County Durham Local Teenage Pregnancy Strategy - Full Document
County Durham Local Teenage Pregnancy Strategy - Full Document
County Durham Local Teenage Pregnancy Strategy - Full Document

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>County</strong> <strong>Durham</strong> <strong>Local</strong> <strong>Teenage</strong><br />
<strong>Pregnancy</strong> <strong>Strategy</strong><br />
2. Acronyms<br />
3. Executive Summary<br />
5. Background & Information<br />
Contents Page<br />
7. Part A, Section 1<br />
8. Strategic Vision<br />
8. Principles and Values<br />
9. Joined Up Action and Structures<br />
14. Consultation and Involvement of other Stakeholders<br />
15. Links to other Policies<br />
16. <strong>Strategy</strong> Goals<br />
17. Part A, Section 2<br />
18. <strong>Local</strong> Context<br />
22. <strong>Local</strong> Profile of <strong>Teenage</strong> <strong>Pregnancy</strong>, including Audit of<br />
Current Service Provision<br />
39. Part A, Section 3<br />
41. <strong>Local</strong> Media Campaign<br />
51. Better Sex & Relationships Education (SRE)<br />
65. Better Contraception and Advice Services<br />
89. Better Support for <strong>Teenage</strong> Parents<br />
103. Consultation with Young People<br />
107. Part B<br />
Annual Report, March 2000/2001<br />
111. Part C<br />
<strong>Teenage</strong> <strong>Pregnancy</strong> <strong>Local</strong> Implementation Fund<br />
113. Part D<br />
Certificate of Agreement and Partnership<br />
115. Conclusion<br />
1
Acronyms<br />
SEU Social Exclusion Unit<br />
SRE Sex & Relationships Education<br />
SHPS Specialist Health Promotion Service<br />
DFEE Department for Education & Employment<br />
SSD Social Services Department<br />
PSHE Personal, Social & Health Education<br />
PCGs Primary Care Groups<br />
2
Executive Summary<br />
• Britain has the highest rate of teenage births in Western Europe. In<br />
1998 there were around 41,000 conceptions to under 18s in England,<br />
resulting in 23,600 live births.<br />
• In June 1999 the Government produced a National <strong>Teenage</strong> <strong>Pregnancy</strong><br />
Report with two main goals:<br />
- To halve the rate of conceptions among under 18 year olds in<br />
England by 2010 and to set a downward trend in conception<br />
rates for under 16s.<br />
- To reduce long term social exclusion for teenage pregnancy<br />
and their children.<br />
• Guidance from the <strong>Teenage</strong> <strong>Pregnancy</strong> Unit stated that ten year<br />
strategies (to include three year action plans) should be produced at<br />
local authority level. The strategies must be coterminous with education<br />
and local authority boundaries. In <strong>County</strong> <strong>Durham</strong> and Darlington this<br />
has been structured thus:<br />
Two strategies have been developed. One strategy for <strong>County</strong> <strong>Durham</strong><br />
and one strategy for Darlington.<br />
• The strategies are consistent with the following principles and values as<br />
detailed in the <strong>Teenage</strong> <strong>Pregnancy</strong> Guidance:<br />
- Young people centred<br />
- Partnership working<br />
- Long term and sustainable<br />
- Addressing inequalities<br />
- Evidence based practice.<br />
• To secure partnership working a county wide Steering Group and sub<br />
groups were established for <strong>County</strong> <strong>Durham</strong> and Darlington, with<br />
representatives from Health, Education, Social Services and the<br />
Voluntary Sector.<br />
• The groups established current provision of service and developed<br />
action plans which would aim to:<br />
- Achieve the target 55% reduction in the under 18 conception<br />
rate by 2010 (the target set for <strong>County</strong> <strong>Durham</strong> and Darlington<br />
by the <strong>Teenage</strong> <strong>Pregnancy</strong> Unit) and achieve a downward<br />
trend in conceptions in under 16s.<br />
- Better Support <strong>Teenage</strong> Parents to lead active, fulfilled lives<br />
as valued citizens.<br />
3
• Particular efforts have been made to consult with young people and with<br />
stakeholders. Comments from the consultation stage have been<br />
incorporated into the strategy.<br />
• <strong>County</strong> <strong>Durham</strong> and Darlington have an indicative annual allocation of<br />
£250,000 for the next three years from the <strong>Teenage</strong> <strong>Pregnancy</strong> Unit<br />
(TPU) <strong>Local</strong> Implementation Fund to support implementation of the local<br />
action plans. It is expected by the TPU that initiatives will be mainstream<br />
funded after that.<br />
4
Background and Information<br />
Within Western Europe, the UK now stands out as having the highest rate of<br />
teenage births. The UK has teenage birth rates which are twice as high as in<br />
Germany, three times as high as in France and six times as high as in the<br />
Netherlands. 1<br />
In June 1999, the Government produced a national teenage pregnancy strategy<br />
with two goals:<br />
• To halve the rate of conceptions among under 18 year olds in<br />
England by 2010, and set firmly established downward trend in the<br />
conception rates for under 16s by 2010.<br />
• To achieve a reduction in the risk of long term social exclusion for<br />
teenage parents and their children. 2<br />
The <strong>Teenage</strong> <strong>Pregnancy</strong> Unit published a document entitled Guidance on<br />
Developing a <strong>Local</strong> <strong>Teenage</strong> <strong>Pregnancy</strong> <strong>Strategy</strong>. The guidance stated that<br />
local strategies must be produced to tackle teenage pregnancy and that those<br />
strategies must be coterminous with local authority and social services<br />
boundaries. <strong>County</strong> <strong>Durham</strong> and Darlington each needed its own strategy.<br />
The guidance stated that each document must contain a ten year strategy and<br />
a three year action plan to include detailed proposals and actions.<br />
5<br />
1. Social Exclusion Unit (1999)<br />
2. <strong>Teenage</strong> <strong>Pregnancy</strong> Unit<br />
The <strong>Teenage</strong> <strong>Pregnancy</strong> Unit has stated that the Health Authority and <strong>Local</strong><br />
(Social Services/Education) Authorities have joint responsibility for the<br />
development and implementation of the local strategy. It states that there<br />
should be joined up action between Health, Education, Social Services and<br />
Voluntary Agencies and that there should be consultation with key<br />
stakeholders, particularly young people. The joined up action should be based<br />
on Better Prevention to include:<br />
• Better Sex and Relationships Education<br />
• Better Information, Advice and Contraceptive Services<br />
• Better support for <strong>Teenage</strong> Parents<br />
• The production of a <strong>Local</strong> Media <strong>Strategy</strong>.<br />
A countywide steering group was established with representatives from the<br />
Health Authority, <strong>Local</strong> Authorities of <strong>County</strong> <strong>Durham</strong> and Darlington, and<br />
Voluntary Agencies. It was agreed that young people would be consulted when<br />
the draft strategy was completed. In addition, key stakeholders including young<br />
people, parents and at risk groups, will be consulted during the implementation<br />
process.
The strategic goals for <strong>County</strong> <strong>Durham</strong> and Darlington are:<br />
• To achieve a 55% reduction in the under 18s conception rate by<br />
2010, and to achieve a 10% reduction in that rate by 2004.<br />
• To establish a downward trend in the under 16s conception rate.<br />
• To achieve a reduction in the risk of long term social exclusion for<br />
teenage parents and their children.<br />
The <strong>Teenage</strong> <strong>Pregnancy</strong> Unit <strong>Local</strong> Implementation Fund is intended to kick<br />
start initiatives over the next three years. After that, work aiming to reduce<br />
teenage pregnancy rates and to support teenage parents must be mainstream<br />
funded.<br />
6
PART A<br />
SECTION 1<br />
7
Strategic Vision<br />
The countywide steering group for <strong>County</strong> <strong>Durham</strong> and Darlington, including<br />
representatives from Health, Education, Social Services and the Voluntary<br />
Sector, provided the strategic vision during the working meeting in September<br />
2000.<br />
Our strategic vision is to create an environment in which children and young<br />
people are confident, comfortable and in control of their sexual lives. Part of<br />
this environment will include improved opportunities for all young people. We<br />
will work to enable them to make the best possible choices for their current<br />
circumstances, and see beyond where they are now to where they could be.<br />
Within this context of raised aspirations and self-esteem, service will support<br />
and enable young people to make informed health and life decisions. Together<br />
these environmental and individual approaches will contribute to bringing about<br />
a reduction in the number of unplanned pregnancies.<br />
Principles and Values<br />
The work of the steering group has been to develop a strategy to tackle<br />
teenage pregnancies in line with the principles already signed up to by all<br />
agencies in <strong>County</strong> <strong>Durham</strong> and Darlington, through Investing in Children. We<br />
also endorse the principles of the <strong>Teenage</strong> <strong>Pregnancy</strong> Unit and the links<br />
between the two sets of principles and values are clearly stated below.<br />
Investing in Children<br />
The aim is to work in partnership with children and young people to promote<br />
their best interests and enhance their quality of life. We will achieve this by:<br />
Consulting with children, young people and their families about decisions<br />
affecting their lives and the development of services.<br />
<strong>Teenage</strong> <strong>Pregnancy</strong> Unit: Young People Centred<br />
We fully recognise that the involvement of young people is crucial to the<br />
successful planning and implementation of this strategy.<br />
Promoting partnerships between individuals and agencies to address young<br />
peoples issues.<br />
<strong>Teenage</strong> <strong>Pregnancy</strong> Unit: Partnership Working<br />
We fully acknowledge the need for the involvement of a wide range of<br />
stakeholders and the need to work together whilst respecting different<br />
approaches and beliefs. Our partnership working is demonstrated in the<br />
membership of the steering group and sub-groups. (See Joined Up Action)<br />
8
<strong>Teenage</strong> <strong>Pregnancy</strong> Unit: Long Term and Sustained<br />
We will review the progress made towards meeting the action plan goals using<br />
the steering group and sub-groups. We will aim to review progress quarterly by<br />
asking representatives from the lead agencies to report to the group actions<br />
achieved*. In this way we will seek continued commitment from all agencies<br />
and we will review progress made towards reducing teenage pregnancy in<br />
high-risk areas.<br />
* Projects/initiatives, which have been judged to be successful, will be brought<br />
into mainstream funding.<br />
Developing accessible children, young people and family centred services that<br />
promote dignity and independence and which do not discriminate or stigmatise.<br />
<strong>Teenage</strong> <strong>Pregnancy</strong> Unit: Addressing Inequalities<br />
To ensure that the strategy and action plans meet set targets, high-risk areas<br />
within <strong>County</strong> <strong>Durham</strong> and Darlington must be identified. Information is being,<br />
and will continue to be, obtained through a number of data sources.<br />
We have adopted an ‘across the county’ approach in the allocation of the <strong>Local</strong><br />
Implementation Fund.<br />
Ensuring that when making decisions on policies and services, consideration is<br />
given to their potential impact on the lives of children and young people.<br />
<strong>Teenage</strong> <strong>Pregnancy</strong> Unit: Evidence Based<br />
Research, which is vast in both its variety and amount informed the <strong>Teenage</strong><br />
<strong>Pregnancy</strong> Report (1999) 3 . The strategy and local action plans will take<br />
account of this and other evidence. New evidence will also be used as it is<br />
published on the teenage pregnancy website and in journals. We will aim to<br />
strengthen links with local universities to enable evaluation of our own practice.<br />
3 – Social Exclusion Unit<br />
Joined Up Action<br />
Structure<br />
The <strong>County</strong> <strong>Durham</strong> and Darlington wide tackling <strong>Teenage</strong> <strong>Pregnancy</strong> Coordinator<br />
is funded by the <strong>Teenage</strong> <strong>Pregnancy</strong> Unit and is employed by the<br />
Health Authority. The Co-ordinator is based at Dales PCG. (The Regional Coordinator,<br />
Anne Graney has agreed that there should be a co-ordinator based<br />
in Darlington as the strategies are co-terminous with local authority<br />
boundaries.) The co-ordinator has been guided and supported by lead<br />
contacts from both local authorities (<strong>County</strong> <strong>Durham</strong> and Darlington) as<br />
members of the <strong>County</strong> Wide Steering Group or as members of the Darlington<br />
Group or the <strong>County</strong> Sub-groups. Two strategies must be submitted, one for<br />
<strong>County</strong> <strong>Durham</strong> and one for Darlington.<br />
9
Structure<br />
Two strategies must be coterminous with local authority boundaries:<br />
<strong>County</strong> <strong>Durham</strong> Darlington<br />
10-Year <strong>Strategy</strong> 10-Year <strong>Strategy</strong><br />
3-Year <strong>Local</strong> Action<br />
Plan<br />
Joined Up Working<br />
<strong>County</strong> <strong>Durham</strong> and Darlington Steering Group<br />
Post Service / Organisation<br />
Service Development Manager Darlington Social Services<br />
Bishop Auckland Member Community Health Council<br />
Head of Midwifery / Senior Midwife South <strong>Durham</strong> Health Care NHS<br />
Trust<br />
Project Manager Investing in Children<br />
Project Manager End House, <strong>Durham</strong> Young Peoples<br />
Centre<br />
Specialist Health Promotion Manager Derwentside PCG / <strong>Durham</strong> &<br />
Chester-le-Street PCG<br />
Specialist Health Promotion Manager Dales PCG and Darlington PCG<br />
Specialist Health Promotion Manager Easington PCG and Sedgefield PCG<br />
Service Manager Learning Support Services, <strong>County</strong><br />
<strong>Durham</strong><br />
Senior Worker Community Education, <strong>County</strong><br />
<strong>Durham</strong><br />
Senior Nurse Paediatrics South <strong>Durham</strong> Health Care NHS<br />
Trust<br />
Health Promotion Strategist Lead Health Authority<br />
Consultant in Reproductive Medicine South <strong>Durham</strong> Health Care NHS<br />
and Family Planning<br />
Trust<br />
Assistant Chief Executive Derwentside PCG<br />
Children’s Services Manager <strong>Durham</strong> Social Services<br />
Chair Association of School Governors<br />
Professor of Sociology<br />
University of <strong>Durham</strong><br />
10<br />
3-Year <strong>Local</strong> Action<br />
Plan
Head of Service Connexions, <strong>County</strong> <strong>Durham</strong> Careers<br />
Service<br />
GP Darlington<br />
Women’s Service Manager North <strong>Durham</strong> Health Care NHS Trust<br />
<strong>County</strong> Sure Start Co-ordinator Education Department, <strong>County</strong><br />
Tackling <strong>Teenage</strong> <strong>Pregnancy</strong><br />
Co-ordinator<br />
11<br />
<strong>Durham</strong><br />
<strong>County</strong> <strong>Durham</strong> and Darlington<br />
Health Authority<br />
The sub groups were established to ensure that both strategies/action plans<br />
were fully informed of local issues and to enable each part of the strategy to<br />
be planned in detail. The sub groups considered the following issues:<br />
• Better prevention<br />
• Better sex and relationship education<br />
• Better contraception and advice services<br />
• Better support for teenage parents.<br />
Joined Up Working<br />
Membership of Darlington Groups<br />
Membership of the group demonstrates joined up working.<br />
Better Contraception and Advice Services<br />
Post<br />
School Doctor and Consultant in<br />
M.O.and Family Planning<br />
Consultant in Reproductive Medicine<br />
and Family Planning<br />
Health Promotion Manager<br />
Tackling <strong>Teenage</strong> <strong>Pregnancy</strong><br />
Co-ordinator<br />
Service/Organisation<br />
South <strong>Durham</strong> Health Care NHS Trust<br />
South <strong>Durham</strong> Health Care NHS Trust<br />
Darlington PCG<br />
<strong>County</strong> <strong>Durham</strong> and Darlington Health<br />
Authority<br />
GP Seconded to the PCG Board for young<br />
people’s issues
Better Sex and Relationship Education<br />
Post<br />
Manager<br />
Team leader<br />
Secondary Education Advisor<br />
Head of Pupil Support Services<br />
Assistant Director of Education<br />
Development Manager<br />
1 Residential Social Work Manager<br />
2 x Senior Residential Social Workers<br />
Head of Service<br />
Project Manager<br />
Manager<br />
Tackling <strong>Teenage</strong> <strong>Pregnancy</strong><br />
Co-ordinator<br />
Better Support for <strong>Teenage</strong> Parents<br />
Post<br />
Service Development Manager<br />
Manager<br />
Project Manager<br />
Early Years Partnership<br />
Head of Service<br />
Community Midwife<br />
Health Visitor<br />
Tackling <strong>Teenage</strong> <strong>Pregnancy</strong> Coordinator<br />
Joined Up Working<br />
12<br />
Service/Organisation<br />
Community Education Service<br />
School Nurses, South <strong>Durham</strong> Health<br />
Care NHS Trust<br />
Education Department<br />
Education Department<br />
Education Department<br />
Social Services<br />
Social Services<br />
Social Services<br />
Home and Hospital Teaching Service<br />
NCH Tubwell Project<br />
Youth Offending Team<br />
<strong>County</strong> <strong>Durham</strong> and Darlington Health<br />
Authority<br />
Service/Organisation<br />
Membership of <strong>County</strong> <strong>Durham</strong> Sub-groups<br />
Better Contraception, Advice and Information Services<br />
Post<br />
Specialist Health Promotion Manager<br />
Specialist Health Promotion Manager<br />
Specialist Health Promotion Manager<br />
Consultant in Reproductive Medicine &<br />
Family Services<br />
GP<br />
Social Services<br />
Housing Association – Stonham<br />
NCH - Tubwell Project<br />
Education Department<br />
Home and Hospital Teaching Service<br />
South <strong>Durham</strong> Health Care NHS Trust<br />
South <strong>Durham</strong> Health Care NHS Trust<br />
<strong>County</strong> <strong>Durham</strong> and Darlington Health<br />
Authority<br />
Service/Organisation<br />
Darlington/Dales PCGs<br />
Derwentside/<strong>Durham</strong> & Chester-le-<br />
Street PCGs<br />
Easington/Sedgefield PCGs Project<br />
South <strong>Durham</strong> Health Care NHS Trust<br />
Seconded to PCG
School Nurse Manager<br />
Women’s Services Manager<br />
Project Manager<br />
Head of Child Health Services<br />
Better Sex and Relationships Education<br />
Post<br />
Head of Service<br />
Education Advisor/Inspector<br />
Chair<br />
Manager – Connexions<br />
Manager – School Nursing<br />
Healthy Schools Co-ordinator<br />
Manager and Senior Worker<br />
Head Teacher<br />
Sexual Health Trainer<br />
Tackling <strong>Teenage</strong> <strong>Pregnancy</strong> Coordinator<br />
Better Support<br />
Post<br />
Better Service<br />
Health Visitor<br />
Development Manager<br />
Head of Service<br />
Co-ordinator<br />
Regeneration Officer<br />
Manager<br />
Children’s Services Manager<br />
Community Nurse<br />
Children’s Services Manager<br />
Women’s Services<br />
Senior Midwife<br />
Sure Start Co-ordinator<br />
Tackling <strong>Teenage</strong> <strong>Pregnancy</strong> Coordinator<br />
13<br />
South <strong>Durham</strong> Health Care NHS Trust<br />
North <strong>Durham</strong> Health Care NHS Trust<br />
End House<br />
South <strong>Durham</strong> Health Care NHS Trust<br />
Service/Organisation<br />
Learning Support Service<br />
Education Department<br />
Association of School Governors<br />
Connexions/Community Education<br />
North <strong>Durham</strong> Health Care NHS Trust<br />
Health Promotion/Health Authority<br />
Community Education<br />
Representative of Head Teachers<br />
Association<br />
Community Education<br />
<strong>County</strong> <strong>Durham</strong> and Darlington Health<br />
Authority<br />
Service/Organisation<br />
Connexions/Co <strong>Durham</strong> Carers<br />
Service<br />
South <strong>Durham</strong> Health Care NHS Trust<br />
Darlington Social Services<br />
Home and Hospital Teaching Service<br />
Darlington<br />
Home and Hospital Teaching Service<br />
<strong>Durham</strong><br />
<strong>County</strong> <strong>Durham</strong> Education<br />
Housing Association<br />
<strong>Durham</strong> Social Services<br />
North <strong>Durham</strong> Health Care NHS Trust<br />
North <strong>Durham</strong> Health Care NHS Trust<br />
North <strong>Durham</strong> Health Care NHS Trust<br />
South <strong>Durham</strong> Health Care NHS Trust<br />
Darlington, Sure Start<br />
<strong>County</strong> <strong>Durham</strong> and Darlington Health<br />
Authority<br />
The Darlington groups and the <strong>County</strong> <strong>Durham</strong> sub-groups met to discuss the<br />
process of strategy development. In each case it was felt that a half-day<br />
working session was the most appropriate way of devising a ten year strategy<br />
and three year action plans. Key tasks and a lead agency or agencies were<br />
identified and timescales were set for delivery of the action.
