Correction of Residual Hyperopia After Cataract Surgery ... - Iogen
Correction of Residual Hyperopia After Cataract Surgery ... - Iogen
Correction of Residual Hyperopia After Cataract Surgery ... - Iogen

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Correction</strong> <strong>of</strong> <strong>Residual</strong> <strong>Hyperopia</strong> <strong>After</strong> <strong>Cataract</strong> <strong>Surgery</strong><br />
Using the Light Adjustable Intraocular Lens Technology<br />
ARTURO CHAYET, CHRISTIAN A. SANDSTEDT, SHIAO H. CHANG, PAUL RHEE, BARBARA TSUCHIYAMA,<br />
AND DANIEL SCHWARTZ<br />
● PURPOSE: To determine whether residual hyperopia<br />
could be corrected postoperatively using the light adjustable<br />
lens technology in patients undergoing cataract<br />
surgery and light adjustable lens implantation.<br />
● DESIGN: Prospective, nonrandomized clinical trial.<br />
● METHODS: Fourteen eyes <strong>of</strong> 14 patients were studied. The<br />
manifest refraction, uncorrected visual acuity (UCVA), and<br />
best-corrected visual acuity (BCVA) were determined with<br />
follow-up time to determine the achieved refractive corrections<br />
and their stability.<br />
● RESULTS: Of 14 eyes, 13 eyes (92.9%) achieved <br />
0.25 diopters (D) <strong>of</strong> the target refraction at one day post<br />
lock-in, with 100% <strong>of</strong> the eyes achieving the targeted<br />
refractive adjustment within 0.5 D or better up to six<br />
months postoperative follow-up. All eyes treated show no<br />
change in manifest spherical refraction >0.25 D between<br />
one day post lock-in, and three and six months postoperative<br />
visits. The data demonstrate the stability <strong>of</strong> the<br />
achieved refractive change after the adjustment and<br />
lock-in procedures. The mean rate <strong>of</strong> change was 0.006<br />
D per month, which is six times more stable than that <strong>of</strong><br />
refractive procedures.<br />
● CONCLUSIONS: <strong>Residual</strong> hyperopia errors in the range <strong>of</strong><br />
0.25 to 2.0 D were successfully corrected with precision<br />
and significant improvement in UCVA and without<br />
compromising BCVA using the light adjustable intraocular<br />
lens technology. (Am J Ophthalmol 2009;147:392–397.<br />
© 2009 by Elsevier Inc. All rights reserved.)<br />
HYPEROPIA IS ONE OF THE LEAST DESIRABLE REfractive<br />
outcomes after cataract surgery. While<br />
careful preoperative biometry and intentional<br />
targeting for a small amount <strong>of</strong> residual myopia can<br />
prevent most hyperopic surprises, residual hyperopia has<br />
been more difficult to eliminate in refractive surgery<br />
patients who subsequently develop cataracts. Attributable<br />
to corneal changes following laser in situ keratomileusis<br />
(LASIK) or photorefractive keratectomy (PRK), corneal<br />
power is <strong>of</strong>ten overestimated, and these patients are<br />
frequently left hyperopic after cataract surgery. 1–13 A broad<br />
Accepted for publication Aug 26, 2008.<br />
From the Codet Vision Institute (A.C.), Tijuana, Mexico, Calhoun<br />
Vision Inc (C.A.S., S.H.C., P.R., B.T.), Pasadena, California, and the<br />
Department <strong>of</strong> Ophthalmology, University <strong>of</strong> California at San Francisco<br />
(D.S.), San Francisco, California.<br />
Inquiries to Arturo Chayet, Ave. Padre Kino No. 10159, Tijuana,<br />
Mexico 22320; e-mail: arturo.chayet@codetvision.com<br />
array <strong>of</strong> intraocular lens (IOL) power calculation formulas<br />
has been developed to better estimate IOL power in these<br />
