232F. WHlTWELLNeoprene casts, reconstruction models, <strong>and</strong>dissections <strong>of</strong> <strong>the</strong> bronchial tree show that sacculesare <strong>the</strong> bulbous terminations <strong>of</strong> <strong>the</strong> first to thirdbranchings <strong>of</strong> <strong>the</strong> segmental bronchi. As adultbronchioles arise only after about 18 branchingsfrom <strong>the</strong> segmental bronchi (Broman, 1923; Reid,1950). <strong>the</strong> saccules clearly cannot be <strong>of</strong> bronchiolarorigin.Saccules are <strong>the</strong> direct continuations <strong>of</strong> largebronchi, <strong>the</strong>y are encased within extension <strong>of</strong>'<strong>the</strong>peribronchial fibrous septa, <strong>and</strong> <strong>the</strong>y are placedclose to <strong>and</strong> parallel with branches <strong>of</strong> pulmonaryarteries. Their situation suggests that <strong>the</strong>y wereoriginally bronch:, <strong>and</strong> not bronchopulmonaryexcavations.CAUSE OF DILATATION. First, it is possible toeliminate certain <strong>of</strong> <strong>the</strong> factors that are <strong>of</strong>tensuggested as causes <strong>of</strong> dilatation. Alveolar collapseis negligible in <strong>the</strong>se specimens <strong>and</strong> cannot beconsidered as a possible cause, in spite <strong>of</strong> absoluteperipheral bronchial obstruction. Fibrous tissuefound in <strong>the</strong> saccular walls occurs only as a replacement<strong>of</strong> original bronchial structures. This fibrosisis concentric with <strong>the</strong> saccules, <strong>and</strong> not in a planewhere, by contracting, it could exert any dilatingforce on <strong>the</strong> bronchi. Most writers link toge<strong>the</strong>rfibrosis <strong>and</strong> contraction, especially when discussing<strong>bronchiectasis</strong>. However, <strong>the</strong> behaviour <strong>of</strong> fibroustissue is perverse, <strong>and</strong> many examnples occur <strong>of</strong> itsproperty <strong>of</strong> ungoverned stretching, e.g., aorticaneurysms <strong>and</strong> in repaired hernias. Probably <strong>the</strong>stretching <strong>of</strong> fibrous tissue in saccular walls is afactor in <strong>the</strong> production <strong>of</strong> dilatation.The clinical findings <strong>of</strong> this group <strong>of</strong> patientsshow that while in many cases <strong>the</strong> <strong>bronchiectasis</strong>dated from an attack <strong>of</strong> bronchopneumonia, innearly half <strong>the</strong> patients <strong>the</strong> disease had an insidiousonset which escaped notice.It is considered that saccular <strong>bronchiectasis</strong>begins as a chronic mural inflammation <strong>of</strong> <strong>the</strong>medium-sized bronchi. This condition destroysbronchial wall structures <strong>and</strong> obliterates peripheralbranches (Fig. 30), but is not sufficiently acute ordiffuse to produce parenchymal scarring or tointerfere with <strong>the</strong> establishment <strong>of</strong> a collateral air.circulation, provided all segments <strong>of</strong> a lobe arenot affected.The saccular shape <strong>of</strong> <strong>the</strong> diseased brolnchi isprobably produced after <strong>the</strong> destruction <strong>of</strong> supportingtissues <strong>and</strong> occlusion <strong>of</strong> peripheral branches,<strong>and</strong> results from distension by contained pus, <strong>the</strong>pressure <strong>of</strong> which is increased by <strong>the</strong> partial occlusion<strong>of</strong> pre-saccular bronchi (see Fig. 28). Support islent to this <strong>the</strong>ory by <strong>the</strong> compression-collapseseen in several specimens in perisaccular alveoli(Fig. 29) suggesting that an expansile force iscentred within <strong>the</strong> saccules.The <strong>the</strong>ory that dilatation is produced throughdistension <strong>of</strong> <strong>the</strong> bronchi by pus was originally putforward by Laennec, but only a few (Riviere, 