- Page 1:
KEY NOTES ON Plastic Surgery ADRIAN
- Page 4 and 5:
© 2002 by Blackwell Science Ltd a
- Page 7 and 8:
Foreword I am particularly critical
- Page 9 and 10:
Abbreviations ABPI ankle brachial p
- Page 11 and 12:
ABBREVIATIONS ix LME line of maximu
- Page 13 and 14:
1 General principles Structure and
- Page 15 and 16:
Collagen fibres STRUCTURE AND FUNCT
- Page 17 and 18:
BLOOD SUPPLY TO THE SKIN 5 Vascular
- Page 19 and 20:
Neural innervation BLOOD SUPPLY TO
- Page 21 and 22:
CLASSIFICATION OF FLAPS 9 Circulati
- Page 23 and 24:
CLASSIFICATION OF FLAPS 11 • Exam
- Page 25 and 26:
GEOMETRY OF LOCAL FLAPS 13 • Borg
- Page 27 and 28:
The five-flap plasty GEOMETRY OF LO
- Page 29 and 30:
V-Y GEOMETRY OF LOCAL FLAPS 17 •
- Page 31 and 32:
The rhomboid flap The rhomboid flap
- Page 33 and 34:
WOUND HEALING AND SKIN GRAFTS 21 Wo
- Page 35 and 36:
Collagen WOUND HEALING AND SKIN GRA
- Page 37 and 38:
WOUND HEALING AND SKIN GRAFTS 25
- Page 39 and 40:
WOUND HEALING AND SKIN GRAFTS 27
- Page 41 and 42:
• Cortical bone consists of: BONE
- Page 43 and 44:
Intrinsic graft factors NERVE HEALI
- Page 45 and 46:
• First-degree injury NERVE HEALI
- Page 47 and 48:
TENDON HEALING 35 • Graft lengths
- Page 49 and 50:
Inflammation TENDON HEALING 37 •
- Page 51 and 52:
Active flexion • This results in
- Page 53 and 54:
ALLOPLASTIC IMPLANTATION 41 • Dis
- Page 55 and 56:
ALLOPLASTIC IMPLANTATION 43 • It
- Page 57 and 58:
Methylmethacrylate ALLOPLASTIC IMPL
- Page 59 and 60:
SUTURES AND SUTURING 47 • They ar
- Page 61 and 62:
Intradermal skin suturing SUTURES A
- Page 63 and 64:
Polydioxanone TISSUE EXPANSION 51
- Page 65 and 66:
• In the vicinity of an immature
- Page 67 and 68:
FURTHER READING 55 Jackson IT. Loca
- Page 69 and 70:
Actinic keratosis BENIGN NON- PIGME
- Page 71 and 72:
BENIGN NON- PIGMENTED SKIN LESIONS
- Page 73 and 74:
BENIGN PIGMENTED SKIN LESIONS 61
- Page 75 and 76:
Junctional naevi BENIGN PIGMENTED S
- Page 77 and 78:
Naevus of Ito MALIGNANT NON- PIGMEN
- Page 79 and 80:
• Infiltrative MALIGNANT NON- PIG
- Page 81 and 82:
MALIGNANT MELANOMA 69 • These tum
- Page 83 and 84:
MALIGNANT MELANOMA 71 Clark’s lev
- Page 85 and 86:
MALIGNANT MELANOMA 73 • Excision
- Page 87 and 88:
Koops et al. • J Clin Oncol 1998;
- Page 89 and 90:
Deep sarcomas Presentation SARCOMA
- Page 91 and 92:
3 The head and neck Embryology, 79
- Page 93 and 94:
CRANIOFACIAL SURGERY 81 • The lat
- Page 95 and 96:
Cleft 4 • This is also known as t
- Page 97 and 98:
CRANIOFACIAL SURGERY 85 • The loc
- Page 99 and 100:
Apert’s syndrome CRANIOFACIAL SUR
- Page 101 and 102: CRANIOFACIAL SURGERY 89 • Median
- Page 103 and 104: Orbit CRANIOFACIAL SURGERY 91 • P
- Page 105 and 106: 3 Free-tissue transfer 4 Osteotomie
- Page 107 and 108: CLEFT LIP 95 • Failure of mesench
- Page 109 and 110: Schweckendiek technique CLEFT LIP 9
- Page 111 and 112: • Advantages: • The technique i
