> centre contains an exp<strong>and</strong>inggranulomatous mass (which has arisen from <strong>the</strong>bronchiole <strong>and</strong> peribronchiolar tissues) pressurewithin <strong>the</strong> lobule becomes raised. This tensionproduces both flattening <strong>of</strong> <strong>the</strong> weakened bronchiolarwalls, which reduces <strong>the</strong> lumen to a narrowcleft, <strong>and</strong> compression collapse <strong>of</strong> <strong>the</strong> alveolioutside <strong>the</strong> area <strong>of</strong> pneumonia.THE AETIOLOGY OF FOLLICULAR BRONCHIECTASISThe important clinical facts are that <strong>the</strong> conditionusually begins in early childhood <strong>and</strong> is asequel to whooping-cough, measles, or primarybronchopneumonia. This <strong>bronchiectasis</strong> may alsohave an insidious onset.The essential lesions are destructive muralbronchitis, bronchiolitis, <strong>and</strong> interstitial inflammation,<strong>and</strong> <strong>the</strong> <strong>pathology</strong> appears very closely relatedto <strong>the</strong> acute interstitial pneumonias which werereported by MacCallum (1940) in fatal cases <strong>of</strong>measles <strong>and</strong> influenza <strong>and</strong> whooping-cough.MacCallum described <strong>the</strong> lesions found in servicepersonnel, but Engel (1947) has reported a similar
226F. WHITWELLFIG. 22.-Saccular <strong>bronchiectasis</strong> <strong>of</strong> right lower lobe (Case 395)2.5 cm. from hium. Haematoxylin <strong>and</strong> eosin >' 1.5.multifocal condition in children, under <strong>the</strong> name<strong>of</strong> destructive mural bronchiolitis. MacCallum saysthat this condition always follows a virus infection<strong>and</strong> haemophilic organisms can usually be grownfrom <strong>the</strong> lungs, <strong>and</strong> Engel has suggested a viralorigin for his " nodal bronchiolitis."Follicular <strong>bronchiectasis</strong> is very like rodent<strong>bronchiectasis</strong> (Cruikshank, 1948), which has beenshown by Nelson (1946) to be <strong>of</strong> viral origin.Follicular <strong>bronchiectasis</strong> is probably <strong>the</strong> sequel<strong>of</strong> acute viral infection <strong>of</strong> <strong>the</strong> lungs contracted inearly childhood. Usually this infection occurs withwhooping-cough or measles, or, when influenzal itis described as primary bronchopneumonia. Insome cases it may be relatively symptomless, likeo<strong>the</strong>r virus pneumonias, <strong>and</strong> pass unnoticed byparents. The original inflammation is probablymultifocal, <strong>and</strong> normally clears up without anyresidual damage, but in bronchi which are inadequatelydrained <strong>of</strong> secretions <strong>the</strong> permanent changes<strong>of</strong> follicular <strong>bronchiectasis</strong> may arise.SACCULAR BRONCHIECTASIS"Saccular " is an apt word because it fits both<strong>the</strong> anatomical <strong>and</strong> <strong>the</strong> bronchographic appearance,though many specimens which did not show thisFIG. 23.-Saccular <strong>bronchiectasis</strong> <strong>of</strong> right lower lobe 4 cm. fromhilum (Case 395). Haematoxylin <strong>and</strong> eosin x 1.5.type <strong>of</strong> <strong>pathology</strong> could have been described assaccular from <strong>the</strong> bronchograms.Twenty-three examples <strong>of</strong> this condition occurredin <strong>the</strong> present series. Two <strong>of</strong> <strong>the</strong>m will be describedin some detail, <strong>and</strong> <strong>the</strong> <strong>pathology</strong>, clinical features,<strong>and</strong> <strong>pathogenesis</strong> <strong>of</strong> saccular <strong>bronchiectasis</strong> will bedi-cussed.CASE 395.-A 33-year-old woman, previously healthyapart from bad head colds, had suffered from a troublesomecough for three years, <strong>and</strong> her symptoms hadbecome more severe recently. Her sputum was copious,purulent, <strong>and</strong> occasionally blood-stained. She hadfinger clubbing <strong>and</strong> was dyspnoeic on slight exertion.Bronchograms showed <strong>bronchiectasis</strong> limited to <strong>the</strong>right middle <strong>and</strong> lower lobes. Right lower lobectomywas performed.Macroscopic Appearance <strong>of</strong> Specimen.-The specimenis an aerated, pigmented lobe with pleural thickeningover <strong>the</strong> apical <strong>and</strong> diaphragmatic surfaces.On section (Figs. 22 <strong>and</strong> 23) <strong>the</strong> apical segment showssome collapse, emphysema, <strong>and</strong> interstitial pneumoniabut <strong>the</strong> bronchi appear normal. The base <strong>of</strong> <strong>the</strong> lobeshows gross <strong>bronchiectasis</strong>, with <strong>the</strong> main bronchi <strong>of</strong>normal calibre, though slightly thickened <strong>and</strong> occludedby folds <strong>of</strong> hypertrophic epi<strong>the</strong>lium, while more peripheralbronchi form pus-filled cavities. These sacculesare surrounded by aerated alveoli, <strong>and</strong> <strong>the</strong>re isfibrous thickening <strong>of</strong> <strong>the</strong> interlobular septa.
X * a! tvo,,,, s^
~~~~~~~~~~~~~~~~~~~~~~.228F. WHITWELLThe pre-saccular bronchishow marked polypoid changesin <strong>the</strong> epi<strong>the</strong>lium. In Fig. 25polyposis <strong>of</strong> <strong>the</strong> basal segmentalbronchi can be compared with<strong>the</strong> smooth epi<strong>the</strong>lial lining <strong>of</strong><strong>the</strong> normal apical bronchus.The epi<strong>the</strong>lial lining <strong>of</strong> <strong>the</strong>saccules is flatter than in <strong>the</strong>previous specimen, <strong>and</strong> areas <strong>of</strong>squamous metaplasia are moreextensive. No connexion wasfound between <strong>the</strong> saccules <strong>and</strong>any distal bronchial tree-infact no intact distal bronchi arepresent, though respiratory bronchiolesoccur in <strong>the</strong> parenchyma.The base <strong>of</strong> <strong>the</strong> lobe is wellaerated except for a narrow zone<strong>of</strong> collapse around <strong>and</strong> between<strong>the</strong> saccules. In <strong>the</strong> areas <strong>of</strong> collapse<strong>the</strong> alveoli are flattened concentricallyaround <strong>the</strong> saccules.There is no inflammatoryreaction in <strong>the</strong> parenchyma, <strong>and</strong>only within <strong>the</strong> peribronchial,perisaccular, <strong>and</strong> interlobularsepta is an increase <strong>of</strong> fibroustissue to be found.THE PATHOLOGY OF SACCULARBRONCHIECTASISFIG. 26.-Saccular <strong>bronchiectasis</strong> 5 cm. from hilum (Case 451). Haematoxylin <strong>and</strong> eosin x 1.5. These two examples arethought to be <strong>the</strong> end-resultconspicuous by thickening <strong>of</strong> interlobular fibrous septa. <strong>of</strong> a distinctive t: ;ype <strong>of</strong> <strong>bronchiectasis</strong>. AlthoughWithin <strong>the</strong>se lobules <strong>the</strong>re are some respiratory bron- only 17% <strong>of</strong> s,pecimens show <strong>the</strong>se lesions,chioles, but terminal bronchioles are replaced by fibrous some <strong>of</strong> <strong>the</strong> unclatssifiedlobes are probably earlierscars. stages <strong>of</strong> <strong>the</strong> ssame condition. CharacteristicCASE 451.-An 18-year-old boy was admitted to features are grossloss <strong>of</strong> bronchial structures in <strong>the</strong>hospital because <strong>of</strong> a troublesome cough <strong>and</strong> a single saccules, normaliity <strong>of</strong> <strong>the</strong> alveoli around <strong>the</strong>slight haemoptysis. Bronchitis had occurred during <strong>the</strong>sprevious four winters, but <strong>the</strong>re was no history <strong>of</strong> earlier polyposis" <strong>of</strong> <strong>the</strong> pre-saccular<strong>and</strong>saccules, rrespiratory complaint or infectious diseases. He pro- bronchi,*etain normal supporting tissues.whlch rduced 3 oz. <strong>of</strong> purulent sputum daily, had marked finger The saccules <strong>and</strong> <strong>the</strong> pre-saccular bronchi can beclubbing, <strong>and</strong> bronchograms showed <strong>bronchiectasis</strong> considered separaltely, <strong>the</strong> former being regarded aslimited to <strong>the</strong> left lower lobe. This lobe was excised. <strong>the</strong> primary abno irmality.Macroscopic Appearance <strong>of</strong> Specimen.