Monovision With the Light Adjustable Lens for Presbyopia ... - Iogen
Monovision With the Light Adjustable Lens for Presbyopia ... - Iogen
Monovision With the Light Adjustable Lens for Presbyopia ... - Iogen

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
COVER STORY<br />
<strong>Monovision</strong> <strong>With</strong> <strong>the</strong><br />
<strong>Light</strong> <strong>Adjustable</strong> <strong>Lens</strong> <strong>for</strong><br />
<strong>Presbyopia</strong> Correction<br />
The lens can be adjusted postoperatively to optimize monovision or<br />
switch to emmetropia in both eyes.<br />
There are a variety of <strong>the</strong>rapeutic approaches to<br />
presbyopia correction, all of which have <strong>the</strong><br />
same goal: to provide patients with spectacle<br />
independence. Currently, implantation of multifocal<br />
or accommodating IOLs and pseudophakic<br />
monovision are popular options; however, <strong>the</strong>se often<br />
require an additional refractive procedure after treatment<br />
to achieve spectacle independence. Despite<br />
advances in biometry and small-incision surgery, <strong>the</strong><br />
accuracy of IOL calculation remains limited by <strong>the</strong> variation<br />
in <strong>the</strong> measurements of corneal power, axial length,<br />
and anterior chamber depth.<br />
One potential alternative to avoid <strong>the</strong> need <strong>for</strong> secondary<br />
correction of presbyopia and residual refractive<br />
50 I CATARACT & REFRACTIVE SURGERY TODAY EUROPE I JANUARY 2009<br />
BY CHRISTOPH WINKLER VON MOHRENFELS, MD<br />
error is <strong>the</strong> <strong>Light</strong> <strong>Adjustable</strong> <strong>Lens</strong> (LAL; Calhoun Vision,<br />
Inc., Pasadena, Cali<strong>for</strong>nia). The LAL contains photosensitive<br />
macromers that enable a noninvasive postoperative<br />
adjustment of refractive power using ultraviolet light<br />
(UV light; 365 nanometers). These molecules are precisely<br />
distributed throughout <strong>the</strong> lens; approximately 2<br />
weeks after implantation, <strong>the</strong>y are irradiated with UV<br />
light to cause selective polymerization.<br />
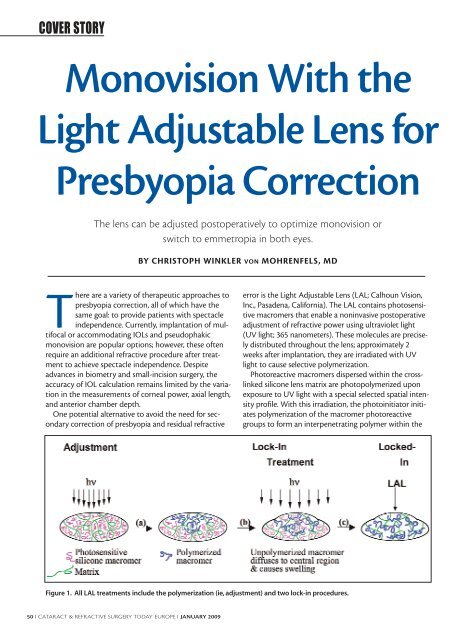
Photoreactive macromers dispersed within <strong>the</strong> crosslinked<br />
silicone lens matrix are photopolymerized upon<br />
exposure to UV light with a special selected spatial intensity<br />
profile. <strong>With</strong> this irradiation, <strong>the</strong> photoinitiator initiates<br />
polymerization of <strong>the</strong> macromer photoreactive<br />
groups to <strong>for</strong>m an interpenetrating polymer within <strong>the</strong><br />
Figure 1. All LAL treatments include <strong>the</strong> polymerization (ie, adjustment) and two lock-in procedures.
TAKE-HOME MESSAGE<br />
• Photosensitive macromers in <strong>the</strong> LAL are distributed<br />
through <strong>the</strong> lens and are polymerized when <strong>the</strong>y are<br />
irradiated with UV light.<br />
• Diffussion of <strong>the</strong> remaining, unirradiated macromers induces<br />
a change in <strong>the</strong> lens shape, <strong>the</strong> refractive index, or both.<br />
• Patients can be adjusted to emmetropia in both eyes if<br />
<strong>the</strong>y do not tolerate monovision.<br />
lens matrix. Diffusion of <strong>the</strong> remaining, unirradiated<br />
macromers into <strong>the</strong> irradiated areas induces a change in<br />
<strong>the</strong> lens shape or refractive index, or both, to produce a<br />
predictable power change. Every adjustment procedure<br />
allows 2.00 D correction of myopia, hyperopia, and astigmatism.<br />
It is important that all photoreactive macromers<br />
are polymerized, and every patient has to undergo two<br />
lock-in procedures (Figure 1).<br />
The LAL may be used during cataract surgery or <strong>for</strong><br />
refractive lens exchange. Currently <strong>for</strong> monovision, <strong>the</strong><br />
correction in <strong>the</strong> dominant eye is aimed <strong>for</strong> distance<br />
emmetropia; <strong>the</strong> o<strong>the</strong>r eye is aimed <strong>for</strong> -1.00 D. Two<br />
weeks after surgery, we evaluate patient satisfaction. If<br />
<strong>the</strong> patient is doing well with monovision, <strong>the</strong> correction<br />
is locked in. If <strong>the</strong> patient does not tolerate monovision,<br />
he is adjusted <strong>for</strong> emmetropia.<br />
CASE REPORT<br />
A 58-year-old patient presented with cataract and a<br />
preoperative refraction of -5.00 -0.50 X 170° and<br />
-5.25 -0.75 X 18° in <strong>the</strong> right and left eyes, respectively.<br />
The LAL was implanted bilaterally; <strong>the</strong> right was targeted<br />
<strong>for</strong> emmetropia and <strong>the</strong> left <strong>for</strong> -1.00 D. Two weeks after<br />
surgery, his far UCVA was 1.0 in <strong>the</strong> right eye and 0.6 in<br />
<strong>the</strong> left. Near visual acuity was J2. We discussed <strong>the</strong> possibility<br />
of more or less myopia in his left eye; however, he<br />
was satisfied with <strong>the</strong> far and near visual acuities.<br />
There<strong>for</strong>e, we locked in both eyes.<br />
CONCLUSION<br />
<strong>Monovision</strong>, with <strong>the</strong> use of this technology, provides a<br />
good refractive and visual outcome. The LAL may be able<br />
to provide a multifocal correction in <strong>the</strong> future; however,<br />
this is not yet possible. In my opinion, use of this technology<br />
will be important <strong>for</strong> <strong>the</strong> correction of presbyopia<br />
because it provides a perfect distance refraction. ■<br />
Christoph Winkler von Mohrenfels, MD, is a surgeon at<br />
Technical University, Munich, Germany. Dr. Winkler von<br />
Mohrenfels states that he has no financial interest in <strong>the</strong><br />
products or companies mentioned. He may be reached at<br />
e-mail: christoph.wvm@web.de.