The Steering group and sub-groups will continue to meet quarterly to assess<br />
progress made towards the actions identified in the three year action plan.<br />
Consultation and Involvement of other<br />
Stakeholders<br />
After extensive debate with key representatives from young people’s<br />
advocacy services, it was decided not to invite young people to the steering or<br />
sub-groups, it was felt that they may not feel able to express themselves fully<br />
and honestly in such a forum. For that reason young peoples groups are<br />
being sent the draft strategy and are being asked to comment on it at their<br />
leisure. The writer particularly asked about readability as well as the plans.<br />
Young people were asked to comment on how appropriate the actions are<br />
and on how they would like to see local services improved, and the local<br />
media campaign move forward. Young people were contacted through<br />
agencies/groups including:<br />
Investing in Children, End House Young Peoples Centre.<br />
As actions are planned in more detail and implemented, young people will be<br />
consulted again before plans are actioned. Focus groups will be used both to<br />
consult and to evaluate projects.<br />
The draft strategy was sent to all members of the Steering group, Darlington<br />
Groups and the <strong>County</strong> Sub-groups for consultation. In addition, Chief<br />
Executives of the Health Authority and all Primary Care Group Chairs and<br />
Chief Executives were asked to comment. <strong>Local</strong> Further Education Colleges<br />
were involved in the consultation process. The feedback will be incorporated<br />
into the final version of the strategy to be submitted to the <strong>Teenage</strong><br />
<strong>Pregnancy</strong> Unit.<br />
After consultation with stakeholders the strategy and action plans were<br />
revised to incorporate their views.<br />
14
Links to other Policies<br />
The <strong>Teenage</strong> <strong>Pregnancy</strong> <strong>Strategy</strong> links with a range of other policies and strategies:<br />
<strong>Local</strong><br />
Housing<br />
Strategies<br />
PCG Action<br />
Plans<br />
Sexual Health<br />
<strong>Strategy</strong><br />
Connexions<br />
<strong>Strategy</strong><br />
Health<br />
Improvement<br />
Programmes<br />
Education<br />
Development &<br />
Education<br />
Support Plans<br />
NHS<br />
National<br />
Plan<br />
<strong>Teenage</strong><br />
<strong>Pregnancy</strong><br />
<strong>Strategy</strong><br />
Mental<br />
Health<br />
NSF<br />
Neighbour<br />
-hood<br />
Renewal<br />
15<br />
Healthy<br />
Schools<br />
Policy<br />
Quality<br />
Projects<br />
Children’s<br />
Services<br />
Plan<br />
Key<br />
Sure Start<br />
Strong Links<br />
Less Strong Links
<strong>Strategy</strong> Goals<br />
Each part of the strategy details a specific strategic goal or vision, but broadly we aim to achieve in ten years time:<br />
• The target reduction of 55% in the under 18s conception rate, including working towards a 10% reduction in the rate by 2004.<br />
• Establish a downward trend in the under 16s conception rate.<br />
• Better advice, information and contraception services which are accessible and used by young people.<br />
• Better sex and relationship education in schools, but also in residential care settings, youth offending services,<br />
community/youth education and the voluntary sector agencies.<br />
• Improve the self esteem and confidence of young people through various community wide activities, such as the Healthy<br />
Schools Award, Better Sex and Relationships Education and through the Personal, Social and Health Education Programme.<br />
• Better support for teenage parents, in terms of services available, including housing.<br />
• Continue to develop the links between Health, Education, Social Services and the Voluntary Sector.<br />
• Develop an on-going consultation with young people and other key stakeholders as the strategy action plans are reviewed and<br />
revised over time.<br />
• Further develop data collection systems to measure the impact of action plans.<br />
• The reduction of Social Exclusion of young people in <strong>County</strong> <strong>Durham</strong> is a priority.<br />
16
PART A<br />
SECTION 2<br />
17
<strong>Local</strong> Context<br />
Main Findings from <strong>Local</strong> Analysis, March 2000, including<br />
Demographic Information<br />
<strong>County</strong> <strong>Durham</strong> and Darlington Health Authority covers a wide range of living<br />
conditions and economic circumstances. The west part is mainly rural, with<br />
population densities in Weardale and Teesdale being among the lowest nationally.<br />
Estimates of the resident population in mid –2000 for the Primary Care Group areas<br />
are as follows:<br />
Darlington 99,900<br />
Sedgefield 89,900<br />
The Dales, Including Weardale and Teesdale 87,400<br />
Derwentside 86,000<br />
<strong>Durham</strong> and Chester-le-Street 146,900<br />
Easington 95,900<br />
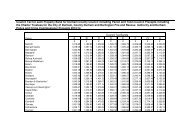
<strong>County</strong> <strong>Durham</strong> and Darlington have relatively small ethnic minority populations<br />
however each ethnic group is represented in the county. Details of residents by<br />
ethnic group are detailed below. ( Boundaries of <strong>Local</strong> Authorities (LAs) are as at<br />
April 1998.)<br />
LAs White Carib<br />
bean<br />
Afric<br />
an<br />
Black<br />
Other<br />
Indian Pakis<br />
tani<br />
18<br />
Bangl<br />
adeshi<br />
Asian<br />
Other<br />
Darlingtn 98.5 0.1 0.1 0.1 0.5 0.1 0.2 0.1 0.2 0.2<br />
Chester-le-<br />
Street<br />
99.3 0.0 0.0 0.1 0.1 0.0 0.0 0.1 0.2 0.1<br />
Derwentside 99.6 0.0 0.0 0.0 0.1 0.0 0.0 0.0 0.1 0.1<br />
<strong>Durham</strong> 98.9 0.0 0.1 0.0 0.2 0.1 0.0 0.3 0.2 0.2<br />
Easington 99.4 0.0 0.0 0.0 0.2 0.1 0.0 0.1 0.1 0.1<br />
Sedgefield 99.6 0.0 0.0 0.0 0.1 0.0 0.0 0.1 0.1 0.1<br />
Teesdale 99.6 0.1 0.0 0.0 0.0 0.0 0.0 0.1 0.0 0.1<br />
Wear Valley 99.5 0.1 0.0 0.0 0.1 0.0 0.0 0.1 0.1 0.1<br />
Chin<br />
ese<br />
Other<br />
With the downturn in the farming sector, rural deprivation is a real issue in these<br />
areas. At the same time areas in the east and north of the Health Authority have<br />
traditionally relied on heavy industry such as coal mining and steel making, which<br />
have now ceased, again leaving considerable pockets of social deprivation, despite<br />
vigorous and partially successful efforts to attract inward investment. <strong>Durham</strong> City<br />
has the benefit of the University, and tourist attractions which enhance the local<br />
economy. Darlington Borough Council has Unitary status, is situated on the fringe of<br />
Teesside, and has more diverse sources of employment than most parts of <strong>County</strong><br />
<strong>Durham</strong> and Darlington Health Authority.
The latest measure of deprivation, the DETR Index of Multiple Deprivation 2000<br />
(IMD2000), is a ward level index, based on the premise that multiple deprivation is<br />
made up of separate dimensions or domains of deprivation. The domains are:<br />
Income, Employment, Health Deprivation & Disability, Education Skills & Training,<br />
Geographical Access to Services and Housing. Of the 177 wards in <strong>County</strong> <strong>Durham</strong><br />
and Darlington:<br />
• Two wards are ranked in the 100 most deprived wards in England, (Eden Hill<br />
and Deneside).<br />
• 110 wards (62%) are in the top 25% most deprived wards in England.<br />
IMD Rankings for the Most Deprived Wards in each Primary Care Group Area.<br />
Most<br />
deprived<br />
ward<br />
The Dales Woodhouse<br />
Close (119)<br />
Darlington Central<br />
(290)<br />
Derwentside South<br />
Stanley<br />
<strong>Durham</strong> &<br />
Chester-le-<br />
Street<br />
(160)<br />
Easington Eden Hill<br />
(21)<br />
2 nd most<br />
deprived<br />
ward<br />
St Helens<br />
(185)<br />
Eastbourne<br />
South (359)<br />
Craghead<br />
(214)<br />
Pelaw (332) Chester<br />
West (690)<br />
Deneside<br />
(53)<br />
Sedgefield West (372) Thickley<br />
(382)<br />
Co. <strong>Durham</strong><br />
& Darlington<br />
Eden Hill<br />
(21)<br />
Deneside<br />
(53)<br />
19<br />
3 rd most<br />
deprived<br />
ward<br />
Coundon<br />
(396)<br />
Cockerton<br />
West (519)<br />
Consett<br />
(314)<br />
New<br />
Brancepeth<br />
(789)<br />
Dawdon<br />
(162)<br />
Cornforth<br />
(405)<br />
Woodhouse<br />
Close (119)<br />
4 th most<br />
deprived<br />
ward<br />
Henknowle<br />
(409)<br />
Eastbourne<br />
North (559)<br />
South Moor<br />
(531)<br />
Shadforth<br />
(807)<br />
Shotton<br />
(165)<br />
Old<br />
Trimdon<br />
(514)<br />
South<br />
Stanley<br />
(160)<br />
5 th most<br />
deprived<br />
ward<br />
Stanley<br />
(511)<br />
Park East<br />
(637)<br />
Catchgate<br />
(597)<br />
Grange<br />
Villa (883)<br />
Easington<br />
Colliery<br />
(176)<br />
Sunnydale<br />
(820)<br />
Dawdon<br />
(162)<br />
This is the setting in which two <strong>Local</strong> Government Districts within the Health<br />
Authority have rates of teenage pregnancy in the highest ten in England. The link is<br />
an environment in which young people’s personal aspirations and goals, may be<br />
limited by what seem to them poor opportunities and prospects for their communities<br />
as a whole. The challenge this represents is partially addressed in this report in<br />
terms of service provision, but of course ties in to the much larger strategy for<br />
economic regeneration. The apparent clusters of high rates at a ward level do not so<br />
far as our understanding at this stage goes tie in with areas for which these problems<br />
are especially marked. This raises the question of the extent to which our action plan<br />
should be targeted to areas with apparently high rates, which may fluctuate<br />
considerably, versus maintaining a focus on improving services overall. There are<br />
also geographical issues in terms of service delivery, particularly to teenage parents<br />
under 16, where issues of access include physical distance and costs of transport.
The development work that resulted in report of March 2000 and in this report, has<br />
identified a number of strengths for <strong>County</strong> <strong>Durham</strong> and Darlington Health Authority<br />
and our partner agencies. The first is the considerable depth and range of goodwill,<br />
concern and willingness to act to address the issue of teenage pregnancy.<br />
There are also some examples of excellent practice. End House in <strong>Durham</strong> City is<br />
one of these in the provision of sexual health advice and contraceptive services to<br />
young people. The Before and After Group in Darlington is a second one, for its<br />
holistic approach to work with teenage mothers under 16.<br />
A third strength is the capacity to develop a Reference Group of young people, which<br />
is possible through the work of the Investing in Children initiative in <strong>County</strong> <strong>Durham</strong>,<br />
and the Peer Educators Group in Darlington.<br />
Finally, the location of Specialist Health Promotion Services, with a strategic lead<br />
responsible for co-ordinating this report, and services linked closely with the Primary<br />
Care Groups (PCGs), has enhanced our ability to network effectively, and move<br />
towards joined up service provision.<br />
The exercise in March 2000 together with this report identified a number of key areas<br />
for development. The first is the need to develop better baseline data in relation to<br />
service provision (particularly contraceptive service uptake, housing needs,<br />
curriculum coverage of sex and relationships education) and a better understanding<br />
of the distribution and cause of local clusters of teenage pregnancy in young women<br />
under 16.<br />
A linked need identified in March 2000 was for better co-ordination. This required an<br />
identified dedicated co-ordinator, whose job would involve communicating about<br />
service developments, ensuring a joined up approach, feeding research based<br />
practice into local developments, working with the media, encouraging effective local<br />
progress, monitoring against baseline data, addressing issues of equity, and linking<br />
local work with national developments. This post need support at a local (PCG) level,<br />
which was suggested in the form of Outreach Workers, based in the contraceptive<br />
services developed for young people, but with a link role with vulnerable groups as<br />
well as mainstream agencies working with young people. These posts would also act<br />
as direct entry points to services for young people who have used emergency<br />
contraception, who have just had a pregnancy confirmed, or who have had a baby<br />
but may not necessarily take up contraceptive services automatically.<br />
Two issues affecting the <strong>Local</strong> Education Authorities have emerged. One is that the<br />
devolution of their support role to schools makes it difficult for them to respond fully<br />
to central initiatives such as the improvement of sex and relationships education<br />
within PSHE. Secondly is that in terms of attendance at school, teenage pregnancy<br />
is a much more serious risk of social exclusion for girls, than is permanent exclusion<br />
for other reasons. Equitable provision for this group is therefore a major issue in<br />
service planning.<br />
20
Primary Care Groups have a crucial role in developing services to address the<br />
considerable estimated levels of unmet need for contraceptive services and sexual<br />
health advice for young people. This is through direct service provision, through<br />
developing appropriate services in partnership with Trusts including maximise the<br />
potential of school nurses, and the Voluntary Sector, and by streamlining the flow of<br />
information to the public about all aspects of sexual health services.<br />
In addressing the needs of teenage parents, there is a good service basis in terms of<br />
provision for under 16s. This needs to be built on to ensure the service is accessible<br />
to all who need it, and to address the needs of young parents aged 16-18. In doing<br />
this the importance of recognising the variety of circumstances and needs within the<br />
category ‘teenage parents’ is crucial.<br />
Finally, the role of the wider community is important if the underlying issues of open<br />
and direct communication about matters related to sexual health are to be<br />
addressed. Developmental work with parents is one part of this work.<br />
There is no doubt that the potential to both reduce teenage pregnancies and to<br />
promote the sexual health of our communities is there.<br />
We look forward to working locally and with others nationally to achieve an<br />
appropriate balance between specific targeted work, and an approach to young<br />
people as a whole.<br />
21
<strong>Local</strong> Profile of <strong>Teenage</strong> <strong>Pregnancy</strong><br />
Incidence at <strong>Local</strong> Authority Level<br />
Table 1 below shows the summary profile of the conception rate for girls under 16<br />
within <strong>County</strong> <strong>Durham</strong> and Darlington. The rate for 1996 – 98 higher than the rate<br />
for England and Wales and it is higher than the rate for the Northern and Yorkshire<br />
Region.<br />
Analysis at the level of local authority is included. However, caution should be<br />
exercised in interpreting these figures as the numbers are small in any one year.<br />
That being said, both Wear Valley and Easington show the highest levels of<br />
conceptions in girls under 16.<br />
Table 1<br />
Conception rates for under 16s in 1996 – 1998<br />
(Rate per 1000 girls aged 13 – 15)<br />
Data for <strong>Local</strong> Authorities in <strong>County</strong> <strong>Durham</strong> and Darlington<br />
England and Wales<br />
England<br />
Northern & Yorkshire<br />
RO<br />
<strong>County</strong> <strong>Durham</strong> &<br />
Darlington<br />
Darlington UA<br />
Chester-le-Street<br />
Derwentside<br />
<strong>Durham</strong><br />
Easington<br />
Sedgefield<br />
Teesdale<br />
Wear Valley<br />
Number of<br />
conceptions<br />
25,566<br />
23,761<br />
3,757<br />
422<br />
60<br />
26<br />
44<br />
48<br />
103<br />
64<br />
9<br />
68<br />
22<br />
Ages
Table 2<br />
Conception Rates for under 18s 1996 – 1998<br />
(Rate per 1000 women aged 15-17)<br />
Data for <strong>Local</strong> Authorities in <strong>County</strong> <strong>Durham</strong> and Darlington<br />
England and Wales<br />
England<br />
Northern & Yorkshire<br />
RO<br />
<strong>County</strong> <strong>Durham</strong> &<br />
Darlington<br />
Darlington UA<br />
Chester-le-Street<br />
Derwentside<br />
<strong>Durham</strong><br />
Easington<br />
Sedgefield<br />
Teesdale<br />
Wear Valley<br />
Number of<br />
conceptions<br />
Clusters below <strong>Local</strong> Authority level<br />
130,909<br />
122,053<br />
18,424<br />
1,967<br />
352<br />
133<br />
274<br />
186<br />
419<br />
286<br />
51<br />
266<br />
23<br />
Ages
<strong>County</strong> <strong>Durham</strong> (but not Darlington) has been awarded Standards Fund monies to<br />
spend specifically on teenage pregnancy. Learning Support Service records were<br />
used to identify schools in <strong>County</strong> <strong>Durham</strong> within these or nearby wards. Funding<br />
for special projects aimed at reducing teenage conceptions has been directed to six<br />
schools in 2000/2001 an additional two schools will receive money in the financial<br />
year 2001/2002.<br />
The Steering Group will work with supporting agencies to identify the needs of<br />
teenagers of ethnic minority populations in relation to sex education and access to<br />
services.<br />
Table 3 demonstrates conception rates leading to maternities and abortions for girls<br />
aged under 18. Where figures show that the numbers of terminations are particularly<br />
low compared to maternities and conceptions, the possible reasons will be<br />
investigated.<br />
Table 3<br />
Under 18s Conceptions: numbers by <strong>Local</strong> Authority and outcome<br />
1995 – 1997<br />
<strong>Local</strong> Authority Leading to<br />
Maternities<br />
Chester-le-Street<br />
CD<br />
Darlington UA<br />
Derwentside CD<br />
<strong>Durham</strong> CD<br />
Easington CD<br />
Sedgefield CD<br />
Teesdale CD<br />
Wear Valley CD<br />
Conception Numbers Rate per<br />
1000 girls<br />
86<br />
218<br />
182<br />
116<br />
310<br />
193<br />
30<br />
163<br />
Leading to<br />
Abortions<br />
24<br />
51<br />
135<br />
80<br />
63<br />
104<br />
99<br />
23<br />
87<br />
Total<br />
Conceptions<br />
137<br />
353<br />
262<br />
179<br />
414<br />
292<br />
53<br />
250<br />
aged 15-17<br />
47.3<br />
63<br />
55.6<br />
34.6<br />
75.1<br />
56.6<br />
43.9<br />
73.3<br />
Total England 69,500 46,892 116,392 44.4<br />
Total England &<br />
Wales<br />
75,056 49,672 124,728 44.8
Priorities<br />
Priorities have been agreed by the Steering and sub groups as detailed in Part A,<br />
Section 1. Consultation with young people and other key stakeholders took place in<br />
March 2001. Comments from young people and key stakeholders have been<br />
incorporated into the strategy.<br />
<strong>Local</strong> Progress<br />
<strong>Local</strong> progress will be monitored quarterly by the Steering Group and sub groups. It<br />
will also be monitored by the Tackling <strong>Teenage</strong> <strong>Pregnancy</strong> Co-ordinator who will<br />
retain close links with all stakeholders and lead individuals/agencies named in the<br />
action plans. Monitoring arrangements will be considered/planned in more detail in<br />
the first quarterly meeting of the Steering and sub groups.<br />
<strong>County</strong> <strong>Durham</strong><br />
Audit of Current Services and Gaps Identified<br />
This audit is taken from the document entitled ‘Tackling <strong>Teenage</strong> <strong>Pregnancy</strong>: a<br />
response from <strong>County</strong> <strong>Durham</strong> Health Authority, Darlington Borough Council and<br />
<strong>Durham</strong> <strong>County</strong> Council 3 rd March 2000’<br />
<strong>Teenage</strong> <strong>Pregnancy</strong> Unit Report<br />
Summary of action plans:<br />
• Training and support for youth workers<br />
The Community Education Services in both <strong>County</strong> <strong>Durham</strong> and Darlington are<br />
currently looking into developing training and support for youth workers generally<br />
on this issue. For <strong>Durham</strong> Community Education Service a budget of £15,000<br />
(including on-costs) enabled the model of peripatetic support developed for drugs<br />
work to be extended to sexual health activities in the youth work setting. The<br />
Sexual Health Trainer was recruited funded from this money in November 2000.<br />
Encourage Youth and Community Workers to take up the Level 3 Sexual Health<br />
Programme accredited through the Tees and Region Open College Network.<br />
• Parents as Educators<br />
A worker has been employed for 12 months to carry out local action research and<br />
development work with parents to support the Department of Health campaign.<br />
The aim of the post is to clarify what would effectively support parents in their role<br />
as sex educators.<br />
Estimated costs including administrative support and on costs £27,000.<br />
25
• Outreach workers linking contraceptive services with vulnerable young<br />
people<br />
Sexual Health Outreach Workers have been appointed in four of the six PCG<br />
areas. Each area will have a worker in 2001/2002. Their task is to act as an<br />
advocate for young people in using the contraceptive care services, and to<br />
provide Outreach work particularly targeted to settings where young people are<br />
known to be at risk, including children in the looked after system, young<br />
offenders, young people outside mainstream education, young people who are<br />
homeless or with housing difficulties. A further group the Outreach Worker link<br />
with is teenage mothers as a first point of contact when pregnancy is confirmed if<br />
this is not already addressed by health and social services. Follow up could<br />
include encouraging them to access contraceptive services, which does not<br />
always happen despite their experiences. Where possible the Outreach worker<br />
would also link with generic schools and youth services, and would be an access<br />
point for teachers and school nurses encouraging young people to make use of<br />
the services for the first time. In addition the proposal for a protocol to ensure<br />
consistent follow up of young people using emergency contraception, would be<br />
enhanced by the ability to offer an appointment with the Outreach worker, or for<br />
the Outreach worker to directly contact the young person.<br />
• A Tackling <strong>Teenage</strong> <strong>Pregnancy</strong> Co-ordinator has been appointed for <strong>County</strong><br />
<strong>Durham</strong> and Darlington.<br />
Action plans already underway or agreed (A)<br />
• Easington PCG<br />
Subgroup is working on contraceptive provision<br />
• Emergency contraception from Pharmacists<br />
This will take place in line with National Guidelines and over the counter<br />
availability will be based on patient group directions.<br />