1905)have shared his opinion. As early as 1838 Williamsdiscredited Laennec's <strong>the</strong>ory by arguing that mostpatients with copious sputum do not developdilatation, <strong>and</strong> many patients with <strong>bronchiectasis</strong>have little sputum. Williams's argument was falsebecause it did not take into account <strong>the</strong> condition<strong>of</strong> <strong>the</strong> bronchial walls. Andrus (1937) discussedthis subject <strong>and</strong> said:" As a problem in physics it is sufficient to noteat this time that in order to exert a dilating force itwould be necessary that <strong>the</strong> secretion occupy <strong>the</strong> grosssection <strong>of</strong> <strong>the</strong> lumen <strong>of</strong> <strong>the</strong> bronchus; such a conditionwould, however, necessarily result in atelectasis,<strong>and</strong> its possible effects be indistinguishable from <strong>the</strong>latter."His <strong>the</strong>oretical aerodynamics did not allow forcollateral air circulation, <strong>and</strong> <strong>the</strong> illustrated examples.do not support his statement.ATELECTATIC BRONCHIECTASISIn recent years <strong>the</strong>re have been many accounts<strong>of</strong> <strong>the</strong> association <strong>of</strong> lobar <strong>and</strong> segmental collapsewith <strong>bronchiectasis</strong>, <strong>and</strong> it has become widelyaccepted that <strong>the</strong> collapse leads to <strong>the</strong> <strong>bronchiectasis</strong>.In this condition, which has been calledatelectatic <strong>bronchiectasis</strong> (although it is recognizedto be an acquired disease), <strong>the</strong> collapse is usuallythought to be caused by peripheral bronchialobstruction. Many writers have gone even fur<strong>the</strong>r<strong>and</strong> stated that all <strong>bronchiectasis</strong>, even whencongenital, is caused in this way.The specimens which have here been classifiedas follicular <strong>and</strong> saccular rarely showed collapse,even on microscopic exa-mination; where collapsewas found it appeared to be consequent to <strong>the</strong><strong>bronchiectasis</strong>. However, some o<strong>the</strong>rs <strong>of</strong> <strong>the</strong>specimens did show severe alveolar collapse, sa<strong>the</strong>y have been examined as a group in an attemptto find out whe<strong>the</strong>r <strong>the</strong> collapse or <strong>the</strong> <strong>bronchiectasis</strong>comes first, <strong>and</strong> how this condition arises.The specimens lack homogeneity; in some <strong>the</strong>bronchi are collapsed, in o<strong>the</strong>rs <strong>the</strong>re is grossdilatation, <strong>and</strong> in most <strong>of</strong> <strong>the</strong>m <strong>the</strong> bronchi arethickened but only moderately dilated (Fig. 32).However, <strong>the</strong> grouping has been <strong>of</strong> some valuebecause it has shown that " atelectatic <strong>bronchiectasis</strong>"differs from o<strong>the</strong>r forms <strong>of</strong> <strong>the</strong> disease inits lobar <strong>and</strong> segmental distribution, <strong>and</strong> in <strong>the</strong>
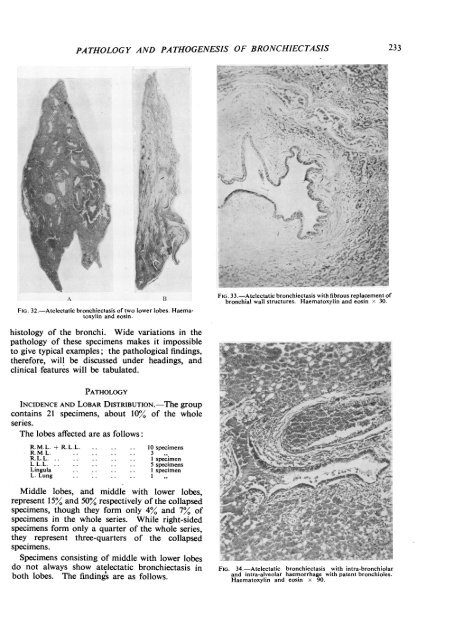
PATHOLOGY AND PATHOGENESIS OF BRONCHIECTASIS 233r-2L ~ ~~~~~ '.1 ~ ~~~~ S+. 1*2-.X~~~~~~\&"AI~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ J%--4s~'''| ~ 1.4'~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~'- '>.P'w^* wq. -1 f\0ziSl v*) FE p 1-4-0-1M#vi *ffhQ\Bs -#--pqee"4 "'" ~*specimens form only a quarter <strong>of</strong> <strong>the</strong> whole series,'<strong>the</strong>y represent three-quarters <strong>of</strong> <strong>the</strong> collapsed tspecimens.*Specimens consisting <strong>of</strong> middle with lower lobes 5 .'-^ . ;>r *-3 ido not always show atelectatic <strong>bronchiectasis</strong> in FIG. 34.-Atelectatic <strong>bronchiectasis</strong> with intra-bronchiolarboth lobes. The findings are as follows. <strong>and</strong> intra-alveolar haemorrhage with patent bronchioles..... -..- I I --.