-The lobe is SACCULES.-Saccules are essentially fibrous struc-epi<strong>the</strong>lium; <strong>the</strong>y have nobulky, aerated, slightly pigmented, <strong>and</strong> has a shiny tures lined by a ciuboidalpleural membrane.elastic tissue, mus,cleor cartilage in <strong>the</strong>ir walls, <strong>and</strong>Sections <strong>of</strong> <strong>the</strong> lobe (Figs. 25 <strong>and</strong> 26) show a normal <strong>the</strong>ir lining memtbranes contain no normal ciliatedapical segment but severe <strong>bronchiectasis</strong> in <strong>the</strong> whole respiratory epi<strong>the</strong>lium.This absence <strong>of</strong> recogniz-saccules has led to speculation<strong>of</strong> <strong>the</strong> base. The segmental basal bronchi <strong>and</strong> <strong>the</strong>ir main able tissues in thiebranches are not thickened or dilated, but <strong>the</strong>y are about <strong>the</strong>ir originpartially occluded by epi<strong>the</strong>lial " polyposis";<strong>and</strong> this subject will be discussedmorelater.distal bronchi are saccular <strong>and</strong> filled with pus. The la er.alveoli <strong>of</strong> <strong>the</strong> basal segments are aerated, except imme- The constant finding <strong>of</strong> areas <strong>of</strong> squamousdiately around <strong>the</strong> saccules where <strong>the</strong>re is some collapse. metaplasia in <strong>the</strong> saccular epi<strong>the</strong>lium is <strong>of</strong> specialMicroscopic Features.-There is obvious similarity interest as this p] ohenomenon is uncommon in any.to <strong>the</strong> previous case, <strong>and</strong> only points <strong>of</strong> difference will <strong>of</strong> <strong>the</strong> o<strong>the</strong>r types <strong>of</strong> <strong>bronchiectasis</strong> examined. Thebe stressed.usual distribution <strong>of</strong> this metaplasia is shown in <strong>the</strong>
_ * _ * ........... r _ r- -[two examples (Figs. 24 <strong>and</strong> 27); sometimes itis less extensive, but in a few specimens <strong>the</strong>whole saccular lining is replaced by squamous Iepi<strong>the</strong>lium extending for some distance up <strong>the</strong>pre-saccular bronchi.Squamous metaplasia is mentioned in most_Xaccounts <strong>of</strong> <strong>bronchiectasis</strong> in <strong>the</strong> literature,but its distribution in <strong>the</strong> diseased lobes has ararely been described. From published illustrationsit is clear that <strong>the</strong> term has been applied indiscriminatelyto various epi<strong>the</strong>lial patterns, suchas <strong>the</strong> layers <strong>of</strong> heaped-up, flattened cells thatrestore breaches <strong>of</strong> epi<strong>the</strong>lial continuity, <strong>and</strong> <strong>the</strong>transitional epi<strong>the</strong>lial appearance seen in obliquely -~ rsectioned bronchi (Engel, 1947). In <strong>the</strong> presentaccount <strong>the</strong> term is used only when prickle cellsor keratinization have been seen; <strong>the</strong> latter isextremely rare <strong>and</strong> was found only in threeFIG. 27.-Model <strong>of</strong> basal segments <strong>of</strong> Case 451 (saccularspecimens.<strong>bronchiectasis</strong>).e§;ev16Robinson (1933, 1939) desei / l{is'>
230F. WHITWELLFIG. 29.-Saccules surrounded by rims <strong>of</strong> compression collapse (CasHaematoxylin <strong>and</strong> eosin x 7.5.monary tuberculosis; Willis's statement cannot<strong>the</strong>refore be accepted.THE PRE-SACCULAR BRONCHI.-NO dilatationoccurs in <strong>the</strong> bronchi <strong>and</strong> <strong>the</strong>re is little destruction<strong>of</strong> supporting tissues, despite <strong>the</strong> severe inflammatoryreaction in <strong>the</strong> bronchial walls. The mainabnormality is polyposis <strong>of</strong> <strong>the</strong> bronchial epi<strong>the</strong>lium,<strong>of</strong>ten extensive enough to produce considerablebronchial obstruction.In <strong>the</strong> present material this change has been seenonly in saccular <strong>bronchiectasis</strong>, but similar lesionsare to be found in <strong>the</strong> bronchi draining chroniclung abscesses <strong>and</strong> secondarily infected tuberculouscavities.The bronchoscopic <strong>and</strong> histological features <strong>of</strong>this polypoid change have been described byJackson <strong>and</strong> Jackson (1932), who thought that itwas an inflammatory reaction produced by continualirritation from pus, an opinion supported by<strong>the</strong> present <strong>study</strong>. Peroni (1934) considered that<strong>the</strong> polyps occurred first, <strong>and</strong> <strong>the</strong>n produced<strong>bronchiectasis</strong> by obstruction. Samsonj (1940) described a severe case <strong>and</strong> thought2 <strong>the</strong> cause was an individual susceptibilityto mucin. Many accounts <strong>of</strong> <strong>the</strong> <strong>pathology</strong><strong>of</strong> <strong>bronchiectasis</strong> mention <strong>the</strong> hypertrophicbronchial epi<strong>the</strong>lium, but <strong>the</strong> site <strong>and</strong>association with saccules have not beenstressed.COLLATERAL AIR CIRCULATION IN. DISEASED SEGMENTS.-Tfle observation thatall bronchi in <strong>the</strong> diseased segments end inblind saccules, <strong>and</strong> that <strong>the</strong>se segmentsare well aerated, is considered to be <strong>of</strong>some importance. It provides histologicalconfirnation <strong>of</strong> <strong>the</strong> existence <strong>of</strong> a collateralair circulation in <strong>bronchiectasis</strong>, whichchallenges <strong>the</strong> validity <strong>of</strong> certain popular<strong>the</strong>ories <strong>of</strong> <strong>pathogenesis</strong>.i Hf Collateral air circulation was originallya <strong>the</strong>oretical conception based upon a* belief in <strong>the</strong> existence <strong>of</strong> alveolar pores.it, Later this <strong>the</strong>ory was tested <strong>and</strong> confirmedby animal experiments (Van Allen <strong>and</strong>Jung, 1931), <strong>and</strong> more recently by Baarsma<strong>and</strong> Dirken (1948) using healthy rabbits,<strong>and</strong> by Baarsma, Dirken, <strong>and</strong> Huizinga(1948) in normal human lungs. Theseworkers considered that a collateral aircirculation occurred only in <strong>the</strong> absence <strong>of</strong>inflammatory change in <strong>the</strong> obstructedsegments.;e 451). The importance <strong>of</strong> this mechanism indiseased lungs has only recently receivedany attention. Churchill (1949), describing <strong>the</strong>radiological appearances <strong>of</strong> isolated bronchiectaticlobes in which <strong>the</strong> bronchi had been filled withlipiodol, mentioned dilated bronchi extending intoair-containing parenchyma but in no way communicatingwith it. These segments contained trappedair, as <strong>the</strong>y did not deflate when <strong>the</strong> lobes wereremoved from <strong>the</strong> body <strong>and</strong> left <strong>the</strong> bronchi open.This trapped air serves <strong>the</strong> function <strong>of</strong> filling upspace but it has no oxygenating value.In <strong>the</strong> two examples <strong>of</strong> saccular <strong>bronchiectasis</strong><strong>the</strong> air must have reached <strong>the</strong> basal parenchymathrough <strong>the</strong> normal apical segments. This suggeststhat <strong>the</strong> intersegmental <strong>and</strong> interlobular fibroussepta are really incomplete fibrous networks which<strong>of</strong>fer no barrier to air. Alveolar pores have beenseen in <strong>the</strong> aerated alveoli <strong>of</strong> most specimenswhenever sought in thick sections (Fig. 31).Although collateral air circulation is most easilydemonstrated in <strong>the</strong> saccular cases, it occurs inmost forms <strong>of</strong> <strong>bronchiectasis</strong> which do not involveentire lobes.