• Sex Education Roadshow<br />
In Darlington teachers are included as part of the target audience for a ‘sex<br />
education roadshow’ training event within the next three to six months<br />
The resource boards have been purchased by Health Promotion Units in <strong>County</strong><br />
<strong>Durham</strong> and are available through that service.<br />
• Standards Fund 2000-2001 <strong>Teenage</strong> <strong>Pregnancy</strong> Grant 19E (94,000)<br />
Activity Two – Proposals<br />
(see section 3.1 for Activity One Proposals)<br />
Funding has been developed in schools in ‘at risk’ areas in order to target<br />
vulnerable young people. An action research project involving a ‘menu’ of<br />
preventative approaches has been provided to enable individual schools to select<br />
suitable approaches linked to the Healthy Schools Initiative. A small amount of<br />
funding will be retained by the LEA to cover an external evaluation of both<br />
activities.<br />
26
The Grant will be managed by a team of LEA Officers, Health Promotion<br />
Specialists and school representatives.<br />
• Guidelines for Youth Workers<br />
In <strong>County</strong> <strong>Durham</strong> the guidelines for youth workers in relation to sex and<br />
relationships education are being updated, and a policy to back these up is<br />
nearly ready. The ten week accredited training programme on sexual health will<br />
be offered to youth workers across the <strong>County</strong>. In addition the National Youth<br />
Agency Sex and Relationships training pack which has recently been launched,<br />
will be piloted.<br />
• Sex education roadshows<br />
<strong>Local</strong> Levy funding via the Education and Training Consortium was used to run a<br />
Roadshow for youth workers across <strong>County</strong> <strong>Durham</strong>, to provide each of them<br />
with materials and training to run their own ‘sex education roadshow’. The same<br />
funding in Darlington was used for a Roadshow targeted to youth workers,<br />
teachers, health visitors, midwives and social workers working with young people,<br />
to train them as facilitators and provide materials to each run their own ‘sex<br />
education roadshow’<br />
session.<br />
• Mobile Services<br />
The Mobile Youth Outreach Health Project in Chester-le-St is Joint Financed and<br />
will be starting a multi-disciplinary outreach service to local villages addressing<br />
sexual health issues as part of a holistic approach, using a vehicle donated by<br />
the Police.<br />
A further bid for Lottery Funding has been put in to enable provision of a second<br />
Youth Bus, for Darlington based on the success of the existing service.<br />
In other areas opportunities to develop mobile services building on the success of<br />
the Youth Bus model will be sought, particularly in Seaham/Peterlee linked with<br />
the Education Action Zones.<br />
• Negotiating skills development<br />
The Dales Healthy Living Centre bid includes a development from the Girls Talk<br />
project which aims to develop skills in negotiating with partners, peers and<br />
parents.<br />
• Sex Education Roadshow<br />
In Darlington a one off pilot “sex education roadshow” took place in March 2000<br />
offered to young people aged 13-16 in the Looked After System, and outside<br />
mainstream education. Funding was from the <strong>Local</strong> Levy via the Education and<br />
Training Consortium. The event was evaluated very favourably.<br />
• Education Action Zones<br />
Curriculum development work to raise aspirations (e.g. positive role models,<br />
mentors from industry), increase educational attainment, and enhance life skills<br />
are being developed in both Peterlee and Seaham Education Action Zones.<br />
Working together with the Careers Service to help increase the proportion of<br />
young people continuing in education and training post 16.<br />
27
• Parents as Educators training<br />
In Easington extend the Community based health groups for members<br />
specifically interested in sexual health.<br />
Healthy Living Centre proposal (The Dales) includes a two part programme for<br />
parents: ten orientation sessions with offered follow up on Talking to <strong>Teenage</strong>rs,<br />
handling <strong>Teenage</strong> Behaviour, Sexual Behaviour, Drugs and Alcohol. The<br />
proposal is a partnership including South <strong>Durham</strong> Health Care, Specialist Health<br />
Promotion Services, Youth and Community, Wear Valley District Council.<br />
• Standards Fund 2000 – 2001 and 2001 – 2002 <strong>Teenage</strong> <strong>Pregnancy</strong> Grant<br />
<strong>County</strong> <strong>Durham</strong> has been awarded Standards Fund Grant. The fund has been<br />
used to help named schools in their work to reduce teenage pregnancy rates and<br />
a specialist reintegration officer has been appointed to work across the county<br />
and liaise with the existing education personnel working with school age mothers.<br />
The officer undertakes some co-ordination of information regarding preventative<br />
approaches and works closely with the <strong>Teenage</strong> <strong>Pregnancy</strong> Co-ordinator and the<br />
Sure Start Partnerships. Childcare costs are available if required to enable full<br />
attendance.<br />
• Education Action Zones<br />
The Peterlee Education Action Zone plans to include work with young parents as<br />
part of its programme. This could include for example work with a teenage mum,<br />
in preparing her child for his or her first SATS. It might involve work with a young<br />
dad using information technology. In either case the objective is to take a whole<br />
family approach, and enhance the parents overall communication and rapport<br />
with the child. This in turn will contribute to improved educational attainment, and<br />
quality of life for the family.<br />
• Sure Start projects include provision for teenage parents<br />
The issue of provision for children with teenage parents is being considered in<br />
the development of each of these projects, which will act as sources of innovation<br />
for development on a wider basis.<br />
• Launch of PSK2 workshops on sexual health for peer education on the<br />
March 2000, and then made available to secondary schools in Darlington.<br />
• Easington Young with a Baby Project<br />
Easington <strong>Teenage</strong> Parenthood Peer Education Project has been funded by the<br />
Easington Health Implementation Group. This is based on a previous project<br />
‘Young With A Baby’.<br />
• Young People’s Reference Group and Sexual Health<br />
Investing in Children will develop a group of young people interested in sexual<br />
health as an interest area, working with a consultant to help them access suitable<br />
material, resolve obstacles, and explore issues in a way relevant and useful to<br />
themselves. Over the period April to December 2000, the group was recruited,<br />
and based on an initial discussion of key issues relate to sexual health and<br />
contraceptive provision, sex and relationships education, and other aspects of<br />
interest to the group members, will embark on a developmental programme. This<br />
28
involves collecting examples of good practice from elsewhere. It could mean that<br />
group members are able to offer family planning clinics, GP Practices etc, a pool<br />
of knowledgeable young people able to “test” their services for user friendliness<br />
and atmosphere. It will definitely provide a group able to enter into dialogue as<br />
the strategy to reduce teenage pregnancies develops.<br />
• <strong>Teenage</strong>rs as Parents<br />
The Dales Healthy Living Centre bid includes <strong>Teenage</strong>rs as Parents (a focused<br />
intervention with the Primary Care Team working in a peer led education model).<br />
• Peterlee Pupil Representation Group<br />
The Education Action Zone in Peterlee has a Pupil Representation Group (1 from<br />
each secondary school in the zone) who will be asked to give their views and<br />
support to work in this area.<br />
Action plans recommended for further development (R)<br />
• Incidence at <strong>Local</strong> Authority level<br />
Investigate trends over a longer time period in order to establish a better<br />
understanding of the long term situation.<br />
• Confidential Inquiry<br />
Establish a confidential local enquiry system to be in place to access data on<br />
teenage conceptions. In particular this would look into local patterns in<br />
terminations/ continuation of pregnancy among under 16s, as research<br />
elsewhere has shown that these can vary considerably within small geographical<br />
areas, and may lead into service development issues.<br />
• Data for 16-18s<br />
Map distribution of pregnancies in young women aged 16-18.<br />
• Equality of Education<br />
Ensure equality of opportunity and equality of access the LEA will be planning<br />
and funding equitable provision rather than a two- tier provision whereby many<br />
excluded pupils receive full time packages and pregnant pupils receive a lesser<br />
provision.<br />
• Housing needs<br />
Northern Consortium of Housing Authorities to co-ordinate needs assessment for<br />
semi-supported housing for lone teenage parents, across <strong>County</strong> <strong>Durham</strong> with<br />
support from Public Health in line with requirement of the <strong>Teenage</strong> <strong>Pregnancy</strong><br />
Unit.<br />
• Contraceptive advice from a GP other than the one you are registered with<br />
Collect information about which GPs have opted to provide contraceptive advice<br />
to all patients, rather than simply their own practice in order to identify gaps in<br />
provision and publicise the provision more widely. 1<br />
1 Obtaining contraceptive advice in more privacy than is often possible in small community surgeries is clearly an important<br />
facility; there is anecdotal evidence that many professionals as well as the public are unaware of the possibility. Some<br />
patients appear to use ‘temporary resident’ arrangements, which could be considered fraudulent in some circumstances.<br />
29
• Practice Development Plans<br />
Ensure that the Postgraduate Medical Education Training programme includes<br />
regular updates on service provision related to sexual health and contraception,<br />
and skills in dealing with young people, as well as medical aspects and<br />
encourage GPs to take up this training. Ensure appropriate training is identified<br />
and made accessible to practice nurses. Provide receptionist training to assist<br />
them in dealing sympathetically with enquiries from young people.<br />
• Specific sessions for contraception<br />
All group practices should be encouraged as the norm to offer contraceptive<br />
services at specific clinics, held at times suitable for young people i.e. after<br />
school or Saturday morning, with discreet waiting areas. GPs may find lunch<br />
times are appropriate. This should be in liaison with other service providers.<br />
• Condoms freely available<br />
Make condoms freely available recurringly 2 , in accordance with a protocol<br />
ensuring adequate explanation for effective use, information and referral to other<br />
services is readily available.<br />
• Saturday morning clinic<br />
Extend End House contraceptive provision available on Saturday morning. This<br />
commenced February 2001.<br />
• Training for other service providers<br />
End House staff would offer training to other groups e.g. youth workers, teachers,<br />
other family planning clinic providers.<br />
• Improve Chester-le-Street Clinic<br />
Modify current service to make it more suitable for young people .<br />
• Central booking<br />
Trusts to develop a central booking system to ensure easy access to family<br />
planning clinics. There have been funding issued around obtaining hardware to<br />
support this. So this may not be a viable option.<br />
• Staff trained to work with young people<br />
Trusts to ensure all staff in family planning clinics have regular training in working<br />
with young people.<br />
• Contraceptive care services<br />
Encourage a shift in name from family planning clinics to contraceptive care<br />
services, young people’s clinics or other broader term.<br />
• Protocol for follow up to emergency contraception<br />
2 Recurring funding has been identified in <strong>Durham</strong>/Chester-le-St, The Dales and Sedgefield and non-recurring funding in<br />
Derwentside and Darlington. Services currently doing this report increased use by young men, and the pilot scheme in<br />
<strong>Durham</strong>/Chester-le-Street demonstrated more men using the GP based service than family planning clinics. The Sedgefield<br />
pilot will be in place from 1 st April 2000, usage will be monitored on a quarterly basis, with annual evaluation.<br />
30
Develop a protocol for the consistent follow up of young people using emergency<br />
contraception including the provision of information about local services for young<br />
people, printed information about contraception and accessing services, and the<br />
offer of an appointment with a local clinic/service.<br />
• Out of hours provision<br />
Publicise access to emergency contraception via NHS Direct.<br />
• Emergency contraception from nurses<br />
Explore protocol development for provision of emergency contraception by<br />
Community Nursing and Family Planning Staff.<br />
• New emergency contraception<br />
Encourage all prescriptions for emergency contraception to use the newly<br />
available form which is more efficient and has fewer side effects.<br />
• Dedicated young people’s services<br />
Ensure there is at least one service per PCG (ideally per main population centre)<br />
dedicated to young people, at a suitable time, with staff trained to work with<br />
young people and systematic user involvement in assessing the quality of<br />
service.<br />
• Publicity for contraceptive services<br />
Organise the collection, updating, printing and regular widespread distribution of<br />
information about sexual health advice, pregnancy testing and counselling and<br />
contraceptive provision within the PCG area.<br />
• Co-ordinated data collection<br />
Agree with all providers a co-ordinated approach to data collection in relation to<br />
uptake of contraceptive services by young people, in order to track improvements<br />
in relation to specific groups such as young men.<br />
• Reinforce condom use<br />
Support general awareness raising about appropriate contraceptive use for<br />
young people, particularly reinforcing the profile of condoms (properly used) as<br />
contraception as well as for protection from sexually transmitted infection.<br />
• Training for school nurses<br />
Ensure all school nurses are appropriately family planning trained e.g. level three<br />
training programme ‘Sexual Health’ accredited through the Tees and Region<br />
Open College Network. To ensure competence of those providing the service.<br />
• Drop in time maintained<br />
Ensure school nursing services are able to sustain ‘drop in time’ in each<br />
secondary school as a source of sexual health information and advice among<br />
other things. There is evidence that the role of school nurses can be effective.<br />
• Pilot condom distribution by school nurses<br />
Seek schools which are prepared to pilot school nurses distributing condoms in<br />
accordance with a suitable protocol.<br />
31
• Training for teachers<br />
Because of devolved budgets the training need expressed by personal social and<br />
health education co-ordinators must complete a six stage process in order to<br />
effect greater provision.<br />
1. Persuade Head Teacher<br />
2. Need identified to LEA<br />
3. LEA offers training<br />
4. INSET co-ordinator informs teachers<br />
5. Teacher applies<br />
6. Head agrees to provide cover.<br />
This sequence can break down at any stage. The recommendation is both to<br />
work hard on all stages of the process; and for the <strong>Teenage</strong> <strong>Pregnancy</strong> Unit to<br />
identify ring fenced funding.<br />
Teachers should be encouraged to take up the level three sexual health training<br />
module accredited through the Tees and Region Open college network.<br />
• Resources for teachers<br />
The range of resources available to assist teachers in delivering sex and<br />
relationships education should be expanded. Allocation of a specific budget for<br />
provision in this area would be an important step forward on a school by school<br />
basis. Enhancement of the resources available from Specialist Health Promotion<br />
Services could be a cost effective way of increasing access to up to date relevant<br />
materials.<br />
• Curriculum development in years 8 & 9<br />
On going work with personal, social and health education co-ordinators should<br />
emphasise the importance of developmental delivery including years 8 & 9, and<br />
addressing areas important to young people particularly relationships skills,<br />
practical approaches to using contraceptives, and access to local contraceptive<br />
advice. Research elsewhere shows the importance of skills in practical<br />
negotiation. The teacher needs to be relevant to high risk situations e.g. after<br />
drinking alcohol.<br />
• School governor training<br />
There has been an input to school governor training in <strong>County</strong> <strong>Durham</strong> LEA for<br />
some time. This work needs to be enhanced.<br />
• Fair Play<br />
Encourage the development of all projects that increase the scope of young<br />
people aspirations.<br />
• Connexions<br />
As part of the longer term action plan the Careers Service will be working more<br />
closely with the Youth Service, Educational Welfare, and Learning Support<br />
Service in order to develop a holistic approach. The Connexions <strong>Strategy</strong> could<br />
32
enable this range of services to provide a multidisciplinary approach to reducing<br />
teenage pregnancy, and to the provision of education other than at school.<br />
• Joined up Services<br />
Make more explicit links between community nurses e.g health visitors, school<br />
nurses, midwives, practice nurses and GP’s, and the support available from<br />
careers, youth workers, educational welfare officers, learning support services.<br />
• Contraceptive provision in colleges<br />
Some colleges would like to encourage provision of contraceptive care services<br />
on site and should work with their Primary Care Group and Trust colleagues to<br />
enable this to happen. All colleges should be encouraged to make condoms<br />
available as a minimum.<br />
• Staff training in colleges<br />
Some colleges would like in service training for staff from health professionals in<br />
order to ensure an accurate and appropriate information is being delivered.<br />
Staff should be encouraged to take up the level three training programme<br />
accredited through the Tees and Region Open College Network.<br />
• Contraceptive provision in the youth setting<br />
Expand on contraceptive provision in the youth setting if consultation with young<br />
people indicates that this is an appropriate source of contraceptive provision. This<br />
would require fresh resources or the reallocation of resources from traditional<br />
family planning clinics. This should not reduce the quality or level of service for<br />
other client groups.<br />
• Training for foster carers<br />
Ensure health promotion skills generally and sexual health specifically form part<br />
of the recruitment, development and basic training package offered to foster<br />
carers in both <strong>Durham</strong> and Darlington (“Payments for Skills Training<br />
Programme”). If appropriate consider extending this basic training for some<br />
carers who specialist for example in work with girls at risk.<br />
• Training for residential staff<br />
Include health promotion skills generally and sexual health specifically as part of<br />
the NVQ Level 3 staff development and training programme related to children’s<br />
homes, which includes the module on young peoples health and development.<br />
Develop links with Specialist Health Promotion Services, providers of sexual<br />
health advice and contraception to support delivery of this programme.<br />
• Enhanced training of “resource staff”<br />
Develop a model in which some children’s home staff act as a “resource person”<br />
who has done accredited training in relation to health promotion theory, skills and<br />
methods and specific subject areas including sexual health, in order to give<br />
generic staff backup in the form of advice, discussion, and access to materials, in<br />
their relationships with young people where sexual health issues arise.<br />
33
• Partnership agreement with carers<br />
<strong>County</strong> <strong>Durham</strong> Looked After System to develop a Partnership Agreement with<br />
the Careers Service for the children in care sector.<br />
• Dissemination of information<br />
Providers of information, resources, sexual health advice to ensure delivery to<br />
relevant access points including residential homes, social security offices, social<br />
services etc.<br />
• Youth Offenders and <strong>Teenage</strong> <strong>Pregnancy</strong> data<br />
Include information about links with teenage pregnancy in the baseline data<br />
collection exercise for young offenders, in order to focus on the specific links, and<br />
inform future progress.<br />
• Young Offenders Institutions<br />
Work with all young offenders institutions to ensure issues of sexual health and<br />
contraception are addressed. Include all Young Offenders Institutions and the<br />
Probation Service in the next development of this Action Plan.<br />
• Improve communication with parents<br />
Improve communication with parents from both schools and health agencies.<br />
This includes informing parents of sex education in the curriculum, in the primary<br />
school setting as well as the secondary school setting.<br />
• Parents as Educators training<br />
Train trainers and training key stakeholders such as school governors to develop<br />
awareness of possible approaches to sex education.<br />
• Improve access to resources<br />
Make widely available access to health education resources available to support<br />
parents, including lending books and packs to parents, putting suitable pre<br />
schools books in the book loan scheme, ensuring a wide range of leaflets is on<br />
display, providing work sheets in school that children can finish with parents help,<br />
and disseminating <strong>Teenage</strong> <strong>Pregnancy</strong> Unit campaign materials for parents on<br />
talking to their children about sex.<br />
• Consistent advice and support<br />
To work with PCGs, Trusts and Social Services to ensure equitable access to<br />
help and advice from all services is consistently offered to young women as soon<br />
as possible after the pregnancy is confirmed.<br />
• Provision of childcare facilities<br />
The young people are dependent upon family support to care for the baby while<br />
they are attending the groups or school. Some young people do not have this<br />
support. There are plans to pursue this issue through involvement in the Sure<br />
Start initiatives within <strong>County</strong> <strong>Durham</strong> linked to Early Years Childcare<br />