patients, but most are wanting, and hyperopia remains a<br />
frequent postoperative outcome. A dramatic method to<br />
overcome refractive imprecision was recently reported by<br />
Mackool and associates 13 in which post-LASIK patients<br />
undergoing cataract surgery underwent immediate postoperative<br />
aphakic refraction and then, one half-hour later,<br />
were returned to the operating room for IOL implantation.<br />
An alternative to the difficulties inherent in predicting<br />
IOL power is use <strong>of</strong> a light adjustable lens. 14–18 The light<br />
adjustable lens contains photosensitive silicone molecules<br />
that enable postoperative, noninvasive adjustment <strong>of</strong> refractive<br />
power using ultraviolet (UV) light. The light<br />
adjustable IOL formulation consists <strong>of</strong> four basic components:<br />
1) silicone matrix polymer, 2) photoreactive macromer,<br />
3) photoinitiator, and 4) UV absorber. The light<br />
adjustable IOL formulation has been described 14 previously<br />
and is based upon the principles <strong>of</strong> photochemistry<br />
and diffusion. The application <strong>of</strong> the appropriate wavelength<br />
<strong>of</strong> light through a defined spatial irradiance pr<strong>of</strong>ile<br />
onto the light adjustable lens polymerizes macromer in the<br />
exposed region producing a change in shape and associated<br />
predictable power change. By controlling the irradiation<br />
dose (ie, beam intensity and duration) and spatial irradiance<br />
pr<strong>of</strong>ile, the refractive power <strong>of</strong> the light adjustable<br />
lens is modified to add or subtract spherical power, eliminate<br />
astigmatic error, and correct higher-order aberrations<br />
(HOAs). For example, to correct hyperopia, irradiation is<br />
preferentially applied to the center <strong>of</strong> the lens. This causes<br />
photopolymerization and subsequent diffusion <strong>of</strong> unpolymerized<br />
macromer into the irradiated zone. Subsequent<br />
swelling <strong>of</strong> the irradiated zone increases lens power to<br />
correct hyperopia. To control the amount <strong>of</strong> hyperopia<br />
corrected, the treatment duration is varied. One day after<br />
light adjustable lens adjustment, the entire lens is irradiated<br />
to polymerize the remaining photosensitive macromer<br />
and prevent additional change in lens power. This second<br />
irradiation procedure is referred to as “lock-in.”<br />
To determine whether residual hyperopia could be<br />
corrected postoperatively using the light adjustable lens<br />
technology, we performed a clinical study in patients<br />
undergoing cataract surgery with light adjustable IOL<br />
implantation. Based on preoperative biometry, light adjustable<br />
lenses were implanted that would purposely result<br />
in hyperopic refractive errors up to 2.0 diopter (D). In<br />
© 2009 BY ELSEVIER INC. ALL RIGHTS RESERVED.<br />
392 0002-9394/09/$36.00<br />
doi:10.1016/j.ajo.2008.08.039
FIGURE 1. Digital light delivery (DLD) device used to treat<br />
patients with light adjustable intraocular lens (IOL) technology.<br />
this fashion, we were able to adjust lens power and test<br />
whether a “hyperopic surprise” could be corrected in the<br />
postoperative period.<br />
METHODS<br />
A PROSPECTIVE, NONRANDOMIZED, SINGLE-CENTER CLINIcal<br />
study was conducted at Codet Vision Institute, Tijuana,<br />
Mexico. Subjects who required cataract extraction<br />
and IOL implantation and volunteered for this study were<br />
screened for eligibility. Subjects with significant anterior<br />