PATHOLOGY AND PATHOGENESIS OF BRONCHIECTASIS 231CLINICAL FEATURES OF SACCULAR BRONCHIECTASISThe age distribution <strong>of</strong> all <strong>the</strong>se patients is shownin Fig. 4. Sixteen case-records were available for \\NORMAL APICALSE\.analysis, <strong>and</strong> <strong>the</strong> details are tabulated.XAGE AT OFERATIONUnder 5 yrs. 0 patients 'il15 0yrs. 5 ,\_26-30yrs.7., 21-25yrs.52| 1 9 $ 9 ''_31 35 Nrs.. . I36-40yrs.I patientOver 40 yrs.AGE AT ONSET OF SYMPTOMS ORMAL BASAL SEGACough " all life time "...patientsUnder 9 vrs. (except above) 09-12yrs .. .. I patient13-18 yrs. .. 6 patients19-25yrs...Over 25 yrs. ..I patientPRE-OPERATIVE DURATION OF SYMPTOMSUnder 2 yrs.3 patien is2-6yrs. 87l1O0 rs. 211-15yrs.Ipatient16 20yrs. IOver 20yrs.INATURE OF ILLNESS AT ONSET-OF SYMPTOMS )'Measles <strong>and</strong>, or whooping cough0 patientsBronchopneumonia .. 9Fairly recent insidious onset 4 -I'Cough all life but no severe childhoodillnesses.3FINGER CLtJBBINGPresent.10 patients FIG. 30.-Development <strong>of</strong> collateral air circulation in saccularDoubtful 2 ,. <strong>bronchiectasis</strong>.Absent. 2Not recorded.2 All patients had copious purulent sputum.PARANASAL SINUS INFECTIONS No correlation was found between <strong>the</strong> extent,Present*9 patients severity, <strong>and</strong> duration <strong>of</strong> <strong>the</strong> disease, <strong>and</strong> <strong>the</strong>Doubtful .. 2Absent .. 3 " presence <strong>of</strong> finger clubbing.Not recorded .. 2It is impossible to correlate <strong>the</strong>ulj|jdegree A <strong>of</strong> polyposis <strong>and</strong> squamousmetaplasia to <strong>the</strong> duration <strong>of</strong> illness.PATHOGENESIS OF SACCULARBRONCHIECTASISAs <strong>the</strong> changes in pre-saccularbronchi are considered secondaryto <strong>the</strong> saccular lesions any discussionon <strong>pathogenesis</strong> amount,to<strong>the</strong> question, "From what <strong>and</strong> howdo <strong>the</strong> saccules arise?""SrrE OF THE SACCULES. -Writershave variously suggested that <strong>the</strong>W iw dilatations ^ w <strong>of</strong> <strong>bronchiectasis</strong> originatefrom <strong>the</strong> bronchi (Robinson,1933; Ogilvie, 1941; Mallory, 1947),<strong>the</strong> bronchioles (L<strong>and</strong>er <strong>and</strong> Davidson,1938), <strong>and</strong> <strong>the</strong> parenchyma(Opie, 1928; Erb, 1933; McNeil,~ _ 4 R Macgregor, <strong>and</strong> Alex<strong>and</strong>er, 1929;IFIG. 31.-Alveolar pores seen in thick sections. Elastic stain with pyronin x 600. Lisa <strong>and</strong> Rosenblatt, 1943).
232F. WHlTWELLNeoprene casts, reconstruction models, <strong>and</strong>dissections <strong>of</strong> <strong>the</strong> bronchial tree show that sacculesare <strong>the</strong> bulbous terminations <strong>of</strong> <strong>the</strong> first to thirdbranchings <strong>of</strong> <strong>the</strong> segmental bronchi. As adultbronchioles arise only after about 18 branchingsfrom <strong>the</strong> segmental bronchi (Broman, 1923; Reid,1950). <strong>the</strong> saccules clearly cannot be <strong>of</strong> bronchiolarorigin.Saccules are <strong>the</strong> direct continuations <strong>of</strong> largebronchi, <strong>the</strong>y are encased within extension <strong>of</strong>'<strong>the</strong>peribronchial fibrous septa, <strong>and</strong> <strong>the</strong>y are placedclose to <strong>and</strong> parallel with branches <strong>of</strong> pulmonaryarteries. Their situation suggests that <strong>the</strong>y wereoriginally bronch:, <strong>and</strong> not bronchopulmonaryexcavations.CAUSE OF DILATATION. First, it is possible toeliminate certain <strong>of</strong> <strong>the</strong> factors that are <strong>of</strong>tensuggested as causes <strong>of</strong> dilatation. Alveolar collapseis negligible in <strong>the</strong>se specimens <strong>and</strong> cannot beconsidered as a possible cause, in spite <strong>of</strong> absoluteperipheral bronchial obstruction. Fibrous tissuefound in <strong>the</strong> saccular walls occurs only as a replacement<strong>of</strong> original bronchial structures. This fibrosisis concentric with <strong>the</strong> saccules, <strong>and</strong> not in a planewhere, by contracting, it could exert any dilatingforce on <strong>the</strong> bronchi. Most writers link toge<strong>the</strong>rfibrosis <strong>and</strong> contraction, especially when discussing<strong>bronchiectasis</strong>. However, <strong>the</strong> behaviour <strong>of</strong> fibroustissue is perverse, <strong>and</strong> many examnples occur <strong>of</strong> itsproperty <strong>of</strong> ungoverned stretching, e.g., aorticaneurysms <strong>and</strong> in repaired hernias. Probably <strong>the</strong>stretching <strong>of</strong> fibrous tissue in saccular walls is afactor in <strong>the</strong> production <strong>of</strong> dilatation.The clinical findings <strong>of</strong> this group <strong>of</strong> patientsshow that while in many cases <strong>the</strong> <strong>bronchiectasis</strong>dated from an attack <strong>of</strong> bronchopneumonia, innearly half <strong>the</strong> patients <strong>the</strong> disease had an insidiousonset which escaped notice.It is considered that saccular <strong>bronchiectasis</strong>begins as a chronic mural inflammation <strong>of</strong> <strong>the</strong>medium-sized bronchi. This condition destroysbronchial wall structures <strong>and</strong> obliterates peripheralbranches (Fig. 30), but is not sufficiently acute ordiffuse to produce parenchymal scarring or tointerfere with <strong>the</strong> establishment <strong>of</strong> a collateral air.circulation, provided all segments <strong>of</strong> a lobe arenot affected.The saccular shape <strong>of</strong> <strong>the</strong> diseased brolnchi isprobably produced after <strong>the</strong> destruction <strong>of</strong> supportingtissues <strong>and</strong> occlusion <strong>of</strong> peripheral branches,<strong>and</strong> results from distension by contained pus, <strong>the</strong>pressure <strong>of</strong> which is increased by <strong>the</strong> partial occlusion<strong>of</strong> pre-saccular bronchi (see Fig. 28). Support islent to this <strong>the</strong>ory by <strong>the</strong> compression-collapseseen in several specimens in perisaccular alveoli(Fig. 29) suggesting that an expansile force iscentred within <strong>the</strong> saccules.The <strong>the</strong>ory that dilatation is produced throughdistension <strong>of</strong> <strong>the</strong> bronchi by pus was originally putforward by Laennec, but only a few (Riviere, 1905)have shared his opinion. As early as 1838 Williamsdiscredited Laennec's <strong>the</strong>ory by arguing that mostpatients with copious sputum do not developdilatation, <strong>and</strong> many patients with <strong>bronchiectasis</strong>have little sputum. Williams's argument was falsebecause it did not take into account <strong>the</strong> condition<strong>of</strong> <strong>the</strong> bronchial walls. Andrus (1937) discussedthis subject <strong>and</strong> said:" As a problem in physics it is sufficient to noteat this time that in order to exert a dilating force itwould be necessary that <strong>the</strong> secretion occupy <strong>the</strong> grosssection <strong>of</strong> <strong>the</strong> lumen <strong>of</strong> <strong>the</strong> bronchus; such a conditionwould, however, necessarily result in atelectasis,<strong>and</strong> its possible