Partnerships.<br />
34
• Develop more structured follow up and support of pupils when they leave<br />
the alternative provision<br />
Although return to school is planned there is no specific outreach/back up support<br />
available for those young people who do not re-engage or who find attendance in<br />
school difficult to maintain.<br />
• Improve Curriculum access<br />
The part-time nature of the alternative provision and the appointment of a single<br />
teacher in each group restricts access to abroad curriculum. Moving towards fulltime<br />
provision and the recruitment of specialist subject would improve curriculum<br />
access.<br />
• Improve professional development of staff<br />
Currently the teachers are employed on part time/casual contracts, which means<br />
they are often excluded from training opportunities.<br />
• Improve the expectation and reality of returning to school<br />
The expected rapid return to school/college faced by young mothers can result in<br />
their dropping out rather than re-engaging in education;<br />
The expectation of returning to school should remain. However, in reality some<br />
young people do not return to school. More flexibility is needed to ensure all<br />
young people remain engaged in some form of education.<br />
• Resources for groupwork<br />
The lack of affordable base/office space for existing professionals to set up any<br />
support group/group work programme. There is a need for resources to allow<br />
successful group work to take place.<br />
• Improve the scope and co-ordination of projects aimed at prevention<br />
There is currently a sporadic and uncoordinated approach to involving these<br />
young parents in schemes promoting the prevention of teenage pregnancy e.g.<br />
peer mentoring schemes.<br />
• Develop wider plans for a range of semi-supported accommodation for<br />
teenage parents<br />
Extend the Darlington scheme using <strong>Local</strong> Authority and Housing Association<br />
Accommodation to make supported accommodation more widely available, with a<br />
variety of formats. This could include providing support in individual<br />
accommodation a form of ‘fostering’ cum tenancy with another family, or<br />
accommodation shared with other young people. The Quality protects work in<br />
<strong>County</strong> <strong>Durham</strong> to develop voluntary sector provision for people with particular<br />
needs could be expanded on. The Social Exclusion Unit report criteria will be<br />
borne in mind and the changes in housing benefits will influence both provision<br />
and take-up. The Northern Consortium of Housing Authorities will provide a coordinating<br />
lead for <strong>County</strong> <strong>Durham</strong>.<br />
• College creche facilities<br />
Work with local colleges to improve creche provision especially for under two’s.<br />
35
• Work with young men<br />
Work to develop effective ways to involve young men in the prevention of<br />
teenage pregnancy. This will involve a range of measures, some included<br />
elsewhere in this report ( eg, the Investing in Children Group referred to in section<br />
4 is likely to include young men, the results of Contraceptive Awareness Week<br />
included young men “trying out” local contraceptive service providers).<br />
Publicity related to well by young men could be part of the development.<br />
Investigation to follow up with young men who are using services (eg Annfield<br />
Plain, End House, South <strong>Durham</strong> Health Care) could identify what the key factors<br />
are and enable these to be more widely utilised.<br />
• Sexual Health Forum<br />
Consider establishing a Sexual Health Forum for Easington and<br />
<strong>Durham</strong>/Chester-le-Street and Derwentside, if there is local practitioner support.<br />
• Research into young women’s choices generating educational materials<br />
A local research project could involve young women’s pathways. The project<br />
would produce narrative data to enable further exploration of what makes a<br />
difference in relation to the “choices” and “decisions” young women make. One<br />
idea is to collect data from pairs of friends where one has become a teenage<br />
mother and the other not, but where they are demographically matched with the<br />
same school background and peer group. Outputs from the project would be<br />
materials to feed back into schools.<br />
A different approach to a similar idea could involve cross generational work such<br />
as discussion/focus groups involving single gender 15/25/35 year olds to explore<br />
changing views and experiences of sex and sexual health. The project would cut<br />
across current generational boundaries in relation to parents/teachers/health<br />
workers versus young people, and yet move beyond peer education and the<br />
problems attached to it. The learning would not necessarily be one directional,<br />
and could begin to break down the them/us barrier. Resources to be sought<br />
separately from Research Funds.<br />
• Developing best practice<br />
Ensure local evaluation and monitoring contributes to developing good practice,<br />
and that local developments use evidence generated nationally and<br />
internationally. If a co-ordinator is funded this could be part of his/her brief.<br />
Suggestions to the <strong>Teenage</strong> <strong>Pregnancy</strong> Unit nationally<br />
• Payment for male contraceptive care<br />
A change in the payment system to enable GP’s to claim for male contraceptive<br />
care including giving advice and condoms would be of great benefit in<br />
encouraging service delivery attractive to young men in the Primary Care setting.<br />
• Enhance the role of Colleges<br />
Colleges are an important venue where many 16 – 18 year olds attend, who can<br />
be offered support through the college setting currently provision is patchy. There<br />
should be a national recommendation to colleges to encourage a consistent<br />
36
approach in this area including availability of condoms. There should also be a<br />
national push to increase creche facilities, particularly for under twos.<br />
37
• Sex and relationships education as part of citizenship<br />
There is a need to highlight sex and relationships education as an important<br />
component of citizenship, in terms of a sense of self, identifying a wide range of<br />
options in terms of futures, and raising young people’s aspirations; there is also a<br />
need to prioritise practical aspects of sex and relationships education, with a<br />
particular focus on relationships skills such as negotiation, and practical skills in<br />
relation to effective contraceptive use.<br />
• Develop up to date sex positive materials<br />
There is a national shortage of good up to date relevant and sex positive<br />
materials for sex and relationships education which would be met more cost<br />
effectively in terms of appropriate piloting and development work at a national<br />
level. Where there are materials there needs to be a national strategy to make<br />
sure they are accessible to schools (this requires a budget, and teacher training<br />
to use them).<br />
• Ring fenced funding for teacher training<br />
There is an identified need at least for the short term, to ring fence funding to<br />
ensure training on sex and relationships education is available to teachers, with<br />
cover provided.<br />
• Advice for teenage parents<br />
Make available advice for teenage parents (Health, Social Services, Benefits etc)<br />
through an existing phone line and publicise widely targeted to young women at<br />
the point when pregnancy is first confirmed.<br />
• Research and Development budget<br />
There is a need to prioritise research into the prevention of teenage pregnancy in<br />
order to continue to develop the evidence base nationally, for example through a<br />
ring fenced budget.<br />
38
PART A<br />
SECTION 3<br />
40
LOCAL MEDIA CAMPAIGN<br />
42
<strong>Local</strong> Media Campaign<br />
<strong>County</strong> <strong>Durham</strong> and Darlington<br />
Strategic Vision<br />
- The local media campaign will reinforce those messages given in the<br />
national campaign as well as enabling the following things to happen.<br />
- Young people will receive information about local services through a<br />
variety of media sources. They will be able to access that information<br />
easily and it will be presented in a form that is useful to all young people.<br />
The local media campaign will move forward from the start with innovative<br />
practice and using a selection of media forms, including credit card sized<br />
information cards, posters and a website based on local information about<br />
advice and services in <strong>County</strong> <strong>Durham</strong> and Darlington.<br />
- It will be the responsibility of a specific post holder to ensure that accurate<br />
and up to date information on services is collected. That information will<br />
be fed to the Tackling <strong>Teenage</strong> <strong>Pregnancy</strong> Co-ordinator who will organise<br />
its collation, distribute it to Sexwise and to local sources as follows:<br />
There will be agreements with local businesses and organisations so that<br />
there is a procedure for replacement of posters and other materials as<br />
they become old, out of date or stolen. Links with the Specialist Health<br />
Promotion Service and library service will be used for this.<br />
43
<strong>Local</strong> Media Campaign<br />
Risk Assessment Of Current Service Provision<br />
Strengths<br />
- <strong>County</strong> <strong>Durham</strong> has successfully piloted a website for young people in the<br />
Looked After System and has now launched it <strong>County</strong> wide. The Looked<br />
After Network can be viewed at ‘www.careon-line.greatxscape.net’<br />
- <strong>County</strong> Health Promotion Specialist Communications lead has good links<br />
with local newspapers.<br />
- A Website for the Healthy Schools Initiative has already been established<br />
for <strong>County</strong> <strong>Durham</strong> and Darlington.<br />
- The Specialist Health Promotion Service Communications lead has good<br />
specialist knowledge and experience, and has a background in journalism.<br />
- The Health Promotion Service Resource Library for <strong>County</strong> <strong>Durham</strong> and<br />
Darlington is on-line and young people are encouraged to access the<br />
library and to open their own accounts so that they can borrow any of the<br />
resources.<br />
- There are strong links between the Specialist Health Promotion Service<br />
Communications Lead and local authorities.<br />
Weaknesses<br />
- This will be the first campaign specifically aimed at tacking teenage<br />
pregnancy.<br />
Opportunities<br />
- There are no precedents which have to be followed and so there are more<br />
opportunities to develop new partnerships and new ways of working.<br />
- Opportunities to develop partnerships with local businesses which may be<br />
usefully included in the local media campaign.<br />
Threats<br />
- It is acknowledged that young people don’t read newspapers and so<br />
information communication technology or ‘new media’ is more appropriate<br />
to target young people.<br />
44
1. Approach to planning and advertising services<br />
All services provided for young people by Voluntary Agencies, Community<br />
Education and Youth Services, Sexual Health Outreach Workers, Health<br />
Agencies etc. will be advertised in sensitive and appropriate ways. For each<br />
service advertising will be planned in a shared forum which will include the<br />
Tackling <strong>Teenage</strong> <strong>Pregnancy</strong> <strong>Local</strong> Implementation Co-ordinator, the Health<br />
Promotion Services Communication Lead, the <strong>County</strong> Sexual Health Outreach<br />
Workers, young people and representatives from the agencies whose services<br />
are to be advertised. The method of advertising will be dependant on the<br />
particular service being advertised, the most appropriate method will be chosen<br />
by the group including young people.<br />
2. Getting the message to young people / Involvement of young people<br />
in the development and distribution of information<br />
We will consult with and involve young people in developing the content for<br />
sexual health and relationship education on the health promotion website<br />
(www.health-promotion.org.uk/name to be arranged) that will contain relevant<br />
local information such as young peoples clinics. It could also contain a direct link<br />
into the Sexwise database at www.ruthinking.co.uk<br />
There will also be a website and intranet system incorporating tackling teenage<br />
pregnancy on the Social Services Department (SSD) IT System which will be<br />
accessible by all SSD staff. It will have links to other relevant sites and will give<br />
details of relevant documentation. In addition there will also be links to those<br />
documents and the <strong>County</strong> <strong>Durham</strong> Tackling <strong>Teenage</strong> <strong>Pregnancy</strong> <strong>Strategy</strong>.<br />
The Health Promotion website will provide links and information which will direct<br />
sexual health/relationships page users to the Health Promotion Information and<br />
Resource Library (www.health-promotion.org.uk/hpac) which has direct links to<br />
quality websites on sexual health and relationships. Some teachers are already<br />
familiar with the resources on offer from the Resource Library and can place<br />
orders for sexual health/relationships material (including the sex, are you thinking<br />
about it materials) on-line for use in PSE classes. The Library has the capacity to<br />
put these materials on-line in a downloadable format if copyright permission can<br />
be secured. Several hundred students also have passwords that enable them to<br />
order materials on-line. Information on materials carried by the Library is not<br />
password protected and anyone can browse the catalogue.<br />
The Healthy Schools pages on the website (www.healthpromotion.org.uk/schools)<br />
are also currently under development and will have<br />
reciprocal links to the sexual health and relationship pages and the Resource<br />
Library.<br />
The Health Promotion site also has the capacity to develop a chat room,<br />
message board or discussion list for teenagers. The type of communication<br />
vehicle chosen would depend on the outcome of consultation with teenagers.<br />
Publicity for the site would be generated through local print media, through direct<br />
contacts already established by the Information & Resource Library’s database<br />
and other forms of direct contact. This could also include Library contacts with<br />
45
professionals working with vulnerable young people. Health Promotion<br />
Specialists are also a crucial link for promoting this.<br />
Usage of the site and requests for information from the Library can be gained<br />
from the web server.<br />
Young people will be consulted to gain an understanding of how they would like<br />
to see the local website develop, what information they would like to see on it and<br />
what it should be called. This will be done by using links already forged with<br />
Education, Social Services and Voluntary Organisations.<br />
3. Plans for using and adapting national campaign materials<br />
All local plans for advertising will be made in reference to the national campaign.<br />
In <strong>County</strong> <strong>Durham</strong> we intend to particularly use nationally produced posters and<br />
post cards in conjunction with locally produced posters and credit card sized<br />
information cards. Messages of the national campaign which we will particularly<br />
reinforce are:<br />
- You can get free confidential advice and information about contraception<br />
whatever your age.<br />
- If you are sexually active, use contraception (to prevent pregnancy and<br />
Sexually Transmitted Diseases).<br />
4. Young Men and Vulnerable Young People<br />
As well as the website, posters and small cards will be distributed throughout the<br />
county detailing local services and giving telephone numbers of relevant sources<br />
of information and advice. The small cards will be used in two ways. Firstly,<br />
there will be a pilot scheme for the county which will run in the Sedgefield PCG<br />
area. Credit card sized information cards will be placed in supermarkets where<br />
pregnancy testing kits can be obtained and they will be included in pregnancy<br />
testing kits dispensed by pharmacists. They will detail telephone numbers of a<br />
range of sources of advice and information. A second pilot scheme in the Dales<br />
locality will involve a dual-sided credit type card which will enable young people<br />
to obtain condom or emergency contraception simply by handing over the card to<br />
any GP’s Surgery within the PCG area. It will be advertised by an accompanying<br />
poster and by an information leaflet which also folds to credit card size. The<br />
posters and cards will be placed in areas where young people can easily see<br />
them and where they can read them privately. Links with local cafes, fast food<br />
outlets, leisure centres, local transport companies and other areas requested by<br />
young people will be forged and developed, and the links already established<br />
with Community Education, Youth Offending Team (YOT), Youth Services, the<br />
Voluntary Sector and Sexual Health Outreach Workers will be used to enable<br />
boys and vulnerable young people to access information in places which they are<br />
at ease and private. For instance, posters and credit card sized information<br />
cards will be placed on the back of toilet doors so that young people can read the<br />
information privately and without being seen by peers or anyone else. The<br />
information cards will be placed in toilets so that young people can take them<br />
away and read them later. Information can also be disseminated to young people<br />
in the Looked After System by incorporating sexual health issues into existing<br />
publications such as the quarterly mail shot ‘Who Cares’. The Investing in<br />
46
Children newsletter would also be a useful means of delivering sexual health<br />
information.<br />
5. Directories of Services<br />
A directory of services has been produced for <strong>County</strong> <strong>Durham</strong> and Darlington<br />
and has been forwarded to the Sexwise database. We envisage that there will<br />
be two types of directory of services in <strong>County</strong> <strong>Durham</strong> and Darlington in addition<br />
to this. There will be a directory intended for use by professionals. This will<br />
enable any professional, education, voluntary sector, social services or health<br />
based to access information quickly and easily should a young person approach<br />
them for that information.<br />
The second directory will be designed by young people and it is intended that any<br />
young person would be able to use this directory directly without having to<br />
approach an intermediary adult. This will enhance the opportunity for young<br />
people to be empowered and to take control of their own sexual health. This<br />
directory could be included in already existing publications for young people such<br />
as the Social Service booklets.<br />
It will be the responsibility of the Tackling <strong>Teenage</strong> <strong>Pregnancy</strong> Co-ordinator to<br />
distribute the directories to relevant agencies and young people’s groups.<br />
6. Details of Services<br />
Details of services will be actively advertised in schools, Health buses, Youth<br />
Clubs, Voluntary Sector, Drop in Services and other places where young people<br />
meet. Again, this will involve local businesses and employers. Links with the<br />
Health Promotion Specialist (HPS for the work place have been made and young<br />
people at work can be targeted in advertising health services.<br />
7. The <strong>Local</strong> Media <strong>Strategy</strong><br />
The local media strategy will be constantly reviewed to ensure that it gives<br />
messages which are consistent with the national campaign and to enable young<br />
people to be involved in the review and evaluation of the local media strategy.<br />
This will ensure that the messages which are given out are relevant and<br />
appropriate in their content and are being displayed in places where young<br />
people can access the information contained there in.<br />
Print media/newspapers will be used to maintain the profile of the Tackling<br />
<strong>Teenage</strong> <strong>Pregnancy</strong> work throughout <strong>County</strong> <strong>Durham</strong> and Darlington. Press<br />
releases and follow ups and radio. Wherever possible the work of difference<br />
agencies, voluntary sector, young peoples groups will be highlighted in this way.<br />
But the advertising of information and services directed at young people will be<br />
through other means (as detailed earlier) to ensure that young people have<br />
access to the messages, they can access the messages privately and they are<br />
therefore given every opportunity to retain the information which they need.<br />
47
LOCAL MEDIA CAMPAIGN – 10 YEAR STRATEGY<br />
Issue Task Planned<br />
Action/Goals<br />
S.E.U. 1. Inform the 1. Sexual Health<br />
Action national Outreach Workers &<br />
Point 15 helplines, TP Co-ordinator to<br />
e.g. Sexwise ensure local<br />
information is accurate<br />
and up to date<br />
2. Tackling <strong>Teenage</strong><br />
<strong>Pregnancy</strong> Coordinator<br />
distributes<br />
information to local<br />
agencies, young<br />
peoples groups<br />
3. National help-line<br />
telephone numbers will<br />
be displayed on local<br />
information<br />
Timescale Who/Lead Assumptions/<br />
Risks, Comments<br />
1. 2001 to 1. <strong>Teenage</strong> <strong>Pregnancy</strong> Co- 1. Assumes there will be<br />
2010<br />
ordinator with SHPS<br />
someone free to do the work<br />
2. 2001 to<br />
2010<br />
3. 2001 to<br />
2010<br />
48<br />
2. <strong>Teenage</strong> <strong>Pregnancy</strong> Coordinator<br />
3. <strong>Teenage</strong> <strong>Pregnancy</strong> Coordinator<br />
with relevant<br />
members of media forum<br />
detailed in text section 1<br />
2. Suggest that any organisation<br />
changing any details about their<br />
service be required to inform the<br />
central database holder so<br />
Sexwise can be kept up to date<br />
3. Risk = some local agencies<br />
may want only local information<br />
on their advertising
LOCAL MEDIA CAMPAIGN – THREE YEAR ACTION PLAN<br />
S.E.U.<br />
Action<br />
Point 16<br />
1. Get young<br />
people to<br />
seek advice<br />
– local<br />
campaign<br />
1. Establish Media<br />
Forum<br />
2. Consult young<br />
people about local<br />
website<br />
3. Develop website<br />
according to results of<br />
no. 2<br />
1. 2001<br />
2. 2001<br />
3. 2001<br />
ongoing<br />
49<br />
1. <strong>Teenage</strong> <strong>Pregnancy</strong> Coordinator,<br />
Sexual Health<br />
Outreach Workers, SHPS &<br />
Communications Lead<br />
2. <strong>Teenage</strong> <strong>Pregnancy</strong> Coordinator,<br />
SHPS &<br />
Communications Lead<br />
3. SHPS & Communications<br />