segment pathology, uncontrolled glaucoma, previous ocular<br />
surgery, macular deceases, current use <strong>of</strong> Flomax, or<br />
7.0 mm dilated pupil diameter were excluded. Fourteen<br />
patients (one eye per patient) were enrolled, 10 females<br />
and four males.<br />
Preoperative biometry was performed using an immersion<br />
biometry unit (Axis II Ophthalmic Echograph; Quantel<br />
Medical, Bozeman, Montana, USA), and the light<br />
adjustable IOL power was selected to result in a postoperative<br />
refractive error <strong>of</strong> up to 2.0 D <strong>of</strong> hyperopia. The<br />
light adjustable IOL is a foldable posterior chamber, UV<br />
absorbing, three-piece photoreactive silicone lens with<br />
blue polymethylmethacrylate modified-C haptics, a 6.0<br />
TABLE 1. Preoperative Refraction and Axial Length, and<br />
Implanted Light Adjustable Intraocular Lens Power for<br />
Patients With Light Adjustable Intraocular Lens<br />
Technology<br />
Eye<br />
Preoperative<br />
Sphere Cylinder Axial Length (mm)<br />
Implanted<br />
Power (D)<br />
1 2.25 1.25 15 22.76 18.0<br />
2 ND a ND a 23.16 20.0<br />
3 0.75 0.75 90 23.43 20.0<br />
4 4.00 1.50 99 22.04 23.5<br />
5 2.75 0.75 80 22.59 21.5<br />
6 2.50 0.00 0 22.63 23.5<br />
7 1.50 0.00 0 22.31 21.5<br />
8 5.00 0.75 100 22.55 23.0<br />
9 3.00 0.75 75 22.85 22.0<br />
10 3.00 0.75 75 22.90 23.0<br />
11 2.00 0.00 0 22.56 22.5<br />
12 3.25 2.00 90 23.58 20.0<br />
13 2.75 0.75 80 22.88 20.5<br />
14 1.75 0.00 0 22.79 22.5<br />
D diopters; ND not determined.<br />
a<br />
No refraction can be measured attributable to dense<br />
cataract.<br />
TABLE 2. Distribution <strong>of</strong> Refractive Adjustments<br />
Attempted for 14 Patients With Light Adjustable<br />
Intraocular Lens Technology<br />
Attempted Sphere n a /N b<br />
0.25 to 0.5 D 3/14 21.4%<br />
0.75 to 1.0 D 6/14 42.9%<br />
1.25 to 1.5 D 4/14 28.6%<br />
1.75 to 2.0 D 1/14 7.1%<br />
D diopters.<br />
a<br />
Number <strong>of</strong> eyes at each attempted sphere.<br />
b<br />
Total eyes enrolled.<br />
mm biconvex optic with squared posterior edge, and an<br />
overall length <strong>of</strong> 13.0 mm.<br />
All patients underwent phacoemulsification using a<br />
topical anesthetic, clear corneal incision (3.0 to 3.5<br />
mm) and anterior capsulotomy (5.5 mm). The light<br />
adjustable IOL <strong>of</strong> the appropriate power was implanted<br />
in the capsular bag using the Nichamin II Foldable Lens<br />
Insertion Forceps (Rhein Medical Inc, Tampa, Florida,<br />
USA). The operative eye was patched following surgery.<br />
The patch was removed the following day, and patients<br />
were instructed to wear Calhoun Vision-supplied UVblocking<br />
photochromic spectacles (7EYE, Pleasanton,<br />
California, USA) at all times when indoors and outdoors<br />
after surgery until the adjustment and lock-in<br />
procedures were completed.<br />
VOL. 147, NO. 3 PSEUDOPHAKIC HYPEROPIA CORRECTION<br />
393<br />
%
TABLE 3. Accountability <strong>of</strong> All Patients Enrolled With Light Adjustable Intraocular Lens Technology as a Function <strong>of</strong><br />
Postoperative Time<br />
The light adjustable IOL was adjusted and locked in<br />
using a digital light device engineered by Carl Zeiss<br />
Meditec (Jena, Germany). 15,16 The digital light device<br />
uses a mercury (Hg) arc lamp fitted with a narrow bandpass<br />
interference filter producing a beam at 365 nm ( 4nm<br />
full width half maximum). The digital light device generates<br />
and projects a spatial irradiance pattern onto the light<br />