effects be indistinguishable from <strong>the</strong>latter."His <strong>the</strong>oretical aerodynamics did not allow forcollateral air circulation, <strong>and</strong> <strong>the</strong> illustrated examples.do not support his statement.ATELECTATIC BRONCHIECTASISIn recent years <strong>the</strong>re have been many accounts<strong>of</strong> <strong>the</strong> association <strong>of</strong> lobar <strong>and</strong> segmental collapsewith <strong>bronchiectasis</strong>, <strong>and</strong> it has become widelyaccepted that <strong>the</strong> collapse leads to <strong>the</strong> <strong>bronchiectasis</strong>.In this condition, which has been calledatelectatic <strong>bronchiectasis</strong> (although it is recognizedto be an acquired disease), <strong>the</strong> collapse is usuallythought to be caused by peripheral bronchialobstruction. Many writers have gone even fur<strong>the</strong>r<strong>and</strong> stated that all <strong>bronchiectasis</strong>, even whencongenital, is caused in this way.The specimens which have here been classifiedas follicular <strong>and</strong> saccular rarely showed collapse,even on microscopic exa-mination; where collapsewas found it appeared to be consequent to <strong>the</strong><strong>bronchiectasis</strong>. However, some o<strong>the</strong>rs <strong>of</strong> <strong>the</strong>specimens did show severe alveolar collapse, sa<strong>the</strong>y have been examined as a group in an attemptto find out whe<strong>the</strong>r <strong>the</strong> collapse or <strong>the</strong> <strong>bronchiectasis</strong>comes first, <strong>and</strong> how this condition arises.The specimens lack homogeneity; in some <strong>the</strong>bronchi are collapsed, in o<strong>the</strong>rs <strong>the</strong>re is grossdilatation, <strong>and</strong> in most <strong>of</strong> <strong>the</strong>m <strong>the</strong> bronchi arethickened but only moderately dilated (Fig. 32).However, <strong>the</strong> grouping has been <strong>of</strong> some valuebecause it has shown that " atelectatic <strong>bronchiectasis</strong>"differs from o<strong>the</strong>r forms <strong>of</strong> <strong>the</strong> disease inits lobar <strong>and</strong> segmental distribution, <strong>and</strong> in <strong>the</strong>
PATHOLOGY AND PATHOGENESIS OF BRONCHIECTASIS 233r-2L ~ ~~~~~ '.1 ~ ~~~~ S+. 1*2-.X~~~~~~\&"AI~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ J%--4s~'''| ~ 1.4'~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~'- '>.P'w^* wq. -1 f\0ziSl v*) FE p 1-4-0-1M#vi *ffhQ\Bs -#--pqee"4 "'" ~*specimens form only a quarter <strong>of</strong> <strong>the</strong> whole series,'<strong>the</strong>y represent three-quarters <strong>of</strong> <strong>the</strong> collapsed tspecimens.*Specimens consisting <strong>of</strong> middle with lower lobes 5 .'-^ . ;>r *-3 ido not always show atelectatic <strong>bronchiectasis</strong> in FIG. 34.-Atelectatic <strong>bronchiectasis</strong> with intra-bronchiolarboth lobes. The findings are as follows. <strong>and</strong> intra-alveolar haemorrhage with patent bronchioles..... -..- I I --.
234Middle Lobe Lower Lobe Specimens No. <strong>of</strong>Collapse only Atelectatic <strong>bronchiectasis</strong> 2Atelectatic <strong>bronchiectasis</strong> Collapse only IAtelectatic <strong>bronchiectasis</strong> Atelectatic <strong>bronchiectasis</strong> 3Atelectatic <strong>bronchiectasis</strong> Saccular <strong>bronchiectasis</strong> ICollapse only Follicular <strong>bronchiectasis</strong> 1Atelectatic <strong>bronchiectasis</strong> Follicular <strong>bronchiectasis</strong> 1Collapse only Unclassified <strong>bronchiectasis</strong> IF. WHITWELLSEGMENTAL DISTRIBUTION.-In all segments <strong>of</strong> anaffected lobe <strong>the</strong> bronchi show similar histologicalchanges. It is very difficult to assess calibre differencesin collapsed specimens, but usually <strong>the</strong>degree <strong>of</strong> dilatation appeared about equal in eachsegment.BRONCHIAL OBSTRUCTION.-The lobar, bronchihave been examined for stenoses <strong>and</strong> o<strong>the</strong>r lesionsthat might cause bronchial obstruction. None ispresent in lobes showing <strong>bronchiectasis</strong>, but inspecimens <strong>of</strong> simple collapse <strong>the</strong> bronchi are alsocollapsed <strong>and</strong> <strong>the</strong>refore obstructed.Sections have been examined microscopically forobstructing lesions <strong>of</strong> <strong>the</strong> peripheral bronchial tree.In contrast to follicular <strong>and</strong> saccular <strong>bronchiectasis</strong>,in which peripheral obstruction is invariable, <strong>the</strong>bronchioles are patent <strong>and</strong> can be followed into <strong>the</strong>pulmonary lobules, where <strong>the</strong> air cells are partlycollapsed (Fig. 34).HILAR LYMPH-GLAND CHANGES.- In many specimens<strong>the</strong> lymph-gl<strong>and</strong>s around <strong>the</strong> hilar bronchiare greatly enlarged, <strong>and</strong> on section showed nonspecificchronic lymphadenitis, <strong>of</strong>ten with fibroticchanges. These gl<strong>and</strong>s are indistinguishable from<strong>the</strong> hilar gl<strong>and</strong>s in follicular <strong>bronchiectasis</strong>.In three <strong>of</strong> <strong>the</strong> middle with lower lobe specimens<strong>the</strong>re are small partly-calcified caseous foci in <strong>the</strong>periphery <strong>of</strong> one lobe (two in middle lobes <strong>and</strong> onein a lower lobe), <strong>and</strong> a similar focus is present in<strong>the</strong> periphery <strong>of</strong> a left lower lobe. In two <strong>of</strong><strong>the</strong>se specimens <strong>the</strong> hilar lymph-gl<strong>and</strong>s containcalcified caseous foci. Except for two specimens <strong>of</strong>tuberculous <strong>bronchiectasis</strong> <strong>and</strong> a saccular <strong>bronchiectasis</strong>with tuberculosis in <strong>the</strong> non-bronchiectaticpart <strong>of</strong> <strong>the</strong> lobe, <strong>the</strong>se are <strong>the</strong> only tuberculouslesions seen in <strong>the</strong> whole series.BRONCHIAL TREE.-The bronchi in collapsedspecimens show similar histology throughout alobe. There may be (1) moderate inflammationwithout any destruction <strong>of</strong> supporting tissues.This was also always seen in specimens <strong>of</strong> simplecollapse. (2) Slight superficial inflammation, butbronchial walls show dense fibrous thickening, <strong>and</strong>contain no elastic tissue, muscle, or cartilage(Fig. 33). (3) Severe inflammatory changes wi<strong>the</strong>pi<strong>the</strong>lial ulcerations <strong>and</strong> destruction <strong>of</strong> supportingtissues.The bronchioles show similar lesions, but are lessseverely affected. In some specimens inflamedbronchial walls contain numerous lymph follicles,but interstitial pneumonia is absent.The type <strong>of</strong> histological change in <strong>the</strong> bronchiappears to be unrelated to <strong>the</strong> degree <strong>of</strong> dilatation.ALVEOLI.-In spite <strong>of</strong> <strong>the</strong> gross reduction in size<strong>of</strong> <strong>the</strong> lobes, <strong>and</strong> <strong>the</strong> apparent total alveolar collapse,<strong>the</strong> microscopic appearances are usuallythose <strong>of</strong> incomplete absorption collapse.Many lobes seem to be infarcted; in <strong>the</strong>se <strong>the</strong>reis extravasation <strong>of</strong> red cells into interstitial tissues,<strong>and</strong> <strong>the</strong> partly collapsed alveoli, <strong>and</strong> some bronchioles,are distended with blood (Fig. 34). MostFIG. 35.-Development <strong>of</strong> atelectatic<strong>bronchiectasis</strong> (a) smallfocus in periphery <strong>of</strong> middle<strong>and</strong> lower lobe; (b) enlargedhilar gl<strong>and</strong>s <strong>and</strong> lobar col-(t }~ 1 tlapse; (c) atelectatic <strong>bronchiectasis</strong>with calcified foci inhilar gl<strong>and</strong>s.abc
