The role of contractual arrangements in improving health sector ...
The role of contractual arrangements in improving health sector ...
The role of contractual arrangements in improving health sector ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Morocco<br />
Draft<br />
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong><br />
<strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g<br />
<strong>health</strong> <strong>sector</strong> performance<br />
Experience from countries <strong>of</strong> the<br />
Eastern Mediterranean Region<br />
Tunisia<br />
Egypt<br />
Lebanon<br />
Jordan<br />
Iran<br />
Afghanistan<br />
Bahra<strong>in</strong><br />
Pakistan
© World Health Organization 2006<br />
All rights reserved.<br />
<strong>The</strong> designations employed and the presentation <strong>of</strong> the material <strong>in</strong> this publication do not imply the<br />
expression <strong>of</strong> any op<strong>in</strong>ion whatsoever on the part <strong>of</strong> the World Health Organization concern<strong>in</strong>g the<br />
legal status <strong>of</strong> any country, territory, city or area or <strong>of</strong> its authorities, or concern<strong>in</strong>g the delimitation<br />
<strong>of</strong> its frontiers or boundaries. Dotted l<strong>in</strong>es on maps represent approximate border l<strong>in</strong>es for which<br />
there may not yet be full agreement.<br />
<strong>The</strong> mention <strong>of</strong> specific companies or <strong>of</strong> certa<strong>in</strong> manufacturers’ products does not imply that they<br />
are endorsed or recommended by the World Health Organization <strong>in</strong> preference to others <strong>of</strong> a similar<br />
nature that are not mentioned. Errors and omissions excepted, the names <strong>of</strong> proprietary products are<br />
dist<strong>in</strong>guished by <strong>in</strong>itial capital letters.<br />
<strong>The</strong> World Health Organization does not warrant that the <strong>in</strong>formation conta<strong>in</strong>ed <strong>in</strong> this publication<br />
is complete and correct and shall not be liable for any damages <strong>in</strong>curred as a result <strong>of</strong> its use.<br />
Publications <strong>of</strong> the World Health Organization can be obta<strong>in</strong>ed from Distribution and Sales, World<br />
Health Organization, Regional Office for the Eastern Mediterranean, PO Box 7608, Nasr City,<br />
Cairo 11371, Egypt (tel: +202 670 2535, fax: +202 670 2492; email: DSA@emro.who.<strong>in</strong>t).<br />
Requests for permission to reproduce WHO EMRO publications, <strong>in</strong> part or <strong>in</strong> whole, or to translate<br />
them – whether for sale or for noncommercial distribution – should be addressed to the Regional<br />
Adviser, Health and Biomedical Information, at the above address (fax: +202 276 5400; email<br />
HBI@emro.who.<strong>in</strong>t).
CONTENTS<br />
FOREWORD.............................................................................................................................. 4<br />
PART ONE: INTRODUCTION AND SYNTHESIS OF COUNTRY EXPERIENCES<br />
1. INTRODUCTION ............................................................................................................ 6<br />
2. SUMMARY ANALYSIS OF COUNTRY EXPEREINCES .......................................... 10<br />
2.1 Introduction ........................................................................................................... 10<br />
2.2 Approach and methodolgy..................................................................................... 10<br />
2.3 Results ................................................................................................................... 11<br />
2.4 Discussion.............................................................................................................. 27<br />
2.5 References ............................................................................................................. 32<br />
3. CONCLUSIONS AND RECOMMENDATIONS OF THE REGIONAL MEETING<br />
ON THE ROLE OF CONTRACTUAL ARRANGEMENTS, CAIRO, APRIL 2005.... 33<br />
PART TWO: COUNTRY STUDIES<br />
AFGHANISTAN ...................................................................................................................... 38<br />
BAHRAIN................................................................................................................................ 48<br />
EGYPT ..................................................................................................................................... 63<br />
ISLAMIC REPUBLIC OF IRAN ............................................................................................ 86<br />
JORDAN ................................................................................................................................ 104<br />
LEBANON ............................................................................................................................. 148<br />
MOROCCO............................................................................................................................ 179<br />
PAKISTAN ............................................................................................................................. 199<br />
TUNISIA ................................................................................................................................ 227
FOREWORD<br />
Contract<strong>in</strong>g out <strong>of</strong> publicly f<strong>in</strong>anced <strong>health</strong> services to the private <strong>sector</strong> has been<br />
the subject <strong>of</strong> extensive debate and discussion for many years among public <strong>health</strong><br />
pr<strong>of</strong>essionals across the world. Indeed, <strong>in</strong> 2003 the World Health Assembly issued a<br />
resolution <strong>in</strong> which it asked Member States to assess the <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong><br />
<strong>in</strong> improv<strong>in</strong>g <strong>health</strong> systems’ performance. <strong>The</strong> resolution provided impetus for<br />
undertak<strong>in</strong>g a multi-country study to better document this experience.<br />
This publication is the result <strong>of</strong> a systematic analysis <strong>of</strong> contract<strong>in</strong>g out <strong>of</strong> <strong>health</strong><br />
services conducted dur<strong>in</strong>g 2004–2005 <strong>in</strong> 10 countries <strong>of</strong> the WHO Eastern Mediterranean<br />
Region: Afghanistan, Bahra<strong>in</strong>, Islamic Republic <strong>of</strong> Iran, Egypt, Jordan, Lebanon,<br />
Morocco, Pakistan, Syrian Arab Republic and Tunisia. It assesses the range <strong>of</strong> <strong>health</strong><br />
services contracted out, the process <strong>of</strong> contract<strong>in</strong>g, features <strong>of</strong> specific <strong>in</strong>terventions, and<br />
factors that <strong>in</strong>fluence contract<strong>in</strong>g out.<br />
Contract<strong>in</strong>g is not synonymous with privatization <strong>of</strong> <strong>health</strong> services. Instead, it<br />
provides an opportunity to better manage the private providers <strong>in</strong> countries with poor<br />
regulatory capacity. When used judiciously, it has the potential to improve <strong>health</strong> system<br />
performance. It can <strong>in</strong>fluence access, equity, quality and efficiency <strong>of</strong> <strong>health</strong> services,<br />
create an environment conducive to public–private collaboration, and promote public<br />
<strong>health</strong> goals. However, the process is challeng<strong>in</strong>g and requires transparent procedures,<br />
well-designed contracts, clear performance obligations and credible fund<strong>in</strong>g mechanisms.<br />
In addition, governments need to be able to monitor the contracts and have credibility as<br />
a trustworthy partner.<br />
Contract<strong>in</strong>g with the private <strong>sector</strong> may seem to be the only way to get the system<br />
mov<strong>in</strong>g quickly <strong>in</strong> post-conflict situations, but the risk <strong>of</strong> bypass<strong>in</strong>g the opportunity for<br />
longer term <strong>health</strong> system development makes this area an important focus for research<br />
and debate. Contract<strong>in</strong>g, thus, is a means rather than an end <strong>in</strong> itself, and should be used<br />
primarily to promote public <strong>health</strong> objectives.<br />
This publication is the first organized effort to review the process <strong>of</strong> outsourc<strong>in</strong>g <strong>of</strong><br />
<strong>health</strong> services among countries <strong>of</strong> the Region, recogniz<strong>in</strong>g that there are gaps <strong>in</strong><br />
<strong>in</strong>formation on the subject which need to be addressed. At the same time, it provides a<br />
basis for develop<strong>in</strong>g a regional strategy on the subject, strengthen<strong>in</strong>g awareness and<br />
capacity among policy-makers and senior managers, and creat<strong>in</strong>g dialogue on the subject<br />
to formulate evidence-based national polices and strategies.<br />
Husse<strong>in</strong> A. Gezairy MD FRCS<br />
Regional Director for the Eastern Mediterranean<br />
4
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
PART ONE: INTRODUCTION AND<br />
SYNTHESIS OF COUNTRY EXPERIENCES<br />
5
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
1. INTRODUCTION<br />
<strong>The</strong> <strong>in</strong>efficiencies <strong>of</strong> publicly f<strong>in</strong>anced and provided <strong>health</strong> services <strong>in</strong> develop<strong>in</strong>g<br />
countries has led many <strong>health</strong> policy-makers to consider alternate means <strong>of</strong> service<br />
provision. Contract<strong>in</strong>g out publicly f<strong>in</strong>anced <strong>health</strong> services to private <strong>sector</strong><br />
organizations or to autonomous public providers is one such <strong>in</strong>tervention. Advocates<br />
claim that the contract<strong>in</strong>g out <strong>of</strong> <strong>health</strong> care services will improve service delivery<br />
performance by stimulat<strong>in</strong>g competition among providers and by creat<strong>in</strong>g economic<br />
<strong>in</strong>centives for improved performance through l<strong>in</strong>k<strong>in</strong>g payment to provider performance.<br />
Critics, however, argue that, <strong>in</strong> many develop<strong>in</strong>g country contexts, contract<strong>in</strong>g out is<br />
unlikely to achieve its <strong>in</strong>tended objectives because the costs <strong>of</strong> adm<strong>in</strong>ister<strong>in</strong>g contract<strong>in</strong>gout<br />
<strong>in</strong>itiatives are high and the market assumptions regard<strong>in</strong>g the number <strong>of</strong> private<br />
providers to compete for contracts are unrealistic [1].<br />
Contract<strong>in</strong>g has been def<strong>in</strong>ed as a purchas<strong>in</strong>g mechanism used to acquire a<br />
specified service, <strong>of</strong> a def<strong>in</strong>ed quality and quantity, at an agreed-on price, from a specific<br />
provider, for a specified period [2].TP PThrough this arrangement one party, the pr<strong>in</strong>cipal or<br />
purchaser, provides compensation to another party, the agent or provider, <strong>in</strong> exchange for<br />
a def<strong>in</strong>ed set <strong>of</strong> <strong>health</strong> services for a def<strong>in</strong>ed target population [3].TP PT<br />
Non-cl<strong>in</strong>ical contract<strong>in</strong>g out <strong>in</strong> the <strong>health</strong> <strong>sector</strong> has been go<strong>in</strong>g on for several<br />
decades. <strong>The</strong> renewed <strong>in</strong>terest <strong>in</strong> contract<strong>in</strong>g has arisen due to the potential for<br />
contract<strong>in</strong>g out cl<strong>in</strong>ical services—hospital as well as primary <strong>health</strong> care—to private<br />
<strong>sector</strong> providers or <strong>in</strong> certa<strong>in</strong> cases to autonomous public <strong>sector</strong> organizations when the<br />
latter have characteristics <strong>of</strong> private providers.<br />
Contract<strong>in</strong>g does not mean privatization. Contract<strong>in</strong>g out should be considered as<br />
an alternate management and regulatory tool <strong>in</strong> the hands <strong>of</strong> public <strong>sector</strong> managers to<br />
achieve public <strong>health</strong> goals, which sometimes are difficult to achieve through direct<br />
provision <strong>of</strong> services. <strong>The</strong>re are several options for contract<strong>in</strong>g between the public and<br />
private <strong>sector</strong>. <strong>The</strong>se <strong>in</strong>clude contract<strong>in</strong>g out or outsourc<strong>in</strong>g, contract<strong>in</strong>g <strong>in</strong>, procurement,<br />
leas<strong>in</strong>g, and subsidy and franchis<strong>in</strong>g. Table 1 provides a brief description <strong>of</strong> each <strong>of</strong> these.<br />
This regional study has focused on the contract<strong>in</strong>g out or outsourc<strong>in</strong>g <strong>of</strong> publicly<br />
f<strong>in</strong>anced services to the private <strong>sector</strong>.<br />
<strong>The</strong> key elements <strong>of</strong> types <strong>of</strong> contract<strong>in</strong>g out vary, depend<strong>in</strong>g on a range <strong>of</strong> factors<br />
that <strong>in</strong>clude the follow<strong>in</strong>g [1]:<br />
• Who are the purchasers: governments, donors, public <strong>in</strong>surers, or private <strong>in</strong>surers?<br />
• Who are the providers: public or private, for-pr<strong>of</strong>it or not-for-pr<strong>of</strong>it, hospitals or<br />
physicians or and <strong>health</strong> workers?<br />
6
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
• What services are contracted out: cl<strong>in</strong>ical or non-cl<strong>in</strong>ical, <strong>in</strong>patients or outpatients,<br />
preventive or curative?<br />
• How are the providers paid: <strong>in</strong>put-based or cost-based, output-based, outcome-based,<br />
or performance-based?<br />
• What are the objectives <strong>of</strong> contract<strong>in</strong>g out: to <strong>in</strong>crease efficiency and productivity, to<br />
promote access to <strong>health</strong> care, to improve quality <strong>of</strong> care, to save costs; to improve<br />
<strong>health</strong> outcomes, or to improve the performance <strong>of</strong> <strong>health</strong> care delivery (the latter can<br />
<strong>in</strong>clude more than one specific objective)?<br />
Table 1. Contract<strong>in</strong>g options for purchas<strong>in</strong>g <strong>health</strong> services [2]<br />
Options Applications<br />
Contract<strong>in</strong>gout<br />
or<br />
outsourc<strong>in</strong>g<br />
Purchase one or more services from an outside source that<br />
provides the service to either a government entity or patients,<br />
us<strong>in</strong>g primarily an external work force and resources. Examples<br />
<strong>of</strong> services provided to government entities <strong>in</strong>clude send<strong>in</strong>g<br />
l<strong>in</strong>ens out to a private laundry or secur<strong>in</strong>g cl<strong>in</strong>ical laboratory<br />
services from a private laboratory.<br />
Examples <strong>of</strong> services provided to patients might <strong>in</strong>clude<br />
contract<strong>in</strong>g with a nongovernmental organization to manage a<br />
number <strong>of</strong> district facilities, or to provide a service package to<br />
identified users <strong>in</strong> their own facilities.<br />
Contract<strong>in</strong>g-<br />
Purchase management services from an outside source that is<br />
a<br />
<strong>in</strong>P P<br />
assigned responsibility for manag<strong>in</strong>g on <strong>in</strong>ternal service or<br />
work force. Examples <strong>in</strong>clude hir<strong>in</strong>g a private firm to manage a<br />
hospital’s housekeep<strong>in</strong>g staff (most <strong>of</strong> whom rema<strong>in</strong> publicly<br />
employed) or external technical assistance to direct an <strong>in</strong>ternal<br />
task force.<br />
Procurement Purchase supplies or materials from one or more outside<br />
sources, as <strong>in</strong> the purchase <strong>of</strong> medic<strong>in</strong>e, food, or medical<br />
equipment Procurement contracts are typically used when a<br />
large volume <strong>of</strong> goods—<strong>in</strong> terms <strong>of</strong> number or cost—are to be<br />
acquired.<br />
Lease or<br />
rental<br />
Secur<strong>in</strong>g the use, but not the ownership, <strong>of</strong> facilities or<br />
equipment from an outside source under a lease agreement.<br />
Leas<strong>in</strong>g is usually used for capital-<strong>in</strong>tensive items. Examples<br />
<strong>in</strong>clude the leas<strong>in</strong>g <strong>of</strong> build<strong>in</strong>gs, specialized medical equipment,<br />
and vehicles.<br />
Subsidy or<br />
Direct or <strong>in</strong>direct f<strong>in</strong>ancial support <strong>in</strong>tended to alter the<br />
b<br />
subventionP P<br />
provision or production <strong>of</strong> a selected service. Direct subsidies<br />
<strong>in</strong>clude grants and budgetary support; <strong>in</strong>direct subsidies may be<br />
<strong>in</strong> the form <strong>of</strong> tax exemptions. Subvention is a form <strong>of</strong> subsidy<br />
commonly used <strong>in</strong> Africa where government provides f<strong>in</strong>ancial<br />
support to religiously sponsored charity hospitals <strong>in</strong> areas not<br />
served by public facilities. <strong>The</strong>se <strong>arrangements</strong> may or may not<br />
be formalized by contract.<br />
Franchise A contractor, or franchisee, is granted the right which may or<br />
may not be exclusive, to provide specified services to a def<strong>in</strong>ed<br />
clientele or <strong>in</strong> a specified geographic region. <strong>The</strong> contractor is<br />
7
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
given the right to collect and reta<strong>in</strong> revenues, but is required to<br />
pay a fee or a percentage to the government for the privilege <strong>of</strong><br />
do<strong>in</strong>g so.<br />
a. Contract<strong>in</strong>g-<strong>in</strong> should not be confused with <strong>in</strong>ternal contracts among governmental agencies. Contract<strong>in</strong>g-<strong>in</strong>, as<br />
used here and <strong>in</strong> some countries (such as <strong>in</strong> Cambodia), refers to br<strong>in</strong>g<strong>in</strong>g <strong>in</strong> outside private management to<br />
operate an <strong>in</strong>ternal government service.<br />
b. Subvention is also used as a public f<strong>in</strong>ance term <strong>in</strong> many Eastern European countries for reallocation <strong>of</strong> f<strong>in</strong>ancial<br />
flows across geographic regions.<br />
Contract<strong>in</strong>g out <strong>health</strong> services is an <strong>in</strong>creas<strong>in</strong>gly prevalent phenomenon <strong>in</strong><br />
develop<strong>in</strong>g countries and governments <strong>in</strong> all regions contract out some type <strong>of</strong> <strong>health</strong> care<br />
service. In develop<strong>in</strong>g countries, contract<strong>in</strong>g out has been an element <strong>of</strong> <strong>health</strong> system<br />
reform programmes <strong>of</strong>ten under the <strong>in</strong>fluence <strong>of</strong> multilateral and bilateral agencies.<br />
<strong>The</strong>se agencies promote a new <strong>role</strong> for the state <strong>in</strong> <strong>health</strong> care provision. Specifically,<br />
they emphasize the state’s <strong>role</strong> as a catalyst for competition among providers and as a<br />
force that encourages greater utilization <strong>of</strong> private providers, rather than promot<strong>in</strong>g the<br />
state as the dispenser <strong>of</strong> services itself.<br />
Contract<strong>in</strong>g out <strong>of</strong> <strong>health</strong> services is receiv<strong>in</strong>g <strong>in</strong>creas<strong>in</strong>g attention among low- and<br />
middle-<strong>in</strong>come countries, but evidence relat<strong>in</strong>g to the benefits and risks <strong>of</strong> the approach,<br />
while accumulat<strong>in</strong>g, is far from conclusive. Despite the grow<strong>in</strong>g experience with<br />
contract<strong>in</strong>g out <strong>of</strong> <strong>health</strong> services <strong>in</strong> develop<strong>in</strong>g countries, limited evidence exists on the<br />
impact these programmes have had on equity, quality, and efficiency or on <strong>health</strong><br />
outcomes.<br />
Resolution WHA56.25 endorsed by the World Health Assembly <strong>in</strong> 2003 asked<br />
Member States to assess the <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> system<br />
performance [4]. <strong>The</strong>re is limited experience, and even less documentation, on<br />
contract<strong>in</strong>g out <strong>of</strong> publicly f<strong>in</strong>anced <strong>health</strong> services among countries <strong>of</strong> the Eastern<br />
Mediterranean Region, although several are at various stages <strong>of</strong> implement<strong>in</strong>g <strong>health</strong><br />
<strong>sector</strong> reforms. <strong>The</strong>re is <strong>in</strong>creas<strong>in</strong>g realization with<strong>in</strong> the Region, as elsewhere, <strong>of</strong> the<br />
importance <strong>of</strong> awareness creation and capacity-build<strong>in</strong>g with<strong>in</strong> m<strong>in</strong>istries <strong>of</strong> <strong>health</strong> <strong>in</strong><br />
contract<strong>in</strong>g out publicly f<strong>in</strong>anced <strong>health</strong> services to the private <strong>sector</strong>.<br />
<strong>The</strong> purpose <strong>of</strong> this document is to share experience <strong>in</strong> contract<strong>in</strong>g from among 10<br />
countries <strong>of</strong> the Region: Afghanistan, Bahra<strong>in</strong>, Islamic Republic <strong>of</strong> Iran, Egypt, Jordan,<br />
Lebanon, Morocco, Pakistan, Syrian Arab Republic and Tunisia. <strong>The</strong> country studies on<br />
contract<strong>in</strong>g <strong>of</strong> publicly f<strong>in</strong>anced services were undertaken between January and<br />
September 2004. Countries were identified represent<strong>in</strong>g the Region, based on the size <strong>of</strong><br />
the private <strong>sector</strong>, on anecdotal evidence <strong>of</strong> experience with <strong>contractual</strong> <strong>arrangements</strong>,<br />
and implementation <strong>of</strong> a programme <strong>in</strong> which <strong>contractual</strong> arrangement with the private<br />
<strong>sector</strong> was the pr<strong>in</strong>cipal strategy.<br />
8
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
<strong>The</strong> study objectives were to: 1) assess the capacity <strong>of</strong> the m<strong>in</strong>istries <strong>of</strong> <strong>health</strong> to<br />
outsource <strong>health</strong> services; 2) review a specific <strong>health</strong> <strong>in</strong>tervention that has taken up<br />
<strong>contractual</strong> <strong>arrangements</strong> as its implementation strategy; and 3) identify key factors that<br />
<strong>in</strong>fluence outsourc<strong>in</strong>g. <strong>The</strong> country studies were presented by the country <strong>in</strong>vestigators <strong>in</strong><br />
a regional meet<strong>in</strong>g <strong>in</strong> April 2005. What follows <strong>in</strong> part one is a summary analysis <strong>of</strong> the<br />
f<strong>in</strong>d<strong>in</strong>gs <strong>of</strong> all the country studies, along with a set <strong>of</strong> recommendations on the <strong>role</strong> <strong>of</strong><br />
contract<strong>in</strong>g <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> system performance developed jo<strong>in</strong>tly by the participants<br />
<strong>of</strong> the regional meet<strong>in</strong>g. Part two conta<strong>in</strong>s selected country studies.<br />
This is the first organized effort to review outsourc<strong>in</strong>g <strong>of</strong> <strong>health</strong> services among<br />
countries <strong>of</strong> the Eastern Mediterranean Region. All ten country studies have contributed<br />
to acquir<strong>in</strong>g a better understand<strong>in</strong>g <strong>of</strong> the subject <strong>in</strong> the Region. All studies have<br />
reviewed features <strong>of</strong> the contract<strong>in</strong>g process <strong>in</strong> their respective countries. However, on its<br />
own each study is different <strong>in</strong> the manner <strong>in</strong> which it depicts the overall policy <strong>of</strong> the<br />
country, its experience with contract<strong>in</strong>g, and the extent and quality <strong>of</strong> the documentation<br />
<strong>of</strong> the experience. While each country study has aimed to collect the best evidence, it is<br />
recognized that there are gaps <strong>in</strong> <strong>in</strong>formation on the subject which need to be filled <strong>in</strong><br />
future efforts.<br />
<strong>The</strong> summary analysis attempts to pull together and synthesize the f<strong>in</strong>d<strong>in</strong>gs <strong>of</strong> the<br />
country studies, and identify the strengths and limitations <strong>of</strong> this multi-country study on<br />
contract<strong>in</strong>g. It is hoped that this effort will serve as the basis for future and more <strong>in</strong> depth<br />
studies on contract<strong>in</strong>g out <strong>of</strong> <strong>health</strong> services so as to assist countries <strong>in</strong> formulat<strong>in</strong>g more<br />
rational and evidence-based policies and strategies on the subject.<br />
References<br />
1. Liu X et al. Contract<strong>in</strong>g for primary <strong>health</strong> services: Evidence on its effects and a<br />
framework for evaluation. 2004 Available at: HTUhttp://www.who.<strong>in</strong>t/reproductive-<br />
<strong>health</strong>/tcc/meet<strong>in</strong>g_documents/hotchkiss_et_al.pdfUTH<br />
2. Hard<strong>in</strong>g A, Preker AS. Private participation <strong>in</strong> <strong>health</strong> services. Human<br />
development Network, Health, Nutrition and Nutrition Series. Wash<strong>in</strong>gton DC, <strong>The</strong><br />
World Bank, 2003.<br />
3. England R. Contract<strong>in</strong>g and performance management <strong>in</strong> the <strong>health</strong> <strong>sector</strong>: A guide<br />
for low and middle <strong>in</strong>come countries. London, the Health System Resource Centre,<br />
Department for International Development, 2000. Available at:<br />
HTUhttp://www.eldis.org/static/DOC10297.htmUTH<br />
4. Fifty-sixth World Health Assembly. (2003) <strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong><br />
improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance <strong>in</strong> countries. Agenda item 14.13; WHA 56.25,<br />
Document A/56.<br />
9
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
2. SUMMARY ANALYSIS OF COUNTRY EXPEREINCES<br />
2.1 Introduction<br />
Contract<strong>in</strong>g is be<strong>in</strong>g <strong>in</strong>creas<strong>in</strong>gly used by the public <strong>sector</strong> <strong>in</strong> develop<strong>in</strong>g countries<br />
for the purchase over time <strong>of</strong> specified services from the private <strong>sector</strong> [1–5] or <strong>in</strong> some<br />
developed countries through contracts with autonomous public providers [6–9].<br />
Contract<strong>in</strong>g is an important element <strong>of</strong> many countries’ <strong>health</strong> <strong>sector</strong> reform programmes<br />
because it provides governments with a management and regulatory tool that creates<br />
<strong>in</strong>centives for improved performance and <strong>in</strong>creased accountability [1,10]. Recent reviews<br />
have suggested that contract<strong>in</strong>g can potentially <strong>in</strong>fluence access, equity, quality and<br />
efficiency <strong>of</strong> <strong>health</strong> services; promote public <strong>health</strong> goals; and create an environment<br />
conducive to public–private collaboration [11–13]. However, the process is challeng<strong>in</strong>g,<br />
and requires transparent bidd<strong>in</strong>g procedures, well-designed contracts, clear performance<br />
obligations and credible fund<strong>in</strong>g mechanisms. In addition, governments need to be able to<br />
monitor the contracts and must have credibility as a trustworthy partner.<br />
<strong>The</strong>re is limited experience among countries <strong>of</strong> the World Health Organization’s<br />
Eastern Mediterranean Region <strong>in</strong> the area <strong>of</strong> contract<strong>in</strong>g out publicly f<strong>in</strong>anced <strong>health</strong><br />
services to the private <strong>sector</strong>, although several countries are at various stages <strong>of</strong><br />
implement<strong>in</strong>g <strong>health</strong> <strong>sector</strong> reforms. A multi-country study was undertaken <strong>in</strong> 10<br />
countries <strong>of</strong> the Region to document experience with outsourc<strong>in</strong>g <strong>of</strong> publicly f<strong>in</strong>anced<br />
<strong>health</strong> services to private <strong>sector</strong> organizations <strong>in</strong> countries with an active private and/or<br />
nongovernmental organization <strong>sector</strong>. <strong>The</strong> objectives <strong>of</strong> the study were to: 1) assess <strong>in</strong><br />
countries, the capacity <strong>of</strong> the public <strong>sector</strong> organizations, especially the m<strong>in</strong>istries <strong>of</strong><br />
<strong>health</strong>, to outsource publicly f<strong>in</strong>anced <strong>health</strong> services; 2) review a specific <strong>health</strong><br />
<strong>in</strong>tervention that has taken up <strong>contractual</strong> <strong>arrangements</strong> as the pr<strong>in</strong>cipal implementation<br />
strategy; 3) identify the key factors that <strong>in</strong>fluence and drive contract<strong>in</strong>g <strong>in</strong> <strong>health</strong>. This is<br />
the first organized effort <strong>in</strong> the Region to comprehend the situation and to craft a regional<br />
strategy on the <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> system performance.<br />
2.2 Approach and methodology<br />
<strong>The</strong> Eastern Mediterranean Region covers 22 countries from Morocco to Pakistan,<br />
with a total population <strong>of</strong> 500 million, and has the demographic pr<strong>of</strong>ile <strong>of</strong> a develop<strong>in</strong>g<br />
region. Overall it is a low middle-<strong>in</strong>come region with a GNP per capita <strong>of</strong> less than<br />
US$ 1700 [14]. Afghanistan, Djibouti, Somalia, Sudan and Yemen are the five least<br />
developed countries <strong>in</strong> the Region. <strong>The</strong> geopolitical situation <strong>of</strong> the Region is perhaps the<br />
most challeng<strong>in</strong>g. Afghanistan and Sudan are countries <strong>in</strong> a post-conflict state, and their<br />
<strong>health</strong> <strong>sector</strong>s are at various stages <strong>of</strong> recovery and reconstruction. Iraq, Palest<strong>in</strong>e and<br />
Somalia cont<strong>in</strong>ue to be <strong>in</strong> a state <strong>of</strong> conflict as a result <strong>of</strong> <strong>in</strong>vasion, occupation or civil<br />
strife.<br />
10
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
<strong>The</strong> country studies on contract<strong>in</strong>g <strong>of</strong> publicly f<strong>in</strong>anced services were undertaken<br />
between January and September 2004. Ten countries were identified to represent the<br />
Region, based on the size <strong>of</strong> the private <strong>sector</strong>, on anecdotal evidence <strong>of</strong> experience with<br />
<strong>contractual</strong> <strong>arrangements</strong>, and on implementation <strong>of</strong> a programme <strong>in</strong> which <strong>contractual</strong><br />
arrangement with the private <strong>sector</strong> was the pr<strong>in</strong>cipal implementation strategy. <strong>The</strong><br />
countries were Afghanistan, Bahra<strong>in</strong>, Islamic Republic <strong>of</strong> Iran, Egypt, Jordan, Lebanon,<br />
Morocco, Pakistan, Syrian Arab Republic and Tunisia.<br />
Contract<strong>in</strong>g was def<strong>in</strong>ed as a purchas<strong>in</strong>g mechanism used to acquire a specified<br />
service, <strong>of</strong> a def<strong>in</strong>ed quantity and quality, at an agreed-on price, from a specific provider,<br />
for a specified period [15]. Contract<strong>in</strong>g out <strong>in</strong> the <strong>health</strong> <strong>sector</strong> was generally def<strong>in</strong>ed as<br />
the development and implementation <strong>of</strong> a documented agreement by which one party<br />
(purchaser) provides compensation to another party (provider) <strong>in</strong> exchange for a def<strong>in</strong>ed<br />
set <strong>of</strong> <strong>health</strong> services for a def<strong>in</strong>ed target population [16]. Here the terms contract<strong>in</strong>g out<br />
and outsourc<strong>in</strong>g <strong>of</strong> <strong>health</strong> services are used <strong>in</strong>terchangeably.<br />
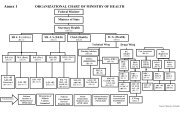
An assessment checklist was developed to facilitate data collection (Annex 1). <strong>The</strong><br />
checklist had two sections: 1) overall capacity <strong>of</strong> the m<strong>in</strong>istries <strong>of</strong> <strong>health</strong> <strong>in</strong> the<br />
contract<strong>in</strong>g <strong>of</strong> <strong>health</strong> services; and 2) review <strong>of</strong> a specific <strong>in</strong>tervention that has taken up<br />
<strong>contractual</strong> <strong>arrangements</strong> as its pr<strong>in</strong>cipal implementation strategy. <strong>The</strong> purpose <strong>of</strong> the<br />
checklist was to serve as a guide to data collection for country researchers and at the<br />
same time to allow for comparison across country studies.<br />
Given the limited experience with contract<strong>in</strong>g <strong>of</strong> <strong>health</strong> services <strong>in</strong> the Region,<br />
<strong>in</strong>clusion criteria were relaxed <strong>in</strong> the selection <strong>of</strong> a specific <strong>in</strong>tervention. Interventions<br />
were selected <strong>in</strong> the follow<strong>in</strong>g order <strong>of</strong> preference: primary <strong>health</strong> care services; hospital<br />
services; non-cl<strong>in</strong>ical services. Those contracts that used some system <strong>of</strong> monitor<strong>in</strong>g or<br />
evaluation <strong>of</strong> performance were given preference. Several country studies covered<br />
experience with contract<strong>in</strong>g <strong>in</strong> two or more service categories.<br />
An electronic network was established for all the country researchers to monitor<br />
progress, share experience and resolve problems as they occurred. Occasional monitor<strong>in</strong>g<br />
<strong>in</strong> the countries was done by the Regional Office staff dur<strong>in</strong>g visits to the countries.<br />
2.3 Results<br />
Summary <strong>of</strong> <strong>in</strong>dividual country studies<br />
An overview <strong>of</strong> the f<strong>in</strong>anc<strong>in</strong>g <strong>of</strong> <strong>health</strong> care allows <strong>in</strong>sight <strong>in</strong>to the context and<br />
nature <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> the respective countries (Table 1). Afghanistan and<br />
Pakistan are low-<strong>in</strong>come countries; Bahra<strong>in</strong> is a high-<strong>in</strong>come country and the rema<strong>in</strong><strong>in</strong>g<br />
countries are middle-<strong>in</strong>come. <strong>The</strong> range <strong>of</strong> total expenditure on <strong>health</strong> as a percentage <strong>of</strong><br />
GDP varies between 3.2% and 11.5%. <strong>The</strong> per capita total <strong>health</strong> expenditure on <strong>health</strong><br />
11
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
for Afghanistan and Pakistan is less than US$ 15 per capita, for all middle-<strong>in</strong>come<br />
countries with the exception <strong>of</strong> Lebanon it ranges between US$ 58–165 and for Bahra<strong>in</strong><br />
and Lebanon goes beyond US$ 500. <strong>The</strong> per capita private <strong>health</strong> expenditure is greater<br />
than the general government expenditure on <strong>health</strong> <strong>in</strong> all countries except Bahra<strong>in</strong>. <strong>The</strong>re<br />
is no consistent association between the level <strong>of</strong> total <strong>health</strong> expenditure, social security<br />
or out-<strong>of</strong>-pocket expenditure on <strong>health</strong> and the nature and extent <strong>of</strong> <strong>contractual</strong><br />
<strong>arrangements</strong> <strong>in</strong> the countries assessed.<br />
Table 1. Health care f<strong>in</strong>anc<strong>in</strong>g <strong>in</strong>dicators for <strong>in</strong>dividual countries, 2002<br />
Country Population<br />
(million)<br />
Total<br />
expenditure<br />
on <strong>health</strong> as<br />
% <strong>of</strong> GDP†<br />
Per capita<br />
general<br />
governmen<br />
t<br />
expenditur<br />
e on <strong>health</strong><br />
at average<br />
exchange<br />
rate (US$)<br />
12<br />
Per capita<br />
private<br />
expenditure<br />
on <strong>health</strong> at<br />
average<br />
exchange<br />
rate (US$)<br />
Social<br />
securi<br />
ty<br />
expen<br />
ditur<br />
e on<br />
healt<br />
h as<br />
% <strong>of</strong><br />
gener<br />
al<br />
gover<br />
nmen<br />
t<br />
expen<br />
ditur<br />
e on<br />
healt<br />
h<br />
Afghanistan 22.9 8.0 6 8 0.0 80.5<br />
Bahra<strong>in</strong> 0.7 4.4 372 145 0.4 69.2<br />
Egypt 70.5 4.9 21 38 22.0 92.0<br />
Islamic<br />
Republic <strong>of</strong><br />
Iran<br />
68.1 6.0 50 54 37.0 96.4<br />
Out<strong>of</strong><br />
-<br />
pock<br />
et<br />
expe<br />
nditu<br />
re on<br />
healt<br />
h as<br />
% <strong>of</strong><br />
priva<br />
te<br />
expe<br />
nditu<br />
re on<br />
healt<br />
h<br />
Jordan 5.3 9.3 76 89 0.7 74.3<br />
Lebanon 3.6 11.5 171 397 43.7 80.0<br />
Morocco 30.1 4.6 18 37 7.6 74.0<br />
Pakistan 149.9 3.2 5 8 42.9 98.3<br />
Syrian Arab<br />
Republic<br />
17.4 5.1 27 31 0.0 100.0<br />
Tunisia 9.7 5.8 63 63 22.7 83.0<br />
Source: WHO National Health Accounts 2002: NHA Website country tables
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
Afghanistan<br />
Afghanistan’s <strong>health</strong> <strong>in</strong>dicators lag significantly beh<strong>in</strong>d other countries <strong>in</strong> the<br />
Region, and most <strong>of</strong> the Afghan population does not have access to basic <strong>health</strong> services.<br />
Dur<strong>in</strong>g 2002, up to 80% <strong>of</strong> the <strong>health</strong> facilities were operated by nongovernmental<br />
organizations, which were directly contracted by the donors with m<strong>in</strong>imal <strong>in</strong>volvement <strong>of</strong><br />
the M<strong>in</strong>istry <strong>of</strong> Public Health [17]. Subsequently, and as a key strategy <strong>of</strong> its national<br />
<strong>health</strong> policy, the M<strong>in</strong>istry focused attention on contract<strong>in</strong>g out the delivery <strong>of</strong> a Basic<br />
Package <strong>of</strong> Health Services (BPHS) to nongovernmental organizations. Although an<br />
alternate service delivery mechanism exists through direct provision <strong>of</strong> BPHS, delivery<br />
through <strong>contractual</strong> <strong>arrangements</strong> predom<strong>in</strong>ates. By January 2005, the population<br />
coverage <strong>of</strong> the BPHS contracted out to nongovernmental organizations had extended to<br />
almost 16.5 million, or over 70% <strong>of</strong> the population; however, the actual extent <strong>of</strong> service<br />
coverage rema<strong>in</strong>s unclear.<br />
<strong>The</strong> BPHS, which forms the core <strong>of</strong> service delivery <strong>in</strong> all primary <strong>health</strong> care<br />
facilities and promotes redistribution <strong>of</strong> <strong>health</strong> services by provid<strong>in</strong>g access especially <strong>in</strong><br />
underserved regions, covers maternal and newborn <strong>health</strong>, child <strong>health</strong> and<br />
immunization, public nutrition, communicable diseases, mental <strong>health</strong>, disability and<br />
supply <strong>of</strong> essential drugs to the four levels <strong>of</strong> <strong>health</strong> facility [18]. <strong>The</strong> estimated cost <strong>of</strong><br />
the BPHS is US$ 4.5 per capita. Programmes such as rout<strong>in</strong>e immunization, nutrition and<br />
malaria, tuberculosis and HIV/AIDS control are not yet fully <strong>in</strong>tegrated to the BPHS, and<br />
they are implemented through vertical approaches that rely heavily on support from<br />
WHO, UNICEF and other UN and <strong>in</strong>ternational agencies.<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public Health has def<strong>in</strong>ed separate geographical regions to utilize<br />
donor funds. <strong>The</strong> World Bank committed US$ 46.3 million, USAID US$ 60 million and<br />
EC Euro 25 million. Out <strong>of</strong> the 34 prov<strong>in</strong>ces, 11 are assigned to the World Bank, 13 to<br />
USAID and 9 to EC funds. <strong>The</strong> Asian Development Bank and TKreditanstalt für<br />
WiederaufbauT (KfW) have also jo<strong>in</strong>ed the partnership, and cover a total <strong>of</strong> 11 districts.<br />
<strong>The</strong> World Bank channels its funds through the contract management unit established<br />
with<strong>in</strong> the M<strong>in</strong>istry <strong>of</strong> Public Health; others do it directly. Nongovernmental<br />
organizations go through a competitive bidd<strong>in</strong>g process, and payment for their services,<br />
<strong>in</strong>clud<strong>in</strong>g the bonus given for extraord<strong>in</strong>ary achievements, is made based on<br />
predeterm<strong>in</strong>ed national <strong>in</strong>dicators. <strong>The</strong> performance is apparently measured through<br />
regular monitor<strong>in</strong>g by the M<strong>in</strong>istry <strong>of</strong> Public Health and by <strong>in</strong>dependent evaluations.<br />
However, a clear monitor<strong>in</strong>g mechanism does not seem to be <strong>in</strong> place. <strong>The</strong>re is anecdotal<br />
evidence that <strong>health</strong> managers <strong>in</strong> the prov<strong>in</strong>ces feel marg<strong>in</strong>alized as they are disconnected<br />
with entire process <strong>of</strong> contract<strong>in</strong>g out <strong>of</strong> <strong>health</strong> services.<br />
<strong>The</strong>re are certa<strong>in</strong> risks <strong>in</strong>herent <strong>in</strong> the contract<strong>in</strong>g out <strong>of</strong> <strong>health</strong> services. Pr<strong>in</strong>cipal<br />
among them <strong>in</strong>clude the possibility <strong>of</strong> emergency withdrawal <strong>of</strong> contracted out services;<br />
the M<strong>in</strong>istry <strong>of</strong> Public Health’s responsibility to provide <strong>health</strong> services directly for the<br />
13
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
30% <strong>of</strong> the uncovered population; <strong>in</strong>creas<strong>in</strong>g demands on central government funds for<br />
manag<strong>in</strong>g hospitals that are under direct M<strong>in</strong>istry control; the reduction <strong>in</strong> external donor<br />
funds for contract<strong>in</strong>g to nongovernmental organizations; and ris<strong>in</strong>g expectations <strong>in</strong> the<br />
population for access, quality and range <strong>of</strong> services. In addition, ongo<strong>in</strong>g debate on the<br />
<strong>role</strong> <strong>of</strong> the nongovernmental organizations and on their non-pr<strong>of</strong>it status calls <strong>in</strong>to<br />
question whether they will cont<strong>in</strong>ue to be the ma<strong>in</strong> provider <strong>of</strong> <strong>health</strong> services <strong>in</strong> the<br />
country.<br />
An evaluation <strong>of</strong> the contract<strong>in</strong>g out <strong>of</strong> <strong>health</strong> services <strong>in</strong> Afghanistan is currently<br />
be<strong>in</strong>g undertaken by a team from Johns Hopk<strong>in</strong>s University with the support <strong>of</strong> the World<br />
Bank. <strong>The</strong> report has yet to be made public.<br />
Bahra<strong>in</strong><br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health has been contract<strong>in</strong>g out various non-cl<strong>in</strong>ical services for a<br />
long time, but there is no experience with contract<strong>in</strong>g out direct <strong>health</strong> care services. At<br />
the other extreme, the M<strong>in</strong>istry is study<strong>in</strong>g the future privatization options and issues for<br />
the new K<strong>in</strong>g Hamad General Hospital, <strong>in</strong> l<strong>in</strong>e with the recent economic policy <strong>of</strong> the<br />
country to promote privatization [19].<br />
<strong>The</strong> selection process for contract<strong>in</strong>g out non-cl<strong>in</strong>ical support services by the<br />
M<strong>in</strong>istry <strong>of</strong> Health was based on bid price as well as the quality <strong>of</strong> technical proposal. A<br />
high level <strong>of</strong> transparency and fairness <strong>of</strong> the selection process was ensured by <strong>in</strong>volv<strong>in</strong>g<br />
an expert third party, the Tender Board. Although the contract design <strong>in</strong>cluded the<br />
standards <strong>of</strong> expected services and contactor performance was strictly monitored, it did<br />
not <strong>in</strong>clude clearly specified performance <strong>in</strong>dicators.<br />
<strong>The</strong> legal framework is sufficiently robust to facilitate contract<strong>in</strong>g between the<br />
public and private <strong>sector</strong>s. <strong>The</strong> public and private <strong>sector</strong>s have the capacity to undertake a<br />
cost and price analysis for support services prior to negotiations. <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health<br />
does not have comprehensive <strong>in</strong>formation system to compute costs <strong>of</strong> various services<br />
dynamically; however, it has adequate cost <strong>in</strong>formation for “make or buy” decisions.<br />
Egypt<br />
Under the Health Sector Reform Programme <strong>in</strong> Egypt, the Family Health Fund was<br />
established by governmental decree as the ma<strong>in</strong> contract<strong>in</strong>g and purchas<strong>in</strong>g agency for<br />
<strong>health</strong> care services. At present, it is function<strong>in</strong>g as a pilot unit <strong>in</strong> the M<strong>in</strong>istry <strong>of</strong> Health<br />
and Population. Its purpose is to: a) separate service f<strong>in</strong>ance from service provision and<br />
ensure competition between service providers to contract with the Fund based on the<br />
quality <strong>of</strong> services <strong>of</strong>fered; b) act as an agent and contractor to purchase <strong>health</strong> services<br />
for families, <strong>in</strong>sured and un<strong>in</strong>sured, through public, private and nongovernmental<br />
organization units; and c) act as a forerunner <strong>of</strong> a national <strong>health</strong> <strong>in</strong>surance fund [20].<br />
14
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
<strong>The</strong> Family Health Fund is <strong>in</strong> its second year <strong>of</strong> operation and has contracted with a<br />
range <strong>of</strong> public and private providers. It is be<strong>in</strong>g piloted <strong>in</strong> five governorates <strong>of</strong> the<br />
country. Based on prelim<strong>in</strong>ary <strong>in</strong>formation, the ma<strong>in</strong> <strong>role</strong> <strong>of</strong> the Fund is to purchase a<br />
package <strong>of</strong> primary <strong>health</strong> care services for registered families <strong>in</strong> a community. In<br />
addition to contract<strong>in</strong>g with private providers and Nongovernmental organizations, the<br />
Fund has <strong>in</strong>itiated contracts with the reformed public <strong>sector</strong> facilities that fall under the<br />
district provider organizations <strong>in</strong> the governorates and provide a def<strong>in</strong>ed package <strong>of</strong><br />
services to the district population. All providers, whether public or private can enter <strong>in</strong>to a<br />
<strong>contractual</strong> arrangement only after hav<strong>in</strong>g received an accreditation certificate from the<br />
M<strong>in</strong>istry <strong>of</strong> Health and Population. Payment mechanisms are still be<strong>in</strong>g piloted on a per<br />
capita as well as fee-for-service basis. A set <strong>of</strong> 30 coverage, utilization and quality<br />
<strong>in</strong>dicators have been identified that will be used for all contract<strong>in</strong>g facilities to allow fair<br />
competition. A formal evaluation <strong>of</strong> the Family Health Fund has yet to be undertaken.<br />
Islamic Republic <strong>of</strong> Iran<br />
<strong>The</strong> Third Socioeconomic Development Plan <strong>of</strong> 1999 encouraged public–private<br />
partnership <strong>in</strong> the country and authorized the M<strong>in</strong>istry <strong>of</strong> Health and Medical Education<br />
to contract out <strong>health</strong> services [21]. Article 192 <strong>of</strong> the Plan focused on privatization <strong>in</strong><br />
general, and on outsourc<strong>in</strong>g <strong>of</strong> <strong>health</strong> care delivery <strong>in</strong> particular. Seven out <strong>of</strong> the 29<br />
medical science universities were selected to pilot outsourc<strong>in</strong>g. Some rushed to contract<br />
out almost all cl<strong>in</strong>ical and non-cl<strong>in</strong>ical services, while others did so on a limited scale.<br />
Despite a comprehensive guidel<strong>in</strong>e for implementation <strong>of</strong> Article 192 to contract out<br />
<strong>health</strong> services, a uniform tool for monitor<strong>in</strong>g and evaluation <strong>of</strong> contracted out services<br />
does not exist and each university has developed its own criteria for assessment <strong>of</strong> private<br />
providers’ performance.<br />
Conflict <strong>of</strong> <strong>in</strong>terest between the purchaser and provider is addressed through<br />
traditional arbitration. Normally, contracts are made for a s<strong>in</strong>gle fiscal year and renewal<br />
and nullify<strong>in</strong>g <strong>of</strong> contracts depends on the outcome <strong>of</strong> assessment <strong>of</strong> providers’<br />
performance, based on <strong>in</strong>dividual checklists developed by the universities. Providers are<br />
selected ma<strong>in</strong>ly through bidd<strong>in</strong>g but sometimes good local reputation and<br />
recommendations by experts and colleagues are used as criteria for provider selection.<br />
Nurs<strong>in</strong>g, laboratory, radiology, operat<strong>in</strong>g room, pharmacy, dentistry, <strong>in</strong>tensive care<br />
and <strong>health</strong> house services are the services most frequently outsourced. <strong>The</strong> universities<br />
purchase a package <strong>of</strong> services from private <strong>in</strong>dividual providers or <strong>health</strong> cooperatives.<br />
A specific budget set aside for this k<strong>in</strong>d <strong>of</strong> purchas<strong>in</strong>g is transferred from the M<strong>in</strong>istry <strong>of</strong><br />
Health and Medical Education to the universities. Capitation is more frequent than global<br />
budgets as a method <strong>of</strong> payment, though both are practised.<br />
<strong>The</strong>re is a perception that contract<strong>in</strong>g out has reduced unit cost, <strong>in</strong>creased access<br />
and improved quality <strong>of</strong> services. <strong>The</strong> stated reasons are restrictions on new employment,<br />
15
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
lower wages and f<strong>in</strong>ancial <strong>in</strong>centives and lower productivity <strong>in</strong> the public <strong>sector</strong>.<br />
Opportunistic behaviour, lack <strong>of</strong> relevant experience among <strong>health</strong> cooperatives, delays<br />
<strong>in</strong> payment, restrictive laws and regulations, and providers’ “play<strong>in</strong>g on both sides <strong>of</strong> the<br />
fence” (public and private <strong>sector</strong>s) are considered the disadvantages <strong>of</strong> outsourc<strong>in</strong>g.<br />
<strong>The</strong>re is no consensus on f<strong>in</strong>ancial risk shar<strong>in</strong>g among contract<strong>in</strong>g parties. <strong>The</strong>re is belief<br />
among some universities that they benefit from a more powerful negotiat<strong>in</strong>g position <strong>in</strong><br />
contract<strong>in</strong>g out <strong>health</strong> services. On balance it is difficult to determ<strong>in</strong>e clearly the impact<br />
<strong>of</strong> contract<strong>in</strong>g out <strong>of</strong> <strong>health</strong> care services <strong>in</strong> the absence <strong>of</strong> a comprehensive evaluation.<br />
Jordan<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health <strong>in</strong> Jordan has been contract<strong>in</strong>g out <strong>health</strong> services to the<br />
private <strong>sector</strong> and other autonomous public <strong>sector</strong> organizations over the past three<br />
decades. Contracts are mostly given by the Health Insurance Directorate <strong>of</strong> the M<strong>in</strong>istry<br />
<strong>of</strong> Health for the provision <strong>of</strong> hospital services. Of the 8 formal contracts for purchase <strong>of</strong><br />
services by the M<strong>in</strong>istry, 5 are with private hospitals and 3 with autonomous public<br />
providers. Of these, 6 are reimbursed accord<strong>in</strong>g to fee-for-service while 2 receive a fixed<br />
payment aga<strong>in</strong>st leas<strong>in</strong>g a specific number <strong>of</strong> hospital beds. Currently, the M<strong>in</strong>istry <strong>of</strong><br />
Health with the support <strong>of</strong> Partnership for Health Reform Plus is implement<strong>in</strong>g a <strong>health</strong><br />
<strong>in</strong>surance pilot project to enhance the capacity <strong>of</strong> the M<strong>in</strong>istry <strong>in</strong> contract design,<br />
monitor<strong>in</strong>g and enforcement.<br />
<strong>The</strong>re is some evidence that contract<strong>in</strong>g has contributed to improv<strong>in</strong>g access and<br />
promot<strong>in</strong>g equity through extension <strong>of</strong> subsidized M<strong>in</strong>istry <strong>of</strong> Health activities to the<br />
poor and vulnerable. In terms <strong>of</strong> efficiency, the cost per admission <strong>in</strong> some autonomous<br />
hospitals reduced to less than US$ 424 as compared to over US$ 706 <strong>in</strong> private hospitals<br />
without contracts. <strong>The</strong>re was no evidence, however, that it contributed to improv<strong>in</strong>g the<br />
quality <strong>of</strong> services.<br />
Lebanon<br />
Lebanon has a large private <strong>health</strong> <strong>sector</strong> and uses <strong>contractual</strong> <strong>arrangements</strong><br />
extensively to provide <strong>health</strong> care and other services to its citizens. Over 80% <strong>of</strong><br />
Lebanese receive <strong>health</strong> care based on one form or another <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong>.<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public Health uses contract<strong>in</strong>g as one <strong>of</strong> the ma<strong>in</strong> tools at its disposal to<br />
perform its functions. This <strong>in</strong>cludes contract<strong>in</strong>g with primary care centres and hospitals to<br />
provide care for the un<strong>in</strong>sured and with local nongovernmental organizations to support<br />
social welfare.<br />
<strong>The</strong>re are many limitations to the current <strong>contractual</strong> <strong>arrangements</strong>. Some <strong>of</strong> these<br />
<strong>in</strong>clude fragmentation <strong>of</strong> contract<strong>in</strong>g mechanisms, lack <strong>of</strong> public capacity for monitor<strong>in</strong>g<br />
<strong>of</strong> performance and outcomes, the limited leverage <strong>of</strong> the public <strong>sector</strong> as compared with<br />
the private <strong>sector</strong>, and the <strong>in</strong>ability <strong>of</strong> current <strong>arrangements</strong> to conta<strong>in</strong> escalat<strong>in</strong>g <strong>health</strong><br />
16
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
care costs. Many perceive current <strong>arrangements</strong> as provid<strong>in</strong>g public–private “cash<br />
transfers” which do not serve the government or the Lebanese citizen <strong>in</strong> the long term.<br />
Consider<strong>in</strong>g that recent large-scale <strong>health</strong> <strong>sector</strong> reform projects have not been<br />
evidently successful, contract<strong>in</strong>g can be used an entry po<strong>in</strong>t to gradual reform. Several<br />
recommendations for improv<strong>in</strong>g performance <strong>of</strong> current <strong>arrangements</strong> can be made, that<br />
<strong>in</strong>clude creation <strong>of</strong> a central contract<strong>in</strong>g body, l<strong>in</strong>k<strong>in</strong>g <strong>in</strong>patient and outpatient care, and<br />
unify<strong>in</strong>g tariffs across f<strong>in</strong>anc<strong>in</strong>g agencies.<br />
Morocco<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health <strong>of</strong> Morocco recognizes the competencies and <strong>in</strong>novative<br />
management procedures <strong>of</strong> private providers and encourages contract<strong>in</strong>g with them.<br />
Morocco follows <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> a broad sense <strong>of</strong> the term, which <strong>in</strong>cludes<br />
purchas<strong>in</strong>g, delegation <strong>of</strong> services to lower levels, and cooperation among partners.<br />
Purchas<strong>in</strong>g has <strong>in</strong>volved the traditional contract<strong>in</strong>g <strong>of</strong> a private provider on a regular<br />
salary to work with<strong>in</strong> a public <strong>health</strong> <strong>in</strong>stitution and provide <strong>health</strong> services that are not<br />
well covered. Such <strong>arrangements</strong> have been on the decl<strong>in</strong>e with the expansion <strong>of</strong> public<br />
<strong>health</strong> services.<br />
More recent experience <strong>in</strong> Morocco relates to its policy <strong>of</strong> hospital autonomy and<br />
decentralization <strong>of</strong> district services and enter<strong>in</strong>g <strong>in</strong>to a <strong>contractual</strong> arrangement with<br />
them. <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health and the M<strong>in</strong>istry <strong>of</strong> F<strong>in</strong>ance and privatization concluded<br />
what have been called workplan contracts with two university hospitals to meet their<br />
statutory responsibilities, namely care, tra<strong>in</strong><strong>in</strong>g and education and research. <strong>The</strong> idea<br />
underly<strong>in</strong>g this tw<strong>in</strong> <strong>in</strong>tervention <strong>of</strong> decentralization and contract<strong>in</strong>g is that these<br />
<strong>in</strong>stitutions will improve management, optimize use <strong>of</strong> resources, be more accountable<br />
and improve overall performance. <strong>The</strong> terms and conditions <strong>of</strong> the contract <strong>in</strong>clude a<br />
global budget and set <strong>of</strong> agreed-upon performance monitor<strong>in</strong>g <strong>in</strong>dicators. A similar<br />
arrangement called programme contracts has been made with the decentralized facilities<br />
<strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health that are responsible for provid<strong>in</strong>g district <strong>health</strong> services.<br />
Another form <strong>contractual</strong> arrangement based on cooperation exists between the<br />
public <strong>sector</strong> and the nongovernmental organizations cover<strong>in</strong>g such activities as contact<br />
trac<strong>in</strong>g for <strong>in</strong>fectious diseases, family plann<strong>in</strong>g and diagnostic and treatment services.<br />
<strong>The</strong> public contribution to these organizations comes not only through formal <strong>contractual</strong><br />
payments but also through annual subsidies, provision <strong>of</strong> medic<strong>in</strong>es and supplies, and<br />
shar<strong>in</strong>g <strong>of</strong> <strong>in</strong>frastructure and human resources. Such agreements usually do not anticipate<br />
the means and tools necessary to control, monitor and follow up the <strong>in</strong>put <strong>of</strong><br />
nongovernmental organizations.<br />
17
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
Pakistan<br />
<strong>The</strong> contract<strong>in</strong>g <strong>arrangements</strong> between the public purchasers and private providers<br />
vary with the level <strong>of</strong> hierarchy, type <strong>of</strong> contract and set <strong>of</strong> services to be provided. <strong>The</strong><br />
purchasers are ma<strong>in</strong>ly the Federal M<strong>in</strong>istry <strong>of</strong> Health, prov<strong>in</strong>cial departments <strong>of</strong> <strong>health</strong><br />
and social welfare, and district governments. <strong>The</strong> private providers are ma<strong>in</strong>ly the<br />
<strong>in</strong>ternational and national nongovernmental organizations, <strong>in</strong>stitutions and private firms.<br />
Contract types <strong>in</strong>clude contract<strong>in</strong>g out, cost-shar<strong>in</strong>g agreements, grants and loans. <strong>The</strong> set<br />
<strong>of</strong> activities covered <strong>in</strong> <strong>contractual</strong> <strong>arrangements</strong> comprise primary <strong>health</strong> care services,<br />
research and development services, and technical and management services.<br />
<strong>The</strong> public <strong>sector</strong> rationale for <strong>contractual</strong> <strong>arrangements</strong> is to partner with the<br />
private <strong>sector</strong> to target priority <strong>health</strong> problems, expand coverage <strong>in</strong> less accessible areas,<br />
meet ris<strong>in</strong>g consumer expectations and test public–private <strong>in</strong>novations. <strong>The</strong> private <strong>sector</strong><br />
<strong>in</strong>terests <strong>in</strong>clude enhanced size and scope <strong>of</strong> activities, recognition and f<strong>in</strong>ancial support,<br />
and humanitarian concerns.<br />
<strong>The</strong>re exists serious political commitment <strong>in</strong> favour <strong>of</strong> public–private partnership.<br />
Despite a cautious approach, support for contract<strong>in</strong>g is <strong>in</strong>creas<strong>in</strong>g, along with the number<br />
<strong>of</strong> projects with <strong>contractual</strong> <strong>arrangements</strong>. <strong>The</strong> early success <strong>of</strong> the flagship project, the<br />
contract<strong>in</strong>g out <strong>of</strong> primary <strong>health</strong> care services <strong>in</strong> district Rahim Yar Khan, has led to its<br />
possibly premature replication <strong>in</strong> several districts <strong>of</strong> the Punjab prov<strong>in</strong>ce. A recent World<br />
Bank-sponsored evaluation showed mixed results. On one hand, the utilization and<br />
physical condition <strong>of</strong> primary <strong>health</strong> care centres have improved, patient satisfaction has<br />
<strong>in</strong>creased, and out-<strong>of</strong>-pocket expenditure has decreased. On the other hand, quality <strong>of</strong><br />
care, drug availability and accessibility by remote communities have rema<strong>in</strong>ed poor. In<br />
addition, contract<strong>in</strong>g out has had little effect on the coverage <strong>of</strong> preventive <strong>health</strong> services<br />
[22].<br />
<strong>The</strong> <strong>in</strong>stitutional <strong>arrangements</strong> for manag<strong>in</strong>g the <strong>contractual</strong> partnerships are<br />
<strong>in</strong>adequately developed. Although private <strong>sector</strong> partners have expressed overall<br />
satisfaction with the support received from their public counterparts dur<strong>in</strong>g plann<strong>in</strong>g and<br />
implementation <strong>of</strong> project activities, delays <strong>in</strong> payment have also been reported due to the<br />
complexity <strong>of</strong> government f<strong>in</strong>ancial procedures.<br />
Many national programmes have developed capacity <strong>in</strong> prepar<strong>in</strong>g bids, evaluat<strong>in</strong>g<br />
technical and f<strong>in</strong>ancial proposals, negotiat<strong>in</strong>g terms and award<strong>in</strong>g contracts. <strong>The</strong>re is<br />
wide variation <strong>in</strong> the technical, managerial and f<strong>in</strong>ancial capacity <strong>of</strong> private providers,<br />
which is <strong>of</strong>ten addressed through short-term expert <strong>in</strong>puts. <strong>The</strong> majority <strong>of</strong> private<br />
providers rely on up-front project fund<strong>in</strong>g for <strong>in</strong>itiat<strong>in</strong>g activities, which makes the longterm<br />
susta<strong>in</strong>ability <strong>of</strong> such activities less certa<strong>in</strong>.<br />
18
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
<strong>The</strong> most common payment method is block payment made aga<strong>in</strong>st an agreed set <strong>of</strong><br />
activities and outputs. However, there are examples <strong>of</strong> payments to private <strong>sector</strong><br />
providers on the basis <strong>of</strong> fee-for-service, and <strong>in</strong>demnification and prepayment. Both<br />
public <strong>sector</strong> managers and most private <strong>sector</strong> organizations have limited ability to<br />
undertake cost and pric<strong>in</strong>g analysis.<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health does not have the capacity to monitor and evaluate ongo<strong>in</strong>g<br />
projects efficiently, even if monitor<strong>in</strong>g <strong>in</strong>dicators are identified. <strong>The</strong>re is thus no regular<br />
arrangement for collect<strong>in</strong>g data on project outputs or outcomes. Independent reviews are<br />
sometimes undertaken through donor support. <strong>The</strong> M<strong>in</strong>istry does not ma<strong>in</strong>ta<strong>in</strong> a database<br />
<strong>of</strong> the private <strong>sector</strong> partners accord<strong>in</strong>g to their areas <strong>of</strong> expertise or work experience.<br />
Syrian Arab Republic<br />
Although the number <strong>of</strong> government contracts with the private <strong>sector</strong> almost<br />
doubled from 260 to 492 dur<strong>in</strong>g the period 2001–2003, most contract<strong>in</strong>g <strong>in</strong> the Syrian<br />
Arab Republic is done for non-cl<strong>in</strong>ical services. <strong>The</strong> areas covered <strong>in</strong>clude ma<strong>in</strong>tenance<br />
<strong>of</strong> hospitals and equipment and cater<strong>in</strong>g, clean<strong>in</strong>g and construction services. <strong>The</strong> M<strong>in</strong>istry<br />
<strong>of</strong> Health cont<strong>in</strong>ues to promote a policy <strong>of</strong> direct provision <strong>of</strong> <strong>health</strong> services through the<br />
establishment <strong>of</strong> new hospitals and <strong>health</strong> centres <strong>in</strong>stead <strong>of</strong> contract<strong>in</strong>g out <strong>health</strong><br />
services to the private <strong>sector</strong>. <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health owns 80% <strong>of</strong> the <strong>health</strong> <strong>in</strong>stitutions<br />
<strong>in</strong> the country and is plann<strong>in</strong>g to establish an additional 74 new hospitals and 350 <strong>health</strong><br />
centres dur<strong>in</strong>g 2006–2010.<br />
<strong>The</strong> overall political and bureaucratic environment is not conducive to contract<strong>in</strong>g<br />
out <strong>health</strong> services at present, nonetheless there is grow<strong>in</strong>g keenness among the private<br />
<strong>sector</strong> to enter <strong>in</strong>to <strong>contractual</strong> <strong>arrangements</strong>, as such <strong>arrangements</strong> would <strong>of</strong>fer a reliable<br />
source <strong>of</strong> revenue, raise the volume <strong>of</strong> under-utilized services and add to the credibility <strong>of</strong><br />
services.<br />
<strong>The</strong> lack <strong>of</strong> experience <strong>in</strong> contract<strong>in</strong>g out <strong>of</strong> cl<strong>in</strong>ical services <strong>in</strong> Syrian Arab<br />
Republic may be attributed to several factors, important among them be<strong>in</strong>g: historical<br />
policy <strong>of</strong> direct provision <strong>in</strong> most social <strong>sector</strong>s; lack <strong>of</strong> knowledge and trust <strong>of</strong> the<br />
advantages that each has to <strong>of</strong>fer; and lack <strong>of</strong> experience <strong>in</strong> the public and private <strong>sector</strong>s<br />
<strong>in</strong> negotiation <strong>of</strong> contracts, their preparation, management, monitor<strong>in</strong>g and evaluation.<br />
Tunisia<br />
<strong>The</strong> Tunisian <strong>health</strong> system has made use <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> s<strong>in</strong>ce 1970,<br />
when the Social Security Fund agreed to pay a lump sum amount to the national treasury<br />
for <strong>health</strong> care provided to their affiliate members and their dependents. <strong>The</strong> process <strong>of</strong><br />
contract<strong>in</strong>g has greatly developed s<strong>in</strong>ce then. In 1987, contract<strong>in</strong>g with the private <strong>sector</strong><br />
<strong>in</strong> Tunisia received a boost when it was realized that the social security fund had to pay<br />
19
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
large sums <strong>of</strong> money to almost 60% <strong>of</strong> patients requir<strong>in</strong>g cardiac surgery <strong>in</strong> order to send<br />
them abroad.<br />
Currently, the relationships between the <strong>health</strong> <strong>in</strong>surance organization (Social<br />
Security Fund) and <strong>health</strong> care providers (both public and private) are managed and<br />
regulated through contract<strong>in</strong>g, which also helps achieve consensus on the <strong>of</strong>ten<br />
conflict<strong>in</strong>g <strong>in</strong>terests <strong>of</strong> the fund and the providers. Several specialized services were not<br />
provided for <strong>in</strong> the <strong>in</strong>itial agreements made between the Social Security Fund and the<br />
M<strong>in</strong>istry <strong>of</strong> Public Health. Most <strong>of</strong> these <strong>health</strong> care services are the subject <strong>of</strong><br />
agreements and memoranda <strong>of</strong> understand<strong>in</strong>g with the M<strong>in</strong>istry, to which some private<br />
specialized care <strong>in</strong>stitutions and the military hospital have been <strong>in</strong>cluded. <strong>The</strong>re is no act<br />
or decree allow<strong>in</strong>g the socially <strong>in</strong>sured to receive <strong>health</strong> care <strong>in</strong> private <strong>health</strong> facilities.<br />
<strong>The</strong> agreements have proved useful as they enable the private facilities to be brought <strong>in</strong>to<br />
the process <strong>of</strong> contract<strong>in</strong>g <strong>of</strong> <strong>health</strong> services.<br />
<strong>The</strong>re are two types <strong>of</strong> <strong>health</strong> coverage schemes operational <strong>in</strong> Tunisia, <strong>health</strong> cards<br />
and reimbursement schemes. Irrespective <strong>of</strong> the scheme, the affiliate members are<br />
entitled to all <strong>health</strong> care services provided <strong>in</strong> the terms <strong>of</strong> agreement. <strong>The</strong> wide range <strong>of</strong><br />
services <strong>in</strong>clude highly sophisticated techniques such as lithotripsy, transplants (bone<br />
marrow, renal and heart), other cardiovascular <strong>in</strong>terventions, thermal treatments,<br />
haemodialysis, and all forms <strong>of</strong> scann<strong>in</strong>g procedures.<br />
In order to participate <strong>in</strong> the <strong>contractual</strong> arrangement, private <strong>in</strong>stitutions are<br />
obliged to accept the follow<strong>in</strong>g conditions: a) reimbursement is made on the basis <strong>of</strong> a<br />
flat rate determ<strong>in</strong>ed at the level <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Public Health; b) private facilities<br />
cannot <strong>in</strong>crease the agreed rates or charge co-payment; c) for cardiovascular<br />
<strong>in</strong>terventions, a justification for the procedure is required from the private <strong>in</strong>stitutions;<br />
and d) private facilities are subject to medical <strong>in</strong>spection, provided for <strong>in</strong> the agreements,<br />
which is also a requirement for public facilities.<br />
Overall capacity for contract<strong>in</strong>g <strong>health</strong> services<br />
Contract<strong>in</strong>g out <strong>of</strong> <strong>health</strong> services occurs more frequently than presumed. <strong>The</strong>re is a<br />
wide range <strong>of</strong> services contracted out that varies from non-cl<strong>in</strong>ical services to primary<br />
care and hospital services. Table 2 shows a comparison <strong>of</strong> the overall capacity <strong>of</strong> the<br />
public <strong>sector</strong> <strong>in</strong> general and m<strong>in</strong>istries <strong>of</strong> <strong>health</strong> <strong>in</strong> particular to contract out <strong>health</strong><br />
services. <strong>The</strong> rationales for contract<strong>in</strong>g out by m<strong>in</strong>istries <strong>of</strong> <strong>health</strong> are to: improve<br />
efficiency; enhance access and coverage; improve quality <strong>of</strong> care; address shortage <strong>of</strong><br />
public hospitals; and provide services targeted at culturally sensitive problems such as<br />
HIV/AIDS through build<strong>in</strong>g partnership between public and private <strong>sector</strong>s.<br />
Most countries, with the exception <strong>of</strong> the Syrian Arab Republic, have a policy that<br />
promotes enhanced <strong>in</strong>volvement <strong>of</strong> private <strong>sector</strong>. Afghanistan has the most explicit<br />
20
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
policy on contract<strong>in</strong>g out <strong>of</strong> primary <strong>health</strong> services. Bureaucratic support for contract<strong>in</strong>g<br />
varies depend<strong>in</strong>g on previous experience both with contract<strong>in</strong>g and with work<strong>in</strong>g with the<br />
private <strong>sector</strong>. Countries such as Jordan, Lebanon, Morocco and Tunisia have a long<br />
experience with contract<strong>in</strong>g, while the experience <strong>in</strong> Afghanistan, Egypt and Pakistan is<br />
relatively recent. <strong>The</strong> legal framework and the necessary rules and procedures for<br />
tender<strong>in</strong>g for goods exist <strong>in</strong> all countries; however, <strong>in</strong> several countries the legal<br />
framework requires updat<strong>in</strong>g for outsourc<strong>in</strong>g <strong>of</strong> <strong>health</strong> services.<br />
Most m<strong>in</strong>istries have limited capacity for cost and price analysis. Estimation <strong>of</strong> the<br />
transaction cost <strong>of</strong> outsourc<strong>in</strong>g <strong>health</strong> services has not been undertaken <strong>in</strong> most countries<br />
except <strong>in</strong> Pakistan, where the adm<strong>in</strong>istrative and transaction cost for the flagship project<br />
<strong>in</strong> Rahim Yar Khan district was estimated at 10% <strong>of</strong> the total project cost.<br />
21
Table 2. Assessment <strong>of</strong> overall country capacity for contract<strong>in</strong>g <strong>health</strong> services<br />
Country Rationale for MOH<br />
to enter <strong>in</strong>to <strong>health</strong><br />
service contracts<br />
Afghanistan Disrupted public<br />
<strong>sector</strong> <strong>health</strong><br />
services due to years<br />
<strong>of</strong> conflict<br />
80% <strong>of</strong> <strong>health</strong><br />
facilities operated by<br />
NGOs dur<strong>in</strong>g and <strong>in</strong><br />
the early postconflict<br />
period<br />
Bahra<strong>in</strong> Improved efficiency<br />
Economies <strong>of</strong> scale<br />
<strong>in</strong> private <strong>sector</strong><br />
Government policy<br />
to <strong>in</strong>volve private<br />
<strong>sector</strong><br />
Egypt Increase coverage <strong>of</strong><br />
services<br />
Utilize advanced<br />
technology available<br />
with private <strong>sector</strong><br />
Improve quality <strong>of</strong><br />
Interest <strong>of</strong> the<br />
NGOs/ private<br />
<strong>sector</strong> <strong>in</strong><br />
contract<strong>in</strong>g<br />
NGOs would<br />
cont<strong>in</strong>ue to be<br />
actively engaged<br />
<strong>in</strong> provision <strong>of</strong><br />
care<br />
NGOs would<br />
receive US$ 4.5<br />
per capita as cost<br />
<strong>of</strong> BPHS<br />
Increase scale <strong>of</strong><br />
work<br />
Assurance <strong>of</strong><br />
regular source <strong>of</strong><br />
revenue<br />
Assurance <strong>of</strong><br />
regular source <strong>of</strong><br />
revenue<br />
Guaranteed<br />
registration <strong>of</strong><br />
families<br />
Political<br />
environment,<br />
bureaucratic<br />
support, legal<br />
framework<br />
Adequate<br />
political,<br />
bureaucratic and<br />
legal framework<br />
did not exist<br />
External donor<br />
<strong>in</strong>fluence to push<br />
for contract<strong>in</strong>g,<br />
e.g. World Bank,<br />
USAID, EC<br />
Government<br />
policy <strong>of</strong><br />
develop<strong>in</strong>g the<br />
private <strong>sector</strong><br />
Supportive<br />
bureaucratic<br />
process<br />
Strong legal<br />
framework<br />
Contract<strong>in</strong>g is part<br />
<strong>of</strong> reform<br />
programme<br />
Legal framework<br />
for contract<strong>in</strong>g<br />
present<br />
Capabilities <strong>of</strong><br />
the purchaser<br />
(strengths and<br />
weaknesses)<br />
MOPH lacked<br />
experience with<br />
purchas<strong>in</strong>g <strong>of</strong><br />
<strong>health</strong> services<br />
General contract<br />
management unit<br />
established <strong>in</strong><br />
MOPH for<br />
manag<strong>in</strong>g World<br />
Bank funds<br />
Other donors<br />
contracted out<br />
directly<br />
Clearly def<strong>in</strong>ed<br />
rules and<br />
procedures<br />
Dedicated section<br />
<strong>in</strong> F<strong>in</strong>ance<br />
M<strong>in</strong>istry<br />
Six technical units<br />
established <strong>in</strong><br />
Family Health<br />
Fund which<br />
support<br />
contract<strong>in</strong>g<br />
Capabilities <strong>of</strong><br />
providers<br />
(strengths and<br />
weaknesses)<br />
NGOs had<br />
previous<br />
experience <strong>of</strong><br />
receiv<strong>in</strong>g contracts<br />
from donors<br />
Lack <strong>of</strong><br />
<strong>in</strong>formation on the<br />
quantity, quality<br />
and distribution <strong>of</strong><br />
workforce among<br />
NGOs<br />
Limited capacity<br />
<strong>of</strong> local companies<br />
for most contracts<br />
Opportunities for<br />
<strong>in</strong>ternational/<br />
regional<br />
companies<br />
Private <strong>sector</strong><br />
provides most <strong>of</strong><br />
ambulatory care<br />
Majority <strong>of</strong><br />
facilities not<br />
accredited by<br />
Risks <strong>of</strong> the process Mechanisms for<br />
monitor<strong>in</strong>g<br />
performance<br />
Reduction <strong>in</strong> external<br />
donor funds for<br />
contract<strong>in</strong>g NGOs<br />
Ris<strong>in</strong>g expectations<br />
<strong>in</strong> population for<br />
access, quality and<br />
range <strong>of</strong> services<br />
NGOs non-pr<strong>of</strong>it <strong>in</strong><br />
pr<strong>in</strong>ciple but not<br />
necessarily <strong>in</strong><br />
practice<br />
M<strong>in</strong>istry <strong>of</strong> Health<br />
has to have a backup<br />
option <strong>in</strong> case <strong>of</strong><br />
failure <strong>of</strong> contractor<br />
to provide services<br />
Fee-for-service and<br />
capitation are be<strong>in</strong>g<br />
tried as two different<br />
methods<br />
Accreditation <strong>of</strong><br />
private facilities may<br />
Performance<br />
monitored by the<br />
MOPH based on<br />
agreed <strong>in</strong>dicators<br />
In practice<br />
monitor<strong>in</strong>g<br />
mechanisms do not<br />
exist, especially<br />
outside the capital<br />
city<br />
MOH approves<br />
hir<strong>in</strong>g <strong>of</strong> personnel<br />
by the contractor<br />
Users report<br />
performance<br />
Previous record<br />
taken <strong>in</strong>to account<br />
11 weighted<br />
performance<br />
<strong>in</strong>dicators<br />
(encompass<strong>in</strong>g<br />
coverage, quality<br />
and utilization)
Islamic<br />
Republic <strong>of</strong><br />
Iran<br />
care (<strong>in</strong>crease<br />
clientele)<br />
Decentralization <strong>of</strong><br />
services<br />
MOH policy to<br />
provide services for<br />
segment <strong>of</strong> rural and<br />
deprived population<br />
contract<strong>in</strong>g out<br />
Jordan Optimize capital<br />
<strong>in</strong>vestments by<br />
private <strong>sector</strong><br />
Improve<br />
accessibility and<br />
efficiency<br />
Decrease wait<strong>in</strong>g<br />
lists at government<br />
hospitals<br />
Lebanon More elaborate<br />
<strong>in</strong>frastructure <strong>of</strong><br />
hospitals <strong>in</strong> the<br />
private <strong>sector</strong><br />
Avoid duplication <strong>of</strong><br />
services already<br />
available <strong>in</strong> private<br />
<strong>sector</strong><br />
Morocco Decentralization <strong>of</strong><br />
services<br />
Improve access to<br />
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
Access to<br />
government<br />
resources for<br />
family<br />
physicians<br />
Utilize spare<br />
capacity<br />
Assurance <strong>of</strong><br />
regular source <strong>of</strong><br />
revenue<br />
Increase<br />
credibility <strong>in</strong><br />
population<br />
through<br />
affiliation with<br />
MOH<br />
Access to major<br />
<strong>in</strong>surers <strong>of</strong><br />
population<br />
Utilize capacity<br />
<strong>in</strong> private <strong>sector</strong><br />
Enhanced<br />
recognition <strong>of</strong><br />
private <strong>sector</strong><br />
Opportunity for<br />
Political and legal<br />
support through<br />
3rd Socioeconomic<br />
Development Plan<br />
passed <strong>in</strong> 1999<br />
Political<br />
environment and<br />
legal framework is<br />
present<br />
Health reforms to<br />
improve equity<br />
and access<br />
Bureaucratic<br />
framework is not<br />
flexible<br />
Legal framework<br />
is adequate<br />
Political will is<br />
lack<strong>in</strong>g for<br />
improv<strong>in</strong>g<br />
contract<strong>in</strong>g<br />
process<br />
No clear policy on<br />
contract<strong>in</strong>g<br />
cl<strong>in</strong>ical services<br />
process MOH be difficult due to<br />
improvements<br />
required<br />
Improve access,<br />
quality and<br />
efficiency <strong>of</strong> PHC<br />
services, especially<br />
to the deprived and<br />
vulnerable<br />
population<br />
Experience <strong>of</strong><br />
contract<strong>in</strong>g for the<br />
past 3 decades<br />
Cost and price<br />
analysis for some<br />
projects<br />
MOH has<br />
experience <strong>in</strong><br />
contract<strong>in</strong>g<br />
Contract<strong>in</strong>g is<br />
highly fragmented<br />
Does not limit cost<br />
<strong>of</strong> <strong>health</strong> care<br />
MOH has<br />
experience <strong>in</strong><br />
contract<strong>in</strong>g<br />
Loose partnership<br />
23<br />
Private <strong>sector</strong> <strong>in</strong><br />
<strong>health</strong> care<br />
markets is not fully<br />
developed and is<br />
ma<strong>in</strong>ly <strong>in</strong>volved<br />
with hospitals <strong>in</strong><br />
cities<br />
Lack <strong>of</strong> experience<br />
with PHC services<br />
Advanced<br />
<strong>in</strong>formation<br />
systems<br />
Experience <strong>in</strong><br />
negotiat<strong>in</strong>g<br />
contracts<br />
Lack <strong>of</strong> skilled and<br />
pr<strong>of</strong>essional<br />
managers<br />
Major provider <strong>of</strong><br />
services<br />
Oversupply <strong>of</strong><br />
specialists and<br />
services<br />
Advanced<br />
diagnostic and<br />
therapeutic<br />
services<br />
Health managers and<br />
their private <strong>sector</strong><br />
counterparts lack<br />
necessary skills for<br />
contract<strong>in</strong>g<br />
Private <strong>sector</strong><br />
demonstrates<br />
opportunistic<br />
behaviour<br />
Delay <strong>in</strong> payments<br />
from the MOH<br />
Concerns <strong>of</strong> quality<br />
<strong>of</strong> care <strong>in</strong> private<br />
<strong>sector</strong><br />
Number <strong>of</strong> providers<br />
is above requirement<br />
Contracts are not<br />
performance based<br />
Difficulty <strong>in</strong> ensur<strong>in</strong>g<br />
quality <strong>of</strong> services<br />
Used at pilot centres<br />
Performance based<br />
service contract<strong>in</strong>g<br />
with measurable<br />
standards and<br />
negative <strong>in</strong>centives<br />
for non-performance<br />
Weak monitor<strong>in</strong>g<br />
mechanisms are a<br />
challenge<br />
Political<br />
environment affects<br />
monitor<strong>in</strong>g <strong>of</strong><br />
contracts<br />
Capacity to monitor<br />
contracts is poor at<br />
MOH<br />
Monitor<strong>in</strong>g<br />
<strong>in</strong>dicators not welldef<strong>in</strong>ed<br />
Adequate
services<br />
Overcome budget<br />
constra<strong>in</strong>ts for<br />
capital projects<br />
Pakistan Enhance<br />
implementation <strong>of</strong><br />
planned activities<br />
Improve access to<br />
services<br />
Expand service<br />
provision for<br />
culturally sensitive<br />
issues, e.g.<br />
HIV/AIDS<br />
Syrian Arab<br />
Republic<br />
Public provision <strong>of</strong><br />
services, cl<strong>in</strong>ical<br />
services not<br />
contracted out<br />
Tunisia Reduce cost <strong>of</strong><br />
foreign treatment by<br />
contract<strong>in</strong>g with<br />
national providers<br />
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
partner<strong>in</strong>g with<br />
public <strong>sector</strong><br />
Enhanced<br />
recognition <strong>of</strong><br />
NGOs by<br />
population<br />
Expansion <strong>of</strong><br />
programme<br />
activities<br />
Access to<br />
government<br />
funds<br />
Most contracts<br />
between MASS<br />
or MOH and<br />
private facilities<br />
are only adherent<br />
to the<br />
agreements<br />
Political<br />
commitment for<br />
public–private<br />
partnerships exists<br />
Bureaucratic<br />
support is<br />
ambivalent<br />
Legal framework<br />
is be<strong>in</strong>g adapted<br />
No bureaucratic<br />
and political<br />
support for<br />
contract<strong>in</strong>g<br />
cl<strong>in</strong>ical services<br />
Only non-cl<strong>in</strong>ical<br />
contracts<br />
Political and legal<br />
framework<br />
supportive<br />
MOH: M<strong>in</strong>istry <strong>of</strong> Health; MASS: M<strong>in</strong>istry <strong>of</strong> Social Affairs and Solidarity<br />
<strong>arrangements</strong> with<br />
public <strong>sector</strong><br />
No dedicated<br />
contract<strong>in</strong>g unit <strong>in</strong><br />
MOH<br />
Limited<br />
experience <strong>of</strong><br />
contract<strong>in</strong>g<br />
Experience limited<br />
to specific national<br />
programmes<br />
Major provider <strong>of</strong><br />
care<br />
Expand<strong>in</strong>g service<br />
<strong>in</strong>frastructure<br />
Social Security<br />
Fund has long<br />
experience with<br />
contract<strong>in</strong>g<br />
Contracts not<br />
directly given to<br />
private facilities<br />
24<br />
Limited experience<br />
<strong>in</strong> contract<strong>in</strong>g <strong>of</strong><br />
cl<strong>in</strong>ical services<br />