adjustable IOL using a digital mirror device. The digital<br />
mirror device is a pixelated, micromechanical spatial light<br />
modulator formed monolithically on a silicon substrate.<br />
The digital mirror device chip enables customization <strong>of</strong> the<br />
irradiation pr<strong>of</strong>ile to correct not only spherical and astigmatic<br />
errors but also HOAs. The surgeon centers and<br />
focuses the treatment beam on the light adjustable lens<br />
using an alignment reticle while patient alignment is<br />
achieved using a fixation target, parcentral to the delivery<br />
beam. The digital light device is shown in Figure 1.<br />
At one to two weeks postimplantation, best-corrected<br />
and uncorrected visual acuity (VA) and residual hyperopic<br />
refractive error were measured. VA assessment and manifest<br />
refraction were performed by an optometrist who was<br />
masked to the patient’s targeted refractive outcome and<br />
light adjustable IOL power. The digital light device was<br />
then used to adjust the light adjustable IOL power to<br />
correct the hyperopic error. Refractive power adjustments<br />
are defined at the spectacle plane. A second irradiation<br />
treatment was given a minimum <strong>of</strong> 20 hours after adjustment<br />
to lock-in the lens. The following study endpoints<br />
were evaluated:<br />
1. Attempted vs achieved lens power change (manifest<br />
refraction).<br />
2. VA (best-corrected and uncorrected distance VA).<br />
3. Stability <strong>of</strong> adjusted lens power (manifest refraction).<br />
4. Complications and adverse events.<br />
RESULTS<br />
A TOTAL OF 14 EYES WERE TREATED FOR REFRACTIVE ADjustments<br />
in the range <strong>of</strong> 0.25 to 2.0 D and were<br />
followed for one to six months postoperatively. Of the 14<br />
patients, 10 were female and four were male. The average<br />
One Month Three Months Six Months<br />
Available for analysis n/N (%) 14/14 100.0% 14/14 100.0% 9/14 64.3%<br />
Discontinued n/N (%) 0/14 0.0% 0/14 0.0% 0/14 0.0%<br />
Missed visit n/N (%) 0/14 0.0% 0/14 0.0% 0/14 0.0%<br />
Not yet eligible for the interval n/N (%) 0/14 0.0% 0/14 0.0% 5/14 35.7%<br />
Lost to follow-up n/N (%) 0/14 0.0% 0/14 0.0% 0/14 0.0%<br />
% Accountability<br />
Availability for Analysis<br />
(Enrolled Discounted Notyeteligible)<br />
14/14 100% 14/14 100% 9/9 100%<br />
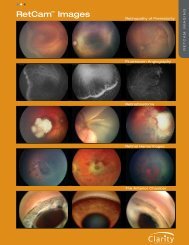
FIGURE 2. Scattergram <strong>of</strong> target vs achieved hyperopic corrections<br />
in patients with light adjustable IOL technology. The<br />
solid line represents achieved refractive adjustments in diopters<br />
(D) equal to the targeted power. Of 14 eyes adjusted, 13 (93%)<br />
achieved 0.25 D <strong>of</strong> the targeted refractive adjustment in the<br />
range <strong>of</strong> 0.25 to 2.0 D. The remaining one eye was within<br />
0.50 D <strong>of</strong> the targeted refraction.<br />
age <strong>of</strong> the study participants was 68 7 years. The power<br />
<strong>of</strong> implanted light adjustable IOL as well as preoperative<br />
refractive errors and axial length are presented in Table 1.<br />
The distribution <strong>of</strong> refractive adjustments attempted can<br />
be found in Table 2. All eyes were accounted for at the<br />
one, three, and six month postoperative visits in Table 3.<br />
There were no missed visits or any patients lost to<br />
follow-up during the study period. An additional 14<br />
patients were implanted with the light adjustable lens and<br />
treated for refractive adjustments in the range <strong>of</strong> 2.0Dto<br />