PATHOLOGY AND PA THOGENESIS OF BRONCHIECTASIS<strong>of</strong> this haemorrhage consists <strong>of</strong> fresh red cells, but(leposits <strong>of</strong> haemosiderin in cells <strong>of</strong> <strong>the</strong> alveolarwalls <strong>and</strong> in intra-alveolar heart-failure cells showsthat some bleeding must have occurred beforeoperation. This intra-alveolar haemorrhage wasrarely seen in o<strong>the</strong>r forms <strong>of</strong> <strong>bronchiectasis</strong>. Theoperative technique was similar in all cases.In <strong>the</strong> lobes showing simple collapse elastictissue in alveolar walls appears to be thickened,probably because <strong>of</strong> its relaxed state. In atelectatic<strong>bronchiectasis</strong> <strong>the</strong> alveolar wall elastic tissue isei<strong>the</strong>r represented by a few short thick curls, or itis completely absent. A variable amount <strong>of</strong>inter-alveolar fibrosis is seen but <strong>the</strong>re are noo<strong>the</strong>r signs <strong>of</strong> inflammation.CLINICAL FEATURES OF ATELECTATICBRONCHIECTASISThe age distribution <strong>of</strong> all cases is shown inFig. 4. The case-records <strong>of</strong> 15 patients wereavailable for analysis, <strong>and</strong> provided <strong>the</strong> followingdetails.AGE AT OPERATIONUnder 5 yrs.5-10 yrs.11-1 5 yrs.16-20yrs.21-25yrs.26-30yrs.Over 30 yrs.AGE AT ONSET OF SYMPTOMSUnder 3 yrs.3-6yrs.15yrs.21-23yrs.Not stated0 patients6 332 -I patient0 ,3 patients7I patientpatients2PRE-OPERATIVE DURATION OF SYMPTOMSUnder I yr. 0 patients1-3 yrs. 54-5 yrs. 36-10 yrs. 3II-I 5 yrs. 2Not stated 2NATURE OF ILLNESS AT ONSET OF SYMPTOMSMeasles <strong>and</strong>/or whooping cough7 patientsPrimary bronchopneumonia 3Insidious onset .. 2Pleurisy .. I patientNotstated.2 patientsFINGER CLUBBINGPresent (recorded as mild)Absent . .Not statedPresentDoubtfulAbsentPARANASAL SINUS INFECTIONS5 patients9 .,I patient3 patients48Three patients who had tuberculous foci in <strong>the</strong>lobes <strong>and</strong> hilar lymph-gl<strong>and</strong>s dated <strong>the</strong>ir symptomsfrom whooping-cough or measles in early childhood.There was a close correlation between <strong>the</strong> amount<strong>of</strong> inflammatory change seen in <strong>the</strong> bronchi <strong>and</strong>235<strong>the</strong> quantity <strong>and</strong> nature <strong>of</strong> <strong>the</strong> sputa; in manycases <strong>the</strong>re was a complete absence <strong>of</strong> sputum.PATHOGENESIS OF ATELECTATIC BRONCHIECTASISThe following features, which are characteristic <strong>of</strong>atelectatic <strong>bronchiectasis</strong> <strong>and</strong> not <strong>of</strong> o<strong>the</strong>r forms <strong>of</strong><strong>the</strong> disease, suggest how atelectatic <strong>bronchiectasis</strong>may arise: (1) <strong>the</strong> generalized distribution <strong>of</strong>collapse <strong>and</strong> <strong>bronchiectasis</strong> in <strong>the</strong> lobes; (2) <strong>the</strong>absence <strong>of</strong> central or peripheral bronchial obstructionin <strong>the</strong> lobes at <strong>the</strong> time <strong>of</strong> operation; (3) <strong>the</strong>presence <strong>of</strong> tuberculous foci in some lobes <strong>and</strong>hilar lymph-gl<strong>and</strong>s; (4) <strong>the</strong> frequency <strong>of</strong> involvement<strong>of</strong> <strong>the</strong> right middle lobe, ei<strong>the</strong>r alone or with<strong>the</strong> lower lobe; (5) <strong>the</strong> variability <strong>of</strong> bronchialchanges, <strong>and</strong> <strong>the</strong> absence <strong>of</strong> inflammation in <strong>the</strong>collapsed parenchyma; (6) <strong>the</strong> absence <strong>of</strong> fingerclubbing, sinus infections, <strong>and</strong> foul sputum inmany patients.The <strong>bronchiectasis</strong> must ei<strong>the</strong>r be <strong>the</strong> cause, or<strong>the</strong> result, <strong>of</strong> collapse. If collapse were secondaryto <strong>bronchiectasis</strong> one would expect <strong>the</strong> segmentaldistribution <strong>of</strong> <strong>the</strong> lesions, <strong>and</strong> <strong>the</strong>ir histology, tobe <strong>the</strong> same as in aerated forms <strong>of</strong> <strong>the</strong> disease.This was not so, so <strong>the</strong> collapse is probably<strong>the</strong> primary condition. There were a few exceptionsto this generalization; <strong>the</strong>y may have beensecondarily-collapsed follicular bronchiectases.If <strong>the</strong> <strong>the</strong>ory that collapse is caused by peripheralbronchial obstruction is accepted, in <strong>the</strong>se casesone is forced to conclude that simultaneous obstructionsoccurred in all peripheral bronchi; o<strong>the</strong>rwise<strong>the</strong> <strong>bronchiectasis</strong> could not affect all branches,<strong>and</strong> collateral air circulation would prevent alveolarcollapse. The improbability <strong>of</strong> such an occurrence,<strong>and</strong> <strong>the</strong> complete absence <strong>of</strong> peripheral obstructioni most <strong>of</strong> <strong>the</strong> specimens, suggests that <strong>the</strong>re is nosound basis for this <strong>the</strong>ory.There is far more evidence supporting <strong>the</strong> viewthat collapse is caused by obstruction <strong>of</strong> lobarbronchi. Although no obstructive lesions <strong>of</strong> <strong>the</strong>proximal bronchi were found in <strong>the</strong>se specimens, orseen in pre-operative bronchograms, <strong>the</strong> frequentfinding <strong>of</strong> enlarged, fibrotic, or caseous hilar lymphgl<strong>and</strong>ssuggests that collapse arose from occlusionby <strong>the</strong>se gl<strong>and</strong>s <strong>of</strong> <strong>the</strong> lobar bronchi. This <strong>the</strong>oryreceives fur<strong>the</strong>r support from <strong>the</strong> high incidence <strong>of</strong>right middle lobe specimens in atelectatic <strong>bronchiectasis</strong>,for Brock (1946) has demonstrated <strong>the</strong>peculiar vulnerability <strong>of</strong> <strong>the</strong> middle lobe bronchusto compression from enlargement <strong>of</strong> <strong>the</strong> surroundinglymph gl<strong>and</strong>s.Recently Brock (1950) has described suppurativechanges, <strong>bronchiectasis</strong>, <strong>and</strong> collapse in middlelobes as a sequel to tuberculous hilar adenitis. He