Different providers<br />
(NGOs, private<br />
practitioners)<br />
Technical,<br />
f<strong>in</strong>ancial capacities<br />
vary widely<br />
Advanced<br />
diagnostic and<br />
therapeutic<br />
services<br />
Advanced<br />
diagnostic and<br />
therapeutic<br />
services<br />
Payments are<br />
normally block<br />
payments concerned<br />
with only quantity<br />
Delay <strong>in</strong> release <strong>of</strong><br />
payments adversely<br />
affects contracts<br />
Difficulty <strong>in</strong> ensur<strong>in</strong>g<br />
quality <strong>of</strong> services<br />
Reimbursements<br />
made on flat rate<br />
determ<strong>in</strong>ed by MOH<br />
and no co-payment<br />
can be charged<br />
<strong>in</strong>formation system<br />
not <strong>in</strong> place<br />
Information system<br />
has limited capacity<br />
to assist <strong>in</strong><br />
monitor<strong>in</strong>g contracts<br />
Most programmes<br />
use separate<br />
report<strong>in</strong>g systems<br />
not used to monitor<br />
quality <strong>of</strong> services<br />
Information system<br />
has limited capacity<br />
to assist <strong>in</strong><br />
monitor<strong>in</strong>g contracts<br />
Medical <strong>in</strong>spection<br />
for assess<strong>in</strong>g<br />
condition <strong>of</strong><br />
hospitals and<br />
treatment facilities
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
<strong>The</strong> capacity <strong>of</strong> private <strong>sector</strong> providers also varies among countries <strong>of</strong> the Region.<br />
Nongovernmental organizations are more actively <strong>in</strong>volved <strong>in</strong> the delivery <strong>of</strong> primary<br />
<strong>health</strong> services <strong>in</strong> some countries, especially Afghanistan and Pakistan. Other countries<br />
such as Egypt are pilot<strong>in</strong>g <strong>in</strong>ternal contracts with the reformed district provider<br />
organizations, as well as external contracts with private providers. <strong>The</strong>re is abundant<br />
experience with contract<strong>in</strong>g out <strong>of</strong> secondary and tertiary services to private providers <strong>in</strong><br />
Jordan, Lebanon, Morocco and Tunisia.<br />
<strong>The</strong>re are several issues with the private providers. <strong>The</strong> most important <strong>of</strong> these are<br />
the quality <strong>of</strong> services provided, and the accreditation <strong>of</strong> the providers. This is especially<br />
the case <strong>in</strong> Afghanistan, Egypt, Lebanon Morocco, Pakistan and Tunisia. Skilled<br />
managerial capacity is lack<strong>in</strong>g among private providers, and their technical and f<strong>in</strong>ancial<br />
capacities also vary widely. Private providers <strong>in</strong> Egypt, Jordan, Lebanon, Morocco and<br />
Tunisia have access to advanced medical technologies that make them attractive to<br />
contract with for secondary and tertiary care services.<br />
<strong>The</strong>re are a number <strong>of</strong> risks <strong>in</strong>herent <strong>in</strong> the contract<strong>in</strong>g process. <strong>The</strong>se <strong>in</strong>clude<br />
delayed payments; differ<strong>in</strong>g <strong>in</strong>terpretations <strong>of</strong> loosely-worded contracts; limited number<br />
<strong>of</strong> providers <strong>in</strong> rural areas; capture <strong>of</strong> contract<strong>in</strong>g process by vested <strong>in</strong>terests; and limited<br />
capacity for monitor<strong>in</strong>g and evaluation. Of these, monitor<strong>in</strong>g and evaluation is especially<br />
problematic, as the capacity to monitor contracts effectively is weak <strong>in</strong> most countries.<br />
With the exception <strong>of</strong> Egypt, performance <strong>in</strong>dicators are not adequately <strong>in</strong>cluded <strong>in</strong> the<br />
design <strong>of</strong> contract and, if <strong>in</strong>cluded, <strong>of</strong>ten are not used. Management <strong>in</strong>formation systems,<br />
especially those cover<strong>in</strong>g private providers, are largely <strong>in</strong>adequate to meet the<br />
requirements for monitor<strong>in</strong>g <strong>of</strong> performance and evaluation. Payment methods for most<br />
<strong>contractual</strong> <strong>arrangements</strong> are <strong>in</strong> the form <strong>of</strong> fee-for-service or block grants. Afghanistan<br />
has experience with payment based on capitation for a specified package <strong>of</strong> <strong>health</strong><br />
services.<br />
Interventions with contract<strong>in</strong>g as the implementation strategy<br />
Table 3 gives a summary <strong>of</strong> the specific <strong>in</strong>terventions with <strong>contractual</strong><br />
<strong>arrangements</strong>. All countries have experience with contract<strong>in</strong>g out <strong>of</strong> non-cl<strong>in</strong>ical services;<br />
however, Bahra<strong>in</strong>, Morocco and Syrian Arab Republic purchase ma<strong>in</strong>ly non-cl<strong>in</strong>ical<br />
support services. Morocco also has experience with purchase <strong>of</strong> cl<strong>in</strong>ical services.<br />
Afghanistan, Egypt, Islamic Republic <strong>of</strong> Iran, Lebanon and Pakistan have experience<br />
with contract<strong>in</strong>g out primary <strong>health</strong> care services, and Jordan, Lebanon and Tunisia<br />
extensively contract out hospital and ambulatory care services to private as well as public<br />
providers.<br />
25
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
Table 3. Assessment <strong>of</strong> an <strong>in</strong>tervention with <strong>contractual</strong> <strong>arrangements</strong><br />
Country Project/programme<br />
selected<br />
Non-cl<strong>in</strong>ical services<br />
Bahra<strong>in</strong> Contract<strong>in</strong>g out <strong>of</strong><br />
non-cl<strong>in</strong>ical services<br />
Morocco Contract<strong>in</strong>g out <strong>of</strong><br />
ma<strong>in</strong>tenance <strong>in</strong><br />
hospitals<br />
Syrian Arab<br />
Republic<br />
Contract<strong>in</strong>g out <strong>of</strong><br />
ma<strong>in</strong>tenance <strong>in</strong><br />
hospitals<br />
Primary care services<br />
Afghanistan Contract<strong>in</strong>g out <strong>of</strong><br />
PHC services<br />
Egypt Contract<strong>in</strong>g through<br />
Family Health Fund<br />
Islamic<br />
Republic <strong>of</strong><br />
Iran<br />
Contract<strong>in</strong>g out by<br />
medical universities<br />
Lebanon Contract<strong>in</strong>g out <strong>of</strong><br />
primary care services<br />
Purchaser Provider Contract<br />
Intervention<br />
MOH Private <strong>sector</strong> Ma<strong>in</strong>tenance <strong>of</strong><br />
medical equipment<br />
SEGMA<br />
Hospital<br />
Centres<br />
Private<br />
providers<br />
MOH Private<br />
providers<br />
MOH<br />
Donor<br />
agencies<br />
International<br />
and national<br />
NGOs<br />
MOH District<br />
provider<br />
organizations,<br />
private<br />
providers<br />
Medical<br />
Universities<br />
Private<br />
providers<br />
Non-cl<strong>in</strong>ical<br />
services: cater<strong>in</strong>g,<br />
security garden<strong>in</strong>g,<br />
bandage<br />
Ma<strong>in</strong>tenance and<br />
clean<strong>in</strong>g <strong>of</strong><br />
hospitals <strong>in</strong> three<br />
governorates<br />
Delivery <strong>of</strong> basic<br />
pack age <strong>of</strong> <strong>health</strong><br />
services<br />
Package <strong>of</strong> primary<br />
<strong>health</strong> care services<br />
Variable – 45<br />
cl<strong>in</strong>ical and 10<br />
non-cl<strong>in</strong>ical<br />
services<br />
MOH NGOs Primary care<br />
service package<br />
26<br />
Population<br />
covered<br />
Payment methods Performance<br />
<strong>in</strong>dicators<br />
Not applicable Block payments<br />
made on quarterly<br />
<strong>in</strong>stalments<br />
Not applicable 10%–40% <strong>of</strong><br />
annual budget<br />
Not applicable Agreed payment<br />
made quarterly<br />
16.5 million Capitation at US$<br />
4.5 as the cost <strong>of</strong><br />
BPHS<br />
Five pilot<br />
governorates<br />
cover<strong>in</strong>g 5.0<br />
million<br />
Not clearly<br />
def<strong>in</strong>ed<br />
Fee-for-service<br />
Some pilot<strong>in</strong>g with<br />
capitation<br />
Block payment<br />
Cost–volume<br />
contracts<br />
50% eligible Reimbursement on<br />
fee-for-service<br />
Standards <strong>of</strong><br />
service stipulated<br />
<strong>in</strong> contract<br />
Not well def<strong>in</strong>ed<br />
Indicators related<br />
to timel<strong>in</strong>ess and<br />
quality <strong>of</strong> clean<strong>in</strong>g<br />
Based on BPHS<br />
Monitor<strong>in</strong>g<br />
system unclear<br />
11 monitor<strong>in</strong>g<br />
<strong>in</strong>dicators<br />
Elaborate system<br />
<strong>of</strong> performance<br />
evaluation,<br />
None specified
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
Country Project/programme Purchaser Provider Contract<br />
Population Payment methods Performance<br />
selected<br />
Intervention covered<br />
<strong>in</strong>dicators<br />
for un<strong>in</strong>sured Lebanese basis<br />
Pakistan Contract<strong>in</strong>g out <strong>of</strong> PHC<br />
services <strong>in</strong> Rahim Yar<br />
Khan district, Punjab<br />
Hospital services<br />
Jordan Contract<strong>in</strong>g with Royal<br />
Medical Services<br />
Contract<strong>in</strong>g with<br />
Jordan University and<br />
K<strong>in</strong>g Abdullah<br />
hospitals<br />
Lebanon Contract<strong>in</strong>g for<br />
hospitalization <strong>of</strong><br />
un<strong>in</strong>sured Lebanese<br />
Tunisia Contract<strong>in</strong>g out <strong>of</strong><br />
hospital services<br />
District<br />
government<br />
MOH<br />
Punjab Rural<br />
Support<br />
Programme<br />
Royal Medical<br />
Services<br />
Autonomous<br />
hospitals<br />
MOH 103 private<br />
hospitals<br />
National<br />
Pension and<br />
Social Security<br />
Fund<br />
(CNRPS)<br />
Private<br />
hospitals<br />
Provision <strong>of</strong><br />
services through<br />
104 PHC centres<br />
Emergency and<br />
hospital care<br />
Emergency<br />
referrals and<br />
tertiary care<br />
Hospital care to<br />
un<strong>in</strong>sured<br />
population<br />
Provision <strong>of</strong><br />
haemodialysis<br />
services<br />
27<br />
≈3 million –<br />
district’s rural<br />
population<br />
Not specified<br />
Annual budget<br />
Block payment<br />
Fee-for-service<br />
Annual balanc<strong>in</strong>g<br />
<strong>of</strong> accounts<br />
Fee-for-service<br />
50% eligible Reimbursement on<br />
fee-for-service<br />
basis<br />
Chronic renal<br />
failure patients<br />
Health facility<br />
utilization<br />
Not well def<strong>in</strong>ed<br />
None specified<br />
Fee-for-service Not well def<strong>in</strong>ed
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
Afghanistan is the only country where, <strong>in</strong> addition to the M<strong>in</strong>istry <strong>of</strong> Public Health,<br />
donors are the direct purchasers <strong>of</strong> <strong>health</strong> services from nongovernmental organizations. In<br />
other countries, the M<strong>in</strong>istry <strong>of</strong> Health, M<strong>in</strong>istry <strong>of</strong> Social Affairs and the Social Security<br />
Department are the ma<strong>in</strong> organizations that purchase primary care as well as hospital services.<br />
<strong>The</strong>re is a wide range <strong>of</strong> providers, which depends largely on the nature <strong>of</strong> the service<br />
purchased. Primary care services are provided ma<strong>in</strong>ly by nongovernmental organizations <strong>in</strong><br />
the case <strong>of</strong> Afghanistan and Pakistan, by private providers <strong>in</strong> the case <strong>of</strong> the Islamic Republic<br />
<strong>of</strong> Iran and Lebanon and by the district provider organizations and private providers <strong>in</strong> Egypt.<br />
Hospital services are purchased from private hospitals <strong>in</strong> Jordan, Lebanon and Tunisia. In the<br />
case <strong>of</strong> Jordan, the M<strong>in</strong>istry <strong>of</strong> Health also has a <strong>contractual</strong> arrangement with the Royal<br />
Medical Services for the provision <strong>of</strong> secondary and tertiary services to the Jordanian<br />
population.<br />
Factors <strong>in</strong>fluenc<strong>in</strong>g contract<strong>in</strong>g out <strong>of</strong> <strong>health</strong> services <strong>in</strong> the Region<br />
Many <strong>of</strong> the reasons for contract<strong>in</strong>g out <strong>of</strong> <strong>health</strong> services <strong>in</strong> countries <strong>of</strong> the Region are<br />
well-known and similar to other regions. Disillusionment <strong>of</strong> the general public with directly<br />
provided public <strong>sector</strong> services; the concern <strong>of</strong> the public <strong>sector</strong> to improve efficiency, access,<br />
utilization and quality <strong>of</strong> services; optimization <strong>of</strong> the hospital bed occupancy <strong>in</strong> public and<br />
private <strong>sector</strong>s; and better target<strong>in</strong>g <strong>of</strong> special populations, such as those <strong>in</strong>fected with HIV,<br />
are among the ma<strong>in</strong> reasons.<br />
Most governments have engendered national policies that promote <strong>in</strong>creased<br />
engagement with the private <strong>sector</strong> and, <strong>in</strong> some countries such as Bahra<strong>in</strong>, actively promote<br />
privatization <strong>of</strong> services. <strong>The</strong>se policies <strong>in</strong>fluence social <strong>sector</strong> m<strong>in</strong>istries to outsource <strong>health</strong><br />
services to the private <strong>sector</strong>. <strong>The</strong> national policies have <strong>in</strong> themselves been <strong>in</strong>fluenced by the<br />
current movement <strong>of</strong> globalization and <strong>in</strong>ternational trade. A robust legal framework and<br />
supportive bureaucratic environment are also important for <strong>contractual</strong> <strong>arrangements</strong> to<br />
succeed.<br />
In some countries, Afghanistan <strong>in</strong> particular, the driv<strong>in</strong>g force for contract<strong>in</strong>g out <strong>of</strong><br />
<strong>health</strong> services has been the donor agencies, especially the World Bank. In contrast,<br />
contract<strong>in</strong>g <strong>in</strong> Pakistan between the district government <strong>of</strong> Rahim Yar Khan and the Punjab<br />
Rural Support Programme, a government-organized nongovernmental organization <strong>of</strong>ten<br />
called GONGO, was purely an <strong>in</strong>digenous <strong>in</strong>itiative. Similarly, <strong>in</strong> the Islamic Republic <strong>of</strong><br />
Iran, the Third Socioeconomic Development Plan <strong>of</strong> 1999 authorized the M<strong>in</strong>istry <strong>of</strong> Health<br />
and Medical Education and its <strong>in</strong>stitutions to contract out <strong>health</strong> services.<br />
2.4 Discussion<br />
Contract<strong>in</strong>g out <strong>of</strong> <strong>health</strong> services is receiv<strong>in</strong>g <strong>in</strong>creas<strong>in</strong>g attention among low- and<br />
middle-<strong>in</strong>come countries <strong>in</strong> almost all regions <strong>of</strong> the world, but evidence relat<strong>in</strong>g to the<br />
advantages and disadvantages <strong>of</strong> the approach, while accumulat<strong>in</strong>g [11,12], is far from<br />
conclusive. This effort is the first <strong>in</strong> the Eastern Mediterranean Region, which covers a large<br />
part <strong>of</strong> the Middle East and North Africa, as well as countries <strong>of</strong> South Asia, to review the<br />
subject systematically across 10 countries. Given the diversity <strong>in</strong> the Region, it is no surprise
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
that there is wide variation among countries <strong>in</strong> the form <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> and the<br />
type <strong>of</strong> services outsourced.<br />
Contract<strong>in</strong>g out <strong>of</strong> <strong>health</strong> services is an evolutionary process. All countries, both<br />
<strong>in</strong>dustrialized and develop<strong>in</strong>g, pass through a learn<strong>in</strong>g curve before contract<strong>in</strong>g is recognized<br />
as an effective management and regulatory tool <strong>in</strong> the hands public <strong>sector</strong> managers.<br />
However, there are two important caveats. First, contract<strong>in</strong>g is a complex process that must<br />
not be regarded as a panacea for all the ills <strong>of</strong> a <strong>health</strong> delivery system. Second, not<br />
everyth<strong>in</strong>g can or should be contracted out. Jordan, Lebanon, Morocco and Tunisia have<br />
decades <strong>of</strong> experience with contract<strong>in</strong>g out hospital and primary care services, yet more time<br />
is needed before the capacities among the purchasers and providers are adequately developed<br />
and procedures streaml<strong>in</strong>ed. <strong>The</strong> experience with outsourc<strong>in</strong>g <strong>in</strong> Afghanistan, Egypt, Islamic<br />
Republic <strong>of</strong> Iran and Pakistan is relatively recent and is mostly <strong>in</strong> the area <strong>of</strong> primary care<br />
services. In these countries, the long-term susta<strong>in</strong>ability <strong>of</strong> the approach has yet to be<br />
ascerta<strong>in</strong>ed.<br />
Assessment <strong>of</strong> the overall contract<strong>in</strong>g process <strong>in</strong> countries <strong>of</strong> the Region (Table 2)<br />
shows that several key issues need to be considered before contract<strong>in</strong>g out <strong>health</strong> services<br />
becomes accepted as a viable alternative to direct provision. First, there needs to be a<br />
supportive overall public policy <strong>in</strong> favour <strong>of</strong> engag<strong>in</strong>g with the non-state <strong>sector</strong>. <strong>The</strong> policy on<br />
the private <strong>sector</strong> has seen a substantial change over the past decade <strong>in</strong> the Region; perhaps<br />
the only exception among the countries studied is the Syrian Arab Republic.<br />
Second, the legal and adm<strong>in</strong>istrative framework for contract<strong>in</strong>g out cl<strong>in</strong>ical services<br />
needs updat<strong>in</strong>g <strong>in</strong> many countries. Many m<strong>in</strong>istries <strong>of</strong> <strong>health</strong> lack a dedicated unit for<br />
contract<strong>in</strong>g. <strong>The</strong> general contract management unit <strong>in</strong> Afghanistan and the contract<strong>in</strong>g unit<br />
under the Family Health Fund <strong>in</strong> Egypt, both established under donor-f<strong>in</strong>anced projects, are<br />
two recent examples. In some middle-<strong>in</strong>come countries, this function falls under the<br />
departments <strong>of</strong> social <strong>health</strong> <strong>in</strong>surance. <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health or the prov<strong>in</strong>cial <strong>health</strong><br />
departments <strong>in</strong> Pakistan lack such a unit and the responsibility has been left to the <strong>in</strong>dividual<br />
programmes, although <strong>health</strong> services are be<strong>in</strong>g <strong>in</strong>creas<strong>in</strong>gly outsourced to the private<br />
providers.<br />
Third, the limited capacity <strong>of</strong> the public <strong>sector</strong> <strong>in</strong> many countries to undertake the<br />
necessary components <strong>of</strong> outsourc<strong>in</strong>g is a challenge that has not been adequately addressed.<br />
<strong>The</strong>se components <strong>in</strong>clude the capacity to design, negotiate and award contracts; undertake a<br />
cost, price and volume analysis <strong>of</strong> services; optimize payment methods; and effectively<br />
monitor contract performance. Unless such capacities and skills are enhanced, the value <strong>of</strong><br />
services contracted out will rema<strong>in</strong> questionable <strong>in</strong> terms <strong>of</strong> improv<strong>in</strong>g access, equity,<br />
efficiency and quality <strong>of</strong> services. Equally important is the capacity <strong>of</strong> the private providers <strong>in</strong><br />
successfully meet<strong>in</strong>g the requirements <strong>of</strong> the <strong>contractual</strong> arrangement <strong>in</strong> terms <strong>of</strong> an effective<br />
process and successful outcome. <strong>The</strong> relationship between the purchaser and the provider is<br />
an important determ<strong>in</strong>ant <strong>of</strong> the success <strong>of</strong> the contract<strong>in</strong>g process. Do the providers see the<br />
purchasers as <strong>in</strong>timidat<strong>in</strong>g because the latter have greater negotiat<strong>in</strong>g power, or does there<br />
exists mutual trust and cooperation <strong>in</strong> their relationship [10]? <strong>The</strong> perception <strong>of</strong><br />
29
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
nongovernmental organizations as pr<strong>of</strong>it-mak<strong>in</strong>g entities needs to be dispelled among public<br />
<strong>sector</strong> managers <strong>in</strong> many countries.<br />
Fourth, there may be substantial transaction costs <strong>in</strong>volved <strong>in</strong> creat<strong>in</strong>g and ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g<br />
the contracts. <strong>The</strong> study could not document the estimated transaction costs <strong>of</strong> contract<strong>in</strong>g <strong>in</strong><br />
the countries reviewed; this is a reflection <strong>of</strong> the capacities <strong>of</strong> the public <strong>sector</strong> <strong>in</strong>stitutions<br />
engaged <strong>in</strong> the contract<strong>in</strong>g process. While it is clear that contract<strong>in</strong>g may <strong>in</strong>cur high<br />
transactions costs, it is important to compare these costs with the explicit and hidden costs <strong>of</strong><br />
directly managed public systems, rather than to view them as entirely <strong>in</strong>cremental. <strong>The</strong> public<br />
agencies may face large costs <strong>in</strong> monitor<strong>in</strong>g staff and output quality, and there may also be<br />
significant costs <strong>in</strong>volved <strong>in</strong> bureaucratic adm<strong>in</strong>istrative mechanisms and <strong>in</strong> the effects <strong>of</strong><br />
political <strong>in</strong>terference [23].<br />
F<strong>in</strong>ally, another challenge is to assess objectively whether providers are actually<br />
provid<strong>in</strong>g the contracted out services on the ground. <strong>The</strong>re are several po<strong>in</strong>ts to be considered:<br />
whether monitor<strong>in</strong>g <strong>in</strong>dicators been <strong>in</strong>cluded <strong>in</strong> the contract; whether the <strong>in</strong>formation will be<br />
reported by the providers or collected by an <strong>in</strong>dependent agency; whether the public <strong>sector</strong><br />
has the means for assess<strong>in</strong>g the reliability and validity <strong>of</strong> the <strong>in</strong>formation provided; and how<br />
will that <strong>in</strong>formation be used. <strong>The</strong> monitor<strong>in</strong>g and evaluation aspects <strong>of</strong> the <strong>contractual</strong><br />
arrangement seem to be deficient <strong>in</strong> many countries <strong>of</strong> the Region. Health <strong>in</strong>formation<br />
systems <strong>in</strong> many <strong>of</strong> the low- and middle-<strong>in</strong>come countries are not well perform<strong>in</strong>g, and even<br />
when functional, they do not cover services provided by the private providers. A monitor<strong>in</strong>g<br />
and evaluation <strong>of</strong> contracts for <strong>health</strong> services <strong>in</strong> Costa Rica showed that the data gathered do<br />
not provide the purchaser with <strong>in</strong>formation directly related to all <strong>of</strong> the contract objectives or<br />
<strong>of</strong> the contract performance [24].<br />
In addition to assessment <strong>of</strong> the overall capacity, the study also assessed a specific<br />
<strong>in</strong>tervention contracted out <strong>in</strong> each country (Table 4). Although the primary <strong>in</strong>terest was <strong>in</strong><br />
contract<strong>in</strong>g out cl<strong>in</strong>ical services, at least three countries, Bahra<strong>in</strong>, Morocco and Syrian Arab<br />
Republic, have more experience with outsourc<strong>in</strong>g non-cl<strong>in</strong>ical services. Afghanistan contracts<br />
out primary <strong>health</strong> care services that cover 70% <strong>of</strong> its population. In Pakistan, follow<strong>in</strong>g the<br />
<strong>in</strong>itial success with contract<strong>in</strong>g out <strong>of</strong> <strong>health</strong> services <strong>in</strong> one district, the project is be<strong>in</strong>g scaled<br />
up rather prematurely <strong>in</strong> several other districts <strong>of</strong> the prov<strong>in</strong>ce <strong>of</strong> Punjab. Most contract<strong>in</strong>g out<br />
<strong>of</strong> primary <strong>health</strong> care services <strong>in</strong> the Region is done with nongovernmental organizations,<br />
especially <strong>in</strong> Afghanistan, Lebanon and Pakistan, and to a lesser extent Egypt. <strong>The</strong>re is more<br />
experience <strong>of</strong> contract<strong>in</strong>g primary <strong>health</strong> services with nongovernmental organizations than<br />
with for-pr<strong>of</strong>it providers <strong>in</strong> the Region, as is the case with other regions [3,25,26]. As<br />
observed <strong>in</strong> Afghanistan, population coverage <strong>in</strong>dicators, though favoured by policy-makers,<br />
can give mislead<strong>in</strong>g <strong>in</strong>formation regard<strong>in</strong>g access to basic <strong>health</strong> services, rather than<br />
<strong>in</strong>form<strong>in</strong>g about the actual services be<strong>in</strong>g received by the population. It is thus important that<br />
service coverage <strong>in</strong>dicators, such as effectiveness <strong>of</strong> treatment, quality <strong>of</strong> treatment or<br />
efficient resource use, are considered while prepar<strong>in</strong>g contracts [24].<br />
Multilateral and bilateral donor agencies, especially the World Bank, have actively<br />
promoted contract<strong>in</strong>g out <strong>of</strong> <strong>health</strong> services <strong>in</strong> some countries <strong>of</strong> the Region, particularly<br />
Afghanistan. This phenomenon has also been seen <strong>in</strong> other countries <strong>in</strong> conflict or early post-<br />
30
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
conflict period <strong>in</strong> the Region. Under such circumstances, the <strong>health</strong> systems are disrupted,<br />
nongovernmental organizations take over as significant providers <strong>of</strong> <strong>health</strong> care, m<strong>in</strong>istries <strong>of</strong><br />
<strong>health</strong> weaken, and donor funds become readily available. M<strong>in</strong>istries <strong>of</strong> <strong>health</strong> are sometimes<br />
<strong>in</strong>fluenced by donors to contract out <strong>health</strong> services to the private <strong>sector</strong>, though the m<strong>in</strong>istry<br />
might have limited capacity to ensure that contract<strong>in</strong>g out <strong>of</strong> <strong>health</strong> services is managed and<br />
monitored effectively. <strong>The</strong>re is risk that a process which is donor-driven <strong>in</strong> the short term may<br />
be less susta<strong>in</strong>able over the longer term, when donor fund<strong>in</strong>g dw<strong>in</strong>dles. What is overlooked is<br />
that susta<strong>in</strong>able <strong>health</strong> improvement is unlikely be achieved unless the physical <strong>in</strong>frastructure<br />
and human resources are revitalized for effective service delivery to the poorest and the<br />
vulnerable populations.<br />
Lebanon suffered a civil war <strong>in</strong> the 1970s and provides lessons on the long-term<br />
consequences <strong>of</strong> contract<strong>in</strong>g out services <strong>in</strong> the absence <strong>of</strong> a cautious approach. Dur<strong>in</strong>g and<br />
follow<strong>in</strong>g the civil war, there was rapid expansion <strong>of</strong> the private <strong>health</strong> <strong>sector</strong> <strong>in</strong> the 1980s and<br />
1990s, sometimes at the cost <strong>of</strong> the public <strong>sector</strong>. <strong>The</strong> result was that the M<strong>in</strong>istry <strong>of</strong> Public<br />
Health had limited <strong>role</strong> <strong>in</strong> service provision and regulatory capacity and contracted out most<br />
services to the private <strong>health</strong> <strong>sector</strong>. Given that Lebanon spends more than US$ 500 per capita<br />
on <strong>health</strong>, its <strong>health</strong> system is arguably the most <strong>in</strong>efficient <strong>in</strong> the Region.<br />
<strong>The</strong> study had several potential limitations. First, it was a challenge to coord<strong>in</strong>ate the<br />
collaborative research across 10 countries given the diverse experience with<strong>in</strong> the Region.<br />
<strong>The</strong> common proposal and the checklist as a guide to undertak<strong>in</strong>g countries studies, the<br />
establishment <strong>of</strong> an electronic network for country researchers, and on-site monitor<strong>in</strong>g dur<strong>in</strong>g<br />
country visits allowed a fair comparison across countries. Second, the wide range <strong>of</strong> services<br />
contracted out, both cl<strong>in</strong>ical to non-cl<strong>in</strong>ical, was an additional challenge that needed to be<br />
addressed. Dur<strong>in</strong>g analysis this did not pose a problem, as there were several examples <strong>of</strong><br />
different types <strong>of</strong> contract<strong>in</strong>g <strong>of</strong> various services from among the countries. In addition,<br />
cl<strong>in</strong>ical and non-cl<strong>in</strong>ical contract<strong>in</strong>g have been considered together <strong>in</strong> a previous study [2].<br />
F<strong>in</strong>ally, the focus <strong>of</strong> the multi-country study was not on the outcome but on the process <strong>of</strong><br />
contract<strong>in</strong>g, which could be argued as a possible limitation. S<strong>in</strong>ce the purpose <strong>of</strong> the study<br />
was to assess the capacity <strong>of</strong> the public <strong>sector</strong> and private providers to respectively f<strong>in</strong>ance<br />
and monitor, and to provide <strong>health</strong> services and to review at least one <strong>in</strong>tervention per country<br />
that has <strong>contractual</strong> arrangement as the implementation strategy, it was better assessed<br />
through a review <strong>of</strong> the contract<strong>in</strong>g process. This does not underestimate the importance <strong>of</strong><br />
assess<strong>in</strong>g the impact <strong>of</strong> contract<strong>in</strong>g out <strong>of</strong> <strong>health</strong> services <strong>in</strong> the Region <strong>in</strong> future studies.<br />
Contract<strong>in</strong>g is not an end <strong>in</strong> itself, nor does it mean that the state divests itself from its<br />
responsibility for <strong>health</strong>. Used prudently, it can be an effective tool to serve and promote<br />
public <strong>health</strong> objectives. When applied judiciously as a purchas<strong>in</strong>g tool, contract<strong>in</strong>g could<br />
contribute to the improvement <strong>of</strong> <strong>health</strong> system performance. Five support<strong>in</strong>g elements have<br />
been proposed for effective <strong>contractual</strong> <strong>arrangements</strong>: 1) a few clearly def<strong>in</strong>ed deliverables; 2)<br />
supportive stakeholders; 3) trust between contractor and agency contracted to deliver services;<br />
4) a source <strong>of</strong> <strong>in</strong>dependent monitor<strong>in</strong>g <strong>in</strong>formation; and 5) a legal system and political<br />
environment which persuades both sides that the contract will actually be enforced [26].<br />
31
2.5 References<br />
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
1. Jack W. Contract<strong>in</strong>g for <strong>health</strong> services: an evaluation <strong>of</strong> recent reforms <strong>in</strong> Nicaragua.<br />
Health policy and plann<strong>in</strong>g, 2003, 18(2):195–204.<br />
2. Mills A. To contract or not to contract? Issues for low and middle <strong>in</strong>come countries.<br />
Health policy and plann<strong>in</strong>g, 1998, 13(1):32–40<br />
3. Abramson WB/Lat<strong>in</strong> American and Caribbean Health Sector Reform Initiative.<br />
Partnerships between the public <strong>sector</strong> and nongovernmental organizations:<br />
contract<strong>in</strong>g for primary <strong>health</strong> care services. A state practice paper. 1999.<br />
http://www.americas.<strong>health</strong>-<strong>sector</strong>-reform.org/english/25hsrpren.pdf.<br />
4. Loev<strong>in</strong>sohn B. Practical issues <strong>in</strong> contract<strong>in</strong>g for primary <strong>health</strong> care delivery: lessons<br />
from two large projects <strong>in</strong> Bangladesh. Wash<strong>in</strong>gton DC, World Bank, 2002.<br />
HThttp://rru.worldbank.org/Documents/PapersL<strong>in</strong>ks/746.docTH<br />
5. V<strong>in</strong><strong>in</strong>g AR, Globerman S. Contract<strong>in</strong>g-out <strong>health</strong> care services: a conceptual<br />
framework. HTHealth policy, TH1999, 46: 77–96<br />
6. Ashton T, Cumm<strong>in</strong>g J, MacLean J. Contract<strong>in</strong>g for <strong>health</strong> services <strong>in</strong> a public <strong>health</strong><br />
system: the New Zealand experience. Health policy, 2004, 69: 21–31<br />
7. Williams G, Flynn R, Pickard S. Paradoxes <strong>of</strong> GP fundhold<strong>in</strong>g: contract<strong>in</strong>g for<br />
community <strong>health</strong> services <strong>in</strong> the British National Health Service. Social science and<br />
medic<strong>in</strong>e. 1997, 45(11):1669–78<br />
8. llen P. A socio-legal and economic analysis <strong>of</strong> contract<strong>in</strong>g <strong>in</strong> the NHS <strong>in</strong>ternal market<br />
us<strong>in</strong>g a case study <strong>of</strong> contract<strong>in</strong>g for district nurs<strong>in</strong>g. Social science and medic<strong>in</strong>e. 2002,<br />
54:255–66<br />
9. Christiansen T. Organization and f<strong>in</strong>anc<strong>in</strong>g <strong>of</strong> the Danish <strong>health</strong> care system. Health<br />
policy, 2002, 59(2):107–18<br />
10. Contract<strong>in</strong>g for <strong>health</strong> services, lesson from New Zealand. Manila, WHO Regional<br />
Office for the Western Pacific, 2004.<br />
HThttp://www.wpro.who.<strong>in</strong>t/NR/rdonlyres/B7DB4D58-7E19-4884-BD63-<br />
6F90D2DC1C47/0/Contract<strong>in</strong>g_for_<strong>health</strong>.pdfTH<br />
11. Liu X et al. Contract<strong>in</strong>g for primary <strong>health</strong> services: evidence on its effects and a<br />
framework for evaluation. Partnership for Health Reformplus 2004;<br />
HThttp://www.phrplus.org/Pubs/Tech053_f<strong>in</strong>.pdfTH<br />
12. Loev<strong>in</strong>sohn B, Hard<strong>in</strong>g A. Buy<strong>in</strong>g results? Contract<strong>in</strong>g for <strong>health</strong> service delivery <strong>in</strong><br />
develop<strong>in</strong>g countries. Lancet. 2005, 366:676–81<br />
13. Perrot J. <strong>The</strong> <strong>role</strong> <strong>of</strong> contract<strong>in</strong>g <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> systems performance. Discussion<br />
paper No. 1. Geneva, World Health Organization, 2004 (EIP/FER/DP/E.04.1).<br />
14. Health system priorities <strong>in</strong> the Eastern Mediterranean Region: challenges and strategic<br />
directions. Cairo, WHO Regional Office <strong>of</strong> the Eastern Mediterranean, 2004. (Technical<br />
paper EM/RC51/5). HThttp://www.emro.who.<strong>in</strong>t/RC51/media/EMRC5105.docTH<br />
15. Taylor RJ. Contract<strong>in</strong>g for <strong>health</strong> services. In: Hard<strong>in</strong>g A, Preker A, eds. Private<br />
participation <strong>in</strong> <strong>health</strong> services. Wash<strong>in</strong>gton DC, <strong>The</strong> World Bank, 2003.<br />
16. England R. Contract<strong>in</strong>g and performance management <strong>in</strong> the <strong>health</strong> <strong>sector</strong>: some<br />
po<strong>in</strong>ters on how to do it. Health Systems Resource Centre (HSRC). London,<br />
Department For International Development, 2000.<br />
HThttp://www.dfid<strong>health</strong>rc.org/shared/publications/Toolkits/Contract<strong>in</strong>g.PDFTH<br />
32
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
17. M<strong>in</strong>istry <strong>of</strong> Public Health, Transitional Islamic Government <strong>of</strong> Afghanistan.<br />
Afghanistan National Health Resources Assessment (ANHRA). Prepared for the<br />
M<strong>in</strong>istry <strong>of</strong> Public Health by MSH, HANDS and MSH Europe. 2002.<br />
HThttp://www.msh.org/afghanistan/ANHRA_2002_LITE.pdfTH<br />
18. A Basic Package <strong>of</strong> Health Services <strong>in</strong> Afghanistan. M<strong>in</strong>istry <strong>of</strong> Public Health,<br />
Afghanistan 2003<br />
19. Future privatization options and issues. Australian Hospital Design Group (AHDG).<br />
Manama, M<strong>in</strong>istry <strong>of</strong> Health, Bahra<strong>in</strong>, 2004<br />
20. M<strong>in</strong>istry <strong>of</strong> Health and Population, Egypt. Family Health Fund and Contract<strong>in</strong>g<br />
Strategy: Health F<strong>in</strong>ance and Insurance Group. Cairo, Health Sector Reform<br />
Programme, 2003<br />
21. Management and Plan Organization, Islamic Republic <strong>of</strong> Iran. <strong>The</strong> Third<br />
Socioeconomic Development Plan <strong>of</strong> 1999<br />
22. An external evaluation: Chief M<strong>in</strong>ister’s <strong>in</strong>itiative on primary <strong>health</strong> care, Rahim Yar<br />
Khan district Punjab (discussion draft). <strong>The</strong> World Bank, South Asia Human<br />
Development Unit, August 2005.<br />
23. Mills A, Broomberg J. Experience <strong>of</strong> contract<strong>in</strong>g <strong>health</strong> services: an overview <strong>of</strong> the<br />
literature. HEFP work<strong>in</strong>g paper 01/98. London School <strong>of</strong> Hygiene and Tropical<br />
Medic<strong>in</strong>e, 1998.<br />
HThttp://www.hefp.lshtm.ac.uk/publications/downloads/work<strong>in</strong>g_papers/01_98.pdfTH<br />
24. Abramson WB. Monitor<strong>in</strong>g and evaluation <strong>of</strong> contracts for <strong>health</strong> service delivery <strong>in</strong><br />
Costa Rica. Health policy and plann<strong>in</strong>g. 16(4):404–11<br />
25. Mercer A et al. Effectiveness <strong>of</strong> an NGO primary <strong>health</strong> care <strong>in</strong> rural Bangladesh:<br />
evidence from the management <strong>in</strong>formation system. Health policy and plann<strong>in</strong>g,<br />
19(4):187–98.<br />
26. Macka B, Azariah S. Contract<strong>in</strong>g NGOs: DFIDs five support<strong>in</strong>g elements. Futures<br />
Group, 2005. HThttp://www.futuresgroup.com/Documents/Contract<strong>in</strong>g_NGOs.pdfTH<br />
33
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
3. CONCLUSIONS AND RECOMMENDATIONS OF THE REGIONAL MEETING<br />
ON THE ROLE OF CONTRACTUAL ARRANGEMENTS, CAIRO, APRIL 2005<br />
<strong>The</strong> follow<strong>in</strong>g conclusions and recommendations to countries are based on the analysis and<br />
pr<strong>in</strong>cipal f<strong>in</strong>d<strong>in</strong>gs <strong>of</strong> the country studies and on the proceed<strong>in</strong>gs <strong>of</strong> the three day regional<br />
consultative meet<strong>in</strong>g <strong>of</strong> researchers, policymakers and representatives <strong>of</strong> academic and<br />
<strong>in</strong>ternational agencies, held <strong>in</strong> April 2005, <strong>in</strong> which the country studies were presented and the<br />
subject <strong>of</strong> contract<strong>in</strong>g out debated at length.<br />
Contract<strong>in</strong>g is be<strong>in</strong>g recognized as an <strong>in</strong>creas<strong>in</strong>gly important tool for implement<strong>in</strong>g <strong>health</strong><br />
polices and programmes <strong>in</strong> the Region.<br />
Contract<strong>in</strong>g depends on the overall governance features <strong>of</strong> the country, such as the legal<br />
frameworks, rule <strong>of</strong> law and enforcement mechanisms <strong>in</strong> place. To be effective,<br />
contract<strong>in</strong>g requires m<strong>in</strong>istries <strong>of</strong> <strong>health</strong> to have capacity to design, award and manage<br />
contracts.<br />
Enhanced capacity <strong>of</strong> the private <strong>sector</strong> to implement contracts and <strong>of</strong> m<strong>in</strong>istries <strong>of</strong> <strong>health</strong> to<br />
monitor is equally important.<br />
Contract<strong>in</strong>g is a means and not and end <strong>in</strong> itself, and should be used primarily to promote public<br />
<strong>health</strong> objectives.<br />
Cont<strong>in</strong>ued research is needed for evaluat<strong>in</strong>g the impact <strong>of</strong> contract<strong>in</strong>g on <strong>health</strong> outcomes <strong>in</strong> the<br />
Region.<br />
Recommendations<br />
1. Review the political, legal and adm<strong>in</strong>istrative structure <strong>of</strong> m<strong>in</strong>istries <strong>of</strong> <strong>health</strong> and<br />
ensure the presence <strong>of</strong> well function<strong>in</strong>g <strong>in</strong>formation systems that allow effective<br />
monitor<strong>in</strong>g and supervision <strong>of</strong> the contracted out services.<br />
2. Def<strong>in</strong>e public <strong>health</strong> goals <strong>in</strong> national <strong>health</strong> policies and use <strong>contractual</strong> <strong>arrangements</strong><br />
primarily to help achieve these goals. A guid<strong>in</strong>g pr<strong>in</strong>ciple is that delivery <strong>of</strong> <strong>health</strong><br />
services may be contracted out, but not the authority and responsibility, or other aspects<br />
related to governance and oversight <strong>of</strong> the <strong>health</strong> system.<br />
3. Ensure that contract<strong>in</strong>g with the private <strong>sector</strong> seeks only to harness its <strong>role</strong> <strong>in</strong><br />
achievement <strong>of</strong> public policy goals and is not considered as privatization <strong>of</strong> <strong>health</strong> care.<br />
4. Review legislation and play a proactive part <strong>in</strong> development <strong>of</strong> legislation for<br />
contract<strong>in</strong>g <strong>of</strong> services <strong>in</strong> the country.<br />
5. Consider use <strong>of</strong> contract<strong>in</strong>g <strong>in</strong> national programmes to promote equity <strong>of</strong> <strong>health</strong> services<br />
through target<strong>in</strong>g the poor and vulnerable populations.<br />
6. To improve quality <strong>of</strong> <strong>health</strong> services and to ensure that cl<strong>in</strong>ical guidel<strong>in</strong>es are followed,<br />
<strong>in</strong>clude <strong>in</strong> the <strong>contractual</strong> arrangement clearly def<strong>in</strong>ed <strong>in</strong>dicators that assess quality <strong>of</strong><br />
<strong>health</strong> care.
<strong>The</strong> <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance<br />
7. Enhance capacities at national level to better implement and understand contract<strong>in</strong>g.<br />
Managerial: contract design, <strong>in</strong>formation systems, accreditation <strong>of</strong> contractors<br />
Technical: knowledge <strong>of</strong> the areas under consideration<br />
Monitor<strong>in</strong>g: develop<strong>in</strong>g <strong>in</strong>dicators, measur<strong>in</strong>g performance, protocols, standards<br />
F<strong>in</strong>ancial: cost–benefit analysis, <strong>health</strong> accounts<br />
Consumer satisfaction<br />
Governance capacity<br />
Relevant and adapted legal, economic and f<strong>in</strong>ancial frameworks<br />
Human resource capacities<br />
Human resource negotiation capacities<br />
35
Afghanistan<br />
PART TWO: COUNTRY STUDIES
Afghanistan<br />
AFGHANISTAN<br />
37
INTRODUCTION<br />
Background<br />
Afghanistan<br />
Afghanistan’s history <strong>of</strong> the past two decades is characterized by war, anarchy,<br />
<strong>in</strong>security, political <strong>in</strong>stability and <strong>in</strong>ternational neglect. Dur<strong>in</strong>g this time drastic changes <strong>in</strong><br />
regimes have disabled the country from mak<strong>in</strong>g strides towards structural development.<br />
Although peace has prevailed s<strong>in</strong>ce 2002, the country faces real challenges <strong>in</strong> the form <strong>of</strong><br />
extreme poverty, <strong>in</strong>security, political <strong>in</strong>stability, lack <strong>of</strong> <strong>in</strong>frastructure and large gender<br />
disparities. In addition, the lack <strong>of</strong> social and human capital, absence <strong>of</strong> government <strong>in</strong>come<br />
through taxation or natural resources and the volatile political system are add<strong>in</strong>g to the<br />
complexity <strong>of</strong> <strong>health</strong> <strong>sector</strong> development. Civil society (non-pr<strong>of</strong>it) organizations <strong>in</strong><br />
Afghanistan have had a major <strong>role</strong> <strong>in</strong> provision <strong>of</strong> ma<strong>in</strong>ly primary <strong>health</strong> care <strong>in</strong> rural parts <strong>of</strong><br />
the country for more than two decades.<br />
<strong>The</strong> Government <strong>of</strong> Afghanistan, <strong>in</strong> the post-conflict period, has embarked on a policy<br />
<strong>of</strong> contract<strong>in</strong>g out primary <strong>health</strong> care services to the nongovernmental organizations <strong>in</strong>stead<br />
<strong>of</strong> directly provid<strong>in</strong>g essential <strong>health</strong> services, which has been a subject <strong>of</strong> debate <strong>in</strong> the<br />
country and outside. <strong>The</strong> purpose <strong>of</strong> this study is to document the experience <strong>of</strong> outsourc<strong>in</strong>g<br />
publicly f<strong>in</strong>anced <strong>health</strong> services to the private or nongovernmental organization <strong>sector</strong> <strong>in</strong><br />
Afghanistan, identify strengths and weaknesses and apply the lessons learnt with<strong>in</strong> and <strong>in</strong><br />
other post-conflict countries.<br />
Health system <strong>in</strong> Afghanistan<br />
Current <strong>health</strong> and social <strong>in</strong>dicators<br />
<strong>The</strong> overall <strong>health</strong> and social <strong>in</strong>dicators, <strong>in</strong>clud<strong>in</strong>g life expectancy and <strong>in</strong>fant mortality,<br />
are among the worst <strong>in</strong> the world. In addition, maternal mortality and the literacy rate among<br />
women are particularly bad. Table 1 shows some <strong>of</strong> the ma<strong>in</strong> <strong>health</strong> and social <strong>in</strong>dicators.<br />
Table 1. Selected <strong>health</strong> and social <strong>in</strong>dicators for Afghanistan<br />
Total population 23.85 million<br />
Life expectancy at birth (average) 44.5 years<br />
Total fertility rate 6.3%<br />
Contraceptive prevalence rate (modern methods) 22%<br />
Maternal mortality ratio (per 100 000 live births) 1600 deaths<br />
Delivery assisted by <strong>health</strong> pr<strong>of</strong>essional 14%<br />
Under 5 mortality rate (per 1000 live births) 257 deaths<br />
Infant mortality rate (per 1000 live births) 165 deaths<br />
Stunt<strong>in</strong>g due to chronic malnutrition 45%–59%<br />
Literacy among women 12.7%<br />
Household access to safe dr<strong>in</strong>k<strong>in</strong>g water 13%<br />
Households with adequate sanitation facilities 12%<br />
Sources: Afghanistan Health and Social Indicators Fact Sheet (Updated March 2005), M<strong>in</strong>istry <strong>of</strong> Public Health<br />
Afghanistan Human Development Report, United Nations Development Programme, February 2005<br />
38
Current <strong>health</strong> services delivery<br />
Afghanistan<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public Health has focused its attention on the delivery <strong>of</strong> a Basic<br />
Package <strong>of</strong> Health Services (BPHS) and an Essential Package <strong>of</strong> Hospital Services (EPHS) to<br />
which the M<strong>in</strong>istry <strong>of</strong> Public Health and its partners are committed. Until 2002, around 80%<br />
<strong>of</strong> the <strong>health</strong> facilities were functional through nongovernmental organization setups, which<br />
were contracted by the donor and received funds directly. <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public Health was<br />
not <strong>in</strong>volved <strong>in</strong> the contract<strong>in</strong>g process. <strong>The</strong> situation has changed s<strong>in</strong>ce then. Currently, the<br />
external grants, especially those <strong>of</strong> the World Bank, are provided either through the M<strong>in</strong>istry<br />
<strong>of</strong> Public Health or <strong>in</strong> close collaboration with the M<strong>in</strong>istry <strong>of</strong> Public Health, as <strong>in</strong> the case <strong>of</strong><br />
the United States Agency for International Development (USAID), European Commission<br />
(EC), Asia Development Bank (ADB).<br />
<strong>The</strong>re are two service delivery mechanisms for the BPHS, contract<strong>in</strong>g out to<br />
nongovernmental organizations and direct provision by the M<strong>in</strong>istry <strong>of</strong> Public Health through<br />
its strengthen<strong>in</strong>g mechanism. By January 2005, the funds committed for implementation <strong>of</strong> the<br />
BPHS could ensure delivery <strong>of</strong> this package to a population <strong>of</strong> roughly 71% through<br />
nongovernmental organizations and about 5% through the M<strong>in</strong>istry <strong>of</strong> Public Health. F<strong>in</strong>anc<strong>in</strong>g<br />
and delivery <strong>of</strong> secondary-level <strong>health</strong> care is still the ma<strong>in</strong> responsibility <strong>of</strong> the government. In<br />
order to have a standard package for hospital services <strong>in</strong> the country, the M<strong>in</strong>istry <strong>of</strong> Public<br />
Health developed a hospital policy and recently f<strong>in</strong>alized the Essential Package <strong>of</strong> Hospital<br />
Services (EPHS). Although donors and the M<strong>in</strong>istry <strong>of</strong> F<strong>in</strong>ance have shown less <strong>in</strong>terest <strong>in</strong><br />
support<strong>in</strong>g hospitals dur<strong>in</strong>g the past two years, the M<strong>in</strong>istry <strong>of</strong> Public Health has secured a<br />
commitment <strong>of</strong> US$ 10.4 million for implement<strong>in</strong>g this package dur<strong>in</strong>g 2005–2006.<br />
Programmes such as rout<strong>in</strong>e immunization, nutrition and malaria, tuberculosis and HIV<br />
AIDS control are not yet fully <strong>in</strong>tegrated <strong>in</strong>to the BPHS and their implementation mechanisms are<br />
through vertical approaches. United Nations agencies such as UNICEF, WHO, UNFPA and the<br />
Global Fund are support<strong>in</strong>g the M<strong>in</strong>istry <strong>of</strong> Public Health <strong>in</strong> this regard technically and to some<br />
extent f<strong>in</strong>ancially.<br />
Civil society (non-pr<strong>of</strong>it organizations) <strong>in</strong> Afghanistan had a major <strong>role</strong> <strong>in</strong> provision <strong>of</strong><br />
ma<strong>in</strong>ly primary <strong>health</strong> care <strong>in</strong> rural parts <strong>of</strong> the country for more than two decades. Currently<br />
they are work<strong>in</strong>g under mutual agreement and close coord<strong>in</strong>ation with the M<strong>in</strong>istry <strong>of</strong> Public<br />
Health. <strong>The</strong>y are contracted to provide BPHS for 71% (16.5 million) <strong>of</strong> the population. <strong>The</strong><br />
government has not yet decided whether, <strong>in</strong> the long run, it wants to take on responsibility for<br />
deliver<strong>in</strong>g public <strong>health</strong> services itself or to cont<strong>in</strong>ue contract<strong>in</strong>g with nongovernmental<br />
organizations. <strong>The</strong> decision on this will be made based on rigorous evaluation <strong>of</strong> current<br />
contracts, grants, and the M<strong>in</strong>istry <strong>of</strong> Public Health strengthen<strong>in</strong>g mechanism <strong>in</strong> late 2006.<br />
National <strong>health</strong> policy and strategy<br />
<strong>The</strong> National Health Policy 2005–2009 guides the overall context for all <strong>health</strong> and<br />
<strong>health</strong>-related work and outl<strong>in</strong>es the priorities for accelerat<strong>in</strong>g implementation for the fiveyear<br />
period, 2005–2009 (Box 1).<br />
39
Afghanistan<br />
Box 1. National <strong>health</strong> policy priorities 2005–2009<br />
Delivery <strong>of</strong> <strong>health</strong> services<br />
1. *Implement the basic package <strong>of</strong> <strong>health</strong> services<br />
2. *Implement the essential package <strong>of</strong> hospital services<br />
3. *Establish prevention and promotion programmes<br />
4. Promote greater community participation<br />
5. Improve coord<strong>in</strong>ation <strong>of</strong> <strong>health</strong> services<br />
6. Strengthen the coverage <strong>of</strong> quality support programmes<br />
Reduc<strong>in</strong>g morbidity and mortality<br />
7. *Improve the quality <strong>of</strong> maternal and reproductive <strong>health</strong> care<br />
8. *Improve the quality <strong>of</strong> child <strong>health</strong> <strong>in</strong>itiatives<br />
9. *Strengthen the delivery <strong>of</strong> cost effective <strong>in</strong>tegrated communicable disease control programmes<br />
10. Reduce prevalence <strong>of</strong> malnutrition, <strong>in</strong>creas<strong>in</strong>g access to iodized salt and micronutrients, and <strong>in</strong>crease<br />
exclusive breastfeed<strong>in</strong>g<br />
Institutional development<br />
11. *Promote <strong>in</strong>stitutional and management development<br />
12. *Strengthen human resources development, especially <strong>of</strong> female staff<br />
13. *Strengthen <strong>health</strong> plann<strong>in</strong>g, monitor<strong>in</strong>g and evaluation<br />
14. Develop <strong>health</strong> f<strong>in</strong>anc<strong>in</strong>g and national <strong>health</strong> accounts<br />
15. Strengthen prov<strong>in</strong>cial level management and coord<strong>in</strong>ation<br />
16. Cont<strong>in</strong>ue to implement priority restructur<strong>in</strong>g and reform<br />
17. Establish quality assurance<br />
18. Develop and enforce public and private <strong>sector</strong> regulations and laws<br />
*Top priority<br />
Source: National <strong>health</strong> policy 2005–2009 and national <strong>health</strong> strategy 2005–2006, M<strong>in</strong>istry <strong>of</strong> Health Afghanistan, April<br />
2005<br />
OBJECTIVES AND METHODOLOGY<br />
This study aims to document the experience <strong>of</strong> outsourc<strong>in</strong>g publicly f<strong>in</strong>anced <strong>health</strong><br />
services to private organizations or the nongovernmental organization <strong>sector</strong> <strong>in</strong> Afghanistan.<br />
<strong>The</strong> specific objectives <strong>of</strong> the study are to: present an overview <strong>of</strong> the context <strong>in</strong> which<br />
contract<strong>in</strong>g out is function<strong>in</strong>g <strong>in</strong> the <strong>health</strong> <strong>sector</strong>; highlight actual experiences <strong>in</strong>clud<strong>in</strong>g<br />
factors that <strong>in</strong>fluence contract<strong>in</strong>g <strong>in</strong> <strong>health</strong>; share the f<strong>in</strong>d<strong>in</strong>gs about the contract<strong>in</strong>g <strong>of</strong> Basic<br />
Package <strong>of</strong> Health Services (BPHS) as a specific public <strong>health</strong> programme that has taken up<br />
<strong>contractual</strong> <strong>arrangements</strong> as its pr<strong>in</strong>cipal implementation strategy; and summarize lessons<br />
learnt to date regard<strong>in</strong>g the <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> post-conflict Afghanistan.<br />
An extensive review was undertaken <strong>of</strong> the reports developed by the M<strong>in</strong>istry <strong>of</strong> Public<br />
Health and <strong>in</strong>ternational development agencies <strong>in</strong>volved <strong>in</strong> <strong>health</strong>. Donor mission reports on<br />
the <strong>role</strong> <strong>of</strong> contract<strong>in</strong>g out <strong>of</strong> <strong>health</strong> services were reviewed, <strong>in</strong> addition to published and<br />
unpublished literature on contract<strong>in</strong>g out <strong>of</strong> <strong>health</strong> services. Detailed discussions were held<br />
40
Afghanistan<br />
with the staff <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Public Health and those directly <strong>in</strong>volved <strong>in</strong> contract<strong>in</strong>g,<br />
especially <strong>in</strong>ternational advisers to the M<strong>in</strong>istry <strong>of</strong> Public Health. <strong>The</strong> checklist provided by<br />
the WHO Regional Office for the Eastern Mediterranean for assess<strong>in</strong>g the overall capacity<br />
for contract<strong>in</strong>g out <strong>of</strong> <strong>health</strong> services was used as a guide for data collection.<br />
FINDINGS<br />
Wider governmental context for contract<strong>in</strong>g<br />
As a result <strong>of</strong> war, no legislation was passed dur<strong>in</strong>g the past 25 years and the exist<strong>in</strong>g<br />
laws were largely irrelevant to the current situation <strong>in</strong> the <strong>health</strong> <strong>sector</strong>. <strong>The</strong> legal framework<br />
was thus obsolete. Such a situation provides a new opportunity for updat<strong>in</strong>g legislation to<br />
support contract<strong>in</strong>g out <strong>of</strong> <strong>health</strong> services <strong>in</strong> Afghanistan. With an elected government <strong>in</strong> place<br />
the environment is conducive to develop<strong>in</strong>g legislation to support <strong>health</strong> <strong>sector</strong> reforms.<br />
<strong>The</strong> policy <strong>of</strong> the government on contract<strong>in</strong>g out <strong>of</strong> <strong>health</strong> services was developed and is<br />
be<strong>in</strong>g implemented with<strong>in</strong> the framework <strong>of</strong> the 2004 Constitution <strong>of</strong> Afghanistan and the<br />
Public Investment Programme (2004). <strong>The</strong> Constitution is supportive <strong>of</strong> the private <strong>sector</strong> and<br />
its further development <strong>in</strong> the country.<br />
In recent years the government worked to prepare legislation to support the <strong>role</strong> <strong>of</strong><br />
nongovernmental organizations <strong>in</strong> the country, which is to be submitted to the country’s<br />
president for endorsement. This legislation has been subject to heated discussion <strong>in</strong> the<br />
cab<strong>in</strong>et, especially one <strong>of</strong> the articles which prohibits the nongovernmental organizations<br />
from participat<strong>in</strong>g <strong>in</strong> construction and other pr<strong>of</strong>it-mak<strong>in</strong>g bidd<strong>in</strong>g processes. Although the<br />
proposed bill prohibits the nongovernmental organizations from participat<strong>in</strong>g <strong>in</strong> any k<strong>in</strong>d <strong>of</strong><br />
bidd<strong>in</strong>g, it has yet not been approved by the president, and discussions cont<strong>in</strong>ue <strong>in</strong> the media<br />
as there are diverse views on the experience <strong>of</strong> work<strong>in</strong>g with nongovernmental organizations.<br />
Of specific concern is the issue <strong>of</strong> nongovernmental organizations, which by nature are nonpr<strong>of</strong>it<br />
entities, be<strong>in</strong>g <strong>in</strong>volved <strong>in</strong> pr<strong>of</strong>it-mak<strong>in</strong>g ventures.<br />
Contract<strong>in</strong>g policy<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public Health is closely follow<strong>in</strong>g the legislative process, s<strong>in</strong>ce its<br />
experience <strong>of</strong> work<strong>in</strong>g and coord<strong>in</strong>at<strong>in</strong>g with nongovernmental organizations has been<br />
successful <strong>in</strong> the past. <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public Health has also ga<strong>in</strong>ed considerable experience<br />
<strong>in</strong> monitor<strong>in</strong>g and evaluation and regulation <strong>of</strong> nongovernmental organizations. <strong>The</strong> M<strong>in</strong>istry<br />
believes that nongovernmental organizations can play effective <strong>role</strong>s <strong>in</strong> the development <strong>of</strong><br />
Afghanistan through delivery <strong>of</strong> essential <strong>health</strong> services, while the M<strong>in</strong>istry itself can focus<br />
on effectively regulat<strong>in</strong>g the organizations and on further strengthen<strong>in</strong>g its monitor<strong>in</strong>g and<br />
evaluation capacity.<br />
A key priority <strong>in</strong> the Public Investment Programme (2004) is expansion <strong>of</strong> delivery,<br />
coverage and quality <strong>of</strong> both basic <strong>health</strong> services and hospital services. <strong>The</strong> public<br />
<strong>in</strong>vestment programme calls for strengthen<strong>in</strong>g and accelerat<strong>in</strong>g implementation throughout<br />
government, s<strong>in</strong>ce it acknowledges that ‘implementation will make or break Afghanistan’s<br />
41
Afghanistan<br />
reconstruction efforts’. <strong>The</strong> programme also takes <strong>in</strong>to consideration that while<br />
implementation strategies will vary across <strong>sector</strong>s, reflect<strong>in</strong>g specific circumstances, there<br />
will be key common elements (such as priority restructur<strong>in</strong>g and reform <strong>of</strong> facilities) that<br />
accelerate m<strong>in</strong>isterial reforms. <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public Health is closely <strong>in</strong>volved <strong>in</strong> this<br />
process.<br />
Rationale for contract<strong>in</strong>g<br />
A Jo<strong>in</strong>t Donor Mission conducted <strong>in</strong> early 2002, based on the estimate that that some<br />
80% <strong>of</strong> <strong>health</strong> facilities were be<strong>in</strong>g operated by nongovernmental organizations,<br />
recommended that the government should move from direct <strong>in</strong>volvement service provision <strong>in</strong><br />
favour <strong>of</strong> a stewardship <strong>role</strong> while focus<strong>in</strong>g on policy development and regulation. <strong>The</strong><br />
M<strong>in</strong>istry <strong>of</strong> Public Health favoured the option <strong>of</strong> contract<strong>in</strong>g <strong>in</strong> or contract<strong>in</strong>g out <strong>health</strong><br />
services through establishment <strong>of</strong> performance-based partnership agreements between the<br />
M<strong>in</strong>istry <strong>of</strong> Public Health and nongovernmental organizations. <strong>The</strong> rationales for this decision<br />
<strong>in</strong>cluded the devastated public <strong>health</strong> system and <strong>in</strong>frastructure; large and credible presence <strong>of</strong><br />
nongovernmental organizations with a long history <strong>of</strong> experience with <strong>health</strong> services <strong>in</strong><br />
Afghanistan; better flexibility <strong>of</strong> nongovernmental organizations <strong>in</strong> management <strong>of</strong> resources;<br />
lack <strong>of</strong> human resources and capacity with<strong>in</strong> the M<strong>in</strong>istry; openness <strong>of</strong> the new ideas and<br />
approaches <strong>of</strong> the new M<strong>in</strong>istry <strong>of</strong> Public Health adm<strong>in</strong>istration, with many <strong>of</strong> its staff com<strong>in</strong>g<br />
from nongovernmental organization backgrounds; global experience <strong>of</strong> efficiency <strong>in</strong><br />
contract<strong>in</strong>g, especially <strong>in</strong> post-conflict Cambodia; donors’ <strong>in</strong>terest and <strong>in</strong>fluence.<br />
A performance-based partnership agreement strategy was designed based on the lessons<br />
learnt from a similar project <strong>in</strong> Cambodia which tested the performance <strong>of</strong> two different<br />
contract<strong>in</strong>g models aga<strong>in</strong>st service delivery by the government itself. Afghanistan’s transition<br />
to post-conflict status co<strong>in</strong>cided with the completion <strong>of</strong> the pilot evaluation <strong>in</strong> November<br />
2001, which concluded that government contract<strong>in</strong>g <strong>of</strong> the provision <strong>of</strong> <strong>health</strong> services to nongovernment<br />
entities was: feasible, cost-effective, high perform<strong>in</strong>g and equitable. Eventually,<br />
this concept became the backbone <strong>of</strong> the national <strong>health</strong> policy, and served to steer policy<br />
development <strong>in</strong> such a way that would facilitate <strong>health</strong> service delivery through performancebased<br />
partnership agreements.<br />
Dur<strong>in</strong>g the many years <strong>of</strong> war, <strong>health</strong> services were delivered <strong>in</strong> fragmented pockets <strong>of</strong><br />
isolation by different providers. <strong>The</strong> limited <strong>health</strong> services that were available were provided<br />
by humanitarian agencies, <strong>in</strong>clud<strong>in</strong>g local and <strong>in</strong>ternational nongovernmental organizations<br />
and United Nations agencies.<br />
In the immediate post-conflict period, the government <strong>in</strong> general and the M<strong>in</strong>istry <strong>of</strong><br />
Public Health <strong>in</strong> particular had three possible options.<br />
1) <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public Health could be the ma<strong>in</strong> provider while also develop<strong>in</strong>g its<br />
stewardship <strong>role</strong>.<br />
2) A balance could be developed between the provision <strong>of</strong> public <strong>sector</strong> <strong>health</strong> services and<br />
contracted-<strong>in</strong> or contracted-out <strong>health</strong> services to the private <strong>sector</strong>; <strong>in</strong> this <strong>in</strong>stance,<br />
nongovernmental organizations.<br />
42
Afghanistan<br />
3) Greater emphasis could be placed on either contracted-<strong>in</strong> or contracted-out <strong>health</strong><br />
services through establishment <strong>of</strong> performance-based partnership agreements between<br />
the M<strong>in</strong>istry <strong>of</strong> Public Health and nongovernmental organizations which would allow<br />
the M<strong>in</strong>istry <strong>of</strong> Public Health to utilize exist<strong>in</strong>g nongovernmental organization capacity<br />
to deliver services while still ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g control over the strategic direction <strong>of</strong> the<br />
<strong>health</strong> <strong>sector</strong>.<br />
<strong>The</strong> Basic Package <strong>of</strong> Health Services<br />
<strong>The</strong> government has committed itself to ensur<strong>in</strong>g that the BPHS is delivered to all<br />
Afghans, regardless <strong>of</strong> location, ethnicity or gender, as soon as possible. <strong>The</strong> government will<br />
cont<strong>in</strong>ue to pursue this over-arch<strong>in</strong>g goal as its first priority, as a means to provide a peace<br />
dividend to Afghans and to achieve the Millennium Development Goals (MDGs). <strong>The</strong> BPHS<br />
was def<strong>in</strong>ed <strong>in</strong> early 2003 with the assistance <strong>of</strong> WHO. <strong>The</strong> key elements <strong>in</strong>cluded: those<br />
services which would have the greatest impact on the major <strong>health</strong> problems; services that<br />
were cost-effective <strong>in</strong> address<strong>in</strong>g the problems faced by many people; and services which<br />
could be delivered to give equal access to both rural and urban populations.<br />
<strong>The</strong> BPHS has two purposes: to provide a standardized package <strong>of</strong> basic services which<br />
forms the core <strong>of</strong> service delivery <strong>in</strong> all primary <strong>health</strong> care facilities; and to promote a<br />
redistribution <strong>of</strong> <strong>health</strong> services by provid<strong>in</strong>g equitable access, especially <strong>in</strong> underserved<br />
areas. <strong>The</strong> BPHS provides a comprehensive list <strong>of</strong> services: maternal and newborn <strong>health</strong>;<br />
child <strong>health</strong> and immunization; public nutrition; communicable disease control; mental <strong>health</strong><br />
care; and disability. It also <strong>in</strong>cludes a supply <strong>of</strong> essential drugs to be <strong>of</strong>fered at four standard<br />
levels <strong>of</strong> <strong>health</strong> facility: the <strong>health</strong> post, basic <strong>health</strong> centre comprehensive <strong>health</strong> centre, and<br />
district hospital. <strong>The</strong>se facility categories replace a number <strong>of</strong> different nomenclature systems,<br />
and will help create a more uniform system <strong>of</strong> classify<strong>in</strong>g and denot<strong>in</strong>g <strong>health</strong> facilities.<br />
Once the current content <strong>of</strong> the BPHS has been successfully delivered to all Afghans,<br />
the government <strong>in</strong>tends to broaden the scope <strong>of</strong> the BPHS to <strong>in</strong>clude additional services such<br />
as mental <strong>health</strong>, community care for the disabled, and prevention <strong>of</strong> HIV/AIDS. This will<br />
likely be implemented <strong>in</strong> 2010, but could beg<strong>in</strong> earlier if progress cont<strong>in</strong>ues at current rates.<br />
43
Implementation <strong>of</strong> BPHS<br />
Afghanistan<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public Health based on its decision to contract out, the potential<br />
fund<strong>in</strong>g possibility <strong>of</strong> donors and the prelim<strong>in</strong>ary cost<strong>in</strong>g <strong>of</strong> the BPHS at US$ 4.5 per capita<br />
has def<strong>in</strong>ed separate geographic regions to use donor fund for the delivery <strong>of</strong> the package.<br />
Initially the World Bank committed to use US$ 46.3 million <strong>of</strong> its grants, USAID committed<br />
US$ 60 million and the EC Euro 8 million, with possible additional annual grants for<br />
implementation <strong>of</strong> BPHS. <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public Health agreed to identify certa<strong>in</strong> number <strong>of</strong><br />
prov<strong>in</strong>ces out the 34 prov<strong>in</strong>ces for the earmarked funds (Figure 1). Through this process, 11<br />
prov<strong>in</strong>ces are covered by World Bank funds, 13 by USAID and 10 prov<strong>in</strong>ces by the EC<br />
(Table 2). <strong>The</strong> Asian Development Bank, KfW (German Credit Bank) later jo<strong>in</strong>ed this process<br />
as well, cover<strong>in</strong>g 11 districts.<br />
Source: M<strong>in</strong>istry <strong>of</strong> Public Health, Afghanistan (updated 20February 2005)<br />
Figure 1. Distribution <strong>of</strong> geographical regions for delivery <strong>of</strong> BPHS by fund<strong>in</strong>g<br />
agency<br />
44
Afghanistan<br />
Table 2. Implementation <strong>of</strong> BPHS<br />
Donor WB ($ 47 million) USAID<br />
($ 58 million)<br />
EC (€ 25 million) ADB ($ 3 million)<br />
Pre selection EOI Pre qualification Eligible<br />
nongovernmental<br />
organizations<br />
EOI<br />
Tender RFP RFA RFP RFP<br />
Selection QCBS QBS QBS QCBS<br />
Type <strong>of</strong> Performance-based Grant Agreement Grant Contract Performance<br />
contract service contract<br />
based service<br />
contract<br />
Payment Lump sum Expenditure based Expenditure based Lump sum<br />
Management M<strong>in</strong>istry <strong>of</strong> Public M<strong>in</strong>istry <strong>of</strong> Public M<strong>in</strong>istry <strong>of</strong> Public M<strong>in</strong>istry <strong>of</strong> Public<br />
Health<br />
Health–MSH Health–EC<br />
Health–<br />
nongovernmental<br />
organization<br />
trustee<br />
size <strong>of</strong><br />
implement<br />
Prov<strong>in</strong>ce wide District wide Mix District wide<br />
Evaluation Third Party + M<strong>in</strong>istry <strong>of</strong> Public Health + Donor<br />
EOI – Expression <strong>of</strong> <strong>in</strong>terest; RFP – Request for proposal; RFA – Request for application; QCBS – Quality and cost based<br />
selection; QBS - Quality based selection;<br />
After identification <strong>of</strong> geographical coverage, the second issue was the size <strong>of</strong><br />
<strong>in</strong>dividual contracts. <strong>The</strong> World Bank favoured contracts with wider coverage size (prov<strong>in</strong>ce<br />
wide); USAID favoured relatively smaller sizes (districts or a cluster <strong>of</strong> districts); and the EC<br />
proposed prov<strong>in</strong>cial and district levels, consider<strong>in</strong>g the realities <strong>of</strong> different prov<strong>in</strong>ces.<br />
Contract<strong>in</strong>g mechanisms<br />
<strong>The</strong> <strong>in</strong>itial agreement between the M<strong>in</strong>istry <strong>of</strong> Public Health and donors was for<br />
contract<strong>in</strong>g out, preferably through performance-based partnership agreement contracts. <strong>The</strong><br />
five primary donors that support contract<strong>in</strong>g out use different mechanisms to contract out to<br />
nongovernmental organizations. For example, the M<strong>in</strong>istry <strong>of</strong> Public Health is responsible for<br />
contract<strong>in</strong>g nongovernmental organizations who compete for World Bank funds. <strong>The</strong><br />
M<strong>in</strong>istry’s Grant and Contract Management Unit (GCMU), which was established <strong>in</strong> April<br />
2003, manages these contracts. <strong>The</strong> Asian Development Bank and USAID have each tasked a<br />
nongovernmental organization to undertake the contract<strong>in</strong>g process, and the EC and KfW<br />
undertake this work by themselves. <strong>The</strong> M<strong>in</strong>istry, through the GCMU, is fully <strong>in</strong>volved <strong>in</strong> the<br />
contract<strong>in</strong>g processes <strong>of</strong> other donors as well. So far, BPHS implementation and third party<br />
monitor<strong>in</strong>g and evaluation are the only service delivery contracts for <strong>health</strong> <strong>in</strong> Afghanistan.<br />
Monitor<strong>in</strong>g performance <strong>of</strong> contracts<br />
<strong>The</strong> monitor<strong>in</strong>g <strong>of</strong> contracts and the assessment <strong>of</strong> performance has been a challenge for<br />
the GCMU because <strong>of</strong> the absence <strong>of</strong> a functional <strong>health</strong> <strong>in</strong>formation system. Monitor<strong>in</strong>g and<br />
45
Afghanistan<br />
evaluation is primarily undertaken through third parties. A Monitor<strong>in</strong>g and Evaluation Board<br />
has been established for this purpose; however, it is not fully functional. <strong>The</strong> public <strong>health</strong><br />
managers <strong>in</strong> prov<strong>in</strong>ces report feel<strong>in</strong>g marg<strong>in</strong>alized and disconnected from the entire process<br />
<strong>of</strong> contract<strong>in</strong>g out.<br />
In collaboration with the Johns Hopk<strong>in</strong>s School <strong>of</strong> Public Health, the M<strong>in</strong>istry <strong>of</strong> Public<br />
Health <strong>in</strong>troduced a <strong>health</strong> <strong>sector</strong> balanced score card <strong>in</strong> 2004. <strong>The</strong> balanced score card<br />
provides comprehensive basel<strong>in</strong>e <strong>in</strong>formation on service provision, the assessment <strong>of</strong> which is<br />
generally quite low. <strong>The</strong> perceptions <strong>of</strong> <strong>health</strong> workers that use good outpatient care practices<br />
and basic <strong>health</strong> centres that see a targeted number <strong>of</strong> outpatients were particularly low<br />
(median 10% each). Provid<strong>in</strong>g delivery care accord<strong>in</strong>g to the BPHS guidel<strong>in</strong>es was also quite<br />
low (median 14%).<br />
Analysis <strong>of</strong> the strengths, weaknesses and risks <strong>of</strong> the contract<strong>in</strong>g process<br />
Purchaser<br />
Strengths<br />
• <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public Health has a clear policy for outsourc<strong>in</strong>g the basic <strong>health</strong> care<br />
delivery to nongovernmental organizations and has rema<strong>in</strong>ed committed to it;<br />
• <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public Health has established a Grants and Contracts Management Unit<br />
which is <strong>in</strong>dependently manag<strong>in</strong>g the US$ 60 million grant <strong>of</strong> World Bank for<br />
performance-based partnership agreement contracts to nongovernmental organizations<br />
and has enabled the M<strong>in</strong>istry to:<br />
help expand the delivery <strong>of</strong> the BPHS;<br />
strengthen its stewardship <strong>role</strong> <strong>in</strong> the <strong>health</strong> <strong>sector</strong>;<br />
<strong>in</strong>tegrate donor, multilateral, and nongovernmental organization efforts; and<br />
develop its capacity to work effectively with stakeholders <strong>in</strong> establish<strong>in</strong>g an effective<br />
and efficient public–private mix.<br />
• <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public Health has made every effort to ensure transparency <strong>in</strong> the<br />
contract<strong>in</strong>g process through which donor funds are channelled for the delivery <strong>of</strong> BPHS.<br />
• <strong>The</strong> effective leadership and coord<strong>in</strong>ation skills <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Public Health has<br />
played a key <strong>role</strong> <strong>in</strong> the success <strong>of</strong> the contracts.<br />
• <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public Health has worked to create a friendly work<strong>in</strong>g environment with<br />
nongovernmental organizations and to deal with them as partners rather than<br />
implementers.<br />
Weaknesses<br />
• <strong>The</strong>re is a huge dependence on external grants for purchas<strong>in</strong>g services.<br />
• <strong>The</strong> government has little previous experience <strong>in</strong> contract<strong>in</strong>g.<br />
• Reliable data for decision-mak<strong>in</strong>g are lack<strong>in</strong>g.<br />
• Capacity for <strong>health</strong> plann<strong>in</strong>g is low.<br />
• A monitor<strong>in</strong>g and evaluation system has not yet been developed.<br />
46
Provider<br />
Strengths<br />
Afghanistan<br />
• Nongovernmental organizations work<strong>in</strong>g <strong>in</strong> Afghanistan have long experience with<br />
contract<strong>in</strong>g and familiarity with purchaser–provider relationships.<br />
• A large number <strong>of</strong> national and <strong>in</strong>ternational nongovernmental organizations are present<br />
<strong>in</strong> the <strong>health</strong> <strong>sector</strong>.<br />
• Many providers have rich experience <strong>in</strong> <strong>health</strong> service delivery, especially <strong>in</strong> rural areas,<br />
and better understand<strong>in</strong>g <strong>of</strong> what is meant by a def<strong>in</strong>ed package <strong>of</strong> services.<br />
• Some nongovernmental organizations have good technical and managerial capability.<br />
Weaknesses<br />
• Nongovernmental organizations have experience <strong>in</strong> contract<strong>in</strong>g directly with donors and<br />
are new to <strong>contractual</strong> <strong>arrangements</strong> with the government.<br />
• Many nongovernmental organizations may lose <strong>in</strong>terest once donor fund<strong>in</strong>g dries out.<br />
• <strong>The</strong> overhead adm<strong>in</strong>istrative costs <strong>of</strong> nongovernmental organizations may be high, which<br />
may compromise the quality <strong>of</strong> services.<br />
• Nongovernmental organizations are focused on the curative aspects <strong>of</strong> the benefit package<br />
and can easily overlook the promotive and preventive element.<br />
Risks<br />
• Emergency withdrawal lead<strong>in</strong>g to collapse <strong>of</strong> contracted out services.<br />
• Reductions <strong>in</strong> external donor funds for contract<strong>in</strong>g out with nongovernmental<br />
organizations.<br />
• Increas<strong>in</strong>g demands on central government funds for hospital services.<br />
• Ris<strong>in</strong>g expectations <strong>in</strong> the population for access, quality and range <strong>of</strong> services.<br />
• More services provided by private medical services <strong>in</strong> the ma<strong>in</strong> urban centres.<br />
• Scarcity <strong>of</strong> skilled <strong>health</strong> workforce <strong>in</strong> the country.<br />
• Problems <strong>of</strong> security, especially <strong>in</strong> rural and remote areas.<br />
Lessons learnt<br />
<strong>The</strong> experience <strong>of</strong> contract<strong>in</strong>g out <strong>health</strong> services to nongovernmental organizations <strong>in</strong><br />
Afghanistan has produced several lessons, which are summarized below. Box 2 gives the<br />
prerequisites for successful contract<strong>in</strong>g based on experiences from Afghanistan.<br />
• In post-conflict countries, “buy<strong>in</strong>g the capacity” for contract management is only a short<br />
term solution. “Build<strong>in</strong>g the capacity” is essential over the long term.<br />
• <strong>The</strong> contract management entity should be autonomous .<br />
• <strong>The</strong> <strong>role</strong>s and responsibilities <strong>of</strong> the purchaser and provider should be absolutely clear and<br />
should be stated <strong>in</strong> the contract document.<br />
• Involvement <strong>of</strong> related departments <strong>in</strong> all stages ensures broad acceptance.<br />
47
Afghanistan<br />
• Change <strong>in</strong> th<strong>in</strong>k<strong>in</strong>g <strong>of</strong> public <strong>of</strong>ficials towards contract<strong>in</strong>g requires “change management”<br />
rather than only directives.<br />
• Local contractors should be preferred over <strong>in</strong>ternational ones, and their capacity should be<br />
developed to ensure susta<strong>in</strong>ability.<br />
• Independent performance evaluation is a key for determ<strong>in</strong><strong>in</strong>g <strong>health</strong> outcomes as well as<br />
ensur<strong>in</strong>g transparency.<br />
• <strong>The</strong> better def<strong>in</strong>ed scope <strong>of</strong> work, the better coord<strong>in</strong>ated the approach the more successful<br />
the contract.<br />
Box 2. Prerequisites for successful contract<strong>in</strong>g–Afghanistan experience<br />
• Country regulations and procedures are well developed<br />
• Officials are committed<br />
• National capacity is present<br />
• Targets are clear<br />
• Roles and responsibilities <strong>of</strong> all are well def<strong>in</strong>ed<br />
• Appraisal is regular<br />
• Compensation mechanism is effective<br />
• Transparency is ensured<br />
• Security is present<br />
48
Bahra<strong>in</strong><br />
BAHRAIN
INTRODUCTION<br />
Bahra<strong>in</strong><br />
This study was conducted as part <strong>of</strong> an <strong>in</strong>itiative by the WHO Regional Office for the<br />
Eastern Mediterranean to assess the <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong><br />
<strong>sector</strong> performance <strong>in</strong> countries <strong>of</strong> the Eastern Mediterranean Region. <strong>The</strong> scope <strong>of</strong> this<br />
<strong>in</strong>itiative is to undertake exploratory case studies to document experience with outsourc<strong>in</strong>g <strong>of</strong><br />
publicly f<strong>in</strong>anced <strong>health</strong> services to private <strong>sector</strong> organization <strong>in</strong> those countries <strong>of</strong> the region<br />
that have a large private and/or nongovernmental organizations <strong>sector</strong>, and to assist <strong>in</strong><br />
develop<strong>in</strong>g a regional strategy on public private partnership <strong>in</strong> <strong>health</strong> <strong>in</strong> the Eastern<br />
Mediterranean Region. <strong>The</strong> specific objectives are: to assess the overall capacity for<br />
contract<strong>in</strong>g out <strong>health</strong> services to private <strong>sector</strong> <strong>in</strong> the country; to assess a project/programme<br />
<strong>in</strong> <strong>health</strong> that had taken up <strong>contractual</strong> arrangement as an implementation modality; to<br />
organize a national meet<strong>in</strong>g <strong>of</strong> the concerned stakeholders on <strong>contractual</strong> <strong>arrangements</strong> for<br />
improv<strong>in</strong>g the performance <strong>of</strong> the <strong>health</strong> <strong>sector</strong> and present the f<strong>in</strong>d<strong>in</strong>g <strong>of</strong> the study; and to<br />
participate <strong>in</strong> a regional meet<strong>in</strong>g on the subject to present the f<strong>in</strong>d<strong>in</strong>gs <strong>of</strong> the study.<br />
METHODOLOGY<br />
After an extensive review <strong>of</strong> the literature, two data collection tools were designed to<br />
facilitate assessment (one for overall country capacity, and the other for contract/agreement<br />
case study). <strong>The</strong> <strong>in</strong>formation was gathered by the follow<strong>in</strong>g approaches:<br />
Extensive review <strong>of</strong> available reliable documents, <strong>in</strong>clud<strong>in</strong>g:<br />
Related legislative decrees.<br />
Tender Central Board rules and regulations.<br />
Civil Service Bureau rules and regulations.<br />
M<strong>in</strong>istry <strong>of</strong> F<strong>in</strong>ance and National Economy rules and regulations.<br />
M<strong>in</strong>istry <strong>of</strong> Health rules and regulations.<br />
Contracts/agreements and related reports.<br />
Consultants reports (KPMG, International Monetary Fund and Arthur Anderson).<br />
K<strong>in</strong>g Hamad General Hospital Committee documents on Future privatization options<br />
and issues.<br />
Australian Hospital Design Group reports.<br />
Meet<strong>in</strong>g with concerned <strong>of</strong>ficials <strong>in</strong> the M<strong>in</strong>istry <strong>of</strong> Health Headquarter, Directorate <strong>of</strong> F<strong>in</strong>ance,<br />
Directorate <strong>of</strong> Medical Equipment, Directorate <strong>of</strong> Services and Salmania Medical<br />
Complex.<br />
Meet<strong>in</strong>g with concerned managers <strong>in</strong> private <strong>sector</strong>s (private hospitals and private companies).<br />
RESULTS AND DISCUSSION: OVERALL CAPACITY<br />
Internal factors affect<strong>in</strong>g capacity to contract<br />
Human resources<br />
Sufficient staff with appropriate skills are essential prerequisites for successful<br />
contract<strong>in</strong>g process. In particular, skilled staff are needed at the outset to identify potential<br />
50
Bahra<strong>in</strong><br />
services to be contracted-out, decid<strong>in</strong>g whether to undertake contract<strong>in</strong>g-out, and ensur<strong>in</strong>g<br />
high quality contract design.<br />
Identification <strong>of</strong> services to be contracted<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health currently does not contract out any <strong>of</strong> the cl<strong>in</strong>ical <strong>health</strong><br />