- Page 113 and 114: CLEFT PALATE 101 • The muscle bun
- Page 115 and 116: • A: abnormal face • T: thymic
- Page 117 and 118: CLEFT PALATE 105 • The muscle sli
- Page 119 and 120: HEAD AND NECK CANCER 107 • N3: a
- Page 121 and 122: Comprehensive neck dissection HEAD
- Page 123 and 124: • Of these, the complications may
- Page 125 and 126: • Larynx • Trachea and upper br
- Page 127 and 128: Mucoepidermoid carcinoma HEAD AND N
- Page 129 and 130: HEAD AND NECK CANCER 117 • The co
- Page 131 and 132: Treatment HEAD AND NECK CANCER 119
- Page 133 and 134: HEAD AND NECK CANCER 121 • Bony r
- Page 135 and 136: FACIAL FRACTURES AND SOFT- TISSUE I
- Page 137 and 138: FACIAL FRACTURES AND SOFT- TISSUE I
- Page 139 and 140: • Malocclusion FACIAL FRACTURES A
- Page 141 and 142: FACIAL FRACTURES AND SOFT- TISSUE I
- Page 143 and 144: • CT scanning FACIAL FRACTURES AN
- Page 145 and 146: FACIAL FRACTURES AND SOFT- TISSUE I
- Page 147 and 148: FACIAL FRACTURES AND SOFT- TISSUE I
- Page 149 and 150: FACIAL FRACTURES AND SOFT- TISSUE I
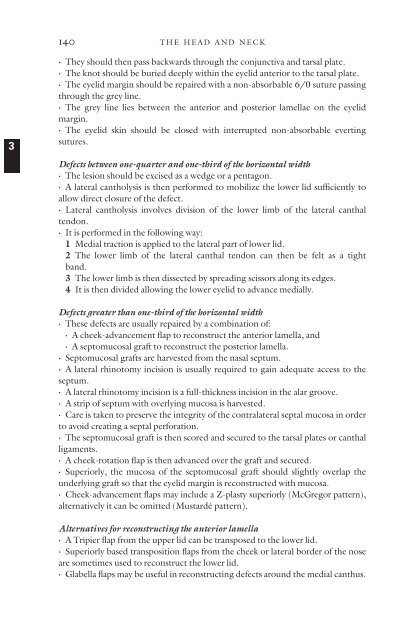
- Page 151: OCULOPLASTIC SURGERY 139 • The up
- Page 155 and 156: OCULOPLASTIC SURGERY 143 Excision o
- Page 157 and 158: • They occur in: • Patients wit
- Page 159 and 160: 5 Cervical branch FACIAL PALSY 147
- Page 161 and 162: FACIAL PALSY 149 • A strip of spe
- Page 163 and 164: • Nerve transfers FACIAL PALSY 15
- Page 165 and 166: ABNORMALITIES OF THE EAR 153 • Th
- Page 167 and 168: ABNORMALITIES OF THE EAR 155 • Th
- Page 169 and 170: ABNORMALITIES OF THE EAR 157 Specif
- Page 171 and 172: VASCULAR ABNORMALITIES 159 • The
- Page 173 and 174: Non-invasive treatments VASCULAR AB
- Page 175 and 176: VASCULAR ABNORMALITIES 163 • They
- Page 177 and 178: • It is associated with: • Meni
- Page 179 and 180: FURTHER READING 167 Spauwen PH, Goo
- Page 181 and 182: BREAST REDUCTION 169 • The anteri
- Page 183 and 184: • This technique has the followin
- Page 185 and 186: • Herniation of the NAC • Stret
- Page 187 and 188: Excisional techniques BREAST AUGMEN
- Page 189 and 190: BREAST AUGMENTATION 177 • This te
- Page 191 and 192: • Non-invasive tumours • Ductal
- Page 193 and 194: Surgical treatment BREAST CANCER 18
- Page 195 and 196: BREAST RECONSTRUCTION 183 • Lesio
- Page 197 and 198: BREAST RECONSTRUCTION 185 • Varia
- Page 199 and 200: Superior gluteal perforator flaps B
- Page 201 and 202: CHEST WALL RECONSTRUCTING 189 • E
- Page 203 and 204:
FURTHER READING 191 Pectoralis majo
- Page 205 and 206:
Embryology 5 The upper limb Embryol
- Page 207 and 208:
1 Failure of formation • Transver
- Page 209 and 210:
CONGENITAL DEFORMITIES 197 Classifi
- Page 211 and 212:
CONGENITAL DEFORMITIES 199 • Ulna
- Page 213 and 214:
Camptodactyly CONGENITAL DEFORMITIE
- Page 215 and 216:
CONGENITAL DEFORMITIES 203 • Clin
- Page 217 and 218:
• Type 2: duplicated distal phala