236F. WHITWELLstates that in some cases this gl<strong>and</strong>ular enlargementmay be non-tuberculous, <strong>and</strong> that similar changesmay occur in o<strong>the</strong>r lobes. Specimens in this groupwere not examined for calcified foci radiologically,but <strong>the</strong>y were dissected carefully <strong>and</strong> all hilarlymph gl<strong>and</strong>s were examined.Some specimens in this group showed absorptioncollapse without <strong>bronchiectasis</strong>. In <strong>the</strong>se lobes <strong>the</strong>bronchi were collapsed with <strong>the</strong>ir walls in apposition,<strong>and</strong> no irreversible histological changes werepresent, ei<strong>the</strong>r in <strong>the</strong> bronchi or alveoli.It is thought that this is similar to <strong>the</strong> state <strong>of</strong> alobe when its hilar bronchus had been occludedby lymph gl<strong>and</strong> enlargement. When <strong>the</strong>se gl<strong>and</strong>sshrink <strong>the</strong> lobar bronchus becomes patent <strong>and</strong> aircan again enter <strong>the</strong> bronchial tree. In many casesthis is followed by aeration <strong>of</strong> <strong>the</strong> collapsed alveoli<strong>and</strong> <strong>the</strong> restoration <strong>of</strong> <strong>the</strong> lobe to normal, but ifsevere inflammatory changes have occurred in <strong>the</strong>bronchi, or if fibrosis has taken place in <strong>the</strong> parenchyma,<strong>the</strong> lobe is unable to exp<strong>and</strong> again. Insuch a case (Fig. 35), permanently collapsed alveolisurround aerated bronchi, which dilate because <strong>of</strong>*destruction <strong>of</strong> <strong>the</strong>ir supporting tissues <strong>and</strong> accumulation<strong>of</strong> bronchial secretions. The slight reductionin intra-pleural pressure, which might occur aftercollapse <strong>of</strong> a middle lobe, could exert little dilatingforce on its bronchi.Bronchial dilatation in <strong>the</strong>se cases may beexplained on mechanical grounds without <strong>the</strong>necessity <strong>of</strong> <strong>the</strong>re being severe inflammatorychanges, though <strong>the</strong> initial cause <strong>of</strong> <strong>the</strong> hilarlymphadenopathy is usually inflammatory. Theabsence <strong>of</strong> finger clubbing, sinus infections, <strong>and</strong>purulent sputum in many <strong>of</strong> this group <strong>of</strong> patientssupports this <strong>the</strong>ory <strong>of</strong> a mechanical disorder.DISCUSSIONAlthough in this investigation a great variety <strong>of</strong>bronchiectatic lesions has been found, <strong>the</strong> accounthas been limited to a. description <strong>of</strong> three commonforms which were seen in operation specimens. Inno instance could <strong>the</strong> bronchial dilatation havebeen considered to be reversible; it was always <strong>the</strong>result <strong>of</strong> destructive inflammatory processes, permanentalveolar collapse, or abnormal developmentresulting in bronchi <strong>of</strong> wide calibre.Follicular <strong>and</strong> saccular <strong>bronchiectasis</strong> havedistinctive lesions <strong>and</strong> natural histories. Atelectatic<strong>bronchiectasis</strong> is a less specific <strong>and</strong> largely amechanical disorder, which usually follows occlusionby hilar adenitis <strong>of</strong> a lobar brorchus. The causes<strong>of</strong> lymphadenopathy are not restricted to anyperiod <strong>of</strong> life, nei<strong>the</strong>r are <strong>the</strong> specimens frompatients <strong>of</strong> any particular age, though <strong>the</strong>y aremostly from young children. It is natural that <strong>the</strong>hilar adenitis seen in follicular <strong>bronchiectasis</strong>should, in some instances, produce total obstruction<strong>of</strong> lobar bronchi, <strong>and</strong> result in specimens whichshow a mixture <strong>of</strong> follicular <strong>and</strong> atelectatic lesions.All <strong>the</strong>se lesions have been described previouslyon many occasions, but in <strong>the</strong> literature <strong>the</strong>y haveusually been regarded as variations in a singledisease entity. it is not intended to review thisliterature; excellent summaries can be found in<strong>the</strong> works <strong>of</strong> Ewart (1900), Ballon, Singer, <strong>and</strong>Graham (1931), Ogilvie (1941), <strong>and</strong> Lisa <strong>and</strong>Rosenblatt (1943). It is sufficient to remark thatonly three accounts appear to be inconsistent with<strong>the</strong> present <strong>study</strong>. L<strong>and</strong>er <strong>and</strong> Davidson (1938),reporting on 140 operation specimens, found littledestruction <strong>of</strong> bronchial wall structures, <strong>and</strong> inmany cases only slight indications <strong>of</strong> inflammation.Specimens such as <strong>the</strong>se were extremely rare in <strong>the</strong>present series; <strong>the</strong>y were not considered to be true<strong>bronchiectasis</strong>, <strong>and</strong> <strong>the</strong>ir removal had been dueto misinterpretation <strong>of</strong> radiological <strong>and</strong> clinicalfeatures. Lisa <strong>and</strong> Rosenblatt (1943), reporting on110 post-mortem specimens, remarked that <strong>the</strong>bronchial elastic tissues were relatively unimpaired.In <strong>the</strong> present <strong>study</strong> one <strong>of</strong> <strong>the</strong> earliest <strong>and</strong> mostconstant features <strong>of</strong> affected bronchi <strong>and</strong> bronchioleshas been <strong>the</strong> destruction <strong>of</strong> elastic tissue. Moore,Kobernick, <strong>and</strong> Wiglesworth (1949) have statedthat <strong>the</strong>re is little correlation between <strong>the</strong> bronchographicappearances <strong>of</strong> a lobe <strong>and</strong> <strong>the</strong> condition <strong>of</strong><strong>the</strong> bronchi; in fact, <strong>the</strong>ir work suggests thatsegmental resections can be <strong>of</strong> little value. Theopposite conclusion has been reached from <strong>the</strong>present <strong>study</strong>.Literature on <strong>the</strong> <strong>pathogenesis</strong> <strong>of</strong> <strong>bronchiectasis</strong>is even more voluminous than that on its <strong>pathology</strong>;<strong>and</strong> it is much more confusing. One reason is,perhaps, that many <strong>the</strong>ories are based on <strong>pathology</strong>which is inferred ra<strong>the</strong>r than observed. For example,similar radiological appearances are described ascollapse, fibrosis, <strong>and</strong> pneumonia, by differentwriters who deduce that <strong>the</strong>se various conditionsare <strong>the</strong> cause <strong>of</strong> <strong>bronchiectasis</strong>. Ano<strong>the</strong>r source<strong>of</strong> confusion is <strong>the</strong> vague use <strong>of</strong> <strong>the</strong> word " <strong>bronchiectasis</strong>."For example, it is used in describingsome histological findings in fatal cases <strong>of</strong> pneumonia(Opie, 1928; McNeil et al., 1929), <strong>the</strong> gross lesionsproduced in animals by experimental methods(Weinberg, 1937; Tannenberg <strong>and</strong> Pinner, 1942),<strong>and</strong> <strong>the</strong> temporary bronchographic changes foundin 90% <strong>of</strong> university students who suffer fromrecurrent bronchitis (Ochsner, 1930). From studiesin similar ra<strong>the</strong>r restricted fields many writers have