Lead<br />
1. Will have to take place out of<br />
school hours so that young people<br />
can attend<br />
2. Will have to take place out of<br />
school hours so that young people<br />
can attend<br />
3. Website will have links to<br />
national websites and local<br />
Healthy Schools site & Health<br />
Promotion Sites & to the<br />
Connexions website
LOCAL MEDIA CAMPAIGN – THREE YEAR ACTION PLAN<br />
S.E.U.<br />
Action<br />
Point 16<br />
S.E.U.<br />
Action<br />
Point 16<br />
1. Get young<br />
people to<br />
seek advice<br />
– local<br />
campaign<br />
1. Get young<br />
people to<br />
seek advice<br />
– local<br />
campaign<br />
1. Develop ‘credit<br />
card’ of telephone<br />
no’s pilot re:<br />
pregnancy testing kits<br />
2. Launch cards with<br />
pharmacies and<br />
supermarkets<br />
3. Develop credit<br />
card pilot and launch<br />
more PCG area<br />
4. Use local media<br />
forum to plan<br />
posters/cards for local<br />
use<br />
1. Establish links with<br />
local business and<br />
transport companies<br />
2. Launch local<br />
cards/posters<br />
1. Jan 2001 to<br />
April 2001<br />
2. July 2001<br />
3. 2001<br />
4. 2001 to 2002<br />
1. 2001/2002<br />
2. 2001/2<br />
50<br />
1. PCG <strong>Teenage</strong> <strong>Pregnancy</strong><br />
Planning Group<br />
2. PCG <strong>Teenage</strong> <strong>Pregnancy</strong><br />
Planning Group<br />
3. SHPS, <strong>Teenage</strong> <strong>Pregnancy</strong><br />
Co-ordinator & PCG<br />
4. <strong>Teenage</strong> <strong>Pregnancy</strong> Coordinator<br />
& Media Forum<br />
1. <strong>Teenage</strong> <strong>Pregnancy</strong> Coordinator<br />
2. <strong>Teenage</strong> <strong>Pregnancy</strong> Coordinator<br />
& Media Forum<br />
3. Will be closely evaluated and<br />
extended to non-clinical settings<br />
Must be out of school hours to<br />
ensure the input of young people<br />
1. Build relationships to ensure<br />
smooth operationalisation of<br />
advertising advice and sexual<br />
health services<br />
2. Pilot schemes will be already<br />
underway and being evaluated, the<br />
county posters/cards scheme can<br />
draw on that evaluation information
LOCAL MEDIA CAMPAIGN – THREE YEAR ACTION PLAN<br />
S.E.U.<br />
Action<br />
Point 16<br />
S.E.U.<br />
Action<br />
Point 17<br />
S.E.U.<br />
Action<br />
Point 17<br />
1.Get young<br />
people to<br />
seek advice<br />
– local<br />
campaign<br />
2.Get young<br />
people to<br />
seek advice<br />
– local<br />
campaign<br />
1. Develop checklist/<br />
Directory of Services<br />
for professionals<br />
2. Develop Directory<br />
of Services for young<br />
people<br />
1. Publicity 1. Seek print media<br />
coverage<br />
1. Publicity Develop SSD Website<br />
for professional re:<br />
Tackling <strong>Teenage</strong><br />
<strong>Pregnancy</strong> Links to<br />
relevant<br />
documents/directory<br />
for services for<br />
professional use<br />
1. 2001 /2002<br />
2. 2002<br />
51<br />
1. <strong>Teenage</strong> <strong>Pregnancy</strong> Coordinator<br />
& Media Forum<br />
2. <strong>Teenage</strong> <strong>Pregnancy</strong> Coordinator<br />
& Media Forum<br />
1. 2001 1. <strong>Teenage</strong> <strong>Pregnancy</strong> Coordinator<br />
& Communications<br />
Lead<br />
1. 2001 to 2002 1. SSD Communications/<br />
I.T. Lead<br />
1. Use that produced for Sexwise<br />
database initially<br />
2. Sexual Health Outreach<br />
Workers & Voluntary Sector will<br />
have links with young people<br />
1. Use to launch strategy & at<br />
intervals to maintain the profile of<br />
Tackling <strong>Teenage</strong> <strong>Pregnancy</strong><br />
1. Can link with website produced<br />
by <strong>County</strong> Communications Lead
BETTER SEX & RELATIONSHIPS<br />
EDUCATION (SRE)<br />
52
Better Sex & Relationship Education (SRE)<br />
<strong>County</strong> <strong>Durham</strong><br />
VISION<br />
VISION STATEMENT FOR SEX AND RELATIONSHIPS EDUCATION<br />
Sex and relationships education is part of a lifelong process of learning<br />
information and skills, forming beliefs, values and attitudes about sex,<br />
sexuality, sexual health and emotions. It should involve a range of<br />
agencies, parents and carers, along with young people themselves as<br />
peer educators, in supporting children and young people to cope with<br />
adolescence and prepare them for an adult life in which they can:<br />
• Be aware of and enjoy their sexuality<br />
• Behave responsibly within personal and sexual relationships and<br />
understand the consequences of their actions<br />
• Communicate effectively<br />
• Have sufficient information and skills to protect themselves and, where<br />
they have one, their partner from unintended/unwanted conceptions,<br />
and sexually transmitted infections including HIV<br />
• Access confidential advice and support<br />
• Avoid being exploited or exploiting others<br />
• Develop positive values and moral framework that will guide their<br />
decisions, judgements and behaviour.<br />
53
Better Sex & Relationship Education<br />
The Current Position – Where We Are Now<br />
1) Implementation of DFEE guidelines on Sex & Relationship ensuring<br />
all secondary schools are delivering Sex & Relationship Education<br />
• Emphasis is placed on consistency of information and also liaison with<br />
Health Promotion Services.<br />
• Healthy Schools Standards adhered to.<br />
• Continue to offer training support for staff, in and out of school as part of<br />
the Healthy School Standards, both for knowledge updating and<br />
development of delivery skills.<br />
• Continue to work with School Nursing Teams to identify priorities,<br />
including support work in schools.<br />
• On-going monitoring of delivery of sex and relationship education<br />
through Healthy Schools Standards Audit Mechanism.<br />
• Continue to improve liaison in PSHE networks.<br />
• Continue to plan sex and relationship education programmes relating to<br />
the needs of the young people, by consulting with them.<br />
• Continue to offer training for primary school teachers, on the delivery of<br />
SRE.<br />
• Continue to support and promote “the Sex Education Road Show” and<br />
other ad hoc events in schools, linked to Healthy Schools Standards, i.e.<br />
Contraception Awareness week/ North East Area AIDS Day.<br />
• Continue close liaison with the School Nursing Service, several of whom<br />
have undergone Family Planning Training and are therefore not only<br />
involved in the delivery or advising on contraception care in schools, but<br />
also in the local Family Planning Clinics and Young Peoples Centres.<br />
Lead<br />
The lead on the these tasks would be shared by a multi-disciplinary group<br />
consisting of Health Promotion Services, LEA, School Nursing Service,<br />
Healthy Schools Standards Steering Group and individual schools.<br />
54
Timescale<br />
• On-going - delivery of staff training.<br />
• 2001 – onwards for the development of tasks and identification of<br />
priorities.<br />
• 1 year – all schools made aware of guidance.<br />
• 2-3 years – all schools understand the content and requirements.<br />
• 3-5 years – programme planning in consultation with young people.<br />
• 3-5 years – provide examples of delivery models, i.e. develop a team of<br />
skilled, confident, interested teachers to deliver sex and relationship<br />
education.<br />
• 3-5 years – Healthy Schools Audit for external monitoring.<br />
2) Addressing the needs of young people at risk and in high rate areas<br />
• Continue to encourage engagement of schools in high risk areas, with<br />
regard to the Healthy Schools Standards. Promotion could be developed<br />
via the internet, PSHE meetings and networking and school profiling.<br />
• Continue to work with schools in high risk areas and encourage them to<br />
work on the sex and relationship education standard involving students<br />
in discussion and planning.<br />
• Continue to provide guidance on sex and relationship education in outof-school<br />
settings, i.e. provision for excluded children, children of<br />
Travellers and children in the looked-after-system, by developing training<br />
and awareness raising for identified staff, working in tandem with Health<br />
Promotion Services and the Community Education Service.<br />
• Re-integration of teenage mothers, into the school setting, with increased<br />
emphasis on the post of the Re-integration Officer, with possible<br />
mainstreaming of this post with additional funding.<br />
• There is a peer education project in one PCG area.<br />
• To date, there is part-time support and educational provision for teenage<br />
mothers, which should be extended to full time.<br />
• Continue increased emphasis on development of Connexions Service<br />
role. Connexions Advisors will be invited to be members of local<br />
<strong>Teenage</strong> <strong>Pregnancy</strong> Action Groups and the <strong>County</strong> Advisor will continue<br />
to be part of the Steering Group.<br />
55
• Ensure quality of access to impartial advice and information through the<br />
development of “One Stop Shops” in schools and in the community as a<br />
pilot project. Funding would be requested.<br />
• Continue to support Sexual Health Outreach Workers in each PCG area<br />
whose work is primarily with young people at risk and in high rate areas.<br />
• Continue to work with Investors in Children.<br />
• Using a joined up approach to SRE across a variety of settings including<br />
the Looked After System, the Youth Offending System, the Youth<br />
Service and in alternative Provision we will reduce the likelihood of<br />
young people experiencing social exclusion in terms of educational<br />
underachievement.<br />
Lead<br />
Healthy Schools, Standards Partnership, Community Education Service<br />
including LEA, Youth Workers, Social Services, Investors in Children,<br />
Connexions Services, Sexual Health Outreach Workers.<br />
Timescale<br />
• To date, Sexual Health Outreach Workers, Health Promotion<br />
Professionals and Youth Workers are working with local young people on<br />
joint projects.<br />
• A Peer Education Project on the realities of young parenthood runs in<br />
Easington.<br />
• 1 year – provide guidance on sex and relationship education by offering<br />
training on DFEE Guidelines leading to the development of a policy for<br />
identified staff. Funding would be required.<br />
• 1 year – consider mainstreaming of Re-integrated Officers post within<br />
LSS. This would require additional funding of £35,000.<br />
• 1 year – full time support (at present, part-time) and educational<br />
provision for teenage mothers, would require extra funding of £10-<br />
12,000.<br />
56
3) Addressing single gender work and the needs of boys and young<br />
men<br />
• Continue to use the Healthy Schools Standards, ensuring equality and<br />
equity of provision.<br />
• Continue to liaise with young people to identify their needs.<br />
• Continue to work closely with Investors in Children.<br />
• Youth Workers to continue assessing and prioritising needs, their own as<br />
well as young peoples needs.<br />
• Continue to encourage young men to access services re: Family<br />
Planning Clinics and Young Peoples Centres, through information given<br />
in schools, Colleges, Youth Clubs and Leisure Centres.<br />
Lead<br />
Youth & Community Workers, LEA, Health Promotion Services, Community<br />
Education.<br />
Timescale<br />
• On-going work working with groups of young people and on one-to-one.<br />
• 1 year – essential that funding is continued for voluntary organisations,<br />
providing young people’s services i.e. End House Young Peoples<br />
Centre.<br />
4) In-service training and support for professionals, governors and<br />
parents/carers<br />
At present:<br />
• TROCN (Tees Regional Open College Network). Level III, an accredited<br />
programme is being offered for people who have a remit for, and an<br />
interest in, working in the field of sexual health promotion.<br />
This programme is in conjunction with Tees Open College Network and<br />
Specialist Health Promotion Services in <strong>County</strong> <strong>Durham</strong> (and Darlington)<br />
Primary Care Group.<br />
• School & Governor Support Unit on board.<br />
• Dedicated post in Easington.<br />
• Course for Governors – (Sex Education – Your School – Your<br />
Responsibility) gives them the opportunity to discuss new issues<br />
pertaining to sex and relationship education, and how to<br />
implement/improve sex education in their particular school.<br />
57
• Training for the trainers – set up when need identified.<br />
• School Nursing Service works closely with Schools & Health Promotion<br />
Service.<br />
• Regular up-dates for school nurses to take place at the beginning of each<br />
term – needs identified by the school nurses.<br />
• Training and updating on issues pertaining to young people and sexual<br />
health, has been undertaken by all members of Primary Health Care<br />
Teams in one local PCG area. Other PCG areas are at present planning<br />
similar programmes.<br />
• Courses for parents have been held in one PCG area.<br />
Future Plans<br />
• Develop TROCN Level III for teaching staff – a focussed shorter course<br />
which may depend on the availability of teachers able to attend.<br />
2001 - Establish a multi-disciplinary working group.<br />
2002 - Submission of the training programme.<br />
Develop or identify relevant training for Youth Workers, Education Social<br />
Workers, Residential Social Workers.<br />
• Develop TROCN Level II for parents and carers including foster parents<br />
by:<br />
2001 - establishing a multi-agency working group.<br />
2002 - Submission of the training programme.<br />
• Support in-school programmes for INSET.<br />
2002 - with the development of distance learning materials.<br />
• Work with the Governors through the Governor Support Unit of <strong>County</strong><br />
<strong>Durham</strong> (& Darlington).<br />
• Encourage participation by parents and carers – other local training events<br />
through the school and Health Promotion Services.<br />
• Identify staff training needs through the Healthy Schools Standard Audit.<br />
• Carry out audit of current training opportunities.<br />
• Joint training events for all involved in delivering/or working in the field of<br />
Sexual Health Promotion.<br />
• Joint working with LEA, Health Promotion Services, Community Education,<br />
Connexions, Youth Workers and School Nursing Service.<br />
58
5) Developing sex and relationship education policies in the youth<br />
services, residential homes etc.<br />
• Community Education Service is at present reviewing the current draft of<br />
the Sex and Relationship Education Policy and guidelines through an<br />
established Review Group, which will plan the progress and report on the<br />
review and recommendations.<br />
• Sex and relationship education is to become an integral part of the<br />
Community Education Service Youth Work Curriculum.<br />
The review of this curriculum will ensure that sex and relationship<br />
education will be prioritised in the statement guidelines by 2002.<br />
• There is a need for the establishment of a Sexual Health Worker post, to<br />
train and support the staff through the development of training<br />
programmes, 2002-2003, depending on funding available.<br />
• There is a need to broaden the range of learning opportunities around sex<br />
and relationship education, using the expertise of other professionals.<br />
• Work to continue with young people in the community using drama,<br />
community art workers, and community education workers and sexual<br />
health outreach workers.<br />
Future<br />
• It is important to have and develop training link with foster carers and<br />
residential social workers, regarding sex and relationship education.<br />
• Links can be developed between sexual health outreach workers and<br />
looked after networks.<br />
• It is crucial to have continued funding for End House, the Young Peoples<br />
Centre.<br />
• All of this work will help to ensure that young people are less likely to be at<br />
risk of social exclusion.<br />
6) Using young people / parents and carers as educators<br />
• Peer education and peer mentoring is underway in schools and Youth<br />
Services at present.<br />
• Involve parents and carers in discussion around sex and relationship<br />
education offering local supported mini-courses if requested.<br />
• Develop an accredited course for young people, peer led, as suggested in<br />
TROCNII/III guidelines, this is underway.<br />
This work is currently being discussed by several organisations and<br />
individuals, and could be undertaken by joint working with Health Promotion<br />
and Community Education.<br />
59
7) Mechanisms for Quality Assurance for delivery of Sex and<br />
Relationship Education<br />
• Auditing provision as part of the Healthy Schools Standard (<strong>County</strong><br />
<strong>Durham</strong> & Darlington).<br />
• Audit is active in all participating schools and then checked annually.<br />
• The audit tool is currently under review and will continue to be up-dated<br />
annually.<br />
• Continue to ensure consistent messages from the trainers by setting up<br />
joint training programmes for Health Authority and LEA Support Staff.<br />
Lead<br />
Healthy Schools Partnerships.<br />
Future<br />
• Development of a forum of providers to establish agreed quality standards.<br />
• Clarify the role of the School Nursing Service, i.e. involvement / provision,<br />
1-3 years.<br />
• Schools and school nurses to jointly audit the sex and relationship<br />
education delivered in schools, by setting up a working group with the LEA<br />
and School Nursing Service.<br />
8) Mechanisms for involving and consulting parents and young people,<br />
using a range of professionals<br />
• A multi-agency approach required.<br />
• Continue to encourage parents/carers to be involved with the school by<br />
setting up mini-courses for parents as carers/resources and inviting their<br />
comments on the sex and relationship education curriculum content.<br />
• Link with training organised by Social Services for foster carers.<br />
• Audit of student involvement using the Healthy School Standards, in<br />
individual schools. This is underway and will be on-going in participating<br />
schools.<br />
60
Child Care in local Colleges<br />
Further Education Colleges are committed to supporting teenage parents and<br />
their return to education.<br />
• Darlington College<br />
14 places from 2 years (Day Nursery)<br />
• East <strong>Durham</strong> & Houghall Community College<br />
55 places – day nursery – from birth (Students take priority)<br />
• Bishop Auckland College<br />
100 places – day nursery<br />
& (portable day care – nursery nurses attend to cover local community<br />
courses).<br />
• New College <strong>Durham</strong><br />
29 places – day nursery.<br />
• Derwentside College<br />
Derwentside College has a child care scheme with local nurseries and<br />
registered childminders to provide free childcare to all those who are<br />
eligible (including all 16 to 18 year olds).<br />
61
BETTER SRE – THREE YEAR ACTION PLAN<br />
Issue Task Planned Action/Goals Timescale Who/Lead Assumptions/<br />
Risks, Comments<br />
S.E.U. 1. New 1. Delivery of staff 1. Ongoing Multi-agency group of:<br />
Action Guidance on training.<br />
Health Promotion<br />
Point 8 SRE in 2. Development of 2. 2001 onwards Service, LEAs, School<br />
Schools tasks/identify priorities<br />
Nursing, Healthy<br />
SEU 1. New 1. All schools made 1. 2001/2<br />
Schools Steering<br />
Action Guidance on aware of guidance<br />
Group and Schools<br />
Point 8 SRE in All schools understand<br />
Schools the content and<br />
requirements<br />
Raise profile of<br />
Connexions<br />
2. 2001 to 2003<br />
S.E.U. 1. New 1. Programme planning 1. 2001 – 2006<br />
Action Guidance on in consultation with<br />
Point 8 SRE in<br />
Schools<br />
young people<br />
S.E.U. 1. New 1. Provide examples of 1. 2001 – 2006 Develop a team of skilled,<br />
Action Guidance on delivery models<br />
confident, interested teachers<br />
Point 8 SRE in<br />
to deliver sex and relationship<br />
Schools<br />
education<br />
S.E.U. 1. New 1. Health Schools Audit 1. 2001 –2006<br />
Action Guidance on for external monitoring<br />
Point 8 SRE in<br />
Schools<br />
62
SRE THREE YEAR ACTION PLAN<br />
S.E.U.<br />
Action<br />
Point 8<br />
S.E.U.<br />
Action<br />
Point 8<br />
S.E.U.<br />
Action<br />
Point 8<br />
S.E.U.<br />
Action<br />
Point 8<br />
1. New<br />
Guidance on<br />
SRE in<br />
Schools<br />
1. New<br />
Guidance on<br />
SRE in<br />
Schools<br />
1. New<br />
Guidance on<br />
SRE in<br />
Schools<br />
1. New<br />
Guidance on<br />
SRE in<br />
Schools<br />
1. Provide guidance on<br />
DFEE Guidelines<br />
leading to the<br />
development of a policy<br />
for identified staff<br />
1. Consider<br />
mainstreaming of<br />
Reintegration Officers<br />
within LSS<br />
1. <strong>Full</strong> time support<br />
(present part time) and<br />
educational provision for<br />
teenage mothers<br />
1. Working with groups<br />
of young people and one<br />
to one<br />
1. 2001 – 2002 Healthy Schools<br />
Standards<br />
Partnership, LEA,<br />
Youth Workers, Social<br />
Services, Investors in<br />
Children, Connexions<br />
Service<br />
Funding would be required<br />
1. 2002<br />
1. 2002 – 2010 Healthy Schools<br />
Standards<br />
Partnership, LEA,<br />
Youth Workers, Social<br />
Services, Investors in<br />
Children, Connexions<br />
63<br />
Service<br />
1. Ongoing Youth & Community<br />
Workers, LEA, Health<br />
Promotion,<br />
Community Education<br />
Would require additional<br />
funding of £35,000<br />
Would require extra funding of<br />
£10-12,000
SRE THREE YEAR ACTION PLAN<br />
S.E.U.<br />
Action<br />
Point 8<br />
S.E.U.<br />
Action<br />
Point 12<br />
S.E.U.<br />
Action<br />
Point 12<br />
1. New<br />
Guidance on<br />
SRE in<br />
Schools<br />
1. Continued support of<br />
voluntary organisations,<br />
e.g. End House<br />
1. New 1. 1. Develop TROCN<br />
Guidance on level III for teaching and<br />
SRE in inter agency staff as<br />
Schools follows:<br />
2. a) Establish a multidisciplinary<br />
working<br />
group<br />
3. b) Submission of<br />
training programme<br />
1.<br />
Awareness<br />
raising<br />
1. 1. Develop TROCN II<br />
training for parents and<br />
carers, establish multiagency<br />
group<br />
2. 2. Submission of<br />
training programme<br />
1. 2001 - 2002 Youth & Community<br />
Workers, LEA, Health<br />
Promotion,<br />
Community Education<br />
a) 2001<br />
b) 2002<br />
1. 2003/4<br />
2. 2002/2003<br />
64<br />
Education, Healthy<br />
Schools and partner<br />
agencies.<br />
Education, Healthy<br />
Schools, Social<br />
Services and others<br />
who work with<br />
parents.<br />
TROCN group<br />
A shorter course to enable<br />
more teachers and other<br />
professionals to attend.<br />
Flexibility of length of course<br />
restricted by TROCN<br />
regulations.<br />
Professor Sue Scott (University<br />
of <strong>Durham</strong>) is researching<br />
Parents as Sex Educators.<br />
Their interim report is available<br />
locally.