- Page 219 and 220:
• Microvascular free joint or bon
- Page 221 and 222:
• Abnormalities of the scalene mu
- Page 223 and 224:
NERVE COMPRESSION 211 • Tinel’s
- Page 225 and 226:
NERVE COMPRESSION 213 1 Neurolysis
- Page 227 and 228:
• Sensory signs include: • A po
- Page 229 and 230:
TENDON TRANSFERS 217 Symptoms Pain
- Page 231 and 232:
• The ideal tension varies betwee
- Page 233 and 234:
DUPUYTREN’ S DISEASE 221 • ECRB
- Page 235 and 236:
3 The lateral digital sheet 4 Grays
- Page 237 and 238:
Fat • Lipoma • Angiolipoma •
- Page 239 and 240:
Carpometacarpal boss TUMOURS 227
- Page 241 and 242:
TUMOURS 229 Giant cell tumours of t
- Page 243 and 244:
• Pseudogout • Systemic lupus e
- Page 245 and 246:
1 Proliferationasynovial swelling a
- Page 247 and 248:
• Findings on examination include
- Page 249 and 250:
ARTHRITIS 237 • The resultant imb
- Page 251 and 252:
Chronic tophaceous gout HAND INFECT
- Page 253 and 254:
4 Pain on passive extension. HAND I
- Page 255 and 256:
6 The lower limb Leg ulcers, 243 Lo
- Page 257 and 258:
• It is normally in the region of
- Page 259 and 260:
Mangled extremity severity score LO
- Page 261 and 262:
LOWER- LIMB TRAUMA 249 4 This fasci
- Page 263 and 264:
The lymphatic system Anatomy LYMPHO
- Page 265 and 266:
2Infection LYMPHOEDEMA 253 • The
- Page 267 and 268:
LYMPHOEDEMA 255 • Phase twoaconse
- Page 269 and 270:
4 Heel 5 Malleolus 6 Occiput. PRESS
- Page 271 and 272:
• Pressure dispersion PRESSURE SO
- Page 273 and 274:
FURTHER READING 261 Eshima I, Mathe
- Page 275 and 276:
Embryology of the sexual organs Int
- Page 277 and 278:
HYPOSPADIAS 265 • The tunica albu
- Page 279 and 280:
HYPOSPADIAS 267 The Mathieu procedu
- Page 281 and 282:
• The dorsal surface of the penis
- Page 283 and 284:
VAGINAL AGENESIS 271 • Patients w
- Page 285 and 286:
Thermal burns 8 Burns Thermal burns
- Page 287 and 288:
• A high respiratory rate • Con
- Page 289 and 290:
THERMAL BURNS 277 • Adults with b
- Page 291 and 292:
THERMAL BURNS 279 • Full-thicknes
- Page 293 and 294:
6Disability CHEMICAL BURNS 281 •
- Page 295 and 296:
FURTHER READING 283 • Lightning s
- Page 297 and 298:
PATHOPHYSIOLOGY OF VESSEL HEALING 2
- Page 299 and 300:
TECHNIQUE 287 Equipment Successful
- Page 301 and 302:
POST- OPERATIVE MANAGEMENT 289 Post
- Page 303 and 304:
FURTHER READING 291 Further reading
- Page 305 and 306:
BLEPHAROPLASTY 293 • This is asse
- Page 307 and 308:
BLEPHAROPLASTY 295 • The fat pads
- Page 309 and 310:
The greater auricular nerve • Thi
- Page 311 and 312:
Rhinoplasty Anatomy Skeleton The sk
- Page 313 and 314:
Techniques RHINOPLASTY 301 • Some
- Page 315 and 316:
• Sutures can be placed: LIPOSUCT
- Page 317:
FURTHER READING 305 Hamra ST. The d
- Page 320 and 321:
308 INDEX breast (cont.) screening
- Page 322 and 323:
310 INDEX interpolation flaps—19
- Page 324 and 325:
312 INDEX skin grafts—26-8 follow