services; however, many <strong>of</strong> the support services (such as clean<strong>in</strong>g <strong>of</strong> facilities, ma<strong>in</strong>tenance <strong>of</strong><br />
medical and other equipment and <strong>in</strong>c<strong>in</strong>eration <strong>of</strong> medical waste) are contracted out to the<br />
private <strong>sector</strong>. <strong>The</strong> M<strong>in</strong>istry, jo<strong>in</strong>tly with M<strong>in</strong>istry <strong>of</strong> F<strong>in</strong>ance and National Economy and<br />
external consultants, is currently study<strong>in</strong>g the possibility <strong>of</strong> contract<strong>in</strong>g out cater<strong>in</strong>g and<br />
laundry services.<br />
Although previous contracted-out services were based on a partial analysis as an ad hoc<br />
solution to some problems, the M<strong>in</strong>istry <strong>of</strong> Health is currently study<strong>in</strong>g with the Australian<br />
Hospital Design Group (AHDG) the future privatization options and issues for the new K<strong>in</strong>g<br />
Hamad General Hospital (KHGH), which is at its f<strong>in</strong>al stage <strong>of</strong> design [1]. <strong>The</strong> AHDG<br />
concluded that the full or partial privatization <strong>of</strong> KHGH is possible on a number <strong>of</strong> levels<br />
<strong>in</strong>clud<strong>in</strong>g:<br />
Full or partial privatization <strong>of</strong> the operational management <strong>of</strong> the hospital.<br />
Privatization <strong>of</strong> various hospital cl<strong>in</strong>ical support services such as pathology and radiology.<br />
Privatization <strong>of</strong> any or all <strong>of</strong> the various general support services such as cater<strong>in</strong>g, clean<strong>in</strong>g,<br />
eng<strong>in</strong>eer<strong>in</strong>g, l<strong>in</strong>en services, security, car park<strong>in</strong>g.<br />
Consideration could be given to undertak<strong>in</strong>g a form <strong>of</strong> limited private practice which<br />
not only provides greater rewards to the best doctors and keeps them fully or predom<strong>in</strong>antly <strong>in</strong><br />
the public <strong>health</strong> system, but also <strong>of</strong>fers a greater range <strong>of</strong> medical skills to those Bahra<strong>in</strong>i<br />
citizens who choose to use the private system. Hospitals such as KHGH with a strong<br />
emphasis on a speciality such as women’s and children’s <strong>health</strong> have typically <strong>of</strong>fered greater<br />
opportunities for private practice development than general hospitals.<br />
Some <strong>of</strong> the rationales for the M<strong>in</strong>istry <strong>of</strong> Health to enter <strong>in</strong>to <strong>health</strong> services contracts<br />
with nongovernmental organizations or the private <strong>sector</strong> are given below:<br />
Cost effectiveness and improved efficiency.<br />
Reduced management work to allow it to focus on more important services.<br />
Better accountability.<br />
Develop<strong>in</strong>g the private <strong>sector</strong>.<br />
Utilization <strong>of</strong> economies <strong>of</strong> scale enjoyed by the contractor (ma<strong>in</strong>tenance <strong>of</strong> equipment).<br />
Avoid<strong>in</strong>g <strong>in</strong>vestment <strong>in</strong> expensive tools and diagnostic equipment.<br />
Access to highly skilled personnel (especially <strong>in</strong> <strong>in</strong>formation technology) without employ<strong>in</strong>g<br />
them.<br />
In the case <strong>of</strong> clean<strong>in</strong>g <strong>of</strong> hospitals, <strong>health</strong> centres and other facilities, the M<strong>in</strong>istry had<br />
experienced problems <strong>in</strong> supervis<strong>in</strong>g the clean<strong>in</strong>g <strong>of</strong> its facilities, which resulted <strong>in</strong><br />
51
Bahra<strong>in</strong><br />
deterioration <strong>in</strong> quality. With 20 <strong>health</strong> centres spread across the country, it was very difficult<br />
to closely supervise the clean<strong>in</strong>g without putt<strong>in</strong>g a foreman <strong>in</strong> each <strong>health</strong> centre. Absenteeism<br />
was another major factor which prompted the M<strong>in</strong>istry to look for contract<strong>in</strong>g alternatives. At<br />
the time when clean<strong>in</strong>g was contracted out, it was less expensive to use contractors, as they<br />
had access to the expatriate workforce. This has now changed as new regulations require<br />
contractors to employ only Bahra<strong>in</strong>is and to pay them a m<strong>in</strong>imum wage. This has resulted <strong>in</strong><br />
an enormous <strong>in</strong>crease <strong>in</strong> the contract cost (an <strong>in</strong>crease <strong>of</strong> between 150% and 200%).<br />
In the case <strong>of</strong> ma<strong>in</strong>tenance <strong>of</strong> equipment, the ma<strong>in</strong>tenance <strong>of</strong> highly specialized<br />
equipment is contracted out because the repair and ma<strong>in</strong>tenance requires expensive tools and<br />
s<strong>of</strong>tware and highly skilled personnel. Employ<strong>in</strong>g such personnel is not economical.<br />
Ma<strong>in</strong>tenance <strong>of</strong> computer networks, hardware and s<strong>of</strong>tware has also been contracted-out for<br />
similar reasons. Similarly, <strong>in</strong> the case <strong>of</strong> medical waste disposal, the old <strong>in</strong>c<strong>in</strong>erator needed<br />
replacement and the amount required for a new <strong>in</strong>c<strong>in</strong>erator was substantial. It was therefore<br />
decided to contract out this service. <strong>The</strong> M<strong>in</strong>istry has a 10-year contract.<br />
In the case <strong>of</strong> vehicles, the M<strong>in</strong>istry used to buy vehicles from the private <strong>sector</strong>.<br />
However, high ma<strong>in</strong>tenance and repair costs and frequent breakdowns resulted <strong>in</strong> the<br />
Government chang<strong>in</strong>g its policy. It was decided that all the M<strong>in</strong>istries would lease vehicles<br />
from the private <strong>sector</strong>. <strong>The</strong> contractor has to ma<strong>in</strong>ta<strong>in</strong> and service the vehicles and provide<br />
replacement vehicles when a vehicle is out <strong>of</strong> service. This has removed a significant f<strong>in</strong>ancial<br />
burden from the M<strong>in</strong>istry. <strong>The</strong> M<strong>in</strong>istry has secured better rates by <strong>of</strong>fer<strong>in</strong>g longer contracts.<br />
Quality <strong>of</strong> contract design<br />
Poorly specified contracts, particularly with respect to quality, were found <strong>in</strong> virtually<br />
all cases analysed <strong>in</strong> a 1998 study on contract<strong>in</strong>g <strong>in</strong> the <strong>health</strong> <strong>sector</strong> [2]. <strong>The</strong> various<br />
contracts signed by the M<strong>in</strong>istry <strong>of</strong> Health were generally designed very well and conta<strong>in</strong>ed<br />
standard and specific clauses <strong>in</strong> consultation with legal experts from the M<strong>in</strong>istry and F<strong>in</strong>ance<br />
and National Economy.<br />
Contract legal framework. <strong>The</strong> legal framework is quite strong and robust enough to facilitate<br />
contract<strong>in</strong>g between the public and private <strong>sector</strong>s. All the contracts conta<strong>in</strong> on the<br />
govern<strong>in</strong>g law and on arbitration clauses.<br />
“This agreement is made <strong>in</strong> Bahra<strong>in</strong> subject to the laws <strong>of</strong> Bahra<strong>in</strong>. All dates and<br />
periods mentioned <strong>in</strong> this agreement shall be reckoned accord<strong>in</strong>g to the Gregorian<br />
Calendar.”<br />
“All disputes and differences which may arise between the M<strong>in</strong>istry and the<br />
Contractor touch<strong>in</strong>g on the provisions <strong>of</strong> this agreement or any part there<strong>of</strong> or<br />
operation or construction there<strong>of</strong> or the rights or liabilities <strong>of</strong> the parties hereunder<br />
shall be amicably settled, but fail<strong>in</strong>g such amicable settlement shall be referred to<br />
arbitration to be held <strong>in</strong> Bahra<strong>in</strong> by one or more arbitrators agreed upon between the<br />
parties or appo<strong>in</strong>ted by the competent Court <strong>in</strong> Bahra<strong>in</strong> on the application <strong>of</strong> either<br />
party <strong>in</strong> case they fail to agree on such appo<strong>in</strong>tment. <strong>The</strong> award to be made by the<br />
arbitrator or arbitrators shall be f<strong>in</strong>al and b<strong>in</strong>d<strong>in</strong>g on the parties and the persons<br />
52
Bahra<strong>in</strong><br />
claim<strong>in</strong>g under them respectively and shall not be the subject <strong>of</strong> any objection or<br />
appeal by either party.”<br />
Dispute recourse. <strong>The</strong> contractor as well the M<strong>in</strong>istry can pursue the stipulated legal process <strong>in</strong><br />
case <strong>of</strong> dispute. Contracts conta<strong>in</strong> different mechanisms to recourse <strong>in</strong> the event <strong>of</strong> a<br />
dispute between the two contract<strong>in</strong>g partners. Arbitration is the preferred option and it is<br />
clearly stated <strong>in</strong> the contracts. Various laws are currently be<strong>in</strong>g reviewed by the<br />
Government to provide options to the parties to the contract. (Note: to be expanded after<br />
speak<strong>in</strong>g to legal experts).<br />
Implement<strong>in</strong>g sanctions and term<strong>in</strong>ation for non-performance or poor performance. Although<br />
the contracts were lack<strong>in</strong>g performance <strong>in</strong>dicators and quality assurance mechanisms,<br />
term and conditions for sanctions and term<strong>in</strong>ation <strong>of</strong> contract were clearly built <strong>in</strong> the<br />
contracts.<br />
Fair distribution <strong>of</strong> risks. Risks are fairly distributed between contractors and the M<strong>in</strong>istry <strong>of</strong><br />
Health <strong>in</strong> all contracts. <strong>The</strong> biggest risk for the M<strong>in</strong>istry is “contractor failure,” <strong>in</strong> which<br />
case there must be fallback options. Various dimensions <strong>of</strong> this risk relate to the type <strong>of</strong><br />
contract. Are the assets owned by the M<strong>in</strong>istry? Can the Government take over the<br />
operations without much dislocation? Who employs the staff? Is the service delivered<br />
from the M<strong>in</strong>istry’s premises?<br />
Contracts conta<strong>in</strong><strong>in</strong>g appropriate performance <strong>in</strong>centives. Although an appropriate performance<br />
<strong>in</strong>centive enhances contractors’ performance, none <strong>of</strong> the contracts <strong>in</strong>cluded such<br />
<strong>in</strong>centives. Sanctions are generally used to ensure a certa<strong>in</strong> level <strong>of</strong> performance <strong>of</strong> the<br />
contractors.<br />
Strategic functions/awareness <strong>of</strong> broader system-wide implications. S<strong>in</strong>ce all contracts were for<br />
non-cl<strong>in</strong>ical support services, there were no significant impacts on broader system-wide<br />
implications. All, except the contract for <strong>in</strong>c<strong>in</strong>eration for medical waste, were <strong>of</strong> short<br />
duration (two years). This is unlikely to place the <strong>in</strong>cumbent <strong>in</strong> a monopoly position for<br />
future contracts.<br />
Management and <strong>in</strong>formation system<br />
Adequate <strong>in</strong>formation systems are key to successful contract<strong>in</strong>g. <strong>The</strong>y help the<br />
contract<strong>in</strong>g agency to decide which services to contract, help ensure appropriate design and<br />
suitable <strong>in</strong>centives, and facilitate proper monitor<strong>in</strong>g <strong>of</strong> contracts.<br />
Cost and price analysis<br />
<strong>The</strong> public and private <strong>sector</strong>s are quite capable <strong>of</strong> undertak<strong>in</strong>g cost and price analysis<br />
for support services prior to negotiations. In some cases the public <strong>sector</strong> takes the help <strong>of</strong><br />
external consultants to advise it on these aspects. Traditionally, hospitals <strong>in</strong> countries such as<br />
Bahra<strong>in</strong> have been funded on an <strong>in</strong>put method based on what it will cost to operate the<br />
hospital/<strong>health</strong> centre for the com<strong>in</strong>g year, for example 20 million Bahra<strong>in</strong> d<strong>in</strong>ars (BHD) for<br />
salaries, BHD 5 million for medical supplies, ma<strong>in</strong>tenance and other supplies and so on. <strong>The</strong><br />
problem with this type <strong>of</strong> <strong>in</strong>put-based fund<strong>in</strong>g is that there are no <strong>in</strong>centives for efficiency and<br />
improvement. Indeed, the opposite effect <strong>of</strong>ten develops, <strong>in</strong> which the perception is that if<br />
53
Bahra<strong>in</strong><br />
allocations are not fully spent one year, less will be allocated the next year. Furthermore,<br />
rewards for <strong>in</strong>efficiency might predom<strong>in</strong>ate.<br />
Exist<strong>in</strong>g <strong>in</strong>formation systems (sources)<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health does not have comprehensive <strong>in</strong>formation system to<br />
dynamically compute costs <strong>of</strong> various services however it has adequate cost <strong>in</strong>formation for<br />
“make or buy” decisions. <strong>The</strong> new Bahra<strong>in</strong> Health Information System Project (BHIS)<br />
currently <strong>in</strong> its early stage <strong>of</strong> implementation will adopt some form <strong>of</strong> output or casemix<br />
method <strong>of</strong> payments based on predeterm<strong>in</strong>ed <strong>in</strong>dex <strong>of</strong> payment <strong>in</strong> its third and last phase<br />
(Bus<strong>in</strong>ess Intelligence) [3,4]. One group <strong>of</strong> products, for example, be<strong>in</strong>g discharged <strong>in</strong>patients<br />
classified <strong>in</strong>to diagnosis related groups (DRGs). By adopt<strong>in</strong>g this payment method <strong>health</strong><br />
services could (for some less complex services) be purchased <strong>in</strong> the private <strong>sector</strong> for public<br />
funded patients. This might not only help to better utilize private <strong>health</strong> <strong>sector</strong> capital stocks<br />
(currently underutilized <strong>in</strong> Bahra<strong>in</strong>), but also limit the amount <strong>of</strong> future public capital<br />
expenditure required for new bed stocks and should further <strong>in</strong>crease access to public funded<br />
<strong>health</strong> services <strong>in</strong> areas <strong>of</strong> need.<br />
Budgetary framework and f<strong>in</strong>ancial control mechanism<br />
<strong>The</strong> f<strong>in</strong>ancial system needs to provide <strong>in</strong>formation on the total budget for contract<strong>in</strong>g<br />
and on expenditure aga<strong>in</strong>st the budget. For clean<strong>in</strong>g and ma<strong>in</strong>tenance services, this will be<br />
relatively straightforward; however, for cl<strong>in</strong>ical services the requirements are more complex.<br />
Before decid<strong>in</strong>g to contract out, the M<strong>in</strong>istry studies the cost <strong>of</strong> provid<strong>in</strong>g the service <strong>in</strong>house.<br />
<strong>The</strong> costs are divided <strong>in</strong>to different categories such as manpower, materials, utilities<br />
and ma<strong>in</strong>tenance. <strong>The</strong> costs are further classified as direct and <strong>in</strong>direct costs. It is also<br />
determ<strong>in</strong>ed whether there are any costs that will still rema<strong>in</strong> (fixed overheads) if the service is<br />
contracted out. “Relevant cost” is then calculated, and compared with the expected cost <strong>of</strong><br />
contract<strong>in</strong>g out the service. While cost is a major factor, due consideration is also given to the<br />
opportunity to improve efficiency. If it is felt that efficiency will improve then the importance<br />
given to the cost factor is reduced.<br />
Performance <strong>in</strong>dicators for monitor<strong>in</strong>g quality<br />
A detailed set <strong>of</strong> contractor performance criteria, quality assurance and customer<br />
satisfaction standards needs to be put <strong>in</strong> place with regular surveys <strong>of</strong> customers via<br />
questionnaires and audits <strong>of</strong> contractor performance. This sort <strong>of</strong> quality assurance survey<strong>in</strong>g<br />
should be put <strong>in</strong> place for both <strong>in</strong>-house and external options but becomes especially critical<br />
when us<strong>in</strong>g an external contractor. <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health has established a Directorate <strong>of</strong><br />
Quality and <strong>in</strong>tends to implement a system <strong>of</strong> performance management, performance<br />
measurements/<strong>in</strong>dicators and performance evaluation/assessment. Although expected outputs<br />
are specified <strong>in</strong> the contracts, outcomes are not built <strong>in</strong>, and <strong>in</strong> some cases evaluation is<br />
cumbersome because <strong>of</strong> lack <strong>of</strong> detail.<br />
54
F<strong>in</strong>anc<strong>in</strong>g<br />
Bahra<strong>in</strong><br />
<strong>The</strong>re is a clear doubt whether the contracted services are a priority one. Despite the fact<br />
that clean<strong>in</strong>g and ma<strong>in</strong>tenance services are protected by the contracts, the hospital budget has<br />
not been severely cut. This gives the hospital flexibility to transfer funds from low-priority to<br />
high-priority areas. <strong>The</strong> contracted services are f<strong>in</strong>anced by the M<strong>in</strong>istry <strong>of</strong> Health regular<br />
budget. In many cases, as the cost <strong>of</strong> contracts goes up from year to year, it is easier to secure<br />
additional budget from the M<strong>in</strong>istry and F<strong>in</strong>ance and National Economy to cover the <strong>in</strong>crease,<br />
although additional justification has to be provided. <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health cont<strong>in</strong>ues to have<br />
the flexibility to manage its budget from the services provided <strong>in</strong>-house.<br />
Communication between task networks<br />
All parties at all levels are <strong>in</strong>volved at different stages <strong>of</strong> the process <strong>in</strong>clud<strong>in</strong>g<br />
concerned directorates <strong>in</strong> the M<strong>in</strong>istry <strong>of</strong> Health and concerned departments <strong>in</strong> the hospital.<br />
Furthermore various responsibilities for contract<strong>in</strong>g are assigned. This has meant that<br />
contracts are strongly specified and enforced and well implemented at the local level, where<br />
authority for monitor<strong>in</strong>g the contract exists.<br />
External factors affect<strong>in</strong>g capacity to contract<br />
Institutional context<br />
Bureaucratic structure<br />
<strong>The</strong> bureaucratic establishment supports contract<strong>in</strong>g out <strong>of</strong> services to the private <strong>sector</strong>.<br />
Long before the government announced the policy <strong>of</strong> privatization and contract<strong>in</strong>g out, the<br />
M<strong>in</strong>istry <strong>of</strong> Health proactively contracted out services like ma<strong>in</strong>tenance and clean<strong>in</strong>g. <strong>The</strong><br />
bureaucratic structure poses no h<strong>in</strong>drance to this process. On the contrary, it supports and<br />
encourages such <strong>in</strong>itiatives. <strong>The</strong>re are clear laws, rules, regulations and procedures. <strong>The</strong>se are<br />
quite transparent and provide sufficient opportunities for contract<strong>in</strong>g out. It should be noted,<br />
however, that any contract<strong>in</strong>g out requires prior approval <strong>of</strong> the Civil Service Bureau, because<br />
it <strong>in</strong>volves contract<strong>in</strong>g human resource services, as well as the Tender Board. <strong>The</strong> renewal <strong>of</strong><br />
such contracts must also be approved by both agencies. This procedure is well def<strong>in</strong>ed <strong>in</strong> the<br />
Standard F<strong>in</strong>ance Manual [5] and the Government Tender and Purchases law [6]. It appears<br />
that the exist<strong>in</strong>g Civil Service Bureau regulations do not prevent further contract<strong>in</strong>g out,<br />
although it might delay the overall contract<strong>in</strong>g process.<br />
Capabilities <strong>of</strong> the purchaser (M<strong>in</strong>istry <strong>of</strong> Health) for successful contracts<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health follows the national laws, rules and regulations for enter<strong>in</strong>g <strong>in</strong>to<br />
contracts. Any contract for a sum <strong>of</strong> BHD 10 000 (US$ 26 500) or more has to be tendered.<br />
Based on a set <strong>of</strong> tender specifications, the contractors submit their competitive bids <strong>in</strong> closed<br />
envelopes to the Tender Board. <strong>The</strong> bids are opened <strong>in</strong> public and handed over to the<br />
respective m<strong>in</strong>istry for evaluation. <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health has a separate department that<br />
deals with materials management (i.e. purchas<strong>in</strong>g, stor<strong>in</strong>g, distribut<strong>in</strong>g and contract<strong>in</strong>g). <strong>The</strong><br />
55
Bahra<strong>in</strong><br />
department is headed by a director. Other directors are also members <strong>of</strong> various tender<br />
evaluation committees, to br<strong>in</strong>g together expertise from different areas. In the case <strong>of</strong> major<br />
new contracts, the M<strong>in</strong>istry appo<strong>in</strong>ts outside consultants (such as KPMG, Arthur Anderson) to<br />
help it with the process <strong>of</strong> develop<strong>in</strong>g specifications, tender<strong>in</strong>g and evaluation. <strong>The</strong> M<strong>in</strong>istry<br />
and F<strong>in</strong>ance and National Economy has a dedicated section which looks after contract<strong>in</strong>g out.<br />
<strong>The</strong> assistance <strong>of</strong> this section is available as and when required. In study<strong>in</strong>g the possibility <strong>of</strong><br />
contract<strong>in</strong>g out cater<strong>in</strong>g and laundry services, the M<strong>in</strong>istry <strong>of</strong> Health has worked very closely<br />
with this section as well as external consultants. <strong>The</strong> M<strong>in</strong>istry has also been work<strong>in</strong>g on a<br />
major <strong>health</strong> <strong>in</strong>formation system project to contract out build<strong>in</strong>g and ma<strong>in</strong>tenance <strong>of</strong><br />
<strong>in</strong>formation systems for the M<strong>in</strong>istry. External consultants were appo<strong>in</strong>ted at <strong>in</strong>itial stages <strong>of</strong><br />
the project. Experts from the Central Informatics Organization and the F<strong>in</strong>ancial Information<br />
Directorate <strong>of</strong> the M<strong>in</strong>istry and F<strong>in</strong>ance and National Economy have shared their expertise <strong>in</strong><br />
this regard.<br />
After requisite approvals are received from the Tender Board for award<strong>in</strong>g the contract,<br />
the materials management department <strong>in</strong> coord<strong>in</strong>ation with the user department and F<strong>in</strong>ance<br />
Directorate prepares a draft contract. <strong>The</strong> M<strong>in</strong>istry and F<strong>in</strong>ance and National Economy<br />
provides standard contract formats; however, many contracts require specific provisions to be<br />
<strong>in</strong>serted. <strong>The</strong>se are negotiated with the proposed contractor <strong>in</strong> the presence <strong>of</strong> legal experts<br />
from the M<strong>in</strong>istry and F<strong>in</strong>ance and National Economy. <strong>The</strong> <strong>in</strong>terest <strong>of</strong> the government is<br />
looked after by the legal experts. <strong>The</strong> M<strong>in</strong>istry itself has limited expertise on legal matters.<br />
After necessary approvals, the contract is awarded.<br />
Monitor<strong>in</strong>g mechanisms and evaluation systems<br />
<strong>The</strong> standards <strong>of</strong> service expected from the contractor are specified <strong>in</strong> the contract. <strong>The</strong><br />
monitor<strong>in</strong>g depends on type <strong>of</strong> contract. For example, <strong>in</strong> a contract for ma<strong>in</strong>tenance <strong>of</strong><br />
computer equipment and a help desk, the monitor<strong>in</strong>g is on a day-to-day basis. <strong>The</strong> Health<br />
Information Directorate ensures that adequately qualified staff specified <strong>in</strong> the contract are<br />
provided to the M<strong>in</strong>istry. <strong>The</strong> curriculum vitae <strong>of</strong> various contract staff are sent to the<br />
M<strong>in</strong>istry <strong>in</strong> advance for evaluation and approval. In other cases, such as medical equipment<br />
ma<strong>in</strong>tenance, daily monitor<strong>in</strong>g is not appropriate as the technicians and eng<strong>in</strong>eers are not<br />
required to be present every day. However, the standards <strong>of</strong> service are stipulated <strong>in</strong> the<br />
contract. <strong>The</strong> service reports require authorization by the Medical Equipment Directorate<br />
before they can be accepted by Directorate <strong>of</strong> F<strong>in</strong>ance for payment. <strong>The</strong> Medical Equipment<br />
Directorate ensures that preventive service is carried out as scheduled. This Directorate also<br />
certifies whether the contractor has responded with<strong>in</strong> the stipulated time to the repair requests<br />
<strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health. In the case <strong>of</strong> clean<strong>in</strong>g contracts, the Directorate <strong>of</strong> Services<br />
ma<strong>in</strong>ta<strong>in</strong>s a log <strong>of</strong> service reports duly signed by the users. <strong>The</strong> users are asked to rate the<br />
service at the end <strong>of</strong> each month. <strong>The</strong> contractors are served notices if the service is not as per<br />
the contract and to the satisfaction <strong>of</strong> the user. <strong>The</strong> contractor is asked to improve the service<br />
with<strong>in</strong> a certa<strong>in</strong> number <strong>of</strong> days. Payment for contractors is based on monthly/quarterly<br />
<strong>in</strong>voices submitted by the contractors. <strong>The</strong> <strong>in</strong>voices must be certified by the respective<br />
directorates and then sent to the Directorate <strong>of</strong> F<strong>in</strong>ance for payment. <strong>The</strong> Directorate <strong>of</strong><br />
F<strong>in</strong>ance reviews the payment request and forwards it to the M<strong>in</strong>istry and F<strong>in</strong>ance and<br />
National Economy for payment. Most contracts allow 40 days for payment from the date <strong>of</strong><br />
56
Bahra<strong>in</strong><br />
receipt <strong>of</strong> the <strong>in</strong>voice. <strong>The</strong> payments are generally on time unless some <strong>of</strong> the documentation<br />
is miss<strong>in</strong>g. <strong>The</strong> performance <strong>of</strong> a contractor is taken <strong>in</strong>to account before renew<strong>in</strong>g any<br />
contract. Even when the contracts are re-tendered, prior poor performance can disqualify a<br />
contractor.<br />
Private <strong>sector</strong> <strong>in</strong>stitutional context<br />
<strong>The</strong> private <strong>sector</strong> is <strong>in</strong>terested <strong>in</strong> receiv<strong>in</strong>g public <strong>sector</strong> f<strong>in</strong>anc<strong>in</strong>g for the primary<br />
reason <strong>of</strong> a mak<strong>in</strong>g pr<strong>of</strong>it. Assured regular payment, stability <strong>of</strong> bus<strong>in</strong>ess, leverag<strong>in</strong>g the<br />
exist<strong>in</strong>g capital <strong>in</strong>vestment and creat<strong>in</strong>g economies <strong>of</strong> scale are some <strong>of</strong> the additional benefits<br />
which keep the private <strong>sector</strong> <strong>in</strong>terested <strong>in</strong> receiv<strong>in</strong>g public <strong>sector</strong> f<strong>in</strong>anc<strong>in</strong>g.<br />
<strong>The</strong> strengths and weaknesses <strong>of</strong> the provider that should be taken <strong>in</strong>to consideration<br />
when enter<strong>in</strong>g <strong>in</strong>to a <strong>contractual</strong> agreement depend on the type <strong>of</strong> contract. <strong>The</strong> size <strong>of</strong> the<br />
Bahra<strong>in</strong> market makes it difficult for the private <strong>sector</strong> to provide some <strong>of</strong> the services.<br />
Recent analysis by the KHGH Committee showed that the private <strong>sector</strong> can accommodate<br />
outsourc<strong>in</strong>g grounds, agriculture and transport services, but it cannot supply laundry and<br />
l<strong>in</strong>en, cater<strong>in</strong>g and dietary and housekeep<strong>in</strong>g services. However, <strong>in</strong>ternational and regional<br />
companies have expressed <strong>in</strong>terest <strong>in</strong> operat<strong>in</strong>g from Bahra<strong>in</strong>, and their <strong>in</strong>terest may <strong>in</strong>crease<br />
if the ma<strong>in</strong> hospital (Salmaniya Medical Complex) is <strong>in</strong>cluded <strong>in</strong> this outsourc<strong>in</strong>g.<br />
Economic factors<br />
It is doubtful that the Government <strong>of</strong> Bahra<strong>in</strong> <strong>in</strong> the future will be able to provide all <strong>of</strong><br />
the capital and recurrent resources for <strong>health</strong> services (without divert<strong>in</strong>g expenditure from<br />
other areas), or can <strong>in</strong>crease the tax base to be able to <strong>in</strong>crease the supply <strong>of</strong> public funded<br />
hospital beds to meet all possible needs. Consequently <strong>in</strong> order to limit the demands on<br />
government capital and recurrent hospital and <strong>health</strong> care expenditure, the private <strong>sector</strong> may<br />
play an <strong>in</strong>creas<strong>in</strong>g <strong>role</strong> <strong>in</strong> help<strong>in</strong>g to meet the future <strong>health</strong> care needs <strong>of</strong> the country,<br />
particularly <strong>in</strong> develop<strong>in</strong>g and br<strong>in</strong>g<strong>in</strong>g more hospital beds to the market.<br />
Political and social factors<br />
Government policy on contract<strong>in</strong>g<br />
Recogniz<strong>in</strong>g the persist<strong>in</strong>g budgetary deficit beg<strong>in</strong>n<strong>in</strong>g <strong>in</strong> the 1990s, the Government <strong>of</strong><br />
Bahra<strong>in</strong> <strong>in</strong>vited the International Monetary Fund (IMF) to undertake a comprehensive review<br />
<strong>of</strong> public f<strong>in</strong>ance <strong>in</strong> the country and to recommend reforms that would promote efficiency and<br />
economy <strong>in</strong> the government and suggest ways <strong>in</strong> which the reforms could be implemented.<br />
Based on the IMF report [7], the Cab<strong>in</strong>et <strong>of</strong> M<strong>in</strong>isters approved a memorandum on Public<br />
Expenditure Management Strategy (PEMSY), 1997–2006” <strong>in</strong> March 1996 [8]. <strong>The</strong> Cab<strong>in</strong>et<br />
memorandum envisaged that the <strong>role</strong> <strong>of</strong> the Government would gradually shift from that <strong>of</strong><br />
“control” to “direction” and that the public <strong>sector</strong> should create opportunities for added<br />
<strong>in</strong>vestment <strong>in</strong> the private <strong>sector</strong> so as to enhance employment generation, expand exports,<br />
improve the GDP, and accelerate economic growth.<br />
57
Bahra<strong>in</strong><br />
One <strong>of</strong> the components <strong>of</strong> PEMSY is contract<strong>in</strong>g out. <strong>The</strong> basic pr<strong>in</strong>ciple <strong>of</strong> this<br />
strategy is to divest the government <strong>of</strong> activities and services which could be provided by the<br />
private <strong>sector</strong> more competently and at lesser cost. This will not only result <strong>in</strong> sav<strong>in</strong>gs but will<br />
also enable the government to concentrate on more important and core areas <strong>of</strong> work. It will<br />
also contribute to the development <strong>of</strong> the private <strong>sector</strong>. Before decid<strong>in</strong>g to contract out an<br />
activity, the actual runn<strong>in</strong>g cost <strong>of</strong> the operation must be calculated by cost<strong>in</strong>g each and every<br />
component <strong>of</strong> the activity. In contract<strong>in</strong>g out, the activity is thrown open to the private <strong>sector</strong><br />
for market competition. <strong>The</strong> concept is similar to outsourc<strong>in</strong>g <strong>of</strong> goods and services, and is<br />
sometimes referred to as “strategic contract<strong>in</strong>g” to differentiate it from “market test<strong>in</strong>g or<br />
market orientation” under which the M<strong>in</strong>istry also competes with private <strong>sector</strong> bidders.<br />
Bahra<strong>in</strong> is a signatory to the World Trade Agreement and is negotiat<strong>in</strong>g the Free Trade<br />
Agreement with the United States <strong>of</strong> America. <strong>The</strong>se provide an easily accessible <strong>in</strong>vestment<br />
environment for some <strong>in</strong>ternational companies <strong>in</strong> the local market.<br />
Political environment<br />
<strong>The</strong> political environment is enabl<strong>in</strong>g for the execution <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong><br />
the <strong>health</strong> <strong>sector</strong> and it <strong>in</strong>fluences the negotiation and execution <strong>of</strong> contracts. A legislative<br />
decree (Government Tender and Purchase Law) was issued by the government October 2002<br />
mak<strong>in</strong>g privatization a part <strong>of</strong> the economic policy <strong>of</strong> Bahra<strong>in</strong> [9]. <strong>The</strong> International Monetary<br />
Fund, <strong>in</strong> a review report <strong>of</strong> public f<strong>in</strong>ance <strong>in</strong> Bahra<strong>in</strong>, clarified that privatization could be<br />
implemented <strong>in</strong> four directions:<br />
1) Transferr<strong>in</strong>g all commercial agencies to the private <strong>sector</strong>;<br />
2) Allow<strong>in</strong>g the private <strong>sector</strong> to operate all the new projects;<br />
3) Sell<strong>in</strong>g the government sharehold<strong>in</strong>gs to the private <strong>sector</strong>;<br />
4) Transferr<strong>in</strong>g to the private <strong>sector</strong> those activities which could be managed better by the<br />
private <strong>sector</strong>.<br />
<strong>The</strong> <strong>role</strong> <strong>of</strong> contract<strong>in</strong>g will be vital <strong>in</strong> the case <strong>of</strong> 1), 2) and 4) above. A clear <strong>in</strong>dication<br />
<strong>of</strong> the government’s resolve to transfer the services to the private <strong>sector</strong> is shown <strong>in</strong> the<br />
recently approved compulsory <strong>health</strong> <strong>in</strong>surance for expatriates <strong>in</strong> the country, <strong>in</strong> which it is<br />
proposed that <strong>health</strong> <strong>in</strong>surance will be provided by the private <strong>sector</strong>.<br />
<strong>The</strong> Government Tender and Purchases law is comprehensive and provides complete<br />
transparency. All the powers related to tender<strong>in</strong>g for purchase <strong>of</strong> goods and services (such as<br />
oversee<strong>in</strong>g tender transactions, endors<strong>in</strong>g technical specifications, receiv<strong>in</strong>g bids, approv<strong>in</strong>g<br />
and award<strong>in</strong>g bids) are vested <strong>in</strong> the <strong>in</strong>dependent Central Tender Board which reports directly<br />
to the Council <strong>of</strong> M<strong>in</strong>isters. Execution <strong>of</strong> the contracts is based on well written contracts. <strong>The</strong><br />
Standard F<strong>in</strong>ance Manual conta<strong>in</strong>s clear procedures with regard to management <strong>of</strong> contracts.<br />
<strong>The</strong> contract<strong>in</strong>g M<strong>in</strong>istry is authorized and accountable for the performance as per terms <strong>of</strong><br />
the contract. Sanctions are clearly def<strong>in</strong>ed <strong>in</strong> the contract for poor performance or nonperformance.<br />
<strong>The</strong> political environment does not <strong>in</strong>terfere with the process <strong>of</strong> contract<strong>in</strong>g and<br />
its execution. Adequate transparency is ma<strong>in</strong>ta<strong>in</strong>ed at each stage.<br />
58
Bahra<strong>in</strong><br />
RESULTS AND DISCUSSION: CASE STUDIES<br />
Description<br />
To better understand some <strong>of</strong> the practical issues with contract<strong>in</strong>g, the experience <strong>of</strong> two<br />
support service projects <strong>in</strong> the M<strong>in</strong>istry <strong>of</strong> Health that employed contract<strong>in</strong>g is described.<br />
<strong>The</strong>se projects were the contract<strong>in</strong>g out <strong>of</strong> medical equipment ma<strong>in</strong>tenance [10] and<br />
contract<strong>in</strong>g out <strong>of</strong> clean<strong>in</strong>g services [11] <strong>of</strong> Salmaniya Medical Complex. No contract<strong>in</strong>g<br />
projects for medical services were available to be <strong>in</strong>cluded <strong>in</strong> the review.<br />
Reasons for contract<strong>in</strong>g<br />
<strong>The</strong> reasons why the M<strong>in</strong>istry <strong>of</strong> Health contracted out medical equipment ma<strong>in</strong>tenance<br />
were: government policy <strong>of</strong> contract<strong>in</strong>g out non-core services and promot<strong>in</strong>g the <strong>role</strong> <strong>of</strong> the<br />
private <strong>sector</strong>; concentrate on core <strong>health</strong> services; provide efficient cost-effective services<br />
with better accountability; make use <strong>of</strong> economies <strong>of</strong> scale created by the contractor, avoid<br />
<strong>in</strong>vestment <strong>in</strong> spares and tools, <strong>in</strong>clud<strong>in</strong>g s<strong>of</strong>tware for advanced medical equipment; reduce<br />
“down” time due to breakdown <strong>of</strong> equipment; and reduce workforce and avoid recruit<strong>in</strong>g<br />
more personnel for ma<strong>in</strong>tenance <strong>of</strong> new equipment. Reasons why the contractor accepted to<br />
contract with the M<strong>in</strong>istry <strong>of</strong> Health for this service were: pr<strong>of</strong>it-mak<strong>in</strong>g; build<strong>in</strong>g economies<br />
<strong>of</strong> scale; build<strong>in</strong>g relationship with the M<strong>in</strong>istry <strong>of</strong> Health for other bus<strong>in</strong>ess, such as supply<br />
<strong>of</strong> medical equipment and pharmaceuticals; leverag<strong>in</strong>g relationships with the pr<strong>in</strong>cipals (i.e.<br />
manufacturers <strong>of</strong> the equipment); and better utilization <strong>of</strong> <strong>in</strong>puts which are required to meet<br />
warranty requirements for medical equipment supplied to various <strong>health</strong> facilities <strong>in</strong> Bahra<strong>in</strong><br />
(<strong>in</strong>clud<strong>in</strong>g M<strong>in</strong>istry <strong>of</strong> Health).<br />
Reasons why the M<strong>in</strong>istry <strong>of</strong> Health contracted out clean<strong>in</strong>g services were provid<strong>in</strong>g<br />
better quality <strong>of</strong> cost-effective services with better accountability; government policy <strong>of</strong><br />
contract<strong>in</strong>g out non-core services; concentrat<strong>in</strong>g on core <strong>health</strong> services; improv<strong>in</strong>g staff<br />
efficiency; reduc<strong>in</strong>g supervision requirements; avoid<strong>in</strong>g disruption <strong>of</strong> service due to<br />
absenteeism; and reduc<strong>in</strong>g workforce and avoid recruit<strong>in</strong>g more personnel for clean<strong>in</strong>g<br />
services. <strong>The</strong> reasons for contractors to provide this service were: pr<strong>of</strong>it-mak<strong>in</strong>g; build<strong>in</strong>g<br />
economies <strong>of</strong> scale; utilization <strong>of</strong> cheap foreign labour (this situation has now changed); better<br />
utilization <strong>of</strong> equipment, as it can be used across various contracts; and assured payment.<br />
Bidd<strong>in</strong>g and selection process<br />
<strong>The</strong> experience <strong>of</strong> contract<strong>in</strong>g equipment ma<strong>in</strong>tenance showed that the process <strong>of</strong> the<br />
specifications required for contract<strong>in</strong>g out this services started with review<strong>in</strong>g exist<strong>in</strong>g<br />
ma<strong>in</strong>tenance contracts and new equipment for which the warranty was expir<strong>in</strong>g out. After<br />
review, the M<strong>in</strong>istry <strong>of</strong> Health prepares tender specifications to enable bidders to submit their<br />
<strong>of</strong>fers. <strong>The</strong>se specifications are kept as general as possible. <strong>The</strong> specifications also conta<strong>in</strong><br />
requirements such as: response time (i.e. service/repair call must be responded with<strong>in</strong> a<br />
certa<strong>in</strong> time frame); the cost <strong>of</strong> spare parts required (<strong>in</strong> some cases major parts like X-Ray<br />
tubes are excluded from the specifications); presence <strong>of</strong> a qualified service eng<strong>in</strong>eer stationed<br />
59
Bahra<strong>in</strong><br />
<strong>in</strong> Bahra<strong>in</strong> or <strong>in</strong> the region to attend to calls; provision <strong>of</strong> replacement equipment <strong>in</strong> certa<strong>in</strong><br />
cases until the equipment is repaired; and carry<strong>in</strong>g out preventive service every quarter.<br />
Clarity <strong>of</strong> bidd<strong>in</strong>g and selection process<br />
<strong>The</strong> M<strong>in</strong>istry publishes the tender <strong>in</strong> local newspapers <strong>in</strong> both Arabic and English.<br />
Through this advertisement, the contractors are asked to collect tender documents (on<br />
payment <strong>of</strong> stipulated fee) from the M<strong>in</strong>istry. A clos<strong>in</strong>g date for submission <strong>of</strong> bids by the<br />
contractor is stated <strong>in</strong> the advertisement, which also gives the date and time <strong>of</strong> open<strong>in</strong>g the<br />
tender and <strong>in</strong>vites the contractors to attend the open<strong>in</strong>g <strong>of</strong> bids. <strong>The</strong> contractors can seek<br />
further <strong>in</strong>formation and clarification <strong>in</strong> writ<strong>in</strong>g. Responses to queries by any contractor are<br />
sent to all contractors who bought the tender documents.<br />
Contractor selection process<br />
After the advertisement is placed, the follow<strong>in</strong>g steps are taken.<br />
Bids are accepted <strong>in</strong> a sealed envelope at the M<strong>in</strong>istry and F<strong>in</strong>ance and National Economy and<br />
National Economy on behalf <strong>of</strong> the Tender Board until the clos<strong>in</strong>g date.<br />
<strong>The</strong> day after the clos<strong>in</strong>g date, the bids are opened by the Tender Board <strong>in</strong> the presence <strong>of</strong><br />
bidders.<br />
All the bids are listed on a display board show<strong>in</strong>g the price quoted by each bidder.<br />
Each page <strong>of</strong> these bids is stamped and punched with the Government logo so that no pages can<br />
be added later.<br />
All the bids are handed over to the contract<strong>in</strong>g M<strong>in</strong>istry, i.e. the M<strong>in</strong>istry <strong>of</strong> Health <strong>in</strong> this case,<br />
for evaluation.<br />
<strong>The</strong> bids are carefully studied by the Directorate <strong>of</strong> Medical Equipment for completeness and to<br />
determ<strong>in</strong>e whether the bids meet the M<strong>in</strong>istry <strong>of</strong> Health specifications.<br />
<strong>The</strong> f<strong>in</strong>d<strong>in</strong>gs are then presented to the Tender Evaluation Committee, which comprises members<br />
<strong>of</strong> the Directorate <strong>of</strong> F<strong>in</strong>ance, Directorate <strong>of</strong> Materials Management and Directorate <strong>of</strong><br />
Medical Equipment.<br />
<strong>The</strong> committee makes f<strong>in</strong>al recommendation for award <strong>of</strong> the contract to a bidder. Various<br />
factors considered by this committee <strong>in</strong>clude prices quoted, ability <strong>of</strong> the contractor to<br />
meet requirements, contractor’s past history <strong>of</strong> reliability, M<strong>in</strong>istry’s past experience with<br />
the contractor etc.<br />
<strong>The</strong> recommendation <strong>of</strong> the Tender Evaluation Committee is then sent to the M<strong>in</strong>ister <strong>of</strong> Health<br />
for approval. Once it is approved by the M<strong>in</strong>ister, the award <strong>of</strong> contract is sent to the<br />
Tender Board for their f<strong>in</strong>al approval. After receiv<strong>in</strong>g the approval from the Tender Board,<br />
the contract is awarded to the selected contractor.<br />
<strong>The</strong> contract is then signed between the M<strong>in</strong>istry and the contractor.<br />
<strong>The</strong> format <strong>of</strong> the contract is standard, as approved by the M<strong>in</strong>istry and F<strong>in</strong>ance and National<br />
Economy.<br />
In both case studies, the selection was based on bid price as well as on the quality <strong>of</strong><br />
technical proposal. No scor<strong>in</strong>g criteria were used for bidders’ proposals. Involvement <strong>of</strong> an<br />
expert third party (Tender Board) ensures transparency and fairness <strong>of</strong> the selection process.<br />
60
Bahra<strong>in</strong><br />
<strong>The</strong> competitive bidd<strong>in</strong>g process used was successful <strong>in</strong> keep<strong>in</strong>g the cost <strong>of</strong> the contracts low<br />
(controll<strong>in</strong>g bidd<strong>in</strong>g price).<br />
Contract management and implementation issues<br />
L<strong>in</strong>k<strong>in</strong>g contracts to tangible results<br />
Although detailed specifications and requirements were built <strong>in</strong>to the equipment<br />
ma<strong>in</strong>tenance contract, no tangible achievement outcomes were specified <strong>in</strong> either case study.<br />
<strong>The</strong>re was no performance bonus <strong>in</strong>cluded <strong>in</strong> the contracts which could motivate contractors<br />
to improve their outputs.<br />
Duration <strong>of</strong> contract<br />
Both contracts were <strong>of</strong> short duration (2 years), which will help avoid monopoly with<br />
regard to future contracts. However, <strong>in</strong> the <strong>contractual</strong> <strong>arrangements</strong> for <strong>in</strong>c<strong>in</strong>eration <strong>of</strong><br />
medical waste, a 10-year contract was signed because <strong>of</strong> the huge <strong>in</strong>vestment made by the<br />
contractor for equipment [12].<br />
Payment <strong>of</strong> contractors<br />
Delayed/slow payment to contractor is a serious risk and can easily lead to the<br />
breakdown <strong>of</strong> the contract<strong>in</strong>g process. Experience <strong>in</strong> the Bangladesh Integrated Nutrition<br />
Project showed that the delayed payment to contractor lead to the suspension <strong>of</strong> services for a<br />
few weeks. As a result <strong>of</strong> this issue some nongovernmental organizations decided not to<br />
participate <strong>in</strong> subsequent phases <strong>of</strong> the project [3]. In both case studies <strong>in</strong> Bahra<strong>in</strong>, one <strong>of</strong> the<br />
ma<strong>in</strong> motives for private for-pr<strong>of</strong>it organizations to participate <strong>in</strong> bidd<strong>in</strong>g process was the<br />
assurance <strong>of</strong> payment from the government. In the equipment ma<strong>in</strong>tenance contract the<br />
payment was made <strong>in</strong> regular quarterly <strong>in</strong>stalments <strong>in</strong> arrears, while under the clean<strong>in</strong>g<br />
services contract the payment was made monthly <strong>in</strong> arrears.<br />
Field supervision and monitor<strong>in</strong>g<br />
Field supervision was built up <strong>in</strong> both contracts. Monitor<strong>in</strong>g <strong>of</strong> contractor performance<br />
was carried out by contractor field supervisors. <strong>The</strong> equipment ma<strong>in</strong>tenance contract placed<br />
responsibility on the contractor to require their eng<strong>in</strong>eers/technicians to report to the<br />
respective department eng<strong>in</strong>eers <strong>in</strong> the Medical Equipment Directorate <strong>in</strong> all ma<strong>in</strong>tenance<br />
matters, but there was no clear mechanism for contactor performance monitor<strong>in</strong>g. It is<br />
relatively easy to monitor service quality for non-cl<strong>in</strong>ical services without a sophisticated<br />
<strong>in</strong>formation system. Although the outputs and standard <strong>of</strong> services expected from the<br />
contractors were specified <strong>in</strong> the contracts, no clear performance <strong>in</strong>dicators were built <strong>in</strong>to the<br />
contract.<br />
61
Type <strong>of</strong> disputes and ways <strong>of</strong> handl<strong>in</strong>g<br />
Bahra<strong>in</strong><br />
Disputes were clearly addressed <strong>in</strong> both contracts <strong>in</strong> the form <strong>of</strong> a step-wise mechanism<br />
for the settlement <strong>of</strong> disputes: amicable settlement, or arbitration to be held <strong>in</strong> Bahra<strong>in</strong> by one<br />
or more arbitrators agreed upon between the parties or appo<strong>in</strong>ted by the competent court. <strong>The</strong><br />
award made by the arbitrator/s is considered to be f<strong>in</strong>al.<br />
Sanctions and term<strong>in</strong>ation <strong>of</strong> contract<br />
Term and conditions for sanctions and term<strong>in</strong>ation <strong>of</strong> contract were built <strong>in</strong>to the<br />
contract. Giv<strong>in</strong>g the M<strong>in</strong>istry <strong>of</strong> Health the right <strong>of</strong> 90 days notice <strong>of</strong> term<strong>in</strong>ation without<br />
specify<strong>in</strong>g a reason <strong>in</strong> writ<strong>in</strong>g to the contractor has a serious drawback <strong>of</strong> los<strong>in</strong>g bidders’<br />
<strong>in</strong>terest and might lead to fewer bids <strong>in</strong> the future.<br />
REFERENCES<br />
1. Future privatisation options and issues. Manama, Australian Hospital Design Group<br />
(AHDG), M<strong>in</strong>istry <strong>of</strong> Health, April 2004.<br />
2. Bennett S, Mills A. Government capacity to contract: <strong>health</strong> <strong>sector</strong> experience and<br />
lessons. London, London School <strong>of</strong> Hygiene and Tropical Medic<strong>in</strong>e, Health Economics<br />
and F<strong>in</strong>anc<strong>in</strong>g Programme, 1998.<br />
3. Health <strong>in</strong>formation and communication technology strategy: <strong>health</strong> services without<br />
walls. Manama, Bahra<strong>in</strong>, M<strong>in</strong>istry <strong>of</strong> Health, Health Information Directorate, 2003.<br />
4. Bahra<strong>in</strong> <strong>health</strong> <strong>in</strong>formation system project. Manama, Bahra<strong>in</strong> M<strong>in</strong>istry <strong>of</strong> Health,<br />
Health Information Directorate.<br />
5. Standard f<strong>in</strong>ance manual. Manama, Bahra<strong>in</strong>, M<strong>in</strong>istry <strong>of</strong> F<strong>in</strong>ance, 1984.<br />
6. Government Tender and Purchases Law. Manama, K<strong>in</strong>gdom <strong>of</strong> Bahra<strong>in</strong>, April 2002.<br />
7. International Monetary Fund (IMF) Report. Manama, Bahra<strong>in</strong>.<br />
8. Mr. Sethumadhawan, Advisor to Budget Directorate. Public Expenditure Management<br />
Strategy (PEMSY) for 1997-2006. MOFNE, Manama, K<strong>in</strong>gdom <strong>of</strong> Bahra<strong>in</strong>, March<br />
1996.<br />
9. Legislation Decree no. 41 <strong>of</strong> 2002 with Respect to Policies and Guidel<strong>in</strong>es <strong>of</strong><br />
privatisation. Riffa Palace, K<strong>in</strong>gdom <strong>of</strong> Bahra<strong>in</strong>, 14 October 2002.<br />
10. Medical Equipment Ma<strong>in</strong>tenance Contract. Service Agreement no. 159/2003. Manama,<br />
M<strong>in</strong>istry <strong>of</strong> Health, 25 June 2003.<br />
62
Bahra<strong>in</strong><br />
11. SMC Clean<strong>in</strong>g Services Contract. Service Agreement No. 239/2003. Manama, M<strong>in</strong>istry<br />
<strong>of</strong> Health, 1 July 2003.<br />
12. Inc<strong>in</strong>eration <strong>of</strong> Medical Waste Contract. Service Agreement no. 106/2000. Manama,<br />
M<strong>in</strong>istry <strong>of</strong> Health, 26 September 2000.<br />
13. Loev<strong>in</strong>sohn B. Practical issues <strong>in</strong> contract<strong>in</strong>g for primary <strong>health</strong> care delivery: lessons<br />
from two large projects <strong>in</strong> Bangladesh. Wash<strong>in</strong>gton DC, <strong>The</strong> Word Bank, 1996.<br />
FURTHER READING<br />
Abramson W. Partnerships between the public <strong>sector</strong> and non-governmental organizations:<br />
contract<strong>in</strong>g for primary <strong>health</strong> care services, a state practice paper – an analysis <strong>of</strong><br />
contract<strong>in</strong>g primary <strong>health</strong> care services to NGOs <strong>in</strong> five Lat<strong>in</strong> American and Caribbean<br />
countries. Lat<strong>in</strong> American and Caribbean Health Sector Reform (LACHSR), Primer for<br />
Policymakers. Bethesda, Maryland, Partnership for Health Reform (PHR) Resource Center,<br />
Abt Associates Inc., August 1999.<br />
Barr D. Research protocol to evaluate the effectiveness <strong>of</strong> public private partnership <strong>in</strong><br />
enhanc<strong>in</strong>g <strong>health</strong> and welfare system development. Palo Alto, California, Stanford University<br />
Center for Health Policy Institute for International Studies, February 2004.<br />
Jack W. Contract<strong>in</strong>g for <strong>health</strong> services: an evaluation <strong>of</strong> recent reforms <strong>in</strong> Nicaragua. Health<br />
policy and plann<strong>in</strong>g, 2003, 18(2): 195–204.<br />
McPake B. et al. Is the Colombian <strong>health</strong> system reform improv<strong>in</strong>g the performance <strong>of</strong> public<br />
hospital <strong>in</strong> Bogota. Health policy and plann<strong>in</strong>g, 2003, 18(2): 182–94.<br />
Public private partnership policy: achiev<strong>in</strong>g value for money <strong>in</strong> public <strong>in</strong>frastructure and<br />
service delivery. Brisbane, Department <strong>of</strong> State Development, Queensland Government, 21<br />
November 2003.<br />
Webb R, Pulle B. Public private partnerships: an <strong>in</strong>troduction. Canberra, Australia,<br />
Department <strong>of</strong> the Parliamentary Library, September 2002 (Research Paper No. 1 2002–03).<br />
63
Egypt<br />
EGYPT
INTRODUCTION<br />
Egypt<br />
<strong>The</strong> <strong>health</strong> <strong>sector</strong> reform programme established the Family Health Fund to act as the<br />
ma<strong>in</strong> contract<strong>in</strong>g and purchas<strong>in</strong>g agency for quality <strong>health</strong> care services on behalf <strong>of</strong> the<br />
beneficiaries, the population <strong>of</strong> Egypt, with the follow<strong>in</strong>g objectives:<br />
• to separate service f<strong>in</strong>ance from service provision, which will ensure both high-quality<br />
service and competition between service providers to contract with the fund on equal<br />
criteria based upon quality <strong>of</strong> service.<br />
• to act as an agent and contractor to purchase <strong>health</strong> services for families (both under<br />
social <strong>in</strong>surance and non-<strong>in</strong>sured <strong>in</strong>dividuals) through <strong>health</strong> units (Public, NGO and<br />
Private).<br />
• to ensure susta<strong>in</strong>ability <strong>of</strong> f<strong>in</strong>ance.<br />
• to act as the precursor to the National Health Insurance Fund.<br />
<strong>The</strong> Family Health Fund is a f<strong>in</strong>ancially <strong>in</strong>dependent body established as a pilot<br />
f<strong>in</strong>anc<strong>in</strong>g and <strong>in</strong>surance unit to put <strong>in</strong>to effect the separation between service provision and<br />
f<strong>in</strong>ance. Its policy and strategy were developed by the M<strong>in</strong>istry <strong>of</strong> Health and Population and<br />
it is be<strong>in</strong>g implemented as technical support and projects <strong>in</strong> the current phase. This phase is<br />
pend<strong>in</strong>g forthcom<strong>in</strong>g legislation and establishment <strong>of</strong> the National Family Health Insurance<br />
Fund as a national goal to be gradually realized progressively, <strong>in</strong> conformity with the strategic<br />
plan for <strong>health</strong> <strong>sector</strong> reform.<br />
<strong>The</strong> Family Health Fund is permitted to contract with a wide range <strong>of</strong> public and private<br />
providers. <strong>The</strong> ma<strong>in</strong> <strong>role</strong> <strong>of</strong> the Fund is to purchase curative and preventive primary <strong>health</strong><br />
care to be extended to secondary care <strong>in</strong> the future. <strong>The</strong> process takes place by contract<strong>in</strong>g<br />
<strong>health</strong> service providers <strong>in</strong> both governmental and nongovernmental <strong>sector</strong>s through current<br />
and future <strong>health</strong> care provision organizations designated for all family members <strong>in</strong> the<br />
community, with<strong>in</strong> the framework <strong>of</strong> recognized quality standards. Thus, it is actually pav<strong>in</strong>g<br />
the way for competition and availability.<br />
<strong>The</strong> Fund applies necessary f<strong>in</strong>ance mechanisms to collect and disburse resources <strong>in</strong> a<br />
cost effective manner with<strong>in</strong> the framework <strong>of</strong> regulations, legislation and the Constitution.<br />
Currently the Fund is contracted directly with public and nongovernmental organization<br />
<strong>health</strong> facilities. <strong>The</strong> Family Health Fund also has several contracts with the District Provider<br />
Organizations <strong>in</strong> which the latter provide a def<strong>in</strong>ed packages <strong>of</strong> services to the district<br />
population. This is achieved through public, private and nongovernmental organization<br />
providers accord<strong>in</strong>g to the national standards <strong>of</strong> quality and with agreed upon prices subject to<br />
monitor<strong>in</strong>g and evaluation mechanisms.<br />
Includ<strong>in</strong>g the private and nongovernmental organization <strong>sector</strong>s <strong>in</strong> the programme adds<br />
a significant dimension, compared with work<strong>in</strong>g only with the M<strong>in</strong>istry <strong>of</strong> Health and<br />
Population facilities. Improv<strong>in</strong>g the quality <strong>of</strong> <strong>health</strong> services dur<strong>in</strong>g the implementation <strong>of</strong><br />
the module is the first priority for the M<strong>in</strong>istry facilities, followed by the cost and revenue <strong>of</strong><br />
services. Typically, private and nongovernmental organizations facilities put cost and revenue<br />
65
Egypt<br />
as the top priority. Tak<strong>in</strong>g this difference <strong>in</strong> consideration, it is a challenge to use the same<br />
model <strong>of</strong> the family physician concept and standards <strong>of</strong> quality to be implemented <strong>in</strong> private<br />
and nongovernmental organization <strong>health</strong> facilities.<br />
Current contracts <strong>of</strong> the Family Health Fund with private and nongovernmental<br />
organization providers present a great opportunity for the M<strong>in</strong>istry <strong>of</strong> Health and Population<br />
towards the development <strong>of</strong> effective partnership for the <strong>health</strong> <strong>sector</strong> reform programme.<br />
Deploy<strong>in</strong>g the same monitor<strong>in</strong>g and evaluation <strong>in</strong>dicators used with the public <strong>sector</strong> should<br />
allow fair competition between the two <strong>sector</strong>s.<br />
<strong>The</strong> scope <strong>of</strong> this study is to document the experience <strong>of</strong> M<strong>in</strong>istry <strong>of</strong> Health and<br />
Population through the <strong>health</strong> <strong>sector</strong> reform programme <strong>in</strong> contract<strong>in</strong>g with the private and<br />
nongovernmental organization <strong>sector</strong>s to provide packaged <strong>health</strong> services.<br />
<strong>The</strong> study focuses on assess<strong>in</strong>g the overall capacity for contract<strong>in</strong>g out <strong>health</strong> services to<br />
the private/nongovernmental organization <strong>sector</strong>, and assess<strong>in</strong>g the Family Health Fund,<br />
which has taken up <strong>contractual</strong> <strong>arrangements</strong> as an implementation modality.<br />
BACKGROUND<br />
Providers<br />
Health services <strong>in</strong> Egypt are currently managed, f<strong>in</strong>anced and provided by agencies <strong>in</strong><br />
various <strong>sector</strong>s <strong>of</strong> the government under different laws, operat<strong>in</strong>g with variable levels <strong>of</strong><br />
<strong>in</strong>dependence. <strong>The</strong>y are also <strong>of</strong>fered by private providers <strong>of</strong> variable categories and at<br />
<strong>in</strong>consistent levels <strong>of</strong> <strong>in</strong>tervention with variable quality standards.<br />
Public governmental <strong>sector</strong><br />
<strong>The</strong> public governmental <strong>sector</strong> represents the activities <strong>of</strong> m<strong>in</strong>istries that receive funds<br />
from the M<strong>in</strong>istry <strong>of</strong> F<strong>in</strong>ance. Government <strong>health</strong> services <strong>in</strong> Egypt are organized as an<br />
<strong>in</strong>tegrated delivery system <strong>in</strong> which the f<strong>in</strong>anc<strong>in</strong>g and provider functions are subsumed under<br />
the same organizational structure. This means that government providers receiv<strong>in</strong>g budgetary<br />
support from the government general revenues (M<strong>in</strong>istry <strong>of</strong> F<strong>in</strong>ance) are also subject to the<br />
adm<strong>in</strong>istrative rules and regulations that govern all civil service organizations.<br />
Public <strong>in</strong>stitutional <strong>sector</strong><br />
<strong>The</strong> public <strong>in</strong>stitutional <strong>sector</strong> comprises parastatal, or quasi-governmental,<br />
organizations <strong>in</strong> which government m<strong>in</strong>istries have a controll<strong>in</strong>g share <strong>of</strong> decision-mak<strong>in</strong>g.<br />
<strong>The</strong>se <strong>in</strong>clude the Health Insurance Organization, Curative Care Organization, and other<br />
public <strong>sector</strong> organizations provid<strong>in</strong>g ma<strong>in</strong>ly hospital services.<br />
Though a dist<strong>in</strong>ction between the government <strong>sector</strong> and the parastatal or quasigovernmental<br />
<strong>sector</strong> is usually made when describ<strong>in</strong>g the Egyptian <strong>health</strong> <strong>sector</strong>, both <strong>sector</strong>s<br />
are <strong>in</strong> practice run by the state. From an operational and a f<strong>in</strong>ancial perspective, the parastatals<br />
66
Egypt<br />
are governed by their own set <strong>of</strong> rules and regulations, have separate budgets, and exercise<br />
more autonomy <strong>in</strong> daily operations. However, from a political perspective, the M<strong>in</strong>istry <strong>of</strong><br />
Health and Population has a controll<strong>in</strong>g share <strong>of</strong> decision-mak<strong>in</strong>g <strong>in</strong> parastatal organizations.<br />
Private <strong>sector</strong><br />
Private <strong>sector</strong> provision <strong>of</strong> services <strong>in</strong>cludes for-pr<strong>of</strong>it and non-pr<strong>of</strong>it organizations and<br />
covers everyth<strong>in</strong>g, <strong>in</strong>clud<strong>in</strong>g traditional midwives, private pharmacies, private doctors and<br />
private hospitals <strong>of</strong> all sizes. Also <strong>in</strong> this <strong>sector</strong> are a large number <strong>of</strong> nongovernmental<br />
organizations provid<strong>in</strong>g services, <strong>in</strong>clud<strong>in</strong>g religiously affiliated cl<strong>in</strong>ics and other charitable<br />
organizations, all <strong>of</strong> which are registered with the M<strong>in</strong>istry <strong>of</strong> Health and Population as well<br />
as the M<strong>in</strong>istry <strong>of</strong> Social Affairs.<br />
<strong>The</strong>re is another category <strong>of</strong> <strong>health</strong> care providers belong<strong>in</strong>g to pr<strong>of</strong>essional syndicates.<br />
Most <strong>of</strong> these are operat<strong>in</strong>g through an <strong>in</strong>surance scheme consist<strong>in</strong>g <strong>of</strong> a per-capita fee<br />
comb<strong>in</strong>ed with co-payments from beneficiaries, and their services are subject to a restricted<br />
range <strong>of</strong> <strong>in</strong>clusions as well as a ceil<strong>in</strong>g level <strong>of</strong> cost per contract period.<br />
Private facilities<br />
After the declaration <strong>of</strong> an open economic policy <strong>in</strong> 1974, the private <strong>health</strong> <strong>sector</strong><br />
began to grow. Between 1975 and 1990, the total number <strong>of</strong> private beds grew significantly.<br />
Private care providers <strong>in</strong> Egypt range from large modern hospitals to smaller hospitals, day<br />
care centres, polycl<strong>in</strong>ics and <strong>in</strong>dividual cl<strong>in</strong>ics.<br />
Religious cl<strong>in</strong>ics operated by religious social agencies, a predom<strong>in</strong>ant type <strong>of</strong><br />
nongovernmental organization, are perceived to be popular and successful providers <strong>of</strong><br />
ambulatory <strong>health</strong> care <strong>in</strong> Egypt.<br />
Nongovernmental organizations for <strong>health</strong> services are <strong>in</strong>creas<strong>in</strong>gly localized <strong>in</strong> the<br />
larger prov<strong>in</strong>cial cities, particularly those governorate capitals with medical universities and<br />
teach<strong>in</strong>g hospitals. Those <strong>in</strong> metropolitan Cairo are known for their quality medical care,<br />
thriv<strong>in</strong>g on low-cost services that are readily accessible to low-<strong>in</strong>come households. <strong>The</strong>se are<br />
mostly staffed by senior to mid-level university medical staff.<br />
Recently, nongovernmental organizations have started to hire university consultants and<br />
to <strong>in</strong>troduce modern technology. This situation not only <strong>in</strong>creases their power and<br />
participation <strong>in</strong> the <strong>health</strong> care system, but also enhances access and the will<strong>in</strong>gness <strong>of</strong> the<br />
population to utilize their facilities.<br />
Nongovernmental organization <strong>health</strong> care providers rarely <strong>of</strong>fer <strong>health</strong> education,<br />
provide public <strong>in</strong>formation and awareness campaigns, conduct <strong>health</strong> outreach to their<br />
patients and communities or promote preventive care.<br />
67
Egypt<br />
<strong>The</strong> nongovernmental organization <strong>health</strong> <strong>sector</strong> is f<strong>in</strong>ancially self-support<strong>in</strong>g through<br />
user fees. Overall, the nongovernmental organization <strong>sector</strong> receives only a very small<br />
share—just 1%––<strong>of</strong> <strong>health</strong> care expenditure <strong>in</strong> Egypt.<br />
<strong>The</strong> nongovernmental organization <strong>health</strong> <strong>sector</strong>’s overall contribution to <strong>health</strong> care<br />
across Egypt is marg<strong>in</strong>al when measured objectively aga<strong>in</strong>st the share <strong>of</strong> <strong>health</strong> care<br />
expenditure that goes to private physicians, pharmacies and public-<strong>sector</strong> and university<br />
hospitals.<br />
Private providers<br />
At present there is very little organized f<strong>in</strong>anc<strong>in</strong>g <strong>of</strong> the private <strong>health</strong> services.<br />
Most <strong>of</strong> the transactions occur as household out-<strong>of</strong>-pocket payments to the provider on a<br />
fee-for-service basis for both ambulatory and <strong>in</strong>patient care. <strong>The</strong>re is no formal mechanism <strong>in</strong><br />
place to monitor and evaluate the rates be<strong>in</strong>g charged and the quality <strong>of</strong> the <strong>health</strong> care service<br />
<strong>of</strong>fered by different categories <strong>of</strong> private providers, although the Medical Syndicate may have<br />
some <strong>in</strong>formation on medical fees charged by member physicians.<br />
On a very limited scale, private firms and private <strong>in</strong>surance companies enter <strong>in</strong>to<br />
<strong>contractual</strong> <strong>arrangements</strong> with private providers. With the proposed expansion <strong>of</strong> the Family<br />
Health Fund over the com<strong>in</strong>g years, it is expected that an <strong>in</strong>creas<strong>in</strong>g number <strong>of</strong> private<br />
providers will enter <strong>in</strong>to provider–payer arrangement.<br />
<strong>The</strong> number <strong>of</strong> <strong>health</strong> service providers jo<strong>in</strong><strong>in</strong>g the nongovernmental organization <strong>sector</strong><br />
with<strong>in</strong> the few past years has <strong>in</strong>creased dramatically as a result <strong>of</strong> socioeconomic pressures.<br />
Some <strong>of</strong> the factors related to this phenomenon are attributed to certa<strong>in</strong> characteristics <strong>of</strong> this<br />
<strong>sector</strong>:<br />
<strong>The</strong>re are no strict rules or regulations govern<strong>in</strong>g this <strong>sector</strong>.<br />
Nongovernmental organizations are tax exempt.<br />
It is considered an attractive <strong>sector</strong> for physicians who are not capable <strong>of</strong> f<strong>in</strong>anc<strong>in</strong>g their private<br />
practice.<br />
It is considered an alternative <strong>sector</strong> for <strong>in</strong>dividuals and bus<strong>in</strong>essmen to enhance their reputation<br />
by the donations they provide.<br />
<strong>The</strong> Health Sector Reform Programme<br />
In early 1996, the M<strong>in</strong>istry <strong>of</strong> Health and Population <strong>in</strong>itiated an assessment <strong>of</strong> the<br />
<strong>health</strong> <strong>sector</strong> situation and recognized a need to explore alternatives for a comprehensive<br />
reform. As a result <strong>of</strong> these discussions, the government adopted a <strong>health</strong> <strong>sector</strong> reform<br />
programme (HSRP) which lays out a framework for undertak<strong>in</strong>g comprehensive reform <strong>of</strong> the<br />
<strong>health</strong> <strong>sector</strong> over the medium and long term.<br />
68
Egypt<br />
One <strong>of</strong> the key objectives <strong>of</strong> the HSRP is to achieve universal <strong>in</strong>surance coverage for all<br />
Egyptians. In addition to the reform and expansion <strong>of</strong> the social <strong>health</strong> <strong>in</strong>surance functions,<br />
the HSRP <strong>in</strong>cludes the follow<strong>in</strong>g objectives.<br />
Redef<strong>in</strong><strong>in</strong>g the <strong>role</strong> <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health and Population to develop its regulatory functions,<br />
notably to establish quality norms and standards, to establish a mechanism <strong>of</strong><br />
accreditation and licensure to enforce those standards, and to consolidate the multiple<br />
vertical public <strong>health</strong> programmes.<br />
Strengthen<strong>in</strong>g the programme for tra<strong>in</strong><strong>in</strong>g and retra<strong>in</strong><strong>in</strong>g <strong>of</strong> family <strong>health</strong> care doctors, nurses<br />
and allied <strong>health</strong> pr<strong>of</strong>essionals, with greater emphasis on preventive <strong>health</strong> care.<br />
Decentraliz<strong>in</strong>g management <strong>of</strong> government <strong>health</strong> delivery system to the governorate and<br />
district level, and <strong>in</strong>troduc<strong>in</strong>g greater managerial autonomy at the facility level.<br />
Rationalization <strong>of</strong> the public <strong>in</strong>vestment <strong>in</strong> <strong>health</strong> <strong>in</strong>frastructure and <strong>health</strong> workforce based on<br />
governorate and district <strong>health</strong> plans that identify the actual needs and the availability <strong>of</strong><br />
resources to susta<strong>in</strong> the <strong>in</strong>vestments.<br />
<strong>The</strong> first phase <strong>of</strong> the HSRP was developed as a programme jo<strong>in</strong>tly f<strong>in</strong>anced by the<br />
Government <strong>of</strong> Egypt, World Bank, European Union and Unites States Agency for<br />
International Development. In 2000, the African Development Bank jo<strong>in</strong>ed the f<strong>in</strong>ancial<br />
stakeholders <strong>of</strong> the programme.<br />
DISCUSSION<br />
What is the rationale for the M<strong>in</strong>istry <strong>of</strong> Health and Population to enter <strong>in</strong>to <strong>health</strong><br />
services contracts with nongovernmental organizations or private <strong>sector</strong> providers?<br />
<strong>The</strong> ma<strong>in</strong> goal <strong>of</strong> the <strong>health</strong> <strong>sector</strong> reform programme is to support the <strong>health</strong> system<br />
that assures universal coverage <strong>of</strong> the population with a pre-def<strong>in</strong>ed package <strong>of</strong> <strong>health</strong><br />
services based on universality, equity, affordability, and susta<strong>in</strong>ability.<br />
<strong>The</strong> public <strong>sector</strong> <strong>in</strong> Egypt cannot provide all <strong>health</strong> care services because <strong>of</strong> the<br />
cont<strong>in</strong>uous <strong>in</strong>crease <strong>of</strong> <strong>health</strong> services cost. <strong>The</strong> <strong>in</strong>tention is to provide a hybrid model <strong>of</strong> both<br />
public and private <strong>sector</strong> provision. <strong>The</strong> aim is to encourage private <strong>sector</strong> <strong>in</strong>vestment where<br />
the local market conditions make it susta<strong>in</strong>able.<br />
<strong>The</strong> <strong>health</strong> <strong>sector</strong> reform programme, through the pilot governorate’s master plans, is<br />
prepar<strong>in</strong>g to cover 35%–40% <strong>of</strong> the urban population through the M<strong>in</strong>istry <strong>of</strong> Health and<br />
Population <strong>health</strong> services, while the rest will be covered by private or nongovernmental<br />
organization providers. Partnership with these providers will give the opportunity for HSRP to<br />
enable the coverage <strong>of</strong> underserved areas with the family <strong>health</strong> model and basic benefits<br />
package.<br />
Hav<strong>in</strong>g a contract with the private <strong>sector</strong> will help ma<strong>in</strong>ta<strong>in</strong> national quality standards<br />
among different types <strong>of</strong> <strong>health</strong> service providers. <strong>The</strong>se standards are be<strong>in</strong>g implemented <strong>in</strong><br />
the <strong>health</strong> <strong>sector</strong> reform programme pilot sites. This will provide an equity dimension for both<br />
public and private <strong>sector</strong> patients.<br />
69
Egypt<br />
<strong>The</strong> <strong>health</strong> <strong>sector</strong> reform programme organized a provider survey and several focus<br />
groups for nongovernmental organization providers to assess the size <strong>of</strong> their market. <strong>The</strong><br />
follow<strong>in</strong>g is a summary <strong>of</strong> f<strong>in</strong>d<strong>in</strong>gs, which <strong>in</strong>dicate a recent <strong>in</strong>crease <strong>in</strong> the magnitude <strong>of</strong><br />
nongovernmental organization work.<br />
Nongovernmental organizations serve a wide rage <strong>of</strong> beneficiaries, mostly at the low and mid<br />
socioeconomic levels, which represent the majority <strong>of</strong> the population.<br />
Well-tra<strong>in</strong>ed university pr<strong>of</strong>essors <strong>in</strong>creas<strong>in</strong>gly jo<strong>in</strong> the nongovernmental organization <strong>sector</strong>.<br />
Nongovernmental organizations are based on a non-pr<strong>of</strong>it concept, which gives more trust <strong>in</strong><br />
deal<strong>in</strong>g with population versus the private <strong>sector</strong> target<strong>in</strong>g to pr<strong>of</strong>it.<br />
Several nongovernmental organizations have <strong>in</strong>troduced the diagnostic services technology<br />
<strong>in</strong>clud<strong>in</strong>g MRI, CATscan and ultrasonography, result<strong>in</strong>g <strong>in</strong> an <strong>in</strong>crease <strong>in</strong> the utilization<br />
rate.<br />
Most nongovernmental organizations receive donations, which ma<strong>in</strong>ta<strong>in</strong> their f<strong>in</strong>ancial<br />
susta<strong>in</strong>ability.<br />
What is the <strong>in</strong>terest <strong>of</strong> nongovernmental organizations/private <strong>sector</strong> <strong>in</strong> receiv<strong>in</strong>g public<br />
<strong>sector</strong> f<strong>in</strong>anc<strong>in</strong>g?<br />
Accord<strong>in</strong>g to the District Provider Organization approach, all district populations have<br />
to be covered with the family <strong>health</strong> model. <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health and Population primary<br />
<strong>health</strong> care facilities cover only a percentage <strong>of</strong> this population; nongovernmental<br />
organization and private facilities will cover the rema<strong>in</strong><strong>in</strong>g population. Montazah Health<br />
District <strong>in</strong> Alexandria Governorate, with a population <strong>of</strong> 1 million, is a good example for such<br />
approach, <strong>in</strong> which the M<strong>in</strong>istry facilities will cover 35%–40% <strong>of</strong> the population, and private<br />
and nongovernmental organization facilities will cover 60%–75% <strong>of</strong> the population.<br />
Contract<strong>in</strong>g with private cl<strong>in</strong>ics will guarantee the registration <strong>of</strong> a number <strong>of</strong> families<br />
to the cl<strong>in</strong>ics based on the size <strong>of</strong> the facility. Refus<strong>in</strong>g the contract<strong>in</strong>g issue will waste a<br />
chance for the private/nongovernmental organization to have a pool <strong>of</strong> families <strong>in</strong> its<br />
catchment area.<br />
Does the political environment enable/disable the execution <strong>of</strong> such <strong>contractual</strong><br />
<strong>arrangements</strong>?<br />
<strong>The</strong> approach <strong>of</strong> the District Provider Organization with<strong>in</strong> the <strong>health</strong> <strong>sector</strong> reform<br />
programme’s long-term objectives is to encourage <strong>contractual</strong> <strong>arrangements</strong> between the<br />
M<strong>in</strong>istry <strong>of</strong> Health and Population and the private <strong>sector</strong>. <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health and<br />
Population carried out several studies assess<strong>in</strong>g: the capacity <strong>of</strong> private <strong>sector</strong> services,<br />
<strong>in</strong>clud<strong>in</strong>g mosque and church cl<strong>in</strong>ics; the Family Heath Fund contract<strong>in</strong>g strategy, and SWOT<br />
(strengths, opportunities, weaknesses, threats) analysis for private–public partnership. <strong>The</strong><br />
M<strong>in</strong>istry has highlighted on several occasions the urgent need for partnership between the<br />
public and private <strong>sector</strong>s, and m<strong>in</strong>isterial decrees have been issued to emphasize the <strong>role</strong> <strong>of</strong><br />
the Family Health Fund <strong>in</strong> support<strong>in</strong>g <strong>contractual</strong> <strong>arrangements</strong> with private and<br />
nongovernmental organization providers.<br />
70
Egypt<br />
Is the legal framework robust enough to facilitate contract<strong>in</strong>g between the public and<br />
private <strong>sector</strong>s?<br />
<strong>The</strong> Family Health Fund was established accord<strong>in</strong>g to M<strong>in</strong>isterial decree no. 294 <strong>of</strong><br />
1999. <strong>The</strong> Decree acknowledged open<strong>in</strong>g a bank account named “Family Health Fund <strong>of</strong> the<br />
Health Sector Reform Programme”. This Decree was followed by M<strong>in</strong>isterial decree no. 160<br />
<strong>of</strong> 2001 regard<strong>in</strong>g the constituency <strong>of</strong> the govern<strong>in</strong>g bodies <strong>of</strong> the Fund, which laid the basis<br />
for management <strong>of</strong> this account and its responsibilities.<br />
M<strong>in</strong>isterial decree no. 109 determ<strong>in</strong>ed the organizational structure <strong>of</strong> the Family Health<br />
Fund at the central and peripheral levels, as well as its organigram, f<strong>in</strong>ancial and<br />
adm<strong>in</strong>istrative system and sources <strong>of</strong> revenue and expenditures. <strong>The</strong> decree gives legal<br />
support for contract<strong>in</strong>g with private and nongovernmental organization providers.<br />
What is the nature <strong>of</strong> the public <strong>sector</strong> organization that is outsourc<strong>in</strong>g its services?<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health and Population has firm policies to enhance the level <strong>of</strong> <strong>health</strong><br />
care for all Egyptians <strong>in</strong> cities, villages and rural areas. <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health and Population<br />
aims to extend <strong>health</strong> <strong>in</strong>surance to all citizens and for all public categories. It also aims to<br />
distribute <strong>health</strong> services fairly, <strong>in</strong> addition to present<strong>in</strong>g the services with<strong>in</strong> a quality<br />
framework and with the participation <strong>of</strong> the community to achieve maximum effectiveness.<br />
To accomplish this, it is important to separate the service provision from its f<strong>in</strong>ance.<br />
Separation <strong>of</strong> these functions ensures that the level <strong>of</strong> <strong>health</strong> services can be upgraded and<br />
<strong>of</strong>fered accord<strong>in</strong>g to quality standards.<br />
With this <strong>in</strong> m<strong>in</strong>d, the M<strong>in</strong>istry <strong>of</strong> Health and Population decide to create a body<br />
responsible to f<strong>in</strong>ance <strong>health</strong> services and make agreements with all those provid<strong>in</strong>g these<br />
services, <strong>in</strong>clud<strong>in</strong>g the private <strong>sector</strong> and nongovernmental organizations. It was also decided<br />
to apply the family physician system at all levels. In 1999, an account, the “Family Health<br />
Fund”, was established by the M<strong>in</strong>istry <strong>of</strong> Health and Population decree no. 294.<br />
What are the f<strong>in</strong>anc<strong>in</strong>g sources <strong>of</strong> the Family Health Fund?<br />
In order for the Family Health Fund to perform its function, legislation had to be put<br />
<strong>in</strong>to place to organize the Fund activities. <strong>The</strong> sources <strong>of</strong> f<strong>in</strong>anc<strong>in</strong>g were identified through the<br />
M<strong>in</strong>istry <strong>of</strong> Health and Population decree no. 160 for 2001.<br />
Revenues that result from all contracted bodies <strong>in</strong>clud<strong>in</strong>g the Health Insurance Organization<br />
with its branches and the <strong>health</strong> affairs directorates <strong>in</strong> the governorates.<br />
Amounts given by the M<strong>in</strong>istry <strong>of</strong> Health and Population to support the Fund’s budget for the<br />
performance <strong>of</strong> its tasks and commitments to execute the <strong>health</strong> reform programme.<br />
Other donations and grants <strong>of</strong>fered by different organizations.<br />
Amounts given by the M<strong>in</strong>istry <strong>of</strong> F<strong>in</strong>ance to support the Fund’s account.<br />
71
Egypt<br />
Later legislation (M<strong>in</strong>isterial decree no. 147) added another source <strong>of</strong> funds through the<br />
adoption <strong>of</strong> a co-payment system, <strong>in</strong> which the beneficiaries (at M<strong>in</strong>istry <strong>of</strong> Health and<br />
Population <strong>health</strong> facilities) share <strong>in</strong> cover<strong>in</strong>g the cost <strong>of</strong> service provision.<br />
What is the capacity <strong>of</strong> the purchaser (Family Health Fund) <strong>in</strong> order to successfully<br />
enter <strong>in</strong>to a contract?<br />
To augment the capacity <strong>of</strong> the Family Health Fund <strong>in</strong> terms <strong>of</strong> monitor<strong>in</strong>g and<br />
supervision and regulation and payment mechanisms, each <strong>of</strong> the five pilot governorates,<br />
Alexandria, Menoufia, Sohag, Suez and M<strong>in</strong>ya, created six <strong>in</strong>ternal units affiliated with Fund.<br />
<strong>The</strong>se have the technical capacity to follow up with contract<strong>in</strong>g procedures and their<br />
implementation. <strong>The</strong>se units are the: Policy and Plann<strong>in</strong>g Unit; Monitor<strong>in</strong>g and Evaluation<br />
Unit; Information System Unit; the Contract<strong>in</strong>g and Quality Unit; F<strong>in</strong>ance, Adm<strong>in</strong>istration<br />
and Legal Unit; and Information, Education and Communication Unit.<br />
What types <strong>of</strong> contract does the Family Health Fund have?<br />
At present, the Family Health Fund has two types <strong>of</strong> work<strong>in</strong>g contract, per-capita and<br />
fee-for-service.<br />
What are the strengths/weaknesses <strong>of</strong> the Family Health Fund that should be taken <strong>in</strong>to<br />
consideration when enter<strong>in</strong>g <strong>in</strong>to a <strong>contractual</strong> agreement?<br />
<strong>The</strong> Family Health Fund is a s<strong>in</strong>gle purchaser on behalf <strong>of</strong> the district population. This<br />
strengthens its position <strong>in</strong> <strong>contractual</strong> agreements with the private <strong>sector</strong>. However, it is still a<br />