SRE THREE YEAR ACTION PLAN<br />
S.E.U.<br />
Action<br />
Point 12<br />
S.E.U.<br />
Action<br />
Point 8<br />
1.Awareness<br />
raising<br />
1. New<br />
Guidance on<br />
SRE in<br />
Schools<br />
1. Support in-school<br />
programmes for INSET<br />
1. Develop Distance<br />
Learning Materials for<br />
work with Governors,<br />
Parents/Carers<br />
1. Identify staff training<br />
needs through Healthy<br />
Schools Audit<br />
2. Audit of current<br />
training opportunities<br />
3. Joint training events<br />
for all involved in<br />
delivering or working in<br />
sexual health promotion<br />
1. Ongoing Education, Healthy<br />
Schools/Health<br />
Promotion Services<br />
1. 2002/3 Education, Healthy<br />
Schools, Social<br />
Services<br />
1. 2001/2<br />
2. 2001/2<br />
3. 2002/3 & ongoing<br />
65<br />
Education, Healthy<br />
Schools<br />
Joint working with LEA, Health<br />
Promotion, Community<br />
Education, Connexions, Youth<br />
Workers & School Nursing<br />
Service
BETTER CONTRACEPTION AND<br />
ADVICE SERVICES<br />
66
Better Contraception And Advice Services<br />
Strategic Vision – <strong>County</strong> <strong>Durham</strong><br />
Young people will be empowered and helped to use mainstream<br />
contraceptive services as they grow into adulthood. There will be a coordinated<br />
network of services, which will be easily accessible to all regardless<br />
of age, gender, ethnicity, socio-economic status or disability. The same<br />
quality of care will be available at which ever point of contact a young person<br />
accesses the service. There will be co-ordinated contraception and advice<br />
services, which are specifically dedicated to young people. (In ten years time<br />
young people may also be involved in service delivery).<br />
There will be a range of sources of contraception available to young people so<br />
that they feel comfortable with accessing contraception and advice services.<br />
67
Contraception & Advice Service Risk Assessment<br />
SWOT Analysis<br />
Strengths<br />
• Committed individuals who will represent their organisations through<br />
partnership working (see weaknesses)<br />
• Staff flexibility<br />
• Good communication<br />
• Joint working between NHS Trusts, PCGs and General Practices<br />
• Staff working across settings + localities<br />
• Established working practices covering links between different working<br />
groups – e.g.: access to consultant: referral + community pathways<br />
(see next table)<br />
provision of condoms, pregnancy testing equipment,<br />
recent and ongoing service review.<br />
• Established policies for HR + clinical governance.<br />
• Contraception services are available in some non-clinical settings,<br />
supported by outreach nursing.<br />
Weaknesses<br />
• Lack of infrastructure for information gathering (still on paper) = needs to<br />
be updated in regard to I.T. (This needs to be compatible with the ‘GP<br />
systems’) (Across six PCG sites) (3 yrs).<br />
• Use of services by different ethnic group criteria is not yet monitored.<br />
• Lack of career structure for doctors + nurses working in Family Planning<br />
Services.<br />
• Translation services for groups or individuals including: Asian dialects only<br />
available on a one-off basis. This service needs further consideration.<br />
- Impact on access to services<br />
- Telephone provision (speakerphones – conference facilities)<br />
• Lack of permanent funding for subject’s area.<br />
Opportunities<br />
• (10 yrs) An agreement on co-ordinated service delivery across all Health<br />
providers.<br />
• Central Specialist Service within the provision of a core service and<br />
maximising on the current + future staffing complement + skill base, within<br />
general practice + community practices.<br />
• Developing the GP ‘Specialist Role’ (with associated pay structure) –<br />
currently operating in Darlington + evaluating well. Possible rollout<br />
programme across <strong>County</strong> <strong>Durham</strong>.<br />
• Working with Education on translation issues.<br />
• Service provision review in general practice clinics and other clinics to<br />
identify gaps in service and to identify agencies best able to fill the gap.<br />
• The service provision review in accordance with the <strong>Teenage</strong> <strong>Pregnancy</strong><br />
Unit Best Practice Guidance will be acted upon appropriately at a local<br />
level.<br />
68
• Service provision in places such as YMCA, youth clubs, or expansion of<br />
young people’s contact bus<br />
• Look at possibility of involving young people in service delivery –<br />
consultation on practical implications is needed.<br />
Threats<br />
Staff<br />
• Availability of doctors + nurses to provide a service at unsociable times on<br />
a part time or ‘bank’ basis. Core service provision – critical mass required<br />
to continue providing training for doctors and nurses.<br />
• Career structure/ we must anticipate medical staff leaving the<br />
service/retiring<br />
• Salary issues- particularly for community clinic doctors.<br />
• Training – must consider training needs of all staff including receptionists.<br />
Transient Population<br />
• Difficult to ensure the use of services by and consistent follow-up of<br />
transient populations.<br />
69
CORE SERVICE<br />
Consultant and Community Clinics<br />
REFERRAL PATHWAYS<br />
• Information Available at each outlet<br />
• Confidentiality Minimum service<br />
expectation/specification<br />
• Child protection addressed (+ client experience)<br />
• Patient-Group/Directives<br />
• Prescribing<br />
• Under 16 friendly<br />
CLIENT<br />
SPECIALIST GP Other Health Personnel<br />
School nurses, GUM clinics, etc.<br />
70<br />
GP PARTNER<br />
ORGANISATION
2. Plans to disseminate and implement national guidance<br />
(Guidance for health professionals on contraception for under 16s available<br />
from autumn 2000).<br />
After initial local guidelines are developed and a training programme for health<br />
professionals on contraception for the under 16s is delivered, we will maintain<br />
DoH guidance and work with professionals from partner agencies to ensure a<br />
concerted and consistent approach.<br />
3. Planning and use of mainstream funding to ensure services are<br />
provided for young people using a variety of models and<br />
approaches which are appropriate to the local context and the<br />
needs and preferences of young people<br />
Plans will be drawn up to assess the community clinics already in operation<br />
and to test which of them could be most usefully changed into young people<br />
specific clinics.<br />
A variety of models will be used to ensure services are provided for young<br />
people. Assessments will be made of each proposal, young people will be<br />
consulted and their views will be taken into account when services are<br />
planned. Issues, which will be considered, include:<br />
• Confidentiality – the local implementation co-ordinator will ensure that the<br />
confidentiality tool kit developed by the Royal College of General<br />
Practitioners and Brook is being used and adhered to by General<br />
Practices, Primary Care Groups and Trusts.<br />
• Continued training for GPs, nurses and receptionists to ensure that<br />
services available to young people meet their needs and preferences.<br />
• Availability of condoms through distribution network schemes and<br />
machines. Condom or c-cards will be available for use by young people<br />
as well as older adults. In each of the pick up points the front of house<br />
staff will be trained particularly to deal with issues of confidentiality and<br />
other issues specifically relevant to young people.<br />
• The issue of condom distribution in schools will be investigated and any<br />
action taken will be with the full agreement of schools, governors, parents,<br />
young people, the local education authority, school nurses, NHS Trusts,<br />
PCGs and General Practices.<br />
• In <strong>County</strong> <strong>Durham</strong> a pilot scheme is testing a credit card sized information<br />
card. It will be given out by pharmacists to adults and young people who<br />
request pregnancy testing kit. The card will list telephone numbers of a<br />
range of local services. After evaluation, this will be replicated in<br />
Darlington.<br />
71
• In <strong>County</strong> <strong>Durham</strong> the links between health services and pregnant school<br />
girl/ young mums groups will continue. This enables further links between<br />
the young people and mainstream services leading to a reduction in the<br />
risk of their becoming socially excluded.<br />
• A young persons centre is being established from mainstream funding at a<br />
YMCA base and contraception services will be available in a youth friendly<br />
centre.<br />
• The mobile bus will continue to provide contraceptive advice and condom<br />
distribution.<br />
• Voluntary Organisations such as End House will continue the provision of<br />
contraceptive advice and provision.<br />
• Further use of the Sex Education Roadshow to give more opportunities for<br />
young people and professionals to experience etc.<br />
• Community Education will be consulted on their possible involvement in<br />
the distribution of contraception and advice services. Any action will again<br />
be in consultation with health, mainstream education and young people.<br />
• The Health Authority will continue to develop and monitor the provision of<br />
Emergency Hormonal Contraception through pharmacies. A proposal to<br />
provide Levonelle2 free of charge will be monitored and progress will be<br />
noted on this in the Annual Report.<br />
• There will be more nurse led clinics offering contraceptive services in ten<br />
years time as examples of current best practice are built upon.<br />
4. Use of multi-professional teams to deliver a range of service<br />
provision, ensuring young people are actively supported to<br />
access services for prevention, advice and support.<br />
<strong>County</strong> <strong>Durham</strong> and Darlington is committed to the use of multi-professional<br />
teams. It is envisaged that in ten years time the provision of advice and<br />
information will be delivered through a range of professionals and services.<br />
The Core Service Provision will be in the form of community clinics with links<br />
between the clinics and specialist GPs and mainstream GPs, nurses,<br />
midwives, health visitors. Additionally there will be links between all of the<br />
service providers and agencies, which can provide information to young<br />
people about services, which are available. Links will be made and<br />
maintained between the medical services and:<br />
Pharmacies, schools, workplaces, sexual health outreach workers, community<br />
settings, social services, media, shops/supermarkets, community education<br />
and youth offending teams.<br />
72
Community<br />
Education<br />
YOTs<br />
Shops/Supermarkets<br />
Advice & Information. 10 year plan<br />
Pharmacies<br />
GPs, Nurses, Midwives,<br />
Health Visitors<br />
Specialist<br />
GPs<br />
Core Service<br />
Provision<br />
(Community<br />
cn<br />
73<br />
Schools<br />
Media – Radio Mags<br />
Newspapers<br />
Workplaces<br />
Sexual Health<br />
Outreach<br />
Workers<br />
Community<br />
Settings<br />
Social<br />
Services
5. Plans to improve the monitoring of service uptake by age, gender,<br />
race<br />
In ten years time at each point where sexual health information, advice and/or<br />
contraception can be obtained, monitoring procedures will be in place to<br />
measure the uptake of services. This will be developed in conjunction with<br />
service users, NHS Trusts, PCGs and General Practitioners. Where<br />
appropriate the guidance for evaluation and the toolkit provided by the Health<br />
Promotion Research Unit will be used. (Sexual Health Services for Yo ung<br />
People, August 2000).<br />
6. Cross referral and planning of services to ensure coverage at key<br />
times and periods such as holidays, weekends etc.<br />
There will be a cross referral pattern demonstrated on a flowchart which every<br />
health, social, education and community worker can refer to. The flowchart<br />
will detail information about services, their availability, and opening hours so<br />
that any of the above professionals can refer a young person to the<br />
appropriate place/service. This will link with the Directory of Services referred<br />
to in the media section of this strategy.<br />
To ensure continuity of care referral pathways will be used so that with<br />
permission of the client, relevant information can be shared between other<br />
professionals and health professionals. It will only be possible to establish<br />
this procedure via a management agreement. In ten years time, it is<br />
envisaged that this procedure will be in place and that it will be established by<br />
using a network of professionals with local knowledge about how it will work in<br />
practice.<br />
7. Plans for involving young people in planning, delivery and review<br />
of services.<br />
A number of methods by which young people can be involved in the planning,<br />
delivery and review of services are being considered. The ten-year strategy<br />
and action plan will be used as a consultation document on which young<br />
people have been asked to comment. The views of young people will be<br />
integrated into the document as they consider the plans for contraception<br />
services herein.<br />
Some of the possibilities by which young people could be involved in the<br />
delivery of services are indicated below. At this stage they are only<br />
possibilities and will not be acted upon until approved by young people, NHS<br />
Trusts, PCGs, General Practice and other concerned bodies.<br />
Possibilities for involving young people in the delivery of services:<br />
74
- A young person may work with sexual health outreach workers as a<br />
link to vulnerable young people who may otherwise not access a<br />
service.<br />
- A young person who has previously used an advice, information<br />
and/or contraception service may be ‘employed’ as voluntary<br />
receptionists or they may be employed part-time.<br />
- A young person could be part of a clinic team and could act as a<br />
young person’s liaison officer.<br />
- Linking with Sure Start it may be possible for young people to act as<br />
parent educators regarding contraception advice.<br />
- The young person at a clinic may also become the person that<br />
outside agencies contact on behalf of a young person who wants to<br />
access an information/advice/contraceptive service.<br />
- Young people can give advice to professionals via a particular<br />
group, for instance young people could be drawn from schools,<br />
youth groups, drop-in centres and as a result of contact with Sexual<br />
Health Outreach Workers, and could form their own group which<br />
advises, guides and informs the medical professionals about the<br />
services offered.<br />
- These are all possibilities for action in ten years time, they will be<br />
assessed and those accepted will be formatted and set out in<br />
procedures for action.<br />
8. Mechanisms to periodically check/research young peoples level<br />
of awareness of services and their perceptions and experiences.<br />
To advertise services a set of procedures must be established which detail<br />
how the advertising will be funded. For instance, posters of clinic times and<br />
places must be planned centrally, printed and there must be an agreement<br />
about who will be responsible for changing them when updated information is<br />
sent to various agencies/community settings. See Media part of this strategy<br />
for details of how this is to be achieved.<br />
To check levels of awareness of services, perceptions and experiences:<br />
Awareness of services – short questionnaires may be carried out in various<br />
settings, for example schools, further education colleges, youth clubs,<br />
residential settings, youth offenders institutions.<br />
Perceptions and Experiences – use of the evaluation tool kit promoted by the<br />
Health Promotion Research Unit (August 2000) will enable professionals to<br />
assess how young people felt about using the information/advice/<br />
contraceptive service.<br />
75
BETTER CONTRACEPTION 3 YEAR PLAN<br />
Issue S.E.U.<br />
Action Point<br />
S.E.U. Action<br />
Point 13<br />
Clearer guidance<br />
for all health<br />
professionals on<br />
contraception for<br />
under 16s<br />
S.E.U. Action<br />
Point 13<br />
Clearer guidance<br />
for all health<br />
professionals on<br />
contraception for<br />
under 16s<br />
Task Planned<br />
Action/Goals<br />
1. Implement 1. Develop written<br />
DoH local guidelines<br />
guidance for 2. Implement a<br />
health training programme<br />
professionals for health<br />
professionals<br />
including key<br />
elements for service<br />
delivery for under 16<br />
year olds, e.g. Gillick<br />
Competence<br />
3. Liaise with Family<br />
Planning training<br />
providers e.g. Teeside<br />
University<br />
1. Implement 1. All staff working in<br />
DoH Family Planning<br />
guidance for clinics to have regular<br />
health training in working<br />
professionals with young people.<br />
2. School nurses to<br />
have contraceptive<br />
awareness training<br />
Timescale Who/Lead Assumptions/Risks, Comments<br />
1. 2002/3<br />
1. 2002/3<br />
2. 2002/3<br />
76<br />
NHS Trust<br />
Training Leads,<br />
Specialist<br />
Health<br />
Promotion<br />
Services, PCG<br />
Training and<br />
Education<br />
Forums<br />
PCGs with<br />
NHS Trusts.<br />
Family<br />
Planning<br />
Services,<br />
Midwifes,<br />
Health Visitors<br />
Funding to be negotiated<br />
A timescale for the training will be<br />
drawn up locally<br />
Funding to be negotiated
BETTER CONTRACEPTION 3 YEAR PLAN<br />
S.E.U. Action<br />
Point 13<br />
Clearer guidance<br />
for all health<br />
professionals on<br />
contraception for<br />
under 16s<br />
S.E.U. Action<br />
Point 13<br />
Clearer guidance<br />
for all health<br />
professionals on<br />
contraception for<br />
under 16s<br />
1. Implement<br />
DoH<br />
guidance for<br />
health<br />
professionals<br />
1. Implement<br />
DoH<br />
guidance for<br />
health<br />
professionals<br />
1. Ensure practice<br />
nurses receive<br />
appropriate training re<br />
young people’s<br />
services.<br />
2. Ensure<br />
receptionists receive<br />
training to assist them<br />
in dealing<br />
sympathetically with<br />
enquiries from young<br />
people<br />
1. Encourage GPs to<br />
attend regular updates<br />
on service provision<br />
related to sexual<br />
health, contraception<br />
and skills in dealing<br />
with young people<br />
including training on<br />
the local condom<br />
distribution scheme<br />
1. 2001<br />
2. 2001/2003<br />
1. 2001 &<br />
ongoing<br />
77<br />
PCGs Training<br />
and Education<br />
Groups<br />
PCGs<br />
This has already begun
BETTER CONTRACEPTION 3 YEAR PLAN<br />
Issue Task Planned<br />
Action/Goals<br />
S.E.U. Action<br />
Point 14<br />
S.E.U. Action<br />
Point 14<br />
S.E.U. Action<br />
Point 14<br />
1. Effective<br />
and<br />
responsible<br />
youth<br />
contraception<br />
and advice<br />
services<br />
1. Effective<br />
and<br />
responsible<br />
youth<br />
contraception<br />
and advice<br />
services<br />
1. Effective<br />
and<br />
responsible<br />
youth<br />
contraception<br />
and advice<br />
services<br />
1. Development of<br />
a co-ordinated<br />
approach to data<br />
collection<br />
measuring the<br />
uptake of<br />
contraceptive<br />
services by young<br />
people<br />
1. Further develop<br />
the <strong>Teenage</strong><br />
Parent Peer<br />
Education Project<br />
already in one area<br />
of <strong>County</strong> <strong>Durham</strong><br />
(Easington)<br />
1. Develop a<br />
sexual health<br />
resource service<br />
for parents<br />
Timescale Who/Lead Assumptions/<br />
Risks,<br />
1. 2002<br />
1. Ongoing<br />
1. 2001<br />
78<br />
<strong>Teenage</strong><br />
<strong>Pregnancy</strong><br />
Co-ordinator/<br />
Manager<br />
Comments<br />
Use of evaluation<br />
procedures<br />
developed by the<br />
Health Promotion<br />
Unit<br />
SHPS Ongoing<br />
mainstream<br />
funded<br />
SHPS
S.E.U. Action<br />
Point 14<br />
S.E.U. Action<br />
Point 14<br />
1. Effective<br />
and<br />
responsible<br />
youth<br />
contraception<br />
and advice<br />
services<br />
1. Effective<br />
and<br />
responsible<br />
youth<br />
contraception<br />
and advice<br />
services<br />
1. Develop an<br />
accredited course<br />
on sexual health<br />
information for<br />
young people<br />
1. Develop a<br />
sexual health<br />
training programme<br />
for parents around<br />
communication<br />
with their<br />
teenagers/children<br />
1. 2003<br />
onwards<br />
2. April<br />
2003<br />
onwards<br />
79<br />
SHPS<br />
PCGs
BETTER CONTRACEPTION 3 YEAR PLAN<br />
Issue Task Planned<br />
Timescale Who/Lead Assumptions/<br />
Action/Goals<br />
Risks, Comments<br />
S.E.U. Action 1. Effective and 1. Accessible to all 1. 3 to 10 1. <strong>Local</strong><br />
Point 14 responsible but particularly to year plan Authority,<br />
youth<br />
young people at<br />
NHS Trust,<br />
contraception special risk e.g. in<br />
PCG, Sexual<br />
and advice Looked After<br />
Health<br />
services System, asylum<br />
Outreach<br />
seekers and<br />