plano; these will be detailed in a separate report.<br />
● TARGET VS ACHIEVED HYPEROPIC CORRECTIONS:<br />
The accuracy <strong>of</strong> the achieved sphere to the targeted<br />
refractive adjustment is demonstrated in the scattergram<br />
presented in Figure 2 and data in Table 4. Thirteen <strong>of</strong> the<br />
14 eyes (92.9%) treated were within 0.25 D <strong>of</strong> the target<br />
refraction at one day post lock-in follow up visit with<br />
100% <strong>of</strong> the eyes achieving 0.50 D <strong>of</strong> the targeted<br />
refractive adjustment at one day post lock-in, three and six<br />
months postoperative visits. Similar results were demonstrated<br />
in the analysis <strong>of</strong> accuracy <strong>of</strong> the achieved manifest<br />
394 AMERICAN JOURNAL OF OPHTHALMOLOGY<br />
MARCH 2009
TABLE 4. Accuracy <strong>of</strong> Sphere to Target – Hyperopic <strong>Correction</strong>s in Patients With Light<br />
Adjustable Intraocular Lens Technology<br />
Sphere<br />
One Day Post Lock-In<br />
refraction spherical equivalent presented in Table 5 demonstrating<br />
no significant change was induced on cylinder.<br />
● STABILITY OF REFRACTIVE ADJUSTMENT: One hundred<br />
percent (14/14) <strong>of</strong> the eyes were stable within 0.25<br />
D with 13 eyes showing no change at one to six months<br />
follow-up visits as compared with refraction at one day<br />
after lock-in treatment (Table 6). The mean rate <strong>of</strong> change<br />
was 0.006 D per month, which is six times more stable<br />
than that <strong>of</strong> refractive procedures. 19<br />
● STABILITY OF UNCORRECTED VISUAL ACUITY: All<br />
eyes demonstrated stability <strong>of</strong> uncorrected visual acuity<br />
(UCVA) after lock-in. The bar graph <strong>of</strong> UCVA before<br />
and after refractive adjustments is shown in Figure 3. The<br />
data demonstrated significant improvement in UCVA for<br />
64% <strong>of</strong> the 14 eyes and the UCVA is stable for a follow-up<br />
period up to six months. Seventy-one percent (10/14) <strong>of</strong><br />
eyes achieved UCVA <strong>of</strong> 20/25 or better. All eyes were<br />
20/30 or better. The four eyes that did not achieve UCVA<br />
Three Months<br />
Postoperative<br />
Six Months<br />
Postoperative<br />
n/N % n/N % n/N %<br />
% within 0.25 D <strong>of</strong> attempted 13/14 92.9% 13/14 92.9% 8/9 88.9%<br />
% within 0.50 D <strong>of</strong> attempted 14/14 100.0% 14/14 100.0% 9/9 100.0%<br />
% within 1.0 D <strong>of</strong> attempted 14/14 100.0% 14/14 100.0% 9/9 100.0%<br />
D diopters.<br />
TABLE 5. Accuracy <strong>of</strong> Manifest Refraction Spherical Equivalent to Target – Hyperopic<br />
<strong>Correction</strong>s in Patients With Light Adjustable Intraocular Lens Technology<br />
MRSE<br />
One Day Post Lock-In<br />
Three Months<br />
Postoperative<br />
Six Months<br />
Postoperative<br />
n/N % n/N % n/N %<br />
% within 0.25 D <strong>of</strong> attempted 13/14 92.9% 13/14 92.9% 8/9 88.9%<br />
% within 0.50 D <strong>of</strong> attempted 14/14 100.0% 14/14 100.0% 9/9 100.0%<br />
% within 1.0 D <strong>of</strong> attempted 14/14 100.0% 14/14 100.0% 9/9 100.0%<br />
D diopter; MRSE manifest refraction spherical equivalent.<br />
TABLE 6. Stability <strong>of</strong> Refractive Adjustment in Patients<br />
With Light Adjustable Intraocular Lens Technology<br />
Change <strong>of</strong> Refraction (D) Number <strong>of</strong> Eyes Total 14 Follow-up Time (mos)<br />
0 13 1–6<br />
0.25 1 1–3<br />
D diopters; mos months.<br />
<strong>of</strong> 20/25 or better had residual astigmatism that was not<br />