new concept, and one to which private and nongovernmental organization providers may be<br />
hesitant to commit. As well, the <strong>contractual</strong> requirement <strong>of</strong> follow<strong>in</strong>g quality standards, is<br />
costly and may limit the number <strong>of</strong> private or nongovernmental organization providers will<strong>in</strong>g<br />
to accept such a commitment.<br />
What are the strengths/weaknesses <strong>of</strong> the provider taken <strong>in</strong>to consideration when<br />
enter<strong>in</strong>g <strong>in</strong>to a <strong>contractual</strong> agreement?<br />
<strong>The</strong> private/nongovernmental organization <strong>sector</strong> has a very strong negotiat<strong>in</strong>g position,<br />
as it controls most <strong>of</strong> the outpatient services (more than 80% <strong>in</strong> Egypt). However, it is likely<br />
that the patient will prefer to go to public <strong>health</strong> services as long as they provide good quality<br />
service at a lower price. This will create strong competition for the private local facility and<br />
weaken the negotiation power <strong>of</strong> private and nongovernmental organization providers.<br />
What risks and <strong>in</strong>centives does each party <strong>in</strong>cur when enter<strong>in</strong>g <strong>in</strong>to a contract?<br />
<strong>The</strong>re are risks for the Family Health Fund <strong>in</strong> the case <strong>of</strong> a contract term<strong>in</strong>ation. In this<br />
case, the assigned population must be moved to other providers, who might <strong>in</strong>sist on higher<br />
cost <strong>of</strong> services. Incentives for the Family Health Fund to contract with private and<br />
nongovernmental organization providers <strong>in</strong>clude:<br />
72
Egypt<br />
<strong>The</strong> opportunity for the HSRP to enable the coverage <strong>of</strong> the underserved areas with family<br />
<strong>health</strong> model and basic benefits package.<br />
Unification <strong>of</strong> all <strong>health</strong> services under one system.<br />
Dissem<strong>in</strong>ation <strong>of</strong> quality concepts among different types <strong>of</strong> <strong>health</strong> service providers.<br />
It is beneficial for the M<strong>in</strong>istry <strong>of</strong> Health and Population to have private<br />
nongovernmental organization providers to provide <strong>health</strong> services. This approach removes an<br />
enormous burden from the M<strong>in</strong>istry, <strong>in</strong>clud<strong>in</strong>g the cost <strong>of</strong> <strong>in</strong>frastructure and management, and<br />
overhead costs.<br />
A risk for the private and nongovernmental organization providers is pursu<strong>in</strong>g facility<br />
accreditation, which is a costly procedure. Failure to ma<strong>in</strong>ta<strong>in</strong> the contract could lead to the<br />
loss <strong>of</strong> the <strong>in</strong>vestment without any returns. <strong>The</strong> <strong>in</strong>centive for such facilities is the guaranteed<br />
number <strong>of</strong> families <strong>in</strong> their catchment area.<br />
What is the payment mechanism <strong>of</strong> the contract with private nongovernmental<br />
organization, and to what extent does it promote efficiency, equity and quality?<br />
<strong>The</strong> percentage <strong>of</strong> <strong>in</strong>centives is determ<strong>in</strong>ed based on the monthly performance <strong>of</strong> the<br />
<strong>health</strong> team whose performance is appraised through a set <strong>of</strong> performance <strong>in</strong>dicators. <strong>The</strong>se<br />
cover all aspects <strong>of</strong> service provision, whether curative or preventive, and reflect the<br />
efficiency and quality. <strong>The</strong>re are eleven performance <strong>in</strong>dicators, each with a target standard as<br />
shown <strong>in</strong> Table 1.<br />
<strong>The</strong> performance <strong>in</strong>dicators are divided <strong>in</strong>to two ma<strong>in</strong> categories accord<strong>in</strong>g to their<br />
importance:<br />
<strong>The</strong> first category comprises those <strong>in</strong>dicators with the “all or none” rule, which means that if the<br />
facility fails to achieve the targeted standard for these <strong>in</strong>dicators, no <strong>in</strong>centive will be<br />
paid, e.g. family plann<strong>in</strong>g, immunization, antenatal care and drug rationalization.<br />
<strong>The</strong> second category comprises <strong>in</strong>dicators with second priority, where the facility receives only<br />
half <strong>of</strong> the amount <strong>of</strong> <strong>in</strong>centives allocated for these <strong>in</strong>dicators if it fails to achieve the<br />
targeted standards, e.g. referral rate, complet<strong>in</strong>g medical records, number <strong>of</strong> visits per day,<br />
and patient wait<strong>in</strong>g time.<br />
73
Table 1. Performance <strong>in</strong>dicators<br />
Egypt<br />
Serial Indicator Target standard<br />
1. Number <strong>of</strong> visits/day 20–48<br />
2. Number <strong>of</strong> drugs per visit < 2<br />
3. Referral rate 1%–8%<br />
4. Completion <strong>of</strong> visit encounter forms Over 98%<br />
5. Patient satisfaction rate Over 90%<br />
6. Completion <strong>of</strong> medical records data Over 90%<br />
7. Family plann<strong>in</strong>g (protection years) Over 50%<br />
8. Immunization 95%<br />
9. Patient wait<strong>in</strong>g time < 20 m<strong>in</strong>utes<br />
10. Antenatal care (visit/pregnant woman) Over ½ visit per month<br />
11. Follow<strong>in</strong>g medical protocols Over 98%<br />
Do all performance <strong>in</strong>dicators have the same weight?<br />
Each performance <strong>in</strong>dicator has a certa<strong>in</strong> “weight” accord<strong>in</strong>g to its importance, which<br />
serves to encourage the providers to give more attention to <strong>in</strong>dicators that have nationwide<br />
impact, such as family plann<strong>in</strong>g and immunization. <strong>The</strong> weights are as follows.<br />
Family plann<strong>in</strong>g (35%)<br />
Immunization (35%)<br />
Drug rationalization (30%)<br />
Patient satisfaction (30%)<br />
Referral rate (30%)<br />
Number <strong>of</strong> visits per day (30%)<br />
Patient wait<strong>in</strong>g time (20%)<br />
Completion <strong>of</strong> encounter form (20%)<br />
Completion <strong>of</strong> registration (20%)<br />
How would performance <strong>in</strong>dicators ma<strong>in</strong>ta<strong>in</strong> the equity for private/nongovernmental<br />
organization patient and M<strong>in</strong>istry <strong>of</strong> Health and Population patients?<br />
<strong>The</strong> performance <strong>in</strong>dicators are used at the primary <strong>health</strong> facilities <strong>in</strong> the pilot<br />
governorates to evaluate the staff for the monthly <strong>in</strong>centive. <strong>The</strong> HSRP is strongly <strong>in</strong>terested<br />
<strong>in</strong> us<strong>in</strong>g the same <strong>in</strong>dicators <strong>in</strong> both private and public facilities to ma<strong>in</strong>ta<strong>in</strong> equity for the<br />
public <strong>health</strong> facility patient and the private or nongovernmental organization <strong>health</strong> facility<br />
patient.<br />
Is the Family Health Fund capable <strong>of</strong> undertak<strong>in</strong>g a cost and price analysis prior to<br />
negotiations?<br />
Through the Research Unit at the Family Health Fund, several studies have been<br />
conducted to estimate the cost <strong>of</strong> services per visit and the average number <strong>of</strong> visit per family.<br />
74
Egypt<br />
<strong>The</strong> Research Unit <strong>in</strong>cludes Family Health Fund staff and groups <strong>of</strong> university staff <strong>in</strong><br />
addition to short-term and long-term consultants from HSRP donors. <strong>The</strong> unit has focused its<br />
activities on the issues affect<strong>in</strong>g the implementation <strong>of</strong> the reform, <strong>in</strong>clud<strong>in</strong>g changes that<br />
could be reflected <strong>in</strong> the purchas<strong>in</strong>g activities <strong>of</strong> the Family Health Fund, provider, patient<br />
perspective, cost and quality management. Results <strong>of</strong> these studies are available dur<strong>in</strong>g the<br />
negotiations with private and nongovernmental organization providers.<br />
Which <strong>in</strong>formation systems are used by FHF to carry out the contract and assess<br />
performance <strong>of</strong> the contract<strong>in</strong>g private agency?<br />
<strong>The</strong> National Information Centre <strong>of</strong> Health and Population at the M<strong>in</strong>istry <strong>of</strong> Health and<br />
Population has designed the Patient-Based System (PBS) application, which requires a local<br />
area network with a m<strong>in</strong>imum <strong>of</strong> three workstations, one <strong>in</strong> each <strong>of</strong> the follow<strong>in</strong>g: registration<br />
and fil<strong>in</strong>g room, family physician cl<strong>in</strong>ic and pharmacy.<br />
Sources <strong>of</strong> data for the PBS are the various forms enclosed <strong>in</strong> the family folder. <strong>The</strong><br />
ma<strong>in</strong> areas <strong>in</strong>clude but are not limited to:<br />
essential family data<br />
house status description<br />
patient demographic data<br />
encounter visits data<br />
family plann<strong>in</strong>g visits<br />
antenatal care visits<br />
neonatal follow-up data<br />
<strong>in</strong>fants vacc<strong>in</strong>ation data<br />
all pharmacy and drug store transactions data.<br />
<strong>The</strong> system is extremely flexible and easily adapted to the conditions and needs <strong>of</strong> each<br />
facility. This is achieved through flexible setup menus for all ma<strong>in</strong> variables with<strong>in</strong> the<br />
system.<br />
<strong>The</strong> system produces weekly reports that conta<strong>in</strong> the follow<strong>in</strong>g data: number <strong>of</strong> visits<br />
per physician; number <strong>of</strong> visits by age group; list <strong>of</strong> prescribed drugs; number <strong>of</strong> cases for a<br />
specific diagnosis; number <strong>of</strong> laboratory <strong>in</strong>vestigations; number <strong>of</strong> X-ray <strong>in</strong>vestigations; and<br />
number <strong>of</strong> referral cases.<br />
BPS provides the Family Health Fund with all data needed to evaluate the performance<br />
<strong>of</strong> <strong>health</strong> facilities. <strong>The</strong> system undergoes a cont<strong>in</strong>uous upgrad<strong>in</strong>g process accord<strong>in</strong>g to<br />
experience and feedback from field implementation.<br />
What monitor<strong>in</strong>g mechanisms and evaluation systems are <strong>in</strong> place for the Family Health<br />
Fund and what challenges exist <strong>in</strong> this area?<br />
Us<strong>in</strong>g the same monitor<strong>in</strong>g and evaluation <strong>in</strong>dicators <strong>in</strong> both the public and private<br />
<strong>sector</strong>s allows fair competition between the two <strong>sector</strong>s and presents challenges <strong>in</strong> <strong>contractual</strong><br />
<strong>arrangements</strong>.<br />
75
Egypt<br />
<strong>The</strong> Monitor<strong>in</strong>g and Evaluation Unit at the Family Health Fund employs skilled and<br />
experienced staff to achieve the unit objectives, which <strong>in</strong>clude:<br />
Ensur<strong>in</strong>g the accuracy <strong>of</strong> data regard<strong>in</strong>g the performance status <strong>of</strong> the contracted facilities.<br />
Identify<strong>in</strong>g the obstacles to performance <strong>in</strong> the contracted facilities, work<strong>in</strong>g out their resolution<br />
and tra<strong>in</strong><strong>in</strong>g the staff <strong>in</strong> these facilities to prevent recurrence <strong>of</strong> the obstacles <strong>in</strong> the future.<br />
Ensur<strong>in</strong>g the application <strong>of</strong> the required performance standards and study<strong>in</strong>g the capabilities <strong>of</strong><br />
the contracted facilities to perform <strong>health</strong> services accord<strong>in</strong>g to the pre-set and agreedupon<br />
quality standards.<br />
Coord<strong>in</strong>at<strong>in</strong>g with the Policies and Plann<strong>in</strong>g Unit <strong>of</strong> the Family Health Fund to update the<br />
performance standards as necessary to improve the quality <strong>of</strong> <strong>health</strong> services delivered at<br />
the contracted facilities.<br />
Internal periodical monitor<strong>in</strong>g <strong>of</strong> the Fund’s operation to support and assist the adm<strong>in</strong>istration <strong>in</strong><br />
ensur<strong>in</strong>g effectiveness and compliance to the pre-set plans (quarterly).<br />
Who is the purchaser and who is the provider?<br />
<strong>The</strong> Family Heath Fund represents the purchas<strong>in</strong>g agent, on behalf <strong>of</strong> the population<br />
that lives <strong>in</strong> the <strong>health</strong> district. <strong>The</strong> providers <strong>in</strong>clude private cl<strong>in</strong>ics and polycl<strong>in</strong>ics,<br />
university cl<strong>in</strong>ics and religiously-affiliated nongovernmental organizations.<br />
<strong>The</strong>re are two approaches to sign<strong>in</strong>g the contract, which is a one-year renewable<br />
contract.<br />
For providers located <strong>in</strong> districts and work<strong>in</strong>g under the District Provider Organization (DPO)<br />
approach, the Family Health Fund signs the contract with the DPO, where the latter has a<br />
service level agreement with the provider.<br />
For providers located <strong>in</strong> districts but not work<strong>in</strong>g under the DPO approach, the Family Health<br />
Fund signs the contract directly with the provider.<br />
What is the basis <strong>of</strong> disbursement from the Fund account?<br />
<strong>The</strong> <strong>in</strong>ternal rules and regulations <strong>of</strong> the Family Health Fund control the disbursements<br />
from the Fund account.<br />
<strong>The</strong> Fund signs contracts with governmental and nongovernmental <strong>health</strong> <strong>in</strong>stitutions to buy<br />
<strong>health</strong> care services. However, these <strong>in</strong>stitutions must fulfil the conditions and standards<br />
<strong>of</strong> accreditation determ<strong>in</strong>ed by the M<strong>in</strong>istry <strong>of</strong> Health and Population.<br />
<strong>The</strong> Fund pays a monthly <strong>in</strong>centive to the bodies it contracts with, the <strong>health</strong> service providers,<br />
depend<strong>in</strong>g on the performance rates required.<br />
<strong>The</strong> Fund will be committed to cover its managerial and operat<strong>in</strong>g expenses.<br />
<strong>The</strong> Fund manager can <strong>in</strong>vest any excess funds through the Fund’s f<strong>in</strong>ancial department.<br />
76
Egypt<br />
How was the nongovernmental organization or private provider selected? How<br />
transparent was the entire selection process?<br />
Selection <strong>of</strong> a private or nongovernmental organization provider as a pilot needs to pass<br />
through several steps. <strong>The</strong> follow<strong>in</strong>g is a summary <strong>of</strong> the steps.<br />
Select a <strong>health</strong> district. It is preferable to select the district with the lowest number <strong>of</strong> HSRP<br />
<strong>health</strong> facilities to be the pilot district. This is because private and nongovernmental<br />
organization facilities cannot reduce their prices to compete with HSRP <strong>health</strong> facilities,<br />
which provide services with a high level <strong>of</strong> quality. Thus it could be futile for them to jo<strong>in</strong><br />
the reform programme s<strong>in</strong>ce they will be immediately out <strong>of</strong> the competition. For this<br />
reason, it is advisable to start the first contact with private nongovernmental organization<br />
providers <strong>in</strong> a district that has not yet started the implementation <strong>of</strong> the programme.<br />
List all <strong>in</strong>terested private and nongovernmental organization facilities. <strong>The</strong> Governorate Health<br />
Directorate have lists <strong>of</strong> all active privates and nongovernmental organization facilities<br />
sorted by district. <strong>The</strong> selection process starts by send<strong>in</strong>g the facilities a copy <strong>of</strong> the<br />
Manual for Contract<strong>in</strong>g with Non Public Organizations. <strong>The</strong> manual is designed by the<br />
Quality Improvement Department at M<strong>in</strong>istry <strong>of</strong> Health and Population <strong>in</strong> coord<strong>in</strong>ation<br />
with Family Health Fund. <strong>The</strong> manual <strong>in</strong>cludes summary <strong>of</strong> the HSRP and the family<br />
<strong>health</strong> model, steps for contract<strong>in</strong>g with the Fund, criteria for <strong>health</strong> facility selection,<br />
quality improvement <strong>in</strong>dicators, scor<strong>in</strong>g system and a model contract.<br />
Request feedback from these facilities <strong>in</strong> order to limit the number <strong>of</strong> field visits.<br />
Conduct field visits. <strong>The</strong> objectives <strong>of</strong> field visits to the facilities that have sent positive<br />
responses, are ma<strong>in</strong>ly for prelim<strong>in</strong>ary assessment to decide if the sites meet the quality<br />
standards. Hence, it is quite beneficial to have a member <strong>of</strong> the quality improvement team<br />
<strong>in</strong> these visits. It is also advisable to meet the director <strong>of</strong> the facility and evaluate the<br />
management capacity. <strong>The</strong> facilities will usually fall <strong>in</strong>to one <strong>of</strong> the follow<strong>in</strong>g patterns:<br />
− facilities that need major renovation such as equipment and furniture to meet the<br />
quality standards and are not will<strong>in</strong>g to undertake such expenses and changes.<br />
− facilities that are will<strong>in</strong>g to stage the needs to meet the quality standards.<br />
− Facilities that are ultimately unwill<strong>in</strong>g to accept the new model.<br />
Develop a score for each facility based on the criteria for selection. Accord<strong>in</strong>g to this score, the<br />
selection decision will be taken.<br />
Does the Family Health Fund play a <strong>role</strong> <strong>in</strong> the market<strong>in</strong>g and communication with the<br />
community?<br />
<strong>The</strong> Family Health Fund plays a major <strong>role</strong> <strong>in</strong> communication and rais<strong>in</strong>g awareness<br />
about the HSRP among both service providers and beneficiaries. This <strong>in</strong>cludes rais<strong>in</strong>g<br />
awareness <strong>of</strong> the family medic<strong>in</strong>e concept and its potential for alleviat<strong>in</strong>g <strong>health</strong> and f<strong>in</strong>ancial<br />
burdens from citizens, especially the poor. <strong>The</strong> Family Health Fund coord<strong>in</strong>ates <strong>in</strong> produc<strong>in</strong>g<br />
brochures and other materials for the mass media, advertisement and social market<strong>in</strong>g <strong>of</strong> the<br />
HSRP.<br />
77
Egypt<br />
How are the issues <strong>of</strong> expected services, monitor<strong>in</strong>g and evaluation, performance<br />
assessment, transfer <strong>of</strong> funds, and settlement <strong>of</strong> disputes addressed <strong>in</strong> the contract?<br />
Expected services are addressed <strong>in</strong> item 5 <strong>of</strong> the contract: “<strong>The</strong> primary <strong>health</strong> care services<br />
delivered by Second Party to <strong>in</strong>dividuals related to First Party <strong>in</strong>clude services def<strong>in</strong>ed by<br />
the Primary Health Care Services basic benefit package, and clarified <strong>in</strong> the attached<br />
schedule except immunization services which are carried out through the related <strong>health</strong><br />
<strong>of</strong>fice. Second Party is committed to deliver all data <strong>of</strong> the <strong>in</strong>dividuals who will take<br />
immunization.”<br />
Monitor<strong>in</strong>g and evaluation are addressed <strong>in</strong> item 18 <strong>of</strong> the contract: “Second Party is committed<br />
to facilitate the processes <strong>of</strong> review<strong>in</strong>g for the evaluation and monitor<strong>in</strong>g department<br />
affiliated to First Party on monthly basis. <strong>The</strong>y are also committed to all the policies and<br />
work procedures <strong>of</strong> HSRP and any modification or updates that may become valid.”<br />
Performance assessment and transfer <strong>of</strong> funds are addressed <strong>in</strong> item 17 <strong>of</strong> the contract:<br />
“Payments are succeeded on four terms quarterly per year, such that each term will be<br />
paid as follows:<br />
− 50% <strong>of</strong> the term <strong>in</strong> return for contract<strong>in</strong>g (Flat Rate)<br />
− Rema<strong>in</strong><strong>in</strong>g 50% <strong>in</strong> return for service performance, based on quality and<br />
performance <strong>in</strong>dicators def<strong>in</strong>ed <strong>in</strong> the Family Health Fund (First Party).”<br />
Settlement <strong>of</strong> disputes is addressed <strong>in</strong> item 24 <strong>of</strong> the contract: “Any differences <strong>in</strong><br />
implement<strong>in</strong>g, execut<strong>in</strong>g or expla<strong>in</strong><strong>in</strong>g any item <strong>of</strong> the contract or any dispute that may<br />
occur should be referred to the Governorate Adm<strong>in</strong>istrative Legal Authorities (State’s<br />
Council Courts). In case <strong>of</strong> referr<strong>in</strong>g back to court or to any other side, Second Party<br />
should cont<strong>in</strong>ue provid<strong>in</strong>g services for beneficiaries and with the same conditions <strong>of</strong> the<br />
contract until the dispute is settled by a court decision or by a f<strong>in</strong>al decision from the<br />
specialized authority or by pay<strong>in</strong>g all the sums <strong>of</strong> money obta<strong>in</strong>ed <strong>in</strong> return for cancell<strong>in</strong>g<br />
the contract”.<br />
What are the types <strong>of</strong> services <strong>of</strong>fered by the provider? On which basis have they been<br />
selected, e.g. for a specific population?<br />
<strong>The</strong> basic benefits package is designed to prevent and treat the most prevalent and<br />
press<strong>in</strong>g <strong>health</strong> problems among <strong>in</strong>dividuals <strong>in</strong> a population. <strong>The</strong> basic benefits package<br />
<strong>in</strong>cludes: child <strong>health</strong> services, women’s <strong>health</strong> services, <strong>health</strong> services for all age groups and<br />
laboratory work.<br />
In order to design and select <strong>health</strong> services <strong>in</strong> the package for Egypt, four criteria were<br />
used:<br />
<strong>The</strong> most common <strong>health</strong> needs <strong>of</strong> the population to reduce suffer<strong>in</strong>g and improve well-be<strong>in</strong>g.<br />
Severity <strong>of</strong> illnesses and diseases affect<strong>in</strong>g the population.<br />
Cost-effectiveness <strong>of</strong> <strong>in</strong>terventions to treat or cure those illnesses and diseases and atta<strong>in</strong> the<br />
most <strong>health</strong> value for money spent.<br />
Availability <strong>of</strong> f<strong>in</strong>ancial resources.<br />
78
Egypt<br />
How did the approved list <strong>of</strong> services evolve?<br />
<strong>The</strong> design <strong>of</strong> the basic benefits package has gone through several steps to reach its f<strong>in</strong>al<br />
form:<br />
Precise data collection for all outpatient visits for a number <strong>of</strong> primary <strong>health</strong> care facilities. <strong>The</strong><br />
data represent three months <strong>of</strong> utilization for urban and rural <strong>health</strong> districts.<br />
Discussions with M<strong>in</strong>istry <strong>of</strong>ficials and local experts <strong>in</strong> epidemiology. <strong>The</strong> discussions <strong>in</strong>cluded<br />
top <strong>health</strong> needs <strong>of</strong> the population accord<strong>in</strong>g to gender and age groups. Representatives <strong>of</strong><br />
HSRP donors also attended the meet<strong>in</strong>gs.<br />
Complet<strong>in</strong>g a draft list <strong>of</strong> contents for the basic benefits package, which has cont<strong>in</strong>ued evolv<strong>in</strong>g<br />
through several updates to meet the needs <strong>of</strong> urban and rural areas. At the same time, the<br />
available f<strong>in</strong>ancial resources have been taken <strong>in</strong>to consideration for the long-term<br />
susta<strong>in</strong>ability <strong>of</strong> the programme with good standards <strong>of</strong> quality.<br />
Would the service quality standards have a <strong>role</strong> <strong>in</strong> the contract?<br />
Health facility accreditation is mandatory prior to contract<strong>in</strong>g with the Family Health<br />
Fund. Primary assessment is made <strong>of</strong> the facility to evaluate the current situation and the<br />
required needs to fulfil the accreditation programme. This is followed by tra<strong>in</strong><strong>in</strong>g <strong>of</strong> the staff<br />
on quality improvement, <strong>in</strong>fection control, leadership, accreditation programme and cl<strong>in</strong>ical<br />
guidel<strong>in</strong>es. <strong>The</strong> third step is pre-accreditation through on-the-job tra<strong>in</strong><strong>in</strong>g to evaluate the<br />
current performance and to set the improvement plan. <strong>The</strong> technical support team <strong>in</strong> each<br />
governorate is responsible to follow up the implementation <strong>of</strong> the improvement plan.<br />
F<strong>in</strong>al accreditation is based on measur<strong>in</strong>g eight categories: patient rights, patient care,<br />
management <strong>of</strong> the facility, management <strong>of</strong> human resources, management <strong>of</strong> support<br />
services, management <strong>of</strong> <strong>in</strong>formation, quality improvement programme and <strong>in</strong>fection control<br />
programme. Each category <strong>in</strong>cludes several standards that focus on key processes, activities,<br />
or outcomes that facilities should achieve. Dur<strong>in</strong>g the accreditation survey, facilities are<br />
assessed to determ<strong>in</strong>e their compliance with standards <strong>in</strong> each category.<br />
Item 1 <strong>of</strong> the contract presents the <strong>role</strong> <strong>of</strong> accreditation <strong>in</strong> the contract: “Second Party<br />
should provide primary <strong>health</strong> care services for the <strong>in</strong>dividuals related to First Party through<br />
obta<strong>in</strong><strong>in</strong>g accreditation from the General Department <strong>of</strong> Quality <strong>in</strong> the M<strong>in</strong>istry <strong>of</strong> Health and<br />
Population and accord<strong>in</strong>g to the standards issued concern<strong>in</strong>g private and nongovernmental<br />
organizations units. This accreditation should rema<strong>in</strong> valid dur<strong>in</strong>g the contract<strong>in</strong>g period and <strong>in</strong><br />
case <strong>of</strong> withdraw<strong>in</strong>g this accreditation, this contract would be automatically <strong>in</strong>valid and void.”<br />
What is the outcome <strong>of</strong> the facility quality improvement process?<br />
Based on the evaluation <strong>of</strong> the facility:<br />
Facilities with a score <strong>of</strong> less than 50% are not accredited and an improvement plan is set to<br />
<strong>in</strong>clude the standard score, responsible person/team, the needs, and the required time.<br />
79
Egypt<br />
Facilities scor<strong>in</strong>g 50%–80% will be accredited for one year, and an improvement plan will be<br />
set to be followed up by the technical support team.<br />
Facilities scor<strong>in</strong>g more than 80% will be accredited for two years with cont<strong>in</strong>uous follow-up by<br />
the technical support team for two years. After this, the facility must be re-accredited and<br />
will not be permitted to achieve less than 80% <strong>in</strong> subsequent assessments.<br />
What k<strong>in</strong>d <strong>of</strong> procedures followed for providers not adher<strong>in</strong>g to quality standards?<br />
<strong>The</strong> Family Health Fund has the right to break the contract with any contracted facility,<br />
even fully accredited, if under any circumstances the facility does not follow or abide by the<br />
stated performance <strong>in</strong>dicators. See item 1 <strong>of</strong> the contract (Annex 1).<br />
CONCLUSIONS AND RECOMMENDATIONS<br />
<strong>The</strong> political environment is supportive <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> the <strong>health</strong> <strong>sector</strong>.<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health and Population cont<strong>in</strong>ues to highlight the need for partnership<br />
between public and private <strong>sector</strong>s, and m<strong>in</strong>isterial decrees have been issued to help<br />
emphasize the <strong>role</strong> <strong>of</strong> the Family Health Fund <strong>in</strong> support<strong>in</strong>g the <strong>contractual</strong> <strong>arrangements</strong> with<br />
private and nongovernmental organization providers.<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health and Population is responsible for the <strong>health</strong> and welfare <strong>of</strong> the<br />
Egyptian population and is committed to carry<strong>in</strong>g out this obligation. Indeed, it may be that<br />
the partial privatization process under way <strong>in</strong> other areas <strong>of</strong> the public <strong>sector</strong> will result <strong>in</strong><br />
mak<strong>in</strong>g available greater government resources and capacity to strengthen the social <strong>sector</strong>s<br />
such as <strong>health</strong> care. Instead <strong>of</strong> privatization, the Egyptian <strong>health</strong> <strong>sector</strong> reform programme<br />
needs to strengthen the private <strong>health</strong> care <strong>sector</strong> <strong>in</strong> order to support those set goals and<br />
priorities <strong>in</strong> an effort to adhere to universally accepted standards <strong>of</strong> quality <strong>of</strong> care <strong>in</strong> Egypt.<br />
Currently, the <strong>role</strong> <strong>of</strong> the Family Health Fund is develop<strong>in</strong>g and mov<strong>in</strong>g towards<br />
purchas<strong>in</strong>g <strong>health</strong> care services at the level <strong>of</strong> the <strong>health</strong> district. <strong>The</strong> Family Health Fund is <strong>in</strong><br />
the process <strong>of</strong> contract<strong>in</strong>g with the District Provider Organization (DPO) <strong>in</strong> parallel to<br />
contract<strong>in</strong>g directly with family <strong>health</strong> facilities. <strong>The</strong> Family Health Fund will pay a global<br />
budget to the DPO accord<strong>in</strong>g to the <strong>health</strong> needs assessment <strong>of</strong> the population, pend<strong>in</strong>g the<br />
negotiations between the two parties <strong>of</strong> the contract, putt<strong>in</strong>g <strong>in</strong> consideration the age<br />
distribution and other risk factors <strong>of</strong> roster population. <strong>The</strong> DPO will use different payment<br />
mechanisms (per capita, fee for service, etc) to compensate the facility.<br />
<strong>The</strong> Family Health Fund, act<strong>in</strong>g on behalf <strong>of</strong> the district population, is support<strong>in</strong>g its<br />
position <strong>in</strong> the <strong>contractual</strong> agreement with the private or nongovernmental organization<br />
provider as a s<strong>in</strong>gle purchaser. <strong>The</strong> Family Health Fund needs to use this opportunity to<br />
design a dynamic market<strong>in</strong>g campaign to promote the concept <strong>of</strong> <strong>contractual</strong> agreement with<br />
the private and nongovernmental organization <strong>sector</strong>.<br />
As the next step, the Family Health Fund needs to expand its contract<strong>in</strong>g with the<br />
private <strong>sector</strong> to a much larger scale, especially outside the pilot governorates, <strong>in</strong> urban<br />
80
Egypt<br />
districts, where private and nongovernmental organization facilities control the outpatient<br />
<strong>health</strong> service market.<br />
<strong>The</strong> Fund needs to establish a plan <strong>of</strong> action for approach<strong>in</strong>g the private and<br />
nongovernmental organization <strong>sector</strong>. At the same time, efforts need to be directed towards<br />
encourag<strong>in</strong>g private and nongovernmental organization providers to contract with the Family<br />
Health Fund through <strong>of</strong>fer<strong>in</strong>g some <strong>in</strong>centives, such as<br />
Reduc<strong>in</strong>g taxes levied on private providers when jo<strong>in</strong><strong>in</strong>g the Health Sector Reform Programme.<br />
Sett<strong>in</strong>g-up an <strong>in</strong>formation system and provid<strong>in</strong>g private and nongovernmental organization<br />
providers with family folders.<br />
Support<strong>in</strong>g the market<strong>in</strong>g plans <strong>of</strong> private and nongovernmental organization providers.<br />
Encourag<strong>in</strong>g private and nongovernmental organization facilities to provide public <strong>health</strong><br />
services as a long term objective.<br />
<strong>The</strong> World Bank, through the Social Fund, has established a new project with the<br />
Quality Improvement Department at the M<strong>in</strong>istry <strong>of</strong> Health and Population focus<strong>in</strong>g on<br />
support and tra<strong>in</strong><strong>in</strong>g <strong>of</strong> nongovernmental organizations. Ten nongovernmental organizations<br />
<strong>in</strong> three governorates have been selected for accreditation as the first step <strong>in</strong> contract<strong>in</strong>g with<br />
the Family Health Fund. Donors need to support this approach <strong>in</strong> order to help spread the<br />
concept to other governorates.<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health and Population through Health Sector Reform Programme and<br />
Family Health Fund needs to study the legality <strong>of</strong> rent<strong>in</strong>g or leas<strong>in</strong>g primary <strong>health</strong> care<br />
facilities to the private <strong>sector</strong>. Such an approach would remove the enormous managerial<br />
burden <strong>of</strong> runn<strong>in</strong>g the facilities and allow the M<strong>in</strong>istry <strong>of</strong> Health and Population to work as a<br />
regulator rather than as a provider.<br />
To date, the Family Health Fund is contract<strong>in</strong>g only for outpatient services. It needs to<br />
move towards <strong>in</strong>patient services and address the relevant issues with the private and<br />
nongovernmental organization <strong>sector</strong> with regard to contract<strong>in</strong>g, especially given that the<br />
Quality Improvement Department has now developed tools for accreditation <strong>of</strong> <strong>in</strong>patient<br />
services.<br />
REFERENCES<br />
1. Alexandria Governorate master plan.<br />
2. Sen, Dave. Case studies <strong>of</strong> mosque and church cl<strong>in</strong>ics <strong>in</strong> Cairo, Egypt. Report <strong>of</strong> a study<br />
supported by the United States Agency for International Development, Egypt.<br />
December 1994.<br />
3. El-Zanaty F, Way AA. Egypt Interim Demographic and Health Survey, 2003. Cairo,<br />
M<strong>in</strong>istry <strong>of</strong> Health and Population, 2004.<br />
81
Egypt<br />
4. Egypt Health Sector Analysis and Future Strategies, HSRP. 2003.<br />
5. Donaldson, DS. Egypt: Health Sector Brief, Partnership for Health Reform Plus, Data<br />
for Decision Mak<strong>in</strong>g (DDM) Project, November 1993.<br />
6. M<strong>in</strong>istry <strong>of</strong> Health and Population, El-Zanaty Associates, and ORC Macro. Egypt<br />
Service Provision Assessment Survey. Calverton, Maryland, ORC Macro, 2002.<br />
7. Stepnick L, Rice JA. Leadership <strong>in</strong> public–private partnership for heath. Seventh<br />
Annual International Summit on Public–Private Partnership for Health Ga<strong>in</strong>, 8–11<br />
December 2002.<br />
8. Family Health Facility Implementation Manual, HSRP.<br />
9. Family Health Fund and Contract<strong>in</strong>g Strategy. Health F<strong>in</strong>ance and Insurance Group.<br />
HSRP.<br />
10. Reich, M. Political mapp<strong>in</strong>g <strong>of</strong> <strong>health</strong> policy: a guide for manag<strong>in</strong>g the political<br />
dimensions for <strong>health</strong> policy. Data for Decision-Mak<strong>in</strong>g Project, Harvard School <strong>of</strong><br />
Public Health, 1994.<br />
11. Private–public partnership study. Mission report. Health Sector Reform Programme/<br />
Family Health Fund. June 2002.<br />
12. SWOT analysis for public private partnership. Health Sector Reform Programme,<br />
Family Health Fund. 2003.<br />
13. Rice, A. Toward a new public–private mix for <strong>health</strong> ga<strong>in</strong>. Plymouth, M<strong>in</strong>nesota,<br />
Lakeland Color Press, 1995.<br />
82
Egypt<br />
Annex 1<br />
Contract copy between FHF and private/NGO<br />
Contract for provid<strong>in</strong>g the basic benefits package for primary <strong>health</strong> care services<br />
with the family <strong>health</strong> centre <strong>in</strong> governorate<br />
Signed on …………., between<br />
1- FHF, legally represented by Dr. ………..(First Party) <strong>in</strong> ………<br />
And,<br />
2- <strong>The</strong> Legal representative <strong>of</strong> the FHC, legally represented by …….., Director <strong>of</strong><br />
………. Centre/Unit (Second Party)<br />
Preface<br />
M<strong>in</strong>istry <strong>of</strong> Health and Population is currently implement<strong>in</strong>g the Health Sector Reform<br />
Programme policy by provid<strong>in</strong>g primary <strong>health</strong> care for all Egyptians through the concept <strong>of</strong><br />
Family Physician. <strong>The</strong> m<strong>in</strong>istry is effect<strong>in</strong>g this policy by the separation between service<br />
provision and its f<strong>in</strong>anc<strong>in</strong>g, <strong>in</strong> cooperation with the private <strong>sector</strong> and NGOs.<br />
<strong>The</strong> two parties have agreed on:<br />
Item 1: Second Party should provide primary <strong>health</strong> care services for the <strong>in</strong>dividuals related<br />
to First Party through obta<strong>in</strong><strong>in</strong>g an accreditation from the General Department <strong>of</strong> Quality <strong>in</strong><br />
MOHP and accord<strong>in</strong>g to the standards issued concern<strong>in</strong>g private and NGOs units (Attachment<br />
1). This accreditation should rema<strong>in</strong> valid dur<strong>in</strong>g the contract<strong>in</strong>g period and <strong>in</strong> case <strong>of</strong><br />
withdraw<strong>in</strong>g this accreditation, this contract would be automatically <strong>in</strong>valid and void.<br />
Item 2: Second Party should <strong>in</strong>form First Party <strong>of</strong> the names <strong>of</strong> all physicians and nurses<br />
legally registered to provide primary <strong>health</strong> care services and who are clarified <strong>in</strong> Item (1) <strong>of</strong><br />
the contract.<br />
Item 3: Second Party should <strong>in</strong>form First Party about any change <strong>of</strong> employees that may<br />
occur with<strong>in</strong> a maximum time limit <strong>of</strong> seven days from the change date.<br />
Item 4: Second Party is committed to notify all its employees with the items and conditions <strong>of</strong><br />
this contract and to confirm the completion <strong>of</strong> this process to the First Party <strong>in</strong> writ<strong>in</strong>g.<br />
Item 5: <strong>The</strong> primary <strong>health</strong> care services delivered by Second Party to <strong>in</strong>dividuals related to<br />
First Party <strong>in</strong>clude services def<strong>in</strong>ed by MOHP Primary Health Care Services BBP, and<br />
83
Egypt<br />
clarified <strong>in</strong> the attached schedule (Attachment 2) except immunization services which are<br />
carried out through the related <strong>health</strong> <strong>of</strong>fice. Second Party is committed to deliver all data <strong>of</strong><br />
the <strong>in</strong>dividuals who will take immunization.<br />
Item 6: Health services provided by Second Party are available for 12 hours a day, all days <strong>of</strong><br />
the week and through two 6-hour shifts from:<br />
Shift 1: ………………… AM – Until ………………… PM<br />
Shift 2:.………………….PM – Until ……………….. ...PM<br />
Emergency services are provided out <strong>of</strong> these times and dur<strong>in</strong>g <strong>of</strong>ficial holidays.<br />
Item 7: Second Party is <strong>in</strong> charge <strong>of</strong> (1500 – 2000 families) for each family medic<strong>in</strong>e room,<br />
as each family physician is committed to serve (750 – 1000 families).<br />
Item 8: Physicians are def<strong>in</strong>ed for each family medic<strong>in</strong>e room by (2 physicians for each room<br />
<strong>in</strong> the morn<strong>in</strong>g + even<strong>in</strong>g). A patient is allowed to visit the room dur<strong>in</strong>g work<strong>in</strong>g hours (12<br />
hours), as the available physician is committed to provide the patient with the medical service<br />
they need. No other physician is allowed to provide the same service except dur<strong>in</strong>g long<br />
vacations, transfer or tra<strong>in</strong><strong>in</strong>g.<br />
Item 9: Second Party is committed to provide complete and accurate data about the names <strong>of</strong><br />
registered service beneficiaries <strong>in</strong> the centre and distribut<strong>in</strong>g them accord<strong>in</strong>g to their <strong>in</strong>surance<br />
categories (Attachment 3). Second Party should <strong>in</strong>form First Party with patients’ visits as per<br />
the visit form prepared by First Party on a monthly basis (Attachment 4).<br />
Item 10: Second Party is committed to provide the necessary teamwork needed for service<br />
provision dur<strong>in</strong>g the contracted work<strong>in</strong>g hours <strong>in</strong> case <strong>of</strong> absence <strong>of</strong> any member <strong>of</strong> the<br />
teamwork for any particular reason such as: annual leave, emergency leave or tra<strong>in</strong><strong>in</strong>g.<br />
Item 11: Second Party is committed to follow the referral procedures whether <strong>in</strong>ternal to the<br />
specialist or external to …….. Public District Hospital (for non-<strong>in</strong>sured patients) or to the<br />
Comprehensive Health Insurance Cl<strong>in</strong>ic (for the <strong>in</strong>sured) accord<strong>in</strong>g to the referral regulations<br />
<strong>of</strong> the BBP and HSRP (Attachment 5).<br />
Item 12: Second Party will bear the responsibility <strong>of</strong> any pr<strong>of</strong>essional oversights that may<br />
occur from the medical team for any registered beneficiaries, as there is no responsibility on<br />
First Party regard<strong>in</strong>g these mistakes.<br />
Item 13: Second Party is committed to implement all the items <strong>of</strong> HE M<strong>in</strong>ister <strong>of</strong> Health and<br />
Population’s Decree No 147 <strong>of</strong> 2003 (Attachment 7), and the regulations related to any<br />
organizational procedures that follow (Attachment 8) and decree 239 <strong>of</strong> 1997 (Attachment 9)<br />
and <strong>health</strong> <strong>in</strong>surance laws (For the <strong>in</strong>sured people) while keep<strong>in</strong>g revenues <strong>of</strong> medical<br />
exam<strong>in</strong>ation (LE …) exam<strong>in</strong>ations and check ups (accord<strong>in</strong>g to the attached regulation) and<br />
84
Egypt<br />
deposit the fees <strong>of</strong> open<strong>in</strong>g new files and 1/3 <strong>of</strong> the price <strong>of</strong> drugs to the fund on monthly<br />
basis. A monthly report is to be provided to the fund as well.<br />
Item 14: First Party should provide medications accord<strong>in</strong>g to the Essential Drug List <strong>of</strong> the<br />
programme. Second Party is committed to follow the rules and regulations for drugs<br />
prescription systems accord<strong>in</strong>g to the Programme’s special regulation (Attachment 11) and<br />
(Attachment 13). Dispens<strong>in</strong>g drugs is applicable only for those registered who paid for the<br />
open<strong>in</strong>g <strong>of</strong> files and are listed <strong>in</strong> the fund. Violations to this rule will be penalized by<br />
collect<strong>in</strong>g the violation fee and <strong>in</strong>form<strong>in</strong>g the authorized legal authority.<br />
Item 15: This contract is valid dur<strong>in</strong>g the period <strong>of</strong> accreditation and will be renewed<br />
automatically with the authorization renewal from the General Department <strong>of</strong> Quality <strong>in</strong><br />
M<strong>in</strong>istry <strong>of</strong> Health and Population, unless any <strong>of</strong> the two parties are <strong>in</strong>formed otherwise 3<br />
months before end <strong>of</strong> contract.<br />
Item 16: First Party is committed to pay the sum <strong>of</strong> LE ….. <strong>in</strong> return for an annual service<br />
provision <strong>of</strong> medical service for each registered beneficiary (who has paid for open<strong>in</strong>g the<br />
file) <strong>in</strong> the unit / centre (<strong>of</strong> the Second Party).<br />
Item 17: Payments are succeeded on four terms quarterly per year, such that each term will be<br />
paid as follows:<br />
• 50 % <strong>of</strong> the term <strong>in</strong> return for contract<strong>in</strong>g (Flat Rate)<br />
• Rema<strong>in</strong><strong>in</strong>g 50% <strong>in</strong> return for service performance, based on quality and performance<br />
<strong>in</strong>dicators def<strong>in</strong>ed <strong>in</strong> FHF (First Party) (Attachment 12 <strong>of</strong> Performance Indicators).<br />
Item 18: Second Party is committed to facilitate the processes <strong>of</strong> review<strong>in</strong>g for the evaluation<br />
and monitor<strong>in</strong>g department affiliated to First Party on monthly basis. <strong>The</strong>y are also committed<br />
to all the policies and work procedures <strong>of</strong> HSRP and any modification or updates that may<br />
become valid (Attachment 6).<br />
Item 19: Second Party is committed to establish a Cost<strong>in</strong>g Unit to monitor the actual cost <strong>of</strong><br />
service. <strong>The</strong>y are also committed to provide any data to the cost<strong>in</strong>g unit <strong>of</strong> the fund to<br />
exchange <strong>in</strong>formation and data related to this cost (Attachment 10).<br />
Item 20: Family folders are considered a private property <strong>of</strong> the Family Health Fund. <strong>The</strong>y<br />
are kept at the centre <strong>in</strong> a safe and confidential location. <strong>The</strong> fund has the right to review them<br />
whenever needed and without any objection from Second Party.<br />
In case <strong>of</strong> end <strong>of</strong> contract for any particular reason, Second Party is obliged to deliver all the<br />
folders that he has and all the data available <strong>in</strong> the Family Health Fund immediately after the<br />
end <strong>of</strong> contract, while keep<strong>in</strong>g all data and <strong>in</strong>formation confidential. In case the Second<br />
Party’s abstention, Second Party has to pay for a penalty <strong>of</strong> pay<strong>in</strong>g the sum <strong>of</strong> LE 100,000 for<br />
temporary compensation until all legal procedures are taken aga<strong>in</strong>st him for violat<strong>in</strong>g<br />
trusteeship.<br />
85
Egypt<br />
Item 21: Second Party should <strong>in</strong>form specialized authorities about any found or suspicious<br />
epidemic cases.<br />
Item 22: Any <strong>of</strong> the two parties has the right to cancel the contract under the provision <strong>of</strong><br />
notify<strong>in</strong>g the other party (<strong>in</strong> writ<strong>in</strong>g) 3 months before end <strong>of</strong> contract.<br />
Item 23: This contract is valid once the accreditation is received from the General Department<br />
<strong>of</strong> Quality Improvement <strong>in</strong> M<strong>in</strong>istry <strong>of</strong> Health and Population, and the centre is committed to<br />
start work<strong>in</strong>g with<strong>in</strong> 3 months from contract sign<strong>in</strong>g date.<br />
Item 24: Any differences <strong>in</strong> implement<strong>in</strong>g - execut<strong>in</strong>g or expla<strong>in</strong><strong>in</strong>g any item <strong>of</strong> the contract<br />
or any dispute that may occur should be referred to the Governorate Adm<strong>in</strong>istrative Legal<br />
Authorities (State’s Council Courts). In case <strong>of</strong> referr<strong>in</strong>g back to court or to any other side,<br />
Second Party should cont<strong>in</strong>ue provid<strong>in</strong>g services for beneficiaries and with the same<br />
conditions <strong>of</strong> the contract until the dispute is settled by a court decision or by a f<strong>in</strong>al decision<br />
from the specialized authority or by pay<strong>in</strong>g all the sums <strong>of</strong> money obta<strong>in</strong>ed <strong>in</strong> return for<br />
cancell<strong>in</strong>g the contract.<br />
Item 25: This contract is issued <strong>in</strong> three copies. One copy for each party and the third to the<br />
Technical Support Tem at M<strong>in</strong>istry <strong>of</strong> Health and Population (Central FHF). A copy <strong>of</strong><br />
attachments to be delivered to Second Party.<br />
First Party Second Party<br />
Dr…………… Dr. ……………..<br />
FHF…….. Director <strong>of</strong> …….., ……..<br />
86
Islamic Republic <strong>of</strong> Iran<br />
ISLAMIC REPUBLIC OF IRAN
ABBREVIATIONS<br />
Islamic Republic <strong>of</strong> Iran<br />
1. MOH/MOHME: M<strong>in</strong>istry <strong>of</strong> Health/M<strong>in</strong>istry <strong>of</strong> Health and Medical Education<br />
2. UHSR: Unit <strong>of</strong> Health Sector Reform<br />
3. SSO: Social Security Organization<br />
4. MSIO: Medical Services Insurance Organization<br />
5. ICCU: Intensive/Cardiac Care Unit<br />
6. GDP: Gross Domestic Product<br />
7. PBO/MPO: Plan and Budget Organization/Management and Plann<strong>in</strong>g Organization<br />
8. TQM: Total Quality Management<br />
9. TUMS: Teheran Medical Sciences University<br />
10. MUMS: Meshed Medical Sciences University<br />
88
INTRODUCTION<br />
Islamic Republic <strong>of</strong> Iran<br />
F<strong>in</strong>anc<strong>in</strong>g <strong>health</strong> care is a critical concern for rich and poor countries alike, as <strong>health</strong><br />
care systems account for about 9% <strong>of</strong> global production. Develop<strong>in</strong>g countries face<br />
particularly serious challenges as they attempt to improve the well-be<strong>in</strong>g <strong>of</strong> their populations,<br />
achieve economic development objectives, and <strong>in</strong>tegrate themselves with the global economy.<br />
Health care f<strong>in</strong>anc<strong>in</strong>g is a particular concern for these develop<strong>in</strong>g countries, which account for<br />
about 84% <strong>of</strong> the world’s population and around 93% <strong>of</strong> its disease burden, but only 18% <strong>of</strong><br />
its <strong>in</strong>come and 11% <strong>of</strong> its <strong>health</strong> expenditure (Schieber, 1997).<br />
Rebuild<strong>in</strong>g <strong>of</strong> f<strong>in</strong>ancial resources is a major component <strong>of</strong> <strong>health</strong> <strong>sector</strong> reform policies.<br />
In this respect, the adoption <strong>of</strong> market-based performance approaches <strong>in</strong> <strong>health</strong> care service<br />
provision, <strong>in</strong> other words, marketization and privatization, were supposed to be a panacea.<br />
Arguments <strong>in</strong> favour <strong>of</strong> the use <strong>of</strong> market <strong>in</strong>centives <strong>in</strong> <strong>health</strong> care may be summarized as<br />
follows:<br />
Contract<strong>in</strong>g/outsourc<strong>in</strong>g may <strong>in</strong>crease competition among <strong>health</strong> care providers;<br />
Increased provider competition may <strong>in</strong>crease technical efficiency on the supply side and<br />
therefore allocative efficiency with<strong>in</strong> the system;<br />
Contractual relationships enhance efficiency on the purchaser and provider sides via the<br />
<strong>in</strong>centive structure <strong>in</strong>herent <strong>in</strong> the contract;<br />
<strong>The</strong> contract<strong>in</strong>g process itself may promote transparency <strong>in</strong> trad<strong>in</strong>g and decentralization <strong>of</strong><br />
managerial responsibility, both <strong>of</strong> which may have beneficial effects on efficiency<br />
(Palmer N, 2000).<br />
Even where there is competition, there is no evidence that the private <strong>sector</strong> <strong>in</strong>variably<br />
provides greater efficiency or quality (Witter et al, 2000). For example, <strong>in</strong> the United States <strong>of</strong><br />
America, competitive markets have been shown to have higher costs, more duplication <strong>of</strong><br />
services, longer length <strong>of</strong> stay, and higher staff ratios than non-competitive markets. In the<br />
national <strong>health</strong> service, implementation <strong>of</strong> purchaser–provider split and quasi-market policies<br />
<strong>in</strong> the public <strong>sector</strong> have not yet been successfully evaluated. However, there are no<br />
generalized f<strong>in</strong>d<strong>in</strong>gs from studies conducted <strong>in</strong> <strong>health</strong> <strong>sector</strong> and <strong>health</strong> f<strong>in</strong>anc<strong>in</strong>g reform,<br />
therefore, the applicability <strong>of</strong> these assumptions to <strong>health</strong> care services, especially <strong>in</strong><br />
develop<strong>in</strong>g countries, must be questioned. Indeed, attempts to translate such po<strong>in</strong>ts <strong>of</strong> view<br />
<strong>in</strong>to practice have highlighted several questionable assumptions, particularly that:<br />
Enough potential providers exist to enable the creation <strong>of</strong> provider competition;<br />
Provider competition, without any change on the purchas<strong>in</strong>g side, can enhance efficiency;<br />
<strong>The</strong> benefits <strong>of</strong> <strong>in</strong>troduc<strong>in</strong>g market <strong>in</strong>centives outweigh the costs <strong>of</strong> their implementation and<br />
ma<strong>in</strong>tenance;<br />
Government has adequate capacity to enter <strong>in</strong>to and manage <strong>contractual</strong> relationships with the<br />
private <strong>sector</strong> (Palmer, N. 2000).<br />
Effective utilization <strong>of</strong> resources seems to be central <strong>in</strong> <strong>health</strong> <strong>sector</strong> reform. Internal<br />
market competition <strong>in</strong>troduced <strong>in</strong> the United K<strong>in</strong>gdom and New Zealand, and managed care<br />
competition implemented <strong>in</strong> the United States <strong>of</strong> America, are known as two major strategies<br />
89
Islamic Republic <strong>of</strong> Iran<br />
<strong>in</strong> this respect. However, none <strong>of</strong> them have been fully adopted for the purpose <strong>of</strong> reform <strong>in</strong><br />
<strong>health</strong> care markets <strong>of</strong> the Islamic Republic <strong>of</strong> Iran.<br />
<strong>The</strong> objectives <strong>of</strong> the study were to identify:<br />
types <strong>of</strong> care for contract<strong>in</strong>g,<br />
the way <strong>of</strong> choos<strong>in</strong>g contract counterparts,<br />
methods <strong>of</strong> payment for their services, and deal<strong>in</strong>g with problems aris<strong>in</strong>g dur<strong>in</strong>g the period <strong>of</strong><br />
contract,<br />
evaluation <strong>of</strong> contract counterparts’ performance,<br />
conditions <strong>in</strong> which nullification or renew<strong>in</strong>g <strong>of</strong> contracts are met,<br />
f<strong>in</strong>ancial risk-bear<strong>in</strong>g by contract counterparts,<br />
effects and outcomes <strong>of</strong> contracts <strong>in</strong> terms <strong>of</strong> cost conta<strong>in</strong>ment, <strong>in</strong>creas<strong>in</strong>g access and improv<strong>in</strong>g<br />
quality,<br />
characteristics <strong>of</strong> the group who is responsible for management, implementation and evaluation<br />
<strong>of</strong> contract<strong>in</strong>g out <strong>in</strong> each medical sciences university.<br />
2. APPROACH AND METHODOLOGY<br />
For the purpose <strong>of</strong> data collection from medical sciences universities, a questionnaire<br />
was developed <strong>in</strong>clud<strong>in</strong>g both closed and open-ended questions. <strong>The</strong> questionnaire was based<br />
on lists <strong>of</strong> questions provided by WHO with regard to the study. <strong>The</strong> type <strong>of</strong> services<br />
contracted, conditions for renew<strong>in</strong>g or nullify<strong>in</strong>g contracts, ways <strong>of</strong> conflict management<br />
between contract parties, select<strong>in</strong>g/choos<strong>in</strong>g counterparts, and strength and weakness’ <strong>of</strong><br />
<strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> practice, as well as wider social and organizational environment,<br />
were determ<strong>in</strong>ed as the questions <strong>of</strong> the study (Annex 1).<br />
An attempt has been made to send the questionnaires to the universities <strong>of</strong> medical<br />
sciences through Health Sector Reform Unit <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health and Medical Education,<br />
but it failed. Parallel to this attempt, a request submitted to “Health Economics and Program<br />
Budget” <strong>of</strong>fice <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health and Medical Education, to facilitate and help data<br />
collection process. It was also unsuccessful.<br />
Personal relations and direct contacts with <strong>of</strong>ficials <strong>of</strong> universities were the last option<br />
to data collection. <strong>The</strong> questionnaire was mailed to Tabriz, Teheran, Meshed, Lorestan, and<br />
Uromieh, medical sciences universities to be filled and returned. Contact <strong>in</strong>formation was also<br />
provided for question and requests for clarification by the respondents.<br />
To expand on <strong>in</strong>formation provided by the universities, semi-structured <strong>in</strong>terviews were<br />
conducted with <strong>of</strong>ficials <strong>in</strong> M<strong>in</strong>istry <strong>of</strong> Health and Medical Education and universities, both<br />
<strong>in</strong>dividually and <strong>in</strong> small groups. <strong>The</strong> questionnaire was considered as a framework for<br />
<strong>in</strong>terviews. Collected data were analysed qualitatively and quantitatively.<br />
90
Islamic Republic <strong>of</strong> Iran<br />
OVERVIEW OF THE IRANIAN HEALTH SYSTEM<br />
<strong>The</strong> <strong>health</strong> system <strong>in</strong> the Islamic Republic <strong>of</strong> Iran is structured <strong>in</strong>to three levels.<br />
Specialty and super-specialty curative services are located and delivered at the upper level,<br />
ma<strong>in</strong>ly <strong>in</strong> mega cities and urban areas. <strong>The</strong> bottom two levels belong to primary <strong>health</strong> care<br />
services, and their activities cover rural, deprived, and remote areas’ populations as well as the<br />
urban poor.<br />
<strong>The</strong> <strong>health</strong> system is highly centralized, and almost all decisions regard<strong>in</strong>g general<br />
goals, policies and allocation <strong>of</strong> resources are made at the central level by the M<strong>in</strong>istry <strong>of</strong><br />
Health and Medical Education. <strong>The</strong> M<strong>in</strong>istry has the legal authority to oversee, license and<br />
regulate the activities <strong>of</strong> the private <strong>health</strong> <strong>sector</strong> (Mehriar et al, 2004).<br />
Primary <strong>health</strong> care services are basically delivered by the public <strong>sector</strong> and are almost<br />
free <strong>of</strong> charge, particularly for the poor. Upper-level services (specialty and super-specialty<br />
curative services), are the area <strong>in</strong> which private <strong>sector</strong> plays a dist<strong>in</strong>ctive <strong>role</strong>. <strong>The</strong>re are about<br />
123 well-equipped, urban-centred, private deliver<strong>in</strong>g specialty and super-specialty service<br />
hospitals <strong>in</strong> the Islamic Republic <strong>of</strong> Iran.<br />
Emergency, curative, diagnostic and pharmaceutical services are delivered by private<br />
hospital. Although there is a tariff schedule for <strong>health</strong> care services determ<strong>in</strong>ed by High<br />
Council <strong>of</strong> Medical Services Insurance (headed by the M<strong>in</strong>ister <strong>of</strong> Health and Medical<br />
Education), the private <strong>sector</strong> does not apply it consistently. Among these hospitals, almost all<br />
practise fee-for-service payment and charge their patients accord<strong>in</strong>g to their own fee<br />
schedules. Regulation and monitor<strong>in</strong>g <strong>of</strong> private <strong>sector</strong> performance are not as effective as<br />
expected. <strong>The</strong> well-known physicians and specialists <strong>of</strong> the public <strong>sector</strong> work <strong>in</strong> the private<br />
<strong>sector</strong> as well. Nurs<strong>in</strong>g and technical staff <strong>of</strong> private hospitals also come ma<strong>in</strong>ly from the<br />
public <strong>sector</strong>. <strong>The</strong>re is not a clear division between public and private <strong>sector</strong>s with regard to<br />
<strong>health</strong> care service delivery <strong>in</strong> the Islamic Republic <strong>of</strong> Iran, creat<strong>in</strong>g confusion <strong>in</strong> the area <strong>of</strong><br />
public–private partnership. <strong>The</strong> overlapp<strong>in</strong>g <strong>of</strong> human resource functions can affect quality <strong>of</strong><br />
care, effectiveness <strong>of</strong> regulations and management <strong>of</strong> services on the whole. <strong>The</strong> issue <strong>of</strong><br />
public <strong>sector</strong> resources exploitation by the private <strong>sector</strong> rema<strong>in</strong>s to be studied.<br />
<strong>The</strong> private <strong>sector</strong>, due partly to its <strong>in</strong>herent for-pr<strong>of</strong>it orientation and partly to poor<br />
organizational behaviour <strong>of</strong> public <strong>sector</strong>, does not participate actively <strong>in</strong> provid<strong>in</strong>g and<br />
deliver<strong>in</strong>g primary <strong>health</strong> care services. Private hospitals also do not show keenness to<br />
contract with the M<strong>in</strong>istry <strong>of</strong> Health and Medical Education, because <strong>of</strong> low tariffs, extra<br />
paperwork and delays <strong>in</strong> payment.<br />
Structurally, and apart from the private <strong>sector</strong>, there are other organizations and<br />
<strong>in</strong>stitutions which play a lead<strong>in</strong>g <strong>role</strong> <strong>in</strong> <strong>health</strong> care management <strong>of</strong> Islamic Republic <strong>of</strong> Iran,<br />
<strong>in</strong> terms <strong>of</strong> policy-mak<strong>in</strong>g, tariff-sett<strong>in</strong>g, and service provision and delivery. <strong>The</strong> Social<br />
Security Organization (SSO) and Armed Forces Health Services Insurance are examples.<br />
Moreover, charity organizations, which focus ma<strong>in</strong>ly on outpatient services, Imam Khome<strong>in</strong>i<br />
Relief Committee, which serves ma<strong>in</strong>ly the poor, and several units <strong>of</strong> <strong>health</strong> care delivery<br />
91
Islamic Republic <strong>of</strong> Iran<br />
affiliated with banks, municipalities, and other organizations further complicate the system,<br />
and perhaps make it less efficient.<br />
Table 1 shows the number and types <strong>of</strong> hospitals <strong>in</strong> terms <strong>of</strong> the <strong>sector</strong>s to which they<br />
belong.<br />
Table 1. Number and types <strong>of</strong> hospitals<br />
Type <strong>of</strong> Hospital No<br />
University 484<br />
Private 123<br />
Charity 238<br />
Social Security Organization 50<br />
Others 33<br />
Total 928<br />
Source: M<strong>in</strong>istry <strong>of</strong> Health and Medical Education, 2001<br />
It is worth not<strong>in</strong>g that most private hospitals are well-equipped with modern technology<br />
and are located <strong>in</strong> major cities, particularly <strong>in</strong> Teheran.<br />
Whereas conflict <strong>of</strong> <strong>in</strong>terests, <strong>in</strong>efficiency, <strong>in</strong>equity, poor management and public<br />
dissatisfaction characterize the costly, urban-oriented curative services (public and private<br />
<strong>sector</strong>), primary <strong>health</strong> care services run satisfactorily.<br />
<strong>The</strong> ma<strong>in</strong> reasons for the notable success <strong>of</strong> the primary <strong>health</strong> care system <strong>of</strong> Islamic<br />
Republic <strong>of</strong> Iran are believed to be the firm commitment <strong>of</strong> the government to <strong>health</strong> and the<br />
relatively proactive public <strong>health</strong> approach adopted s<strong>in</strong>ce the development <strong>of</strong> the primary<br />
<strong>health</strong> care network. Allocat<strong>in</strong>g a relatively modest share <strong>of</strong> government budget (around 7%)<br />
and GDP (around 1.7%) to public <strong>health</strong>, and us<strong>in</strong>g low cost, culturally appropriate and<br />
acceptable public <strong>health</strong> strategies, the Islamic Republic <strong>of</strong> Iran has succeeded <strong>in</strong> reach<strong>in</strong>g<br />
almost universal levels <strong>of</strong> immunization, breastfeed<strong>in</strong>g and use <strong>of</strong> iodized salt, <strong>in</strong> provid<strong>in</strong>g<br />
safe dr<strong>in</strong>k<strong>in</strong>g-water to almost all communities and extend<strong>in</strong>g relatively <strong>in</strong>expensive (if not<br />
entirely free) but efficient public <strong>health</strong> services to the remotest corners <strong>of</strong> the country. In<br />
addition to tra<strong>in</strong><strong>in</strong>g low-cost community-based primary <strong>health</strong> workers, the country has also<br />
managed to expand opportunities for classical medical education opportunities at both general<br />
practice and specialized levels and has developed its pharmaceutical <strong>in</strong>dustry to a level that<br />
can meet the basic needs <strong>of</strong> the country (Mehriar et al, 2004). Figure 1 shows the structure <strong>of</strong><br />
Islamic Republic Iran’s <strong>health</strong> care system (public <strong>sector</strong>) <strong>in</strong> which the lowest levels <strong>of</strong> the<br />
system (<strong>health</strong> houses, and rural/urban <strong>health</strong> centres) ma<strong>in</strong>ly deliver primary <strong>health</strong> care<br />
preventive services under supervision <strong>of</strong> the public <strong>sector</strong>. <strong>The</strong> private <strong>sector</strong> has not been<br />
<strong>in</strong>volved or participated <strong>in</strong> delivery <strong>of</strong> services <strong>in</strong> these areas. Only dur<strong>in</strong>g recent years, after<br />
the waves <strong>of</strong> privatization which were legalized through the third major socio-economic<br />
development plan, have universities <strong>of</strong> medical sciences begun to contract primary <strong>health</strong> care<br />
services or part <strong>of</strong> them to the private <strong>sector</strong> (see Annex 2). At district level, however, the<br />
private <strong>sector</strong> does participate actively, even dom<strong>in</strong>antly, <strong>in</strong> hospital-based service delivery.<br />
92
Delivery<br />
Facility<br />
Health<br />
House<br />
Source: Abolhasani, 2001<br />
Islamic Republic <strong>of</strong> Iran<br />
M<strong>in</strong>istry <strong>of</strong> Health and<br />
Medical Education<br />
School <strong>of</strong> … Director <strong>of</strong> District<br />
University Teach<strong>in</strong>g<br />
Health Network<br />
Hospital<br />
District Health Centre District General<br />
Hospital<br />
Rural Health Centre Urban Health Centre<br />
Health<br />
House<br />
Health<br />
House<br />
Medical University <strong>of</strong> the<br />
Prov<strong>in</strong>ce<br />
Health<br />
Post<br />
Figure 1. Organigram <strong>of</strong> the public <strong>health</strong> care system <strong>of</strong><br />
the Islamic Republic <strong>of</strong> Iran<br />
93<br />
Health<br />
Post<br />
Health<br />
Post
Islamic Republic <strong>of</strong> Iran<br />
CURRENT STATUS OF CONTRACTING OUT HEALTH CARE SERVICES<br />
Legal status <strong>of</strong> contract<strong>in</strong>g out<br />
Contract<strong>in</strong>g out <strong>in</strong> the Iranian <strong>health</strong> care system commenced with the <strong>in</strong>troduction <strong>of</strong> the<br />
Third Socio-economic Development Plan <strong>in</strong> 1999. <strong>The</strong> Plan authorized the M<strong>in</strong>istry <strong>of</strong> Health<br />
and Medical Education to adopt policies by which public–private partnership was to be<br />
achieved. Article 192, <strong>in</strong>cluded <strong>in</strong> the law <strong>of</strong> the Plan focused on privatization <strong>in</strong> general, and<br />
outsourc<strong>in</strong>g <strong>in</strong> particular, <strong>in</strong> <strong>health</strong> care delivery. Another similar regulation (Circular 88) was<br />
later promulgated by the Plann<strong>in</strong>g and Budget Organization (PBO now MPO) to facilitate<br />
purchas<strong>in</strong>g services from private <strong>sector</strong>. While Article 192 emphasized ma<strong>in</strong>ly privatization and<br />
contract<strong>in</strong>g out cl<strong>in</strong>ical services, no clear dist<strong>in</strong>ction was made between cl<strong>in</strong>ical and non-cl<strong>in</strong>ical<br />
services, <strong>in</strong> terms <strong>of</strong> contract<strong>in</strong>g out, <strong>in</strong> Circular 88. Consequently, medical sciences<br />
universities, as contract<strong>in</strong>g agents, were faced with at least two guidel<strong>in</strong>es with remarkable<br />
differences. <strong>The</strong> universities utilize the guidel<strong>in</strong>e they prefer, creat<strong>in</strong>g a complex environment <strong>in</strong><br />
terms <strong>of</strong> performance evaluation, homogeneous <strong>in</strong>formation generation and policy cont<strong>in</strong>uity.<br />
An attempt has been made to pilot Article 192, <strong>in</strong> the catchment areas <strong>of</strong> 7 selected<br />
universities <strong>of</strong> medical sciences <strong>in</strong> different prov<strong>in</strong>ces <strong>of</strong> the country (UHSR, 2003). In<br />
practice, unified performance has not been observed <strong>in</strong> this respect. Some <strong>of</strong> universities<br />
rushed to contract out almost all cl<strong>in</strong>ical and non-cl<strong>in</strong>ical services, while others did so with<strong>in</strong><br />
a very limited framework, and the rest rema<strong>in</strong>ed <strong>in</strong>different.<br />
Accord<strong>in</strong>g to a report <strong>in</strong> 2004, 46 units <strong>of</strong> <strong>health</strong> care delivery were transferred to the<br />
private <strong>sector</strong> through contract<strong>in</strong>g. Contract<strong>in</strong>g for purchas<strong>in</strong>g 45 items <strong>of</strong> cl<strong>in</strong>ical services,<br />
together with 10 items <strong>of</strong> non-cl<strong>in</strong>ical services, was also reported. Tabriz Medical Sciences<br />
University is the pioneer among the universities <strong>in</strong> terms <strong>of</strong> contract<strong>in</strong>g out cl<strong>in</strong>ical services<br />
and privatization. Shiraz and Gilan universities <strong>in</strong> contract<strong>in</strong>g out <strong>health</strong> services.<br />
Apart from well-known medical sciences universities <strong>in</strong> major cities, the rema<strong>in</strong><strong>in</strong>g<br />
universities have ma<strong>in</strong>ly chosen to purchase non-cl<strong>in</strong>ical services from the private market;<br />
this approach seems to be similar with other countries’ experiences <strong>in</strong> privatization (Witter’s<br />
et al. 2000).<br />
Experience <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health and Medical Education<br />
Performance-based service contract<strong>in</strong>g<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health and Medical Education has decided to provide <strong>health</strong> care<br />
services for a large segment <strong>of</strong> the population (ma<strong>in</strong>ly rural and deprived) through contract<strong>in</strong>g<br />
out, establish<strong>in</strong>g a referral system, and employ<strong>in</strong>g family physicians. This is a new approach<br />
<strong>in</strong> Islamic Republic <strong>of</strong> Iran’s <strong>health</strong> care delivery policy which the M<strong>in</strong>istry has adopted <strong>in</strong><br />
response to a parliamentary requirement for <strong>health</strong> <strong>in</strong>surance coverage <strong>of</strong> the rural population.<br />
Among different types <strong>of</strong> contract<strong>in</strong>g, the M<strong>in</strong>istry <strong>of</strong> Health and Medical Education<br />
relies on performance-based service contract<strong>in</strong>g (PBSC), def<strong>in</strong>ed as follows.<br />
94
Islamic Republic <strong>of</strong> Iran<br />
PBSC <strong>in</strong>volves strategies, methods and techniques that describe and communicate measurable<br />
outcomes rather than direct performance processes. It is structured around def<strong>in</strong><strong>in</strong>g a service<br />
requirement <strong>in</strong> terms <strong>of</strong> performance objectives and provid<strong>in</strong>g contractors the latitude to determ<strong>in</strong>e<br />
how to meet these objectives. In other words, it is simply a method <strong>of</strong> acquir<strong>in</strong>g what is required<br />
and plac<strong>in</strong>g the responsibility for how to accomplish it on the contracts. In this respect the<br />
government has developed measurable standards <strong>of</strong> performance together with negative <strong>in</strong>centives<br />
for non-performance, and fee for performance, as major characteristics, or key concepts <strong>of</strong> PBSC.<br />
It seems that with<strong>in</strong> the PBSC poorly managed contracts could be big money losers.<br />
Stages <strong>of</strong> implementation<br />
An adm<strong>in</strong>istrative and technical committee has been organized <strong>in</strong> the M<strong>in</strong>istry <strong>of</strong> Health<br />
and Medical Education for the purpose <strong>of</strong> design<strong>in</strong>g the service packages, performance<br />
monitor<strong>in</strong>g system, and contract<strong>in</strong>g and process standards. A database was designed for<br />
devolved units and for f<strong>in</strong>ancial processes and a tra<strong>in</strong><strong>in</strong>g package was provided and tra<strong>in</strong><strong>in</strong>g<br />
workshops conducted <strong>in</strong> this respect. A situation analysis was also conducted <strong>in</strong> order to<br />
operationalize Article 192.<br />
Types <strong>of</strong> services contracted out/devolved<br />
<strong>The</strong> follow<strong>in</strong>g categories <strong>of</strong> services have been devolved:<br />
Outpatient services (general practitioner, specialist and dentist)<br />
Pharmacy<br />
Rehabilitation services<br />
Laboratory services<br />
Diagnostic radiology services<br />
Hospitals’ wards<br />
Primary <strong>health</strong> care services<br />
Table 2 shows the trend <strong>of</strong> devolved units <strong>of</strong> <strong>health</strong> care services <strong>in</strong> 3 successive years.<br />
Table 2. Number <strong>of</strong> devolved units, 2002–2004<br />
2002 2003 2004<br />
Urban <strong>health</strong> centre 83 120 11<br />
Health post 19 86 172<br />
Rural <strong>health</strong> centre 8 14 24<br />
Radiology 10 23 15<br />
Laboratory 6 14 101<br />
Pharmacy and paramedical cl<strong>in</strong>ic 4 11 14<br />
Hospital wards 5 57 271<br />
Emergency wards 6 36 51<br />
Total number 140 360 568<br />
Three steps were taken by the M<strong>in</strong>istry <strong>of</strong> Health and Higher Education with regard to<br />
designation <strong>of</strong> performance-based contract<strong>in</strong>g for family physicians’ activities as follows:<br />
95
Islamic Republic <strong>of</strong> Iran<br />
Job analysis, which determ<strong>in</strong>es needs, services and outputs expected.<br />
Performance work statement (PWS), which meets def<strong>in</strong>ed and precise <strong>contractual</strong> agreements<br />
with family physicians <strong>in</strong> relation to measurable performance standards for their activities<br />
(output).<br />
Performance assessment plan (PAP), which enables the M<strong>in</strong>istry <strong>of</strong> Health and Higher<br />
Education to evaluate and assess the performance <strong>of</strong> the contracts.<br />
<strong>The</strong> size <strong>of</strong> population covered by a family physician, patients’ satisfaction, quality <strong>of</strong><br />
data records are used as part <strong>of</strong> quantitative and qualitative measures for performance<br />
evaluation. Input criteria, such as human resources, equipment and build<strong>in</strong>g, also have been<br />
employed <strong>in</strong> this respect. <strong>The</strong>se three categories <strong>of</strong> criteria, together with a coefficient which<br />
meets differences and diversities <strong>of</strong> service delivery sett<strong>in</strong>gs, provides a total score for<br />
performance <strong>of</strong> a FP <strong>in</strong> a specific period <strong>of</strong> time and helps to the M<strong>in</strong>istry <strong>of</strong> Health and<br />
Higher Education to manage payment for contracted family physicians. <strong>The</strong> relationship<br />
between performance total score and percentage <strong>of</strong> payment is as follows:<br />
Performance score % <strong>of</strong> payment<br />
90–100 100<br />
80–89 90<br />
70–79 80<br />
60–69 70<br />
<strong>The</strong> contract is nullified if the total performance scores <strong>of</strong> a family physician rema<strong>in</strong><br />
below 60% after three evaluations.<br />
General environment and public–private <strong>sector</strong>s<br />
As is expected from a centralized, mixed and undeveloped socioeconomic structure, the<br />
private <strong>sector</strong> <strong>in</strong> the Islamic Republic <strong>of</strong> Iran, particularly <strong>in</strong> <strong>health</strong> care markets, is not yet<br />
fully developed. As a for-pr<strong>of</strong>it <strong>sector</strong>, it is ma<strong>in</strong>ly <strong>in</strong>volved <strong>in</strong> the hospital <strong>in</strong>dustry, located <strong>in</strong><br />
major cities, and has been reluctant to <strong>in</strong>vest <strong>in</strong> preventive care and <strong>in</strong> remote or deprived<br />
areas. <strong>The</strong> performance <strong>of</strong> the private <strong>sector</strong> is not effectively regulated. This <strong>sector</strong> rarely<br />
uses the M<strong>in</strong>istry <strong>of</strong> Health and Higher Education’s tariff schedule, or evaluates services<br />
delivered, and accreditation <strong>of</strong> <strong>in</strong>stitutions/hospitals <strong>in</strong> this <strong>sector</strong>, seem to be less effective <strong>in</strong><br />
improv<strong>in</strong>g public–private relationship. At the tertiary level <strong>of</strong> <strong>health</strong> care delivery <strong>in</strong> the<br />
Iranian system, the private <strong>sector</strong> is highly active and seems to exploit the public <strong>sector</strong>’ s<br />
resources, particularly human resources.<br />
In contrast, the public <strong>sector</strong> suffers from <strong>in</strong>adequate managerial skills and capacity,<br />
<strong>in</strong>appropriate executive and legal context and <strong>in</strong>sufficient knowledge and experience with<br />
respect to the <strong>health</strong> care <strong>in</strong>dustry. <strong>The</strong>se deficiencies are possible reasons for the significant<br />
change <strong>in</strong> approach reflected <strong>in</strong> Article 192. For example, while <strong>in</strong> the early days <strong>of</strong><br />
implementation it was <strong>of</strong>ficially documented that the <strong>health</strong> houses and package <strong>of</strong> services<br />
delivered there must be privatized (<strong>in</strong> any way), this policy was proposed to be nullified<br />
beg<strong>in</strong>n<strong>in</strong>g <strong>in</strong> March 2004. Lack <strong>of</strong> stability <strong>in</strong> policy leaves room for <strong>in</strong>dividual preferences <strong>of</strong><br />
96
Islamic Republic <strong>of</strong> Iran<br />
authorities <strong>of</strong> medical sciences universities, which <strong>in</strong> turn may <strong>in</strong>crease complexity <strong>of</strong> the<br />
system and reduce its efficiency.<br />
A very comprehensive guidel<strong>in</strong>e, <strong>in</strong>clud<strong>in</strong>g the philosophy <strong>of</strong> privatization and<br />
decentralization, decentralization <strong>in</strong> <strong>health</strong> care systems, standards for contract<strong>in</strong>g and<br />
methods <strong>of</strong> payment, examples <strong>of</strong> bidd<strong>in</strong>g and contract<strong>in</strong>g forms, packages <strong>of</strong> services and<br />
monitor<strong>in</strong>g and evaluation <strong>of</strong> services, has been developed by the Unit for Health Sector<br />
Reform <strong>in</strong> the M<strong>in</strong>istry <strong>of</strong> Health and Higher Education. However, there is still room for more<br />
clarification and elaboration <strong>of</strong> Article 192, possibly for the unification <strong>of</strong> approaches used by<br />
medical sciences universities to privatization and <strong>contractual</strong> <strong>arrangements</strong>. An executive<br />
guidel<strong>in</strong>e is be<strong>in</strong>g developed <strong>in</strong> the M<strong>in</strong>istry <strong>in</strong> order to move ahead <strong>in</strong> efforts to achieve the<br />
goals <strong>of</strong> the Third Socioeconomic Development Plan. However, contract<strong>in</strong>g for <strong>health</strong> care <strong>in</strong><br />
the Islamic Republic <strong>of</strong> Iran is <strong>in</strong> its nascency and may require time and other resources to be<br />
successfully implemented and managed.<br />
In terms <strong>of</strong> types <strong>of</strong> contracts, and methods <strong>of</strong> payment, it can be said that block<br />
contracts and cost-volume contracts are dom<strong>in</strong>ant. Per capita, global and even capped fee-forservice<br />
methods <strong>of</strong> payment are practised for services purchased from the private <strong>sector</strong><br />
(Appendix 2).<br />
Contract<strong>in</strong>g out or purchas<strong>in</strong>g services from the private <strong>sector</strong> is a new approach to<br />
deal<strong>in</strong>g with <strong>health</strong> care market problems <strong>in</strong> develop<strong>in</strong>g countries <strong>in</strong> general, and <strong>in</strong> the<br />
Islamic Republic <strong>of</strong> Iran <strong>in</strong> particular. Attempts to adopt policies regard<strong>in</strong>g reform <strong>in</strong> <strong>health</strong><br />
care services <strong>in</strong> the Islamic Republic <strong>of</strong> Iran date back only three years, and contract<strong>in</strong>g out <strong>in</strong><br />
<strong>health</strong> care markets suffers from lack <strong>of</strong> organizational and managerial capacities <strong>in</strong> both the<br />
public and private <strong>sector</strong>s. Because <strong>of</strong> this environment, there is no uniformity among the<br />
medical sciences universities (as agents <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health and Higher Education) with<br />
regard to purchas<strong>in</strong>g services from the private <strong>sector</strong>.<br />
At the present, preventive care, paramedical services and dentistry are the most common<br />
services, contracted respectively. <strong>The</strong> universities contract out for packages <strong>of</strong> (ma<strong>in</strong>ly)<br />
preventive services, and are generally satisfied with this strategy. Improvements <strong>in</strong> access to<br />
services, <strong>in</strong>creased efficiency, promotion <strong>of</strong> quality <strong>of</strong> services and responsiveness are given<br />
as outcomes <strong>of</strong> this strategy (Appendix 2).<br />
DISCUSSION<br />
In management <strong>of</strong> contracts for purchas<strong>in</strong>g any/cl<strong>in</strong>ical services from the private <strong>sector</strong>,<br />
transaction costs, methods <strong>of</strong> payment, competition and risk-shar<strong>in</strong>g, opportunistic behaviour<br />
on purchaser and provider sides, and contract goals and nature are discussed <strong>in</strong> relevant<br />
literature. <strong>The</strong> efficiency and types <strong>of</strong> contract, conditions for sett<strong>in</strong>g successful contracts,<br />
l<strong>in</strong>ks with total quality management, renewal positions (if any), penalties for nonperformance,<br />
process for resolv<strong>in</strong>g disagreements, and advantages and disadvantages <strong>of</strong> contracts are also<br />
important concepts <strong>in</strong> this respect (Witter S. et al. 2000; Flood M.C, 2000).<br />
97
Islamic Republic <strong>of</strong> Iran<br />
In <strong>health</strong> <strong>sector</strong> reform policies, the impact <strong>of</strong> contract<strong>in</strong>g is thought to be dependent on<br />
how it is implemented. Done well, it can improve technical efficiency (by promot<strong>in</strong>g cost<br />
control), allocative efficiency (by redirect<strong>in</strong>g resources), and cl<strong>in</strong>ical and service quality (if<br />
the contract <strong>in</strong>cludes measurable performance goals). As well, contract<strong>in</strong>g to improve access<br />
by requir<strong>in</strong>g a volume <strong>of</strong> free care on thereby improve the equity <strong>of</strong> system performance<br />
(Robert JM et al, 2004).<br />
Contract implementation and management, however, particularly <strong>in</strong> a complex <strong>health</strong><br />
care environment <strong>in</strong> a develop<strong>in</strong>g country such as Islamic Republic <strong>of</strong> Iran, require<br />
managerial capacity and skills, adequate human and f<strong>in</strong>ancial resources, <strong>in</strong>ter<strong>sector</strong>al and<br />
<strong>in</strong>tra<strong>sector</strong>al coord<strong>in</strong>ation and collaboration, and broad cultural, legal and political<br />
agreements.<br />
<strong>The</strong> Iranian <strong>health</strong> care system faces a number <strong>of</strong> <strong>in</strong>stitutional, f<strong>in</strong>ancial and<br />
adm<strong>in</strong>istrative gaps: gaps between the public and private <strong>sector</strong>s, levels <strong>of</strong> <strong>health</strong> care delivery<br />
(disrupted referral system), payments and remuneration, physician and staff earn<strong>in</strong>gs <strong>in</strong><br />
hospitals (between different groups <strong>of</strong> physicians and between physicians and non-physician<br />
staff), and rules and laws as practice guidel<strong>in</strong>es <strong>in</strong> provision and delivery <strong>of</strong> <strong>health</strong> care<br />
services.<br />
Neither <strong>health</strong> care managers nor their counterparts <strong>in</strong> the private <strong>sector</strong> have been<br />