PATHOLOGY AND PATHOGENESIS OF BRONCHIECTASIS237generalized about <strong>the</strong> <strong>pathogenesis</strong> <strong>of</strong> clinical<strong>bronchiectasis</strong>.Fortunately, <strong>the</strong> number <strong>of</strong> <strong>the</strong>ories <strong>of</strong> <strong>pathogenesis</strong>is limited; in fact, apart from <strong>the</strong> possibleinfluence <strong>of</strong> allergy <strong>and</strong> sinus infections, no new<strong>the</strong>ory has been propounded in <strong>the</strong> last hundredyears. Nearly all writers are agreed that normalbronchi do not dilate when subjected to variousmechanical stresses, <strong>and</strong> most <strong>the</strong>ories accept aprimary basis <strong>of</strong> bronchial weakness, due ei<strong>the</strong>r toinflammation or developmental defects.Developmental abnormalities <strong>and</strong> <strong>the</strong> mostcommonly suggested secondary causes <strong>of</strong> dilatationare discussed below.DEVELOPMENTAL ABNORMALITIESAbout 10% <strong>of</strong> <strong>the</strong> specimens were examples <strong>of</strong>congenital cystic lung, which is a developmentalabnormality. In five o<strong>the</strong>r specimens <strong>the</strong> bronchiwere thin-walled, <strong>and</strong> <strong>the</strong> calibre <strong>of</strong> <strong>the</strong> smallbranches was unduly wide, <strong>of</strong>ten, indeed, muchwider than <strong>the</strong> proximal bronchi. No inflammatory,fibrotic, or destructive lesions were present, <strong>and</strong> <strong>the</strong>parenchyma was entirely normal. In three <strong>of</strong> <strong>the</strong>sespecimens, however, <strong>the</strong> bronchial supportingtissues seemed to be underdeveloped. The widecalibre appeared to be <strong>the</strong>ir natural condition <strong>and</strong>not due to dilatation.Apart from <strong>the</strong>se few specimens no evidence wasfound <strong>of</strong> any developmental abnormalities; norwas it necessary to postulate any such defects inorder to explain <strong>the</strong> <strong>bronchiectasis</strong>.PRESSURE OF SECRETION IN BRONCHIThis <strong>the</strong>ory, <strong>and</strong> <strong>the</strong> objections to it, have beendiscussed on page 232. The terminal dilatationsin saccular <strong>bronchiectasis</strong> probably result fromdistension <strong>of</strong> weakened bronchi by <strong>the</strong>ir containedsecretions. The same mechanism may account formany <strong>of</strong> <strong>the</strong> dilatations <strong>of</strong> follicular <strong>and</strong> atelectatic<strong>bronchiectasis</strong>, though this is more difficult tosubstantiate.FIBROSISThe usual <strong>the</strong>ory supposes that bronchi becomedilated by <strong>the</strong> contraction <strong>of</strong> b<strong>and</strong>s <strong>of</strong> fibroustissue running between <strong>the</strong>m, but no such arrangement<strong>of</strong> fibrous tissue was seen in <strong>the</strong> specimens.Fibrosis occurred as a thickening <strong>of</strong> <strong>the</strong> normalfibrous structures in <strong>the</strong> peribronchial, perivascular,interlobular, <strong>and</strong> pleural connective tissues. Occasionallyconcentric fibrosis was seen in <strong>the</strong> walls <strong>of</strong>diseased bronchi, <strong>and</strong> it was always present in <strong>the</strong>walls <strong>of</strong> saccules. Inter-alveolar fibrosis wasQfound in some areas <strong>of</strong> chronic interstitial pneumonia,<strong>and</strong> in absorption collapse.In most forms <strong>of</strong> <strong>bronchiectasis</strong> fibrosis is a latedevelopment. It is <strong>the</strong> stretching <strong>of</strong> fibrous bronchialwalls in saccular <strong>bronchiectasis</strong> that leads todilatation; it is <strong>the</strong> parenchymal fibrosis <strong>of</strong>atelectatic <strong>bronchiectasis</strong> which prevents re-aeration.BRONCHO-PULMONARY EXCAVATIONIn a few lobes <strong>the</strong> dilatations appeared to bere-epi<strong>the</strong>lialized abscess cavities, which had originatedin <strong>the</strong> parenchyma. However, <strong>the</strong>se lesionswere uncommon <strong>and</strong> not seen in <strong>the</strong> three types<strong>of</strong> <strong>bronchiectasis</strong> described.PERIPHERAL BRONCHIAL OBSTRUCTION ANDALVEOLAR ABSORPTION COLLAPSEThese two lesions are linked in most recentdiscussion on <strong>pathogenesis</strong> (Warner <strong>and</strong> Graham,1933; Boyd, 1935; Andrus, 1937, 1940; L<strong>and</strong>er<strong>and</strong> Davidson, 1938; Fleischner, 1940; L<strong>and</strong>er,1946; Coope, 1948). It is argued that collapsefollows obstruction, <strong>and</strong> dilatation occurs inbronchi proximal to <strong>the</strong> obstruction. These bronchiare subjected to a great dilating stress, which iscaused by <strong>the</strong> difference in pressure between <strong>the</strong>pleural space <strong>and</strong> <strong>the</strong> atmosphere in <strong>the</strong> bronchi.From <strong>the</strong> present <strong>study</strong> <strong>the</strong>re appears to be nosound basis for this <strong>the</strong>ory. Obstruction <strong>of</strong> peripheralbronchi was always present in follicular <strong>and</strong>saccular <strong>bronchiectasis</strong>, but absorption collapsewas absent, probably because <strong>of</strong> adequate collateralair circulation. Absorption collapse was found in10% <strong>of</strong> <strong>the</strong> specimens but it affected whole lobes,not lobules or segments. No peripheral bronchialor bronchiolar obstruction was present in <strong>the</strong>selobes, <strong>and</strong> <strong>the</strong> collapse had probably been causedby proximal bronchial obstruction.Many o<strong>the</strong>r arguments can be raised against this<strong>the</strong>ory. In cases where only a few small bronchiin one segment are affected <strong>the</strong>re could be nosignificant alteration <strong>of</strong> pleural pressure to create adilating force, even if collapse occurred distal to<strong>the</strong> <strong>bronchiectasis</strong>. The absence <strong>of</strong> radiologicalcollapse in many cases has been explained in manyunconvincing ways. Andrus (1940) states thatpatchy collapse is diagnosed as pneumonia, thatcollapse is concealed by <strong>the</strong> heart shadow, <strong>and</strong> thatcollapse may cause lung injury " <strong>and</strong> <strong>the</strong>n bedissipated." Perry <strong>and</strong> King (1940) think thatcollapse can "lie dormant" for many years untilpurulent bronchitis supervenes. These reasons for<strong>the</strong> absence <strong>of</strong> radiological collapse, even if accepted,do not explain <strong>the</strong> normal aeration <strong>of</strong> so many
2)38F. WHITWELLTABLE IIIPATHOLOGY OF BRONCHIECTASISFollicular I Saccular Atelectatic84% left-sided 72% left-sided 36% left-sidedIso'ated bronchi affected Isolated bronchi affected All bronchi involvedChronic inflammatory changes in bronchi Chronic inflammatory changes in bronchi Variable degree <strong>of</strong> inflammatory change,<strong>and</strong> bronchioles, with formation <strong>of</strong> lymph <strong>and</strong> saccules, no lymph follicle formation lymph follicles sometimes seenfolliclesDestruction <strong>of</strong> elastic tissue <strong>and</strong> muscle, some Little destruction <strong>of</strong> supporting tissues except Variable amount <strong>of</strong> destruction, sometimesdestruction <strong>of</strong> cartilage <strong>and</strong> mucous gl<strong>and</strong>s within saccules, where none remain very littleBronchial epi<strong>the</strong>lium intact <strong>and</strong> smooth, Bronchial epi<strong>the</strong>lium intact but polypoid. Bronchial epi<strong>the</strong>lium usually intact <strong>and</strong>small ulcerations in bronchioles. No Some ulcerations in saccules <strong>and</strong> promi- smooth. Few ulcerations, no squamoussquamous metaplasia nent squamous metaplasia metaplasiaBronchio'es narrowed or obliterated Bronchioles obliterated Bronchioles patentAlveoli mostly well aerated, but some inter- Alveoli well aerated, no chronic interstitial Marked alveolar collapse, uniform throughstitialpneumonia around affected bronchi pneumonia. Some compression collapse out lobe. Little inflammatory change in<strong>and</strong> bronchioles. Some compression around saccules collapsed alveoli, but some fibrosiscollapse around areas <strong>of</strong> pneumoniaClinical FindingsAge at onset <strong>of</strong> symptomsDuration <strong>of</strong> symptomsAge at time <strong>of</strong> operationIllness at onset <strong>of</strong> symptomsBronchogramsNasal sinus involvementClubbing__TABLE IVCLINICAL ASPECTS OF DIFFERENT TYPES OF BRONCHIECTASISFollicularSaccular53% under 3 yrs. 78% under 7 25% complained <strong>of</strong> symptoms allyrs. <strong>the</strong>ir lives. 