treated.<br />
● STABILITY OF BEST-CORRECTED VISUAL ACUITY: BCVA<br />
before and after refractive adjustments is displayed in<br />
Figure 4. All 14 eyes were stable and able to maintain<br />
their preadjustment BCVA following refractive adjustment<br />
and lock-in treatments with follow-up time up to<br />
six months.<br />
● COMPLICATIONS: Any adverse events or complications<br />
were recorded. In addition to typical adverse events associated<br />
with IOLs, we looked carefully for evidence <strong>of</strong><br />
uveitis, UV keratopathy, elevated intraocular pressure,<br />
posterior capsular opacity, glare, and halos. There were no<br />
adverse events or complications reported.<br />
DISCUSSION<br />
HYPEROPIC REFRACTIVE ERROR AFTER CATARACT SURgery<br />
is particularly undesirable since affected patients have<br />
no clear uncorrected far point. <strong>Residual</strong> hyperopia is<br />
particularly common after corneal refractive procedures<br />
where preoperative keratometry measurements are unreliable.<br />
Despite a wide array <strong>of</strong> empirical formulas, IOL power<br />
remains difficult to predict in patients who develop cataracts<br />
after refractive surgery. Herein, we demonstrate<br />
feasibility <strong>of</strong> correcting residual hyperopic error after cataract<br />
surgery using the light adjustable lens technology.<br />
VOL. 147, NO. 3 PSEUDOPHAKIC HYPEROPIA CORRECTION<br />
395
FIGURE 3. Bar graph <strong>of</strong> uncorrected visual acuity (UCVA) before and after hyperopic corrections in patients with light<br />
adjustable IOL technology. UCVA was expressed by converting the Snellen fraction to a numerical number, 20/20 1.0,<br />
20/25 0.8, 20/30 0.67, 20/40 0.5, 20/50 0.4, 20/60 0.33, 20/80 0.25, and 20/100 0.2. Significant<br />
improvement in UCVA was observed in 64% <strong>of</strong> eyes. Of 14 eyes, 10 eyes (71%) achieved an UCVA <strong>of</strong> 20/25 or better. All<br />
eyes were 20/30 or better and stable for a follow-up period up to six months.<br />
FIGURE 4. Bar graph <strong>of</strong> best-corrected visual acuity (BCVA) before and after hyperopic corrections in patients with light<br />
adjustable IOL technology. BCVA was expressed by converting the Snellen fraction to a numerical number, 20/20 1.0,<br />
20/25 0.8, 20/30 0.67, 20/40 0.5, 20/50 0.4, 20/60 0.33, 20/80 0.25, and 20/100 0.2. All eyes were stable<br />
and able to maintain their preadjustment BCVA.<br />
<strong>Correction</strong> <strong>of</strong> hyperopia between 0.25 to 2.0 D was<br />
achieved with 90% <strong>of</strong> patients corrected to within 0.25<br />
D <strong>of</strong> the intended refraction. While this was a feasibility<br />
study and adjustments were performed in patients who had<br />
not had previous refractive surgery, it is likely that correction<br />
<strong>of</strong> hyperopia could be performed in a similar fashion in<br />
these patients as well.<br />
Uncorrected VA improved in 64% <strong>of</strong> patients while<br />
BCVAs was maintained after lock-in in all patients. The<br />
uncorrected and best-corrected VAs were stable for all<br />
patients up to six months follow-up visit. One hundred<br />
percent <strong>of</strong> the eyes were stable within 0.25 D with 13<br />
eyes showing no change at one to six months follow-up<br />
visits.<br />
396 AMERICAN JOURNAL OF OPHTHALMOLOGY<br />
MARCH 2009
An important aspect <strong>of</strong> the light adjustable lens is the<br />
need to wear UV protective spectacles until lock-in is<br />
performed. This is because the photoreactive silicone<br />