tra<strong>in</strong>ed and acquired necessary skills for quality contract<strong>in</strong>g Meshed Medical Services<br />
University. <strong>The</strong> private <strong>sector</strong> is not yet very well organized and on occasion demonstrates<br />
opportunistic behaviour. For example, accord<strong>in</strong>g to some <strong>of</strong> <strong>in</strong>terviewees, the private <strong>sector</strong><br />
still <strong>in</strong>terested <strong>in</strong> hav<strong>in</strong>g a middle man’s <strong>role</strong> <strong>in</strong>stead <strong>of</strong> actively participat<strong>in</strong>g <strong>in</strong> production<br />
and productive processes Teheran Medical Services University.<br />
Lower payment, together with oversecurity <strong>of</strong> employees’ positions <strong>in</strong> public <strong>sector</strong><br />
(and lack <strong>of</strong> economic th<strong>in</strong>k<strong>in</strong>g among managers <strong>in</strong> different organizational level<br />
(Momensaraie and Pourreza, 2002), are <strong>in</strong>dicated as the ma<strong>in</strong> reasons for <strong>in</strong>efficiency <strong>in</strong><br />
public <strong>sector</strong> performance.<br />
It is a fact that the nations least equipped to make their public <strong>sector</strong> function effectively<br />
are <strong>of</strong>ten those least able to discipl<strong>in</strong>e private markets to achieve public ends (Robert, M. et.<br />
al). However, even <strong>in</strong> an environment with these better characteristics, on some occasions<br />
contract<strong>in</strong>g out produces more results. For example, out sourc<strong>in</strong>g <strong>of</strong> a laboratory <strong>in</strong> one <strong>of</strong><br />
Teheran’s hospitals led to more tests and greater <strong>in</strong>come (TUMS).<br />
CONCLUSION AND RECOMMENDATIONS<br />
Conclusions<br />
Contract<strong>in</strong>g out <strong>of</strong> <strong>health</strong> care services <strong>in</strong> the Islamic Republic <strong>of</strong> Iran was <strong>in</strong>itiated<br />
under the Third Socioeconomic Development Plan <strong>in</strong>troduced <strong>in</strong> 1999. In fact it can be<br />
considered a privatization policy emphasized <strong>in</strong> the plan and its legislation (Article 192).<br />
98
Islamic Republic <strong>of</strong> Iran<br />
From an adm<strong>in</strong>istrative po<strong>in</strong>t <strong>of</strong> view, contract<strong>in</strong>g parties, both medical sciences<br />
universities and the private <strong>sector</strong>, suffer from relevant background, experienced staff, and<br />
organized uniform approach <strong>in</strong> terms <strong>of</strong> services to be contracted, methods <strong>of</strong> payment, and<br />
rules and laws practised.<br />
Providers’ play<strong>in</strong>g both sides <strong>of</strong> the street contam<strong>in</strong>ate public–private partnership, and<br />
lack <strong>of</strong> reliable <strong>in</strong>formation, or regular evaluation <strong>of</strong> private <strong>sector</strong>/providers h<strong>in</strong>der decisionmak<strong>in</strong>g<br />
regard<strong>in</strong>g contract renewal and cont<strong>in</strong>uity <strong>of</strong> the policy.<br />
A volatile bureaucratic decision-mak<strong>in</strong>g environment has led to an <strong>in</strong>dividualistic<br />
approach <strong>in</strong> purchas<strong>in</strong>g services from private <strong>sector</strong> by the universities (lack <strong>of</strong> uniformity and<br />
homogeneity). Some universities rely on the Article 192 and others on Circular 88. While<br />
Article 192 emphasizes marketization <strong>of</strong> cl<strong>in</strong>ical services Circular 88 permits all cl<strong>in</strong>ical and<br />
non-cl<strong>in</strong>ical services to be contracted out. This may be a reason for the different approaches to<br />
purchas<strong>in</strong>g services from the private <strong>sector</strong>.<br />
Services contracted by the universities ma<strong>in</strong>ly cover primary <strong>health</strong> care, outpatient and<br />
non-cl<strong>in</strong>ical services. Limited and mostly <strong>in</strong>expensive types <strong>of</strong> service are contracted out.<br />
Information result<strong>in</strong>g from evaluations <strong>of</strong> the performance <strong>of</strong> private providers, has not yet<br />
been organized. Such <strong>in</strong>formation rema<strong>in</strong>s unavailable, though it has been emphasized <strong>in</strong><br />
Circular 88 that every medical sciences university should submit a copy <strong>of</strong> contract<strong>in</strong>g parties’<br />
performance to the Management and Plann<strong>in</strong>g Organization.<br />
Privatization and contract<strong>in</strong>g out <strong>in</strong> Islamic Republic <strong>of</strong> Iran has ma<strong>in</strong>ly focused on<br />
primary <strong>health</strong> care services and expensive specialty urban-oriented curative services have<br />
rema<strong>in</strong>ed almost untouched. S<strong>in</strong>ce primary <strong>health</strong> care services <strong>in</strong> Iran are delivered almost<br />
free <strong>in</strong> rural and poor urban areas, this approach, if accompanied by user fees, may <strong>in</strong> the long<br />
term widen gaps <strong>in</strong> equity between rural and urban areas, and limit access to <strong>health</strong> care<br />
services.<br />
It seems that unemployment <strong>of</strong> numbers <strong>of</strong> young physicians and paramedical graduates<br />
has played a significant <strong>role</strong> <strong>in</strong> develop<strong>in</strong>g <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> <strong>health</strong> care services<br />
delivery <strong>in</strong> the Islamic Republic <strong>of</strong> Iran. It means that adoption <strong>of</strong> privatization, and <strong>in</strong> some<br />
extent contract<strong>in</strong>g out policy, is determ<strong>in</strong>ed by force rather than choice. Other reasons should<br />
also be taken <strong>in</strong>to account <strong>in</strong> this respect. However, implement<strong>in</strong>g a policy which designed<br />
and developed <strong>in</strong> <strong>in</strong>dustrialized countries decades ago <strong>in</strong> a develop<strong>in</strong>g country with poor<br />
organizational structures and management will hardly work effectively, at least <strong>in</strong> a short<br />
period <strong>of</strong> time. In relevant literature, <strong>in</strong>dividualism, rationalism, utilitarianism and legalism<br />
have been <strong>in</strong>dicated as the bedrocks <strong>of</strong> socioeconomic development <strong>of</strong> <strong>in</strong>dustrialized<br />
countries. “Organizational cultural lag” as a dom<strong>in</strong>ant characteristic <strong>of</strong> develop<strong>in</strong>g countries,<br />
<strong>in</strong>clud<strong>in</strong>g Iran, may h<strong>in</strong>der these essential components <strong>of</strong> development.<br />
Actions to be undertaken<br />
As a first step, the long-term process <strong>of</strong> reform, particularly <strong>in</strong> the <strong>health</strong> <strong>sector</strong>, should<br />
be appreciated and acknowledged by policy-makers. However, the reform itself seems to be<br />
99
Islamic Republic <strong>of</strong> Iran<br />
the product <strong>of</strong> the experience <strong>of</strong> <strong>in</strong>dustrialized countries’, and its applicability <strong>in</strong> the context<br />
<strong>of</strong> a develop<strong>in</strong>g country such as Islamic Republic <strong>of</strong> Iran with traditional, religious,<br />
fragmented and complex structures, is yet to be determ<strong>in</strong>ed.<br />
At strategic level<br />
Justification among top decision-makers about the necessity, importance and usefulness <strong>of</strong><br />
contract<strong>in</strong>g out;<br />
Achiev<strong>in</strong>g commitment high-ranked managers and politicians;<br />
Provid<strong>in</strong>g appropriate, updated and evidence-based legal environment, as well as f<strong>in</strong>ancial<br />
resources, for its successful implementation.<br />
At operational level<br />
Identification <strong>of</strong> capable <strong>in</strong>dividuals/<strong>in</strong>stitutions <strong>in</strong> private <strong>sector</strong> as counterpart for contract<strong>in</strong>g;<br />
Identification <strong>of</strong> services purchasable from the private <strong>sector</strong>;<br />
Standardization <strong>of</strong> delivery <strong>of</strong> purchasable services;<br />
Publiciz<strong>in</strong>g necessity for reform <strong>in</strong> <strong>health</strong> care/social market<strong>in</strong>g;<br />
Design<strong>in</strong>g and implement<strong>in</strong>g a management <strong>in</strong>formation system for record<strong>in</strong>g and evaluat<strong>in</strong>g<br />
private <strong>sector</strong> performance;<br />
Capacity-build<strong>in</strong>g <strong>in</strong>/empowerment <strong>of</strong> both the public and private <strong>sector</strong>, requir<strong>in</strong>g tra<strong>in</strong><strong>in</strong>g the<br />
right personnel for the purpose <strong>of</strong> manag<strong>in</strong>g <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> <strong>health</strong> services;<br />
Capacity-build<strong>in</strong>g for teamwork and utiliz<strong>in</strong>g other specialties, capacities and capabilities<br />
<strong>in</strong>stead <strong>of</strong> monopoliz<strong>in</strong>g reform plans and activities by only one group <strong>of</strong> pr<strong>of</strong>essionals<br />
(physicians or the others).<br />
SOURCES<br />
1. Roberts JM et al. Gett<strong>in</strong>g <strong>health</strong> reform right: a guide to improv<strong>in</strong>g performance and<br />
equity. Oxford University Press, 2004.<br />
2. Flood MC. International <strong>health</strong> care reform: a legal, economic and political analysis.<br />
London, Routledge, 2000.<br />
3. Palmer N. <strong>The</strong> use <strong>of</strong> private-<strong>sector</strong> contracts for primary <strong>health</strong> care: theory, evidence<br />
and lessons for low-<strong>in</strong>come and middle-<strong>in</strong>come countries. WHO Bullet<strong>in</strong>, 2000, 78, (6):<br />
821–830.<br />
4. Witter S et al. Health economics for develop<strong>in</strong>g countries: a practical guide. BUPA,<br />
Macmillan Education Ltd, 2000.<br />
5. Mehryar AH et al. Primary Health Care and Rural Poverty Eradication <strong>in</strong> the Islamic<br />
Republic <strong>of</strong> Iran. Population Studies and Research Centre for Asia and the Pacific,<br />
Work<strong>in</strong>g Paper No: 10.<br />
100
Islamic Republic <strong>of</strong> Iran<br />
6. Shieber JG. (1997), Innovations <strong>in</strong> Health Care F<strong>in</strong>anc<strong>in</strong>g, Proceed<strong>in</strong>g <strong>of</strong> a World Bank<br />
Conference, World Bank Discussion Paper No. 365.<br />
7. Laws and Regulations <strong>of</strong> MOH and Iran’ s government <strong>in</strong>clud<strong>in</strong>g:<br />
− Article 192 <strong>in</strong> “Law <strong>of</strong> the third socio-economic plan 2000-2004”, MPO<br />
publications, 2001, Teheran, Iran.<br />
− Circular 88, MPO, 2002, Teheran, Iran.<br />
8. Momensaraie M, Pourreza A. <strong>The</strong> status <strong>of</strong> economic th<strong>in</strong>k<strong>in</strong>g among hospital managers<br />
and decision makers. Journal <strong>of</strong> School <strong>of</strong> Public Health, Teheran Medical Sciences<br />
University, 2002, 2: 1.<br />
9. Regulations for implementation <strong>of</strong> Article 192. Teheran, Unit for Health Sector Reform,<br />
M<strong>in</strong>istry <strong>of</strong> Health and Medical Education, 2003.<br />
FURTHER READING<br />
Slack K, Saved<strong>of</strong>f D W. Public purchaser–private provider contract<strong>in</strong>g for <strong>health</strong> services,<br />
examples from Lat<strong>in</strong> America and the Caribbean. Wash<strong>in</strong>gton, D.C, Inter-American<br />
Development Bank, Susta<strong>in</strong>able Development Department, Technical Papers Series, 2001.<br />
McPake B, Hongoro C. Contract<strong>in</strong>g out <strong>of</strong> cl<strong>in</strong>ical services <strong>in</strong> Zimbabwe, Soc. Sci. Med.<br />
1995, 41(1): 13–24.<br />
England R. Contract<strong>in</strong>g and performance management <strong>in</strong> the <strong>health</strong> <strong>sector</strong>: some po<strong>in</strong>ters on<br />
how to do it. London, DFDI Health Systems Resource Centre, 2000.<br />
McPake B et al. Is the Colombian <strong>health</strong> system reform improv<strong>in</strong>g the performance <strong>of</strong> public<br />
hospitals <strong>in</strong> Bogota? Health policy and plann<strong>in</strong>g, 2003, 18(2).<br />
Loev<strong>in</strong>sohn, B.(?), Practical Issues <strong>in</strong> Contract<strong>in</strong>g for Primary Health Care Delivery: Lessons<br />
from Two Large Projects <strong>in</strong> Bangladesh, World Bank, USA.<br />
Barr D. Research protocol to evaluate the effectiveness <strong>of</strong> public/private partnerships <strong>in</strong><br />
enhanc<strong>in</strong>g <strong>health</strong> and welfare systems development. Center for Health Policy, Institute for<br />
International Studies, Stanford University, 2004.<br />
Jack W. Contract<strong>in</strong>g for <strong>health</strong> services: an evaluation <strong>of</strong> recent reforms <strong>in</strong> Nicaragua. Health<br />
policy and plann<strong>in</strong>g, 2002, 18(2).<br />
101
Islamic Republic <strong>of</strong> Iran<br />
Annex 1<br />
QUESTIONNAIRE<br />
1. Do you have any contract(s) for <strong>health</strong> care purchas<strong>in</strong>g from private <strong>sector</strong>? If yes,<br />
would you please specify the services <strong>in</strong> this respect?<br />
2. How do you choose your private <strong>sector</strong> partner for contract<strong>in</strong>g out? Based on previous<br />
familiarity, colleagues’ advice, bidd<strong>in</strong>g, good reputation or else?<br />
3. How do you pay for services purchased from private <strong>sector</strong>? Fee for service, global, per<br />
unit, or else?<br />
4. Have you ever experienced problems/difficulties (legally or adm<strong>in</strong>istratively) <strong>in</strong><br />
conduct<strong>in</strong>g contracts with private <strong>sector</strong> (such as delay on payments and so on)? If yes<br />
how did you solve the problem(s)? Through referr<strong>in</strong>g them to the court, arbitrary, or<br />
other ways?<br />
5. Do you use any evaluation process for services purchased from and delivered by private<br />
<strong>sector</strong>? How? What is your <strong>in</strong>strument and who does (do) conduct the process?<br />
6. How renew<strong>in</strong>g <strong>of</strong> contracts takes place? On what conditions/circumstances?<br />
7. How and when a contract is nullified?<br />
8. Which part <strong>of</strong> the contract (university or private <strong>sector</strong>) ga<strong>in</strong>s more pr<strong>of</strong>it/benefit from<br />
contract<strong>in</strong>g processes?<br />
9. What was/were the consequences <strong>of</strong> out-sourc<strong>in</strong>g and purchas<strong>in</strong>g services from private<br />
<strong>sector</strong>? Decrease <strong>in</strong> unit cost, <strong>in</strong>crease <strong>in</strong> accessibility, <strong>in</strong>crease <strong>in</strong> quality <strong>of</strong> services,<br />
<strong>in</strong>crease equity, or else?<br />
10. Is there any specific team/group or unit <strong>in</strong> your university responsible for contract<strong>in</strong>g<br />
out and purchas<strong>in</strong>g services from private <strong>sector</strong>? If yes, please expla<strong>in</strong> more about its<br />
structure <strong>in</strong> terms <strong>of</strong> its personnel work and educational experience.<br />
11. On the whole what is your prediction about the future <strong>of</strong> this process (out sourc<strong>in</strong>g and<br />
contract<strong>in</strong>g out <strong>of</strong> <strong>health</strong> care services?<br />
102
Medical<br />
Sciences<br />
University<br />
Islamic Republic <strong>of</strong> Iran<br />
Annex 2<br />
UNIVERSITIES CONTRACTING PRIMARY HEALTH CARE SERVICES TO THE PRIVATE SECTOR<br />
Contracts<br />
with private<br />
<strong>sector</strong><br />
Teheran Yes ICU, pharmacy,<br />
dentistry,<br />
laboratory,<br />
radiology, and<br />
<strong>health</strong> posts<br />
services<br />
Name <strong>of</strong> services Way <strong>of</strong> choos<strong>in</strong>g<br />
private<br />
contractor(s)<br />
Methods <strong>of</strong><br />
payment<br />
Bidd<strong>in</strong>g Fee-for-service<br />
+ global<br />
Difficulties<br />
dur<strong>in</strong>g contract<br />
period<br />
Method <strong>of</strong><br />
problem solv<strong>in</strong>g<br />
Yes Negotiation,<br />
dialog and<br />
persuasion<br />
Orumieh Yes PHC services Bidd<strong>in</strong>g Global Yes Negotiation,<br />
dialog and<br />
persuasion<br />
Meshed Yes Laboratory and<br />
pharmacy services.<br />
Bidd<strong>in</strong>g Per-capita Yes Negotiation,<br />
dialog and<br />
E<br />
v<br />
al<br />
u<br />
at<br />
io<br />
n<br />
<strong>of</strong><br />
se<br />
r<br />
vi<br />
ce<br />
s<br />
p<br />
u<br />
rc<br />
h<br />
as<br />
e<br />
d<br />
Tools and<br />
responsibilitie for<br />
evaluation<br />
Yes Through a<br />
questionnaire/<br />
checklist + field<br />
visit and process<br />
evaluation<br />
Yes Checklist/team<br />
Yes Checklist/team
PHC services<br />
Open heart<br />
services<br />
Tabriz Yes Screen<strong>in</strong>g/preventi<br />
ve care<br />
Lorestan Yes -Nurs<strong>in</strong>g, theatre,<br />
laboratory and<br />
radiology services<br />
WHO-EM/XXX/XXX/E<br />
Page 104<br />
104<br />
persuasion<br />
Bidd<strong>in</strong>g Capitation No – Yes Checklist/team<br />
Familiarity<br />
Colleagues’<br />
advice<br />
Global yes Negotiation,<br />
dialog and<br />
persuasion<br />
Because <strong>of</strong> limited number <strong>of</strong> private contractors <strong>in</strong> the prov<strong>in</strong>ce (semi-monopolistic situation), bidd<strong>in</strong>g is not applicable .<br />
Yes Checklist/weekly<br />
reports
Jordan<br />
JORDAN
ACRONYMS<br />
Jordan<br />
GDP Gross Domestic Product<br />
JD Jordanian D<strong>in</strong>ar<br />
WHO World Health Organization<br />
MOH M<strong>in</strong>istry <strong>of</strong> Health<br />
RMS Royal Medical Services<br />
JUH Jordan University Hospital<br />
KAH K<strong>in</strong>g Abdullah Hospital<br />
CHIP Civil Health Insurance Plan<br />
JUST University <strong>of</strong> Science and Technology<br />
HID Health Insurance Directorate<br />
UNRWA United Nations Relief and Works Agency for Palest<strong>in</strong>e<br />
Refugees <strong>in</strong> the Near East<br />
MCH Maternity and Child Health<br />
JNHA Jordan’s National Health Accounts<br />
NGO Nongovernmental organizations<br />
PHR Partners for Health Reform<br />
MOF M<strong>in</strong>istry <strong>of</strong> F<strong>in</strong>ance<br />
MOP M<strong>in</strong>istry <strong>of</strong> Plann<strong>in</strong>g<br />
SWOT Strengths, Weaknesses, Opportunities, Threats<br />
MHIP Military Health Insurance Plan<br />
HCC Al-Husse<strong>in</strong> Cancer Center<br />
CH Crescent Hospital<br />
HIPP Health Insurance Pilot Project<br />
IU Implementation Unit<br />
106
INTRODUCTION<br />
Jordan<br />
This study documents the experience <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health <strong>in</strong> Jordan <strong>in</strong><br />
contract<strong>in</strong>g out services with the private <strong>sector</strong> and the other autonomous public<br />
<strong>sector</strong>s such as the Royal Medical Services, Jordan University Hospital and K<strong>in</strong>g<br />
Abdullah University Hospital. <strong>The</strong> study also <strong>in</strong>cludes a general assessment <strong>of</strong> these<br />
<strong>contractual</strong> <strong>arrangements</strong> to identify areas <strong>of</strong> strengths, weakness and opportunities<br />
for improvement. <strong>The</strong> specific objectives <strong>of</strong> the study were to:<br />
• Acquire <strong>in</strong>-depth understand<strong>in</strong>g <strong>of</strong> nature, extent and presence <strong>of</strong><br />
enabl<strong>in</strong>g/disabl<strong>in</strong>g factors that promote/prevent public–private partnership <strong>in</strong><br />
<strong>health</strong> <strong>in</strong> Jordan.<br />
• Develop a base for a national strategy on public–private partnership <strong>in</strong> <strong>health</strong> that<br />
would promote access, efficiency, equity and quality.<br />
A special data collection tool (Annex 1) was developed by the researcher to<br />
assess the <strong>contractual</strong> <strong>arrangements</strong> between the M<strong>in</strong>istry <strong>of</strong> Health and other <strong>health</strong><br />
care providers. This tool covers the follow<strong>in</strong>g areas:<br />
Type <strong>of</strong> service covered<br />
Selection mechanism and length <strong>of</strong> contract<br />
Regulation, who enforces and what level<br />
Payment mechanism<br />
F<strong>in</strong>ancial and other <strong>in</strong>centives for the purchaser and provider<br />
Level <strong>of</strong> performance based measures<br />
Purchasers level <strong>of</strong> effort <strong>in</strong> management and adm<strong>in</strong>istration<br />
Providers level <strong>of</strong> effort <strong>in</strong> management and adm<strong>in</strong>istration<br />
Geographical scope <strong>of</strong> contract<br />
Monitor<strong>in</strong>g and evaluation characteristics.<br />
This report presents a brief analysis <strong>of</strong> the <strong>health</strong> care f<strong>in</strong>anc<strong>in</strong>g and delivery <strong>in</strong><br />
Jordan, assessment <strong>of</strong> the overall capacity for contract<strong>in</strong>g <strong>health</strong> services, and<br />
assessment <strong>of</strong> the <strong>contractual</strong> agreements between the M<strong>in</strong>istry <strong>of</strong> Health and other<br />
<strong>health</strong> care providers. Conclusions and recommendations are presented <strong>in</strong> the last<br />
section.<br />
OVERVIEW OF HEALTH CARE FINANCING AND DELIVERY IN JORDAN<br />
Socioeconomic background<br />
Jordan is low middle-<strong>in</strong>come country, with a population <strong>of</strong> 5.3 million <strong>in</strong> 2002.<br />
It is a relatively small country <strong>of</strong> only 91 100 km 2, 90% <strong>of</strong> which is desert. Its Gross<br />
Domestic Product (GDP) amounted to JD 6259 (US$ 9308) billion <strong>in</strong> 2002 with per<br />
capita <strong>in</strong>come <strong>of</strong> JD 1237 (US$ 1747). Approximately 40% <strong>of</strong> the population is under<br />
the age <strong>of</strong> 15 years, and the total fertility rate (TFR) is 3.7, one <strong>of</strong> the highest <strong>in</strong> the<br />
107
Jordan<br />
region. This, coupled with the cont<strong>in</strong>ued decl<strong>in</strong>e <strong>in</strong> <strong>in</strong>fant mortality (22 deaths per<br />
1000 live births for 2002) and the rise <strong>in</strong> life expectancy at birth (70.6 and 72.4 years<br />
for males and females, respectively), represents a significant social and economic<br />
challenge to the government (M<strong>in</strong>istry <strong>of</strong> Health Annual Book, 2002).<br />
Jordan has a small economy with limited natural resources, arid land mostly<br />
unsuitable for agriculture, and chronic water shortages. It imports most <strong>of</strong> the energy<br />
it consumes. <strong>The</strong> economic situation is aggravated by the political environment,<br />
which makes efforts to revive the economy difficult task. Although the GDP growth<br />
rate slightly improved between 2001 and 2002 (4.2% versus 4%), the cost <strong>of</strong> liv<strong>in</strong>g<br />
also <strong>in</strong>creased. <strong>The</strong> unemployment figure is still high between 14.7%–16% accord<strong>in</strong>g<br />
to different estimates. Nearly 12% <strong>of</strong> the Jordanian population is below the national<br />
poverty l<strong>in</strong>e (World Bank Group, 2002).<br />
Based on the commonly used development <strong>in</strong>dicators, Jordan fares better than<br />
most countries <strong>in</strong> the low–middle <strong>in</strong>come category. <strong>The</strong> majority <strong>of</strong> the population<br />
has access to basic <strong>in</strong>frastructure such as safe water, sanitation and electricity, and<br />
lives <strong>in</strong> permanent dwell<strong>in</strong>g structures. Government commitments to improve the<br />
overall quality <strong>of</strong> life and the social standards <strong>of</strong> its people have borne impressive<br />
results. Primary and secondary <strong>health</strong> care services are distributed all over the country<br />
with 98% to 100% population access to local <strong>health</strong> services (WHO, Country<br />
Pr<strong>of</strong>iles, 2003). <strong>The</strong> total literacy rate is 89.7% and Jordan has a well developed<br />
human resource base.<br />
Health <strong>sector</strong> brief<br />
Jordan has one <strong>of</strong> the most modern <strong>health</strong> care <strong>in</strong>frastructures <strong>in</strong> the Middle<br />
East. Jordan’s <strong>health</strong> system is a complex amalgam <strong>of</strong> three major <strong>sector</strong>s: public,<br />
private and donors. <strong>The</strong> public <strong>sector</strong> consists <strong>of</strong> two major public programmes that<br />
f<strong>in</strong>ance as well as deliver care: the M<strong>in</strong>istry <strong>of</strong> Health and Royal Medical Services.<br />
Other smaller public programmes <strong>in</strong>clude several university-based programmes, such<br />
as Jordan University Hospital <strong>in</strong> Amman and K<strong>in</strong>g Abdullah Hospital <strong>in</strong> Irbid. In<br />
2001, the total expenditure on <strong>health</strong> services accounted for about JD 598 million,<br />
9.5% <strong>of</strong> the GDP. Health expenditure per capita was JD 115 (Jordan’s National Health<br />
Accounts, Draft Report, 2004). Each <strong>of</strong> the <strong>health</strong> care sub-<strong>sector</strong>s has its own<br />
f<strong>in</strong>anc<strong>in</strong>g and delivery system that reflects directly on <strong>contractual</strong> <strong>arrangements</strong><br />
among these <strong>sector</strong>s. <strong>The</strong> follow<strong>in</strong>g description gives an <strong>in</strong>stitutional overview <strong>of</strong> the<br />
<strong>health</strong> care f<strong>in</strong>anc<strong>in</strong>g and delivery <strong>of</strong> each <strong>sector</strong>.<br />
M<strong>in</strong>istry <strong>of</strong> Health<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health is the major s<strong>in</strong>gle <strong>in</strong>stitution f<strong>in</strong>ancer and provider <strong>of</strong><br />
<strong>health</strong> care services <strong>in</strong> Jordan. It is the largest <strong>in</strong> terms <strong>of</strong> the size <strong>of</strong> its operation and<br />
utilization as compared to Royal Medical Services, Jordan University Hospital, K<strong>in</strong>g<br />
Abdullah Hospital, or others <strong>in</strong> the private <strong>sector</strong>. <strong>The</strong> M<strong>in</strong>istry owns and operates 27<br />
hospitals <strong>in</strong> 11 governorates, with 3462 hospital beds account<strong>in</strong>g for 37% <strong>of</strong> total<br />
108
Jordan<br />
hospital beds <strong>in</strong> Jordan. In terms <strong>of</strong> utilization, 44% <strong>of</strong> <strong>in</strong>patient care and 41% <strong>of</strong><br />
outpatient care occur with<strong>in</strong> its hospitals. <strong>The</strong> bed occupancy rate <strong>in</strong> M<strong>in</strong>istry<br />
hospitals was 72% for 2002 (MOH Statistical Book, 2002). <strong>The</strong> M<strong>in</strong>istry employs<br />
25% <strong>of</strong> all practis<strong>in</strong>g physicians <strong>in</strong> Jordan.<br />
In 2001 and 2002, the M<strong>in</strong>istry <strong>of</strong> Health budget accounted for 6% and 5.7% <strong>of</strong><br />
the general budget respectively (MOH, 2002). <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health is the largest<br />
M<strong>in</strong>istry <strong>in</strong> terms <strong>of</strong> expenditures, which accounted for 29.3% <strong>of</strong> total <strong>health</strong><br />
expenditures <strong>in</strong> 2001. Over 76% <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health expenditures are f<strong>in</strong>anced<br />
through the government budget, some 11% from <strong>in</strong>surance premiums from Civil<br />
Health Insurance en<strong>role</strong>es, and the rem<strong>in</strong>der from user charges and donors. In 2001,<br />
the M<strong>in</strong>istry <strong>of</strong> Health allocated 85% <strong>of</strong> its fund (JD 175 million) to facilities it owns<br />
and operates, and the rema<strong>in</strong><strong>in</strong>g amount (JD 26 million) was spent on reimburs<strong>in</strong>g<br />
private and other public providers for their services (Jordan’s National Health<br />
accounts, Draft Report, 2004).<br />
In addition to its general public <strong>health</strong> functions, the M<strong>in</strong>istry <strong>of</strong> Health has a<br />
dual f<strong>in</strong>anc<strong>in</strong>g function. First, it is responsible for adm<strong>in</strong>ister<strong>in</strong>g the Civil Health<br />
Insurance Plan (CHIP) which covers civil servants and their dependents. Individuals<br />
certified as poor, the disabled, children below the age <strong>of</strong> six years and blood donors<br />
are also formally covered under the CHIP, which covers a total <strong>of</strong> 20% <strong>of</strong> the<br />
population. Second, the M<strong>in</strong>istry is <strong>in</strong> effect the <strong>in</strong>surer <strong>of</strong> last resort for the entire<br />
population, s<strong>in</strong>ce any <strong>in</strong>dividual can come to the M<strong>in</strong>istry <strong>of</strong> Health facilities and pay<br />
highly subsidized rates (15% to 20% <strong>of</strong> the costs) for the entire range <strong>of</strong> M<strong>in</strong>istry<br />
services (World Bank Group, 1997)<br />
Royal Medical Services<br />
Royal Medical Services (RMS) is the second largest public programme <strong>in</strong> terms<br />
<strong>of</strong> expenditures (15% <strong>of</strong> total expenditures on <strong>health</strong> <strong>in</strong> 2001), but largest <strong>in</strong> terms <strong>of</strong><br />
<strong>in</strong>dividuals covered by <strong>health</strong> <strong>in</strong>surance. Its ma<strong>in</strong> <strong>role</strong> is to provide primary and<br />
curative <strong>health</strong> care to the armed forces through 5 outpatients centres and 10 ma<strong>in</strong><br />
hospitals spread all over the country. <strong>The</strong>se benefits are extended to the dependents <strong>of</strong><br />
military personnel, to public security and civil defence personnel and their<br />
dependents, and to retired personnel and their dependents. This system covers about<br />
1.52 million <strong>in</strong>dividuals, account<strong>in</strong>g for 29% <strong>of</strong> the population (RMS Annual Report,<br />
2002).<br />
RMS also acts as a referral centre through provid<strong>in</strong>g high quality care,<br />
<strong>in</strong>clud<strong>in</strong>g some complex procedures and specialty treatment to Jordanian (<strong>in</strong>clud<strong>in</strong>g<br />
M<strong>in</strong>istry <strong>of</strong> Health beneficiaries) and other patients. It plays a major <strong>role</strong> politically<br />
by send<strong>in</strong>g medical teams and field hospitals to disaster and conflict area such as<br />
Afghanistan, Croatia, Eritrea, Iraq and West Bank. <strong>The</strong> RMS has 1791 hospital beds<br />
(20% <strong>of</strong> total beds <strong>in</strong> Jordan) with occupancy rate <strong>of</strong> 76%. It employs 8% <strong>of</strong> all<br />
practis<strong>in</strong>g physicians (RMS Annual Report, 2002; MOH Annual Report, 2002).<br />
109
Jordan<br />
<strong>The</strong> RMS, like all other public providers, receives most <strong>of</strong> its annual budget (JD<br />
87 million <strong>in</strong> 2001) from the M<strong>in</strong>istry <strong>of</strong> F<strong>in</strong>ance, almost 61%. <strong>The</strong> rema<strong>in</strong><strong>in</strong>g source<br />
<strong>of</strong> funds comes from other government entities <strong>in</strong>clud<strong>in</strong>g the M<strong>in</strong>istry <strong>of</strong> Health<br />
(27.5%), households (9%), donors (1.1%) and private firms (1.4%), (Jordan’s<br />
National Health Accounts, Draft Report, 2004).<br />
Jordan University Hospital<br />
Jordan University Hospital (JUH) was established <strong>in</strong> 1971 under the name <strong>of</strong><br />
Amman Grand Hospital. Its name was changed <strong>in</strong> 1975 after it was affiliated with<br />
Jordan University and its medical school. With over 531 beds, its one <strong>of</strong> the most<br />
specialized and high-tech medical centres <strong>in</strong> the public <strong>sector</strong>, along with K<strong>in</strong>g<br />
Husse<strong>in</strong> Medical Centre and K<strong>in</strong>g Abdullah Hospital.<br />
JUH patients are referrals from the M<strong>in</strong>istry <strong>of</strong> Health, employees <strong>of</strong> Jordan<br />
University and their dependents, employees <strong>of</strong> private firms with whom JUH has<br />
<strong>contractual</strong> agreements, as well as some <strong>in</strong>dependent private patients. It has 5.8% <strong>of</strong><br />
the total number <strong>of</strong> hospital beds <strong>in</strong> Jordan and accounted for 3.8% <strong>of</strong> the hospital<br />
admissions for 2002 (MOH Statistical Book, 2002). JUH has an occupancy rate <strong>of</strong><br />
68% and employs 2% <strong>of</strong> physicians. Approximately 42% <strong>of</strong> the JUH revenue <strong>in</strong> 2002<br />
was from the M<strong>in</strong>istry <strong>of</strong> Health resources (Health Insurance Dept., 2002).<br />
K<strong>in</strong>g Abdullah Hospital<br />
K<strong>in</strong>g Abdullah Hospital (KAH) was established <strong>in</strong> 2002 by Jordan University <strong>of</strong><br />
Science and Technology (JUST). <strong>The</strong> total capacity <strong>of</strong> the hospital is 650 beds and the<br />
operat<strong>in</strong>g (opened beds) are 200 beds. <strong>The</strong> hospital serves as a teach<strong>in</strong>g hospital to the<br />
Faculty <strong>of</strong> Medic<strong>in</strong>e at JUST and as a referral hospital for all public <strong>sector</strong>s <strong>in</strong> the<br />
northern region. More than 85% <strong>of</strong> the hospital admissions are for patients referred by<br />
the M<strong>in</strong>istry <strong>of</strong> Health and the RMS (KAH Annual Report, 2002; HID Annual Report,<br />
2003). Thus, the two agencies are the ma<strong>in</strong> source <strong>of</strong> funds for KAH.<br />
United Nations Relief and Works Agency for Palest<strong>in</strong>e Refugees <strong>in</strong> the Near East<br />
<strong>The</strong> United Nations Relief and Works Agency for Palest<strong>in</strong>e Refugees <strong>in</strong> the<br />
Near East (UNRWA) is a relief and human development agency that was established<br />
by the United Nations General Assembly <strong>in</strong> 1949 to carry out direct relief works<br />
programmes for Palest<strong>in</strong>e refugees. It provides education, <strong>health</strong> care, social and<br />
emergency aid.<br />
UNRWA provides care to over 600 000 Palest<strong>in</strong>ian refugees <strong>in</strong> Jordan, many <strong>of</strong><br />
whom are also covered through the M<strong>in</strong>istry <strong>of</strong> Health and RMS (World Bank, 1997).<br />
UNRWA provides basically community-oriented <strong>health</strong> programmes that <strong>of</strong>fer<br />
comprehensive <strong>health</strong> care to eligible refugee population <strong>in</strong>clud<strong>in</strong>g preventive, and<br />
curative cure and family plann<strong>in</strong>g services. Its services also <strong>in</strong>clude school <strong>health</strong> and<br />
110
Jordan<br />
<strong>health</strong> education programmes. It also provides environmental <strong>health</strong> services to the<br />
refugee camps.<br />
Currently, UNRWA operates 23 <strong>health</strong> centres and maternal and child <strong>health</strong><br />
centres, 17 noncommunicable disease cl<strong>in</strong>ics, 23 family <strong>health</strong> cl<strong>in</strong>ics, 13 specialist<br />
cl<strong>in</strong>ics, 21 laboratories and 21 dental cl<strong>in</strong>ics. For <strong>in</strong>patient services, it used to contract<br />
with the M<strong>in</strong>istry <strong>of</strong> Health, RMS and some private hospitals for this service. UNRWA<br />
<strong>health</strong> expenditure amounted to almost JD 8 million <strong>in</strong> 2001 and accounted for 1.3% <strong>of</strong><br />
total <strong>health</strong> expenditures (Jordan’s National Health Accounts, Draft Report, 2004).<br />
Private <strong>sector</strong><br />
<strong>The</strong> private <strong>sector</strong> plays an important <strong>role</strong> <strong>in</strong> terms <strong>of</strong> both the f<strong>in</strong>anc<strong>in</strong>g and<br />
delivery <strong>of</strong> services. Many private firms provide <strong>health</strong> care coverage for their<br />
employees either through self <strong>in</strong>sur<strong>in</strong>g or the purchase <strong>of</strong> private <strong>health</strong> <strong>in</strong>surance.<br />
Accord<strong>in</strong>g to the Jordan’s National Health Accounts (JNHA), 49% <strong>of</strong> <strong>health</strong><br />
expenditure went to private <strong>sector</strong> physicians and hospitals <strong>in</strong> 2001. Many<br />
<strong>in</strong>dividuals, <strong>in</strong>clud<strong>in</strong>g those with public coverage, purchase services privately through<br />
direct out-<strong>of</strong>-pocket payment. <strong>The</strong> JNHA reported that the total out-<strong>of</strong> pocket<br />
expenditure from households amounted to JD 274 million <strong>in</strong> 2001. <strong>The</strong> private <strong>sector</strong><br />
received 81% <strong>of</strong> this amount, while the public <strong>sector</strong> received only 19%.<br />
In terms <strong>of</strong> service delivery, the private <strong>sector</strong> accounts for 36% <strong>of</strong> hospital<br />
beds and 59% <strong>of</strong> hospitals <strong>in</strong> Jordan, with an occupancy rate <strong>of</strong> 44%. In addition, the<br />
private <strong>sector</strong> employs 63% <strong>of</strong> all physicians, 94% <strong>of</strong> all pharmacists, 71% <strong>of</strong> all<br />
dentists, and 52% <strong>of</strong> all pr<strong>of</strong>essional physicians (MOH Statistical Book, 2002).<br />
<strong>The</strong> private <strong>sector</strong> conta<strong>in</strong>s much <strong>of</strong> the country’s advanced diagnostic capacity.<br />
This <strong>sector</strong> cont<strong>in</strong>ues to attract significant numbers <strong>of</strong> foreign patients from nearby<br />
Arab nations. <strong>The</strong> JNHA reported that the private <strong>sector</strong> received about US$ 600<br />
million <strong>in</strong> revenue from foreign patients <strong>in</strong> 2001. This <strong>sector</strong> under the absence <strong>of</strong><br />
strict regulatory environment is flourish<strong>in</strong>g and grow<strong>in</strong>g steadily.<br />
Pr<strong>of</strong>ile <strong>of</strong> the <strong>health</strong> subsystem<br />
Table 1 provides a brief overview <strong>of</strong> the Jordanian <strong>health</strong> <strong>sector</strong> <strong>in</strong> terms <strong>of</strong><br />
<strong>health</strong> services coverage, source <strong>of</strong> f<strong>in</strong>anc<strong>in</strong>g, prevail<strong>in</strong>g provider–payer<br />
relationships, and the size <strong>of</strong> each <strong>of</strong> the <strong>health</strong> care subsystems. This pr<strong>of</strong>ile serves as<br />
a background for better understand<strong>in</strong>g <strong>of</strong> the <strong>contractual</strong> <strong>arrangements</strong> among the<br />
various <strong>health</strong> care providers <strong>in</strong> Jordan.<br />
111
Table 1. Pr<strong>of</strong>iles <strong>of</strong> <strong>health</strong> subsystems <strong>in</strong> Jordan<br />
Benefits by <strong>health</strong><br />
subsystems<br />
Describes types <strong>of</strong> services<br />
and benefits available.<br />
Government services/M<strong>in</strong>istry <strong>of</strong> Health<br />
Provides comprehensive<br />
public <strong>health</strong> services;<br />
primary, preventive, and<br />
curative care through its<br />
facilities<br />
Performs the follow<strong>in</strong>g<br />
f<strong>in</strong>anc<strong>in</strong>g functions:<br />
Adm<strong>in</strong>isters Civil Health<br />
Insurance programme<br />
(CHIP)<br />
Insurer <strong>of</strong> last resort for the<br />
poor<br />
Jordan<br />
Coverage/special categories Pr<strong>in</strong>cipal f<strong>in</strong>anc<strong>in</strong>g<br />
source<br />
Describes coverage and<br />
eligibility criteria, special<br />
programmes for specific<br />
population groups.<br />
Civil servants and dependents;<br />
and <strong>in</strong>dividuals certified as poor,<br />
the disabled, children under age<br />
<strong>of</strong> six, and blood donors<br />
Highly subsidized primary and<br />
curative care for the entire<br />
population<br />
Describes ma<strong>in</strong><br />
sources <strong>of</strong> f<strong>in</strong>anc<strong>in</strong>g<br />
M<strong>in</strong>istry <strong>of</strong> F<strong>in</strong>ance<br />
(general tax<br />
revenues)<br />
M<strong>in</strong>istry <strong>of</strong> Social<br />
Affairs<br />
Services fees<br />
collected at <strong>health</strong><br />
facilities<br />
Co-payment for<br />
services and<br />
pharmaceuticals<br />
Payroll deductions<br />
Donor assistance<br />
World Bank loan<br />
112<br />
Provider–payer relationship Percentage <strong>of</strong><br />
population covered<br />
or eligible<br />
Describes relationship between<br />
f<strong>in</strong>anc<strong>in</strong>g and service delivery<br />
functions<br />
M<strong>in</strong>istry <strong>of</strong> Health <strong>in</strong>tegrated<br />
delivery system-services<br />
provided by government<br />
facilities f<strong>in</strong>anced through<br />
budget and salaried civil services<br />
staff<br />
Number <strong>of</strong> people<br />
covered or eligible by<br />
<strong>health</strong> system<br />
nationwide<br />
20% (persons enrolled<br />
<strong>in</strong> CHIP)<br />
Under public law,<br />
MOH is required to<br />
provide subsidized<br />
care to all Jordanian<br />
citizens<br />
Size <strong>of</strong> operation<br />
As <strong>in</strong>dicated by<br />
staff, beds, or<br />
number <strong>of</strong> facilities<br />
Operates<br />
53 comprehensive<br />
<strong>health</strong> centres<br />
336 primary <strong>health</strong><br />
centres<br />
258 village <strong>health</strong><br />
centres<br />
351 maternity and<br />
child <strong>health</strong> care<br />
centres<br />
247 dental cl<strong>in</strong>ics<br />
11 chest diseases<br />
centres<br />
27 hospitals<br />
3462 hospital beds<br />
(37%)
Jordan<br />
Benefits by <strong>health</strong> subsystems Coverage/special categories Pr<strong>in</strong>cipal f<strong>in</strong>anc<strong>in</strong>g<br />
source<br />
Royal Medical Services<br />
Primary and curative care<br />
services<br />
Jordan University Hospital<br />
Serves as a fee-for-service<br />
referral centre for other public<br />
programmes and private payers<br />
Owns and operates outpatient<br />
cl<strong>in</strong>ics and <strong>in</strong>patient facilities<br />
for primary and curative care<br />
K<strong>in</strong>g Abdullah Hospital<br />
Serves as a fee-for-service<br />
referral centre for other public<br />
programmes and private payers<br />
Owns and operates outpatient<br />
cl<strong>in</strong>ics and <strong>in</strong>patient facilities<br />
for primary and curative care<br />
Military personnel and their<br />
dependents<br />
Other referrals From MOH and<br />
<strong>contractual</strong> agreements with<br />
public firms<br />
Covers its employees and<br />
dependents<br />
Covers its employees and<br />
dependents<br />
Government budget<br />
User fees<br />
Premiums<br />
(based on army rank<br />
and status)<br />
M<strong>in</strong>or cost shar<strong>in</strong>g<br />
for pharmaceuticals<br />
M<strong>in</strong>istry <strong>of</strong> F<strong>in</strong>ance<br />
M<strong>in</strong>istry <strong>of</strong> Health<br />
User fees<br />
M<strong>in</strong>istry <strong>of</strong> F<strong>in</strong>ance<br />
M<strong>in</strong>istry <strong>of</strong> Health<br />
User fees<br />
RMS<br />
113<br />
Provider–payer relationship Percentage <strong>of</strong><br />
population covered<br />
or eligible<br />
Integrated delivery system<br />
compris<strong>in</strong>g RMS outpatient<br />
cl<strong>in</strong>ics and hospitals<br />
Referrals to MOH facilities<br />
Serves as fee-for-service<br />
referral centre for other public<br />
programmes and private payers<br />
Serves as fee-for-service<br />
referral centre for other public<br />
programmes and private payers<br />
Size <strong>of</strong> operation<br />
25.5% Operates:<br />
5 <strong>health</strong> centre<br />
10 hospitals<br />
1791 hospital beds<br />
(19.7%)<br />
1.33% Operates<br />
1 hospital<br />
531 beds (5.8%)<br />
1.0% Operates:<br />
1 hospital<br />
650 hospital beds (the<br />
hospital operates now<br />
200 beds only)
Benefits by <strong>health</strong> subsystems Coverage/special<br />
categories<br />
United Nations Relief Works Agency<br />
Owns and runs primary <strong>health</strong><br />
care centres<br />
Refers hospital care to the<br />
M<strong>in</strong>istry <strong>of</strong> Health or private<br />
facilities<br />
Private <strong>health</strong> <strong>sector</strong><br />
Owns and operates private<br />
cl<strong>in</strong>ics and hospitals for<br />
primary and curative care<br />
Own and operates pharmacies<br />
Provides care to 0.6 million<br />
Palest<strong>in</strong>ian refugees<br />
Beneficiaries <strong>of</strong> any private<br />
<strong>health</strong> plan self-<strong>in</strong>sured<br />
Company employees and<br />
their dependents<br />
All citizens with<br />
will<strong>in</strong>gness to pay<br />
Sources: Jordan National Health Account, Draft Report, 2004.<br />
M<strong>in</strong>istry <strong>of</strong> Health Annual Report, 2002.<br />
Jordan<br />
Pr<strong>in</strong>cipal f<strong>in</strong>anc<strong>in</strong>g<br />
source<br />
F<strong>in</strong>anced through<br />
outside donor<br />
contributions<br />
Direct out-<strong>of</strong>-pocket<br />
payment<br />
Payments from<br />
<strong>in</strong>surance plans<br />
Payments from<br />
employees and<br />
employers<br />
114<br />
Provider–payer relationship Percentage <strong>of</strong><br />
population covered<br />
or eligible<br />
Operates and owns primary<br />
<strong>health</strong> care cl<strong>in</strong>ics managed by<br />
its staff<br />
Private hospitals and cl<strong>in</strong>ics, by<br />
contract<br />
Fee-for-service, or through a<br />
third-party payer (<strong>in</strong>surance<br />
company or employer)<br />
Size <strong>of</strong> operation<br />
9% Operates<br />
23 <strong>health</strong> centres<br />
30 cl<strong>in</strong>ics<br />
23 family <strong>health</strong><br />
cl<strong>in</strong>ics<br />
21 dental cl<strong>in</strong>ics<br />
All citizens with<br />
will<strong>in</strong>gness to pay are<br />
eligible<br />
Operates:<br />
Number <strong>of</strong> cl<strong>in</strong>ics<br />
not available<br />
56 hospitals<br />
3402 hospital beds<br />
(36.2%)<br />
1564 pharmacies
Jordan<br />
Table 2. Summary <strong>of</strong> <strong>health</strong> expenditure statistics, Jordan, 2001<br />
Total population 5 182 000<br />
Total <strong>health</strong> care expenditures JD 597 834 320<br />
Per capita <strong>health</strong> care expenditures JD 1154<br />
Gross domestic product (GDP) JD 6 258 800 000<br />
Gross national product (GNP) JD 6 391 500 000<br />
Per capita GDP JD 1221<br />
Health care expenditures as percent <strong>of</strong> GDP 9.5%<br />
Health care expenditures as percent <strong>of</strong> GNP 9.4%<br />
Percentage <strong>of</strong> government<br />
budget allocated to <strong>health</strong><br />
9.6%<br />
Sources <strong>of</strong> <strong>health</strong> care f<strong>in</strong>anc<strong>in</strong>g (percent distribution)<br />
Public<br />
37.0%<br />
Private<br />
58.1%<br />
Donors<br />
Distribution <strong>of</strong> <strong>health</strong> expenditure<br />
4.9%<br />
Public<br />
45.0%<br />
Private<br />
48.7%<br />
UNRWA<br />
1.3<br />
Nongovernmental organizations<br />
5.1%<br />
Public <strong>health</strong> expenditure as percentage <strong>of</strong> GDP 3.5%<br />
Private <strong>health</strong> expenditure as percentage <strong>of</strong> GDP 5.6%<br />
International <strong>health</strong> expenditure as percentage <strong>of</strong> GDP 0.5%<br />
Total expenditure on pharmaceuticals JD 184 630 938<br />
Per capita pharmaceutical expenditure JD 35.6<br />
Pharmaceuticals as percentage <strong>of</strong> GDP<br />
Pharmaceuticals as percentage <strong>of</strong><br />
3.0%<br />
total <strong>health</strong> expenditure<br />
Distribution <strong>of</strong> pharmaceuticals expenditure<br />
30.9%<br />
Public<br />
18.5%<br />
Private<br />
81.5%<br />
Source: Jordan National Health Account, Draft Report, 2004.<br />
115
Table 3.Sources <strong>of</strong> funds to f<strong>in</strong>anc<strong>in</strong>g agents, JD, 2001<br />
F<strong>in</strong>anc<strong>in</strong>g Agents<br />
MOF MOP Other Government<br />
entities<br />
Jordan<br />
116<br />
Primary sources <strong>of</strong> funds<br />
Private firms Household UNRWA Other donors Total<br />
MOH 134 543 792 1 195 784 1 000 000 21 799 453 8 934 422 167 473 451<br />
RMS 53 917 300 393 700 23 996 600 1 180 000 5 601 360 85 088 960<br />
JUH 185 000 3 067 259 350 000 95 000 431 000 4 128 259<br />
Other Gov. Entities 2 478 000 2 478 000<br />
Public Universities 2 852 300 1 429 700 4 282 000<br />
Social Security 1 836 000 1 836 000<br />
Private Insurance Enterprises 21 688 716 1 934 612 23 623 328<br />
Household 241 940 021 241 940 021<br />
NGOs 8 868 413 8 868 413<br />
Private Firms 47 535 544 990 200 48,526,744<br />
Private Universities 1 022 850 712 150 1 735 000<br />
UNRWA 7 836 144 7 836 144<br />
Total 188 461 092 1 774 484 30 916 159 73 613 110 273 512 296 7 836 144 21 721 035 597 834 320<br />
Source: Jordan National Health Account, Draft Report, 2004.
Jordan<br />
ASSESSMENT OF OVERALL CAPACITY FOR CONTRACTING HEALTH<br />
SERVICES<br />
Introduction and rationale for contract<strong>in</strong>g<br />
S<strong>in</strong>ce 1970, private for-pr<strong>of</strong>it hospitals and other autonomous public <strong>sector</strong><br />
bodies, ma<strong>in</strong>ly the RMS, have witnessed remarkable expansion and development <strong>in</strong><br />
secondary and tertiary medical care. In contrast, the M<strong>in</strong>istry <strong>of</strong> Health hospitals have<br />
been less advantaged, less developed and under-funded. <strong>The</strong> government <strong>health</strong> care<br />
facilities provide highly subsidized (80%–85%) services for the un<strong>in</strong>sured and free <strong>of</strong><br />
charge services for the <strong>in</strong>sured and the poor. As M<strong>in</strong>istry facilities clearly form the<br />
backbone <strong>of</strong> the Jordanian hospital “safety net”, they have been over-burdened and<br />
have concentrated on primary and secondary medical care. <strong>The</strong> hospital bed<br />
occupancy at the M<strong>in</strong>istry <strong>of</strong> Health hospitals <strong>in</strong> major cities (Amman, Zerqa, Irbid)<br />
ranged from 78% to 83% <strong>in</strong> 2002, while the occupancy rate <strong>in</strong> private hospitals was<br />
44% (MOH Annual Report, 2002). <strong>The</strong>refore, the M<strong>in</strong>istry <strong>of</strong> Health has been heavily<br />
<strong>in</strong>volved dur<strong>in</strong>g the past three decades <strong>in</strong> contract<strong>in</strong>g with the private <strong>sector</strong> and other<br />
autonomous public <strong>sector</strong>s (i.e. RMS and JUH) to meet the <strong>health</strong> needs <strong>of</strong> its<br />
beneficiaries and un<strong>in</strong>sured poor people.<br />
This section assesses the overall capacity for contract<strong>in</strong>g out <strong>health</strong> services <strong>in</strong><br />
Jordan. <strong>The</strong> ma<strong>in</strong> topics covered <strong>in</strong>clude: the rationale for the M<strong>in</strong>istry <strong>of</strong> Health and<br />
other providers to contract; the political, legal, economic and social factors related to<br />
contract<strong>in</strong>g; the strengths and weaknesses <strong>of</strong> purchasers and providers; and the<br />
adm<strong>in</strong>istrative and technical capabilities <strong>of</strong> each party.<br />
<strong>The</strong> reasons beh<strong>in</strong>d the policy decision <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health <strong>in</strong> Jordan to<br />
contract out <strong>health</strong> services are related directly to the provision <strong>of</strong> <strong>health</strong> services or<br />
to <strong>health</strong> and social policy.<br />
Reasons related to the provision <strong>of</strong> services <strong>in</strong>clude:<br />
Unavailability <strong>of</strong> services (mostly tertiary level services as: cardiology and<br />
cardiovascular surgery, neurosurgery, plastic and constructive surgery, organ<br />
transplants, etc…)<br />
Shortage <strong>of</strong> beds, ma<strong>in</strong>ly <strong>in</strong> Amman, Zerqa and Irbid.<br />
Shortage <strong>of</strong> private rooms.<br />
Emergency cases.<br />
Patients’ preference (restricted for some private hospitals and usually <strong>in</strong>volves copayment).<br />
Lack <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health hospitals (Aqaba, Taffilah, some areas <strong>in</strong> Amman).<br />
Shortage <strong>of</strong> diagnostic facilities.<br />
Shortage <strong>of</strong> medic<strong>in</strong>e.<br />
Long wait<strong>in</strong>g lists.<br />
With regard to <strong>health</strong> policy reasons for contract<strong>in</strong>g out <strong>in</strong>clude:<br />
117
Jordan<br />
• Enhanc<strong>in</strong>g equity by referr<strong>in</strong>g <strong>in</strong>sured patients to other <strong>sector</strong>s <strong>in</strong> order to provide<br />
access to the M<strong>in</strong>istry <strong>of</strong> Health services for poor and disadvantaged people who<br />
cannot afford treatment cost <strong>in</strong> private hospitals.<br />
• Tak<strong>in</strong>g <strong>in</strong>to consideration the high unemployment rate (16%) and the high<br />
percentage (12%) <strong>of</strong> people below the poverty l<strong>in</strong>e, contract<strong>in</strong>g out <strong>health</strong><br />
services is becom<strong>in</strong>g a social policy tool <strong>in</strong> Jordan.<br />
• Conta<strong>in</strong><strong>in</strong>g <strong>health</strong> costs by us<strong>in</strong>g underutilized hospital beds <strong>in</strong> private and other<br />
public <strong>sector</strong>s, <strong>in</strong>stead <strong>of</strong> <strong>in</strong>vest<strong>in</strong>g <strong>in</strong> build<strong>in</strong>g new hospitals.<br />
• Provid<strong>in</strong>g <strong>in</strong>centives for private hospitals to stay <strong>in</strong> the bus<strong>in</strong>ess and develop their<br />
services to attract more patients from other countries. This will have a positive<br />
impact on macroeconomic level and <strong>in</strong>crease the national <strong>in</strong>come from “medical<br />
tourism” which was about JD 400 million <strong>in</strong> 2002.<br />
• Reliev<strong>in</strong>g the M<strong>in</strong>istry <strong>of</strong> Health <strong>of</strong> the provision <strong>of</strong> some highly specialized<br />
medical services that require costly <strong>in</strong>vestment <strong>of</strong> capital and human resources.<br />
This will allow the M<strong>in</strong>istry <strong>of</strong> Health to divert resources, develop and extend<br />
primary <strong>health</strong> care services.<br />
• Chang<strong>in</strong>g the negative <strong>role</strong> <strong>of</strong> the government towards private hospitals to a more<br />
positive and supportive <strong>role</strong>. Instead <strong>of</strong> buy<strong>in</strong>g the bankrupt private hospitals (e.g.<br />
Queen Alia Hospital <strong>in</strong> Amman, Al-Nadim Hospital <strong>in</strong> Madaba, and the Specialty<br />
Hospital <strong>in</strong> Mafraq) the government policy now encourages purchas<strong>in</strong>g services<br />
from private hospitals to help them prosper and stay <strong>in</strong> bus<strong>in</strong>ess.<br />
• Build<strong>in</strong>g partnership between the public and private <strong>sector</strong>s based on serv<strong>in</strong>g<br />
mutual <strong>in</strong>terests <strong>of</strong> both parties.<br />
Reasons for the private <strong>sector</strong> to enter <strong>in</strong>to <strong>contractual</strong> <strong>arrangements</strong> with the<br />
M<strong>in</strong>istry <strong>of</strong> Health <strong>in</strong>clude the follow<strong>in</strong>g.<br />
• Fully utiliz<strong>in</strong>g the bed capacity (1905 beds) and the advanced diagnostic<br />
technology <strong>in</strong> private hospitals <strong>in</strong> order to achieve better return for <strong>in</strong>vestment<br />
and <strong>in</strong>crease net pr<strong>of</strong>it.<br />
• Ensur<strong>in</strong>g regular cashflow to meet recurrent hospital expenses.<br />
• Strengthen<strong>in</strong>g the competitive situation <strong>of</strong> the private hospital. It is considered as<br />
government accreditation.<br />
• Secur<strong>in</strong>g a stable and cont<strong>in</strong>uous revenue. Contract<strong>in</strong>g with the public <strong>sector</strong><br />
<strong>in</strong>creases the revenue mix <strong>of</strong> the private hospitals and safeguards them aga<strong>in</strong>st<br />
economic fluctuation.<br />
Political and legal environment<br />
Jordan began adopt<strong>in</strong>g a liberal economic policy as early as 1985 based on the<br />
redef<strong>in</strong>ition <strong>of</strong> the <strong>role</strong>s <strong>of</strong> the government and the private <strong>sector</strong>. <strong>The</strong> primary<br />
responsibility is be<strong>in</strong>g assigned to the government for supervision, follow-up,<br />
regulation, safeguard<strong>in</strong>g rights and ensur<strong>in</strong>g equality <strong>of</strong> opportunities and<br />
competition. In 1996, the Jordanian privatization programme was <strong>of</strong>ficially<br />
announced. <strong>The</strong> ma<strong>in</strong> objectives <strong>of</strong> the programme were: attract<strong>in</strong>g private<br />
<strong>in</strong>vestment; improv<strong>in</strong>g the efficiency <strong>of</strong> enterprise; and develop<strong>in</strong>g the local market to<br />
118
Jordan<br />
attract foreign <strong>in</strong>vestment, technology and know-how. Strengthen<strong>in</strong>g public–private<br />
partnership is one <strong>of</strong> the major policy directions <strong>of</strong> his majesty K<strong>in</strong>g Abdullah to<br />
successive governments.<br />
Privatization and partnership policies <strong>in</strong> Jordan are not <strong>in</strong>tended to replace the<br />
traditional <strong>role</strong> <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health <strong>in</strong> the provision <strong>of</strong> <strong>health</strong> services. Rather,<br />
they aim to complement this <strong>role</strong> by open<strong>in</strong>g wide doors <strong>in</strong>to the private <strong>sector</strong> to<br />
utilize its <strong>health</strong> resources <strong>in</strong> an effective and efficient way that reflects positively on<br />
both parties and on the overall economy <strong>of</strong> the country.<br />
Contract<strong>in</strong>g out services with the private <strong>sector</strong> is used by the government, to<br />
extend highly subsidized and free the M<strong>in</strong>istry <strong>of</strong> Health services to the poor and the<br />
vulnerable. <strong>The</strong> <strong>in</strong>creas<strong>in</strong>g number <strong>of</strong> contracts between the M<strong>in</strong>istry <strong>of</strong> Health over<br />
the past three years (e.g. K<strong>in</strong>g Abdullah Hospital, Al-Husse<strong>in</strong> Cancer Centre, Lozmila<br />
Hospital, Al-Mowasah Hospital, Al-Hayah Hospital) is evidence <strong>of</strong> the high political<br />
commitment towards the execution <strong>of</strong> <strong>contractual</strong> agreements.<br />
<strong>The</strong> exist<strong>in</strong>g legal mandates and regulations give authority to the M<strong>in</strong>istry <strong>of</strong><br />
Health to contract with private and autonomous public <strong>health</strong> providers. This legal<br />
authority is stated explicitly <strong>in</strong> Article 26 <strong>of</strong> the Civil Health Insurance law number<br />
10, issued <strong>in</strong> 1983. This article reads: “<strong>The</strong> M<strong>in</strong>ister <strong>of</strong> Health has the authority to<br />
contract out <strong>health</strong> services with private and autonomous public <strong>sector</strong>s (hospitals,<br />
doctors, laboratories, etc.) to provide <strong>health</strong> services for CHIP enrollees.”<br />
Article 4 <strong>of</strong> the high Health Council Law states that the Council should develop<br />
policies to strengthen the partnership between public and private <strong>health</strong> <strong>sector</strong>s and<br />
ensure that the two <strong>sector</strong>s complete and support each other. Policy number 6 <strong>in</strong> the<br />
Strategic Health Plan for 2004–2006 reflects high commitment <strong>of</strong> the government<br />
towards build<strong>in</strong>g robust relationships among the different <strong>health</strong> <strong>sector</strong>s to provide<br />
high quality, effective and efficient <strong>health</strong> services. <strong>The</strong> plan <strong>in</strong>cludes for the first time<br />
some projects related to the private <strong>sector</strong>.<br />
Jordan also has an advanced and <strong>in</strong>dependent judicial system. <strong>The</strong> Jordanian<br />
Constitution guarantees the <strong>in</strong>dependence <strong>of</strong> the judicatory authority. Thus, there are<br />
efficient and transparent mechanisms to recourse <strong>in</strong> the event <strong>of</strong> a dispute between the<br />
M<strong>in</strong>istry <strong>of</strong> Health and any contract<strong>in</strong>g partner.<br />
M<strong>in</strong>istry <strong>of</strong> Health capabilities, strengths and weaknesses regard<strong>in</strong>g contract<strong>in</strong>g<br />
Due to its accumulated experience <strong>in</strong> contract<strong>in</strong>g, the M<strong>in</strong>istry <strong>of</strong> Health has<br />
developed essential adm<strong>in</strong>istrative and f<strong>in</strong>ancial skills <strong>in</strong> contract management over<br />
time, especially with<strong>in</strong> the Health Insurance Directorate (HID). <strong>The</strong> majority <strong>of</strong> the<br />
exist<strong>in</strong>g <strong>contractual</strong> <strong>arrangements</strong> are merely agreement protocols that lack<br />
competitive bidd<strong>in</strong>g procedures, performance evaluation or <strong>in</strong>tegrated computerized<br />
<strong>in</strong>formation systems. <strong>The</strong>refore, most <strong>of</strong> the experience accumulated <strong>in</strong> the HID is<br />
limited to review<strong>in</strong>g providers’ claims, process<strong>in</strong>g reimbursement transactions and<br />
119
Jordan<br />
monitor<strong>in</strong>g adm<strong>in</strong>istrative <strong>arrangements</strong> to ensure that providers adhere to the<br />
conditions specified <strong>in</strong> each agreement.<br />
<strong>The</strong> fee-for-service system, which is prom<strong>in</strong>ent at the M<strong>in</strong>istry <strong>of</strong> Health,<br />
creates <strong>in</strong>centive for conduct<strong>in</strong>g multiple, sometimes unnecessary procedures, as well<br />
as over-bill<strong>in</strong>g by providers. As this type <strong>of</strong> payment mechanisms has proved to be<br />
less efficient worldwide and does not promote equity and quality (Hsiao W., 1997),<br />
the M<strong>in</strong>istry <strong>of</strong> Health has <strong>in</strong>troduced new payment mechanisms such as leas<strong>in</strong>g<br />
private hospital beds for a fixed payment per bed or a def<strong>in</strong>ed payment for a bundle<br />
fee per episode. <strong>The</strong> HID has also <strong>in</strong>itiated steps to computerize its entire account<strong>in</strong>g<br />
system and network it with other governorates.<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health, with technical support from PHRplus project (funded by<br />
USAID), is now implement<strong>in</strong>g a Health Insurance Pilot Project (HIPP) to expand the<br />
adm<strong>in</strong>istrative and technical capacity <strong>of</strong> the staff <strong>of</strong> the HID <strong>in</strong> the areas <strong>of</strong> contract<br />
design, contract monitor<strong>in</strong>g and contract enforcement. This pilot project is based open<br />
bidd<strong>in</strong>g procedures and is expected also to have a positive impact on improv<strong>in</strong>g<br />
contract<strong>in</strong>g skills <strong>of</strong> private hospitals.<br />
<strong>The</strong> exist<strong>in</strong>g bureaucratic set-up <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health does not provide the<br />
Health Insurance Directorate (HID) with sufficient authority and flexibility to manage<br />
contracts efficiently. <strong>The</strong> laws govern<strong>in</strong>g the HID are <strong>in</strong>flexible and the decisions<br />
related to <strong>contractual</strong> <strong>arrangements</strong>, <strong>in</strong>clud<strong>in</strong>g reimbursement rates, are taken at the<br />
central level <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health. <strong>The</strong> civil <strong>health</strong> <strong>in</strong>surance budget is also<br />
managed at the central level and it is outside the control <strong>of</strong> its managers. This<br />
exogenous budget<strong>in</strong>g system affords very little control or <strong>in</strong>dependence <strong>in</strong> f<strong>in</strong>ancial<br />
decision-mak<strong>in</strong>g or monitor<strong>in</strong>g expenditures (Jordan’s National Health Accounts,<br />
Draft Report, 2004)<br />
Some genu<strong>in</strong>e efforts have been made recently by the HID to undertake cost<br />
and price analysis prior to negotiations for new contracts. <strong>The</strong> lack <strong>of</strong> comprehensive<br />
and advanced computerized <strong>in</strong>formation system is a real obstacle fac<strong>in</strong>g the<br />
development <strong>of</strong> these efforts. Capacity to undertake a price and cost analysis also<br />
needs urgent strengthen<strong>in</strong>g <strong>in</strong> order to expand <strong>health</strong> <strong>in</strong>surance coverage through<br />
<strong>health</strong> <strong>in</strong>surance reform which is considered now a top national <strong>health</strong> priority.<br />
Monitor<strong>in</strong>g and controll<strong>in</strong>g the quality <strong>of</strong> the contracted services is one <strong>of</strong> the<br />
major challenges fac<strong>in</strong>g the M<strong>in</strong>istry <strong>of</strong> Health. Current monitor<strong>in</strong>g procedures for<br />
contracts are not efficient, especially for measur<strong>in</strong>g the quality and appropriateness <strong>of</strong><br />
the <strong>health</strong> services provided by the private <strong>sector</strong>.<br />
Private <strong>sector</strong> capabilities, strengths and weaknesses regard<strong>in</strong>g contract<strong>in</strong>g<br />
Compared with the public <strong>sector</strong>, the private <strong>sector</strong> has better capabilities and<br />
experience <strong>in</strong> terms <strong>of</strong> technical and f<strong>in</strong>ancial management capacity. Most private<br />
hospitals have <strong>in</strong>troduced computerized <strong>in</strong>formation systems to manage their<br />
120
Jordan<br />
bus<strong>in</strong>esses efficiently. <strong>The</strong> managers <strong>of</strong> the private hospitals are more powerful and<br />
can adapt easily to the chang<strong>in</strong>g environment. S<strong>in</strong>ce 55% <strong>of</strong> the country <strong>health</strong><br />
expenditures are <strong>in</strong> the private <strong>sector</strong>, this <strong>sector</strong> has developed <strong>contractual</strong><br />
<strong>arrangements</strong> with different <strong>in</strong>surance companies, third party adm<strong>in</strong>istrators and<br />
private firms. <strong>The</strong>refore, private hospitals have better contract<strong>in</strong>g skills and f<strong>in</strong>ancial<br />
management that could reflect positively on its partnership with the public <strong>sector</strong>.<br />
<strong>The</strong> follow<strong>in</strong>g are the ma<strong>in</strong> strengths and weaknesses <strong>of</strong> the private <strong>sector</strong> that<br />
should be taken <strong>in</strong>to consideration when enter<strong>in</strong>g <strong>in</strong>to a <strong>contractual</strong> agreement:<br />
Strengths:<br />
Advanced medical equipment <strong>of</strong> large hospitals.<br />
Skilled technical workforce.<br />
Good reputation outside Jordan, s<strong>in</strong>ce one third <strong>of</strong> private hospitals’ revenue is<br />
from foreign patients.<br />
Good quality services especially hotel services.<br />
Relatively advanced computerized <strong>in</strong>formation system, especially f<strong>in</strong>ancial and<br />
management systems.<br />
Good experience <strong>in</strong> negotiat<strong>in</strong>g contracts, especially with private <strong>health</strong><br />
<strong>in</strong>surance companies.<br />
Weaknesses:<br />
Most private hospital beds (75%) are located <strong>in</strong> Amman (ma<strong>in</strong>ly <strong>in</strong> West<br />
Amman).<br />
Cashflow problems.<br />
Low bed occupancy rate (44%).<br />
Excess capacity <strong>in</strong> certa<strong>in</strong> medical equipment and services.<br />
Less advanced equipment for small hospitals compared with large hospitals.<br />
Shortage <strong>of</strong> qualified nurses and paramedical personnel.<br />
Lack <strong>of</strong> treatment protocols and systematic quality control programmes.<br />
Inefficient <strong>role</strong> <strong>of</strong> the Private Hospital Association.<br />
Lack <strong>of</strong> skilled and pr<strong>of</strong>essional managers.<br />
Inefficient cooperation with<strong>in</strong> the <strong>sector</strong>.<br />
A strategic analysis show<strong>in</strong>g strengths, weaknesses, threats and opportunities<br />
(SWOT) <strong>of</strong> the private <strong>sector</strong> is given <strong>in</strong> detail <strong>in</strong> Figure 1.<br />
121
• Advanced medical equipment <strong>of</strong> large<br />
hospitals.<br />
• Skilled technical workforce.<br />
• Good reputation outside Jordan, s<strong>in</strong>ce<br />
32% <strong>of</strong> hospital revenues are from<br />
foreign patients.<br />
• More quality services compared with<br />
government hospitals.<br />
Direct effect<br />
Outside environmental effect<br />
• Relations with other players <strong>in</strong> the <strong>sector</strong><br />
(public <strong>sector</strong>, <strong>in</strong>surance and<br />
pharmaceutical companies).<br />
• Mislead<strong>in</strong>g <strong>in</strong>formation regard<strong>in</strong>g the<br />
performance <strong>of</strong> private hospitals.<br />
• Laws and regulations that organize the<br />
<strong>sector</strong> with related parties.<br />
• Low <strong>in</strong>come levels per capita.<br />
• Potential competition.<br />
Jordan<br />
Jordanian private hospitals<br />
• Inefficient <strong>role</strong> for the Private Hospitals Association.<br />
• Cash flow problems.<br />
• Shortage <strong>in</strong> qualified nurses.<br />
• Less advanced equipment for the small hospitals<br />
compared with large hospitals.<br />
• Excess capacity and overlapp<strong>in</strong>g <strong>in</strong> certa<strong>in</strong> medical<br />
equipment and services.<br />
• <strong>The</strong> bed occupancy rates are low (44%) compared with<br />
other <strong>health</strong> services providers.<br />
• Lack <strong>of</strong> skilled management expertise.<br />
• Inefficient cooperation with<strong>in</strong> the <strong>sector</strong>.<br />
Source: Adapted from Deloitte & Touché (M.E.) “F<strong>in</strong>ancial and Regulatory Study <strong>of</strong> Jordanian Private Hospitals”,<br />
2001.<br />
Figure 1. Strategic analysis <strong>of</strong> the private hospital <strong>sector</strong> <strong>in</strong> Jordan<br />
122<br />
Direct effect<br />
Outside environmental effect<br />
• Privatization <strong>of</strong> public <strong>in</strong>stitution creates<br />
additional demand on private hospital <strong>sector</strong>.<br />
• <strong>The</strong> Higher Health Council, headed by the<br />
Prime M<strong>in</strong>ister, is determ<strong>in</strong>ed to regulate the<br />
hospital <strong>sector</strong> to ma<strong>in</strong>ta<strong>in</strong> its competence and<br />
excellence on the regional level.<br />
• <strong>The</strong> implementation <strong>of</strong> a national <strong>health</strong><br />
<strong>in</strong>surance plan is expected to <strong>in</strong>crease demand<br />
on <strong>health</strong> care services, which will directly<br />
<strong>in</strong>fluence the performance <strong>of</strong> private<br />
hospitals.<br />
• Investment <strong>in</strong>centives and tax exemptions.
Expected risks and <strong>in</strong>centives<br />
M<strong>in</strong>istry <strong>of</strong> Health<br />
Risks<br />
Jordan<br />
• <strong>The</strong> amount <strong>of</strong> f<strong>in</strong>ancial claims from contracted hospitals may exceed the amount<br />
allocated <strong>in</strong> HID budget.<br />
• <strong>The</strong> tendency <strong>of</strong> the private hospitals to provide unnecessary or low quality <strong>health</strong><br />
services to maximize revenues.<br />
• Some private qualified providers may be reluctant to participate <strong>in</strong> the contract<strong>in</strong>g<br />
process due to anxiety over work<strong>in</strong>g with the public <strong>sector</strong>.<br />
• <strong>The</strong>re is a possibility that private providers may change their behaviour and give<br />
priority to private patients. This may create long wait<strong>in</strong>g lists and <strong>in</strong>crease<br />
wait<strong>in</strong>g time for the M<strong>in</strong>istry <strong>of</strong> Health patients.<br />
• <strong>The</strong>re is a possibility that some political parties may misunderstand the objectives<br />
<strong>of</strong> the government from contract<strong>in</strong>g. <strong>The</strong>y may consider contract<strong>in</strong>g as a way <strong>of</strong><br />
“privatiz<strong>in</strong>g” <strong>health</strong> care and allow<strong>in</strong>g government to avoid its responsibilities to<br />
provide services for the poor.<br />
Incentives<br />
• Improves accessibility for the M<strong>in</strong>istry <strong>of</strong> Health beneficiaries and poor patients.<br />
• Decreases pressure on and over-utilization <strong>of</strong> M<strong>in</strong>istry <strong>of</strong> Health facilities,<br />
especially <strong>in</strong> Amman.<br />
• Optimizes the utilization <strong>of</strong> <strong>health</strong> care resources <strong>in</strong> the country.<br />
• Could provide, if well negotiated and managed, better quality services with less<br />
cost.<br />
• Builds skills and experience <strong>in</strong> negotiation, preparation, management, monitor<strong>in</strong>g<br />
and evaluation <strong>of</strong> contracts.<br />
Private <strong>sector</strong><br />
Risks<br />
• Delay <strong>in</strong> accounts settlement due to bureaucratic procedures or shortage <strong>of</strong><br />
budget allocations.<br />
• Due to competition, discounted contract prices may not be economically feasible.<br />
• Abrupt changes <strong>in</strong> government directions could <strong>in</strong>cur f<strong>in</strong>ancial loss for private<br />
hospitals.<br />
Incentives<br />
• Increas<strong>in</strong>g bed occupancy rates and revenues.<br />
• Acquir<strong>in</strong>g public f<strong>in</strong>anc<strong>in</strong>g and cash flow.<br />
• Improv<strong>in</strong>g the competitive position <strong>of</strong> the hospital.<br />
123
Jordan<br />
ASSESSMENT OF THE CONTRACTUAL ARRANGEMENTS BETWEEN<br />
THE MINISTRY OF HEALTH AND OTHER HEALTH CARE PROVIDERS<br />
Overview<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health has more than 10 contracts/agreements with private<br />
hospitals and autonomous public providers, as shown <strong>in</strong> Table 4. Accord<strong>in</strong>g to these<br />
contracts, hospital services are provided to M<strong>in</strong>istry <strong>of</strong> Health beneficiaries accord<strong>in</strong>g<br />
to the terms specified <strong>in</strong> each contract and funds are transferred by the M<strong>in</strong>istry <strong>of</strong><br />
Health to each provider, as shown <strong>in</strong> Figure 2. <strong>The</strong> Health Insurance Directorate<br />
(HID) manages these contracts and agreements on behalf <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health.<br />
<strong>The</strong> management process <strong>in</strong>cludes negotiat<strong>in</strong>g, specify<strong>in</strong>g terms and conditions <strong>of</strong> the<br />
contract or agreement, controll<strong>in</strong>g and monitor<strong>in</strong>g performance, review<strong>in</strong>g and<br />
authoriz<strong>in</strong>g claims and reimbursement.<br />
<strong>The</strong> different <strong>contractual</strong> <strong>arrangements</strong> between the M<strong>in</strong>istry <strong>of</strong> Health and<br />
other <strong>health</strong> care providers may be grouped <strong>in</strong>to three categories accord<strong>in</strong>g to method<br />
<strong>of</strong> payment:<br />
1) Fee-for-service contracts<br />
Royal Medical Services.<br />
Jordan University Hospital.<br />
K<strong>in</strong>g Abdallah Hospital.<br />
Al-Husse<strong>in</strong> Cancer Centre.<br />
Lozmila Hospital.<br />
Crescent Hospital.<br />
Other private hospitals (for emergency cases only).<br />
2) Bed leas<strong>in</strong>g contracts<br />
Al-Mowasah Hospital.<br />
Al-Hayah Hospital.<br />
3) Bundl<strong>in</strong>g <strong>of</strong> services contracts.<br />
124
Jordan<br />
Table 4. Pr<strong>of</strong>ile <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> between the M<strong>in</strong>istry <strong>of</strong> Health and other <strong>health</strong> care providers<br />
Provider Type <strong>of</strong><br />
provider<br />
Date <strong>of</strong><br />
contract<br />
Length<br />
<strong>of</strong><br />
contract<br />
RMS Public/military 1982 Open Tertiary/secondary<br />
levels<br />
JUH Public/university 1973 Open Tertiary/secondary<br />
levels<br />
Al-<br />
Husse<strong>in</strong><br />
Cancer<br />
Centre<br />
Philanthropy/notfor-pr<strong>of</strong>it<br />
2001 Annual Haematology and<br />
cancer cases<br />
KAH Public/university 2002 Annual Ma<strong>in</strong>ly tertiary<br />
level<br />
Al-<br />
Mowasah<br />
and Al-<br />
Hayah<br />
Hospitals<br />
Lozmila<br />
Hospital<br />
Red<br />
Crescent<br />
Hospital<br />
Other<br />
private<br />
hospitals<br />
Private/for pr<strong>of</strong>it July<br />
/2003<br />
Services covered Geographical<br />
scope <strong>of</strong><br />
contract<br />
Annual Ma<strong>in</strong>ly secondary<br />
(General<br />
medic<strong>in</strong>e+ General<br />
Surgery<br />
Private/for pr<strong>of</strong>it 2001 Annual Secondary care<br />
level<br />
Philanthropy/notfor-pr<strong>of</strong>it<br />
1999 Annual Secondary care<br />
level<br />
125<br />
Payment<br />
mechanism<br />
All regions Fee-for-service<br />
(30% discount)<br />
All regions Fee-for-service<br />
(25% discount)<br />
All regions Fee-for-service<br />
(25% discount)<br />
North regions Fee-for-service<br />
(25% discount)<br />
East Amman Bed leas<strong>in</strong>g (all<br />
services<br />
<strong>in</strong>cluded/MOH<br />
specialist<br />
physicians<br />
provide care for<br />
referred patients)<br />
Amman area Fee-for-service<br />
(25% discount)<br />
Amman area Fee-for-service<br />
(30% discount) +<br />
prospective (per<br />
case)<br />
Copayment<br />
Performance<br />
measures<br />
Management<br />
and f<strong>in</strong>ancial<br />
effort<br />
------- ------ High 5<br />
If selfreferred<br />
------ High 11<br />
----- ------ High 1.7<br />
If self<br />
referred<br />
------<br />
------ Direct<br />
supervision<br />
and monitor<strong>in</strong>g<br />
<strong>of</strong> M<strong>in</strong>istry <strong>of</strong><br />
Health<br />
physicians<br />
If self<br />
referred<br />
If self<br />
referred<br />
High 6<br />
Low 1.5<br />
------ High 0.5<br />
------ High 0.4<br />
Private/for pr<strong>of</strong>it ------ ------ Emergency cases All regions Fee-for-service ------ ------ Very High 6<br />
Annual<br />
cost/JD<br />
million
Other private<br />
hospitals<br />
Al-Husse<strong>in</strong> Cancer<br />
Centre<br />
Flow <strong>of</strong> Services<br />
Flow <strong>of</strong> Funds<br />
RMS<br />
Jordan<br />
M<strong>in</strong>istry <strong>of</strong> Health<br />
KAH<br />
Figure 2. Contractual <strong>arrangements</strong> between the M<strong>in</strong>istry <strong>of</strong> Health and other <strong>health</strong> care providers<br />
126<br />
JUH<br />
Al-Mowasah and<br />
Al-Hayah<br />
hospitals<br />
Lozmila and Red<br />
Crescent hospitals
Fee-for-service contracts<br />
Royal Medical Services<br />
Jordan<br />
<strong>The</strong> agreement with Royal Medical Services (RMS) was signed <strong>in</strong> 1982. It def<strong>in</strong>es and<br />
organizes the relationship between the ma<strong>in</strong> two public providers <strong>of</strong> <strong>health</strong> care <strong>in</strong> the country.<br />
Accord<strong>in</strong>g to this agreement, patients and funds flow from both directions (Figure 2). Thus,<br />
beneficiaries <strong>of</strong> civil and military <strong>health</strong> schemes can have access with<strong>in</strong> certa<strong>in</strong> conditions, to<br />
the M<strong>in</strong>istry <strong>of</strong> Health and RMS <strong>health</strong> facilities.<br />
Ma<strong>in</strong> features<br />
• Beneficiaries <strong>of</strong> the Civil Health Insurance Plan (CHIP) may be referred by the M<strong>in</strong>istry <strong>of</strong><br />
Health hospitals for treatment at K<strong>in</strong>g Husse<strong>in</strong> Medical Centre.<br />
• Beneficiaries <strong>of</strong> the CHIP who live <strong>in</strong> Aqaba and Tafilah governorates are treated at RMS<br />
hospitals (M<strong>in</strong>istry <strong>of</strong> Health does not have hospitals <strong>in</strong> either governorate).<br />
• Beneficiaries <strong>of</strong> the Military Health Insurance Plan (MHIP) are treated at any M<strong>in</strong>istry <strong>of</strong><br />
Health <strong>health</strong> centres near their residence.<br />
• Beneficiaries <strong>of</strong> the MHIP can be treated <strong>in</strong> the M<strong>in</strong>istry <strong>of</strong> Health hospitals <strong>in</strong> cities that lack<br />
RMS hospitals (i.e. Ajlun, Ma’an, Jarash, Mafraq).<br />
• Charges will be paid by each party accord<strong>in</strong>g to fee-for-service as specified <strong>in</strong> the <strong>of</strong>ficial fee<br />
schedule for the M<strong>in</strong>istry <strong>of</strong> Health and RMS, with 30% discount.<br />
• Emergency cases for beneficiaries <strong>of</strong> both sides are treated <strong>in</strong> the M<strong>in</strong>istry <strong>of</strong> Health or RMS<br />
facilities.<br />
• A jo<strong>in</strong>t committee from both sides meets every three months or ad hoc to review claims,<br />
settle accounts and resolve problems.<br />
• <strong>The</strong> annual f<strong>in</strong>ancial balance for the past three years has been almost zero, with a total cost <strong>of</strong><br />
approximately JD 5 million for each party.<br />
Strengths<br />
• Improves patients’ access to M<strong>in</strong>istry <strong>of</strong> Health and RMS <strong>health</strong> facilities.<br />
• Improves equity to beneficiaries from both parties by giv<strong>in</strong>g them the chance to benefit from<br />
<strong>health</strong> resources available at the M<strong>in</strong>istry <strong>of</strong> Health and RMS facilities.<br />
• M<strong>in</strong>imizes duplication <strong>of</strong> services and improves economic efficiency <strong>in</strong> the M<strong>in</strong>istry <strong>of</strong><br />
Health and RMS. Thus, the M<strong>in</strong>istry <strong>of</strong> Health does not have to <strong>in</strong>vest <strong>in</strong> tertiary medical<br />
services available <strong>in</strong> RMS hospitals, and RMS does not have to <strong>in</strong>vest <strong>in</strong> establish<strong>in</strong>g <strong>health</strong><br />
centres or hospitals <strong>in</strong> locations served by MOH facilities.<br />
• Needs m<strong>in</strong>imum monitor<strong>in</strong>g and audit<strong>in</strong>g efforts from both sides as the two parties are public<br />
not pr<strong>of</strong>it driven organizations. This is reflected clearly <strong>in</strong> Table 5, which shows that the cost<br />
per admission <strong>in</strong> RMS was JD 295, while it was JD 1563 <strong>in</strong> private hospitals with no formal<br />
contracts and JD 583 <strong>in</strong> all hospitals.
Weaknesses and limitations<br />
Jordan<br />
• With the absence <strong>of</strong> an effective referral system and co-payment, eligible patients may abuse<br />
the services available <strong>in</strong> the two <strong>sector</strong>s.<br />
• <strong>The</strong> account<strong>in</strong>g systems <strong>in</strong> both <strong>sector</strong>s, especially at the M<strong>in</strong>istry <strong>of</strong> Health, are not<br />
sufficiently well developed to trace and document all services provided to patients and the<br />
due charges. <strong>The</strong>refore, the reported claims do not represent the real bill that should be<br />
reimbursed.<br />
• Some terms and articles <strong>in</strong> the agreement are not well stated and may have different<br />
mean<strong>in</strong>gs and <strong>in</strong>terpretations.<br />
Table 5. Admissions and outpatient visits for <strong>in</strong>sured patients treated outside M<strong>in</strong>istry <strong>of</strong><br />
<strong>health</strong> facilities and their cost, 2003<br />
Organization/hospital Admissions Cost<br />
(JD)<br />
128<br />
Cost per<br />
admission<br />
(JD)<br />
Outpatient<br />
visits<br />
Cost<br />
(JD)<br />
Total costs<br />
(JD)<br />
RMS 8088 2 404 250 297 65 477 1 218 157 3 622 407<br />
Pr<strong>in</strong>ce Zeid Hospital/RMS 1832 203 526 111 27 717 508 300 711 826<br />
JUH 14 349 6 166 458 429 245 923 4 806 258 10 972 716<br />
KAH 7209 4 432 719 614 30 796 1 399 806 5 832 525<br />
Al-Husse<strong>in</strong> Cancer Centre 745 1 407 305 1889 2602 259 855 1 667 160<br />
Red Crescent Hospital 445 245 833 552 --- --- 245 833<br />
Lozmila Hospital 627 419 600 669 --- --- 419 600<br />
Al-Mowasah Hospital* 1450 480 000 331 --- --- 480 000<br />
Al-Hayah Hospital* 547 292 500 535 --- --- 292 500<br />
Other private hospitals<br />
(emergency cases)<br />
2682 4 192 014 1563 --- --- 4 192 014<br />
Total 37 974 20 244 205 533 372 515 8 192 376 28 436 581<br />
Source: Directorate <strong>of</strong> Health Insurance.<br />
*<strong>The</strong> data for both hospitals cover the period from July–December, 2003<br />
Jordan University Hospital and K<strong>in</strong>g Abdullah Hospital<br />
Jordan University Hospital (JUH) was built <strong>in</strong> 1973 by the M<strong>in</strong>istry <strong>of</strong> Health as a referral<br />
hospital. In 1975 it was handed over by the government to Jordan University to function as<br />
teach<strong>in</strong>g hospital to the Faculty <strong>of</strong> Medic<strong>in</strong>e. <strong>The</strong> law by which the hospital was handed over to<br />
the University stated that the JUH should cont<strong>in</strong>ue to act as referral hospital to the M<strong>in</strong>istry <strong>of</strong><br />
Health and that the government should f<strong>in</strong>ance 50% <strong>of</strong> the hospital budget. <strong>The</strong> f<strong>in</strong>ancial<br />
arrangement between the government, represented by the M<strong>in</strong>istry <strong>of</strong> Health, and JUH has<br />
changed frequently. <strong>The</strong> exist<strong>in</strong>g agreement, which was signed <strong>in</strong> 1998, specifies the obligations<br />
and responsibilities <strong>of</strong> JUH as <strong>health</strong> care provider and the M<strong>in</strong>istry <strong>of</strong> Health as purchaser and<br />
payer.