travellers<br />
Workers<br />
2.<strong>Teenage</strong> 2. 3 to 10 2. <strong>Local</strong><br />
<strong>Pregnancy</strong> as year plan Authority,<br />
strategic issue on all<br />
NHS Trust,<br />
agendas, Sure Start,<br />
SRB, Connexions<br />
etc.<br />
PCG<br />
S.E.U. Action 1. Effective and 1.Review<br />
1. 2001 1. PCGs 1. Ongoing Review<br />
Point 14 responsible contraceptive advice - 2002<br />
has begun in the<br />
youth<br />
and services run by<br />
Dales<br />
contraception GP practices<br />
and advice 2.Review provision 2. 2001 - 2. PCGs 2. Operational<br />
services of condoms in<br />
practices<br />
2002<br />
since June 2000<br />
3.Review provision 3. 2001- 3. PCGs 3. Will need<br />
of emergency<br />
contraception by<br />
pharmacists<br />
2002<br />
funding by PCGs<br />
80
BETTER CONTRACEPTION 3 YEAR PLAN<br />
S.E.U. Action<br />
Point 14<br />
S.E.U. Action<br />
Point 14<br />
S.E.U. Action<br />
Point 14<br />
S.E.U. Action<br />
Point 14<br />
1. Effective and<br />
responsible<br />
youth<br />
contraception<br />
and advice<br />
services<br />
1.Effective and<br />
responsible<br />
youth<br />
contraception<br />
and advice<br />
services<br />
1.Effective and<br />
responsible<br />
youth<br />
contraception<br />
and advice<br />
services<br />
1. Effective and<br />
responsible<br />
youth<br />
contraception<br />
and advice<br />
services<br />
1. Develop a<br />
protocol for the<br />
consistent follow up<br />
of young people<br />
using emergency<br />
contraception<br />
2. Review central<br />
booking pilots in<br />
county<br />
1.Extend current<br />
young peoples<br />
clinics across the<br />
county<br />
1. Review current<br />
Family Planning<br />
services and young<br />
peoples centres (see<br />
appendix B)<br />
1. Extend out of<br />
hours provision to<br />
practices<br />
1. 2001/3<br />
2. 2001/2<br />
2. 2002/3<br />
1. 2001<br />
1. 2002<br />
81<br />
1. PCGs with<br />
Trusts &<br />
Family<br />
Planning<br />
Services<br />
2. PCGs,<br />
NHS Trusts<br />
1. PCGs &<br />
NHS Trusts<br />
1. NHS Trust,<br />
Family<br />
Planning,<br />
PCG or<br />
Subcontract<br />
to Consultant<br />
1. Occurs on<br />
wards. School<br />
Nurses possibly<br />
involved<br />
2. Consider<br />
outcome of<br />
evaluation.<br />
1. Roll-out over 2-<br />
3 years.<br />
1. PCGs 1. Collaboration<br />
between Trusts is<br />
necessary
S.E.U. Action<br />
Point 14<br />
S.E.U. Action<br />
Point 14<br />
1. Effective and<br />
responsible<br />
youth<br />
contraception<br />
and advice<br />
services<br />
1. Effective and<br />
responsible<br />
youth<br />
contraception<br />
and advice<br />
services<br />
1. Condoms freely<br />
available in all<br />
practices in<br />
accordance with a<br />
protocol.<br />
2. Review condom<br />
provision in youth<br />
centres and Further<br />
Education Colleges.<br />
3. Investigate<br />
feasibility of piloting<br />
condom provision in<br />
schools via School<br />
Nurses<br />
1. Provide<br />
information &<br />
support to young<br />
people at risk of<br />
pregnancy via<br />
Sexual Health<br />
Outreach Worker<br />
and/or<br />
Subcontracted<br />
Services<br />
2. Raise profile of<br />
Midwives in giving<br />
advice on pregnancy<br />
1. 2001<br />
2. 2001/2<br />
3. 2001/3<br />
1. 2000/4<br />
2. 2001/4<br />
82<br />
1. PCGs<br />
2. PCGs<br />
3. PCGs/NHS<br />
Trusts<br />
1. SHPS<br />
2. PCGs,<br />
NHS Trusts<br />
1. Base line review<br />
needed<br />
2. Provided in<br />
some areas by<br />
SHPS<br />
3. Link to schools<br />
with highest rates<br />
of conception<br />
1. Dependant on<br />
TPU funding<br />
2. Partly via cards<br />
with pregnancy<br />
testing kits being<br />
piloted in one area
S.E.U. Action<br />
Point 14<br />
1. Effective and<br />
responsible<br />
youth<br />
contraception<br />
and advice<br />
services<br />
1. School Nurses to<br />
provide ‘drop in’<br />
sessions at<br />
secondary schools<br />
for sexual health<br />
information<br />
1. 2001/3<br />
83<br />
1. School<br />
Nurses with<br />
PCG/Trust<br />
support<br />
1. Depends on<br />
support of<br />
individual schools
BETTER CONTRACEPTION 3 YEAR PLAN<br />
Issue S.E.U,<br />
Action Point<br />
S.E.U. Action<br />
Point 15<br />
Clearer<br />
guidance for<br />
all health<br />
professionals<br />
on<br />
contraception<br />
for under 16s<br />
Task Planned<br />
Action/Goals<br />
1. National<br />
Helpline –<br />
<strong>Local</strong><br />
Implications<br />
1.Work with NHS<br />
Direct to customise<br />
information<br />
2.Maintain accurate<br />
info. services for<br />
young people e.g.<br />
Sexwise<br />
Timescale Who/Lead Assumptions<br />
Risks,<br />
Comments<br />
Ongoing 1. SHPS<br />
Ongoing<br />
84<br />
2. SHPS
Issue Task Planned<br />
Action/Goals<br />
S.E.U. Action<br />
Point 16<br />
S.E.U. Action<br />
Point 16<br />
S.E.U. Action<br />
Point 16<br />
1. Get<br />
young<br />
people to<br />
seek advice<br />
1. Get<br />
young<br />
people to<br />
seek advice<br />
1. Get<br />
young<br />
people to<br />
seek advice<br />
Review accessibility<br />
of services<br />
Dedicate funding for<br />
a post to focus on<br />
sexual health and<br />
contraceptive issues<br />
for young people.<br />
Focus on intensive<br />
support for schools,<br />
FE colleges, Youth<br />
Service, young<br />
people in the Looked<br />
After System and in<br />
Young Offenders<br />
Institutions<br />
1.Develop a strategy<br />
to increase uptake of<br />
services by boys and<br />
young men<br />
Timescale Who/Lead Assumptions/<br />
Risks,<br />
2001-3 PCGs, NHS<br />
Trusts<br />
1.Ongoing<br />
for 3 years<br />
1. 2001/3<br />
85<br />
PCGs with<br />
partners from<br />
Education,<br />
Social<br />
Services,<br />
Community<br />
Education,<br />
Further<br />
Education<br />
Colleges,<br />
NHS Trusts.<br />
Comments<br />
Depends on<br />
continued<br />
support from<br />
partner<br />
agencies<br />
PCG May need<br />
focused work<br />
with boys and<br />
young men
Issue Task Planned Action/Goals Timescale Who/Lead Assumptions/<br />
Risks,<br />
S.E.U. Action<br />
Point 17<br />
S.E.U. Action<br />
Point 17<br />
S.E.U. Action<br />
Point 17<br />
1. Publicity 1. Ensure appropriate<br />
local response to national<br />
campaigns<br />
2. Ensure that<br />
appropriate personnel<br />
with the appropriate skills<br />
are in place to work<br />
across client groups.<br />
Particularly re boys and<br />
young men<br />
1. Publicity 1. Review provision of<br />
information to young<br />
people<br />
2.Provide consistent<br />
updated information on<br />
services<br />
1. Publicity 1.Support awareness<br />
raising about appropriate<br />
contraceptive use for<br />
young people, particularly<br />
reinforcing the profile of<br />
condoms<br />
1.Encourage the growth<br />
and development of the<br />
Sexual Health Forum in<br />
part of the <strong>County</strong> to<br />
other areas of the <strong>County</strong><br />
1. Ongoing<br />
2. 2003/4<br />
1. 2001/2<br />
2. 2001 &<br />
ongoing<br />
1. 2001 &<br />
ongoing<br />
86<br />
Communications<br />
SHPS/ Media<br />
Post<br />
PCGs,<br />
SHPS<br />
Youth and<br />
Community<br />
Education<br />
1. PCGs<br />
1. 2001/4 SHPS<br />
2. PCGs/<br />
Communications<br />
Lead<br />
SHPS/ National<br />
Campaigns<br />
Comments<br />
1. PCGs and<br />
Steering<br />
Group at<br />
<strong>County</strong> Level<br />
2. Need time<br />
to collect,<br />
collate, update<br />
and print
Issue Task Planned<br />
Action/Goals<br />
S.E.U. Action<br />
Point 13<br />
S.E.U. Action<br />
Point 16<br />
1. Clearer<br />
Guidance for<br />
professionals<br />
1. Get young<br />
people to seek<br />
advice<br />
Ensure<br />
Confidentiality Tool-<br />
Kit is being used by<br />
GPs, PCGs and<br />
Trusts<br />
1. Pilot of<br />
contraception/emerg<br />
ency contraception<br />
card in the Dales<br />
area of county<br />
2. Pilot of information<br />
card with pregnancy<br />
testing kits in one<br />
area of county,<br />
Sedgefield<br />
Timescale Who/Lead Assumptions/<br />
Risks,<br />
1. 2001 &<br />
ongoing<br />
1. 2001/2<br />
2. 2001<br />
87<br />
<strong>Teenage</strong><br />
<strong>Pregnancy</strong> Coordinator<br />
1. SHPS,<br />
<strong>Teenage</strong><br />
<strong>Pregnancy</strong> Coordinator,<br />
PCG<br />
2. PCG Team,<br />
<strong>Pregnancy</strong><br />
Planning Group<br />
Comments<br />
By letter via<br />
Clinical<br />
Governance<br />
Leads<br />
Will be closely<br />
evaluated and<br />
extended to<br />
non-clinical<br />
settings
S.E.U. Action<br />
Point 16<br />
S.E.U. Action<br />
Point 16<br />
S.E.U. Action<br />
Point 16<br />
S.E.U. Action<br />
Point 16<br />
1. Get young<br />
people to seek<br />
advice<br />
1. Get young<br />
people to seek<br />
advice<br />
1. Get young<br />
people to seek<br />
advice<br />
1. Get young<br />
people to seek<br />
advice<br />
1. Development of<br />
youth centre<br />
specifically for<br />
sexual health issues<br />
Derwentside<br />
1. Continue support<br />
of mobile Youth<br />
Project Bus in<br />
Darlington.<br />
1. Continue support<br />
of Voluntary<br />
Organisations<br />
providing<br />
contraception<br />
1. Involve young<br />
people in planning<br />
and review of<br />
services<br />
1. Launch<br />
Sept 2001<br />
88<br />
Sexual Health<br />
Outreach Worker<br />
2001/2010 SHPS and<br />
Community<br />
Education<br />
2001/2010 SHPS and<br />
<strong>Teenage</strong><br />
<strong>Pregnancy</strong> Coordinator<br />
2001/2010 <strong>Teenage</strong><br />
<strong>Pregnancy</strong> Coordinator<br />
Encourage<br />
similar in<br />
<strong>County</strong><br />
<strong>Durham</strong>
BETTER SUPPORT FOR<br />
TEENAGE PARENTS<br />
90
Better Support For <strong>Teenage</strong> Parents<br />
<strong>County</strong> <strong>Durham</strong><br />
VISION<br />
In ten years time we will provide a support package to young parents which will<br />
take account of their differing needs according to ethnicity, faith, cultural needs,<br />
socio economic circumstances and family support available (the support<br />
package will ensure that every young parent, male or female, has equal access<br />
to full-time educational provision). There will be partnership working between<br />
the Voluntary Sector, Education, Health Care, Social Services and Housing<br />
Department to provide a choice of opportunities through a range of provision for<br />
young parents. Multi-agency services designed specifically for young people<br />
will be accessible and sustainable. Through partnership working young parents<br />
will still be offered support after the birth of their baby even if that support was<br />
initially refused by the young person. We will promote the welfare of the young<br />
parent and child. The young person will be supported as a parent, student/<br />
employee and as a sexually active person.<br />
91
Better Support for pregnant school pupils<br />
Where we are now – health<br />
• Information, advice and support relating to options for either continuance<br />
or termination of the pregnancy, with referral to the appropriate agency, if<br />
required.<br />
This information is available from GP’s, School Nurses, family planning<br />
nurses, Health Visitors and midwives and is on-going.<br />
• Antenatal care is offered with a choice of venues, i.e. GP, hospital,<br />
community clinics or home. We will aim to make all venues welcoming to<br />
young women and teenage mothers.<br />
• Details of parent/mother craft classes are available from the Community<br />
Midwife and in some instances, can be specifically set up to encourage<br />
teenagers to attend. These classes are often set up as required.<br />
• Information is given on choices available relating to care during<br />
pregnancy, labour, delivery and post-natal care.<br />
• Early post-natal support (up to 28 days) is tailored to individual need and<br />
circumstances (at present under National Review).<br />
• Initial advice on future family planning and the clinics available, ideally<br />
are discussed with both teenage parents and can be given by the GP,<br />
family planning service, midwife, health visitor or school nurse.<br />
Social Services<br />
• Young people in the Looked After System receive information on a<br />
variety of issues in a number of ways including a website, young people<br />
friendly booklets such as “got the house, now get the knowledge” and<br />
credit card information packs.<br />
• Sexual health issues and a directory of services can be integrated into<br />
these already existing publications.<br />
• We are looking to develop services for young fathers. Any new provision<br />
will be evidence based and closely evaluated.<br />
92
Getting back into education<br />
• Continue to encourage under 16 year old mothers to resume and<br />
complete full time education, with support from the appropriate services,<br />
i.e. child care agencies, support for parents of teenage parents.<br />
• Continue to offer support through multi-disciplinary agencies, i.e. GP,<br />
Midwife, health visitor, Home and Hospital Support, Social Services for<br />
both parents.<br />
• Continue to offer access to quality, affordable child care as appropriate,<br />
i.e. out of five local colleges, three have nursery provision from birth<br />
onwards, one has provision from age two years and one college has no<br />
provision (details of each college and number of placements below).<br />
• Continue to provide lessons in parent craft and the development of<br />
practical skills for all young people in the education system.<br />
• Individual tailored educational packages following assessment of social<br />
support required and the educational needs of the young person.<br />
• To incorporate the Connexions Personal Advisor into the home and<br />
hospital support service.<br />
• To continue Lifelong Learning Programme with input from FE and<br />
Careers Service.<br />
• To continue to support Sure Start Programmes.<br />
• To continue with the sex and education programmes in school, enabling<br />
young people to discuss issues and have access to up-to-date<br />
information – multi agency support.<br />
• To continue to promote and extend the child care available in colleges,<br />
see earlier section.<br />
• To continue to promote the availability of childcare in the local<br />
community. Lists of carers available from Social Services.<br />
• To continue to promote Out of School Hours provision.<br />
93
Needs, circumstances, culture and ethnicity of young parents<br />
• Each young person has individual needs.<br />
• Continue support from multi-agency sources from the young people.<br />
• Support for the parents of the teenage parents with information and<br />
advice – in some instances these parents become the child carer, to<br />
enable the young mother to return to education or employment.<br />
Mechanisms in place to monitor truancy or exclusion of under school age<br />
girls known to be pregnant<br />
Truancy - Education Welfare Officer liasing with schools – on-going.<br />
- School routine of attendance – on-going<br />
Exclusion when pregnant<br />
• The young woman would not be excluded because she was pregnant.<br />
• Involvement of school nurse to carry out home visit.<br />
• Health Visitor involvement offering ante natal advice.<br />
• Midwife involvement providing ante natal and post natal advice and care.<br />
• Use referral system to the appropriate agency.<br />
• Develop a close, multi-agency partnership to ensure that young pregnant<br />
girl and her family have all the relevant information or support needed<br />
during pregnancy and following the birth of her child.<br />
The following action plans detail services which aim to reintegrate teenage<br />
parents into education and give support to them intended to reduce the risk of<br />
their becoming socially excluded.<br />
94
BETTER SUPPORT TEN YEAR PLAN<br />
Issue Task Planned<br />
Action/Goals<br />
a) Access to 1. Establish 1. Links to Early<br />
Child Care suitable Years & Childcare<br />
childcare<br />
facilities across<br />
the county<br />
Development Plan<br />
b) Access to 1. Establish 1. Links with Early<br />
parenting discreet Years and Childcare<br />
education parenting/health<br />
education<br />
sessions for the<br />
younger parent<br />
Development Plan<br />
c) Child friendly 1. Affordable 1. Lobby Government<br />
workplaces care in the<br />
workplace<br />
2. Lobby local firms<br />
d) Forward 1. Continue to 1. Develop strategy<br />
planning for develop access for future plans<br />
those who will to health<br />
be teenagers in services<br />
10 years time information and<br />
expand the<br />
Connexions<br />
Service<br />
Timescale Who/Lead Assumptions/<br />
Risks, Comments<br />
10 years Reintegration Difficult because of<br />
Officer and Early geographical spread<br />
Years Co-ordinator in <strong>County</strong> <strong>Durham</strong><br />
10 years Health Promotion,<br />
Reintegration<br />
Officer<br />
96<br />
Currently for under<br />
16s, could be<br />
extended to under<br />
18s<br />
5-10 years Police Resources required<br />
10 years LEA/Health/Social<br />
Services/Voluntary<br />
Organisations
BETTER SUPPORT 3 YEAR PLAN<br />
Issue Task Planned<br />
Action/Goals<br />
a) Accessing 1. Discussion 1. Identify Services<br />
Services with young<br />
people. Find<br />
out what they<br />
want /need<br />
currently available<br />
b) Information<br />
on services<br />
available<br />
c) Multi-agency<br />
response and<br />
responsibility.<br />
d) Co-ordination<br />
of services<br />
e) Entitlement<br />
of range of<br />
professional<br />
support.<br />
1. Produce a<br />
directory of<br />
services for<br />
pregnant<br />
teenagers under<br />
18 years<br />
1. Establish a<br />
multi-agency<br />
management<br />
team.<br />
1. Appoint a<br />
<strong>Teenage</strong><br />
<strong>Pregnancy</strong><br />
Support Co-<br />
ordinator<br />
1. Vision<br />
statement.<br />
2. Inform<br />
schools<br />
1. Seek information<br />
from each agency –<br />
identify gaps<br />
1. Establish a multiagency<br />
management<br />
team.<br />
1. To ensure the<br />
capture of young<br />
people not in<br />
education or<br />
excluded<br />
1. Write statement.<br />
2. Write protocols<br />
with other agencies<br />
Timescale Who/Lead Assumptions/<br />
Risks, Comments<br />
1. 2001-2 <strong>Teenage</strong> Ethnic<br />
<strong>Pregnancy</strong> Co- minorities/special<br />
ordinator and<br />
Multi-agency<br />
support<br />
needs<br />
1. 2002/3<br />
1. 2001/2<br />
97<br />
Multi-agency,<br />
<strong>Teenage</strong><br />
pregnancy Coordinator<br />
and<br />
support coordinator<br />
<strong>Local</strong> <strong>Teenage</strong><br />
<strong>Pregnancy</strong> Coordinator.<br />
Will make agencies<br />
aware of their own<br />
services<br />
<strong>Full</strong> commitment<br />
required<br />
1. 2001/4 Health Authority Funding available –<br />
recurring with review<br />
2001/2 Advisory Reintegration<br />
officer.<br />
Needs the cooperation<br />
of all<br />
agencies
f) Completion of<br />
education<br />
g) Support for<br />
pregnant<br />
teenagers<br />
1. Compile<br />
database<br />
1. Develop<br />
further links with<br />
specialist<br />
agencies<br />
h) Special Units 1. To ensure<br />
childcare<br />
provision links<br />
to existing<br />
services<br />
i) Life Long<br />
Learning<br />
j) Education on<br />
prevention of<br />
teenage<br />
pregnancies<br />
1. Career/FE<br />
input<br />
1. Promote<br />
contraception<br />
care and<br />
services<br />
k) Sure Start 1. Expand and<br />
develop Sure<br />
Start<br />
programme for<br />
young people<br />
who are parents<br />
1. Keep records on all<br />
girls countywide<br />
1. Establish links<br />
between Connexions<br />
Service and Home<br />
and Hospital support<br />
team<br />
1. Ensure that<br />
pregnant schoolgirls<br />
who choose to remain<br />
in mainstream<br />
education have same<br />
access to services<br />
1. Every girl to have<br />
interviews for careers.<br />
(University)<br />
1. Expand education<br />
programme in<br />
schools, youth clubs.<br />
1. Review existing<br />
programmes<br />
2 Years LEA/Sexual health Chase liaison<br />
with schools<br />
2 years Connexion and Early stage<br />
HSSS Team. discussions<br />
underway<br />
2 years Education/<br />
Health/Social<br />
Services<br />
Ongoing<br />
98<br />
Recognise that<br />
units can be<br />
centres of<br />
inclusion where<br />
range of provision<br />
can be accessed<br />
(rather than<br />
exclusive)<br />
Integration Officer Attendance of<br />
pupils vital.<br />
Now LEA and Health<br />
Promotion<br />
3 years Sure Start Coordinator<br />
& <strong>Teenage</strong><br />
<strong>Pregnancy</strong> Coordinator<br />
Sexual Health<br />
Outreach Worker<br />
to liase with<br />
schools and<br />
voluntary<br />
agencies<br />
Will programmes<br />
continue beyond<br />
3 years
l) Access to<br />
childcare<br />
m) Homeless<br />
Young People<br />
n) Asylum<br />
Seekers<br />
o) Children in<br />
Prostitution<br />
1.Establish<br />
affordable,<br />
flexible childcare<br />
units outside<br />
schools<br />
Reduce<br />
likelihood of<br />
social exclusion<br />
Develop further<br />
support<br />
Offer support &<br />
protection to the<br />
young people at<br />
risk of/ currently<br />
involved in<br />
prostitution<br />
1. Liaise with Early<br />
Years and Childcare<br />
Team to determine<br />
needs<br />