macromer undergoes photopolymerization when exposed<br />
to UV light. The light adjustable lens has approximately<br />
one hour <strong>of</strong> built in UV protection in the absence <strong>of</strong><br />
sunglasses (Chang SH, unpublished data, 2006), but after<br />
that, there is a risk for photopolymerization and optical<br />
changes. Therefore, patients are instructed to wear the UV<br />
blocking sunglasses until lock-in is completed. <strong>After</strong> lockin,<br />
no UV protection is necessary.<br />
While this study demonstrates precise adjustment <strong>of</strong><br />
hyperopia between 0.25 to 2.0 D, the eye would<br />
require a second adjustment to correct more than 2.0 D<br />
before lock-in. Chemical analysis <strong>of</strong> light adjustable lenses<br />
reveals that photoreactive macromer is available to undergo<br />
multiple photo-polymerization leading to additional<br />
refractive change as long as the lens is not locked-in. In<br />
vitro studies have achieved a 3.5 D power change with<br />
secondary adjustments <strong>of</strong> light adjustable lenses.<br />
The light adjustable lens and digital light device provide<br />
surgeons a means to fine tune refractive power in the<br />
postoperative period. In this small pilot series <strong>of</strong> patients<br />
treated for residual hyperopia, adjustments were precise<br />
and stable for up to six months follow-up. This technology<br />
may provide greater confidence in final refractive outcome<br />
as increasing numbers <strong>of</strong> corneal refractive surgery patients<br />
age and develop cataracts.<br />
THIS STUDY WAS SUPPORTED BY SMALL BUSINESS INNOVATIVE RESEARCH GRANT NO. EY12181-02. DRS SANDSTEDT, CHANG,<br />
Rhee, and Tsuchiyama are Calhoun Vision employees. Dr Chayet is a clinical investigator for Calhoun Vision. Dr Schwartz is the founder <strong>of</strong> Calhoun<br />
Vision with financial interest. Involved in design <strong>of</strong> study (A.C., C.S., S.C., B.T., P.R., D.S.); conduct <strong>of</strong> study (A.C.); collection, management, analysis<br />
and interpretation <strong>of</strong> the data (A.C., C.S., S.C., P.R., B.T., D.S.); preparation <strong>of</strong> the manuscript (A.C., S.C., D.S.); and review or approval <strong>of</strong> the<br />
manuscript (A.C., C.S., S.C., B.T., P.R., D.S.). The clinical trial was approved and registered with Ministry <strong>of</strong> Health, the Secretaria de Salud, No.<br />
204/004209, in Mexico City, Mexico. The studies were approved by Codet Vision Institute Institutional Review Board, Comite De Investigacion y Etica,<br />
in Tijuan, Mexico. The study was performed in accordance with the Declaration <strong>of</strong> Helsinki and all patients gave written informed consent for research.<br />
REFERENCES<br />
1. Pepose JS, Lim-Bon-Siong R, Mardelli P. Future shock: the<br />
long-term consequences <strong>of</strong> refractive surgery. Br J Ophthalmol<br />
1997;81:428–429.<br />
2. Seitz B, Langenbucher A, Nguyen NX, Kus MM, Kuchle M.<br />
Underestimation <strong>of</strong> intraocular lens power for cataract surgery<br />
after myopic photorefractive keratectomy. Ophthalmology<br />
1999;106:693–702.<br />
3. Koch DD, Wang L. Calculating IOL power in eyes that have<br />
had refractive surgery. J <strong>Cataract</strong> Refract Surg 2003;29:<br />
2039–2042.<br />
4. Hamed AM, Wang L, Misra M, Koch DD. A comparative<br />
analysis <strong>of</strong> five methods <strong>of</strong> determining corneal refractive<br />
power in eyes that have undergone myopic laser in situ<br />
keratomileusis. Ophthalmology 2002;109:651–658.<br />