Jordan<br />
K<strong>in</strong>g Abdullah Hospital (KAH) was opened <strong>in</strong> 2002 to function as a teach<strong>in</strong>g hospital to<br />
the Faculty <strong>of</strong> Medic<strong>in</strong>e at Jordan University for Science and Technology. It serves as a referral<br />
hospital for all <strong>health</strong> <strong>sector</strong>s <strong>in</strong> Irbid and Northern Region. <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health and KAH<br />
signed an agreement <strong>in</strong> 2001, similar to the JUH agreement, to provide medical services to the<br />
beneficiaries who are referred to KAH by the M<strong>in</strong>istry <strong>of</strong> Health hospitals <strong>in</strong> the Northern<br />
Region.<br />
Ma<strong>in</strong> features<br />
• Emergency cases and patients referred by the M<strong>in</strong>istry <strong>of</strong> Health hospitals are treated without<br />
any co-payment. Self-referred patients pay 10%–30% <strong>of</strong> the hospital costs, depend<strong>in</strong>g on the<br />
category <strong>of</strong> their <strong>in</strong>surance plan.<br />
• <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health pays each hospital accord<strong>in</strong>g to its <strong>of</strong>ficial charge scheme with 25%<br />
discount exclud<strong>in</strong>g medic<strong>in</strong>es.<br />
• <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health pays a monthly deposit to JUH and KAH (JD 400 000 and JD<br />
200 000, respectively).<br />
• <strong>The</strong> two agreements conta<strong>in</strong> some caps to rationalize the utilization <strong>of</strong> services and conta<strong>in</strong><br />
costs (e.g. the referral letter expires after three months, the M<strong>in</strong>istry <strong>of</strong> Health pays only for<br />
two outpatient visits per month for each patient).<br />
• <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health appo<strong>in</strong>ts a full-time liaison committee <strong>in</strong> each hospital. <strong>The</strong><br />
committee reviews and authorizes claims and acts as coord<strong>in</strong>ator between the hospital and<br />
the M<strong>in</strong>istry <strong>of</strong> Health <strong>in</strong> all aspects related to the agreement.<br />
• A higher jo<strong>in</strong>t committee headed by the M<strong>in</strong>ister <strong>of</strong> Health with senior members from both<br />
parties is formed for each hospital to resolve problems, settle disputes and suggest changes<br />
on the terms and conditions <strong>of</strong> the agreement.<br />
Strengths<br />
• Provide access for the M<strong>in</strong>istry <strong>of</strong> Health beneficiaries to tertiary and presumably higher<br />
quality patient care available <strong>in</strong> teach<strong>in</strong>g hospitals.<br />
• M<strong>in</strong>imize pressure and over-utilization <strong>of</strong> the two major M<strong>in</strong>istry <strong>of</strong> Health hospitals located<br />
<strong>in</strong> Amman and Irbid (Al Bashir Hospital and Basma Hospital). This reflects positively on<br />
social equity by giv<strong>in</strong>g the poor and un<strong>in</strong>sured people a chance to be treated <strong>in</strong> highly<br />
subsidized public hospitals almost free <strong>of</strong> charge.<br />
• Improve the utilization rates <strong>in</strong> the two teach<strong>in</strong>g hospitals and provide them with regular<br />
cashflow to meet their recurrent f<strong>in</strong>ancial obligations. In 2002, 64% <strong>of</strong> the total admissions <strong>in</strong><br />
JUH and KAH were the M<strong>in</strong>istry <strong>of</strong> Health beneficiaries (JUH and KAH Annual Reports,<br />
2002).<br />
• Treat<strong>in</strong>g beneficiaries <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health <strong>in</strong> public teach<strong>in</strong>g hospitals is more cost<br />
effective than treat<strong>in</strong>g them <strong>in</strong> private hospitals. <strong>The</strong> average cost <strong>of</strong> admission <strong>in</strong> private<br />
hospitals is almost three times higher than <strong>in</strong> JUH or KAH (Table 5).<br />
• It is more cost effective for the M<strong>in</strong>istry <strong>of</strong> Health to purchase tertiary care for its enrollees<br />
(beneficiaries) than to provide this service directly. In 2003, the M<strong>in</strong>istry <strong>of</strong> Health utilized<br />
129
Jordan<br />
60% <strong>of</strong> JUH beds (300 beds) with an average cost <strong>of</strong> JD 429 per admission, while the<br />
average cost <strong>of</strong> admission <strong>in</strong> all hospitals with which the M<strong>in</strong>istry <strong>of</strong> Health has formal and<br />
<strong>in</strong>formal contracts was JD 533 (Table 5).<br />
• <strong>The</strong> agreements have some built-<strong>in</strong> mechanisms (utilization caps, liaison committees) to<br />
monitor overall performance, control costs and solve problems.<br />
Weaknesses and limitations<br />
• <strong>The</strong> liberal referr<strong>in</strong>g practice <strong>in</strong> the M<strong>in</strong>istry <strong>of</strong> Health hospitals is <strong>in</strong>creas<strong>in</strong>g the f<strong>in</strong>ancial<br />
pressure on the M<strong>in</strong>istry <strong>of</strong> Health budget. In 2003, the cost <strong>of</strong> M<strong>in</strong>istry <strong>of</strong> Health<br />
beneficiaries treated at JUH and KAH was 58% <strong>of</strong> the total costs paid for all non-M<strong>in</strong>istry <strong>of</strong><br />
Health hospitals (Table 5).<br />
• Teach<strong>in</strong>g hospitals, especially <strong>in</strong> the absence <strong>of</strong> practice protocols, tend to provide more<br />
services than patients need. Thus, costs are more likely to <strong>in</strong>crease.<br />
Al-Husse<strong>in</strong> Cancer Centre<br />
Al-Husse<strong>in</strong> Cancer Centre (HCC) was opened <strong>in</strong> 1997 as philanthropic, not-for-pr<strong>of</strong>it<br />
hospital. <strong>The</strong> centre has 131 beds. It provides diagnostic, treatment and rehabilitation services for<br />
cancer patients, <strong>in</strong>clud<strong>in</strong>g chemotherapy and radiotherapy. In 2001, the M<strong>in</strong>istry <strong>of</strong> Health and<br />
HCC signed an agreement for medical and scientific cooperation.<br />
Ma<strong>in</strong> features<br />
• HCC provides medical services for the enrollees <strong>of</strong> the CHIP and un<strong>in</strong>sured patients who are<br />
referred by the M<strong>in</strong>istry <strong>of</strong> Health.<br />
• <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health pays the treatment cost <strong>of</strong> its beneficiaries and the M<strong>in</strong>istry <strong>of</strong><br />
F<strong>in</strong>ance pays the cost <strong>of</strong> the un<strong>in</strong>sured patients.<br />
• Charges are paid accord<strong>in</strong>g to HCC <strong>of</strong>ficial charge scheme with 20% discount exclud<strong>in</strong>g<br />
medic<strong>in</strong>es.<br />
• <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health has a liaison <strong>of</strong>fice at HCC. <strong>The</strong> <strong>of</strong>fice checks eligibility <strong>of</strong> referred<br />
patients, reviews and authorizes bills and coord<strong>in</strong>ates all matters related to the<br />
implementation <strong>of</strong> the agreement.<br />
• HCC allocates 10% <strong>of</strong> its revenues from this agreement for the Cancer Research Fund.<br />
• A jo<strong>in</strong>t cancer research committee from the M<strong>in</strong>istry <strong>of</strong> Health and HCC develops the cancer<br />
research agenda, approves research projects and recommends the budget for each project.<br />
• A higher coord<strong>in</strong>ation committee, headed by the general secretary <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health<br />
with two senior members from each party, is formed to resolve problems and settle disputes<br />
that may arise.<br />
130
Strengths<br />
Jordan<br />
• Provides access to <strong>in</strong>tegrated and highly specialized cancer services for <strong>in</strong>sured and<br />
un<strong>in</strong>sured patients. This reflects positively on equity and quality <strong>of</strong> patient care.<br />
• Decreases pressure on and over-utilization <strong>of</strong> the two public cancer units at K<strong>in</strong>g Husse<strong>in</strong><br />
Medical Centre and Al-Bashir Hospital.<br />
• Improves scientific cooperation between oncologists <strong>in</strong> the M<strong>in</strong>istry <strong>of</strong> Health and HCC and<br />
enhances cancer research <strong>in</strong> the country.<br />
• Improves the utilization rate at HCC and provides it with reasonable cashflow. <strong>The</strong><br />
occupancy rate at HCC was 84% <strong>in</strong> 2003 (MOH Annual Report, 2002).<br />
Weaknesses and limitations<br />
• Reimbursement accord<strong>in</strong>g to fee-for-service, the lack <strong>of</strong> co-payment and the absence <strong>of</strong><br />
treatment protocols are <strong>in</strong>centives to <strong>in</strong>crease the government bill <strong>of</strong> cancer patients. If this<br />
cont<strong>in</strong>ues, it may force the government to reconsider its commitment regard<strong>in</strong>g free<br />
treatment <strong>of</strong> cancer patients.<br />
• Scientific and research cooperation is not yet activated.<br />
• <strong>The</strong>re are delays <strong>in</strong> reimbursement.<br />
Crescent Hospital<br />
Crescent Hospital is a 64-bed not-for-pr<strong>of</strong>it philanthropic general hospital situated <strong>in</strong> East<br />
Amman. Accord<strong>in</strong>g to the agreement which was signed <strong>in</strong> 1999, Al-Bashir Hospital, the largest<br />
M<strong>in</strong>istry <strong>of</strong> Health hospital, can referee beneficiaries to be treated at Crescent Hospital.<br />
Ma<strong>in</strong> features<br />
• Only Al-Bashir Hospital can refer patients.<br />
• Crescent Hospital should only provide patient services related to the medical diagnosis<br />
specified <strong>in</strong> the referral report.<br />
• Except delivery cases, hospital charges are calculated accord<strong>in</strong>g to m<strong>in</strong>imum <strong>of</strong>ficial fees<br />
authorized by the M<strong>in</strong>istry <strong>of</strong> Health and other medical authorities<br />
• Except delivery cases and medic<strong>in</strong>es, the hospital <strong>of</strong>fers 30% discount on the total charges.<br />
• Normal delivery, caesarean section and complicated delivery are charged fixed fees on a per<br />
case basis (JD 80 and 100 respectively).<br />
• Medic<strong>in</strong>es are priced accord<strong>in</strong>g to the drug store prices plus 20%<br />
• <strong>The</strong> director <strong>of</strong> Al-Bashir Hospital should review and authorize all claims before send<strong>in</strong>g<br />
them to the HID for payment.<br />
• <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health has the right to review the medical and f<strong>in</strong>ancial records for any<br />
patient.<br />
131
Strengths<br />
Jordan<br />
• <strong>The</strong> agreement practically provides Al-Bashir Hospital with 64 beds to be used when needed<br />
without capital or fixed costs. At the same time, it improves the bed utilization rate at<br />
Crescent Hospital. Thus, efficiency is improved for both parties.<br />
• It <strong>in</strong>volves as a first some prospective payment mechanisms (per case) as an endeavour by<br />
the M<strong>in</strong>istry <strong>of</strong> Health to conta<strong>in</strong> cost <strong>of</strong> services.<br />
Weaknesses and limitations<br />
• As with other agreements, it lacks practice protocols and quality control mechanisms.<br />
• It does not provide the beneficiaries with the choice to be treated at this hospital and share<br />
part <strong>of</strong> the cost as co-payment.<br />
• <strong>The</strong>re are delays <strong>in</strong> reimbursement.<br />
Lozmila Hospital<br />
Lozmila Hospital is 58-bed private for-pr<strong>of</strong>it general hospital situated <strong>in</strong> the middle <strong>of</strong><br />
Amman. <strong>The</strong> current agreement was signed <strong>in</strong> April 2001. Accord<strong>in</strong>g to this agreement, M<strong>in</strong>istry<br />
<strong>of</strong> Health hospitals can refer beneficiaries to Lozmila Hospital and beneficiaries can go directly<br />
to the hospital and share part <strong>of</strong> the cost as co-payment.<br />
Ma<strong>in</strong> features<br />
• M<strong>in</strong>istry <strong>of</strong> Health hospitals ma<strong>in</strong>ly Al-Bashir Hospital can refer <strong>in</strong>sured patients to Lozmila<br />
Hospital. Beneficiaries can be treated without referral and pay 30% <strong>of</strong> the hospital fees.<br />
• Lozmila should only provide services related to the medical diagnosis as specified <strong>in</strong> the<br />
referral report.<br />
• As with Crescent Hospital, prices are allocated accord<strong>in</strong>g to the m<strong>in</strong>imum fees set by <strong>of</strong>ficial<br />
authorities, with 25% discount exclud<strong>in</strong>g medic<strong>in</strong>e.<br />
• <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health appo<strong>in</strong>ts a committee to monitor and follow up all adm<strong>in</strong>istrative and<br />
technical matters related to this agreement. <strong>The</strong> committee has the right to review medical<br />
and adm<strong>in</strong>istrative records to audit all procedures and services related to the referred patients.<br />
• A hospital stay <strong>of</strong> more than five days requires approval from the committee.<br />
• If the M<strong>in</strong>istry <strong>of</strong> Health refers a patient for specific procedures, the hospital cannot charge<br />
any <strong>in</strong>vestigation without approval <strong>of</strong> the committee.<br />
Strengths<br />
• As with other agreements, it improves the access <strong>of</strong> M<strong>in</strong>istry <strong>of</strong> Health beneficiaries to <strong>health</strong><br />
services and improves the utilization rate at Lozmila Hospital.<br />
132
Jordan<br />
• <strong>The</strong> m<strong>in</strong>imum charge scale, <strong>in</strong> addition to the discount rate and the co-payment mechanism,<br />
provide the M<strong>in</strong>istry <strong>of</strong> Health with relatively low cost <strong>health</strong> care services at (presumably)<br />
accepted quality.<br />
• <strong>The</strong> agreement has some caps on services ordered by the provider (e.g. approval <strong>of</strong> payer if<br />
the patient stay exceeds 5 days).<br />
Weakness and limitations<br />
• As other agreements, it lacks performance measures to assure quality <strong>of</strong> services.<br />
• Dependence on a committee to monitor performance does not guarantee always good results,<br />
as members <strong>of</strong> the committee change frequently and may lose <strong>in</strong>terest if they do not have<br />
<strong>in</strong>centives or are not exposed to close supervision from higher authorities.<br />
• <strong>The</strong>re are delays <strong>in</strong> reimbursement procedures.<br />
Other private hospitals<br />
All private hospitals <strong>in</strong>clud<strong>in</strong>g those who have formal contracts with M<strong>in</strong>istry <strong>of</strong> Health<br />
may admit emergency patients enrolled <strong>in</strong> the Civil Health Insurance Plan. For hospitals that do<br />
not have formal <strong>contractual</strong> relationships with the M<strong>in</strong>istry <strong>of</strong> Health, the M<strong>in</strong>istry will provide<br />
reimbursement only for those patients who are assessed as emergency cases. <strong>The</strong> burden <strong>of</strong> pro<strong>of</strong><br />
is on the hospital that provides the treatment, as well as on the patient.<br />
Specific and detailed procedures should be followed with<strong>in</strong> 24 hours <strong>of</strong> any emergency<br />
admission <strong>in</strong> order that the M<strong>in</strong>istry <strong>of</strong> Health provides reimbursement. In 2003, the cost <strong>of</strong><br />
beneficiaries treated <strong>in</strong> private hospitals as emergency cases was about JD 4 million (Table 5).<br />
<strong>The</strong> cost <strong>of</strong> an emergency admission <strong>in</strong> a private none contract<strong>in</strong>g hospital is about three<br />
times as the cost <strong>of</strong> admission <strong>in</strong> a contract<strong>in</strong>g hospital (Table 5). This provides evidence that<br />
contract<strong>in</strong>g has significant effect on cost conta<strong>in</strong>ment and thus <strong>in</strong>creases efficiency.<br />
Bed leas<strong>in</strong>g contracts<br />
Introduction<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health has recently begun contract<strong>in</strong>g out services with two private<br />
hospitals <strong>in</strong> East Amman on the basis <strong>of</strong> fixed payment aga<strong>in</strong>st leas<strong>in</strong>g a specified number <strong>of</strong><br />
beds. In March 2003, the M<strong>in</strong>istry <strong>of</strong> Health signed a contract with Al-Mowasah Hospital to<br />
lease 40 beds, and <strong>in</strong> July 2003 the M<strong>in</strong>istry signed another contract with Al-Hayah hospital to<br />
lease 30 beds. <strong>The</strong> two contracts have been effective s<strong>in</strong>ce July 2003. Because both contracts<br />
have the same conditions, the M<strong>in</strong>istry <strong>of</strong> Health contract with Al-Mowasah hospital will be<br />
presented here as example for this type <strong>of</strong> contract<strong>in</strong>g.<br />
133
Al-Mowasah hospital<br />
Jordan<br />
Al-Mowasah hospital is a private for-pr<strong>of</strong>it 160-bed hospital. It was opened <strong>in</strong> 2000 <strong>in</strong><br />
Marka Region, east <strong>of</strong> Amman. <strong>The</strong> hospital is located <strong>in</strong> a low- to middle-<strong>in</strong>come, highly<br />
populated area that lacks public and private hospitals. It is well built and equipped to<br />
accommodate most medical and surgical specialties.<br />
<strong>The</strong> hospital economic feasibility study was based on the assumption that the people liv<strong>in</strong>g<br />
<strong>in</strong> East Amman will not go to hospitals <strong>in</strong> west Amman if they have modern and well-equipped<br />
hospital near to their residency.<br />
Before sign<strong>in</strong>g the contract with the M<strong>in</strong>istry <strong>of</strong> Health, the hospital was operat<strong>in</strong>g 48 beds<br />
with 20% average occupancy. As a result <strong>of</strong> the low occupancy rate, the hospital faced f<strong>in</strong>ancial<br />
problems. <strong>The</strong> monthly loss was about JD 50 000 (US$ 75 000), as shown <strong>in</strong> Figure 3.<br />
Figure 3. Net loss <strong>of</strong> Al-Mowasah hospital before contract<strong>in</strong>g with the M<strong>in</strong>istry <strong>of</strong><br />
Health<br />
134
Jordan<br />
<strong>The</strong> ma<strong>in</strong> reasons beh<strong>in</strong>d the low utilization rate, as expressed by the hospital director and<br />
highlighted by the results <strong>of</strong> a recent unpublished study (Baniawad, M., 2004) are summarized as<br />
follows:<br />
• Large percentages <strong>of</strong> people liv<strong>in</strong>g <strong>in</strong> the hospital area are <strong>in</strong>sured by the M<strong>in</strong>istry <strong>of</strong> Health<br />
and RMS and they go to public hospitals.<br />
• Un<strong>in</strong>sured poor people also seek treatment <strong>in</strong> highly subsidized public hospitals, ma<strong>in</strong>ly <strong>in</strong><br />
Al-Bashir Hospital.<br />
• People who are wealthy and will<strong>in</strong>g to pay usually go to private hospitals <strong>in</strong> West Amman,<br />
for reasons <strong>of</strong> social prestige.<br />
• <strong>The</strong> hospital site is <strong>in</strong>convenient (high traffic, overcrowded, near a sewage treatment plant<br />
and slaughterhouse) and does not attract patients from other areas <strong>in</strong> the region.<br />
Ma<strong>in</strong> features<br />
• <strong>The</strong> hospital provides the M<strong>in</strong>istry <strong>of</strong> Health with the full services <strong>of</strong> 40 beds (except<br />
medic<strong>in</strong>es and services <strong>of</strong> attend<strong>in</strong>g physicians).<br />
• <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health pays the hospital a flat rate <strong>of</strong> JD 1950 per bed per month (JD 65 per<br />
day).<br />
• <strong>The</strong> 40 leased beds are distributed by medical specialty as follows:<br />
18 beds for medical cases.<br />
18 beds for surgical cases.<br />
4 beds for <strong>in</strong>tensive care cases.<br />
• One <strong>of</strong> the hospital floors with 36 beds is designated for the M<strong>in</strong>istry <strong>of</strong> Health patients.<br />
Thus, the M<strong>in</strong>istry <strong>of</strong> Health patients do not mix with other private patients.<br />
• <strong>The</strong> beds on the M<strong>in</strong>istry <strong>of</strong> Health floor are distributed equally among private, semi-private<br />
and regular rooms to accommodate the different categories <strong>of</strong> M<strong>in</strong>istry <strong>of</strong> Health<br />
beneficiaries.<br />
• <strong>The</strong> hospital provides the follow<strong>in</strong>g services for the leased beds:<br />
Nurs<strong>in</strong>g services.<br />
In-house doctors.<br />
Diagnostic <strong>in</strong>vestigations exclud<strong>in</strong>g hormone tests, histopathology, MRI and angiography.<br />
All services needed to perform surgical procedures <strong>in</strong>clud<strong>in</strong>g anesthesia agents and<br />
medical gases.<br />
Medical and non-medical supplies exclud<strong>in</strong>g artificial implants and limbs.<br />
Adm<strong>in</strong>istrative facilities and services, such as reception area, <strong>of</strong>fices for M<strong>in</strong>istry liaison<br />
staff, lounge and rest facilities for M<strong>in</strong>istry physicians, pharmacy, store, medical<br />
records area, telephone facilities, patient transportation among hospitals <strong>in</strong> Amman.<br />
• <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health provides the follow<strong>in</strong>g:<br />
Attend<strong>in</strong>g (specialized) physicians to provide medical and surgical care for the M<strong>in</strong>istry <strong>of</strong><br />
Health patients.<br />
Medic<strong>in</strong>es and pharmacists.<br />
135
Jordan<br />
Adm<strong>in</strong>istrative staff to coord<strong>in</strong>ate, supervise and monitor the implementation <strong>of</strong> this<br />
contract on daily basis.<br />
• A committee from the M<strong>in</strong>istry <strong>of</strong> Health is assigned to control and monitor all<br />
adm<strong>in</strong>istrative aspects related to this contract. <strong>The</strong> committee reports directly to the M<strong>in</strong>ister<br />
and should assure full utilization <strong>of</strong> the leased beds, high quality <strong>of</strong> services for the M<strong>in</strong>istry<br />
<strong>of</strong> Health patients and that all contracted services are met by the hospital.<br />
• If the hospital does not meet any <strong>of</strong> its obligations as specified <strong>in</strong> this contract, the M<strong>in</strong>istry<br />
<strong>of</strong> Health control committee has the right to make the necessary arrangement to compensate<br />
for this and deduct the cost from the hospital payment.<br />
• <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health pays the hospital at the end <strong>of</strong> each month.<br />
• <strong>The</strong> hospital provides the M<strong>in</strong>istry <strong>of</strong> Health with six outpatient cl<strong>in</strong>ics for JD 2000 per cl<strong>in</strong>ic<br />
monthly. <strong>The</strong> services provided by the hospital for outpatient cl<strong>in</strong>ics <strong>in</strong>clude physical<br />
facilities and nurs<strong>in</strong>g services only. Diagnostic services are provided to M<strong>in</strong>istry <strong>of</strong> Health<br />
outpatients accord<strong>in</strong>g to the m<strong>in</strong>imum rate, with 25% discount.<br />
• <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health has the right to rent all the beds <strong>of</strong> the hospital. In this case, the<br />
hospital must evacuate its patients with<strong>in</strong> 24 hour notice.<br />
• <strong>The</strong> duration <strong>of</strong> the contract is one year. It is self renewed. However, each party has the right<br />
to discont<strong>in</strong>ue the contract or change its contents aga<strong>in</strong>st written request before two months<br />
<strong>of</strong> the expiry date.<br />
Strengths<br />
For the M<strong>in</strong>istry <strong>of</strong> Health<br />
• It provides <strong>in</strong>stant expansion to Al-Bashir Hospital (40 beds which could be <strong>in</strong>creased to 160<br />
beds) without bear<strong>in</strong>g any capital <strong>in</strong>vestment. <strong>The</strong> average capital cost per hospital bed <strong>in</strong> a<br />
modern general hospital <strong>in</strong> Jordan is about JD 100 000 to JD 150 000. Thus, the contract<br />
saves about JD 5 million for the M<strong>in</strong>istry <strong>of</strong> Health budget.<br />
• It improves the access <strong>of</strong> <strong>in</strong>sured patients to relatively high quality hospital care and<br />
m<strong>in</strong>imizes the pressure on M<strong>in</strong>istry <strong>of</strong> Health hospitals <strong>in</strong> East Amman (ma<strong>in</strong>ly Al-Bashir<br />
Hospital). This has a positive impact on the access <strong>of</strong> the poor to highly subsidized hospital<br />
services <strong>of</strong>fered by the M<strong>in</strong>istry <strong>of</strong> Health.<br />
• <strong>The</strong> average cost per admission is JD 331. This is about 50% <strong>of</strong> the costs that the M<strong>in</strong>istry <strong>of</strong><br />
Health pays to other private hospitals with fee-for-service contracts (Table 3).<br />
• <strong>The</strong> general feedback from patients reflects better satisfaction levels. This is likely because<br />
<strong>of</strong>:<br />
Better standards <strong>of</strong> hotel services.<br />
Flexible visit<strong>in</strong>g hours.<br />
Short wait<strong>in</strong>g lists.<br />
Better response <strong>of</strong> the staff to patients needs.<br />
Geographical accessibility.<br />
Availability <strong>of</strong> private and semi-private rooms.<br />
No crowds.<br />
136
Jordan<br />
• Interviews with the M<strong>in</strong>istry <strong>of</strong> Health staff work<strong>in</strong>g at Al-Mowasah Hospital (five<br />
physicians and five adm<strong>in</strong>istrative and technical staff) reflect high morale and job<br />
satisfaction.<br />
• S<strong>in</strong>ce payment is based on a flat rate, the M<strong>in</strong>istry <strong>of</strong> Health adm<strong>in</strong>istrative and f<strong>in</strong>ancial<br />
costs are low.<br />
• Budgetary allocations are specified <strong>in</strong> advance and f<strong>in</strong>ancial fluctuations are not permitted.<br />
• As the M<strong>in</strong>istry <strong>of</strong> Health physicians are available most <strong>of</strong> the time <strong>in</strong> Al-Mowasah Hospital<br />
and participate <strong>in</strong> the provision <strong>of</strong> patient care, the M<strong>in</strong>istry <strong>of</strong> Health can monitor directly<br />
the quality <strong>of</strong> care and guarantee that <strong>in</strong>sured patients receive proper care.<br />
In brief, this contract provides the M<strong>in</strong>istry <strong>of</strong> Health with effective, efficient, good quality<br />
and accessible patient care with high satisfaction <strong>of</strong> both patients and the M<strong>in</strong>istry <strong>of</strong> Health<br />
staff.<br />
For Al-Mowasah Hospital<br />
• <strong>The</strong> 40 beds leased by the M<strong>in</strong>istry <strong>of</strong> Health <strong>in</strong>creased the work<strong>in</strong>g hospital beds to 83 and<br />
guarantee 48% bed occupancy year-round. Tak<strong>in</strong>g <strong>in</strong>to consideration the beds operated by<br />
the hospital for private patients (43 beds), the average occupancy rate dur<strong>in</strong>g 2003 was about<br />
58%. It was reported by many hospital adm<strong>in</strong>istrators that most private hospitals <strong>in</strong> Amman<br />
usually reach the break-even po<strong>in</strong>t at 40% bed occupancy rate.<br />
• Due to the significant <strong>in</strong>crease <strong>in</strong> bed occupancy rate, the hospital was able to avoid loss and<br />
achieve net pr<strong>of</strong>it (10%–12%) as shown <strong>in</strong> Figure 4.<br />
• <strong>The</strong> contract <strong>in</strong>volves m<strong>in</strong>imal adm<strong>in</strong>istrative costs.<br />
• <strong>The</strong> contract provides the hospital with regular <strong>in</strong>come and cash flow. This reflects positively<br />
on:<br />
<strong>The</strong> f<strong>in</strong>ancial reputation <strong>of</strong> the hospital.<br />
<strong>The</strong> ma<strong>in</strong>tenance <strong>of</strong> physical facilities and equipment.<br />
Job security and morale <strong>of</strong> the hospital employees.<br />
<strong>The</strong> general public image towards the hospital.<br />
Overall productivity <strong>of</strong> the hospital.<br />
Strengths related to economics<br />
137
Jordan<br />
• This contract provided the M<strong>in</strong>istry <strong>of</strong> Health with accessible and cost-effective patient care<br />
with acceptable quality standards. It also provides Al-Mowasah hospital with reasonable<br />
return for <strong>in</strong>vestment (<strong>in</strong>come) to stay <strong>in</strong> bus<strong>in</strong>ess and prosper. Thus, the microeconomics <strong>of</strong><br />
both parties was improved.<br />
• On macroeconomics level, Al-Mowasah hospital, as other private hospitals, is considered a<br />
national asset. Thus, keep<strong>in</strong>g the hospital <strong>in</strong> bus<strong>in</strong>ess saves about JD 10 million (the hospital<br />
<strong>in</strong>vestment) for the country. <strong>The</strong> contract helps the hospital keep about 200 employees on the<br />
job. It improves equity and access <strong>of</strong> <strong>in</strong>sured and un<strong>in</strong>sured poor patients liv<strong>in</strong>g <strong>in</strong> less<br />
advantageous areas <strong>in</strong> East Amman.<br />
• This type <strong>of</strong> contract<strong>in</strong>g represents a model for public–private partnership that achieves the<br />
<strong>in</strong>terests <strong>of</strong> both parties (a w<strong>in</strong>–w<strong>in</strong> model).<br />
• It creates a jo<strong>in</strong>t venture partnership between the public and private <strong>sector</strong>s. It opens the<br />
doors for the M<strong>in</strong>istry <strong>of</strong> Health physicians to practise <strong>in</strong> private hospitals to serve public<br />
<strong>in</strong>sured patients. <strong>The</strong> contract proves and demonstrates that “public wards” can exist <strong>in</strong><br />
private hospitals, chang<strong>in</strong>g the traditional model <strong>of</strong> hav<strong>in</strong>g “private wards” <strong>in</strong> public<br />
hospitals. It is an endeavour to bridge the gap between public and private <strong>sector</strong>s. It creates a<br />
positive atmosphere which both <strong>sector</strong>s complete, rather than compete with, each other.<br />
Weaknesses and limitations<br />
• <strong>The</strong> contract was not based on open bidd<strong>in</strong>g process. <strong>The</strong>refore, other private hospitals,<br />
especially <strong>in</strong> East Amman, claim that they were not given equal opportunity.<br />
• Some conditions and articles <strong>of</strong> the contract were general and not stated <strong>in</strong> explicit terms.<br />
• As other contracts and agreements, it lacks performance <strong>in</strong>dicators to monitor quality <strong>of</strong><br />
services.<br />
Figure 4. Net pr<strong>of</strong>it <strong>of</strong> Al-Mowasah hospital after contract<strong>in</strong>g with the M<strong>in</strong>istry <strong>of</strong> Health<br />
138
Jordan<br />
• This type <strong>of</strong> contract<strong>in</strong>g is not yet robust and may not stand aga<strong>in</strong>st pressures that could be<br />
exerted upon the M<strong>in</strong>istry <strong>of</strong> Health to abandon it.<br />
Bundl<strong>in</strong>g <strong>of</strong> services contracts<br />
Background<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health seeks to expand the adm<strong>in</strong>istrative capacity <strong>of</strong> the Health Insurance<br />
Directorate (HID) <strong>in</strong> the areas <strong>of</strong> contract design, contract monitor<strong>in</strong>g, and contract enforcement.<br />
<strong>The</strong>refore, the M<strong>in</strong>istry is implement<strong>in</strong>g a Health Insurance Pilot Project (HIPP), with support<br />
from the Partners for Health Reformplus (PHRplus) project, Amman, Jordan. It was decided that<br />
obstetric services, which are frequently contracted out to private <strong>sector</strong> hospitals, should<br />
constitute the prelim<strong>in</strong>ary bundle <strong>of</strong> services to be contracted under the HIPP (Khasawneh A.,<br />
PHRplus, 2003).<br />
Prelim<strong>in</strong>ary steps<br />
Prior to implementation, several steps were taken as follows.<br />
• An advisory committee <strong>of</strong> senior-level the M<strong>in</strong>istry <strong>of</strong> Health executives was appo<strong>in</strong>ted to<br />
oversee the development and operation <strong>of</strong> the HIPP.<br />
• An implementation Unit (IU) was established with<strong>in</strong> the HID to manage the contracts.<br />
• An ongo<strong>in</strong>g tra<strong>in</strong><strong>in</strong>g programme was <strong>in</strong>itiated for the IU staff with technical assistance from<br />
the PHRplus project. This programme covers contract design, implementation, monitor<strong>in</strong>g<br />
and enforcement.<br />
• Two geographical sites were selected (East and West Amman) for the project.<br />
• A bundle <strong>of</strong> maternity and maternity-related services was specified, which <strong>in</strong>cludes pre-natal,<br />
delivery and postnatal services.<br />
• A list <strong>of</strong> potential enrollees was established (250 women).<br />
• Cl<strong>in</strong>ical guidel<strong>in</strong>es and standards for prenatal, delivery, post natal and neonatal were<br />
developed. A series <strong>of</strong> focus groups were conducted for physicians to assess the technical<br />
merits <strong>of</strong> the guidel<strong>in</strong>es as well as their prospects for implementation.<br />
• Focus group discussions were conducted by a private market research organization to<br />
establish basel<strong>in</strong>e consumer op<strong>in</strong>ions and expectations.<br />
• A private hospital survey was conducted to gather <strong>in</strong>formation about the capacity <strong>of</strong> private<br />
hospitals for provid<strong>in</strong>g reproductive <strong>health</strong> services and their <strong>in</strong>terest <strong>in</strong> participat<strong>in</strong>g <strong>in</strong> the<br />
project. All hospitals surveyed stated that they would be will<strong>in</strong>g to participate <strong>in</strong> the HIPP.<br />
• A f<strong>in</strong>al HIPP contract was drafted and reviewed by the <strong>of</strong>fice <strong>of</strong> legal affairs with<strong>in</strong> the<br />
M<strong>in</strong>istry <strong>of</strong> Health.<br />
• A management <strong>in</strong>formation system (MIS) was <strong>in</strong>stalled and tested. <strong>The</strong> system will support<br />
the contact<strong>in</strong>g process by ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g patient-specific enrollment, payment and utilization<br />
databases and by support<strong>in</strong>g provider bill<strong>in</strong>g and payment functions.<br />
139
Jordan<br />
• A qualification process was completed, and the bidd<strong>in</strong>g contracts will be distributed to the<br />
qualified hospitals (see Annex 2 for “Request for Qualification” form).<br />
Assumptions <strong>of</strong> the pilot programme<br />
• General programme assumptions<br />
250 <strong>in</strong>sured women, married, seek<strong>in</strong>g to be pregnant.<br />
2–3 hospitals contractors competitively selected, each accept<strong>in</strong>g a fully bundled fee per<br />
episode.<br />
Episode <strong>in</strong>cludes all prenatal care, delivery, newborn care while <strong>in</strong> the hospital, and postnatal<br />
care for the mother <strong>in</strong>clud<strong>in</strong>g family plann<strong>in</strong>g.<br />
Hospital is paid the entire fee by the HID, and hospital is responsible for contract<strong>in</strong>g with<br />
physicians and other necessary services.<br />
Protection from provider <strong>in</strong>centives to under-serve patients by impos<strong>in</strong>g quality standards.<br />
• Enrollment assumptions<br />
Enrollees assigned to a hospital and a specific physician on enrollment (with enrollee<br />
gett<strong>in</strong>g a choice).<br />
Participation <strong>in</strong> pilot is <strong>in</strong> lieu <strong>of</strong> other HID benefits perta<strong>in</strong><strong>in</strong>g to the episode <strong>of</strong> pregnancy.<br />
Woman may select to opt out <strong>of</strong> the pilot by appeal to HID at any time.<br />
Enrollees and husbands will sign an agreement to establish terms and conditions <strong>of</strong><br />
participation.<br />
• Pric<strong>in</strong>g assumptions<br />
Payment is a fixed price per episode, as set forth <strong>in</strong> a payment schedule by HID.<br />
8–10 separate rates def<strong>in</strong>e the rate schedule, accord<strong>in</strong>g to the difficulty <strong>of</strong> the pregnancy,<br />
delivery, and neonatal care needs.<br />
All hospitals will be paid the same rates.<br />
Payment will be paid <strong>in</strong> three sums, after first ante natal visit, after delivery, and after the<br />
episode is complete.<br />
Payment is cont<strong>in</strong>gent on proper HIS data submission, and proper documentation <strong>of</strong> quality<br />
care.<br />
Special provisions need to be made for equitable risk shar<strong>in</strong>g between HID and the<br />
contract<strong>in</strong>g hospitals: outlier supplementary payments, and exclusions for<br />
catastrophic cases.<br />
• MIS assumptions<br />
All encounter forms and enrollment forms will come to the IU <strong>in</strong> hard copy, and will be<br />
entered <strong>in</strong>to the MIS at the IU <strong>of</strong>fices by IU staff.<br />
Medical cod<strong>in</strong>g will be done by IU based upon narrative descriptions provided on<br />
encounter forms, verification may require phone call to provider.<br />
IU will prepare monthly reports for delivery to each contract provider: received bills not<br />
yet paid; total programme activity and payments to date; and enrollees by status.<br />
140
Jordan<br />
CONCLUSIONS AND RECOMMENDATIONS<br />
Conclusions<br />
<strong>The</strong> results <strong>of</strong> the study show that the M<strong>in</strong>istry <strong>of</strong> Health has at least 8 formal contracts or<br />
agreements for purchas<strong>in</strong>g <strong>health</strong> services, 5 with private hospitals and 3 with autonomous public<br />
providers. Six contracts were reimbursed accord<strong>in</strong>g to fee-for-service and two contracts were<br />
paid a fixed payment aga<strong>in</strong>st leas<strong>in</strong>g a specific number <strong>of</strong> hospital beds (Al-Mowasah and Al-<br />
Hayah hospitals). In addition to these formal contracts, the M<strong>in</strong>istry <strong>of</strong> Health has <strong>in</strong>formal<br />
contracts with private hospitals to admit <strong>in</strong>sured patients <strong>in</strong> case <strong>of</strong> emergency. About 38 000<br />
M<strong>in</strong>istry <strong>of</strong> Health enrollees were admitted to the hospitals with which the M<strong>in</strong>istry has formal<br />
and <strong>in</strong>formal <strong>contractual</strong> agreements. <strong>The</strong> total annual cost for these admissions is about JD 28<br />
million, with an average cost <strong>of</strong> JD 535 per admission.<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health, with the support <strong>of</strong> PHRplus, is implement<strong>in</strong>g a Health Insurance<br />
Pilot Project (HIPP). <strong>The</strong> ma<strong>in</strong> objective <strong>of</strong> this project is to expand the adm<strong>in</strong>istrative and<br />
technical capacity <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health <strong>in</strong> the areas <strong>of</strong> contract design, contract monitor<strong>in</strong>g,<br />
and contract enforcement. Obstetric services constitutes the prelim<strong>in</strong>ary bundle <strong>of</strong> services to be<br />
contracted under the HIPP, and payment will be accord<strong>in</strong>g to a fixed price per episode. Several<br />
steps have been taken prior to implementation <strong>of</strong> the project, such as: the establishment <strong>of</strong><br />
implementation unit, development and test<strong>in</strong>g <strong>of</strong> computerized MIS, development <strong>of</strong> cl<strong>in</strong>ical<br />
guidel<strong>in</strong>es and protocols and prepar<strong>in</strong>g f<strong>in</strong>al contracts. <strong>The</strong> qualification process was completed<br />
recently and bidd<strong>in</strong>g documents will be distributed to the qualified hospitals very soon.<br />
<strong>The</strong> results <strong>of</strong> the study showed that most <strong>of</strong> the <strong>contractual</strong> <strong>arrangements</strong> have positive<br />
impacts on the purchaser (the M<strong>in</strong>istry <strong>of</strong> Health) and the providers (private and autonomous<br />
public hospitals). As this report shows, contract<strong>in</strong>g has improved access, efficiency,<br />
susta<strong>in</strong>ability, promoted public <strong>health</strong> goals, and created an environment conductive to public–<br />
private collaboration. Although there is no evidence base, the quality <strong>of</strong> contracted services is<br />
likely to be satisfactory. This may be attributed to the fact that most <strong>of</strong> the contracted hospitals<br />
have highly skilled and well tra<strong>in</strong>ed <strong>health</strong> personnel, advanced medical equipment and<br />
advanced diagnostic facilities, and have achieved a good medical reputation both <strong>in</strong>side and<br />
outside Jordan.<br />
On the macroeconomics level, contract<strong>in</strong>g out services is successfully be<strong>in</strong>g used by the<br />
government as a social and economic policy tool <strong>in</strong> deal<strong>in</strong>g with the effects <strong>of</strong> poverty and<br />
unemployment. Indeed, the admitt<strong>in</strong>g <strong>of</strong> 38 000 <strong>in</strong>sured patients outside the M<strong>in</strong>istry <strong>of</strong> Health<br />
facilities <strong>in</strong> 2003 for example, has provided almost equal number <strong>of</strong> admissions for un<strong>in</strong>sured<br />
poor patients <strong>in</strong> the M<strong>in</strong>istry <strong>of</strong> Health hospitals nearly free <strong>of</strong> charge. Utiliz<strong>in</strong>g some <strong>of</strong> the idle<br />
beds <strong>in</strong> the private <strong>sector</strong> will reflect positively on the government’s efforts to conta<strong>in</strong> the ris<strong>in</strong>g<br />
<strong>health</strong> care expenditures and encourage the private <strong>health</strong> <strong>sector</strong> to grow and participate<br />
effectively <strong>in</strong> the national economy.<br />
141
Jordan<br />
<strong>The</strong> study also identified some challenges that may h<strong>in</strong>der public–private partnership and<br />
should be jo<strong>in</strong>tly addressed. <strong>The</strong>se challenges <strong>in</strong>clude:<br />
• Shortage <strong>of</strong> national adm<strong>in</strong>istrative and technical skills <strong>in</strong> contract design, monitor<strong>in</strong>g and<br />
management.<br />
• Lack <strong>of</strong> <strong>in</strong>adequate computerized management <strong>in</strong>formation system <strong>in</strong> both <strong>sector</strong>s.<br />
• Lack <strong>of</strong> treatment protocols and guidel<strong>in</strong>es to control and monitor the quality <strong>of</strong> services.<br />
Even <strong>in</strong> the presence <strong>of</strong> these protocols, several private hospitals stated that they would be<br />
unwill<strong>in</strong>g to participate <strong>in</strong> the HIPP if cl<strong>in</strong>ical guidel<strong>in</strong>es were proposed (Banks D. and<br />
Shahrouri M., PHRplus, 2003).<br />
• Lack <strong>of</strong> cost analysis and proper pric<strong>in</strong>g mechanisms.<br />
• Creation <strong>of</strong> <strong>in</strong>centives for conduct<strong>in</strong>g multiple unnecessary procedures by the fee-for-service<br />
system, which reflects negatively on cost and quality <strong>of</strong> contracted services.<br />
• Lack <strong>of</strong> open and competitive procedures used for award<strong>in</strong>g contracts. Sole source<br />
recruitment may result <strong>in</strong> “fat and happy contractors” who do not have to <strong>in</strong>novate or<br />
improve their efficiency and have lucrative contracts.<br />
• Delay <strong>in</strong> payment due to bureaucratic procedures or short budget allocations. This delay was<br />
a ma<strong>in</strong> cause <strong>of</strong> poor levels <strong>of</strong> satisfaction with the M<strong>in</strong>istry <strong>of</strong> Health as a client (Banks, D.<br />
and Shahrouri, M., PHRplus, 2003), (Fahmi Alaostah, 2004).<br />
• Oversupply and duplication <strong>of</strong> expensive services caused by the uncontrolled growth <strong>of</strong> the<br />
private <strong>sector</strong>. Aggravated by the <strong>in</strong>efficient <strong>role</strong> <strong>of</strong> the Private Hospital Association, this<br />
situation is likely to weaken the barga<strong>in</strong><strong>in</strong>g position <strong>of</strong> the private hospitals and may lead to<br />
severe discounted prices. This eventually may have a negative impact on the quality <strong>of</strong><br />
contracted services.<br />
• <strong>The</strong> exist<strong>in</strong>g bureaucratic set-up and centralization <strong>of</strong> decision-mak<strong>in</strong>g and budgetary<br />
allocations that prevail <strong>in</strong> the M<strong>in</strong>istry <strong>of</strong> Health, as well as <strong>in</strong> other government<br />
organizations, which could be an obstacle to develop <strong>in</strong>novative and bus<strong>in</strong>ess like<br />
management <strong>in</strong> the Health Insurance Directorate.<br />
• Mutual trust and confidence do not always dom<strong>in</strong>ate the relationship between the M<strong>in</strong>istry <strong>of</strong><br />
Health and the private <strong>sector</strong>.<br />
Recommendations<br />
<strong>The</strong> follow<strong>in</strong>g recommendations are proposed to meet the above challenges and create an<br />
environment conductive to public–private collaboration <strong>in</strong> Jordan.<br />
1. A national programme for capacity build<strong>in</strong>g <strong>in</strong> contract design, monitor<strong>in</strong>g and<br />
management should be developed. This programme would help further strengthen the<br />
capacity <strong>of</strong> the private providers to deliver services effectively and efficiently.<br />
2. Treatment protocols and guidel<strong>in</strong>es should be developed to control the quality and<br />
appropriateness <strong>of</strong> the contracted services. <strong>The</strong> private <strong>sector</strong> should participate <strong>in</strong> the<br />
development <strong>of</strong> these standards.<br />
142
Jordan<br />
3. Prospective payment mechanisms (i.e. capitation, leas<strong>in</strong>g <strong>of</strong> services, case payment,<br />
bundl<strong>in</strong>g <strong>of</strong> services) should be explored and tested.<br />
4. <strong>The</strong> Health Insurance Directorate should be given greater autonomy, to <strong>in</strong>crease<br />
operational efficiency.<br />
5. Patients should be given more freedom to choose among contractors (autonomous public<br />
and private hospitals) with co-payment, <strong>in</strong> order to create market competition and improve<br />
efficiency and quality <strong>of</strong> contracted <strong>health</strong> services.<br />
6. Competitive and open bidd<strong>in</strong>g based on both technical responsiveness and price should be<br />
extended and encouraged. <strong>The</strong> major advantages <strong>of</strong> competitive bidd<strong>in</strong>g are that it will<br />
provide the least cost approach for the delivery <strong>of</strong> services, spark competition based on<br />
effectiveness and efficiency, and provide an objective basis for select<strong>in</strong>g contractors.<br />
7. A cost analysis system should be developed to provide real cost <strong>in</strong>formation for negotiat<strong>in</strong>g<br />
fair contract prices. <strong>The</strong> Jordan’s National Health Accounts Project could provide valuable<br />
<strong>in</strong>formation and technical assistance to develop a cost analysis system <strong>in</strong> public and private<br />
hospitals.<br />
8. <strong>The</strong> public and private <strong>sector</strong>s should develop and implement a computerized <strong>health</strong><br />
<strong>in</strong>formation system to manage contracts effectively and efficiently.<br />
9. On-time payment should be made a top priority for the M<strong>in</strong>istry <strong>of</strong> Health. Some <strong>of</strong> the<br />
options to achieve this <strong>in</strong>clude: remov<strong>in</strong>g bureaucratic barriers, secur<strong>in</strong>g budgetary<br />
allocations, provid<strong>in</strong>g <strong>in</strong>centives to HID staff for on-time payment, and pay<strong>in</strong>g monthly<br />
<strong>in</strong>stallments to providers.<br />
10. <strong>The</strong> private hospitals should work together and share experiences and identify areas (e.g.<br />
quality assurance, utilization review, cost analysis) where they may require additional<br />
tra<strong>in</strong><strong>in</strong>g, technical assistance or operational research. Strengthen<strong>in</strong>g and activat<strong>in</strong>g the<br />
Private Hospital Association should be <strong>of</strong> high priority for the private <strong>health</strong> <strong>sector</strong>.<br />
11. Government <strong>in</strong>centives (e.g. cont<strong>in</strong>u<strong>in</strong>g education, tax <strong>in</strong>centives, tra<strong>in</strong><strong>in</strong>g opportunities,<br />
s<strong>of</strong>t loans and fair prices) are important to the viability <strong>of</strong> the private <strong>sector</strong> and should be<br />
tailored to match the needs and stated <strong>health</strong> policy <strong>of</strong> the country. <strong>The</strong>se <strong>in</strong>centives will<br />
also set the platform for true partnership between the two <strong>sector</strong>s; a partnership that is built<br />
on mutual <strong>in</strong>terest and confidence.<br />
143
SOURCES<br />
Jordan<br />
Al-Aostah F, 2004. <strong>The</strong> Relationship between the Civil Health Insurance and the Private<br />
Hospitals <strong>in</strong> Jordan. Unpublished study, <strong>The</strong> Arab Academy for F<strong>in</strong>ancial and Bank<strong>in</strong>g Sciences,<br />
Amman, Jordan.<br />
Baniawad M, 2003. Assessment <strong>of</strong> the Contract between the MOH and Al-Mowasah Hospital,<br />
unpublished paper, Jordan University <strong>of</strong> Science and Technology, Jordan.<br />
Banks D, Shahrouri M, 2003. <strong>The</strong> Provision <strong>of</strong> Reproductive Health Services <strong>in</strong> Private<br />
Hospitals <strong>in</strong> Amman, Jordan, Partners for Health Reformplus, Amman, Jordan.<br />
Gaumer G, Murphy M, 2003. Health Insurance Pilot Project: Technical Assistance for the<br />
Implementation <strong>of</strong> Management Information System. Trip Report, Partners for Health<br />
Reformplus, Amman, Jordan.<br />
Health Insurance Directorate, 2002. Health Insurance Directorate Annual Report, 2002.<br />
Hsiao W. How Should A Nation F<strong>in</strong>ance Its Health Care? Paper presented to the World Bank<br />
Regional Sem<strong>in</strong>ar on Health Sector <strong>in</strong> Middle East and North Africa, 8–11 June, 1997, Cairo,<br />
Egypt.<br />
Jordan National Health Accounts, 2001. Draft Report, 2004.<br />
Kasawneh A, 2003. Review <strong>of</strong> Work Plan, Technical Accomplishments, Health Insurance Pilot<br />
Project, Partners for Health Reformplus. Amman, Jordan.<br />
K<strong>in</strong>g Abdullah Hospital, 2003. K<strong>in</strong>g Abdullah Hospital Annual Report, 2003<br />
M<strong>in</strong>istry <strong>of</strong> Health, 2002. Annual Report, 2002. Amman, Jordan.<br />
Royal Medical Services, 2002. Royal Medical Services Annual Report, 2002. Amman, Jordan.<br />
World Bank Group, 1997. Hashemite K<strong>in</strong>gdom <strong>of</strong> Jordan: <strong>health</strong> <strong>sector</strong> study. Wash<strong>in</strong>gton, DC.<br />
World Bank Group, 2002. Country pr<strong>of</strong>ile tables. Hhttp://www.worldbank.orgH<br />
World Health Organization, Regional Office for the Eastern Mediterranean 2003. Country<br />
pr<strong>of</strong>iles. Hhttp://www.emro.<strong>in</strong>tH<br />
World Health Organization, Regional Office for the Eastern Mediterranean 2003. <strong>The</strong> Role <strong>of</strong><br />
Contractual Arrangements <strong>in</strong> Improv<strong>in</strong>g Health Sector Performance <strong>in</strong> Countries <strong>of</strong> Eastern<br />
Mediterranean Region, Proposal Document, 2003.<br />
144
Jordan<br />
Annex 1<br />
CONTRACT/AGREEMENT ASSESSMENT TOOL<br />
Name <strong>of</strong> organization/hospital:<br />
Date <strong>of</strong> contract:<br />
Duration <strong>of</strong> the contract:<br />
Reason <strong>of</strong> contract<strong>in</strong>g (from both sides’ perspectives):<br />
Persons eligible:<br />
Services covered by the contract/services not covered:<br />
Patients’ referral system:<br />
Method <strong>of</strong> reimbursement (i.e. fee-for-service, per capita, etc….)<br />
Co-payment (if any):<br />
Claims and f<strong>in</strong>ancial reviews:<br />
Quality control methods (if any):<br />
Types <strong>of</strong> disputes:<br />
Ways <strong>of</strong> handl<strong>in</strong>g disputes:<br />
Contract amendments (if any):<br />
Information provided to beneficiaries about terms and benefits <strong>of</strong> the contract:<br />
Strengths (from both sides’ perspectives):<br />
Weaknesses (from both sides’ perspectives):<br />
Suggestions to improve the contract:<br />
145
Jordan<br />
Annex 2<br />
REQUEST FOR QUALIFICATION<br />
Hashemite K<strong>in</strong>gdom <strong>of</strong> Jordan<br />
Health Insurance Pilot Project (HIPP)<br />
(RFQ-HIPP-001)<br />
<strong>The</strong> Government <strong>of</strong> Jordan via the M<strong>in</strong>istry <strong>of</strong> Health (MOH), and the partners for Health<br />
Reform Plus, is seek<strong>in</strong>g expressions <strong>of</strong> <strong>in</strong>terest from qualified private hospitals <strong>in</strong> Jordan to<br />
participate <strong>in</strong> the Health Insurance Pilot Project (HIPP).<br />
<strong>The</strong> HIPP seeks to promote partnership between the public and private <strong>sector</strong>s, through the<br />
provision <strong>of</strong> hospital-based obstetric and newborn services to MOH beneficiaries. Private<br />
hospitals that participate <strong>in</strong> the HIPP will be selected through a competitive bidd<strong>in</strong>g process.<br />
Interested private hospitals, located <strong>in</strong> Amman, are asked to submit the follow<strong>in</strong>g <strong>in</strong>formation:<br />
A statement <strong>of</strong> qualification that details 1) the length <strong>of</strong> time that the hospital has been<br />
conduct<strong>in</strong>g bus<strong>in</strong>ess <strong>in</strong> Amman; 2) its location; 3) organizational chart, which clearly list<br />
the number <strong>of</strong> department with<strong>in</strong> the hospital; 4) utilization <strong>in</strong>formation: 5) number <strong>of</strong><br />
deliveries and C-sections performed dur<strong>in</strong>g the last year; 6) staff<strong>in</strong>g patterns, to <strong>in</strong>clude<br />
number <strong>of</strong> nurses, midwives, physicians and ancillary staff; 7) description <strong>of</strong> the medical<br />
records system currently be<strong>in</strong>g used; 8) relevant equipment <strong>in</strong>ventory, to <strong>in</strong>clude numbers<br />
and types <strong>of</strong> <strong>in</strong>cubators; 9) types <strong>of</strong> services provided (e.g.’ onsite pharmacy, radiology);<br />
10) number <strong>of</strong> operat<strong>in</strong>g rooms, <strong>in</strong>clud<strong>in</strong>g the availability <strong>of</strong> separate operat<strong>in</strong>g from for Csections;<br />
and 11) the availability <strong>of</strong> outpatient cl<strong>in</strong>ics for obstetrics and pediatrics.<br />
Statements <strong>of</strong> qualifications must be delivered to address below by 9 January 2004:<br />
PHRplus/HIPP<br />
P.O. Box 831152<br />
Amman 11181 Jordan<br />
Interested hospitals may obta<strong>in</strong> further <strong>in</strong>formation by contract<strong>in</strong>g the person listed below,<br />
dur<strong>in</strong>g <strong>of</strong>fice hours:<br />
PHRplus/HIPP<br />
Tel: 567-5507/09 Extension 14<br />
E-mail: akhasawneh@phr.com.jo<br />
146
Lebanon<br />
LEBANON
INTRODUCTION<br />
Lebanon<br />
Contractual <strong>arrangements</strong> play an important <strong>role</strong> <strong>in</strong> the <strong>health</strong> <strong>sector</strong> <strong>in</strong> Lebanon. This owes<br />
to two ma<strong>in</strong> historical developments <strong>in</strong> post-<strong>in</strong>dependence Lebanon: the organization <strong>of</strong><br />
Lebanon’s economy and social structure along a liberal model; and the pr<strong>of</strong>ound consequences<br />
<strong>of</strong> the civil war (1975–1991). S<strong>in</strong>ce its <strong>in</strong>dependence <strong>in</strong> 1943, Lebanese society has been<br />
organized along a liberal model, emphasiz<strong>in</strong>g relatively open markets and encouragement <strong>of</strong><br />
private <strong>in</strong>itiative, lead<strong>in</strong>g to gradual growth <strong>of</strong> the nongovernmental <strong>health</strong> <strong>sector</strong>.<br />
Concomitantly, dur<strong>in</strong>g the relatively prosperous years prior to the civil war, i.e. the 1950s–1960s,<br />
the state took steps towards ensur<strong>in</strong>g and protect<strong>in</strong>g citizens’ <strong>in</strong>terests <strong>in</strong> the <strong>health</strong> area, such as<br />
the establishment <strong>of</strong> the National Social Security Fund (NSSF) <strong>in</strong> 1961 and develop<strong>in</strong>g<br />
legislation to provide free <strong>health</strong> care for the <strong>in</strong>digent.<br />
<strong>The</strong> outbreak <strong>of</strong> civil war <strong>in</strong> 1975 put an end to ambitious plans for public <strong>health</strong><br />
protection, for example through expand<strong>in</strong>g the coverage <strong>of</strong> the NSSF to <strong>in</strong>clude the entire<br />
Lebanese population as well as establishment <strong>of</strong> a strong public <strong>health</strong> system. Dur<strong>in</strong>g the civil<br />
war years, the <strong>role</strong> <strong>of</strong> the government was severely limited. This affected both the provision <strong>of</strong><br />
<strong>health</strong> services, with pr<strong>of</strong>ound deterioration <strong>of</strong> governmental <strong>health</strong> facilities, as well as<br />
regulation <strong>of</strong> the <strong>health</strong> <strong>sector</strong>, <strong>in</strong>clud<strong>in</strong>g the stewardship <strong>role</strong> <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Public Health.<br />
<strong>The</strong> nongovernmental <strong>sector</strong> grew tremendously to fill the gap. For example, nongovernmental<br />
oragnizations played an important <strong>role</strong> <strong>in</strong> provid<strong>in</strong>g essential services <strong>in</strong> different areas <strong>in</strong><br />
Lebanon, across the l<strong>in</strong>es <strong>of</strong> divide. With the dismantl<strong>in</strong>g <strong>of</strong> the economy and worsen<strong>in</strong>g <strong>of</strong><br />
social conditions, the government played an <strong>in</strong>creas<strong>in</strong>gly important <strong>role</strong> as a f<strong>in</strong>ancer <strong>of</strong> <strong>health</strong><br />
services for un<strong>in</strong>sured Lebanese.<br />
In the post-civil war years s<strong>in</strong>ce 1991, the growth <strong>of</strong> the private <strong>sector</strong> cont<strong>in</strong>ued while the<br />
re-construction efforts <strong>of</strong> the successive governments took precedence over rebuild<strong>in</strong>g the <strong>health</strong><br />
care <strong>sector</strong>. <strong>The</strong> nongovernmental <strong>health</strong> <strong>sector</strong> (e.g. private practitioners, hospitals,<br />
nongovernmental organizations) became the dom<strong>in</strong>ant providers <strong>of</strong> <strong>in</strong>creas<strong>in</strong>gly complex, more<br />
expensive and high-tech specialist-based <strong>health</strong> care services, while governmental and public<br />
agencies (e.g. NSSF) became <strong>in</strong>creas<strong>in</strong>gly the f<strong>in</strong>ancers <strong>of</strong> these services. Health care costs skyrocketed<br />
(Lebanon spends 12%–13% <strong>of</strong> its GDP on <strong>health</strong>, second only to the US), but this was<br />
not associated with commensurate improvements <strong>in</strong> <strong>health</strong> outcomes. This led <strong>in</strong> the mid 1990s<br />
to <strong>in</strong>creas<strong>in</strong>g calls for <strong>health</strong> <strong>sector</strong> reforms and culm<strong>in</strong>ated with the formation <strong>of</strong> an <strong>in</strong>term<strong>in</strong>isterial<br />
reform committee to design large-scale reforms, aided by a US$ 37 million loan from<br />
the World Bank. Due to multiple factors, large-scale reform efforts have not proved successful.<br />
While discussions on the scope <strong>of</strong> reform cont<strong>in</strong>ue today, there is <strong>in</strong>creas<strong>in</strong>g recognition <strong>of</strong><br />
the importance <strong>of</strong> smaller scale reforms. For example, the M<strong>in</strong>istry <strong>of</strong> Public Heatlh has tried to<br />
assume a more visible and more effective regulatory <strong>role</strong>, which corresponds to its important<br />
<strong>role</strong>s as a f<strong>in</strong>ancer <strong>of</strong> <strong>health</strong> care services for a large segment <strong>of</strong> the Lebanese population and as a<br />
steward <strong>of</strong> the <strong>health</strong> system. Other f<strong>in</strong>anc<strong>in</strong>g agencies also <strong>in</strong>creas<strong>in</strong>gly see the need to use tools<br />
148
Lebanon<br />
at their disposal for regulat<strong>in</strong>g <strong>health</strong> care services and improv<strong>in</strong>g quality <strong>of</strong> care, while<br />
controll<strong>in</strong>g <strong>health</strong> care costs. Contractual <strong>arrangements</strong> are among the ma<strong>in</strong> tools that these<br />
agencies have for carry<strong>in</strong>g out these tasks. <strong>The</strong> ma<strong>in</strong> objective <strong>of</strong> this report, therefore, is to<br />
evaluate how well this is done given the available opportunities.<br />
<strong>The</strong> specific aims that correspond to this objective <strong>in</strong>clude:<br />
1. Describe current <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> which the ma<strong>in</strong> public agencies are <strong>in</strong>volved.<br />
Focus on <strong>contractual</strong> <strong>arrangements</strong> <strong>of</strong> the MOPH.<br />
Exam<strong>in</strong>e case studies <strong>of</strong> hospitalization and ambulatory care.<br />
2. Evaluate <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> terms <strong>of</strong> their ability to meet the stated needs <strong>in</strong> terms<br />
<strong>of</strong>:<br />
Respond<strong>in</strong>g to demands <strong>of</strong> f<strong>in</strong>anc<strong>in</strong>g agencies.<br />
Fulfill<strong>in</strong>g essential public <strong>health</strong> functions, especially public <strong>health</strong> protection.<br />
3. Address the questions posed <strong>in</strong> the study questionnaire distributed by the WHO Regional<br />
Office for the Eastern Mediterranean..<br />
Contractual <strong>arrangements</strong> are but one tool <strong>in</strong> the hands <strong>of</strong> <strong>health</strong> policy-makers to enhance<br />
performance <strong>of</strong> the <strong>health</strong> <strong>sector</strong>. <strong>The</strong>refore, evaluation <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> must<br />
consider other tools and mechanisms. Nevertheless, <strong>in</strong> a country like Lebanon, where<br />
nongovernmental parties dom<strong>in</strong>ate the <strong>health</strong> <strong>sector</strong>, the <strong>contractual</strong> <strong>arrangements</strong> by themselves<br />
merit evaluation as a key tool for regulat<strong>in</strong>g performance <strong>of</strong> the different functions <strong>of</strong> <strong>health</strong> care<br />
delivery. This is the ma<strong>in</strong> rationale for this effort.<br />
APPROACH AND METHODS<br />
Conceptual framework and approach<br />
<strong>The</strong> first aim <strong>of</strong> the report is to provide a technical overview <strong>of</strong> contract<strong>in</strong>g <strong>arrangements</strong> <strong>in</strong><br />
Lebanon. <strong>The</strong> report attempts to synthesize data from multiple resources to understand, and when<br />
possible assess, the contribution and performance <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> the <strong>health</strong><br />
<strong>sector</strong>. <strong>The</strong> report utilizes commonly available <strong>in</strong>dicators, such as those <strong>of</strong> process <strong>in</strong>dicators,<br />
utilization patterns and expenditures, to achieve this purpose.<br />
<strong>The</strong> report also aims to review <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> light <strong>of</strong> broader <strong>health</strong> care<br />
<strong>sector</strong> and <strong>health</strong> system issues <strong>in</strong> Lebanon. To this end, the report evaluates <strong>contractual</strong><br />
<strong>arrangements</strong> <strong>in</strong> relation to two overarch<strong>in</strong>g concerns, social protection and equity.<br />
Consequently, the report attempts to look beyond cost and technical and adm<strong>in</strong>istrative efficiency<br />
<strong>in</strong>to how contract<strong>in</strong>g <strong>arrangements</strong> are able to serve foremost those most <strong>in</strong> need. Many <strong>of</strong> the<br />
available <strong>in</strong>dicators, however, do not tell the whole story <strong>of</strong> the ability <strong>of</strong> the contract<strong>in</strong>g<br />
<strong>arrangements</strong>, or for that matter the <strong>health</strong> <strong>sector</strong>, to contribute to social protection and to<br />
improv<strong>in</strong>g equity. Other <strong>in</strong>dicators, e.g. those expos<strong>in</strong>g <strong>in</strong>equalities, are needed but are<br />
149
Lebanon<br />
commonly miss<strong>in</strong>g. In such a situation, expos<strong>in</strong>g equity-sensitive deficiencies <strong>of</strong> knowledge,<br />
attitudes, practices by contract<strong>in</strong>g partners, and areas where data needs to be collected, become<br />
important <strong>in</strong> itself and this has been the approach taken here.<br />
Many <strong>of</strong> the major determ<strong>in</strong>ants <strong>of</strong> <strong>health</strong> lie outside the <strong>health</strong> <strong>sector</strong>. Choices and<br />
contents <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> are directly affected by the positions <strong>of</strong> regulat<strong>in</strong>g bodies<br />
(i.e. government) on the relevance <strong>of</strong> broad determ<strong>in</strong>ants to <strong>health</strong> and <strong>health</strong> <strong>sector</strong><br />
performance. Such determ<strong>in</strong>ants are rarely reflected, however, <strong>in</strong> discussions <strong>of</strong> <strong>contractual</strong><br />
<strong>arrangements</strong>. Analyz<strong>in</strong>g <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> light <strong>of</strong> sociopolitical determ<strong>in</strong>ants<br />
requires understand<strong>in</strong>g <strong>of</strong> the performance <strong>of</strong> the Lebanese economy and social and political<br />
organization. While such a broad analysis may be beyond our focus, they constitute the context<br />
with<strong>in</strong> which <strong>contractual</strong> <strong>arrangements</strong> must be understood. As such, an attempt must be made to<br />
br<strong>in</strong>g these perspectives <strong>in</strong> discussions <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong>. <strong>The</strong> Report attempts to do so<br />
<strong>in</strong> a modest way.<br />
If “<strong>health</strong> <strong>sector</strong>” is <strong>in</strong>terpreted broadly to mean “<strong>health</strong> system”, then <strong>contractual</strong><br />
<strong>arrangements</strong> must be evaluated <strong>in</strong> a much broader context. This would necessitate evaluation <strong>of</strong><br />
how <strong>contractual</strong> <strong>arrangements</strong> relate not only to <strong>health</strong> care delivery but also to performance <strong>of</strong><br />
other, broader, components <strong>of</strong> the <strong>health</strong> system, such as nutrition and basic social services.<br />
Because this endeavour is potentially complex and very wide <strong>in</strong> scope, limited reference is made<br />
to <strong>health</strong> system issues beyond care delivery.<br />
While there are opportunities to improve the use <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> as a tool,<br />
recommendations for so do<strong>in</strong>g cannot be separated from the broader issues <strong>of</strong> <strong>health</strong> <strong>sector</strong><br />
reform <strong>in</strong> Lebanon. A detailed consideration <strong>of</strong> <strong>health</strong> <strong>sector</strong> reform <strong>in</strong> Lebanon is beyond the<br />
focus <strong>of</strong> this report. However, an attempt is made to contextualize recommendations for<br />
improv<strong>in</strong>g use <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> relation to previously made recommendations for<br />
<strong>health</strong> <strong>sector</strong> reform <strong>in</strong> Lebanon.<br />
Consider<strong>in</strong>g the sheer number and breadth <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> Lebanon, there<br />
are multiple ways <strong>of</strong> classify<strong>in</strong>g and summariz<strong>in</strong>g these <strong>arrangements</strong>. This can be done<br />
accord<strong>in</strong>g to which agency is <strong>in</strong>volved (e.g. MOPH or NSSF), contracted party (e.g. hospitals,<br />
primary care centres, or other parties), types <strong>of</strong> service provided (e.g. hospitalization versus<br />
outpatient services), or other criteria. In this Report, an attempt was made to provide <strong>in</strong>sights <strong>in</strong>to<br />
<strong>contractual</strong> <strong>arrangements</strong> from different angles to enhance understand<strong>in</strong>g <strong>of</strong> the complexity <strong>of</strong><br />
the issues. A mixed approach is taken <strong>in</strong> which contracts are briefly mentioned accord<strong>in</strong>g to the<br />
different governmental agencies <strong>in</strong>volved, while case studies <strong>in</strong>vestigate specific aspects <strong>of</strong><br />
service delivery.<br />
F<strong>in</strong>ally, an attempt is made to proceed beyond identification <strong>of</strong> problems <strong>in</strong>to recogniz<strong>in</strong>g<br />
aspects <strong>of</strong> good performance and opportunities for improv<strong>in</strong>g performance.<br />
150
Research methods and data sources<br />
Lebanon<br />
<strong>The</strong> follow<strong>in</strong>g methods were <strong>in</strong> light <strong>of</strong> the conceptual framework and approach.<br />
1. Review <strong>of</strong> literature on contract<strong>in</strong>g <strong>arrangements</strong>. Literature on contract<strong>in</strong>g <strong>arrangements</strong><br />
supplied by the Eastern Mediterranean Regional Office was reviewed. Additional peerreviewed<br />
literature was sought on Medl<strong>in</strong>e as well on the <strong>in</strong>ternet us<strong>in</strong>g two <strong>in</strong>dependent<br />
search eng<strong>in</strong>es.<br />
2. Review <strong>of</strong> literature and reports on <strong>health</strong> <strong>sector</strong> <strong>in</strong> Lebanon. Literature concern<strong>in</strong>g <strong>health</strong><br />
<strong>sector</strong> <strong>in</strong> Lebanon was reviewed to better summarize the current Lebanese situation,<br />
develop the conceptual framework <strong>in</strong> light <strong>of</strong> literature on <strong>contractual</strong> <strong>arrangements</strong>, and<br />
identify key performance <strong>in</strong>dicators which are relevant to the Lebanese context. Several<br />
sources <strong>of</strong> data were searched.<br />
Peer reviewed literature on and <strong>health</strong> and <strong>health</strong> <strong>sector</strong> <strong>in</strong> Lebanon was sought on<br />
Medl<strong>in</strong>e. <strong>The</strong> Lebanese Corner at the Saab Medical Library at the American<br />
University, the largest <strong>health</strong> library <strong>in</strong> Lebanon, was manually searched as it conta<strong>in</strong>s<br />
articles that are not electronically <strong>in</strong>dexed.<br />
<strong>The</strong> <strong>in</strong>ternet was searched for relevant documents us<strong>in</strong>g two different search eng<strong>in</strong>es.<br />
<strong>The</strong> <strong>health</strong> <strong>in</strong>formation centre recently created at WHO country <strong>of</strong>fice <strong>in</strong> Beirut was also<br />
searched for additional literature.<br />
Regional journals, such as the Eastern Mediterranean Health Journal, which are not fully<br />
<strong>in</strong>dexed by Medl<strong>in</strong>e were manually searched and issues cover<strong>in</strong>g the past 5 years<br />
were screened for articles concern<strong>in</strong>g <strong>health</strong> and <strong>health</strong> <strong>sector</strong> performance <strong>in</strong><br />
Lebanon.<br />
Documents concern<strong>in</strong>g public <strong>health</strong> <strong>in</strong> Lebanon produced by different governmental<br />
<strong>of</strong>fices, especially the M<strong>in</strong>istry <strong>of</strong> Public Health, <strong>in</strong>ternational agencies, e.g. WHO<br />
and World Bank, academic <strong>in</strong>stitutions were reviewed for material relevant to<br />
<strong>contractual</strong> <strong>arrangements</strong>.<br />
3. Key <strong>in</strong>formant <strong>in</strong>terviews. Interviews were conducted with key <strong>in</strong>formants from the<br />
different public f<strong>in</strong>anc<strong>in</strong>g agencies (e.g. M<strong>in</strong>istry <strong>of</strong> Public Health, M<strong>in</strong>istry <strong>of</strong> Social<br />
Affairs, National Social Security Fund), <strong>in</strong>ternational agencies (e.g. World Health<br />
Organization), academia, public <strong>health</strong> experts, and consumers. <strong>The</strong> scope <strong>of</strong> <strong>in</strong>terviews<br />
could have been expanded quite considerably to <strong>in</strong>clude all partners, but time and<br />
resources were limited. Furthermore, the report draws on the <strong>in</strong>timate knowledge <strong>of</strong> the<br />
author <strong>of</strong> <strong>health</strong> <strong>sector</strong> issues <strong>in</strong> Lebanon, which fills some <strong>of</strong> the gap <strong>in</strong> the <strong>in</strong>terview<br />
schedule. Although the study could have solicited more consumer voices as well as more<br />
151
Lebanon<br />
<strong>in</strong>put from contracted parties, the study was not designed for this purpose and therefore this<br />
was limited <strong>in</strong> scope.<br />
4. Synthesis <strong>of</strong> data. Information from multiple sources was synthesized. In light <strong>of</strong> the<br />
breadth <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> Lebanon, several case studies were conducted,<br />
rather than focus<strong>in</strong>g on one study, to exam<strong>in</strong>e the performance <strong>of</strong> different levels <strong>of</strong> the<br />
<strong>health</strong> <strong>sector</strong> <strong>in</strong> Lebanon. Review<strong>in</strong>g several case studies jo<strong>in</strong>tly also allowed for<br />
identification <strong>of</strong> important opportunities for improv<strong>in</strong>g performance through strategies <strong>of</strong><br />
coord<strong>in</strong>ation and <strong>in</strong>tegration.<br />
5. Summary <strong>of</strong> f<strong>in</strong>d<strong>in</strong>gs and recommendations. Based on exam<strong>in</strong>ation <strong>of</strong> current situation, a<br />
scorecard is developed to illustrate where <strong>contractual</strong> <strong>arrangements</strong> have succeeded and<br />
failed, and to identify future steps that can be taken to improve performance. A set <strong>of</strong><br />
recommendations are provided. <strong>The</strong>se build on identified strengths and weaknesses. <strong>The</strong>y<br />
represent a po<strong>in</strong>t for discussion with different stakeholders <strong>in</strong> Lebanon.<br />
<strong>The</strong> checklist provided by the Regional Office for assess<strong>in</strong>g the <strong>role</strong> <strong>of</strong> <strong>contractual</strong><br />
<strong>arrangements</strong> was useful both <strong>in</strong> guid<strong>in</strong>g <strong>in</strong> the actual research and <strong>in</strong> develop<strong>in</strong>g the report.<br />
However, it was not possible to answer all questions <strong>in</strong> the checklist mean<strong>in</strong>gfully for all the<br />
different <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> Lebanon. This is mostly due to the sheer number <strong>of</strong> these<br />
<strong>arrangements</strong>.<br />
FINDINGS<br />
Health <strong>sector</strong> <strong>in</strong> Lebanon<br />
Lebanon is a middle-<strong>in</strong>come country <strong>of</strong> approximately 4 million <strong>in</strong>habitants (80%<br />
urbanized) who live <strong>in</strong> 6 adm<strong>in</strong>istrative regions, or mohafazat. <strong>The</strong> greater Beirut area houses<br />
more than 40% <strong>of</strong> the population. Around 45% <strong>of</strong> Lebanese are under the age <strong>of</strong> 21 years and<br />
10% are over age 65. Lebanon has favourable <strong>health</strong> <strong>in</strong>dicators compared with other countries <strong>of</strong><br />
the Eastern Mediterranean Region: life expectancy is 72 years for females and 69 years for<br />
males; overall and <strong>in</strong>fant mortality rates are 7 and 28 per 1000, respectively (regional <strong>health</strong><br />
<strong>in</strong>equalities are notable). Lebanon has undergone an epidemiological transition, with over 80%<br />
<strong>of</strong> the current mortality burden due to noncommunicable diseases and 10% due to <strong>in</strong>juries. <strong>The</strong><br />
morbidity pr<strong>of</strong>ile, compiled <strong>in</strong> the context <strong>of</strong> a national burden <strong>of</strong> disease study, suggests a<br />
similar pattern.<br />
Health is an important component <strong>of</strong> economic activities, consum<strong>in</strong>g 12%–13% <strong>of</strong> GDP.<br />
Most <strong>health</strong> spend<strong>in</strong>g, however, is out-<strong>of</strong>-pocket (around 70%–75%), more heavily shouldered<br />
by the poorer segments. Slightly more than 10% <strong>of</strong> all public expenditures go to <strong>health</strong>. <strong>The</strong><br />
ma<strong>in</strong> public f<strong>in</strong>ancers are: the M<strong>in</strong>istry <strong>of</strong> Public Heatlh (receives 4% <strong>of</strong> the total budget and 1%<br />
<strong>of</strong> GDP), NSSF, Civil Service Cooperative (CSC), M<strong>in</strong>istry <strong>of</strong> Defense, M<strong>in</strong>istry <strong>of</strong> the Interior<br />
152
Lebanon<br />
and local municipalities. Enrollees and beneficiaries <strong>of</strong> these f<strong>in</strong>anc<strong>in</strong>g schemes are discussed<br />
later.<br />
Due to past unregulated growth <strong>of</strong> the private <strong>sector</strong>, which dom<strong>in</strong>ates the provision <strong>of</strong><br />
<strong>health</strong> services, and various malfunctions <strong>of</strong> the public <strong>sector</strong>, the <strong>health</strong> <strong>sector</strong> suffers from<br />
chronic <strong>in</strong>efficiency, poor mix <strong>of</strong> providers and waste. This is true for both ambulatory care as<br />
well as hospitalization. Over 160 hospitals are licensed, <strong>of</strong> which more than 85% are private.<br />
<strong>The</strong>re is gross oversupply <strong>of</strong> small (less than 100 beds) hospitals (73%). Only 5 hospitals have<br />
more than 200 beds. Hospital beds are <strong>in</strong> oversupply, with 12 000, beds or around 26 per 1000<br />
population. <strong>The</strong> low occupancy rates (45%–50%) further contribute to poor economies <strong>of</strong> scale.<br />
<strong>The</strong>re is oversupply <strong>of</strong> high technology <strong>in</strong> Lebanon (please see section on CABG under Case<br />
studies) which humbles the limited availability <strong>of</strong> similar technologies <strong>in</strong> many <strong>in</strong>dustrialized<br />
countries. Correspond<strong>in</strong>gly, there is oversupply <strong>of</strong> specialized physicians. Indeed, over 70% <strong>of</strong><br />
physicians <strong>in</strong> Lebanon are specialists, the <strong>in</strong>verse <strong>of</strong> the ratio <strong>in</strong> the United K<strong>in</strong>gdom, where the<br />
specialist/generalist mix is 30/70. Over 11 000 physicians are currently registered <strong>in</strong> the two<br />
Orders <strong>of</strong> Physicians <strong>in</strong> Lebanon. <strong>The</strong> exact number <strong>of</strong> practis<strong>in</strong>g physicians is not known, but<br />
probably 15%–20% are practic<strong>in</strong>g abroad. Medical practices are not commonly organized<br />
accord<strong>in</strong>g to groups <strong>of</strong> either s<strong>in</strong>gle or multiple specialties, thus <strong>in</strong>creas<strong>in</strong>g overhead and cost <strong>of</strong><br />
care and reduc<strong>in</strong>g efficiency. Medical care is mostly fee-for-service or flat-rate based. <strong>The</strong>re are<br />
no managed care or capitation plans <strong>in</strong> Lebanon. Non-physician cl<strong>in</strong>icians are undersupplied <strong>in</strong><br />
Lebanon. For example, the nurs<strong>in</strong>g rate per capita <strong>in</strong> Lebanon is among the lowest <strong>in</strong> the world.<br />
Health care utilization is relatively high <strong>in</strong> Lebanon. Because Lebanon is a small country,<br />
access to medical services is not a major problem, although some areas rema<strong>in</strong> plagued with low<br />
<strong>health</strong> care access rates. Around 12% <strong>of</strong> the population is hospitalized per year. Because <strong>of</strong><br />
multiple factors, <strong>in</strong>clud<strong>in</strong>g undersupply <strong>of</strong> public hospitals, perceived low quality and social<br />
stigma <strong>in</strong> a culture that is image-conscious, most hospitalization is <strong>in</strong> the private <strong>sector</strong>. Around<br />
28% <strong>of</strong> Lebanese uses ambulatory care services per month; the average number <strong>of</strong> ambulatory<br />
care visits per year is 4. <strong>The</strong>re is an abundance <strong>of</strong> public and nongovernmental organization<br />
ambulatory <strong>health</strong> centres, over 110 primary care centres and over 400 dispensaries. However,<br />
most ambulatory care takes place <strong>in</strong> the private <strong>sector</strong> where it is problem-oriented and<br />
specialist-provided. Emphasis on prevention and <strong>health</strong> promotion is severely lack<strong>in</strong>g.<br />
<strong>The</strong>re have been multiple attempts at <strong>health</strong> <strong>sector</strong> reform <strong>in</strong> Lebanon s<strong>in</strong>ce the end <strong>of</strong> the<br />
civil war. This has <strong>in</strong>cluded a large World Bank-funded project. Large ambitious reform<br />
packages have not received political support, despite their perceived urgency. In this climate,<br />
public agencies, especially the M<strong>in</strong>istry <strong>of</strong> Public Health, are try<strong>in</strong>g to rega<strong>in</strong> regulatory powers<br />
and improve their stewardship <strong>of</strong> the <strong>health</strong> <strong>sector</strong>. This has proved to be challeng<strong>in</strong>g consider<strong>in</strong>g<br />
the large and powerful private <strong>sector</strong>, the limited political support, lack <strong>of</strong> citizen engagement<br />
and limited capacities <strong>of</strong> the public <strong>sector</strong>.<br />
153
Contract<strong>in</strong>g <strong>arrangements</strong>: An overview<br />
Lebanon<br />
Contractual <strong>arrangements</strong> <strong>in</strong> Lebanon cover a broad range <strong>of</strong> services. <strong>The</strong>se <strong>in</strong>clude direct<br />
<strong>health</strong> care services, such as hospitalization and ambulatory care, <strong>in</strong>direct <strong>health</strong> care services,<br />
such as procurements <strong>of</strong> essential drugs and vacc<strong>in</strong>es, and public <strong>health</strong> services, such as<br />
adm<strong>in</strong>istration <strong>of</strong> programmes and supply <strong>of</strong> public <strong>health</strong> expertise.<br />
Table 1 summarizes <strong>contractual</strong> <strong>arrangements</strong> for direct <strong>health</strong> care services, the ma<strong>in</strong> form<br />
<strong>of</strong> services provided through contract<strong>in</strong>g <strong>in</strong> Lebanon. <strong>The</strong> 5 major public f<strong>in</strong>anc<strong>in</strong>g schemes,<br />
supported by the M<strong>in</strong>istry <strong>of</strong> Public Health, NSSF, CSC, M<strong>in</strong>istry <strong>of</strong> Defence, and M<strong>in</strong>istry <strong>of</strong><br />
Interior (note these reflect 3 separate funds), cover roughly 80% <strong>of</strong> the Lebanese population. <strong>The</strong><br />
rest <strong>of</strong> the population is covered by private <strong>in</strong>surance and mutuality funds. Health care through<br />
these schemes is mostly based on contract<strong>in</strong>g, which underscores the important <strong>role</strong> <strong>of</strong><br />
contract<strong>in</strong>g <strong>in</strong> Lebanon.<br />
<strong>The</strong> <strong>contractual</strong> <strong>arrangements</strong> cover a range <strong>of</strong> heath care services (Table 2). <strong>The</strong> largest<br />
three f<strong>in</strong>anc<strong>in</strong>g schemes, those <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Public Health, NSSF and CSC, all <strong>in</strong>clude<br />
some level <strong>of</strong> co-payment by beneficiaries. All non-M<strong>in</strong>istry <strong>of</strong> Public Health funds <strong>in</strong>clude<br />
coverage for family members. For Lebanese eligible for the M<strong>in</strong>istry <strong>of</strong> Public Health scheme,<br />
application for coverage must be done on a personal basis. <strong>The</strong>refore, family coverage is not<br />
applicable. <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public Health coverage, a last resort for the un<strong>in</strong>sured and for<br />
services for catastrophic illness not covered by those <strong>in</strong>sured under other schemes, is considered<br />
a temporary solution to improve equity until a more long-term f<strong>in</strong>anc<strong>in</strong>g scheme can be<br />
developed that <strong>in</strong>cludes the whole population. Unfortunately, this has proved difficult to<br />
accomplish despite several attempts at reform over the past decade.<br />
<strong>The</strong> costs <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> Lebanon are substantial (Table 3). Hospitalization<br />
receives the largest share <strong>of</strong> expenditures, when tak<strong>in</strong>g <strong>in</strong>to account all schemes. For non-<br />
M<strong>in</strong>istry <strong>of</strong> Public Health <strong>contractual</strong> schemes, hospitalization services account for<br />
approximately 52%–55% and ambulatory care for 45%–48% <strong>of</strong> direct <strong>health</strong> care costs. What is<br />
most noticeable is the several-fold difference <strong>in</strong> the cost per beneficiary among the different<br />
funds.<br />
154
Lebanon<br />
Table 1. Contractual <strong>arrangements</strong> <strong>in</strong>volv<strong>in</strong>g direct <strong>health</strong> care services<br />
Responsible<br />
governmental party<br />
M<strong>in</strong>istry <strong>of</strong> Public<br />
Health<br />
F<strong>in</strong>anc<strong>in</strong>g body<br />
(Fund)<br />
M<strong>in</strong>istry <strong>of</strong> Public<br />
Health Fund<br />
M<strong>in</strong>istry <strong>of</strong> Labour National Social<br />
Security Fund –<br />
Maternity and<br />
Sickness Fund<br />
Presidency <strong>of</strong> Council<br />
<strong>of</strong> M<strong>in</strong>isters<br />
Civil Servant<br />
Cooperative Health<br />
Fund<br />
Contracted party(ies) Type(s) <strong>of</strong> contracted<br />
party(ies)<br />
Public and public<br />
hospitals, primary care<br />
centres<br />
Private hospitals,<br />
private generalist and<br />
specialist physicians,<br />
midwifes, pharmacies<br />
Mix (governmental/for<br />
pr<strong>of</strong>it/non-pr<strong>of</strong>it/NGO)<br />
Mix (for pr<strong>of</strong>it/non-forpr<strong>of</strong>it)<br />
Number <strong>of</strong><br />
beneficiaries<br />
% <strong>of</strong> population<br />
covered<br />
1 934 415 48 All regions<br />
712 890 18 All regions<br />
Same Same 180 225 5 All regions<br />
M<strong>in</strong>istry <strong>of</strong> Defence Armed Forces Fund Same Same 260 000 7 All regions<br />
M<strong>in</strong>istry <strong>of</strong> the<br />
Interior<br />
Internal Security<br />
Fund<br />
General Services<br />
Fund<br />
Secret Services<br />
Fund<br />
Same Same 53 000 1 All regions<br />
Same Same 9000 0.2 All regions<br />
Same Same 2405 0.1 All regions<br />
Geographical<br />
coverage
Lebanon<br />
Table 2. Coverage <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>of</strong> <strong>health</strong> care services<br />
F<strong>in</strong>anc<strong>in</strong>g body (Fund) Eligibility Coverage Payment by<br />
government (%)<br />
M<strong>in</strong>istry <strong>of</strong> Public Health<br />
Fund<br />
National Social Security<br />
Fund - Maternity and<br />
Sickness Fund<br />
Civil Servant Cooperative<br />
Health Fund<br />
156<br />
Co-payment by<br />
beneficiary (%)<br />
Un<strong>in</strong>sured Lebanese Hospital care 85 15 NA<br />
Un<strong>in</strong>sured Lebanese and <strong>in</strong>sured<br />
Lebanese whose plans do not cover<br />
drugs<br />
Any Lebanese present<strong>in</strong>g to primary<br />
care centre<br />
Dispens<strong>in</strong>g expensive drugs<br />
for catastrophic illness (e.g.<br />
cancer)<br />
Provid<strong>in</strong>g vacc<strong>in</strong>es and<br />
essential drugs to primary<br />
care centre<br />
100 0 NA<br />
100 0 NA<br />
Formal and service <strong>sector</strong> employees,<br />
public wage earners, employees <strong>of</strong><br />
<strong>in</strong>dependent public orgs.<br />
Hospital care 90 10 Yes<br />
Same Ambulatory care 85 15 Yes<br />
Public <strong>sector</strong> staff and dependents Hospital care 90 10 Yes<br />
Same Ambulatory and dental care 75 25 Yes<br />
Armed Forces Fund Army staff and dependents Hospital and ambulatory<br />
care<br />
M<strong>in</strong>istry <strong>of</strong> Interior -<br />
Internal Security Fund<br />
M<strong>in</strong>istry <strong>of</strong> Interior -<br />
General Services Fund<br />
M<strong>in</strong>istry <strong>of</strong> Interior -Secret<br />
Services Fund<br />
Staff and members Hospital and ambulatory<br />
care<br />
Same Hospital and ambulatory<br />
care<br />
Same Hospital and ambulatory<br />
care<br />
100 0 Yes<br />
100 0 Yes<br />
100 0 Yes<br />
100 0 Yes<br />
Coverage <strong>of</strong><br />
family<br />
members
Lebanon<br />
Table 3. Costs <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>of</strong> <strong>health</strong> care services<br />
F<strong>in</strong>anc<strong>in</strong>g body (Fund)<br />
M<strong>in</strong>istry <strong>of</strong> Public<br />
Health Fund<br />
Source <strong>of</strong> f<strong>in</strong>anc<strong>in</strong>g Total expenditures<br />
(US$)<br />
National Social Security<br />
Fund-Maternity and<br />
Sickness Fund<br />
Civil Servant<br />
Cooperative Health<br />
Fund<br />
Expenditure per<br />
beneficiary<br />
Government budget 138 766 667 72<br />
Government budget,<br />
employers, employees *<br />
131 600 000 185<br />
Government budget 29 674 000 165<br />
Armed Forces Fund Same 38 978 000 150<br />
M<strong>in</strong>istry <strong>of</strong> Interior -<br />
Internal Security Fund<br />
Same 24 666 667 465<br />
M<strong>in</strong>istry <strong>of</strong> Interior -<br />
General Services Fund<br />
Same 3 373 333 375<br />
M<strong>in</strong>istry <strong>of</strong> Interior -<br />
Secret Services Fund<br />
Same 1 525 333 634<br />
Contractual <strong>arrangements</strong> <strong>of</strong> public agencies<br />
M<strong>in</strong>istry <strong>of</strong> Public Health<br />
As shown <strong>in</strong> Table 4, the M<strong>in</strong>istry <strong>of</strong> Public Health engages <strong>in</strong> different types <strong>of</strong> contracts<br />
to accomplish its public <strong>health</strong> mission. Key aspects <strong>of</strong> these contracts are highlighted below.<br />
• Support <strong>of</strong> primary care services. More <strong>in</strong>formation about this is <strong>in</strong>cluded under case studies.<br />
• Under-writ<strong>in</strong>g costs <strong>of</strong> hospitalization for the un<strong>in</strong>sured: more <strong>in</strong>formation about this is<br />
<strong>in</strong>cluded under case studies.<br />
• Support <strong>of</strong> NGO work on <strong>health</strong> and <strong>health</strong> determ<strong>in</strong>ants. <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public Health has<br />
contracts with several social/<strong>health</strong> nongovernmental organizations to support their work<br />
provided they spend the allocated funds on <strong>health</strong> or <strong>health</strong>-related aspects, even if the focus<br />
is not directly on primary care services. For example, Dar al Aytam al Islamiah (Islamic<br />
House <strong>of</strong> Orphans) is given support for nutrition and other aspects <strong>of</strong> social support that is<br />
considered by the M<strong>in</strong>istry <strong>of</strong> Public Health to <strong>in</strong>fluence important <strong>health</strong> determ<strong>in</strong>ants. <strong>The</strong><br />
Chronic Care Centre, which serves patients with conditions such as type 1 diabetes and<br />