Strengthen links with<br />
relevant agencies to<br />
support homeless<br />
young people re:<br />
housing needs,<br />
education/training<br />
needs<br />
Review<br />
arrangements and<br />
ensure guidelines are<br />
in place for<br />
supporting young<br />
people who are<br />
asylum seekers<br />
Review<br />
arrangements in line<br />
with government<br />
guidelines<br />
3 years Social Services/<br />
Education<br />
2001/4 <strong>County</strong> Steering<br />
group/ Better<br />
Support Group<br />
2001/4 <strong>County</strong> Steering<br />
Group & Better<br />
Support Groups.<br />
2001/4 <strong>County</strong> <strong>Durham</strong><br />
Social Service<br />
Department<br />
99<br />
Sure Start in<br />
some areas
BETTER SUPPORT HOUSING<br />
Issue Task Planned Action/Goals Who/Lead Assumptions/<br />
Risks, Comments<br />
a) Young mother and Unable to live with 1. Supported Housing available Housing<br />
child – under 18 years her family or partner<br />
b) Young mother and Not yet ready to live 1. Supported housing available Housing<br />
child – under 18 years semi-independently<br />
c) Young mother and Promote father’s 1. Outreach support available Housing<br />
father and child -<br />
under 18 years<br />
active involvement<br />
d) Promote welfare Develop settled living 1. To prevent adverse impact Housing<br />
for the child and arrangements upon pregnant and future life,<br />
mother<br />
chances of young mother,<br />
education/employment<br />
e) Support for mother Co-operation and 1.Times flexible and as<br />
Housing/<br />
and child<br />
support from other<br />
agencies<br />
appropriate<br />
Health<br />
f) Cross-boundary 1. To develop 1. To enable young person to Housing Changes in benefits could adversely<br />
working between sustainable facilities move from supervised semi-<br />
affect a couple under 18 in terms of<br />
LA’s/Supported<br />
independent housing with support<br />
housing and support<br />
housing projects/ and<br />
to appropriate and safe<br />
all housing agencies,<br />
accommodation close to family<br />
i.e. Housing<br />
partner/friends with<br />
Association and<br />
outreach/floating support, to<br />
Private Landlords<br />
promote fully independent living,<br />
maximising individual choice<br />
g) Youth<br />
To ensure that young Promote inter-agency co- Centre<br />
Homelessness people’s needs are operation to prevent and address Point, Multi<br />
met appropriately, youth homelessness<br />
agency<br />
locally<br />
working<br />
100
101
Housing Support<br />
We recognise the importance of a pregnant teenager having a healthy<br />
environment to live in and for the baby to be born into. A settled living<br />
arrangement is more likely to contribute to social inclusion and positive life<br />
chances of the mother and her child.<br />
By 2010 we aim to have a range of supported accommodation for those<br />
mothers under 18 who cannot live with their family or partner. The range of<br />
accommodation will include supported semi-independent living with floating<br />
outreach support. Where a mother is aged 18-25 and needs supported housing,<br />
she will be included in such projects.<br />
Where fathers remain involved with the mother and child, every encouragement<br />
will be given to promote his active involvement.<br />
Housing plans in county <strong>Durham</strong> are currently being developed in more detail at<br />
a local level. The local co-ordinator will work with <strong>Local</strong> Housing Authorities,<br />
Housing Associations and young people to establish need and plan provision<br />
within government guidelines.<br />
102
103
CONSULTATION WITH YOUNG<br />
PEOPLE<br />
104
Consultation with Young People in <strong>County</strong><br />
<strong>Durham</strong><br />
• In <strong>County</strong> <strong>Durham</strong> we remain committed to the concept that young<br />
people need to be part of the debate about how we move forward in<br />
tackling teenage pregnancy.<br />
• This document follows the very focused guidelines issued by the<br />
<strong>Teenage</strong> <strong>Pregnancy</strong> Unit and has been produced in a very limited<br />
timeframe dictated by the Government. In order to make the<br />
consultation with young people in <strong>County</strong> <strong>Durham</strong> meaningful<br />
consultation is still ongoing. We have involved young people in<br />
consultation in <strong>County</strong> <strong>Durham</strong> since the strategy was assessed by the<br />
<strong>Teenage</strong> <strong>Pregnancy</strong> Unit in the following ways:<br />
By consulting with the young people at End House Young People’s Centre at<br />
the next youth forum, and by consulting with the young people in the Investing<br />
in Children Project. The comments from the two groups are now included.<br />
105
Results of Consultations with Young People’s Groups about<br />
the <strong>County</strong> <strong>Durham</strong> Tackling <strong>Teenage</strong> <strong>Pregnancy</strong> <strong>Strategy</strong><br />
The Investing in Children Group based in Pity Me, <strong>Durham</strong>, was consulted via<br />
co-ordinator Liam Cairns. The Investing in Children initiative seeks to support<br />
children and young people to comment on issues of importance to them. The<br />
Investing in Children Initiative assists groups of children and young people who<br />
want to become actively involved in dialogue with decision makers about how<br />
things might change.<br />
The first comment about the strategy was, that because it had to be compiled<br />
in the way it was to comply with TPU guidelines, the strategy was not young<br />
people user friendly. The group felt that the strategy could have been written<br />
in a less complex way which would have made it more understandable for<br />
young people as well as professionals. They would like to see one list of all the<br />
new things planned to help prevent teenage pregnancy and support teenage<br />
parents. They would like a list of how the aims were to be met, as a list rather<br />
than as the action plans included in the strategy.<br />
Comments about sex and relationships education included the need for<br />
teacher training. The young people believed that teachers needed specific<br />
training in how to teach sex and relationships education. They talked about<br />
the negative effects of embarrassed teachers preventing discussion in class<br />
about SRE and the effect on children and young people that they then would<br />
not feel confident to speak about sex and relationships.<br />
Related to the media section and publicising services, the group had a lot of<br />
ideas about where to use information cards and posters, some of which were<br />
included in the strategy, some were not. The strategy outlines the use of<br />
posters and credit card information cards to be used on the back of toilet doors<br />
and in public areas, where young people can easily access the information.<br />
Fast food restaurants and other public areas were suggested in the strategy.<br />
The young people suggested that public areas in leisure centres such as<br />
waiting areas, queuing areas, changing rooms and toilets could all be used, so<br />
that young people could access information privately and that this could be<br />
done in places like pubs, leisure centres, cinemas, bowling alleys, possibly<br />
train stations and bus stations, telephone boxes and schools. The young<br />
people specifically suggested that the cards be reinforced so that they would<br />
keep in a good state for longer.<br />
When the young people disused the directory of services, they suggested that<br />
the directory be divided according to towns or localities, so that young people<br />
could easily access their relevant information especially as <strong>County</strong> <strong>Durham</strong> is<br />
divided up into six Primary Care Group areas, this seems particularly relevant.<br />
Consultation in <strong>County</strong> <strong>Durham</strong> was also conducted with <strong>Durham</strong> Young<br />
People’s Centre, End House, <strong>Durham</strong>, via Co-ordinator Mandy Taylor. This<br />
group of young people included some teenage mums. Again the group was<br />
particularly interested in the media campaign and spent most of the<br />
consultation time discussing that. In relation to posters, this group suggested<br />
using bus shelters, bus tickets and adverts inside buses to advertise local<br />
106
services and or Sexual Health Outreach Workers and their contact points.<br />
They also suggested using the free postcard stands, which are now quite<br />
widespread in places such as cinemas, clubs and pubs. They specifically<br />
talked about nightclubs, which have under eighteen nights, schools and<br />
libraries as suggested venues. The group also made suggestions about a<br />
local radio campaign and suggested particular radio stations which may be of<br />
use and which would reach young people. The group also suggested the use<br />
of one leaflet which concertinas down to the size of a credit card, but which<br />
contains information about contraception, sexual health services as well as<br />
other things such as entertainment venues, youth clubs, cinemas etc. This<br />
concertina leaflet could be divided into different sections, each section giving<br />
details of a different geographical area and its services in <strong>County</strong> <strong>Durham</strong> and<br />
Darlington, so that as well as there being individual leaflets per PCG area,<br />
there would also be one county-wide leaflet which would include sexual health<br />
information, but as part of a broader content.<br />
In relation to the housing strategy, young people were concerned that if there<br />
were one specific site, which housed teenage parents, it would lead to<br />
stigmatisation and stereotyping. They favoured semi-independent housing<br />
and floating support workers. They also favoured links between the young<br />
people housed in such accommodation so that an informal network of social<br />
support was available in a self-help way.<br />
Consultation with groups of young people in <strong>County</strong> <strong>Durham</strong> is still on going.<br />
We recognise that this consultation is limited, but is a starting point on which to<br />
build and develop plans using young people’s ideas about what they would like<br />
to see to help tackle teenage pregnancy.<br />
• We will move forward by connecting with the agenda that young people<br />
see as important linked to the issued raised by the <strong>Teenage</strong> <strong>Pregnancy</strong><br />
Unit and planned for by relevant joined up working in <strong>County</strong> <strong>Durham</strong>.<br />
107
PART B<br />
ANNUAL REPORT<br />
2000/2001<br />
108
Annual Report 2000/2001<br />
Joined Up Action<br />
In <strong>County</strong> <strong>Durham</strong> and Darlington Health Authority a local Co-ordinator was<br />
appointed and took up the post on 1 st November 2000. The co-ordinator has<br />
been responsible for ensuring that strategic planning with key stakeholders<br />
occurred and that decision-making groups met to begin planning strategy<br />
development. A <strong>County</strong>wide Steering Group was established and sub groups<br />
were developed from it to specifically consider key areas of the Darlington<br />
<strong>Strategy</strong> and <strong>County</strong> <strong>Durham</strong> <strong>Strategy</strong>.<br />
Decision making groups were formed around the key areas of:<br />
Better sex and relationship education.<br />
Better contraception and advice services.<br />
Better support for teenage parents.<br />
The groups met twice to agree terms of reference, to establish that<br />
membership was appropriate and to ensure that representatives of all relevant<br />
agencies were represented. Membership of the groups demonstrated joint<br />
partnership working is detailed in part A, section 1 of the local strategy<br />
document. During these initial meeting formulas for strategy development were<br />
discussed.<br />
It was agreed that half day working sessions would be held to kick-start the<br />
joint working and to develop strategic vision and action planing. The working<br />
sessions led to the strategy and three-year action plans contained in the<br />
strategy which also identified lead responsibilities. It was possible to agree on<br />
those leads as each working/discussion making group was a multi-agency<br />
group representing Health, Education, Social Services and voluntary sector as<br />
appropriate.<br />
It was agreed that consultation with a wider group of key stake holders would<br />
be held on production of the draft strategies for <strong>County</strong> <strong>Durham</strong> and<br />
Darlington, and that feedback from the consultation stage would further inform<br />
both the strategies and the work of the decision making groups.<br />
It has also been agreed that the steering group and other decision making<br />
groups (as detailed above) will reconvene quarterly to assess the and monitor<br />
the progress made by agencies and to ensure that the three year action plans<br />
are being delivered.<br />
Partnership arrangements (other than the joined up working via multi-agency<br />
groups) were also agreed in the year 2000/2001. <strong>County</strong> <strong>Durham</strong> and<br />
Darlington Health Authority agreed partnership working with:<br />
• Community Education in <strong>County</strong> <strong>Durham</strong> – for training and support for<br />
youth workers.<br />
• The University of <strong>Durham</strong> – to fund research in to parents as educators.<br />
109
• Darlington Borough Council – to support the Sex Education Roadshow and<br />
to support the part time outreach worker supporting teenage parents.<br />
Action and Achievements<br />
• Appointment of Tackling <strong>Teenage</strong> <strong>Pregnancy</strong> <strong>Local</strong> Implementation Coordinator<br />
for <strong>County</strong> <strong>Durham</strong> and Darlington. (This will change to having<br />
two co-ordintors 2001/2002, one for <strong>County</strong> <strong>Durham</strong> and one for<br />
Darlington).<br />
• Allocation of funds to each PCG area to appoint a Sexual Health Outreach<br />
Worker. In two localities, it was more appropriate to sub contract the work<br />
and this was achieved.<br />
• University of <strong>Durham</strong> are partway through a Parents as Educators Action<br />
Research Project and have produced an interim report which is available<br />
locally.<br />
• <strong>County</strong> <strong>Durham</strong> have appointed a Sexual Health Trainer who is currently<br />
working with youth workers.<br />
• Darlington Social Services Department have employed an outreach worker<br />
to support teenage parents.<br />
• Other actions taken since the march 2000 report were published these are<br />
detailed in the Audit of Current Services in part A, section 3 of the strategy<br />
document.<br />
<strong>Local</strong> Implementation Funding<br />
The allocation of funding from the <strong>Teenage</strong> <strong>Pregnancy</strong> Unit <strong>Local</strong><br />
Implementation Fund for 2000/2001 was £200,000. It was allocated as follows:<br />
• <strong>Local</strong> Implementation Co-ordinator plus admin support - £35K<br />
• Outreach workers managed by Specialist Health Promotion Service but<br />
with strong links with the Youth Service - £115K<br />
(This allocation of money was topped up by the six Primary Care Groups<br />
funds to the effect of £36K to ensure that the full costs of each post were<br />
met.)<br />
• Parents As Educators Action Research - £27K<br />
• Training and Support for Youth Workers(<strong>County</strong> <strong>Durham</strong>) - £15K<br />
• Training and Support for Youth Workers(Darlington) - £8K<br />
• Support for Darlington specific local authority services - £8K<br />
110
Impact of funding<br />
• The <strong>Local</strong> Implementation Co-ordinator, guided by the steering group has<br />
worked in partnership with the representatives from Health, Education,<br />
Social Services and the Voluntary Sector to produce two strategy<br />
documents in line with the <strong>Teenage</strong> <strong>Pregnancy</strong> Unit guidance.. As they<br />
were not in post until 1 st November 200, this has been the major project on<br />
which their time has so far been spent.<br />
• The Sexual Health Outreach Workers have each made major inroads into<br />
working with groups of vulnerable and at risk young people in areas with<br />
high rates of teenage conceptions.<br />
• The Parents As Educators project is at the stage where all the data has<br />
now been collected and a useful interim report is available locally.<br />
• The Community Education Worker in <strong>County</strong> <strong>Durham</strong> and the Outreach<br />
Worker in Darlington are both newly in post but are establishing themselves<br />
in their roles and have had many positive comments made about them by<br />
their employers.<br />
Problems and Solutions<br />
• The major barriers faced in producing the strategy has been the very<br />
limited time between the local Implementation Co-ordinator taking up post<br />
on 1 st November 2000 and the deadline for submission of the strategy of<br />
30 th March 2001.<br />
• To ensure that partnerships had joined up working established and<br />
operating in reality, time first had to be invested in building relationships<br />
between the co-ordinator and the groups as well as between the group<br />
members.<br />
• This meant that the actual work to produce the ten year strategy and three<br />
year action plan was limited to approximately one month with the same<br />
amount of time available to physically write the two strategies.<br />
• The consultation stage was the also very limited so that the co-ordinator<br />
had enough time to incorporate any changes and comments.<br />
• This has been a very challenging time frame in which to produce a vital<br />
document and one of extreme importance.<br />
Support to ensure effective implementation<br />
• The over riding concern shared by professional in all agencies is the issue<br />
of staff training and of backfill for health/ social services /voluntary staff and<br />
supply cover for teaching/educational staff. This concern is shared by staff<br />
at all levels of seniority.<br />
111
• If policy at national level could address this need, it would make staff<br />
training locally a more viable proposition.<br />
PART C<br />
TEENAGE PREGNANCY<br />
LOCAL<br />
IMPLEMENTATION<br />
FUND<br />
112
<strong>Teenage</strong> <strong>Pregnancy</strong> Unit <strong>Local</strong> Implementation Fund<br />
Source and Application of Funds Statement<br />
Sources of<br />
Finance<br />
TPU <strong>Local</strong><br />
Implementation<br />
Fund (LIF)<br />
TPU Co-ordination<br />
Fund<br />
DFEE Standards<br />
Fund<br />
Year 1 Year 2 Year 3 Status Application of<br />
Funds<br />
£250,000 £250,000 £250,000 Indicative • 6 x Sexual<br />
Allocation Health Outreach<br />
Workers - £150,000<br />
• Media/advertisin<br />
g of services -<br />
£18,000<br />
• Community<br />
Education <strong>County</strong><br />
<strong>Durham</strong> and<br />
Darlington -<br />
£12,000<br />
• Co-ordination,<br />
conferences,<br />
Training and<br />
Development fund -<br />
£10,000<br />
• PCG allocation to<br />
be spent in liaison<br />
with local<br />
authorities and<br />
voluntary agencies<br />
- £60,000 (£10,000<br />
per PCG area)<br />
£60,000 £60,000 £60,000 Approved Two co-ordinators,<br />
one for <strong>County</strong><br />
<strong>Durham</strong> and one for<br />
Darlington<br />
£94,000 Unknown Unknown Approved • Support for<br />
teenage parents<br />
thus: Reintegration<br />
Officer and Child<br />
Care<br />
• 8 schools receive<br />
funds to help<br />
reduce teenage<br />
pregnancy rates<br />
113
114
PART D<br />
CERTIFICATE OF<br />
AGREEMENT AND<br />
PARTNERSHIP<br />
115
116
Conclusion<br />
• Following very clear guidelines produced by the <strong>Teenage</strong> <strong>Pregnancy</strong> Unit,<br />
this strategy has been developed using multi-agency working groups,<br />
demonstrating joined up working in <strong>County</strong> <strong>Durham</strong> and Darlington.<br />
• This document details a ten year vision and strategy together with a three<br />
year action plan for each of the following four areas:<br />
• <strong>Local</strong> Media Campaign<br />
• Better Sex & Relationships Education<br />
• Better Contraception & Advice Services<br />
• Better Support for <strong>Teenage</strong> Parents.<br />
• The annual report details how <strong>Teenage</strong> <strong>Pregnancy</strong> Unit <strong>Local</strong><br />
Implementation Funds have been spent 200-2001.<br />
• Part C details how the local implementation funds will be spent 2001-2002.<br />
Finally a huge debt of thanks is paid to all those people who aided the<br />
development and writing of this report. Members of the Steering Group<br />
and working groups have played a vital role. Particular thanks go to cowriter<br />
Irene Bell, Health Consultant. Thanks also to Beverley Palmer,<br />
Health Promotion Manager, Darlington Primary Care Group for managerial<br />
input and to Ceri Mather, Health Promotion Strategist for professional and<br />
personal support during the writing of the <strong>County</strong> <strong>Durham</strong> and Darlington<br />
Tackling <strong>Teenage</strong> <strong>Pregnancy</strong> Strategies.<br />
117