70% began symptomsbetween 13 <strong>and</strong> 25 yrs.1-15 yrs. 50% for 1-5 yrs. 2-20yrs. 50%for2-6yrs.Mainly 6-11 yrs. old, with gradual None under 15 yrs., mostly bedecreaseup to 20 yrs. None tween 15 <strong>and</strong> 25 yrs., with a fewover 20 yrs.cases in older groups~~~~~IVague onset in 25%. Measles <strong>and</strong>y Vague onset in 45% (includingor whooping-cough in 45%. 25% who had symptoms allPrimary bronchopneumonia in <strong>the</strong>ir lives). Unspecified pneumoniain 56%. No association20%with measles or whooping-coughI _ .1Usually cylindrical, sometimes SaccularatelectaticOver 70%Under 50%Over 70()75%1-Atelectatic20% under 3 yrs. 70, under 7yrs.1-15 yrs. 33% for 1-3 yrs.Mostly between 5 <strong>and</strong> 10 yrs.,but no sudden fall-<strong>of</strong>f <strong>of</strong> olderpatientsVague onset rare. Measles orwhooping-cough in 50%/; primarybronchopneumonia in 25%AtelectaticInfrequentInfrequentoperation specimens, such as has been seen in <strong>the</strong>present series, <strong>and</strong> which has frequently beendescribed in <strong>the</strong> literature.SUMMARYThe investigation has consisted <strong>of</strong> <strong>the</strong> examination<strong>of</strong> 200 consecutively removed bronchiectatic lungs<strong>and</strong> lobes. Methods used consisted <strong>of</strong> neopreneinjection casts <strong>of</strong> bronchial trees, large histologicalsections <strong>of</strong> entire lobes, <strong>and</strong> detailed dissections <strong>of</strong>bronchial trees with histological examinations <strong>of</strong>selected areas.The lobar, segmental, <strong>and</strong> intra-segmental distribution<strong>of</strong> <strong>the</strong> lesions have been described (seeTables I <strong>and</strong> 11, <strong>and</strong> Fig. 10).More than half <strong>the</strong> specimens belonged to oneor o<strong>the</strong>r <strong>of</strong> three ra<strong>the</strong>r distinctive types <strong>of</strong> <strong>bronchiectasis</strong>,which have been called follicular,saccular, <strong>and</strong> atelectatic <strong>bronchiectasis</strong>, <strong>and</strong> <strong>the</strong>ir<strong>pathology</strong>, clinical features, <strong>and</strong> <strong>pathogenesis</strong> hasbeen discussed (see Figs. 21, 30, <strong>and</strong> 35, <strong>and</strong>Tables I II <strong>and</strong> IV).Finally, current <strong>the</strong>ories <strong>of</strong> <strong>pathogenesis</strong> havebeen criticized in <strong>the</strong> light <strong>of</strong> <strong>the</strong> present enquiry.This work has been only made possible through <strong>the</strong>co-operation <strong>of</strong> <strong>the</strong> staff <strong>of</strong> <strong>the</strong> Surgical Chest Centre,Broadgreen Hospital. In addition I would like to thankMr. H. Morriston Davies, Mr. F. R. Edwards, <strong>and</strong> Dr.Robert Coope for many valuable discussions on medical<strong>and</strong> surgical aspects <strong>of</strong> <strong>bronchiectasis</strong>. I wish also toacknowledge my indebtedness to Dr. Rachel M. Rawcliffefor her assistance in <strong>the</strong> preparation <strong>of</strong> neoprenecasts <strong>and</strong> in <strong>the</strong> tabulation <strong>of</strong> case-records, <strong>and</strong> toDr. P. J. Taylor for correction <strong>of</strong> <strong>the</strong> MS.
PATHOLOGY AND PATHOGENESIS OF BRONCHIECTASIS239REFERENCESAllison, P. R., Gordon, J., <strong>and</strong> Zinnemann, K. (1943). J. Path. Ba t.,55, 465.Andrus, P. M. (1937). Amer. Rev. Tuberc., 36, 46.(1940). Ibid., 41, 87.Baarsma, P. R., <strong>and</strong> Dirken, M. N. J. (1948). J. thorac. Surg., 17,238.- <strong>and</strong> Huizinga, E. (1948). Ibid., 17, 252.Ballon; H., Singer, J. J., <strong>and</strong> Graham, E. A. (1931). Ibid., 1, 154.Boyd, G. L. (1935). J. Amer. med Ass., 105, 1832.Brock, R. C. (1946). The Anatomy <strong>of</strong> <strong>the</strong> Bronchial Tree. London.-(1950). Thorax, 5, 5.Broman, 1. (1923). Anat. Anz., 57, Suppl. (Verh. anat. Ges.), p. 83.Quoted by Engel.Churchill, E. D. (1949). J. thorac. Surg., 18, 279.-<strong>and</strong> Belsey, R. (1939). Ann. Surg., 109, 481.Coope, R. (1948). Diseases <strong>of</strong> <strong>the</strong> Chest, 2nd ed. Edinburgh.Cruikshank, A. H. (1948). J. Path. Bact., 60, 520.Engel, S. (1947). The Child's Lung. London.Erb, I. H. (1933). Arch. Path., 15, 357.Ewart. W. (1900), Allbutt <strong>and</strong> Rolleston's System <strong>of</strong> Medicine, 2nded., vol. 5, p. 127 seq. London.Fleischner, F. (1940). Amer. Rev. Tuberc., 42, 297.Jackson, C., <strong>and</strong> Jackson, C. L. (1932). J. Amer med. Ass., 99, 1747.Laennec, R. T. H. (1819). Dc L'Auscultation Mediate. Paris.L<strong>and</strong>er, F. P. L. (1946). Thorax, 1, 198.<strong>and</strong> Davidson, M. (1938). Brit. J. Radiol., 11, 65.Lisa, J. R., <strong>and</strong> Rosenblatt, M. B. (1943). Bronchiectasis. London.MacCallum, W. G. (1940). Textbook <strong>of</strong> Pathology, 7th ed. Philadelphia.McNeil, C., Macgregor, A. R., <strong>and</strong> Alex<strong>and</strong>er, W. A. (1929). Arch.Dis. Childh., 4, 170.Mallory, T. B. (1947). New Engi. J. Med., 237, 795.Maximow, A. A., <strong>and</strong> Bloom, W. (1942). Textbook <strong>of</strong> Histology,4th ed. Philadelphia.Miller, W. S. (1947). The Lung, 2nd ed. Springfield, Illinois.Moore, J. R., Kobernick, S. D., <strong>and</strong> Wiglesworth, F. W. (1949).Suirg. Gynec. Obstet., 89, 145.Nelson, J. B. (1946). J. exp. Med., 84, 7 <strong>and</strong> 15.Ochsner, A. (1930). Amer. J. med. Sci., 179, 388.Ogilvie, A. G. (1941). Arch. intern. Med., 68, 395.Opie, E. L. (1928). Arch. Path., Chwago, 5, 285.Overholt, R. H., Betts, R. H., <strong>and</strong> tods F. M. (1947). Dir. Chest,13, 583.Peroni A. (1934). Arch. Otolaryng., 19, 1. Quoted by Samson.Perry, K. M. A., <strong>and</strong> King, D. S. (1940). Amer. Rev. Tuberc., 41,531.Reid, L. McA. (1950). Thorax, 5, 233.Riviere, C. (1905). St. Bart's Hosp. Rep., 41, 123.Robinson, W. L. (1933). Brit. J. Surg., 21, 302.(1939). Amer. J. Path., 15, 638.Samson, P. C. (1940). J. thorac. Surg., 9, 679.Schmidt, H. W. (1947). Ann. Otol., St. Louis, 56, 793.Tannenberg, J., <strong>and</strong> Pinner, M. (1942). J. thorac. Surg., 11, 571.Van Allen, C. M., <strong>and</strong> Jung, T. S. (1931). Ibid., 1, 3.Warner, W. P., <strong>and</strong> Graham, D. (1933). Arch. intern. Med., 52, 888.Watts, C. F., <strong>and</strong> McDonald, J. R. (1948). Arch. Path., Chicago,45, 742.Weinberg, J. (1937). J. thorac. Surg., 6, 402.Williams, C. J. B. (1838). Lond. med. Gaz., n.s. 1, 913.Willis, R. A. (1 948). Pathology <strong>of</strong> Tumours. London.