thalassemia, presents an example <strong>of</strong> direct support for <strong>health</strong> services Around 12<br />
centres/organizations receive such support (each typically <strong>in</strong> the range <strong>of</strong> US$ 300 000),<br />
which is important for their overall function<strong>in</strong>g. In return, these organizations submit an<br />
annual report <strong>of</strong> contract-related activities. Choice <strong>of</strong> nongovernmental organization is<br />
commonly <strong>in</strong>fluenced by political considerations. Thus, these contracts, which are diversified<br />
<strong>in</strong> nature and duration, are not based on an open bidd<strong>in</strong>g or competitive process.<br />
Furthermore, the M<strong>in</strong>istry <strong>of</strong> Public Health has not developed criteria for assess<strong>in</strong>g
Lebanon<br />
Table 4. Contractual <strong>arrangements</strong> <strong>of</strong> M<strong>in</strong>istry <strong>of</strong> Public Health<br />
Area <strong>of</strong> contract Contracted<br />
party(ies)<br />
Hospital services Private hospitals<br />
(103)<br />
Public hospitals<br />
(20)<br />
Primary care<br />
services<br />
Essential drugs for<br />
chronic diseases<br />
PCC (45 centres<br />
<strong>in</strong> 2003)<br />
Type(s) <strong>of</strong><br />
provider<br />
Mix (for<br />
pr<strong>of</strong>it/non-/NGO)<br />
YMCA International<br />
NGO<br />
Start <strong>of</strong> contract<strong>in</strong>g<br />
arrangement<br />
Length <strong>of</strong><br />
contract<br />
Ongo<strong>in</strong>g Annual,<br />
renewable<br />
Public Ongo<strong>in</strong>g Annual,<br />
renewable<br />
Public/NGO Ongo<strong>in</strong>g–national<br />
plan <strong>in</strong>itiated 1996<br />
1991 Annual,<br />
renewable<br />
Immunization UNICEF UN Agency 1991 Annual,<br />
renewable<br />
Basic social services NGO’s NGOs Ongo<strong>in</strong>g Annual,<br />
renewable<br />
National <strong>health</strong><br />
programmes<br />
Public <strong>health</strong><br />
expertise<br />
WHO UN Agency 1991 Annual,<br />
renewable<br />
Health<br />
pr<strong>of</strong>essionals<br />
Maternal care Makassed Health<br />
System<br />
Various <strong>health</strong><br />
pr<strong>of</strong>essionals<br />
Ongo<strong>in</strong>g Annual,<br />
renewable<br />
NGO/non-pr<strong>of</strong>it 2003 Annual,<br />
renewable<br />
Services covered Geographical<br />
coverage<br />
Hospitalization All regions<br />
Hospitalization All regions<br />
5 years Primary care services All regions<br />
Procurement and distribution <strong>of</strong><br />
essential drugs for chonic diseases<br />
to PCCs<br />
Procurement and distribution <strong>of</strong><br />
vacc<strong>in</strong>es to PCCs<br />
All regions<br />
All regions<br />
Basic <strong>health</strong> and social services All regions<br />
Adm<strong>in</strong>istration <strong>of</strong> several national<br />
programmes<br />
Furbish<strong>in</strong>g primary <strong>health</strong><br />
consultations<br />
Provide normal delivery <strong>in</strong> addition<br />
to primary care services<br />
NA<br />
NA<br />
Akkar
Lebanon<br />
performance or mechanisms for monitor<strong>in</strong>g such performance. Nevertheless, the M<strong>in</strong>istry <strong>of</strong><br />
Public Health sees these contracts as serv<strong>in</strong>g the public good and as serv<strong>in</strong>g multi<strong>sector</strong>ality<br />
<strong>in</strong> <strong>health</strong> protection and encourag<strong>in</strong>g <strong>in</strong>clusion <strong>of</strong> various civil society partners.<br />
• Procurement <strong>of</strong> drugs for chronic diseases. <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public Health contracts out to the<br />
local branch <strong>of</strong> a large <strong>in</strong>ternational nongovernmental organization, the Young Men’s<br />
Christian Association (YMCA), for procurement <strong>of</strong> essential drugs for chronic diseases. <strong>The</strong><br />
YMCA purchases essential generic drugs for conditions such as diabetes, hypertension, and<br />
heart disease from <strong>in</strong>ternational markets at bulk rates which are much lower compared with<br />
rates for similar drugs <strong>in</strong> the Lebanese market. <strong>The</strong> YMCA stores and distributes these drugs<br />
us<strong>in</strong>g a network <strong>of</strong> around 400 <strong>health</strong> care outlets (<strong>health</strong> centres and dispensaries). <strong>The</strong>re are<br />
attempts to <strong>in</strong>terl<strong>in</strong>k these us<strong>in</strong>g a computerized system. Around 150 000 people are served<br />
through this network a year, at a cost <strong>of</strong> about US$ 15–20 a year. This <strong>of</strong>fers substantial<br />
sav<strong>in</strong>gs compared with costs <strong>of</strong> the private market. <strong>The</strong> total cost for the programme is about<br />
US$ 2.5 million a year. <strong>The</strong> YMCA is not allowed to turn anyone away for f<strong>in</strong>ancial reasons.<br />
<strong>The</strong> contract covers a small part <strong>of</strong> the overhead for the YMCA and dispens<strong>in</strong>g outlets.<br />
Chances for abuse <strong>in</strong> this system are low. Of note, YMCA procurement <strong>of</strong> essential drugs<br />
started dur<strong>in</strong>g the civil war with the aid <strong>of</strong> foreign donors who filled an important gap after<br />
the breakdown <strong>of</strong> the government-supported primary care and drug delivery <strong>in</strong>frastructure.<br />
After the end <strong>of</strong> the civil war, foreign donations <strong>of</strong> drugs stopped, so the M<strong>in</strong>istry <strong>of</strong> Public<br />
Health decided to cont<strong>in</strong>ue to sponsor this programme because <strong>of</strong> its efficiency and its ability<br />
to promote equitable access to essential drugs. This sponsorship will cont<strong>in</strong>ue for the<br />
foreseeable future.<br />
• Secur<strong>in</strong>g immunization material. <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public Health has a contract with UNICEF<br />
to procure vacc<strong>in</strong>es. UNICEF purchases immunization kits on behalf <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong><br />
Public Health <strong>in</strong> the <strong>in</strong>ternational market and then gives them to the M<strong>in</strong>istry <strong>of</strong> Public<br />
Health which distributes them to its PCC network. This programme has proved to be very<br />
efficient and a source <strong>of</strong> considerable sav<strong>in</strong>gs, as UNICEF is able to secure immunization<br />
material at much lower discounted rates than the M<strong>in</strong>istry <strong>of</strong> Public Health would be able to<br />
(UNICEF purchases vacc<strong>in</strong>es on behalf <strong>of</strong> many other low- and middle-<strong>in</strong>come countries).<br />
UNICEF perceives this programme as provid<strong>in</strong>g opportunities to promote preventive<br />
services.<br />
• Upgrad<strong>in</strong>g maternal care. <strong>The</strong> Project <strong>in</strong> Wadi Khaled is be<strong>in</strong>g implemented through a<br />
contract with Makassed Health System <strong>in</strong> an underserved area <strong>in</strong> north Lebanon which is<br />
part <strong>of</strong> the Akkar district. This area has low maternal <strong>health</strong> <strong>in</strong>dicators, <strong>in</strong>clud<strong>in</strong>g high use <strong>of</strong><br />
traditional birth attendants. <strong>The</strong> aim <strong>of</strong> the project is to encourage better antenatal care and<br />
<strong>of</strong>fer facilities for normal delivery while ensur<strong>in</strong>g that more complicated cases are referred to<br />
other hospitals us<strong>in</strong>g well established referral networks. A currently-operational primary care<br />
centre, with well-tra<strong>in</strong>ed staff, opened <strong>in</strong> May 2003. In additional to the usual set-up<br />
designed for primary care services, this centre also <strong>of</strong>fers specially-designed facilities for<br />
normal delivery. <strong>The</strong> centre is manned around the clock. For complex or high risk deliveries<br />
or when problems arise unexpectedly dur<strong>in</strong>g normal delivery, the centre has established<br />
protocols and procedures for evacuation patients to hospitals. Doctors are expected to deliver<br />
the usual primary care services other than antenatal care, <strong>in</strong>clud<strong>in</strong>g safe motherhood and
Lebanon<br />
postnatal care, vacc<strong>in</strong>ation and other reproductive <strong>health</strong> services, such as family plann<strong>in</strong>g<br />
and <strong>in</strong>fertility services. <strong>The</strong> centre receives a capitated fee per pregnant woman for antenatal<br />
visits and a capitated fee per delivery. This is the only contract that <strong>in</strong>volves monetary cash<br />
flow with a local nongovernmental organization <strong>in</strong> Lebanon. It is too early to assess this<br />
<strong>contractual</strong> project but several aspects <strong>in</strong>vite optimism that it represents a useful model for<br />
other M<strong>in</strong>istry <strong>of</strong> Public Health contracts: the clear terms <strong>of</strong> reference, <strong>in</strong>clud<strong>in</strong>g<br />
performance <strong>in</strong>dicators, adequate staff<strong>in</strong>g, tra<strong>in</strong><strong>in</strong>g <strong>of</strong> personnel, and the <strong>in</strong>terest with<strong>in</strong> the<br />
M<strong>in</strong>istry <strong>of</strong> Public Health <strong>in</strong> pilot and <strong>in</strong>novative projects <strong>of</strong> a limited scope than can be later<br />
expanded.<br />
• Contracts with <strong>in</strong>dividuals. <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public Health contracts on an as-needed basis<br />
with <strong>in</strong>dividuals to deliver certa<strong>in</strong> consultative or operational services. This is done<br />
especially <strong>in</strong> areas with <strong>in</strong>adequate staff<strong>in</strong>g, for example <strong>in</strong> reproductive <strong>health</strong>. <strong>The</strong>re is no<br />
dedicated reproductive <strong>health</strong> programme at the M<strong>in</strong>istry <strong>of</strong> Public Health, and therefore the<br />
M<strong>in</strong>istry contracts periodically with public <strong>health</strong> experts to provide programmatic-like<br />
services <strong>in</strong> this area. Contracts are typically awarded to known qualified people rather than<br />
based on an open process that <strong>in</strong>volves competitive applications. Payments are typically<br />
based on cash transfers upon meet<strong>in</strong>g the terms <strong>of</strong> reference for the contract. <strong>The</strong>re has not<br />
been an assessment <strong>of</strong> the quality <strong>of</strong> outcomes <strong>of</strong> these contracts, but the M<strong>in</strong>istry <strong>of</strong> Public<br />
Health sees such contracts as allow<strong>in</strong>g it to secure public <strong>health</strong> expertise, which is abundant<br />
<strong>in</strong> Lebanon, at reasonable costs without the need to enlarge its pr<strong>of</strong>essional body.<br />
• Contracts with <strong>in</strong>ternational organizations. <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public Health contracts with<br />
<strong>in</strong>ternational organizations operat<strong>in</strong>g <strong>in</strong> Lebanon to achieve certa<strong>in</strong> public <strong>health</strong> goals.<br />
Contract<strong>in</strong>g with UNICEF has already been discussed. <strong>The</strong> M<strong>in</strong>istry also contracts with the<br />
country <strong>of</strong>fice <strong>of</strong> WHO to support several programmes such as the national tobacco control,<br />
noncommunicable disease, and AIDS control programmes. Typically, the M<strong>in</strong>istry <strong>of</strong> Public<br />
Health provides the bulk <strong>of</strong> the f<strong>in</strong>ancial support for these programmes (around 70% if only<br />
cash support is considered but up to 90% if <strong>in</strong>direct costs are also considered) while WHO<br />
contributes the rest. WHO adm<strong>in</strong>isters these programmes under a special “trust fund.” <strong>The</strong><br />
M<strong>in</strong>istry <strong>of</strong> Public Health gets these funds back <strong>in</strong> the form <strong>of</strong> expenditures on programme<br />
activities. WHO charges 13% for adm<strong>in</strong>ister<strong>in</strong>g the funds.<br />
<strong>The</strong> collaborative programmes allow for local expertise to be secured as valued public<br />
<strong>health</strong> pr<strong>of</strong>essionals are paid at WHO scale, which is higher than the MOPH pay scale. Thus,<br />
Lebanon is able to both reta<strong>in</strong> these pr<strong>of</strong>essionals and benefit from their experience. Programme<br />
staff are recruited by the WHO Representative but are usually proposed by the M<strong>in</strong>istry <strong>of</strong><br />
Public Health. However, this is subject to political and other considerations, which limits the<br />
usefulness <strong>of</strong> the open process <strong>of</strong> application and appo<strong>in</strong>tment. However, most <strong>of</strong> the staff have<br />
been <strong>of</strong> high quality and have undergone adequate tra<strong>in</strong><strong>in</strong>g by WHO. <strong>The</strong>refore, these contracts<br />
have allowed for the build<strong>in</strong>g <strong>of</strong> strong human resource teams. Nevertheless, consider<strong>in</strong>g that<br />
Lebanon is a small market that has abundance <strong>of</strong> qualified <strong>health</strong> pr<strong>of</strong>essionals and that many<br />
such pr<strong>of</strong>essionals have already had a lot <strong>of</strong> tra<strong>in</strong><strong>in</strong>g <strong>in</strong> public <strong>health</strong> through the different<br />
programmes, the M<strong>in</strong>istry <strong>of</strong> Public Health can probably handle these programmes on its own<br />
with some help from WHO on an as-needed basis.<br />
160
Lebanon<br />
Overall, the contracts allow the concerned national programmes to receive WHO expertise<br />
on the basis <strong>of</strong> cooperation. In addition to the actual activities <strong>of</strong> programmes, several examples<br />
illustrate that the outcomes <strong>of</strong> cooperation with WHO may go beyond the programmes<br />
themselves. This is shown, for example, <strong>in</strong> the contribution <strong>of</strong> WHO to immunization campaign<br />
follow<strong>in</strong>g the detection <strong>of</strong> the polio case <strong>in</strong> Akkar <strong>in</strong> 2003 and tra<strong>in</strong><strong>in</strong>g <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Public<br />
Health personnel and pharmacists <strong>in</strong> different aspects related to rational dispens<strong>in</strong>g. While the<br />
contract<strong>in</strong>g <strong>arrangements</strong> with WHO have given important benefits, it is difficult to ascribe all<br />
<strong>of</strong> these fruits to the use <strong>of</strong> the contract as a tool. Rather, many <strong>of</strong> the activities are based on the<br />
voluntary participation <strong>of</strong> WHO as a concerned agency <strong>in</strong> Lebanon.<br />
<strong>The</strong>re are certa<strong>in</strong> limitations to the collaborative <strong>arrangements</strong> between the M<strong>in</strong>istry <strong>of</strong><br />
Public Health and WHO. <strong>The</strong> different national programmes commonly contract with other<br />
parties, e.g. consultants or other agencies, to carry out specific tasks on WHO consultancy pay<br />
scales. Additional overhead is paid to these third parties, <strong>in</strong>creas<strong>in</strong>g the overall overhead <strong>of</strong> the<br />
programmes. Furthermore, it is not clear that the different programmes have had the desired<br />
effects. This is seen with regard to the <strong>in</strong>terl<strong>in</strong>ked programmes <strong>of</strong> tobacco control as well as<br />
noncommunicable disease control, which have not been closely coord<strong>in</strong>ated and have not been<br />
able to effect the desired policy change. <strong>The</strong> AIDS control programme is the only collaborative<br />
programme that has a written and declared national strategy. None <strong>of</strong> the other programmes<br />
have clear strategy with <strong>in</strong>dicators, annual reports, performance assessment. Similarly, none <strong>of</strong><br />
the programmes have sub-strategies for the different components <strong>of</strong> the programme. For<br />
example, a primary <strong>health</strong> care strategy cannot be implemented without a sub-strategy on<br />
reproductive <strong>health</strong>, which does not currently exist.<br />
Other publicly-f<strong>in</strong>anced agencies<br />
Several public organizations (Table 1) cover a range <strong>of</strong> social services, e.g. <strong>health</strong> and<br />
education, which may or may not be ma<strong>in</strong>ta<strong>in</strong>ed beyond the age <strong>of</strong> retirement. <strong>The</strong>se<br />
organizations have <strong>health</strong> funds which use contracts to secure <strong>health</strong> care services for their<br />
beneficiaries. Covered <strong>health</strong> services typically <strong>in</strong>clude hospitalization, ambulatory care<br />
(physician- and non-physician provided), drugs, and various <strong>health</strong> enabl<strong>in</strong>g aids. <strong>The</strong> exact<br />
types <strong>of</strong> services, class <strong>of</strong> services, and amount <strong>of</strong> co-payment by beneficiaries do vary among<br />
the different funds. However, all funds have similar mechanisms for contract<strong>in</strong>g for<br />
hospitalization and ambulatory care; these will be discussed under “case studies”.<br />
It may be worthwhile here to make a brief <strong>in</strong>troduction to the largest two <strong>of</strong> these<br />
organizations, the National Social Security Fund (NSSF) and the Civil Servant Cooperative<br />
(CSC). <strong>The</strong> NSSF was set up <strong>in</strong> 1961 and covers employees <strong>of</strong> the formal <strong>sector</strong>, <strong>contractual</strong> and<br />
wage earners <strong>of</strong> the public <strong>sector</strong>, employees <strong>of</strong> autonomous public <strong>in</strong>stitutions and others (e.g.<br />
physicians, public school teachers) and family dependents. <strong>The</strong> number currently enrolled at<br />
NSSF is around 430 000 Lebanese, and the total number <strong>of</strong> beneficiaries (<strong>in</strong>clud<strong>in</strong>g dependent<br />
family members) is estimated to be around 1.3 million, or around a third <strong>of</strong> the Lebanese<br />
161
Lebanon<br />
population. <strong>The</strong> CSC was set up <strong>in</strong> 1970 and covers all civil servants and their dependents,<br />
number<strong>in</strong>g around 190 000.<br />
<strong>The</strong> NSSF and CSC share several characteristics. Adm<strong>in</strong>istratively, both ma<strong>in</strong>ta<strong>in</strong> relative<br />
adm<strong>in</strong>istrative autonomy and f<strong>in</strong>ancial <strong>in</strong>dependence and have <strong>in</strong>dependent advisory boards.<br />
Health spend<strong>in</strong>g at NSSF and CSC is different <strong>in</strong> scale (US$ 251.5 million versus 48.3 million)<br />
but similar <strong>in</strong> k<strong>in</strong>d (48.2% ambulatory care and 51.8% hospitalization). Health care costs borne<br />
by these organizations cont<strong>in</strong>ue to rise. For example, between 2000 and 2002, <strong>health</strong> spend<strong>in</strong>g at<br />
NSSF <strong>in</strong>creased by a whopp<strong>in</strong>g 65% but the relative contribution <strong>of</strong> outpatient versus <strong>in</strong>patient<br />
spend<strong>in</strong>g to the total bill rema<strong>in</strong>ed the same. It must be noted that prior to the civil war, there<br />
were ambitious plans to expand the coverage <strong>of</strong> NSSF to the whole Lebanese population but the<br />
outbreak <strong>of</strong> the civil war put an end to these plans. With this, Lebanon missed a historic<br />
opportunity to provider national <strong>health</strong> coverage.<br />
CASE STUDIES<br />
Contract<strong>in</strong>g for ambulatory and primary care services<br />
Contract<strong>in</strong>g primary care services for un<strong>in</strong>sured Lebanese<br />
Primary care services are provided by four ma<strong>in</strong> parties <strong>in</strong> Lebanon: <strong>health</strong> centres<br />
belong<strong>in</strong>g to the M<strong>in</strong>istry <strong>of</strong> Public Health (these are either operated by the M<strong>in</strong>istry or managed<br />
by other parties but contracted out by the M<strong>in</strong>istry); centres belong<strong>in</strong>g to other public <strong>in</strong>stitutions<br />
(such as the M<strong>in</strong>istry <strong>of</strong> Social Affairs (MOSA) and local municipalities); <strong>health</strong> centres<br />
belong<strong>in</strong>g to local or <strong>in</strong>ternational nongovernmental organizations operat<strong>in</strong>g <strong>in</strong> Lebanon; and<br />
private practitioners (whether hospital or community-based). Health care utilization surveys<br />
<strong>in</strong>dicate that private practitioners provide the largest bulk (over 75%) <strong>of</strong> ambulatory care services<br />
for the un<strong>in</strong>sured population <strong>in</strong> Lebanon. However, <strong>in</strong> this section, we will exam<strong>in</strong>e services that<br />
are partly or fully publicly funded, through either the M<strong>in</strong>istry <strong>of</strong> Public Health or the M<strong>in</strong>istry<br />
<strong>of</strong> Social Affairs, and where contract<strong>in</strong>g is implemented with a wide scope <strong>of</strong> nongovernmental<br />
organizations.<br />
a) M<strong>in</strong>istry <strong>of</strong> Public Health<br />
In response to fragmentation <strong>of</strong> primary care delivery for the un<strong>in</strong>sured, <strong>in</strong>adequacy <strong>of</strong><br />
geographical coverage, and absence <strong>of</strong> control measures and regulatory mechanisms, the<br />
M<strong>in</strong>istry <strong>of</strong> Public Health has developed a national strategy for primary <strong>health</strong> care and has<br />
attempted to implement it through engag<strong>in</strong>g and contract<strong>in</strong>g with public and nongovernmental<br />
organizations <strong>health</strong> centres. While the strategy document is not yet publicly available, the stated<br />
aim is to ensure the availability <strong>of</strong> primary care services to the population <strong>in</strong> all <strong>of</strong> Lebanon us<strong>in</strong>g<br />
a network <strong>of</strong> primary care centres. <strong>The</strong> network was launched <strong>in</strong> 1996 with around 30 centres.<br />
Expansion has been slow, and at present about 45 primary care centres are <strong>in</strong> the network. Three<br />
162
Lebanon<br />
belong to the M<strong>in</strong>istry <strong>of</strong> Social Affairs, 20 to the M<strong>in</strong>istry <strong>of</strong> Public Health and the rest belong<br />
to local or <strong>in</strong>ternational nongovernmental organizations. Another 50 primary care centres are<br />
about to jo<strong>in</strong> soon. <strong>The</strong> target is to <strong>in</strong>clude 150–160 centres by the end <strong>of</strong> 2005, which is<br />
expected to fill the primary care needs for the un<strong>in</strong>sured <strong>in</strong> all <strong>of</strong> Lebanon.<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public Health uses a standard contract with the primary care centre which<br />
describes responsibilities and expectations. Responsibilities <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Public Health<br />
<strong>in</strong>clude provision <strong>of</strong> essential drugs, <strong>health</strong> <strong>in</strong>formation system, and cont<strong>in</strong>u<strong>in</strong>g education and<br />
tra<strong>in</strong><strong>in</strong>g for staff <strong>of</strong> the centre. <strong>The</strong> responsibilities <strong>of</strong> the centre <strong>in</strong>clude commitment to provision<br />
<strong>of</strong> preventive and <strong>health</strong> promotion services, emphasis on essential drug list, use <strong>of</strong> <strong>health</strong><br />
<strong>in</strong>formation system, and adequate staff<strong>in</strong>g <strong>of</strong> the centre (<strong>in</strong> terms <strong>of</strong> physicians, non-physician<br />
<strong>health</strong> staff and adm<strong>in</strong>istration). <strong>The</strong> contract duration is 5 years, (with 6-months’ notice required<br />
for the centre to break the contract without <strong>in</strong>curr<strong>in</strong>g penalties). <strong>The</strong> contract is non-monetary,<br />
i.e. it does not <strong>in</strong>volve exchange <strong>of</strong> cash flow. Support<strong>in</strong>g this network, <strong>in</strong>clud<strong>in</strong>g underwrit<strong>in</strong>g<br />
the operations <strong>of</strong> its centres, accounts for about 2%–3% <strong>of</strong> M<strong>in</strong>istry <strong>of</strong> Public Health budget. For<br />
primary care centres owned by the M<strong>in</strong>istry <strong>of</strong> Public Health and operated by either<br />
nongovernmental organizations or local municipalities, the M<strong>in</strong>istry pays basic expenses<br />
(<strong>in</strong>clud<strong>in</strong>g water and electricity) while the centre is responsible for other operat<strong>in</strong>g expenses<br />
(such as telephone). Contract<strong>in</strong>g is not based on competitive bidd<strong>in</strong>g. <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public<br />
Health chooses primary care centres based on need <strong>in</strong> geographical areas, centre facilities, and<br />
anticipated success <strong>of</strong> contract<strong>in</strong>g based on engagement and quality <strong>of</strong> staff.<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public Health has recently contracted out an <strong>in</strong>dependent evaluation <strong>of</strong> the<br />
M<strong>in</strong>istry–nongovernmental organization <strong>contractual</strong> <strong>arrangements</strong>. Review <strong>of</strong> this evaluation is<br />
beyond the scope <strong>of</strong> this report, but the follow<strong>in</strong>g po<strong>in</strong>ts are relevant.<br />
• Centres belong<strong>in</strong>g to different parties, whether the M<strong>in</strong>istry <strong>of</strong> Public Health, M<strong>in</strong>istry <strong>of</strong><br />
Social Affairs, or nongovernmental organizations, have widely differ<strong>in</strong>g allegiances,<br />
agendas, capacities and resources. Contract<strong>in</strong>g with such diverse groups requires emphasis<br />
on the m<strong>in</strong>imum common denom<strong>in</strong>ator. This limits the usefulness <strong>of</strong> the contract<strong>in</strong>g<br />
mechanism as a means to <strong>in</strong>troduc<strong>in</strong>g drastic changes <strong>in</strong> the functions <strong>of</strong> the contracted<br />
parties.<br />
• <strong>The</strong> performance <strong>of</strong> primary care centres belong<strong>in</strong>g to nongovernmental organizations<br />
depends on the agendas, resources and commitments <strong>of</strong> nongovernmental organizations. For<br />
example, for some nongovernmental organizations with local political affiliations, primary<br />
care centres serve ma<strong>in</strong>ly as vote-maximizers and thus the emphasis has been on delivery <strong>of</strong><br />
services that impress the public.<br />
• <strong>The</strong> <strong>contractual</strong> <strong>arrangements</strong> are mostly about “organiz<strong>in</strong>g” the relationships between the<br />
two parties, s<strong>in</strong>ce many primary care centres are not under the <strong>in</strong>fluence <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong><br />
Public Health (hav<strong>in</strong>g long existed), and thus the M<strong>in</strong>istry <strong>of</strong> Public Health does not have<br />
great leverage over them. Nevertheless, the organiz<strong>in</strong>g aspect <strong>of</strong> the contract allows<br />
reasonable manoeuvr<strong>in</strong>g by the M<strong>in</strong>istry <strong>of</strong> Public Health to <strong>in</strong>troduce some change.<br />
Expectedly, this change has been slow.<br />
163
Lebanon<br />
• Quality control is difficult, as adherence to stated commitments is not easy to measure.<br />
Furthermore, there are no clear mechanisms, or adequate capacities, for follow-up<br />
assessment by the M<strong>in</strong>istry <strong>of</strong> Public Health s<strong>in</strong>ce it is not clear who will follow up on the<br />
different aspects <strong>of</strong> the performance <strong>of</strong> both parities.<br />
• Frequently, the key to effective execution <strong>of</strong> the <strong>contractual</strong> arrangement has been the<br />
presence <strong>of</strong> the right <strong>in</strong>dividuals/personalities at the primary care centre, reflect<strong>in</strong>g the<br />
<strong>in</strong>adequacy <strong>of</strong> long-term organizational or <strong>in</strong>stitutional structures.<br />
• <strong>The</strong>re is lack <strong>of</strong> coord<strong>in</strong>ation between the primary care network and other <strong>health</strong><br />
programmes. For example, there is need for greater coord<strong>in</strong>ation with the national tobacco<br />
control and AIDS control programmes.<br />
b) M<strong>in</strong>istry <strong>of</strong> Social Affairs<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Social Affairs provides primary care services through two types <strong>of</strong> centres:<br />
Development Services Centres (DSCs), <strong>of</strong> which there are currently 67, with an additional 76<br />
branches, and contracted nongovernmental organization centres (currently 148). <strong>The</strong> M<strong>in</strong>istry <strong>of</strong><br />
Social Affairs estimates that up to 450 000 Lebanese benefit from its <strong>health</strong> services, 70 000 <strong>of</strong><br />
which are served through contract<strong>in</strong>g with nongovernmental organizations.<br />
DSCs provide a range <strong>of</strong> basic social services <strong>in</strong>clud<strong>in</strong>g primary care services, e.g. general<br />
and preventive care, paediatrics, maternal and child <strong>health</strong>/reproductive <strong>health</strong>, and dental care<br />
(not provided <strong>in</strong> the M<strong>in</strong>istry <strong>of</strong> Public Health network), although not all centres provide the<br />
same range. Only 3 <strong>of</strong> these centres are <strong>in</strong> the M<strong>in</strong>istry <strong>of</strong> Public Health primary care centres<br />
network. <strong>The</strong> MOSA does not implement contract<strong>in</strong>g with its own DSCs (<strong>in</strong> contrast to the<br />
M<strong>in</strong>istry <strong>of</strong> Public Health approach, with its own primary care centres). Health services account<br />
for around 17% <strong>of</strong> the DSC budget. An additional 5% covers medical equipment and related<br />
material. As for nongovernmental organization centres contracted with the M<strong>in</strong>istry <strong>of</strong> Social<br />
Affairs, a standard contract (Appendix) has been <strong>in</strong> use s<strong>in</strong>ce 1996. <strong>The</strong> contract<strong>in</strong>g arrangement<br />
emphasizes flexibility and m<strong>in</strong>imization <strong>of</strong> bureaucratic burden, at the same time ensur<strong>in</strong>g<br />
mutual transparency. Similar to what is done by the M<strong>in</strong>istry <strong>of</strong> Public Health, there is<br />
del<strong>in</strong>eation <strong>of</strong> responsibilities (nongovernmental organization <strong>health</strong> centre provide similar<br />
services to DSCs) but the M<strong>in</strong>istry <strong>of</strong> Social Affairs has not had the capacity to develop and<br />
implement clear standards and procedures for its contracts with nongovernmental organizations.<br />
A plan is under development to better spell out the legal, f<strong>in</strong>ancial and operational aspects <strong>of</strong> the<br />
contracts emphasiz<strong>in</strong>g criteria and standards. Unlike the M<strong>in</strong>istry <strong>of</strong> Public Health, the M<strong>in</strong>istry<br />
<strong>of</strong> Social Affairs provides cash support for <strong>health</strong> services provided by nongovernmental<br />
organization centres (two-thirds <strong>of</strong> <strong>health</strong> services costs are borne by the M<strong>in</strong>istry <strong>of</strong> Social<br />
Affairs). Consequently, the operational framework is also different with the M<strong>in</strong>istry <strong>of</strong> Social<br />
Affairs hav<strong>in</strong>g a more direct <strong>in</strong>fluence on centre operations through the M<strong>in</strong>istry <strong>of</strong> Social<br />
Affairs–nongovernmental organization committees that oversee the work <strong>of</strong> centres (2 from<br />
each, headed by a M<strong>in</strong>istry <strong>of</strong> Social Affairs representative).<br />
164
Lebanon<br />
Perhaps the more obvious difference relates to the model <strong>of</strong> care emphasized by the<br />
M<strong>in</strong>istry <strong>of</strong> Social Affairs, which comes closer to the orig<strong>in</strong>al primary <strong>health</strong> care through<br />
emphasis on social <strong>health</strong> rather than on provision <strong>of</strong> a limited set <strong>of</strong> primary care services or<br />
essential drugs. Such a model presents a challenge for M<strong>in</strong>istry <strong>of</strong> Public Health network centres,<br />
many <strong>of</strong> which are not equipped to deal with what is needed to implement this model.<br />
Nongovernmental organization <strong>health</strong> centres also rarely implement this model, although the<br />
Islamic Health Council presents a bright exception.<br />
Contract<strong>in</strong>g ambulatory care services for publicly <strong>in</strong>sured Lebanese<br />
As previously noted, the majority (with the exception <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Public Health) <strong>of</strong><br />
public f<strong>in</strong>anc<strong>in</strong>g agencies cover their beneficiaries for a variety <strong>of</strong> ambulatory care services.<br />
<strong>The</strong>se <strong>in</strong>clude, for example, those provided by physicians, both generalists and specialists,<br />
physical therapists, midwives, radiology and laboratory centres, physical therapy centres, and<br />
hear<strong>in</strong>g aid centres. <strong>The</strong> contracted parties must apply to the f<strong>in</strong>anc<strong>in</strong>g agency with documents<br />
certify<strong>in</strong>g tra<strong>in</strong><strong>in</strong>g, qualifications and other aspects. Almost all licensed providers are accepted if<br />
they apply and meet eligibility criteria. In some cases, e.g. contracts with radiology and<br />
laboratory centres, field visits are carried out to ensure the accuracy <strong>of</strong> data presented <strong>in</strong> the<br />
application. Contracted parties sign a standard brief contract. <strong>The</strong>se contracts do not <strong>in</strong>volve<br />
direct cash transfers. Rather, the beneficiary, hav<strong>in</strong>g received and paid for the service out-<strong>of</strong>pocket,<br />
presents documentation <strong>of</strong> the service and is reimbursed by the contract<strong>in</strong>g agency<br />
accord<strong>in</strong>g to a pre-set fee schedule m<strong>in</strong>us the deductible.<br />
<strong>The</strong>re is dissatisfaction by all parties with this arrangement. Providers compla<strong>in</strong> <strong>of</strong> low<br />
fees. Beneficiaries compla<strong>in</strong> <strong>of</strong> hav<strong>in</strong>g to pay over fee schedules to obta<strong>in</strong> the services. <strong>The</strong><br />
f<strong>in</strong>anc<strong>in</strong>g agencies compla<strong>in</strong> <strong>of</strong> corruption <strong>in</strong>volv<strong>in</strong>g both consumers and providers and <strong>of</strong><br />
<strong>in</strong>ability to manage the tremendous responsibilities <strong>of</strong> oversight with a limited staff and large<br />
workload. Other limitations <strong>of</strong> current <strong>arrangements</strong> will be discussed later.<br />
4.2 Contract<strong>in</strong>g for hospitalization and related services<br />
Around 12%–12.5% <strong>of</strong> the Lebanese population gets hospitalized per year. Contract<strong>in</strong>g for<br />
hospitalization is described below accord<strong>in</strong>g to <strong>in</strong>surance coverage <strong>of</strong> citizens.<br />
<strong>The</strong> un<strong>in</strong>sured population<br />
Prior to the start <strong>of</strong> the civil war <strong>in</strong> 1972, the M<strong>in</strong>istry <strong>of</strong> Public Health had begun cover<strong>in</strong>g<br />
costs <strong>of</strong> hospitalization for the <strong>in</strong>digent, which consumed no more than <strong>of</strong> 10% <strong>of</strong> its budget.<br />
Eligibility was extended to <strong>in</strong>clude the un<strong>in</strong>sured as a result <strong>of</strong> consumer and political pressure<br />
(but not legislature) start<strong>in</strong>g <strong>in</strong> 1982. After the civil war ended <strong>in</strong> 1991, this coverage was<br />
conceived to be a temporary measure while plans for national <strong>health</strong> <strong>in</strong>surance coverage, which<br />
were <strong>in</strong> draft stage before the war erupted, were developed. Unfortunately, the latter goal proved<br />
difficult to accomplish. With the escalat<strong>in</strong>g cost <strong>of</strong> hospitalization, this issue has been at the<br />
165
Lebanon<br />
forefront <strong>of</strong> discussions <strong>of</strong> <strong>health</strong> <strong>sector</strong> reform. At present, hospitalization accounts for over<br />
80% <strong>of</strong> the budget <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Public Health.<br />
While 50% <strong>of</strong> the Lebanese population is eligible for M<strong>in</strong>istry <strong>of</strong> Public Health coverage<br />
for hospitalization, it is not known what portion takes advantage <strong>of</strong> this coverage. This is<br />
reflected <strong>in</strong> the number <strong>of</strong> covered hospitalizations: the M<strong>in</strong>istry <strong>of</strong> Public Health currently<br />
covers around 135 000–140 000 per year, while the expected number would be 240 000–<br />
250 000. This may reflect social stigma associated with use <strong>of</strong> M<strong>in</strong>istry <strong>of</strong> Public Health<br />
coverage and the perceived difficulties <strong>in</strong> the application process for eligibility.<br />
Because <strong>of</strong> the <strong>in</strong>adequacy and short supply <strong>of</strong> public hospitals, hospitalization for citizens<br />
covered by the M<strong>in</strong>istry <strong>of</strong> Public Health has been provided mostly by private hospitals. <strong>The</strong><br />
M<strong>in</strong>istry has historically encountered many difficulties <strong>in</strong> deal<strong>in</strong>g with private hospitals. Some <strong>of</strong><br />
these difficulties <strong>in</strong>clude <strong>in</strong>appropriate or false admissions, un-<strong>in</strong>dicated procedures,<br />
overutilization <strong>of</strong> services, spend<strong>in</strong>g over allocations, spend<strong>in</strong>g allocations early <strong>in</strong> the month<br />
and lack <strong>of</strong> protection <strong>of</strong> assigned allocations for emergency room visits throughout the month.<br />
All <strong>of</strong> these problems reflect the opportunity for the contract to be used as a tool for regulat<strong>in</strong>g<br />
the M<strong>in</strong>istry <strong>of</strong> Public Health–hospital relationship, while at the same time improv<strong>in</strong>g<br />
performance and conta<strong>in</strong><strong>in</strong>g costs.<br />
In the 1990s, the M<strong>in</strong>istry <strong>of</strong> Public Health contracted with most <strong>of</strong> the licensed private<br />
hospitals that had applied for a contract. In 2000, the M<strong>in</strong>istry <strong>of</strong> Public Health began an<br />
accreditation programme for hospitals with the purpose <strong>of</strong> ensur<strong>in</strong>g quality <strong>of</strong> services provided<br />
to patients covered by the M<strong>in</strong>istry. In 2001, 46 were accredited, but an additional 30 were added<br />
due to political pressure or lack <strong>of</strong> accredited hospitals <strong>in</strong> certa<strong>in</strong> areas, so the total number<br />
reached 76. In 2003, the total number <strong>in</strong>creased to 103, as more hospitals sought to meet<br />
accreditation standards. <strong>The</strong>se 103 hospitals provide around 2000 beds <strong>in</strong> total.<br />
In contract<strong>in</strong>g with hospitals and <strong>health</strong> care facilities, the M<strong>in</strong>istry <strong>of</strong> Public Health<br />
currently uses two types <strong>of</strong> contracts. Group 1 contracts are <strong>in</strong>tended for acute care. <strong>The</strong> 103<br />
accredited hospitals are currently <strong>in</strong>cluded. More details about these contracts are provided<br />
below. Group 2 contracts are <strong>in</strong>tended for long-term care facilities (such as those that provide<br />
rehabilitation and care for the aged and for patients with long-term debilitat<strong>in</strong>g conditions such<br />
as Alzheimer’s). <strong>The</strong>re are around 50 hospitals and facilities (with a total <strong>of</strong> 4500 beds) <strong>in</strong> this<br />
group. <strong>The</strong> total expenditures/MOPH allocations for these facilities amount to 30 billion<br />
Lebanese pounds (BLP) per year. Payment to these Group 2 facilities is based on flat rates set<br />
accord<strong>in</strong>g to condition. Deal<strong>in</strong>g with these hospitals is generally much simpler than the acute<br />
care hospitals and, therefore, transfer <strong>of</strong> payment (which is usually smaller than that made to<br />
acute care hospitals) is usually done more speedily.<br />
For Group 1 contracts, the M<strong>in</strong>istry <strong>of</strong> Public Health uses a standard contract that has<br />
replaced the contracts used prior to 1997 (improvements have been <strong>in</strong>troduced yearly). <strong>The</strong><br />
contract has been a powerful tool for the M<strong>in</strong>istry <strong>of</strong> Public Health to regulate spend<strong>in</strong>g and<br />
166
Lebanon<br />
quality <strong>of</strong> care <strong>in</strong> the contracted hospitals. <strong>The</strong> ma<strong>in</strong> features <strong>of</strong> the current contract areas as<br />
follows.<br />
Contracts are generally awarded to hospitals that meet accreditation standards.<br />
Allocations are assigned based on M<strong>in</strong>istry <strong>of</strong> Public Health calculations that take <strong>in</strong>to account<br />
number <strong>of</strong> beds, expected MOPH patient volume, location, hospital services, etc.<br />
<strong>The</strong> supervis<strong>in</strong>g physician has a greater <strong>role</strong> <strong>in</strong> ensur<strong>in</strong>g appropriateness <strong>of</strong> care and transparency<br />
<strong>of</strong> bill<strong>in</strong>g.<br />
More detailed specification <strong>of</strong> the responsibilities <strong>of</strong> the contracted hospitals<br />
Penalties are stipulated if contracted hospitals do not adhere to the terms <strong>of</strong> the contract.<br />
Payment to the contracted hospital is distributed over the whole month.<br />
A certa<strong>in</strong> percentage <strong>of</strong> the payment is secured for emergency room visits.<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public Health perceives that implement<strong>in</strong>g <strong>of</strong> contracts has already had an<br />
impact. In previous years, expenditures <strong>of</strong> contracted hospitals exceeded assigned allocations by<br />
around 50%. This has come down to 5% recently. Furthermore, data collected as part <strong>of</strong> the<br />
contract have allowed the supervis<strong>in</strong>g physicians to put together a monthly report about services<br />
and expenditures for M<strong>in</strong>istry <strong>of</strong> Public Health patients. This has empowered the M<strong>in</strong>istry <strong>of</strong><br />
Public Health by provid<strong>in</strong>g a stronger evidence base for its policies.<br />
Among the 103 hospitals are 10 public hospitals (which have become autonomous after<br />
Lebanese Law 544/96). Another 10 hospitals provide hospitalization services to M<strong>in</strong>istry <strong>of</strong><br />
Public Health patients but are not formally covered by contract for political and other reasons.<br />
For example, Tyre Governmental Hospital, which is located <strong>in</strong> al-Rashidiyya refugee camp,<br />
cannot afford to impose co-payments on its users as this may lead to social and political<br />
<strong>in</strong>stability.<br />
In terms <strong>of</strong> payments, the M<strong>in</strong>istry <strong>of</strong> Public Health reimburses private and public hospitals<br />
85% and 95% <strong>of</strong> the bill, respectively. <strong>The</strong> rema<strong>in</strong><strong>in</strong>g balance represents co-payments by<br />
beneficiaries. Payment is based on cash transfer upon approval <strong>of</strong> the bill. <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public<br />
Health commonly reduces submitted bills by up to 25% because <strong>of</strong> the known <strong>in</strong>flation <strong>of</strong> actual<br />
costs.<br />
Us<strong>in</strong>g the contract as a tool, the M<strong>in</strong>istry <strong>of</strong> Public Health <strong>in</strong>troduced the concept <strong>of</strong> the flat<br />
rate for a variety <strong>of</strong> surgical procedures <strong>in</strong> 2001. This has further reduced costs, although there<br />
are no data currently on the f<strong>in</strong>ancial impact <strong>of</strong> this change. <strong>The</strong>re are plans to <strong>in</strong>troduce flat rates<br />
<strong>in</strong> 2004 for medical treatments and procedures. Revenues from the M<strong>in</strong>istry <strong>of</strong> Public Health are<br />
important for many hospitals, especially the smaller ones and those <strong>in</strong> certa<strong>in</strong> urban and rural<br />
areas where the un<strong>in</strong>sured dom<strong>in</strong>ate.<br />
While there are <strong>in</strong>dications that the M<strong>in</strong>istry <strong>of</strong> Public Health is gradually and more<br />
effectively us<strong>in</strong>g the contract as a regulatory tool, many problems rema<strong>in</strong> with the current<br />
<strong>arrangements</strong>. <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public Health still has little leverage over hospitals; it has limited<br />
167
Lebanon<br />
supervision <strong>of</strong> quality <strong>of</strong> care, and no way <strong>of</strong> enforc<strong>in</strong>g certa<strong>in</strong> standards or to l<strong>in</strong>k<br />
hospitalization with preventive services. <strong>The</strong>re is also bilateral distrust; the M<strong>in</strong>istry <strong>of</strong> Public<br />
Health worries about abuse, while private hospitals see undue f<strong>in</strong>ancial and regulatory pressures<br />
by the M<strong>in</strong>istry at a time <strong>of</strong> fiscal difficulty. With the lack <strong>of</strong> sufficient political support for better<br />
use <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> to change the public <strong>health</strong> agenda, many see current<br />
<strong>arrangements</strong> for hospitalization as facilitat<strong>in</strong>g public–private cash transfers that do not serve the<br />
public <strong>in</strong> the long term.<br />
<strong>The</strong> publicly <strong>in</strong>sured population<br />
Contractual <strong>arrangements</strong> for hospitalization are remarkably similar across the different<br />
f<strong>in</strong>anc<strong>in</strong>g agencies, such as NSSF, CSC and others. <strong>The</strong>se agencies contract with most private<br />
hospitals licensed by the M<strong>in</strong>istry <strong>of</strong> Public Health (they do not use the M<strong>in</strong>istry’s accreditation<br />
system). Interested hospitals apply to the concerned agency to provide services for beneficiaries.<br />
Most <strong>of</strong> these hospitals are private, as public hospitals account for less than 5%. Site visits are<br />
carried out to ensure eligibility. Hospitals sign standard contracts which stipulate responsibilities<br />
<strong>of</strong> each party. F<strong>in</strong>anc<strong>in</strong>g agencies have rotat<strong>in</strong>g or stationary supervis<strong>in</strong>g physicians who approve<br />
<strong>in</strong>dication for admission, assess appropriateness <strong>of</strong> care, and review bills either on-site (done by<br />
the same supervis<strong>in</strong>g physician) or at central <strong>of</strong>fices (done by different physicians). Some<br />
agencies, like NSSF, use advisory committees to review applications for coverage <strong>of</strong> expensive<br />
cases. Medical admissions are reimbursed on a fee-for-service basis. Different agencies have<br />
different pay scales but all commonly use flat rates for many (but not all) surgical procedures and<br />
fee-for-service for medical hospitalization.<br />
<strong>The</strong> case <strong>of</strong> <strong>in</strong>vasive <strong>in</strong>terventions for coronary heart disease<br />
Lebanon has undergone an epidemiological transition, and chronic diseases, especially<br />
cardiovascular diseases, account for an important portion <strong>of</strong> mortality, morbidity and <strong>health</strong> care<br />
expenditure. Coronary heart disease consumes considerable resources. Invasive <strong>in</strong>terventions for<br />
coronary heart disease, <strong>in</strong>clud<strong>in</strong>g coronary artery bypass surgery (CABG) and percutaneous<br />
<strong>in</strong>terventions (PCI) such as balloon angioplasty and stent implantation, account for a<br />
considerable portion <strong>of</strong> the costs related to coronary heart disease. Nevertheless, coronary heart<br />
disease is a medical, not surgical, disease and much can be accomplish to reduce related<br />
mortality, morbidity and <strong>health</strong> care costs through well-proven and cost-effective secondary<br />
prevention approaches. <strong>The</strong>se approaches <strong>in</strong>clude medical therapies, such as aspir<strong>in</strong>, blood<br />
pressure and cholesterol lower<strong>in</strong>g agents, and behavioural and lifestyle modification, such as<br />
smok<strong>in</strong>g cessation and physical activity. Secondary prevention approaches are, however, grossly<br />
underutilized <strong>in</strong> patients with coronary heart disease. This is especially strik<strong>in</strong>g consider<strong>in</strong>g the<br />
well-described overuse <strong>of</strong> <strong>in</strong>vasive <strong>in</strong>terventions. Furthermore, lack <strong>of</strong> adequate emphasis on<br />
secondary prevention leads to more costly <strong>in</strong>vasive <strong>in</strong>terventions <strong>in</strong> people with established<br />
coronary heart disease. In addition to high costs and missed opportunities to improve <strong>health</strong><br />
outcomes, overuse <strong>of</strong> <strong>in</strong>vasive <strong>in</strong>terventions exposes potential conflict <strong>of</strong> <strong>in</strong>terest <strong>in</strong> which the<br />
<strong>health</strong> care facilities and physicians may be entangled to secure more lucrative benefits.<br />
168
Lebanon<br />
Correct<strong>in</strong>g this imbalance by emphasiz<strong>in</strong>g secondary prevention should be a ma<strong>in</strong> focus <strong>of</strong><br />
public <strong>health</strong> action to control coronary heart disease.<br />
In Lebanon there is a gross oversupply <strong>of</strong> high-tech facilities for perform<strong>in</strong>g <strong>in</strong>vasive<br />
<strong>in</strong>terventions for coronary heart disease, and oversupply <strong>of</strong> super-specialists to perform them. As<br />
a result, Lebanon has much higher than expected rates <strong>of</strong> CABG and PCI for coronary heart<br />
disease.<br />
• <strong>The</strong>re are 35 centres for PCI and 22 centres for CABG. For CABG, this oversupply (1 per<br />
180 000 population) contrasts with the availability <strong>of</strong> similar facilities <strong>in</strong> an <strong>in</strong>dustrialized<br />
country such as France, where there is currently 1 CABG centre for each 700 000 population.<br />
More recently, there is a move to consolidate centres <strong>in</strong> France to the ratio <strong>of</strong> 1 per 2 million<br />
people. <strong>The</strong>se large centres reduce costs and <strong>of</strong>fer great opportunities for research and<br />
development. <strong>The</strong> situation <strong>in</strong> Lebanon is not expected to change, even after the<br />
implementation <strong>of</strong> the <strong>health</strong> map, due to the dom<strong>in</strong>ant effect <strong>of</strong> current oversupply.<br />
• In Lebanon, 4000–4500 CABGs are carried out per year at a cost <strong>of</strong> around US$ 5500 per<br />
procedure for the M<strong>in</strong>istry <strong>of</strong> Public Health, and up to US$ 10 000 for other f<strong>in</strong>anc<strong>in</strong>g<br />
agencies. <strong>The</strong> Lebanese rate <strong>of</strong> CABG (1/900) exceeds that <strong>of</strong> France (1/1000). This is<br />
surpris<strong>in</strong>g because France has a population that is considerably more aged than Lebanon, and<br />
thus Lebanon would be expected to require CABG far less <strong>of</strong>ten (1/1300–1/1500).<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public Health and other f<strong>in</strong>anc<strong>in</strong>g parties can use the contract with<br />
hospitals to encourage utilization <strong>of</strong> secondary prevention services to achieve several goals:<br />
improve outcomes, improve quality <strong>of</strong> care, reduce costs, and l<strong>in</strong>k <strong>in</strong>patient with outpatient care.<br />
<strong>The</strong>re are several steps that can be taken.<br />
• An additional amount per patient can be appended to the hospital bill per CABG to ensure<br />
follow-up <strong>of</strong> key risk factors such as cholesterol, blood pressure and smok<strong>in</strong>g practices on<br />
regular <strong>in</strong>tervals dur<strong>in</strong>g the first year (the most risky period) after hospitalization. Such<br />
services can be added at bare cost price and would prove to be very cost-effective for<br />
improv<strong>in</strong>g outcomes. This is especially important for citizens covered by the M<strong>in</strong>istry <strong>of</strong><br />
Public Health who lack <strong>in</strong>surance for ambulatory care. Alternative mechanisms for l<strong>in</strong>k<strong>in</strong>g<br />
hospitalization with care provided at primary care centres also need to be explored.<br />
• <strong>The</strong> current oversupply <strong>of</strong> centres which <strong>of</strong>fer CABG must be consolidated. For example, a<br />
m<strong>in</strong>imum number <strong>of</strong> CABGs per centre per year must be demonstrated before a hospital is<br />
contracted for CABG services.<br />
• Compliance <strong>in</strong> provision <strong>of</strong> secondary prevention care before the patient leaves the hospital<br />
and after hospitalization needs to be demonstrated.<br />
• <strong>The</strong> ability <strong>of</strong> the supervis<strong>in</strong>g physicians to ensure proper utilization must be improved.<br />
169
DISCUSSION<br />
Lebanon<br />
This Report has reviewed the contract<strong>in</strong>g <strong>arrangements</strong> <strong>in</strong> <strong>health</strong> engaged by the different<br />
public organizations <strong>in</strong> Lebanon. Contract<strong>in</strong>g for <strong>health</strong> services, both hospitalization and<br />
ambulatory care, dom<strong>in</strong>ates public–private contract<strong>in</strong>g <strong>in</strong> the <strong>health</strong> <strong>sector</strong> and serves over 80%<br />
<strong>of</strong> the Lebanese population. Hospitalization gets the lion share <strong>of</strong> contract<strong>in</strong>g.<br />
<strong>The</strong>re are several features and limitations which are common to all contract<strong>in</strong>g<br />
<strong>arrangements</strong> for <strong>health</strong> services: each agency carries out its own contract<strong>in</strong>g, but the nature <strong>of</strong><br />
contracts is remarkably similar across agencies; agencies contract with a large number <strong>of</strong><br />
providers, well beyond the needs <strong>of</strong> the contract<strong>in</strong>g agencies, thus limit<strong>in</strong>g the possibility <strong>of</strong><br />
effective oversight and monitor<strong>in</strong>g; there are political <strong>in</strong>fluences on the contract<strong>in</strong>g process; the<br />
private <strong>sector</strong> has more manoeuvr<strong>in</strong>g power with<strong>in</strong> current <strong>contractual</strong> <strong>arrangements</strong> than the<br />
public agency; contracts have no emphasis on performance or outcomes; contracts are not<br />
designed, and thus are unable, to limit the escalation <strong>of</strong> <strong>health</strong> care costs.<br />
We have already discussed the strengths and weaknesses <strong>of</strong> the different contract<strong>in</strong>g<br />
<strong>arrangements</strong> <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Public Health. As for publicly funded <strong>in</strong>surance schemes, it may<br />
be <strong>in</strong>structive to discuss limitations common to <strong>contractual</strong> <strong>arrangements</strong> for both ambulatory<br />
care and hospitalization. <strong>The</strong>se <strong>arrangements</strong> reflect a historical development whose time is past,<br />
as is well recognized by the f<strong>in</strong>anc<strong>in</strong>g agencies themselves. <strong>The</strong>re are many limitations <strong>in</strong> the<br />
current situation. Contracts are neither strong nor clear <strong>in</strong> terms <strong>of</strong> quality <strong>of</strong> care or liabilities.<br />
Contract<strong>in</strong>g with a very large number <strong>of</strong> service providers <strong>of</strong>fers beneficiaries choice, although<br />
not necessarily quality service. <strong>The</strong> f<strong>in</strong>anc<strong>in</strong>g agencies have little leverage over the contracted<br />
parties. Different agencies have common <strong>in</strong>terests, contract with the same providers, and use the<br />
same contract<strong>in</strong>g mechanisms. However, agencies do not seem capable or will<strong>in</strong>g to comb<strong>in</strong>e<br />
efforts to improve their barga<strong>in</strong><strong>in</strong>g positions or improve the contract<strong>in</strong>g mechanisms. For<br />
example, with regard to hospitalization, several simple measures are likely to make an impact:<br />
unification <strong>of</strong> pay schedules across the different f<strong>in</strong>anc<strong>in</strong>g agencies; <strong>in</strong>troduction <strong>of</strong> flat rates for<br />
all hospitalizations, medical and surgical, or preferred providers judged on both quality and<br />
costs, or selection <strong>of</strong> sites for certa<strong>in</strong> types <strong>of</strong> hospitalizations. Attempts are under way to unify<br />
pay schedules (especially for surgical procedures), but this has proved difficult for various<br />
political reasons. With regard to ambulatory care, changes that are seen as most urgent <strong>in</strong>clude:<br />
list<strong>in</strong>g preferred providers; gate-keep<strong>in</strong>g through primary care physicians; <strong>in</strong>troduc<strong>in</strong>g methods<br />
<strong>of</strong> risk shar<strong>in</strong>g by providers; <strong>in</strong>stitut<strong>in</strong>g <strong>health</strong> <strong>in</strong>formation systems; and document<strong>in</strong>g <strong>health</strong> care<br />
outcomes. As with the M<strong>in</strong>istry <strong>of</strong> Public Health scheme, many worry about the public–private<br />
cash transfers that current <strong>arrangements</strong> provide without the anticipated returns for citizens.<br />
<strong>The</strong> current fragmentation <strong>of</strong> <strong>health</strong> care f<strong>in</strong>anc<strong>in</strong>g <strong>in</strong> Lebanon is a recognized obstacle.<br />
However, contract<strong>in</strong>g need not be so fragmented. All public agencies contract with the same<br />
providers us<strong>in</strong>g the same <strong>arrangements</strong>. Unification <strong>of</strong> contract<strong>in</strong>g, for example through the<br />
creation <strong>of</strong> a central contract<strong>in</strong>g body which contracts with providers on behalf <strong>of</strong> the different<br />
agencies, can m<strong>in</strong>imize costs and improve effectiveness and barga<strong>in</strong><strong>in</strong>g power. Additionally this<br />
170
Lebanon<br />
could be a first step towards end<strong>in</strong>g the fragmentation <strong>of</strong> <strong>health</strong> f<strong>in</strong>anc<strong>in</strong>g. This step will entail<br />
some challenge <strong>in</strong> terms <strong>of</strong> consolidation <strong>of</strong> adm<strong>in</strong>istrative structures <strong>of</strong> different agencies, but<br />
would be well worth the effort.<br />
Identified problems with current <strong>contractual</strong> <strong>arrangements</strong>, whether they concern the<br />
M<strong>in</strong>istry <strong>of</strong> Public Health or other public f<strong>in</strong>anc<strong>in</strong>g agencies, mostly reflect two key factors.<br />
• Lack <strong>of</strong> political support. A wide range <strong>of</strong> reforms are urgently needed <strong>in</strong> the <strong>health</strong> <strong>sector</strong>.<br />
<strong>The</strong>se <strong>in</strong>clude, most urgently, end<strong>in</strong>g the current fragmentation <strong>of</strong> <strong>health</strong> care f<strong>in</strong>anc<strong>in</strong>g. Use<br />
<strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> as a tool for reform requires political support as contracted<br />
parties, whether hospitals or physicians or other providers, have large powers and can exert<br />
them very effectively over the public <strong>sector</strong>. This is compounded by their dom<strong>in</strong>ance <strong>of</strong><br />
<strong>health</strong> service delivery. <strong>The</strong> difficult economic conditions <strong>of</strong> over-supplied provider groups<br />
<strong>in</strong> the midst <strong>of</strong> ongo<strong>in</strong>g economic difficulties <strong>in</strong> Lebanon further complicates the situation.<br />
Nevertheless, visionary public <strong>health</strong> policies and stewardship and more pressures from<br />
beneficiaries can br<strong>in</strong>g on pr<strong>of</strong>ound changes.<br />
• Lack <strong>of</strong> adequate capacities. It is commonly <strong>in</strong>dicated that current capacities <strong>in</strong> the different<br />
public <strong>health</strong> agencies are not adequate to oversee and monitor a different scope <strong>of</strong><br />
contract<strong>in</strong>g <strong>arrangements</strong> that emphasize quality <strong>of</strong> care and which are outcome based. For<br />
example, most agencies do not have the needed number <strong>of</strong> highly qualified supervisory<br />
physicians. A different and new set-up is needed for <strong>contractual</strong> <strong>arrangements</strong> with different<br />
focus. This <strong>in</strong>cludes a <strong>health</strong> <strong>in</strong>formatics system, <strong>in</strong>terl<strong>in</strong>ked f<strong>in</strong>anc<strong>in</strong>g agencies and<br />
providers and enhanced transfers <strong>of</strong> data and payment.<br />
CONTRACTUAL ARRANGEMENTS: A SCORECARD<br />
Table 5 summarizes strengths and weaknesses <strong>of</strong> contract<strong>in</strong>g <strong>arrangements</strong> accord<strong>in</strong>g to<br />
f<strong>in</strong>anc<strong>in</strong>g agency. It might be also useful here to provide a general overview <strong>of</strong> what contract<strong>in</strong>g<br />
<strong>arrangements</strong> can and cannot do. Contractual <strong>arrangements</strong> provide important contributions to<br />
the performance <strong>of</strong> the <strong>health</strong> care system <strong>in</strong> Lebanon. <strong>The</strong>se <strong>arrangements</strong>:<br />
Provide the legal and organizational framework for public–private <strong>in</strong>teractions to provide <strong>health</strong><br />
care and <strong>health</strong>-related services to large segments <strong>of</strong> the Lebanese population (both the<br />
<strong>in</strong>sured and un<strong>in</strong>sured).<br />
Cover un<strong>in</strong>sured portions <strong>of</strong> the Lebanese population, thereby contribut<strong>in</strong>g to improv<strong>in</strong>g equity.<br />
This is especially important with regards to coverage <strong>of</strong> hospitalization and acute care<br />
services. Coverage <strong>of</strong> primary care services is gradually improv<strong>in</strong>g.<br />
Support selected nongovernmental organizations which provide basic social services beyond <strong>health</strong><br />
care.<br />
Improve the capacity <strong>of</strong> the Government <strong>of</strong> Lebanon to monitor performance <strong>of</strong> contracted <strong>health</strong><br />
care <strong>in</strong>stitutions.<br />
Can lead to upgrad<strong>in</strong>g standards and performance <strong>of</strong> contracted parties.<br />
171
Table 5. Scorecard <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> Lebanon<br />
Lebanon<br />
Contractual arrangement What the arrangement achieves Challenges to meet<br />
MOPH<br />
1) Primary care (primary<br />
care centres)<br />
2) Hospitalization (private<br />
and public hospitals)<br />
3) Social welfare<br />
(nongovernmental<br />
organizations)<br />
• Provide primary care services to un<strong>in</strong>sured Lebanese<br />
• When network is complete, it would cover all geographic areas<br />
• Provide nongovernmental organizations with needed support (e.g.<br />
essential drugs and vacc<strong>in</strong>es) and help them improve performance<br />
• Provide hospitalization services to un<strong>in</strong>sured Lebanese, promot<strong>in</strong>g<br />
equity<br />
• Cover all geographical areas<br />
• Beneficiary chooses provider<br />
• Accreditation system helps select the better hospitals<br />
• Flat rates for many surgical procedures decrease costs<br />
• Supervis<strong>in</strong>g physicians ensure <strong>in</strong>dications, appropriates <strong>of</strong> care, and<br />
appropriate bill<strong>in</strong>g<br />
• Support work <strong>of</strong> nongovernmental organizations on heath and <strong>health</strong><br />
determ<strong>in</strong>ants<br />
• Promote equity<br />
4) Chronic drugs (YMCA) • Procure, store and distribute essential drugs for chronic conditions<br />
• Decrease cost <strong>of</strong> care<br />
• Improve access and thus promote equity<br />
5) Immunization<br />
(UNICEF)<br />
• Secure immunization material<br />
• Decrease costs<br />
• Improve access and thus promote equity<br />
• Monitor and ensure quality<br />
• Assess impact<br />
• Impact the different agendas <strong>of</strong> primary care centre<br />
• Implement a true primary <strong>health</strong> care model (i.e.<br />
beyond primary care)<br />
• Prevent abuse<br />
• Monitor and ensure quality<br />
• Assess impact<br />
• Control escalat<strong>in</strong>g costs<br />
• Apply flat fees to all hospitalizations (surgical and<br />
medical)<br />
• Resist political pressures for <strong>in</strong>clusion <strong>of</strong> more<br />
hospitals<br />
• Hospitals have tremendous leverage<br />
• Monitor performance<br />
• Assess impact<br />
• Monitor and ensure quality <strong>of</strong> prescrib<strong>in</strong>g<br />
• L<strong>in</strong>k to proper management <strong>of</strong> chronic conditions (e.g.<br />
algorithms)<br />
• Develop alternative mechanisms <strong>in</strong> case NGO<br />
withdraws<br />
• F<strong>in</strong>d alternative sources if UNICEF withdraws
Lebanon<br />
Table 5. Scorecard <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> Lebanon (cont.)<br />
Contractual arrangement What the arrangement achieves Challenges to meet<br />
6) Maternal services<br />
(Makassed)<br />
7) Primary <strong>health</strong> expertise<br />
(consultants)<br />
8) Programme<br />
management (WHO)<br />
Other public organizations<br />
1) Ambulatory care<br />
(mostly private providers)<br />
2) Hospitalization (Mostly<br />
private hospitals)<br />
• Provide community access to facilities for normal delivery<br />
• L<strong>in</strong>k primary and maternal care<br />
• L<strong>in</strong>k community maternal care and referral services<br />
• Secure public <strong>health</strong> expertise <strong>in</strong> needed areas<br />
• Avoid add<strong>in</strong>g more regular staff<br />
• Ensures proper management <strong>of</strong> important programmes<br />
• Secures WHO expertise and <strong>in</strong>timate <strong>in</strong>volvement<br />
• Reta<strong>in</strong>s primary <strong>health</strong> pr<strong>of</strong>essionals (on WHO pay scale)<br />
• Provide ambulatory care for beneficiary<br />
• Cover all geographical areas<br />
• Beneficiary chooses provider<br />
• Provide hospitalization services to beneficiaries<br />
• Cover all geographical areas<br />
• Beneficiary chooses provider<br />
• Flat rates for many surgical procedures decrease costs<br />
• Supervis<strong>in</strong>g physicians ensure <strong>in</strong>dications, appropriates <strong>of</strong><br />
care, and appropriate bill<strong>in</strong>g<br />
173<br />
• Too early to assess performance and impact<br />
• Ensure quality <strong>of</strong> contributions<br />
• WHO overhead plus additional overhead when consultants are<br />
recruited<br />
• MOPH can <strong>in</strong>dependently manage programmes with support <strong>of</strong><br />
WHO<br />
• Assess impact <strong>of</strong> programmes<br />
• L<strong>in</strong>k programmes with other MOPH activities (e.g. primary<br />
care and hospitalizations)<br />
• Implement primary care model (<strong>in</strong>clud<strong>in</strong>g gate-keep<strong>in</strong>g)<br />
• Prevent abuse<br />
• Monitor and ensure quality<br />
• Assess outcomes<br />
• Control escalat<strong>in</strong>g costs<br />
• Resist political pressures by strong provider groups.<br />
• Coord<strong>in</strong>ate a common contract<strong>in</strong>g mechanism with other<br />
f<strong>in</strong>anc<strong>in</strong>g agencies<br />
• Prevent abuse<br />
• Monitor and ensure quality<br />
• Assess outcomes<br />
• Apply flat fees to all hospitalizations (surgical and medical)<br />
• Resist political pressures by hospitals (e.g. for <strong>in</strong>clusion <strong>of</strong><br />
more hospitals)<br />
• Coord<strong>in</strong>ate a common contract<strong>in</strong>g mechanism with other<br />
f<strong>in</strong>anc<strong>in</strong>g agencies
Lebanon<br />
However, the effectiveness <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> as a tool for improv<strong>in</strong>g <strong>health</strong><br />
<strong>sector</strong> performance can be improved. <strong>The</strong>se <strong>arrangements</strong>:<br />
Are not yet part <strong>of</strong> a clear national strategy for <strong>health</strong> <strong>sector</strong> reform, therefore their use as a tool can<br />
only be limited <strong>in</strong> effectiveness and scope. <strong>The</strong> ma<strong>in</strong> limitation today is the fragmentation <strong>of</strong><br />
<strong>health</strong> care f<strong>in</strong>anc<strong>in</strong>g. Without a uniform f<strong>in</strong>anc<strong>in</strong>g scheme, which should be the outcome <strong>of</strong><br />
a political process, contracts can only have limited success <strong>in</strong> giv<strong>in</strong>g the government the<br />
needed leverage to manage care. Furthermore, consider<strong>in</strong>g that 65%–70% <strong>of</strong> all <strong>health</strong> care<br />
expenditures <strong>in</strong> Lebanon are borne by the citizens (with the poor spend<strong>in</strong>g disproportionately<br />
high percentages <strong>of</strong> their <strong>in</strong>come), even with optimization <strong>of</strong> contract<strong>in</strong>g mechanisms, there<br />
is a limit to what can be done and the ma<strong>in</strong> focus should be on improv<strong>in</strong>g public f<strong>in</strong>anc<strong>in</strong>g <strong>of</strong><br />
the <strong>health</strong> care delivery.<br />
Rema<strong>in</strong> fragmented with different agencies contract<strong>in</strong>g with the same providers us<strong>in</strong>g different<br />
terms and tariffs.<br />
Are not based on evaluation <strong>of</strong> measurable <strong>in</strong>dicators for both processes and outcomes. <strong>The</strong>refore,<br />
there are very limited capacities at present for evaluation <strong>of</strong> performance <strong>of</strong> contracted<br />
parties.<br />
Favour an ever stronger private <strong>sector</strong> over the public <strong>sector</strong>, which has been underm<strong>in</strong>ed.<br />
Do not provide the government with adequate leverage to shift emphasis from acute care to<br />
preventive and outpatient care. In this sense, contracts serve more to “manage” the current<br />
<strong>health</strong> <strong>sector</strong> crisis <strong>in</strong> Lebanon rather than contribute to effective long term solutions.<br />
Place little emphasis on broad determ<strong>in</strong>ants <strong>of</strong> <strong>health</strong>. Related to this po<strong>in</strong>t, there is little<br />
coord<strong>in</strong>ation with other governmental agencies that work on these determ<strong>in</strong>ants, such as the<br />
M<strong>in</strong>istry <strong>of</strong> Social Affairs.<br />
Rarely solicit the consumer perspective and do not mean<strong>in</strong>gfully <strong>in</strong>volve citizens <strong>in</strong> choice or<br />
monitor<strong>in</strong>g <strong>of</strong> contracts. This relates to issue <strong>of</strong> need for democratization <strong>of</strong> <strong>health</strong> care<br />
policy processes.<br />
Do not adequately emphasize models <strong>of</strong> <strong>in</strong>tegration (e.g. prevention–treatment, <strong>in</strong>-hospital–<br />
community).<br />
CONCLUSIONS AND RECOMMENDATIONS<br />
Contractual <strong>arrangements</strong> <strong>in</strong> the <strong>health</strong> <strong>sector</strong> are abundant <strong>in</strong> Lebanon. <strong>The</strong>y are used<br />
mostly for hospitalization and ambulatory care services, with over 80% <strong>of</strong> the Lebanese<br />
population covered through these contracts. However, contracts also cover a variety <strong>of</strong> public<br />
<strong>health</strong> functions. <strong>The</strong> breadth <strong>of</strong> these contracts reflects the dom<strong>in</strong>ant <strong>role</strong> <strong>of</strong> the<br />
nongovernmental <strong>sector</strong> as compared with the public <strong>health</strong> <strong>sector</strong>. Contract<strong>in</strong>g allows the<br />
different public agencies to obta<strong>in</strong> services needed for beneficiaries <strong>in</strong> all <strong>of</strong> Lebanon. <strong>The</strong><br />
Report has reviewed the different <strong>contractual</strong> <strong>arrangements</strong> <strong>of</strong> different public organizations and<br />
identified strengths and weaknesses. <strong>The</strong>se are summarized <strong>in</strong> Table 5. <strong>The</strong> review also identified<br />
the ma<strong>in</strong> obstacles to improv<strong>in</strong>g <strong>contractual</strong> <strong>arrangements</strong>, which <strong>in</strong>clude lack <strong>of</strong> political
Lebanon<br />
support for wide reform and lack <strong>of</strong> capacities with<strong>in</strong> current agencies for substantial upgrad<strong>in</strong>g<br />
<strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong>.<br />
Based on this review, the follow<strong>in</strong>g steps are recommended to improve the use <strong>of</strong><br />
<strong>contractual</strong> arrangement <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance <strong>in</strong> Lebanon. Although many<br />
recommendations can be made, these steps are highlighted because <strong>of</strong> their perceived feasibility<br />
and potentially large impact.<br />
1. In light <strong>of</strong> the fragmentation <strong>of</strong> the contract<strong>in</strong>g mechanisms, create a central contract<strong>in</strong>g<br />
body which contracts with different providers on behalf <strong>of</strong> the f<strong>in</strong>anc<strong>in</strong>g agencies.<br />
2. If the previous step is not immediately feasible, at the very least unify tarification for<br />
similar services contracted by different agencies.<br />
3. Extend the use <strong>of</strong> flat rates to <strong>in</strong>clude all surgical procedures and <strong>in</strong>troduc<strong>in</strong>g flat fees to a<br />
variety <strong>of</strong> medical conditions.<br />
4. In light <strong>of</strong> the accumulated experience at the M<strong>in</strong>istry <strong>of</strong> Public Health through the<br />
successful partnership with WHO <strong>in</strong> the jo<strong>in</strong>t management <strong>of</strong> several national <strong>health</strong><br />
programmes, the gradually transfer these programmes to be fully managed at the M<strong>in</strong>istry<br />
<strong>of</strong> Public Health.<br />
5. Consider<strong>in</strong>g the current fragmentation <strong>of</strong> <strong>health</strong> care, use current contracts to l<strong>in</strong>k <strong>in</strong>patient<br />
and outpatient care. <strong>The</strong> case <strong>of</strong> management <strong>of</strong> coronary heart disease could be a pilot<br />
study <strong>in</strong> this regard.<br />
6. Incorporate consumer perspectives and mean<strong>in</strong>gful representation and <strong>in</strong>put <strong>in</strong>to the<br />
contract-mak<strong>in</strong>g processes.<br />
7. Although implement<strong>in</strong>g the mechanisms does not appear to be politically feasible at this<br />
po<strong>in</strong>t, study the potential contribution <strong>of</strong> mechanisms such as primary care gate-keep<strong>in</strong>g<br />
and preferred providers to improv<strong>in</strong>g <strong>contractual</strong> <strong>arrangements</strong>.<br />
FURTHER READING<br />
Note: <strong>The</strong> aim <strong>of</strong> this expanded bibliography is to serve as a potentially usefully resource beyond<br />
<strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong>to broader issues <strong>in</strong> <strong>health</strong> <strong>sector</strong> organization and reform <strong>in</strong><br />
Lebanon.<br />
Books concern<strong>in</strong>g <strong>health</strong> <strong>sector</strong> <strong>in</strong> Lebanon<br />
1985<br />
ﺔﻳرﺪﻨﻜﺳﻻا . ﻂﺳﻮﺘﻤﻟا قﺮﺸﻟ ﻲﻤﻴﻠﻗﻹا ﺐﺘﻜﻤﻟا – ﺔﻴﻤﻟﺎﻌﻟا ﺔﺤﺼﻟا ﺔﻤﻈﻨﻣ . نﺎﻨﺒﻟ ﻲﻓ ﺔﻴﺤﺼﻟا ﺔﻳﺎﻋﺮﻟا . ﻞﻔﻧﺮﻗ ﻞﻴﺒﻧ . د و ةوﺮﻣ نﺎﻧﺪﻋ . د<br />
175<br />
. 1
Lebanon<br />
ﺔﻌﺒﻄﻟا ،نﺎﻨﺒﻟ ،توﺮﻴﺑ . ﻲﺑﺮﻌﻟا ﺮﻜﻔﻟا راد . ﺔﻴﺤﺼﻟا ﺔﺳﺎﻴﺴﻟا رﺎﺴﻤﻟ ﺢﻴﺤﺼﺗ و ﻲﺤﺼﻟا قﺎﻔﻧﻹا ﺪﻴﺷﺮﺗ ﻮﺤﻧ . لﻮﻠﺣ و ﻊﻗاو : ﺔﺤﺼﻟا . ﺪﻴﺑﺮﻋ ﺞﻴﻬﺑ . د<br />
2000 ﻰﻟوﻷا<br />
Tabbarah R. <strong>The</strong> <strong>health</strong> <strong>sector</strong> <strong>in</strong> Lebanon. MADMA, Beirut, 2000<br />
Ammar W. Health system and reform <strong>in</strong> Lebanon. Beirut, World Health Organization, 2003<br />
Peer–reviewed literature concern<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance and reform <strong>in</strong> Lebanon<br />
Kronfol NM, Bashshur R. Lebanon’s <strong>health</strong> care policy: a case study <strong>in</strong> the evolution <strong>of</strong> a <strong>health</strong><br />
system under stress. J Public Health Policy 1989; 10(3): 377–96<br />
Van Lerberghe W et al. Reform follows failure: I. unregulated private care <strong>in</strong> Lebanon. Health<br />
Policy and Plann<strong>in</strong>g 1997; 12 (4): 296–311<br />
Van Lerberghe W et al. (1997). Reform follows failure: II. pressure for change <strong>in</strong> the Lebanese<br />
<strong>health</strong> <strong>sector</strong>. Health Policy and Plann<strong>in</strong>g 1997, 12(4): 312–319<br />
Ammar W, Mechbal AH, Awar M. Organisation des services de so<strong>in</strong>s, système de couverture et<br />
contribution du m<strong>in</strong>istère de la santé publique. Leb Med. J 1998; 46: 43–46<br />
Ammar W, Jokhadar A, Awar M. Health <strong>sector</strong> reform <strong>in</strong> Lebanon. Lebanese Medical Journal.<br />
1999; 46(6); 328–334<br />
Ammar W, Awar M. What does the World Health Report 2000 br<strong>in</strong>g to Lebanon?<br />
J Med Liban. 2001, 49(3):123–5<br />
Ammar W, Kasparian R. What is fair <strong>in</strong> f<strong>in</strong>anc<strong>in</strong>g fairness? J Med Liban. 2001 May-Jun; 49(3):<br />
126–8<br />
Reports <strong>of</strong> major surveys on <strong>health</strong> and <strong>health</strong> care <strong>in</strong> Lebanon<br />
Deeb M, ed. Beirut: A <strong>health</strong> pr<strong>of</strong>ile 1984–1994. American University <strong>of</strong> Beirut, Beirut 1997<br />
M<strong>in</strong>istry <strong>of</strong> Social Affairs. Population and Household Survey, 1996<br />
Central Adm<strong>in</strong>istration <strong>of</strong> Statistics. Household liv<strong>in</strong>g conditions, 1997<br />
M<strong>in</strong>istry <strong>of</strong> Social Affairs. National Household Health Expenditure and Utilization Survey, 1999<br />
Major reports and documents concern<strong>in</strong>g <strong>health</strong> <strong>sector</strong> performance and reform <strong>in</strong> Lebanon<br />
176<br />
. 2
Lebanon<br />
Sabri B et al. Health <strong>sector</strong> reform <strong>in</strong> Lebanon. Report <strong>of</strong> a WHO preparatory mission. World<br />
Health Organization, Eastern Mediterranean Regional Office, June 1996.<br />
<strong>The</strong> World Bank, Human Development Group, Middle East and North Africa. Health <strong>sector</strong> <strong>in</strong><br />
Lebanon: Issues and prospects. MNSHD Discussion Paper Series No.4. 2000<br />
M<strong>in</strong>istry <strong>of</strong> Public Health, Office <strong>of</strong> the Director General. Annual Report, 2000<br />
Kronfol NM. <strong>The</strong> Lebanese Health Care System. Options for Reform. M<strong>in</strong>istry <strong>of</strong> Public Health,<br />
2000<br />
Kronfol NM. <strong>The</strong> Rebuild<strong>in</strong>g <strong>of</strong> the Lebanese Healthcare System: Successes and Failures.<br />
December 2002<br />
Hajjar H. Evaluation <strong>of</strong> the agreement between the M<strong>in</strong>istry <strong>of</strong> Public Health and the NGOs<br />
related to primary heath care services. December 2003.<br />
Selected papers from Regional Social Protection <strong>in</strong> an Insecure Era: A South-South Exchange on<br />
Alternative Social Policies Responses to Globalization. Inter-Regional Workshop, February<br />
27th–March 1st, 2001, Beirut<br />
Background/general papers on <strong>contractual</strong> <strong>arrangements</strong><br />
Lavoie JG. Governed by contracts: <strong>The</strong> development <strong>of</strong> <strong>in</strong>digenous primary <strong>health</strong> services <strong>in</strong><br />
Canada, Australia and New Zealand. Journal <strong>of</strong> Aborig<strong>in</strong>al Health January 2004, 6–24.<br />
Barr D et al. Research protocols to evaluate the effectiveness <strong>of</strong> public/private partnerships <strong>in</strong><br />
enhanc<strong>in</strong>g <strong>health</strong> and welfare systems development. Center for Health Policy, Institute for<br />
International Studies, Stanford University, February 2004.<br />
Papers provided by EMRO concern<strong>in</strong>g contract<strong>in</strong>g <strong>arrangements</strong>.<br />
177
Morocco<br />
MOROCCO
INTRODUCTION<br />
Morocco<br />
Dur<strong>in</strong>g the past few years, public organizations have become <strong>in</strong>creas<strong>in</strong>gly open to<br />
work<strong>in</strong>g with the private <strong>sector</strong>. As part <strong>of</strong> public <strong>sector</strong> reform, this openness is the result <strong>of</strong><br />
grow<strong>in</strong>g <strong>in</strong>terest <strong>in</strong> resource efficiency and performance improvement. In the field <strong>of</strong> <strong>health</strong>,<br />
contract<strong>in</strong>g is considered a new mechanism that can enable the <strong>health</strong> <strong>sector</strong> to improve its<br />
responsiveness to changes <strong>in</strong> the <strong>health</strong> system environment and the national context.<br />
<strong>The</strong> <strong>contractual</strong> arrangement <strong>of</strong>fers an opportunity to adapt <strong>in</strong>terventions to a wide range<br />
<strong>of</strong> <strong>health</strong> objectives, as well as to br<strong>in</strong>g together different actors <strong>in</strong> the field <strong>of</strong> <strong>health</strong>. Given<br />
their active <strong>role</strong>s, these actors (service providers, <strong>in</strong>surance agents, <strong>in</strong>dustry, technology, civil<br />
society) are known as stakeholders<br />
In the meantime, the systematic use <strong>of</strong> this new mechanism has become more difficult<br />
due to the diversity <strong>of</strong> its forms and contents. This study attempts to document and analyse the<br />
experiences <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health <strong>of</strong> Morocco <strong>in</strong> the area <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> for<br />
<strong>health</strong>.<br />
OBJECTIVES AND METHODOLOGY<br />
Objectives<br />
This study is a part <strong>of</strong> a regional <strong>in</strong>itiative by the WHO Regional Office for the Eastern<br />
Mediterranean aimed at explor<strong>in</strong>g the potential <strong>of</strong> the countries <strong>of</strong> the Region to contract with<br />
the private <strong>sector</strong> for provision <strong>of</strong> <strong>health</strong> services. Such exploration responds to the need <strong>of</strong><br />
m<strong>in</strong>istries <strong>of</strong> <strong>health</strong> to develop strategies for public–private mix as a way to improve <strong>health</strong><br />
system performance.<br />
Specifically, the study aims at document<strong>in</strong>g the experience <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health <strong>in</strong><br />
undertak<strong>in</strong>g <strong>contractual</strong> <strong>arrangements</strong>, and analysis two specific experiences <strong>of</strong> contract<strong>in</strong>g<br />
with the private <strong>sector</strong> that represent important potentials for outsourc<strong>in</strong>g <strong>health</strong> services <strong>in</strong><br />
Morocco. <strong>The</strong> first is a traditional experience <strong>of</strong> subcontract<strong>in</strong>g <strong>of</strong> hospital support services.<br />
<strong>The</strong> second is an <strong>in</strong>novative experience recently started that consists <strong>of</strong> contract<strong>in</strong>g for<br />
equipment and supplies required for the care <strong>of</strong> end-stage renal disease.<br />
Def<strong>in</strong>ition <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong><br />
<strong>The</strong> <strong>contractual</strong> arrangement is a type <strong>of</strong> a public–private mix that takes the form <strong>of</strong> a<br />
partnership between two or more organizations belong<strong>in</strong>g to different activity <strong>sector</strong>s and<br />
seek<strong>in</strong>g to reach common objectives.<br />
<strong>The</strong> rationale for <strong>in</strong>volv<strong>in</strong>g the private <strong>sector</strong> is the fact that this <strong>sector</strong> accumulates<br />
resources, competencies and management styles sufficiently <strong>in</strong>novative to contribute to the<br />
improvement <strong>of</strong> the <strong>health</strong> system performance. <strong>The</strong> grow<strong>in</strong>g need to modernize public<br />
services and to respond with efficiency to population expectations is <strong>in</strong>centive for the public<br />
<strong>sector</strong> to turn to the private or nongovernmental organization <strong>sector</strong>.<br />
179
Morocco<br />
<strong>The</strong> type <strong>of</strong> <strong>contractual</strong> arrangement depends on the nature <strong>of</strong> the relationship (purchase,<br />
leas<strong>in</strong>g, delegation, cooperation) and the subject (support services, care, etc.). <strong>The</strong> nature <strong>of</strong><br />
1<br />
the <strong>contractual</strong> relationship allows for three types <strong>of</strong> <strong>contractual</strong> arrangementTP PT: purchase or<br />
leas<strong>in</strong>g; delegation <strong>of</strong> responsibility; and cooperation.<br />
Methodology<br />
To implement this work, several data collection methods were used.<br />
Document review. Internal documents were compiled on the experience <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong><br />
Health <strong>in</strong> deal<strong>in</strong>g with <strong>contractual</strong> arrangement. <strong>The</strong>se ma<strong>in</strong>ly comprised legal regulations<br />
and <strong>in</strong>struction guides and <strong>in</strong>formation related to the case studies, such as statistical data<br />
and contract documents.<br />
Interview with key personnel. Six persons were <strong>in</strong>terviewed from the Department <strong>of</strong><br />
Regulations and Conflicts, Department <strong>of</strong> Plann<strong>in</strong>g and F<strong>in</strong>ancial Resources and the<br />
Department <strong>of</strong> Hospitals and Ambulatory Care.<br />
A survey mailed to public hospitals. <strong>The</strong> survey sought to document the experience <strong>of</strong> hospitals<br />
<strong>in</strong> subcontract<strong>in</strong>g. It covered all 74 state hospitals under autonomous management<br />
(SEGMA) gathered <strong>in</strong> 46 prov<strong>in</strong>cial hospital centres. A questionnaire was elaborated for<br />
this purpose and tested <strong>in</strong> a hospital prior to its use (Annex 1). A summary <strong>of</strong> survey<br />
results are attached as Annex 2.<br />
Focus group discussions. <strong>The</strong>se were held with strategic actors <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health and<br />
with private operators hav<strong>in</strong>g experience <strong>in</strong> contract<strong>in</strong>g with the M<strong>in</strong>istry <strong>of</strong> Health.<br />
2.4 Limits and constra<strong>in</strong>ts <strong>of</strong> the study<br />
<strong>The</strong> short time allocated for implement<strong>in</strong>g the study constituted the ma<strong>in</strong> constra<strong>in</strong>t to<br />
the study. Given the orig<strong>in</strong>ality <strong>of</strong> the research topic and the diversity <strong>of</strong> the resources<br />
<strong>in</strong>formation to be consulted, it was difficult to implement the study with<strong>in</strong> three months.<br />
<strong>The</strong> def<strong>in</strong>ition <strong>of</strong> <strong>contractual</strong> arrangement provided <strong>in</strong> the reference statements is<br />
narrow. <strong>The</strong> <strong>contractual</strong> arrangement is a k<strong>in</strong>d <strong>of</strong> strategic alliance that leads to the creation <strong>of</strong><br />
value. In the bus<strong>in</strong>ess world, such value refers either to a pr<strong>of</strong>it or to a privileged position <strong>in</strong><br />
the market. In the field <strong>of</strong> <strong>health</strong>, the added value must necessarily have a social and ethical<br />
aspect. <strong>The</strong>refore it must be protected by one <strong>of</strong> the actors concerned <strong>in</strong> the <strong>contractual</strong><br />
arrangement. This should be the State, given that the State is <strong>in</strong> charge <strong>of</strong> protect<strong>in</strong>g the<br />
general public <strong>in</strong>terest. <strong>The</strong>refore the <strong>contractual</strong> arrangement <strong>in</strong> the field <strong>of</strong> <strong>health</strong> must be<br />
submitted to law; this means necessarily that its def<strong>in</strong>ition must <strong>in</strong>clude the public<br />
organization as <strong>in</strong>itiator.<br />
Build<strong>in</strong>g on the proposed structure to identify the actors <strong>in</strong>volved <strong>in</strong> the governance <strong>of</strong><br />
<strong>health</strong> systems (State, private <strong>sector</strong> and civil society), the follow<strong>in</strong>g def<strong>in</strong>ition is put forward:<br />
1 Classification by Perrot J, Carr<strong>in</strong> G, Sergent F. (1997) L’approche contractuelle: de nouveaux partenariats pour<br />
la santé dans les pays en développement. WHO/ICO/MESD.24<br />
180
Morocco<br />
A <strong>contractual</strong> arrangement is a partnership between a public organization, represent<strong>in</strong>g the<br />
State, and one or many stakeholders that aims to creat<strong>in</strong>g an added social value or an earn<strong>in</strong>g<br />
opportunity. <strong>The</strong> stakeholders can be private, for-pr<strong>of</strong>it organizations or non-pr<strong>of</strong>it<br />
organizations represent<strong>in</strong>g civil society.<br />
RESULTS AND DISCUSSION<br />
Background<br />
Evolution <strong>of</strong> the Moroccan Health System<br />
S<strong>in</strong>ce the formulation <strong>of</strong> the first <strong>health</strong> policy <strong>in</strong> 1959, the Moroccan <strong>health</strong> system was<br />
dom<strong>in</strong>ated by the public <strong>sector</strong> and characterized by the centralization <strong>of</strong> management. <strong>The</strong><br />
State was positioned <strong>in</strong> the heart <strong>of</strong> the <strong>health</strong> system, perform<strong>in</strong>g at once the functions <strong>of</strong><br />
f<strong>in</strong>anc<strong>in</strong>g, adm<strong>in</strong>istration and provision. <strong>The</strong> private <strong>sector</strong> developed <strong>in</strong>dependently <strong>of</strong> the<br />
public <strong>sector</strong>, and with complete autonomy.<br />
In the early 1990s, the problem <strong>of</strong> <strong>health</strong> f<strong>in</strong>anc<strong>in</strong>g brought hospitals to the forefront <strong>of</strong><br />
national <strong>health</strong> agenda, despite the fact that hospitals were the ma<strong>in</strong> beneficiaries <strong>of</strong> <strong>health</strong><br />
spend<strong>in</strong>g. <strong>The</strong> need for hospital reform became associated with the need for overall reform <strong>of</strong><br />
the <strong>health</strong> f<strong>in</strong>anc<strong>in</strong>g system. As a result, a number <strong>of</strong> reform fields are currently be<strong>in</strong>g carried<br />
out <strong>in</strong> the <strong>health</strong> system, focus<strong>in</strong>g on four ma<strong>in</strong> areas:<br />
decentralization<br />
reform <strong>of</strong> public spend<strong>in</strong>g<br />
reform <strong>of</strong> f<strong>in</strong>anc<strong>in</strong>g<br />
reform <strong>of</strong> public hospitals.<br />
<strong>The</strong>se reforms created a receptive environment for the establishment <strong>of</strong> partnerships<br />
with local actors (local collectives, private and civil society <strong>sector</strong>s) aimed at provid<strong>in</strong>g a<br />
timely and appropriate response to the real needs <strong>of</strong> citizens.<br />
<strong>The</strong> decentralization <strong>in</strong>itiative, expressed through a number <strong>of</strong> <strong>sector</strong>-wide measures,<br />
has three ma<strong>in</strong> objectives:<br />