5. Rosa N, Capasso L, Lanza M, et al. Reliability <strong>of</strong> a new<br />
correcting factor in calculating intraocular lens power after<br />
refractive corneal surgery. J <strong>Cataract</strong> Refract Surg 2005;31:<br />
1020–1024.<br />
6. Shammas HJ, Shammas MC, Garabet A, et al. Correcting<br />
the corneal power measurements for intraocular lens power<br />
calculations after myopic laser in situ keratomileusis. Am J<br />
Ophthalmol 2003;136:426–432.<br />
7. Latkany RA, Chokshi AR, Speaker MG, et al. Intraocular<br />
lens calculations after refractive surgery. J <strong>Cataract</strong> Refract<br />
Surg 2005;31:562–570.<br />
8. Gimbel HV, Sun R. Accuracy and predictability <strong>of</strong> intraocular<br />
lens power calculation after laser in situ keratomileusis.<br />
J <strong>Cataract</strong> Refract Surg 2001;27:571–576.<br />
9. Sónego-Krone S, López-Moreno G, Beaujon-Balbi OV, et al.<br />
A direct method to measure the power <strong>of</strong> the central cornea<br />
after myopic laser in situ keratomileusis. Arch Ophthalmol<br />
2004;122:159–166.<br />
10. H<strong>of</strong>fer KJ. Intraocular lens power calculation for eyes after<br />
refractive keratotomy. J Refract Surg 1995;11:490–493.<br />
11. Koch DD, Wang L. Calculating IOL power in eyes that have<br />
had refractive surgery [editorial]. J <strong>Cataract</strong> Refract Surg<br />
2003;29:2039–2042.<br />
12. Masket S, Masket SE. Simple regression formula for intraocular<br />
lens power adjustment in eyes requiring cataract surgery<br />
after excimer laser photoablation. J <strong>Cataract</strong> Refract Surg<br />
2006;32:430–434.<br />
13. Mackool RJ, Ko W, Mackool R. Intraocular lens power<br />
calculation after laser in situ keratomileusis; aphakic refraction<br />
technique. J <strong>Cataract</strong> Refract Surg 2006;32:435–437.<br />
14. Schwartz DM. Light-adjustable lens. Trans Am Ophthalmol<br />
Soc 2003;101:417–436.<br />
15. Schwartz DM, Sandstedt CA, Chang SH, et al. Lightadjustable<br />
lens: development <strong>of</strong> in vitro nomograms. Trans<br />
Am Ophthalmol Soc 2004;102:67–72; discussion 72–74.<br />
16. Sandstedt CA, Chang SH, Grubbs RH, Schwartz DM. Light<br />
adjustable lens: customizing correction for multifocality and<br />
higher-order aberrations. Trans Am Ophthalmol Soc 2006;<br />
104:29–39.<br />
17. Olson R, Mamalis N, Hauge B. A light adjustable lens with<br />
injectable optics. Ophthalmol Clin North Am 2006;19:135–<br />
142.<br />
18. Hayashi K, Hayashi H. Comparison <strong>of</strong> the stability <strong>of</strong> 1-piece<br />
and 3-piece acrylic intraocular lenses in the lens capsule. J<br />
<strong>Cataract</strong> Refract Surg 2005;31:337–342.<br />
19. ANSI Z80.11-2007, American National Standard for Ophthalmics<br />
– Laser Systems for Corneal Reshaping.<br />
VOL. 147, NO. 3 PSEUDOPHAKIC HYPEROPIA CORRECTION<br />
397
Biosketch<br />
Artura Chayet, MD, is the Director <strong>of</strong> Codet Vision Institute, in Tijuana, Mexico and a Past-President <strong>of</strong> the Mexican<br />
Society <strong>of</strong> Refractive <strong>Surgery</strong>. He received his degree in Cornea and Refractive <strong>Surgery</strong> at the University <strong>of</strong> California,<br />
San Diego, California. Dr Chayet has become one <strong>of</strong> the world’s leading refractive surgeons. He has been recognized<br />
worldwide for contributing to the development <strong>of</strong> instruments, techniques, and s<strong>of</strong>tware used in refractive surgery today.<br />
397.e1 AMERICAN JOURNAL OF OPHTHALMOLOGY<br />
MARCH 2009