br<strong>in</strong>g the adm<strong>in</strong>istration closer to people <strong>in</strong> order to respond to their needs and ensure equal<br />
access to public services;<br />
strengthen the dialogue between the State and the local partners <strong>in</strong> order to use reach all levels<br />
<strong>of</strong> society;<br />
re<strong>in</strong>force coherence and coord<strong>in</strong>ation with the peripheral levels <strong>in</strong> order to achieve optimal<br />
programm<strong>in</strong>g at the local level.<br />
One <strong>of</strong> the ma<strong>in</strong> elements <strong>of</strong> the public management reform concerns the adm<strong>in</strong>istrative<br />
function <strong>of</strong> the State, <strong>of</strong> which, appeared the necessity to elaborate and apply a new budget<br />
management style focus<strong>in</strong>g on results, known also as contract<strong>in</strong>g.<br />
181
Morocco<br />
Experience <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health <strong>in</strong> contract<strong>in</strong>g<br />
Contract<strong>in</strong>g arrangement based on purchase or leas<strong>in</strong>g<br />
Purchase <strong>of</strong> cares services<br />
This is one <strong>of</strong> the oldest types <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> between the private and<br />
public <strong>sector</strong>s <strong>in</strong> Morocco, <strong>in</strong>itiated as a way to address a deficit <strong>in</strong> human resources,<br />
particularly medical, <strong>in</strong> the public <strong>sector</strong>. <strong>The</strong> goal <strong>of</strong> this contract<strong>in</strong>g agreement was to assign<br />
physicians, pharmacists and dentists to public <strong>health</strong> <strong>in</strong>stitutions <strong>in</strong> areas with limited <strong>health</strong><br />
care coverage. Such <strong>contractual</strong> arrangement becomes an agreement. This agreement was<br />
formalized by M<strong>in</strong>isterial decree <strong>in</strong> 1972, which def<strong>in</strong>ed the legal status <strong>of</strong> these human<br />
resources.<br />
Such agreements may be signed jo<strong>in</strong>tly by the local representative <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong><br />
Health at the prov<strong>in</strong>ce level, and the <strong>health</strong> workers practis<strong>in</strong>g <strong>in</strong> the private <strong>sector</strong>, subject to<br />
approval by the M<strong>in</strong>ister <strong>of</strong> Health. In 1996, new legislation was <strong>in</strong>troduced requir<strong>in</strong>g<br />
additional approval for such agreements by the National Council <strong>of</strong> the Medical Pr<strong>of</strong>essional<br />
Association.<br />
<strong>The</strong> private practitioner is employed as a part-time <strong>health</strong> worker with<strong>in</strong> a public <strong>health</strong><br />
<strong>in</strong>stitution on the basis <strong>of</strong> the conditions set by the relevant decrees. He or she receives a<br />
monthly salary provided through the budget <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health. <strong>The</strong> use <strong>of</strong> such<br />
<strong>contractual</strong> <strong>arrangements</strong> is decl<strong>in</strong><strong>in</strong>g considerably with the expansion <strong>of</strong> public <strong>health</strong><br />
services.<br />
Purchase <strong>of</strong> non-medical services<br />
Contract<strong>in</strong>g for the purchase <strong>of</strong> non-medical services applies to the purchase by local<br />
public <strong>health</strong> authorities <strong>of</strong> equipment or supplies as part <strong>of</strong> <strong>health</strong> care (biomedical<br />
equipments, pharmaceutical products), or support services that are not part <strong>of</strong> <strong>health</strong> care. This<br />
is regarded as subcontract<strong>in</strong>g, and applies <strong>in</strong> this case to contracts for services such as<br />
ma<strong>in</strong>tenance, clean<strong>in</strong>g, cater<strong>in</strong>g, laundry or security, between the hospital and a private<br />
company.<br />
Such purchas<strong>in</strong>g contracts have a strong legal framework. <strong>The</strong>y are executed <strong>in</strong><br />
compliance procedure laid out <strong>in</strong> the public bids regulations. Depend<strong>in</strong>g on the amount<br />
<strong>in</strong>volved, the adm<strong>in</strong>istration purchases services either through public bid <strong>of</strong>fers or through<br />
purchase orders, with due respect to transparency and fairness <strong>in</strong> competition. <strong>The</strong> procedures<br />
require an early f<strong>in</strong>ancial review prior to implementation <strong>of</strong> the public bid or purchase order to<br />
be submitted to the Office <strong>of</strong> Budget<strong>in</strong>g and Expenditures Control <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> F<strong>in</strong>ance.<br />
Support and logistic services are subcontracted <strong>in</strong> accordance with the public bids<br />
procedure. <strong>The</strong> adm<strong>in</strong>istration identifies the nature and the quantity <strong>of</strong> the services, the<br />
payment calendar and conditions, as well as the quality <strong>in</strong>dicators for evaluation <strong>of</strong> the<br />
182
Morocco<br />
services, as the adm<strong>in</strong>istration is responsible for the monitor<strong>in</strong>g and evaluation <strong>of</strong> the different<br />
operations.<br />
<strong>The</strong> evaluation <strong>of</strong> the different subcontract<strong>in</strong>g experiences that have been <strong>in</strong>troduced <strong>in</strong><br />
the public <strong>health</strong> services showed that these services were <strong>of</strong> higher quality due to their level<br />
<strong>of</strong> pr<strong>of</strong>essionalism, and that the cost to quality ratio was optimal. Subcontract<strong>in</strong>g also allowed<br />
the development <strong>of</strong> small and medium bus<strong>in</strong>esses and for the employment <strong>of</strong> youth.<br />
Various problems persist. In remote areas, far from towns, the competition is limited. In<br />
general, there is only one company that <strong>of</strong>ten comes from a distance and may not have the<br />
required competency. <strong>The</strong> contracts do not <strong>in</strong>clude conditions for the proper evaluation <strong>of</strong> the<br />
service provided.<br />
In order to address these problems, <strong>in</strong> 2002 the M<strong>in</strong>istry <strong>of</strong> Health issued an Act<br />
(No. 49/DHSA/20/21) sett<strong>in</strong>g the terms and conditions for subcontract<strong>in</strong>g bids. Model<br />
contract specifications were attached to this Act. <strong>The</strong>se specifications were developed <strong>in</strong> order<br />
to unify the basic contract<strong>in</strong>g documents and to make use <strong>of</strong> longer-term bids, contracted for<br />
more than a year. In general the length <strong>of</strong> such bids is about 5 years. <strong>The</strong> conditions and<br />
procedures for these bids are set by the public bids regulations.<br />
Regardless <strong>of</strong> the service purchased, as soon as the Office <strong>of</strong> Budget<strong>in</strong>g and<br />
Expenditures Control signs the public bid agreement, the private company receives a service<br />
order request<strong>in</strong>g the implementation <strong>of</strong> the conditions agreed upon <strong>in</strong> the bid document<br />
(<strong>contractual</strong> agreement). Payment is effected after the execution <strong>of</strong> the terms <strong>of</strong> the contract<br />
agreement (delivery <strong>of</strong> goods, implementation <strong>of</strong> work, etc.) with<strong>in</strong> the time-frame specified<br />
<strong>in</strong> the contract and after check-up by the adm<strong>in</strong>istration and review by the M<strong>in</strong>istry <strong>of</strong><br />
F<strong>in</strong>ance. Such contract agreements have been made at the national, regional and local levels,<br />
and occasionally at the <strong>in</strong>ternational level.<br />
Leas<strong>in</strong>g <strong>of</strong> medical equipment and supplies<br />
S<strong>in</strong>ce 2003, Morocco has engaged <strong>in</strong> leas<strong>in</strong>g as a form <strong>of</strong> contract<strong>in</strong>g arrangement with<br />
the private <strong>sector</strong>. This decision was brought about by difficulties faced by the M<strong>in</strong>istry <strong>of</strong><br />
Health <strong>in</strong> mobiliz<strong>in</strong>g funds to purchase equipment or <strong>in</strong> provid<strong>in</strong>g certa<strong>in</strong> services <strong>in</strong> the<br />
context <strong>of</strong> limited resources. Examples are the provision <strong>of</strong> haemodialysis, tomography or<br />
hospital solid waste handl<strong>in</strong>g. <strong>The</strong> experience <strong>of</strong> Morocco <strong>of</strong> leas<strong>in</strong>g equipment to treat 2000<br />
patients with end-stage renal disease is reviewed later <strong>in</strong> this report as a case study.<br />
Contract<strong>in</strong>g <strong>arrangements</strong> based on delegation<br />
<strong>The</strong> external <strong>in</strong>stitutions depend<strong>in</strong>g <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health are organized basically on<br />
two statutes:<br />
<strong>The</strong> functional decentralization (delegation) regard<strong>in</strong>g hospitals;<br />
<strong>The</strong> territorial decentralization regard<strong>in</strong>g adm<strong>in</strong>istrative entities <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health.<br />
183
Morocco<br />
In the context <strong>of</strong> re<strong>in</strong>forc<strong>in</strong>g the responsibility <strong>of</strong> the external <strong>in</strong>stitutions, legislators<br />
considered two types <strong>of</strong> contract<strong>in</strong>g <strong>arrangements</strong> adapted to these two statutes: the work-plan<br />
contract and the program budget.<br />
<strong>The</strong> work-plan contract<br />
<strong>The</strong> first contract<strong>in</strong>g experience between the M<strong>in</strong>istry <strong>of</strong> Health and autonomous public<br />
<strong>in</strong>stitutions was carried out <strong>in</strong> 2002. Two work-plan contracts were made between the State,<br />
represented by the M<strong>in</strong>istry <strong>of</strong> Health and the M<strong>in</strong>istry <strong>of</strong> F<strong>in</strong>ance and Privatization, and two<br />
university hospitals, Ibn S<strong>in</strong>a (Rabat) and Ibn Rochd (Casablanca).<br />
<strong>The</strong>se two work-plan contracts were developed to re<strong>in</strong>force the l<strong>in</strong>ks between the State<br />
and these centres. <strong>The</strong>refore, the objectives assigned to these centres are def<strong>in</strong>ed for the period<br />
<strong>of</strong> the contracts as well as the periodic evaluation <strong>of</strong> the degree <strong>of</strong> fulfilment <strong>of</strong> the terms <strong>of</strong><br />
these contracts.<br />
<strong>The</strong>se two work-plan contracts illustrate the will<strong>in</strong>gness <strong>of</strong> the State to <strong>in</strong>troduce new<br />
contract<strong>in</strong>g relations aim<strong>in</strong>g at:<br />
support<strong>in</strong>g the university hospitals <strong>in</strong> focus<strong>in</strong>g on their statutory responsibilities for care,<br />
education, tra<strong>in</strong><strong>in</strong>g and research;<br />
ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g these university hospitals as national hospital centres <strong>of</strong> reference provid<strong>in</strong>g <strong>health</strong><br />
care services at the tertiary level;<br />
adoption <strong>of</strong> modern management based on accountability;<br />
optimization <strong>of</strong> the university hospitals’ resources and expenditure;<br />
adapt<strong>in</strong>g the <strong>in</strong>stitutional and judicial contexts <strong>of</strong> these two centres to ensure harmonious<br />
development with their environment.<br />
A special monitor<strong>in</strong>g committee conducts monitor<strong>in</strong>g <strong>of</strong> the work-plan contract. Its<br />
membership <strong>in</strong>cludes representatives <strong>of</strong> the contract<strong>in</strong>g parties, with the M<strong>in</strong>ister <strong>of</strong> F<strong>in</strong>ance<br />
and Privatization as its president. <strong>The</strong> monitor<strong>in</strong>g committee meets at least twice a year to<br />
exam<strong>in</strong>e:<br />
reports <strong>of</strong> <strong>in</strong>dependent experts regard<strong>in</strong>g the quality <strong>of</strong> services, the hospital hygiene<br />
programme and the environmental protection measures;<br />
external auditors’ reports;<br />
annual reports <strong>of</strong> the work-plan contract implementation<br />
performance and results obta<strong>in</strong>ed by the hospital centre.<br />
<strong>The</strong> programme budget<br />
<strong>The</strong> programme budget is the second form <strong>of</strong> contract<strong>in</strong>g between the State, represented<br />
by the central <strong>health</strong> adm<strong>in</strong>istration, and external services. It is an outgrowth <strong>of</strong> public<br />
spend<strong>in</strong>g reform <strong>in</strong> the form <strong>of</strong> results-based budget management.<br />
184
Morocco<br />
<strong>The</strong> programme budget is like a programme contract that lays down every year the<br />
central adm<strong>in</strong>istration’s and the external departments’ responsibilities with regard to achiev<strong>in</strong>g<br />
agreed-upon objectives, but with<strong>in</strong> the context <strong>of</strong> flexible three-year programm<strong>in</strong>g with an<br />
annual budget.<br />
In accordance with the Guide for results-based budget management (July 2001), the<br />
programme-budget is “a formal process aim<strong>in</strong>g at determ<strong>in</strong><strong>in</strong>g every year, but with<strong>in</strong> a<br />
flexible three-year programme, the respective responsibilities <strong>of</strong> the Central Adm<strong>in</strong>istration,<br />
hav<strong>in</strong>g the decision power to govern a M<strong>in</strong>istry, and the decentralized Services belong<strong>in</strong>g to<br />
the same M<strong>in</strong>istry and benefit<strong>in</strong>g from a delegation <strong>of</strong> power <strong>in</strong> order to achieve the<br />
2<br />
commonly agreed upon objectives”TP PT.<br />
<strong>The</strong> programme budget allows the central adm<strong>in</strong>istration and the external services to<br />
identify the objectives to be atta<strong>in</strong>ed dur<strong>in</strong>g a three-year period and to provide the necessary<br />
resources to these external services. It also allows for follow-up <strong>of</strong> the implementation<br />
through performance <strong>in</strong>dicators and for giv<strong>in</strong>g special attention to treatment results and to the<br />
terms for use <strong>of</strong> resources.<br />
<strong>The</strong> programme budget is a management tool that particularly allows for:<br />
br<strong>in</strong>g<strong>in</strong>g together the public <strong>health</strong> adm<strong>in</strong>istration and the citizens;<br />
improv<strong>in</strong>g the quality <strong>of</strong> <strong>health</strong> services;<br />
facilitat<strong>in</strong>g decentralization <strong>of</strong> management powers;<br />
establish<strong>in</strong>g an equilibrium between the M<strong>in</strong>istry’s accountability for results and the necessary<br />
autonomy <strong>of</strong> the responsible field managers.<br />
It <strong>in</strong>cludes three components:<br />
An overall document prepared by the central adm<strong>in</strong>istration that complies with <strong>health</strong> objectives<br />
set by the government;<br />
An agreement between the central adm<strong>in</strong>istration and the decentralized services <strong>of</strong> the M<strong>in</strong>istry<br />
<strong>of</strong> Health which covers: general terms, engagement <strong>of</strong> the external services, engagement<br />
<strong>of</strong> the central adm<strong>in</strong>istration and monitor<strong>in</strong>g and evaluation terms;<br />
Performance <strong>in</strong>dicators and control charts.<br />
Results-based budget management is a participatory process <strong>in</strong> which communication<br />
plays an essential <strong>role</strong> and represents its ma<strong>in</strong> strength.<br />
<strong>The</strong> monitor<strong>in</strong>g system is based on two elements: meet<strong>in</strong>gs <strong>of</strong> the monitor<strong>in</strong>g organs<br />
and use <strong>of</strong> support<strong>in</strong>g documents. Organs responsible for monitor<strong>in</strong>g are the orientation<br />
council, which meets once a year; the central committee for guidance, monitor<strong>in</strong>g and<br />
evaluation, which meets twice a year; and the regional committee <strong>of</strong> monitor<strong>in</strong>g and<br />
evaluation, which meets every two months.<br />
2 Ref. Primature, Circulaire n° 12/2001<br />
185
Morocco<br />
<strong>The</strong>re are many support<strong>in</strong>g documents available at the level <strong>of</strong> the decentralized<br />
services, <strong>in</strong>clud<strong>in</strong>g reports on the advancement <strong>of</strong> activities and projects, statistical tables, and<br />
annual activity reports.<br />
Contractual <strong>arrangements</strong> based on cooperative relations<br />
Partnership with nongovernmental organizations<br />
<strong>The</strong> nongovernmental organizations active <strong>in</strong> the field <strong>of</strong> <strong>health</strong> were created by civil<br />
society <strong>in</strong> an effort to address difficulties <strong>in</strong> <strong>health</strong> care and the emergence <strong>of</strong> chronic diseases,<br />
the costs <strong>of</strong> which are a heavy burden for families <strong>in</strong> the absence <strong>of</strong> social services coverage.<br />
In general, the nongovernmental organizations were created by <strong>health</strong> pr<strong>of</strong>essionals to<br />
mobilize efforts towards a public <strong>health</strong> problem, such as kidney disease, <strong>in</strong>fant diabetes,<br />
<strong>in</strong>fant cancer, AIDS, etc. Sometimes these nongovernmental organizations work <strong>in</strong> the public<br />
hospitals side by side with the pr<strong>of</strong>essionals <strong>of</strong> these <strong>health</strong> <strong>in</strong>stitutions.<br />
<strong>The</strong> efforts <strong>of</strong> nongovernmental organizations <strong>in</strong> these cases are <strong>in</strong>tended to augment the<br />
efforts <strong>of</strong> the State, not to replace them. <strong>The</strong>ir actions <strong>in</strong> general complement each other. <strong>The</strong><br />
public <strong>health</strong> <strong>in</strong>stitutions turn to nongovernmental organizations to carry out different actions,<br />
such as:<br />
Provid<strong>in</strong>g diagnostic and treatment activities: cancer, sexually transmitted <strong>in</strong>fections, heart<br />
disease, kidney disease, diabetes)<br />
Provid<strong>in</strong>g family plann<strong>in</strong>g, such as through supply<strong>in</strong>g contraceptive products, tra<strong>in</strong><strong>in</strong>g <strong>health</strong><br />
pr<strong>of</strong>essionals and counterparts (e.g. on AIDS) and provid<strong>in</strong>g public <strong>in</strong>formation,<br />
education and awareness (trachoma control, etc.).<br />
<strong>The</strong> public contribution to the f<strong>in</strong>anc<strong>in</strong>g <strong>of</strong> <strong>health</strong>-related activities <strong>of</strong> nongovernmental<br />
organizations <strong>in</strong>clude the provision <strong>of</strong> annual subsidies and medical supplies (medic<strong>in</strong>es,<br />
contraceptives, various other supplies), assignment <strong>of</strong> facilities, equipment and <strong>of</strong>fice<br />
furniture, and shar<strong>in</strong>g <strong>of</strong> human resources.<br />
<strong>The</strong> nongovernmental organizations work with the public <strong>health</strong> <strong>in</strong>stitutions. An<br />
agreement is established for this purpose stat<strong>in</strong>g the contribution and engagements <strong>of</strong> both<br />
parties as well as the duration <strong>of</strong> this agreement. However, such agreements usually do not<br />
<strong>in</strong>clude the means and tools necessary to control, monitor and follow up the <strong>in</strong>put <strong>of</strong><br />
nongovernmental organizations.<br />
In 2003y, the Prime M<strong>in</strong>ister issued an Act (no. 7/2003) establish<strong>in</strong>g a new partnership<br />
environment <strong>in</strong>tended to be more flexible and to improve coord<strong>in</strong>ation and control through<br />
use <strong>of</strong> a results-based management framework. Through this Act, the government seeks to<br />
develop new relationships with nongovernmental organizations through the renewed<br />
partnership policy on one hand, aimed at optimiz<strong>in</strong>g the work<strong>in</strong>g environment <strong>of</strong> partners, and<br />
on the other hand, def<strong>in</strong><strong>in</strong>g with precision the <strong>in</strong>tervention framework <strong>in</strong> order to optimize the<br />
use <strong>of</strong> resources, focus the partnerships on needy populations and guarantee transparency.<br />
186
Morocco<br />
Accord<strong>in</strong>g to his Act, each time the State’s contribution is equal or more than 50 000<br />
Moroccan dirhams per project, both parties should sign an agreement similar to the model<br />
attached to the Act. <strong>The</strong> acquisition <strong>of</strong> public f<strong>in</strong>anc<strong>in</strong>g is conditional upon the compliance <strong>of</strong><br />
the planned activity or project with the purpose for which the nongovernmental organization<br />
was created and priority actions <strong>of</strong> the government, particularly, combat<strong>in</strong>g poverty, assist<strong>in</strong>g<br />
needy women and <strong>in</strong>fants and develop<strong>in</strong>g <strong>in</strong>frastructure and basic social services.<br />
Partnership with <strong>in</strong>ternational organizations<br />
With<strong>in</strong> the framework <strong>of</strong> their cooperation programmes with the Government <strong>of</strong><br />
Morocco, <strong>in</strong>ternational partners also work with national organizations carry out a number <strong>of</strong><br />
activities.<br />
United Nations agencies<br />
UNDP, UNFP, WHO: family plann<strong>in</strong>g actions, maternal and child <strong>health</strong> and prevention<br />
<strong>of</strong> HIV/AIDS and sexually transmitted <strong>in</strong>fections<br />
UNAIDS: prevention and control <strong>of</strong> HIV/AIDS<br />
UNICEF: maternal and child <strong>health</strong>, <strong>in</strong>formation and awareness, especially for the poor<br />
or those <strong>in</strong> remote areas, and prevention <strong>of</strong> iod<strong>in</strong>e deficiency<br />
Bilateral cooperation services<br />
Research activities<br />
Family plann<strong>in</strong>g services, HIV/AIDS and sexually transmitted disease prevention,<br />
eradication <strong>of</strong> trachoma<br />
Diagnosis and treatment <strong>of</strong> certa<strong>in</strong> diseases<br />
Tra<strong>in</strong><strong>in</strong>g <strong>of</strong> <strong>health</strong> pr<strong>of</strong>essionals<br />
Public education, <strong>in</strong>formation and awareness.<br />
<strong>The</strong> f<strong>in</strong>ancial contributions <strong>of</strong> the <strong>in</strong>ternational organizations may be <strong>in</strong> the form <strong>of</strong><br />
f<strong>in</strong>ancial grants, medical supplies and equipment, <strong>of</strong>fice supplies, transportation means and<br />
logistic support.<br />
F<strong>in</strong>anc<strong>in</strong>g is usually acquired on the basis <strong>of</strong> a project f<strong>in</strong>anc<strong>in</strong>g request that is<br />
submitted by the national organization and that meets the national public <strong>health</strong> objectives and<br />
the orientation <strong>of</strong> the cooperative programme agreed upon between the <strong>in</strong>ternational<br />
organization and the M<strong>in</strong>istry <strong>of</strong> Health. <strong>The</strong> <strong>contractual</strong> <strong>arrangements</strong> stipulate requirements<br />
for a monitor<strong>in</strong>g and evaluation process.<br />
Partnership with local collectives<br />
S<strong>in</strong>ce the early 1990s, a number <strong>of</strong> partnerships with local collectives have been formed<br />
through the establishment <strong>of</strong> multi-year agreements (from 1 to 5 year period).<br />
In 1990, the budgets related to <strong>health</strong> <strong>in</strong>vestment projects were transferred to local<br />
collectives. <strong>The</strong> amount transferred, about 118 621 510, covers two components: projects<br />
meet<strong>in</strong>g local needs as planned by the M<strong>in</strong>istry, and a special programme <strong>of</strong> rehabilitation and<br />
equipment <strong>of</strong> the Ibn Rochd University Hospital Centre <strong>in</strong> Casablanca.<br />
187
Morocco<br />
In 1997, a sem<strong>in</strong>ar on cooperative development with local collectives recommended, as<br />
a <strong>health</strong> measure, the establishment <strong>of</strong> a partnership with local collectives <strong>in</strong> the fields <strong>of</strong><br />
construction, equipment and ma<strong>in</strong>tenance <strong>of</strong> <strong>health</strong> care facilities. Currently, partnerships with<br />
local collectives cover:<br />
Health care facilities construction: hospitals, <strong>health</strong> centres<br />
Support for basic <strong>health</strong> care services;<br />
Purchase <strong>of</strong> equipment and transportation means;<br />
Provision <strong>of</strong> medic<strong>in</strong>es and medical goods;<br />
Part-time assignment <strong>of</strong> <strong>health</strong> workers.<br />
<strong>The</strong> partnerships are <strong>in</strong> general def<strong>in</strong>ed by the agreements. In the absence <strong>of</strong> monitor<strong>in</strong>g<br />
and evaluation tools, it is difficult to evaluate the work <strong>of</strong> the collectives with<strong>in</strong> the<br />
framework <strong>of</strong> these agreements.<br />
Some organization and improvement perspectives for partnership with local collectives<br />
are justified by:<br />
<strong>The</strong> government will<strong>in</strong>gness to carry out a proximity policy <strong>in</strong> the context <strong>of</strong> decentralization;<br />
<strong>The</strong> government statement regard<strong>in</strong>g the opportunities to create employment at the local level;<br />
<strong>The</strong> will<strong>in</strong>gness <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health to strengthen partnership with local collectives <strong>in</strong><br />
order to better respond to the population <strong>health</strong> needs;<br />
<strong>The</strong> extension <strong>of</strong> the local collectives competencies <strong>in</strong> accordance with the decentralization law.<br />
With the launch <strong>of</strong> public spend<strong>in</strong>g reform, the Government <strong>of</strong> Morocco announced the<br />
open<strong>in</strong>g towards form<strong>in</strong>g strategic partnerships seek<strong>in</strong>g improved efficacy <strong>of</strong> public <strong>sector</strong><br />
action. This reform implies four components: globalization <strong>of</strong> the allocated budget, as a prerequisite;<br />
contract<strong>in</strong>g; partnership; and delegation <strong>of</strong> responsibility <strong>in</strong> favour <strong>of</strong> regulation.<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health was among the first <strong>sector</strong>s to adopt this process.<br />
Although the legal context and political will<strong>in</strong>gness exist, the collective partnership<br />
system suffers from lack <strong>of</strong> technical supervision and legal tools. Before they are<br />
<strong>in</strong>stitutionalized through legislation, more organizational experience with such agreements is<br />
needed. Such organizational learn<strong>in</strong>g will entail its share <strong>of</strong> problems, and will also require a<br />
new attitude towards the different partners active <strong>in</strong> the field <strong>of</strong> <strong>health</strong>, <strong>in</strong>clud<strong>in</strong>g the private<br />
<strong>sector</strong>.<br />
Case study 1: Provid<strong>in</strong>g care for end-stage renal disease through leas<strong>in</strong>g <strong>of</strong> equipment<br />
and supplies<br />
End-stage renal (kidney) disease is considered a public <strong>health</strong> problem <strong>in</strong> Morocco. <strong>The</strong><br />
grow<strong>in</strong>g number <strong>of</strong> cases requir<strong>in</strong>g treatment, compounded by high treatment costs, has made<br />
renal disease a priority on the agenda <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health.<br />
<strong>The</strong> <strong>in</strong>cidence <strong>of</strong> end-stage renal disease <strong>in</strong> Morocco is about 3000 new cases per year.<br />
<strong>The</strong> demographic and epidemiological transition under way <strong>in</strong> the country predicts a<br />
progressive <strong>in</strong>crease <strong>in</strong> the number <strong>of</strong> cases requir<strong>in</strong>g treatment.<br />
188
Morocco<br />
<strong>The</strong> number <strong>of</strong> patients currently receiv<strong>in</strong>g treatment is about 3500, <strong>of</strong> which 1420 are<br />
<strong>in</strong> the public <strong>sector</strong>. Another 2135 patients are <strong>in</strong> need <strong>of</strong> treatment and are on the wait<strong>in</strong>g lists<br />
<strong>of</strong> public haemodialysis centres.<br />
Treatment for end-stage renal disease is provided <strong>in</strong> two ways: kidney transplantation<br />
and haemodialysis. In Morocco, haemodialysis constitutes the pr<strong>in</strong>cipal treatment, with<br />
kidney transplantation limited to a few cases per year. Morocco has about 95 haemodialysis<br />
centres, <strong>of</strong> which 28 are <strong>in</strong> the public <strong>sector</strong>. <strong>The</strong> equipment <strong>of</strong> these centres <strong>in</strong>cludes 1023<br />
artificial kidneys, <strong>of</strong> which 351 are <strong>in</strong> the public <strong>sector</strong>.<br />
A haemodialysis generator cost between US$ 12 500 and 16 500. <strong>The</strong> water treatment<br />
unit costs about US$ 4000. Treatment for end-stage renal disease <strong>in</strong> a hospital costs about<br />
3<br />
US$ 187 20TP PT. Care for the 2135 patients wait<strong>in</strong>g treatment will cost, as a recurr<strong>in</strong>g cost,<br />
4<br />
US$ 40 000 000 a year plus an <strong>in</strong>itial <strong>in</strong>vestment <strong>of</strong> US$ 6 450 000TP PT.<br />
<strong>The</strong> high cost <strong>of</strong> <strong>in</strong>frastructure and treatment for renal disease makes it difficult to<br />
respond to the expressed need with<strong>in</strong> a context <strong>of</strong> competitive priorities and budgetary<br />
constra<strong>in</strong>t.<br />
In order to provide haemodialysis services required by patients with end-stage renal<br />
5<br />
disease two different forms <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> were consideredTP PT:<br />
1) Contract<strong>in</strong>g for support from non-pr<strong>of</strong>it associations<br />
This form <strong>of</strong> contract<strong>in</strong>g was to support treatment provision to end-stage renal disease<br />
patients. <strong>The</strong> partnership with the non-pr<strong>of</strong>it associations is organized as follows:<br />
<strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Health assigns staff to the centre and covers some fixed charges (water,<br />
electricity, etc.), blood products and some medic<strong>in</strong>es and pharmacy products (hepar<strong>in</strong>).<br />
<strong>The</strong> associations cover expenses related to equipment, medic<strong>in</strong>es and consumables, <strong>in</strong>clud<strong>in</strong>g<br />
equipment ma<strong>in</strong>tenance.<br />
<strong>The</strong> majority <strong>of</strong> patients contribute to their care expenses (200 to 500 Moroccan dirhams per<br />
session, depend<strong>in</strong>g on the case).<br />
This arrangement depends largely on the availability <strong>of</strong> an association will<strong>in</strong>g to<br />
undertake the <strong>in</strong>vestment. <strong>The</strong> number <strong>of</strong> beneficiaries <strong>of</strong> care is <strong>of</strong>ten limited, and does not<br />
<strong>in</strong>clude all patients <strong>in</strong> need <strong>of</strong> treatment. This contract<strong>in</strong>g option basically amounts to<br />
participation <strong>in</strong> end-stage renal disease care, and is not susta<strong>in</strong>able.<br />
2) Contract<strong>in</strong>g for the lease <strong>of</strong> equipment and supplies<br />
3 Etude sur l’analyse des coûts par activité à l’hôpital d’Agadir, PFGSS, DHSA, M<strong>in</strong>istère de la Santé du Maroc.<br />
4 Cost <strong>of</strong> 336 generators and 50 water treatment units.<br />
5<br />
<strong>The</strong> care strategy regard<strong>in</strong>g f<strong>in</strong>al kidney deficiency <strong>in</strong>cludes also prevention and kidney transplantation that are not<br />
discussed <strong>in</strong> this paper.<br />
189
Morocco<br />
S<strong>in</strong>ce the <strong>health</strong> authorities have to respond to the expressed need for f<strong>in</strong>al kidney<br />
deficiency care, which is cumulat<strong>in</strong>g <strong>in</strong> different levels, and to supervise the different<br />
<strong>in</strong>terventions <strong>in</strong> this field, the M<strong>in</strong>istry <strong>of</strong> Health launched a leas<strong>in</strong>g bid with the private <strong>sector</strong><br />
to provide care to patients. This orientation is justified by the difficulty to mobilize together<br />
human, f<strong>in</strong>ancial and logistic resources (supply and ma<strong>in</strong>tenance) and <strong>in</strong> a recurrent way<br />
throughout the national territory. Comply<strong>in</strong>g with the public–private <strong>contractual</strong><br />
<strong>arrangements</strong>, the private organization is responsible for supply<strong>in</strong>g 240 haemodialysis<br />
generators (artificial kidneys), 34 water treatment units and 225 000 haemodialysis kits per<br />
year for 32 centres at the national level.<br />
<strong>The</strong> contract is between the M<strong>in</strong>istry <strong>of</strong> Health (buyer) and a private organization<br />
specialized <strong>in</strong> haemodialysis equipment (supplier), and deals with the lease <strong>of</strong> haemodialysis<br />
equipment <strong>in</strong>clud<strong>in</strong>g consumable products (kits). <strong>The</strong> contract was established as a five-year<br />
contract. <strong>The</strong> contract is f<strong>in</strong>anced through the general budget <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health, for<br />
about US$ 5 000 000 per year.<br />
<strong>The</strong> supplier is committed to furnish 32 haemodialysis centres and to: <strong>in</strong>stall, operate<br />
and test the new haemodialysis equipment and ensure that this material is recently<br />
manufactured, with attached guarantee certificates delivered by the manufacturer; furnish<br />
consumable haemodialysis products (kits); and provide preventive and curative ma<strong>in</strong>tenance<br />
<strong>of</strong> the haemodialysis equipment, <strong>in</strong>clud<strong>in</strong>g tra<strong>in</strong><strong>in</strong>g <strong>of</strong> personnel on this equipment.<br />
Specifically, the supplier must provide the follow<strong>in</strong>g services:<br />
delivery <strong>of</strong> the rented operational equipment, <strong>in</strong>clud<strong>in</strong>g <strong>in</strong>stallation, utilization and test<strong>in</strong>g at<br />
each haemodialysis centre <strong>in</strong>dicated on the list <strong>of</strong> centres;<br />
employment <strong>of</strong> all the material and human resources required to carry out the contract with<strong>in</strong><br />
the deadl<strong>in</strong>e set for the <strong>in</strong>stallation;<br />
appo<strong>in</strong>tment <strong>of</strong> a competent eng<strong>in</strong>eer to supervise the <strong>in</strong>stallation and the ma<strong>in</strong>tenance <strong>of</strong><br />
equipment;<br />
supply <strong>of</strong> consumable haemodialysis products (kits) <strong>in</strong> compliance with the technical and<br />
quantity specifications described <strong>in</strong> the estimated price table, <strong>in</strong>cluded <strong>in</strong> the contract, to<br />
the designated centres for one year, renewable and valid dur<strong>in</strong>g a 5-year period;<br />
regular preventive and curative ma<strong>in</strong>tenance <strong>of</strong> the equipment <strong>in</strong>stalled at each haemodialysis<br />
centre dur<strong>in</strong>g the contact<strong>in</strong>g period, <strong>in</strong>clud<strong>in</strong>g the supply <strong>of</strong> all labour and parts necessary<br />
to repair equipment;<br />
tra<strong>in</strong><strong>in</strong>g <strong>of</strong> 4 persons <strong>in</strong> each <strong>of</strong> the haemodialysis centres for at least 5 days;<br />
updat<strong>in</strong>g <strong>of</strong> the haemodialysis equipment and consumable products <strong>in</strong> l<strong>in</strong>e with technological<br />
progress <strong>in</strong> this field.<br />
<strong>The</strong> buyer (M<strong>in</strong>istry <strong>of</strong> Health) is obligated to take all appropriate measures to enable<br />
the supplier carry out the required services <strong>in</strong> terms <strong>of</strong> access and storage <strong>of</strong> materials and<br />
tools and supply <strong>of</strong> water and electricity for the mach<strong>in</strong>ery. <strong>The</strong> M<strong>in</strong>istry will put at the<br />
disposal <strong>of</strong> the contract beneficiary:<br />
technical data and <strong>in</strong>formation needed to ensure the success <strong>of</strong> the implementation <strong>of</strong> the<br />
contract requirements;<br />
190
Morocco<br />
facilities and the technical <strong>in</strong>stallations to realize the commitments <strong>in</strong> the contract;<br />
water and electricity supply to the haemodialysis equipment; however, water and electricity fees<br />
are at the expense <strong>of</strong> the supplier.<br />
<strong>The</strong> advantage <strong>of</strong> this form <strong>of</strong> <strong>contractual</strong> arrangement is that it delegates responsibility<br />
for supply and ma<strong>in</strong>tenance to the private <strong>sector</strong>, while enabl<strong>in</strong>g the <strong>health</strong> adm<strong>in</strong>istration to<br />
focus on the regulatory and control function. It also helps ensure appropriate timel<strong>in</strong>ess and<br />
efficiency <strong>of</strong> treatment. As well, this experience shows that the private <strong>sector</strong> can mobilize its<br />
experience and technology <strong>in</strong> order to <strong>of</strong>fer solutions to specific <strong>health</strong> problems.<br />
6<br />
Case study 2: Subcontract<strong>in</strong>g support services for SEGMATP PT hospital centres<br />
Hospitals face significant pressure to undertake a wide range <strong>of</strong> activities that they are<br />
neither ready nor equipped to carry out. In 1996, outsourc<strong>in</strong>g <strong>of</strong> support services by the<br />
SEGMA hospital centres started with the subcontract<strong>in</strong>g out <strong>of</strong> clean<strong>in</strong>g services for<br />
emergency facilities at Al Hoceima hospital. S<strong>in</strong>ce then, the experience has extended to other<br />
fields such as cater<strong>in</strong>g, groundskeep<strong>in</strong>g and security services and to other hospital centres (41<br />
out <strong>of</strong> 46 SEGMA hospitals). <strong>The</strong>se hospitals allocate between 20% and 40% <strong>of</strong> their<br />
function<strong>in</strong>g budgets to subcontract support services.<br />
Accord<strong>in</strong>g to the results <strong>of</strong> a survey (Annex 2) conducted among the 46 hospitals<br />
currently subcontract<strong>in</strong>g out support services, the subcontract<strong>in</strong>g experience has contributed<br />
to:<br />
improvement <strong>in</strong> the quality and efficacy <strong>of</strong> services;<br />
improvement <strong>of</strong> the stand<strong>in</strong>g <strong>of</strong> the hospital centre;<br />
improvement <strong>of</strong> the hospitalization conditions <strong>of</strong> the patients;<br />
<strong>The</strong> adjustment <strong>of</strong> the deficit <strong>in</strong> personnel or its reassignment;<br />
resolution <strong>of</strong> some personnel management problems fac<strong>in</strong>g the adm<strong>in</strong>istration;<br />
better control <strong>of</strong> the costs related to these activities;<br />
improves control <strong>of</strong> support services;<br />
reduction <strong>of</strong> costs due to the competitive nature <strong>of</strong> the bidd<strong>in</strong>g process.<br />
<strong>The</strong> constra<strong>in</strong>ts reported by survey respondents are related to legal, f<strong>in</strong>ancial and<br />
management aspects <strong>of</strong> subcontract<strong>in</strong>g. <strong>The</strong> pr<strong>in</strong>cipal constra<strong>in</strong>ts are:<br />
F<strong>in</strong>ancial pressures that can result <strong>in</strong> hospitals choos<strong>in</strong>g companies on the basis <strong>of</strong> cost rather<br />
than quality;<br />
Absence <strong>of</strong> reference norms for quality control;<br />
Absence <strong>of</strong> clear procedures to evaluate the provided services;<br />
Absence <strong>of</strong> experience among the agents <strong>in</strong> charge <strong>of</strong> monitor<strong>in</strong>g, implementation and control<br />
<strong>of</strong> the conformity <strong>of</strong> the services and the products provided by the companies;<br />
6 Service d’Etat Gérés de Manière Autonome<br />
191
Morocco<br />
Employment by the companies <strong>of</strong> unqualified and underpaid personnel, which affects pr<strong>of</strong>its<br />
and competitiveness.<br />
Suggestions proposed by the contract managers <strong>in</strong>cluded the follow<strong>in</strong>g:<br />
Provid<strong>in</strong>g additional f<strong>in</strong>ancial resources;<br />
Ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g and extend<strong>in</strong>g the application <strong>of</strong> subcontract<strong>in</strong>g to other adm<strong>in</strong>istrative activities<br />
and to other types <strong>of</strong> support services, such as radiology, laboratory, etc.<br />
Dissem<strong>in</strong>at<strong>in</strong>g standard means and tools for control, monitor<strong>in</strong>g and evaluation;<br />
Develop<strong>in</strong>g a manual for management <strong>of</strong> subcontracted activities;<br />
Evaluat<strong>in</strong>g the experience;<br />
Improv<strong>in</strong>g supervision <strong>of</strong> the different stakeholders by the M<strong>in</strong>istry <strong>of</strong> Health;<br />
Transfer <strong>of</strong> activities that the hospital’s resources cannot cover to the central adm<strong>in</strong>istration.<br />
Despite the relative limited experience <strong>in</strong> hospital subcontract<strong>in</strong>g, the majority <strong>of</strong><br />
managers regarded it as an opportunity to overcome the difficulties caused by the demand for<br />
better <strong>health</strong> care quality and the frequent turnover <strong>of</strong> qualified personnel. Indeed, the<br />
majority also requested its extension to other activities. However, this would require the<br />
adoption <strong>of</strong> a systematic approach and the elaboration <strong>of</strong> clear contract<strong>in</strong>g strategy.<br />
CONCLUSIONS AND RECOMMENDATIONS<br />
Contractual <strong>arrangements</strong> represent an important phenomenon <strong>in</strong> the area <strong>of</strong> <strong>health</strong><br />
services organization and management. Though the experience <strong>of</strong> Morocco is recent, this<br />
phenomenon is a promis<strong>in</strong>g means for improv<strong>in</strong>g <strong>health</strong> system performance while<br />
ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g the regulatory position <strong>of</strong> the State with regard to the <strong>health</strong> system.<br />
<strong>The</strong> contributions <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> to the <strong>health</strong> system can be analysed at<br />
different levels.<br />
Stewardship level<br />
<strong>The</strong> contract<strong>in</strong>g <strong>arrangements</strong> constitute an <strong>in</strong>strument for implement<strong>in</strong>g <strong>health</strong> policy<br />
and a means for regulat<strong>in</strong>g the <strong>health</strong> system. As a political <strong>in</strong>strument, the contract<strong>in</strong>g<br />
<strong>arrangements</strong> enable the State to recover a measure <strong>of</strong> efficacy and competitiveness lost due to<br />
bureaucracy. Through contract<strong>in</strong>g <strong>arrangements</strong>, the State:<br />
acknowledges the <strong>role</strong> <strong>of</strong> the partners <strong>in</strong> the <strong>health</strong> system performance;<br />
delegates responsibility directly to the different actors <strong>of</strong> the <strong>health</strong> system,<br />
becomes open to potential choices, thereby allow<strong>in</strong>g better responsive to <strong>health</strong> problems;<br />
develops a sense <strong>of</strong> obligation towards results.<br />
As a regulatory means, the <strong>contractual</strong> <strong>arrangements</strong> enable the State to strengthen its<br />
position as the steward <strong>of</strong> stewards and to guarantee the general <strong>in</strong>terest by establish<strong>in</strong>g rules<br />
for <strong>contractual</strong> <strong>arrangements</strong> (legal context). <strong>The</strong>se rules must permanently seek the added<br />
social value and provide the opportunity for pr<strong>of</strong>it.<br />
Health management organization level<br />
192
Morocco<br />
Evaluation <strong>of</strong> the subcontract<strong>in</strong>g experience and the description <strong>of</strong> the new contract<strong>in</strong>g<br />
networks constituted by the plann<strong>in</strong>g contract and the programme budget yielded two<br />
important observations:<br />
Such <strong>arrangements</strong> respond to an evident need <strong>of</strong> the managers. <strong>The</strong>y serve as a means for<br />
hospitals to express their needs and to compel the State to consider them as full partners.<br />
<strong>The</strong> open<strong>in</strong>g <strong>of</strong> the private <strong>sector</strong> through subcontract<strong>in</strong>g was not technically supervised and has<br />
not been accompanied by associated change <strong>in</strong> management style or attitude.<br />
Care services level<br />
At this level, the State rema<strong>in</strong>s hesitant to outsource services. This may be expla<strong>in</strong>ed by<br />
the ethical and social implications <strong>of</strong> <strong>health</strong> care services and the contrast between these<br />
implications and the pr<strong>of</strong>it-mak<strong>in</strong>g ethos. It is likely that <strong>in</strong> the future the State will have no<br />
choice but to open its <strong>health</strong> system to the private <strong>sector</strong>, as the State will not be able to<br />
respond to all resource deficits and reform needs with its own resources. To ensure that this<br />
open<strong>in</strong>g is carefully considered and planned rather than imposed ad hoc by external forces, it<br />
will be necessary to develop a clear policy and long-term vision that clarifies the<br />
responsibility <strong>of</strong> the private <strong>sector</strong> and civil society, and that puts the State <strong>in</strong> a position to<br />
regulate <strong>contractual</strong> <strong>arrangements</strong>. Such a policy will help ensure that <strong>health</strong> rema<strong>in</strong>s <strong>in</strong> the<br />
middle <strong>of</strong> political, economic and social <strong>in</strong>terests.<br />
Contract<strong>in</strong>g <strong>arrangements</strong> appear to be an opportunity to strengthen <strong>health</strong> systems <strong>in</strong><br />
order to improve their performance. However, certa<strong>in</strong> prerequisites are necessary for their<br />
implementation:<br />
<strong>The</strong> commitment to a clear contract<strong>in</strong>g policy that acknowledges the <strong>role</strong> <strong>of</strong> actors other than<br />
the public organizations <strong>in</strong> the implementation <strong>of</strong> the <strong>health</strong> objectives and that def<strong>in</strong>es the<br />
legal context <strong>of</strong> the <strong>health</strong> <strong>contractual</strong> <strong>arrangements</strong> and the means <strong>of</strong> control necessary to<br />
protect the quest for added social value and the opportunity for pr<strong>of</strong>it;<br />
<strong>The</strong> exploration <strong>of</strong> the potentials <strong>of</strong>fered by the private <strong>sector</strong> with regard to the <strong>health</strong> problems<br />
encountered;<br />
<strong>The</strong> development <strong>of</strong> transparency and communication and coord<strong>in</strong>ation tools suitable to respond<br />
to the requirements <strong>of</strong> the contract<strong>in</strong>g parties;<br />
<strong>The</strong> presence <strong>of</strong> regulatory measures enabl<strong>in</strong>g public organizations to successfully open up to<br />
the private <strong>sector</strong> with no negative effects on <strong>health</strong>.<br />
193
Contract Purchaser <strong>of</strong><br />
service<br />
(hospital)<br />
Supplier<br />
(private<br />
company)<br />
Object <strong>of</strong><br />
the<br />
contract<br />
Morocco<br />
Annex 1<br />
Questionnaire for use <strong>in</strong> the hospital survey<br />
Form and<br />
length <strong>of</strong><br />
contract<br />
Questions about the appreciation <strong>of</strong> the experience:<br />
Inputs <strong>of</strong> subcontract<strong>in</strong>g for the function<strong>in</strong>g <strong>of</strong> the hospital<br />
Limits and constra<strong>in</strong>ts <strong>of</strong> subcontract<strong>in</strong>g<br />
Suggestions.<br />
Types <strong>of</strong><br />
services<br />
provided<br />
Value <strong>of</strong> contract<br />
/function<strong>in</strong>g budget ratio<br />
Payment procedure<br />
Payment<br />
frequency<br />
Voucher<br />
system<br />
Monitor<strong>in</strong>g and evaluation<br />
process
Morocco<br />
Annex 2<br />
EVALUATION OF THE EXPERIENCE OF SUBCONTRACTING BY THE MANAGERS OF THE SEGMA HOSPITAL CENTRES<br />
Public<br />
hospital<br />
centre (PHC)<br />
Pr<strong>in</strong>cipal <strong>in</strong>puts Limits and constra<strong>in</strong>ts Suggestions<br />
Ouarzazate Positive quality improvement <strong>of</strong> services provided by<br />
PHC, reassignment <strong>of</strong> personnel<br />
Inezgane Quality improvement <strong>of</strong> services, clients and personnel<br />
satisfaction, provid<strong>in</strong>g additional technical material,<br />
compensate the deficit <strong>in</strong> personnel, reassignment <strong>of</strong><br />
personnel, considered as creat<strong>in</strong>g jobs along the<br />
hospital reform, Availability <strong>of</strong> services 6 days a week<br />
Taroudant Satisfaction <strong>of</strong> personnel, respect<strong>in</strong>g the deadl<strong>in</strong>e to<br />
provide services, availability 24/24, stead<strong>in</strong>ess <strong>of</strong><br />
agents <strong>in</strong> charge <strong>of</strong> subcontracted activities, recover<strong>in</strong>g<br />
and reassign<strong>in</strong>g the personnel<br />
Subcontract<strong>in</strong>g constitutes an important burden on the<br />
budget, supervision needs and selection <strong>of</strong> companies<br />
tak<strong>in</strong>g <strong>in</strong>to account hospital special status<br />
Absence <strong>of</strong> reference norms, to control the quality <strong>of</strong><br />
the products <strong>in</strong> use, lack <strong>of</strong> qualified members <strong>of</strong> the<br />
committee <strong>in</strong> charge <strong>of</strong> monitor<strong>in</strong>g, execution, control<br />
<strong>of</strong> products conformity, absence <strong>of</strong> clear procedures to<br />
evaluate the services, lack <strong>of</strong> pr<strong>of</strong>essionalism <strong>of</strong> the<br />
companies <strong>in</strong> hospital lodg<strong>in</strong>g, <strong>in</strong>stability <strong>of</strong> their<br />
underpaid personnel<br />
Laundry does not figure among the services considered<br />
for a bid, lack <strong>of</strong> pr<strong>of</strong>essionalism <strong>of</strong> some companies,<br />
hir<strong>in</strong>g personnel less qualified and underpaid, which<br />
could harm a loyal competitiveness<br />
Tiznit Improvement <strong>of</strong> lodg<strong>in</strong>g conditions <strong>in</strong> hospital Delay <strong>in</strong> budget allocation leads to a delay <strong>in</strong> the<br />
approval <strong>of</strong> bids, payment for provided services<br />
depends on the date <strong>of</strong> the approval<br />
El Kalaa Quality improvement and reassignment <strong>of</strong> personnel Pr<strong>of</strong>its not very important, subsidies deficient,<br />
subcontract<strong>in</strong>g rema<strong>in</strong>s limited to some provided<br />
services<br />
195<br />
Ma<strong>in</strong>ta<strong>in</strong> the subcontract<strong>in</strong>g activities<br />
Implication <strong>of</strong> managers <strong>in</strong> the control<br />
<strong>of</strong> services delivery, availability <strong>of</strong><br />
qualified structures <strong>of</strong> control, and <strong>of</strong><br />
the evaluation norms and means,<br />
elaboration management manual for<br />
subcontracted activities, requirement<br />
<strong>of</strong> the payment statement, elaborate<br />
legislation requir<strong>in</strong>g a m<strong>in</strong>imum <strong>of</strong><br />
pr<strong>of</strong>essionalism <strong>in</strong> subcontract<strong>in</strong>g,<br />
extend subcontract<strong>in</strong>g to other<br />
adm<strong>in</strong>istrative activities<br />
Recommend laundry services to be<br />
subcontracted through a bid, <strong>in</strong>volve<br />
labor <strong>in</strong>spection to control<br />
subcontracted companies around the<br />
<strong>health</strong> structures<br />
Extend the application to other fields:<br />
radiology and laboratory
Essaouira Better provided services, reassignment <strong>of</strong> assist<strong>in</strong>g<br />
personnel and agents, satisfaction <strong>of</strong> patients and<br />
visitors<br />
Morocco<br />
Budget <strong>in</strong>sufficient, competitors are limited Extend the application to other fields:<br />
radiology and laboratory, elaboration<br />
<strong>of</strong> charges booklet centralized type,<br />
related to different services provided<br />
El Jadida No comment No comment No suggestions<br />
Safi Disengage from logistic functions, improvement <strong>of</strong><br />
quality services help<strong>in</strong>g clear the hospital image, settle<br />
the personnel deficiency , reassignment <strong>of</strong> personnel,<br />
master <strong>of</strong> costs management related to these activities<br />
Khouribga Settlement <strong>of</strong> lack <strong>of</strong> human resources, no assignment<br />
<strong>of</strong> certa<strong>in</strong> categories, no replacement <strong>of</strong> retir<strong>in</strong>g people,<br />
discipl<strong>in</strong>e, punctuality and quality <strong>of</strong> provided services<br />
are satisfactory<br />
Settat Improvement <strong>of</strong> services quality, concentration <strong>of</strong><br />
managers on other less important activities<br />
Incidence <strong>of</strong> generated costs on the budget, lack <strong>of</strong><br />
society pr<strong>of</strong>essionalism, to turn to qualified companies<br />
is not covered by the budget<br />
Subcontract<strong>in</strong>g constitutes an important burden on the<br />
budget: 50% (lack <strong>of</strong> f<strong>in</strong>ancial resources) outsourc<strong>in</strong>g<br />
groundskeep<strong>in</strong>g is not pr<strong>of</strong>itable, reassignment by the<br />
organization <strong>of</strong> unqualified personnel<br />
Activities represent an important part <strong>in</strong> budget<strong>in</strong>g<br />
between 10% and 23%<br />
Boulemane No comment No comment No comments<br />
Sefrou Subcontract<strong>in</strong>g allows the satisfaction <strong>of</strong> hospital<br />
resources deficiency, ensure the cont<strong>in</strong>uity and<br />
durability <strong>of</strong> permanent services, guarantee the efficacy<br />
and efficiency <strong>of</strong> provided services<br />
Delay <strong>of</strong> budget approval <strong>in</strong>fluences the start <strong>of</strong><br />
provid<strong>in</strong>g services and the execution rate <strong>in</strong> regards to<br />
the amounts <strong>of</strong> the bids<br />
Kénitra No comment No comment No comments<br />
Sidi Kacem Improvement <strong>of</strong> subcontract<strong>in</strong>g provided services,<br />
settle the lack <strong>of</strong> personnel<br />
Competitiveness <strong>of</strong> small and large organizations <strong>in</strong><br />
subcontract<strong>in</strong>g field<br />
196<br />
Increase budget allocated to hospitals<br />
Encourage subcontract<strong>in</strong>g <strong>in</strong> all<br />
assistance activities, standardize the<br />
typical charges booklets, <strong>in</strong>ject<br />
f<strong>in</strong>ancial resources, standardize the<br />
monitor<strong>in</strong>g and control tools<br />
Review the award<strong>in</strong>g procedures <strong>of</strong><br />
the bids <strong>in</strong> order to proceed to their<br />
approval before the budget allocation<br />
Directorate <strong>of</strong> Hospitals and<br />
ambulatory care should provide a list<br />
<strong>of</strong> organizations that did not fulfil their<br />
engagements
Chefchaouen Reassignment <strong>of</strong> agents, positive impact <strong>of</strong> provided<br />
services on the improvement <strong>of</strong> the general function<strong>in</strong>g<br />
Larache Improvement <strong>of</strong> services quality, efficacy control, focus<br />
the efforts on the hospital mission<br />
Tanger Service quality, settlement <strong>of</strong> the problem <strong>of</strong> lack <strong>of</strong><br />
personnel, disengage the adm<strong>in</strong>istration from certa<strong>in</strong><br />
problems related to personnel<br />
Tétouan Improvement <strong>of</strong> the image <strong>of</strong> PHC respond<strong>in</strong>g to<br />
<strong>in</strong>ternal function<strong>in</strong>g needs better conditions, focus on<br />
actors <strong>of</strong> PHC, improvement <strong>of</strong> reception conditions,<br />
work frame, optimize the resources<br />
Errachidia Improvement <strong>of</strong> provided services quality, satisfaction<br />
<strong>of</strong> <strong>in</strong>ternal and external clients, reassignment <strong>of</strong><br />
hospital agents to other activities, good image <strong>of</strong><br />
hospital<br />
Morocco<br />
Limited budget<strong>in</strong>g does not allow regular and<br />
satisfactory subcontract<strong>in</strong>g, tra<strong>in</strong><strong>in</strong>g, competencies and<br />
pr<strong>of</strong>iles <strong>of</strong> agents reassigned by the organizations,<br />
rema<strong>in</strong> <strong>in</strong>appropriate, low salaries to be reviewed<br />
197<br />
Increase <strong>of</strong> subsidies <strong>in</strong> order to<br />
subcontract other activities<br />
F<strong>in</strong>ancial limits Extend the experience to cater<strong>in</strong>g<br />
biomedical ma<strong>in</strong>tenance, etc.<br />
Budget<strong>in</strong>g constra<strong>in</strong>ts do not allow the choice <strong>of</strong><br />
qualified organizations, the pr<strong>of</strong>essional secret is not<br />
protected, and the personnel representative <strong>in</strong>stitutions<br />
protest aga<strong>in</strong>st the subcontract<strong>in</strong>g<br />
No respect <strong>of</strong> labour regulations, lack <strong>of</strong> personnel<br />
tra<strong>in</strong><strong>in</strong>g (hospital wastes, nosocomial <strong>in</strong>fections) budget<br />
limitations, high water consumption, delay <strong>in</strong> start<strong>in</strong>g<br />
work<br />
Subsidies do not allow engagement <strong>of</strong> perform<strong>in</strong>g<br />
organizations, remoteness <strong>of</strong> the prov<strong>in</strong>ce, and<br />
<strong>in</strong>existence <strong>of</strong> local organizations, lack <strong>of</strong> regulations<br />
regard<strong>in</strong>g the garden<strong>in</strong>g function, cater<strong>in</strong>g takes more<br />
than 22% <strong>of</strong> budget<strong>in</strong>g<br />
Ifrane No comments No comment No suggestions<br />
Khénifra Personnel pr<strong>of</strong>it, ease the procedures, improvement <strong>of</strong><br />
provided services quality, acquirement <strong>of</strong> good<br />
experience related to subcontract<strong>in</strong>g<br />
Al Hoceima Permanent availability <strong>of</strong> agents at the level <strong>of</strong> services,<br />
execution <strong>of</strong> works <strong>in</strong> and out <strong>of</strong> the bid<br />
Budget<strong>in</strong>g constra<strong>in</strong>ts, complexity <strong>of</strong> the commitments<br />
<strong>in</strong> the charges booklets, lack <strong>of</strong> expertise <strong>of</strong> the<br />
providers and monitor<strong>in</strong>g agents<br />
Limited allocated budget thus the quality rema<strong>in</strong>s low,<br />
execution <strong>of</strong> works out <strong>of</strong> the bid causes some conflicts<br />
Taza No comments No comments No comments<br />
Intervene <strong>in</strong> order to organize the<br />
exist<strong>in</strong>g organizations <strong>in</strong> the market,<br />
organizations classification, creation<br />
<strong>of</strong> accreditation certificates for these<br />
organizations<br />
Insist on typical charges booklets,<br />
tra<strong>in</strong><strong>in</strong>g the personnel on hospital<br />
wastes and nosocomial <strong>in</strong>fections,<br />
monitor<strong>in</strong>g and evaluation <strong>of</strong> the<br />
organization<br />
Regulate subcontract<strong>in</strong>g <strong>of</strong> <strong>health</strong><br />
services, review <strong>of</strong> subsidies <strong>in</strong>crease<br />
Proceed to an evaluation by the<br />
national <strong>in</strong>stitute <strong>of</strong> <strong>health</strong><br />
adm<strong>in</strong>istration, <strong>in</strong>crease <strong>of</strong> subsidies <strong>in</strong><br />
order to encourage subcontract<strong>in</strong>g<br />
Increase the allocated budget <strong>of</strong><br />
subcontract<strong>in</strong>g to improve quality,<br />
supervision <strong>of</strong> different actors by the<br />
M<strong>in</strong>istry <strong>of</strong> Health
Figuig Improvement <strong>of</strong> the hospital cleanness, free agents<br />
reassigned <strong>in</strong> needs positions<br />
Morocco<br />
Delay <strong>of</strong> organization employees salaries, quality <strong>of</strong><br />
used products, delay <strong>of</strong> budget approval <strong>in</strong>fluences the<br />
engagement and the start <strong>in</strong> the context <strong>of</strong> a bid,<br />
employees are not registered at the social security<br />
Nador Pr<strong>of</strong>it<strong>in</strong>g the personnel number Lack <strong>of</strong> regulations <strong>in</strong> this field respond<strong>in</strong>g to national<br />
norms for the selected partners (audits, controls)<br />
Berkane Service availability (personnel, material, products)<br />
execution efficacy<br />
Problems <strong>of</strong> award<strong>in</strong>g procedures (approval delay,<br />
unavailability <strong>of</strong> funds) no respect <strong>of</strong> the technical<br />
commitments<br />
Oued Eddahab None None None<br />
Laayoune Better service quality, reassignment <strong>of</strong> personnel,<br />
service cont<strong>in</strong>uity, improvement <strong>of</strong> the <strong>in</strong>stitution<br />
image<br />
Lack <strong>of</strong> organization experts, limitation <strong>of</strong><br />
competitiveness, limitation <strong>of</strong> f<strong>in</strong>ancial resources do<br />
not allow subcontract other activities<br />
Tan Tan No comment No comment No comment<br />
Beni Mellal Quality improvement, personnel reassignment Additional costs, week supervision <strong>of</strong> organization’s<br />
personnel<br />
Agadir Qualitative <strong>in</strong>put <strong>of</strong> subcontracted services, personnel<br />
reassignment, less management problems regard<strong>in</strong>g the<br />
subcontracted activities, subcontract<strong>in</strong>g is a must given<br />
the lack <strong>of</strong> personnel<br />
Marrakech<br />
Méd<strong>in</strong>a<br />
Subcontract<strong>in</strong>g can not be extended to other functions<br />
due to budgetary constra<strong>in</strong>ts<br />
No comments No comments None<br />
198<br />
Approve budget <strong>in</strong> good delays, imply<br />
regional <strong>in</strong>spection <strong>of</strong> labour to<br />
supervise the employees and preserve<br />
their rights<br />
Garden<strong>in</strong>g should depend from the<br />
local collectives<br />
Extend subcontract<strong>in</strong>g to all assistance<br />
services, elaborate typical charges<br />
booklets respect<strong>in</strong>g the organization’s<br />
conditions and resources.<br />
Improve the f<strong>in</strong>ancial system <strong>of</strong> PHC,<br />
<strong>in</strong>crease <strong>of</strong> subsidies, review <strong>of</strong> the<br />
price system and implement an equal<br />
system regard<strong>in</strong>g the exoneration <strong>of</strong><br />
organizations from taxes<br />
Encourage subcontract<strong>in</strong>g by<br />
subsidies, organizations should have<br />
an agreement certificate provided by<br />
the state<br />
Give a special attention to the<br />
elaboration <strong>of</strong> the booklets <strong>of</strong> charges
A<strong>in</strong> Seb. Hay<br />
Moh. S. B.<br />
Zenata<br />
El Fida Derb<br />
Soltan<br />
B.S Sidi<br />
Othmane<br />
Morocco<br />
Reassignment <strong>of</strong> the personnel Hospital’s budget does not allow to hire qualified<br />
organizations, s<strong>in</strong>ce they require prices higher than the<br />
adm<strong>in</strong>istration estimation<br />
Costs control, simple procedures, adaptation to quality<br />
norms, flexibility <strong>in</strong> react<strong>in</strong>g to unpredictable events,<br />
advantage <strong>of</strong> advanced management techniques,<br />
adaptation <strong>in</strong> respect to competitiveness<br />
F<strong>in</strong>ancial resources unsatisfactory, weakness <strong>of</strong> the<br />
allocated budgets does not allow the hir<strong>in</strong>g <strong>of</strong> qualified<br />
organizations<br />
Reassignment <strong>of</strong> the personnel High costs <strong>in</strong>creas<strong>in</strong>g every year and consume a large<br />
part <strong>of</strong> the budget, absence <strong>of</strong> efficient control<br />
procedure avoid<strong>in</strong>g budget misuse<br />
Casa Anfa No comment No comment No comment<br />
Mohammadia Disengage hospitals from missions performed badly<br />
due to the number and the pr<strong>of</strong>ile <strong>of</strong> the personnel,<br />
which was recuperated. the quality <strong>of</strong> services is high<br />
Salé Compensate the lack <strong>of</strong> personnel, due to leave,<br />
retirement, <strong>in</strong>validity, sickness, death, recruitment<br />
difficulty. Search for quality <strong>of</strong> pr<strong>of</strong>essionalism,<br />
economy, technicality, quality, settle the problem <strong>of</strong><br />
lack<strong>in</strong>g personnel<br />
Skhirat<br />
Témara<br />
Better control <strong>of</strong> the activity, possibility to change the<br />
contractor<br />
Khémisset Flexibility <strong>of</strong> the process, availability <strong>of</strong> the personnel,<br />
improvement <strong>of</strong> the services<br />
<strong>The</strong> costs represent a large part <strong>of</strong> the budget, activities<br />
<strong>of</strong> security agents are limited by the behaviour <strong>of</strong> the<br />
visitors (aggressiveness), the behaviour <strong>of</strong> the<br />
personnel <strong>of</strong> the organizations is sometimes doubtful<br />
with the patients<br />
Unavailability <strong>of</strong> organization limits competitiveness,<br />
personnel not tra<strong>in</strong>ed <strong>in</strong> garden<strong>in</strong>g and clean<strong>in</strong>g, lack <strong>of</strong><br />
desired pr<strong>of</strong>essionalism<br />
199<br />
Given that there differences <strong>in</strong> the<br />
f<strong>in</strong>ancial resources allocated to<br />
different hospitals, it would be better<br />
to select the providers at the local level<br />
Def<strong>in</strong>e a motivat<strong>in</strong>g system through<br />
budget assistance measures<br />
Subcontract<strong>in</strong>g must be subsidized,<br />
acquire an efficient control method<br />
Extend subcontract<strong>in</strong>g to other<br />
services, establish supervision by<br />
technicians (hygiene and dietician),<br />
adm<strong>in</strong>istration must be react firmly <strong>in</strong><br />
case <strong>of</strong> violation<br />
Establish sheets on evaluation,<br />
experience, seniority, and price<br />
estimation. Turn to bids over 1 to 5<br />
year period; subcontract other services<br />
(plumb<strong>in</strong>g, electricity, carpentry,<br />
construction, etc)<br />
<strong>The</strong> price is very excessive Extend subcontract<strong>in</strong>g to cater<strong>in</strong>g and<br />
to bandage services if the budget is<br />
<strong>in</strong>creased<br />
Companies do not respect their commitments and<br />
disturb the function<strong>in</strong>g <strong>of</strong> the <strong>in</strong>stitution<br />
Establish a list <strong>of</strong> approved companies
Fès Jdid Dar<br />
Dbibegh<br />
Zouagha My<br />
Yacoub<br />
Meknès El<br />
Manzah<br />
Morocco<br />
No comments No comments No comments<br />
No comments No comments No comments<br />
Hygiene and cleanness conditions compatible with<br />
PHC’s requirements, improvement <strong>of</strong> security<br />
conditions<br />
Qualified security and bio-clean<strong>in</strong>g personnel cannot be<br />
hired due to f<strong>in</strong>ancial constra<strong>in</strong>t, <strong>in</strong>stability <strong>of</strong> the<br />
personnel <strong>of</strong> the organizations<br />
Oujda Angad No comments No comments No suggestions<br />
A<strong>in</strong> Chok hay<br />
Hassani<br />
Solve the problem <strong>of</strong> lack<strong>in</strong>g personnel, assign<br />
personnel to strictly <strong>health</strong> activities, the services are<br />
provided by specialists<br />
Bid awarded on the basis <strong>of</strong> the best <strong>of</strong>fer (quality /<br />
price ratio), adm<strong>in</strong>istration not <strong>in</strong>formed on the<br />
personnel changes, require a permanent supervision if<br />
not the quality <strong>of</strong> the service will decrease, delay <strong>in</strong><br />
approv<strong>in</strong>g the bids<br />
200<br />
Availability <strong>of</strong> sufficient budget to hire<br />
qualified organizations, extend the<br />
experience to facilities ma<strong>in</strong>tenance<br />
biomedical materials <strong>in</strong> order to cope<br />
with the lack <strong>of</strong> personnel<br />
No suggestions
Pakistan<br />
PAKISTAN
BACKGROUND<br />
Country pr<strong>of</strong>ile [1]<br />
Pakistan<br />
Pakistan has an area <strong>of</strong> 307 374 square miles (796 095 square kilometres), with an<br />
overall population density <strong>of</strong> 182 persons per square kilometre. <strong>The</strong>re are four prov<strong>in</strong>ces,<br />
Punjab, S<strong>in</strong>dh, North West Frontier Prov<strong>in</strong>ce (NWFP) and Baluchistan, and two regions Azad<br />
Jammu Kashmir (AJK) and Federally Adm<strong>in</strong>istered Northern Area (FANA). Afghan refugees<br />
reside <strong>in</strong> certa<strong>in</strong> areas <strong>of</strong> the country <strong>in</strong> significant numbers.<br />
Punjab is the most populous prov<strong>in</strong>ce <strong>of</strong> Pakistan, with a population <strong>of</strong> 80.3 million and<br />
an area <strong>of</strong> 205 345 square kilometres. About two-thirds <strong>of</strong> its population resides <strong>in</strong> rural areas<br />
and agriculture is the chief source <strong>of</strong> <strong>in</strong>come and employment <strong>in</strong> Punjab. Similarly the<br />
population <strong>of</strong> S<strong>in</strong>dh is 33.8 million. Asian Punjab most people like live <strong>in</strong> rural areas and<br />
work <strong>in</strong> fields to earn their livelihood. <strong>The</strong> population <strong>of</strong> NWFP is 19.4 million, and<br />
Baluchistan is 6.5 million. Baluchistan is the largest prov<strong>in</strong>ce <strong>in</strong> area. <strong>The</strong> population <strong>of</strong> AJK<br />
has been estimated at 3.5 million people, most <strong>of</strong> whom live <strong>in</strong> scattered hilly areas which are<br />
not accessible at times dur<strong>in</strong>g the year due to weather.<br />
<strong>The</strong> human development <strong>in</strong>dicators for Pakistan, particularly for <strong>health</strong>, are still low<br />
despite progress made <strong>in</strong> recent years. <strong>The</strong> national <strong>health</strong> status is characterized by high<br />
population growth (2.2%), low life expectancy (64.0), high <strong>in</strong>fant mortality (82 per 1000live<br />
births) and child (under 5 years) mortality rates (105 per 1000 live births). This is due to the<br />
shortage <strong>of</strong> <strong>health</strong> care personnel, uneven distribution <strong>of</strong> <strong>health</strong> facilities <strong>in</strong> the country, lack<br />
<strong>of</strong> medic<strong>in</strong>es, regional disparities <strong>in</strong> the <strong>health</strong> care services and scarcity <strong>of</strong> adm<strong>in</strong>istrative<br />
<strong>health</strong> care capabilities.<br />
<strong>The</strong> <strong>health</strong> system <strong>of</strong> Pakistan is one <strong>of</strong> the largest <strong>in</strong> south-east Asia. <strong>The</strong> system<br />
comprises an extensive network <strong>of</strong> primary, secondary, and tertiary <strong>health</strong> facilities and<br />
specialized <strong>health</strong> <strong>in</strong>stitutes. Medical facilities <strong>in</strong> the country have improved significantly over<br />
the years. However, there still rema<strong>in</strong>s a very large gap between the availability and<br />
requirements. At present, there are 108 062 registered doctors, 5530 dentists and 46 331<br />
nurses <strong>in</strong> the country, equivalent to ratios <strong>of</strong> 1404 persons per doctor, 27 414 persons per<br />
dentist and one nurse per 3296 persons. <strong>The</strong>re are about 906 hospitals, 4554 dispensaries,<br />
5290 basic <strong>health</strong> units and 552 rural <strong>health</strong> centres. <strong>The</strong> availability <strong>of</strong> hospital beds <strong>in</strong> all<br />
medical facilities has been estimated at 98 684, equivalent to a population–bed ratio <strong>of</strong> 1536<br />
persons per bed. <strong>The</strong> figures available for the medical facilities clearly <strong>in</strong>dicate the need for<br />
further expansion or alternative <strong>arrangements</strong> for provision <strong>of</strong> <strong>health</strong> care.<br />
Both public and private spend<strong>in</strong>g on <strong>health</strong> <strong>in</strong> Pakistan are very low. However, over the<br />
years spend<strong>in</strong>g has <strong>in</strong>creased steadily. Dur<strong>in</strong>g 2003–2004, the total expenditure on <strong>health</strong> was<br />
estimated at 32.8 billion Pakistani rupees (PKR) (PKR 8.5 billion development and PKR 24<br />
billion as recurr<strong>in</strong>g), which amounts to 0.84% <strong>of</strong> GNP and shows an <strong>in</strong>crease <strong>of</strong> 13.8% over<br />
the previous year.<br />
202
Pakistan<br />
To improve the <strong>health</strong> status <strong>of</strong> people and to reduce the burden <strong>of</strong> disease, a series <strong>of</strong><br />
programmes and projects under way. <strong>The</strong>se <strong>in</strong>clude the programme for family plann<strong>in</strong>g and<br />
primary <strong>health</strong> care, Expanded Programme on Immunization, national AIDS control<br />
programme, malaria control programme, tuberculosis control programme and drug abuse<br />
control programme.<br />
Contract<strong>in</strong>g <strong>in</strong> <strong>health</strong> care [2,3]<br />
Contract<strong>in</strong>g is used by the public <strong>sector</strong> for the purchase over time <strong>of</strong> specified services<br />
from the private <strong>sector</strong>, or <strong>in</strong> some cases through <strong>in</strong>ternal contracts with autonomous public<br />
facilities. Contract<strong>in</strong>g is an <strong>in</strong>creas<strong>in</strong>gly important element <strong>of</strong> many countries’ <strong>health</strong> <strong>sector</strong><br />
reform programmes because it provides governments with a management tool that creates<br />
<strong>in</strong>centives for improved performance and <strong>in</strong>creased accountability. Contract<strong>in</strong>g can improve<br />
access, quality, efficiency, and susta<strong>in</strong>ability; promote public <strong>health</strong> goals; and create an<br />
environment conducive to public–private collaboration. However, the process is challeng<strong>in</strong>g<br />
and requires transparent bidd<strong>in</strong>g procedures, well-designed contracts, clear performance<br />
obligations and credible fund<strong>in</strong>g mechanisms. In addition, governments need to be able to<br />
monitor the contracts and have credibility as a trustworthy partner.<br />
Resolution WHA56.25 endorsed by the World Health Assembly <strong>in</strong> 2003 urges Member<br />
States to assess the <strong>role</strong> <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> improv<strong>in</strong>g <strong>health</strong> systems’<br />
performance. <strong>The</strong>re is limited experience or documentation <strong>of</strong> public–private partnership <strong>in</strong><br />
<strong>health</strong> among countries <strong>of</strong> the Eastern Mediterranean Region, although several countries are at<br />
various stages <strong>of</strong> implement<strong>in</strong>g <strong>health</strong> <strong>sector</strong> reforms. <strong>The</strong>re is <strong>in</strong>creas<strong>in</strong>g realization with<strong>in</strong><br />
the Eastern Mediterranean Region <strong>of</strong> the importance <strong>of</strong> awareness creation and capacitybuild<strong>in</strong>g<br />
with<strong>in</strong> m<strong>in</strong>istries <strong>of</strong> <strong>health</strong> <strong>in</strong> contract<strong>in</strong>g out publicly f<strong>in</strong>anced <strong>health</strong> services to the<br />
private <strong>sector</strong>.<br />
As regards the production <strong>of</strong> <strong>health</strong> services <strong>in</strong> the develop<strong>in</strong>g countries, neither the<br />
public nor private <strong>sector</strong> provides full satisfaction, and there is a need to explore new avenues<br />
<strong>in</strong> order to capitalize on the strengths <strong>of</strong> both <strong>sector</strong>s and elim<strong>in</strong>ate their weaknesses. A<br />
modern <strong>health</strong> system br<strong>in</strong>gs <strong>in</strong> a large number <strong>of</strong> parties, each <strong>of</strong> which can play a different<br />
<strong>role</strong>. Those who have divergent objectives and <strong>in</strong>terests may negotiate, so as to f<strong>in</strong>d<br />
agreement that will allow action to be taken: the contract is the element that seals the<br />
agreement and confers legal force to it. A <strong>contractual</strong> agreement is an agreement between two<br />
or more economic agents through which they undertake or assume or rel<strong>in</strong>quish, do or not do<br />
certa<strong>in</strong> th<strong>in</strong>gs. A contract is therefore a voluntary alliance <strong>of</strong> <strong>in</strong>dependent partners. <strong>The</strong><br />
alliance must give the partners an advantage or surplus that would not have existed had the<br />
two partners not been allied. A contract is therefore collaboration between partners. It is an<br />
<strong>in</strong>strument which <strong>in</strong>stitutes <strong>role</strong>s or clauses that establish the possibility <strong>of</strong> cooperative<br />
behaviour <strong>in</strong> the <strong>in</strong>terest <strong>of</strong> both parties.<br />
<strong>The</strong> purchaser, or contract<strong>in</strong>g agency, uses the contract<strong>in</strong>g relationship to obta<strong>in</strong> a<br />
service or product. <strong>The</strong> range <strong>of</strong> government purchasers will reflect a country’s underly<strong>in</strong>g<br />
<strong>health</strong> system. National level m<strong>in</strong>istries <strong>of</strong> <strong>health</strong>, or their regional and local equivalents may<br />
contract directly for <strong>health</strong> care. <strong>The</strong> public <strong>sector</strong> may also contract private providers through<br />
203
Pakistan<br />
a variety <strong>of</strong> <strong>health</strong> <strong>in</strong>surance mechanisms, which aga<strong>in</strong> may be national, regional or local <strong>in</strong><br />
nature. Other non-<strong>health</strong> government entities such as state owned companies or groups may<br />
also directly contract for <strong>health</strong> care. <strong>The</strong> contractor, also referred to as provider or vendor is<br />
an <strong>in</strong>dividual or organization that sells its services or products via the contract<strong>in</strong>g agreement.<br />
Private <strong>sector</strong> contractors generally fall <strong>in</strong>to the for-pr<strong>of</strong>it and non-pr<strong>of</strong>it categories. <strong>The</strong> forpr<strong>of</strong>it<br />
providers <strong>of</strong> <strong>health</strong> care exist to earn pr<strong>of</strong>it for their owners and <strong>in</strong>clude private practice<br />
physicians, nurses, midwives; traditional medical practitioners; hospitals cl<strong>in</strong>ics and <strong>health</strong><br />
centres; and pharmacies and other retail drug and medical supply outlets. <strong>The</strong> non-pr<strong>of</strong>it<br />
providers, many <strong>of</strong> which are known as nongovernmental organizations, are private but def<strong>in</strong>e<br />
their mission <strong>in</strong> terms <strong>of</strong> social or public <strong>health</strong> goal. <strong>The</strong>y also <strong>in</strong>clude pr<strong>of</strong>essional medical<br />
and nurs<strong>in</strong>g associations or philanthropic groups. Community organizations, sometimes also<br />
<strong>in</strong>cluded under the nongovernmental organization category, usually are smaller and less<br />
formally constituted than a nongovernmental organization, serve a limited geographical area,<br />
and are formed to serve the <strong>in</strong>terests <strong>of</strong> their members alone. Public parties can also be<br />
contractors, for example when the M<strong>in</strong>istry <strong>of</strong> Health contract with quasi-governmental<br />
medical stores for drug procurement.<br />
Need for contract<strong>in</strong>g [4]<br />
<strong>The</strong> general theoretical rationale for contract<strong>in</strong>g out relates to theories <strong>of</strong> why<br />
governments fail <strong>in</strong> their provision <strong>of</strong> services. <strong>The</strong>re are two ma<strong>in</strong> schools <strong>of</strong> thought. <strong>The</strong><br />
property rights theory contends that the ma<strong>in</strong> source <strong>of</strong> <strong>in</strong>efficiency <strong>in</strong> the public <strong>sector</strong> is the<br />
weaken<strong>in</strong>g <strong>of</strong> property rights, so that decision-makers face few <strong>in</strong>centives to allocate<br />
resources efficiently. This is contrasted with the <strong>in</strong>centives fac<strong>in</strong>g entrepreneurs or<br />
shareholders <strong>in</strong> the private <strong>sector</strong>. <strong>The</strong> public choice theory contends that politicians and<br />
bureaucrats who control public bureaucracies cannot be assumed to be act<strong>in</strong>g <strong>in</strong> the public<br />
<strong>in</strong>terest, s<strong>in</strong>ce they are more likely to serve their own <strong>in</strong>terests, or those <strong>of</strong> powerful <strong>in</strong>terest<br />
groups. In response to these analyses, the “new public management” envisages the use <strong>of</strong><br />
market mechanisms to generate appropriate price and demand signals, and to weaken the<br />
<strong>in</strong>fluence <strong>of</strong> politicians and pr<strong>of</strong>essionals over public service delivery, thus ensur<strong>in</strong>g that these<br />
services are more responsive to market signals and to customers. It is also argued that private<br />
organizations can br<strong>in</strong>g the advantages <strong>of</strong> functional specifications, as well as speed and<br />
flexibility <strong>in</strong> adjust<strong>in</strong>g to chang<strong>in</strong>g factor prices, technology and demand conditions. A central<br />
theme <strong>of</strong> this th<strong>in</strong>k<strong>in</strong>g is thus the view <strong>of</strong> the state as responsible for enabl<strong>in</strong>g or ensur<strong>in</strong>g<br />
service delivery, rather than for direct delivery <strong>of</strong> service itself, except <strong>in</strong> certa<strong>in</strong> identifiable<br />
circumstances.<br />
Types <strong>of</strong> <strong>contractual</strong> agreements [5]<br />
Contractual agreements come <strong>in</strong> various forms. Two important forms are contract<strong>in</strong>g-<strong>in</strong><br />
and contract<strong>in</strong>g-out. <strong>The</strong> former refers to br<strong>in</strong>g<strong>in</strong>g <strong>in</strong> outside private management to operate<br />
an <strong>in</strong>ternal government service. <strong>The</strong> latter refers to purchas<strong>in</strong>g services from a private source<br />
that provides the service, us<strong>in</strong>g primarily an external workforce and resources. In this latter<br />
situation, contractors have complete responsibility for service delivery, <strong>in</strong>clud<strong>in</strong>g hir<strong>in</strong>g,<br />
fir<strong>in</strong>g, sett<strong>in</strong>g wages, and procur<strong>in</strong>g and distribut<strong>in</strong>g essential drugs and supplies. Other<br />
<strong>contractual</strong> options for purchas<strong>in</strong>g <strong>health</strong> services are franchis<strong>in</strong>g and leas<strong>in</strong>g. In franchis<strong>in</strong>g,<br />
204
Pakistan<br />
the government grants a contractor the right which may or may not be exclusive) to provide<br />
specified services, for which the patient pays, to a particular population. In leas<strong>in</strong>g, the<br />
government secures the use, but not ownership, <strong>of</strong> facilities or equipment from an outside<br />
source under a lease agreement. Furthermore, it is important to recognize that the government<br />
can contract with public providers. For example, governments can establish a <strong>contractual</strong><br />
agreement with autonomous <strong>in</strong>stitutions, which rema<strong>in</strong> under public ownership.<br />
Potential advantages and disadvantages <strong>of</strong> contract<strong>in</strong>g [4,5,6]<br />
<strong>The</strong> potential advantages and disadvantages <strong>of</strong> contract<strong>in</strong>g from a public <strong>sector</strong><br />
perspective as documented <strong>in</strong> literature are summarized as follows.<br />
Benefits<br />
L<strong>in</strong>ks f<strong>in</strong>ancial allocations to <strong>health</strong> services outputs, outcomes and consumption patterns and<br />
thus facilitates measurement <strong>of</strong> and improvement <strong>in</strong> efficiency and equity<br />
Clarifies the <strong>role</strong>s and responsibilities <strong>of</strong> both parties and thus facilitates greater accountability<br />
Can generate pressure on both public and private providers to improve their performance <strong>in</strong><br />
terms <strong>of</strong> both service and price<br />
Requires and may promote better plann<strong>in</strong>g and policy development by improv<strong>in</strong>g the flow <strong>of</strong><br />
<strong>in</strong>formation about volumes <strong>of</strong> goods, services, costs, quality, responsiveness, population<br />
served, <strong>health</strong> needs and other issues<br />
Provides government with a mechanism for purchas<strong>in</strong>g needed <strong>health</strong> services at an agreed-on,<br />
and therefore, predictable price<br />
Improves equity <strong>in</strong> distribution <strong>of</strong> <strong>health</strong> services because government can establish contracts<br />
that focus on deliver<strong>in</strong>g services to vulnerable populations.<br />
Disadvantages<br />
<strong>The</strong> costs <strong>in</strong>volved may be <strong>in</strong>creased substantially. However, the proponents <strong>of</strong><br />
contract<strong>in</strong>g claim, <strong>of</strong>ten implicitly, that the overall benefits <strong>of</strong> contract<strong>in</strong>g will outweigh the<br />
costs <strong>in</strong>volved <strong>in</strong> their creation and ma<strong>in</strong>tenance. <strong>The</strong>se costs <strong>in</strong>clude transaction costs, the<br />
higher costs that may result from the loss <strong>of</strong> monopsony purchas<strong>in</strong>g power, and the social<br />
costs aris<strong>in</strong>g from equity problems. <strong>The</strong>re may be substantial transaction costs <strong>in</strong>volved <strong>in</strong><br />
creat<strong>in</strong>g and ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g the contracts. <strong>The</strong> extent <strong>of</strong> costs will depend on the number <strong>of</strong><br />
contracts that have to be written, the extent <strong>of</strong> detail <strong>in</strong> their specification, and the <strong>in</strong>tensity<br />
with which implementation is monitored. While it is clear that contract<strong>in</strong>g may <strong>in</strong>cur high<br />
transactions costs, it is important to compare these with the explicit and hidden costs <strong>of</strong><br />
directly managed public systems, rather than to view them as entirely <strong>in</strong>cremental. <strong>The</strong> public<br />
agencies may face large costs <strong>in</strong> monitor<strong>in</strong>g staff and output quality, and there may also be<br />
significant costs <strong>in</strong>volved <strong>in</strong> bureaucratic adm<strong>in</strong>istrative mechanisms and <strong>in</strong> the effects <strong>of</strong><br />
political <strong>in</strong>terference.<br />
A second set <strong>of</strong> costs may come from the loss <strong>of</strong> monopsony power result<strong>in</strong>g from<br />
fragmentation <strong>of</strong> the s<strong>in</strong>gle purchas<strong>in</strong>g agency <strong>in</strong> the traditional public <strong>health</strong> <strong>sector</strong>. This will<br />
not however be a problem where a s<strong>in</strong>gle agency contracts for services.<br />
205
Pakistan<br />
<strong>The</strong>re may be a potential conflict between efficiency requirements <strong>of</strong> the market<br />
environment and equity goals, which may act to underm<strong>in</strong>e equity goals. This may <strong>in</strong>clude<br />
loss <strong>of</strong> comprehensiveness <strong>of</strong> local service provision and potential loss <strong>of</strong> consumer choice.<br />
Equity may also be threatened through the practice <strong>of</strong> provider or purchaser selection <strong>of</strong> low<br />
risk patients where payment does not adequately compensate for the level <strong>of</strong> risk <strong>of</strong> specific<br />
patients or types <strong>of</strong> patient.<br />
Selective contract<strong>in</strong>g may also have substantial impact on the wider <strong>health</strong> system.<br />
Introduction <strong>of</strong> contracted providers may lead to fragmentation or lack <strong>of</strong> coord<strong>in</strong>ation with<strong>in</strong><br />
the broader public <strong>health</strong> system. Contract<strong>in</strong>g could also lead to competition between<br />
contractors and public providers for staff resources, lead<strong>in</strong>g to <strong>in</strong>creased salaries and to public<br />
hospitals be<strong>in</strong>g dra<strong>in</strong>ed <strong>of</strong> key personnel, or suffer<strong>in</strong>g from <strong>in</strong>creased staff turnover. Contracts<br />
can lock scarce resources <strong>in</strong>to a particular allocation, even when changed circumstances<br />
dictate a reallocation.<br />
SCOPE, OBJECTIVES AND METHODOLOGY<br />
<strong>The</strong> scope <strong>of</strong> this study is to undertake situation analysis, <strong>in</strong>clud<strong>in</strong>g exploratory case<br />
studies, and document experiences as well as recommendations for outsourc<strong>in</strong>g <strong>of</strong> publicly<br />
f<strong>in</strong>anced <strong>health</strong> services to private <strong>sector</strong> organizations <strong>in</strong> Pakistan. <strong>The</strong> study <strong>in</strong> Pakistan is<br />
part <strong>of</strong> a regional <strong>in</strong>itiative to develop an evidence-based regional strategy on public–private<br />
partnership <strong>in</strong> <strong>health</strong> <strong>in</strong> the Eastern Mediterranean Region.<br />
<strong>The</strong> objectives <strong>of</strong> the study are to review the <strong>arrangements</strong> and experiences <strong>of</strong><br />
“contract<strong>in</strong>g out” and provide recommendations for future programm<strong>in</strong>g by:<br />
assess<strong>in</strong>g the environment and overall capacity <strong>of</strong> providers and purchasers <strong>in</strong> terms <strong>of</strong><br />
contract<strong>in</strong>g out <strong>health</strong> services to the private <strong>sector</strong>, its implementation as well as<br />
evaluation;<br />
assess<strong>in</strong>g the <strong>arrangements</strong> and experiences <strong>of</strong> a project/programme <strong>in</strong> <strong>health</strong> that has taken up<br />
<strong>contractual</strong> <strong>arrangements</strong> as an implementation modality; and<br />
discuss<strong>in</strong>g f<strong>in</strong>d<strong>in</strong>gs on <strong>contractual</strong> <strong>arrangements</strong> with the key stakeholders to <strong>in</strong>form the study<br />
recommendations.<br />
<strong>The</strong> qualitative study uses a mix <strong>of</strong> methods to address the multiplicity and complexity<br />
<strong>of</strong> dimensions <strong>of</strong> the <strong>contractual</strong> <strong>arrangements</strong> for <strong>health</strong> services. <strong>The</strong> methods used <strong>in</strong> the<br />
study are: a) literature review; b) focus group discussion; c) key <strong>in</strong>formant <strong>in</strong>terview; d) case<br />
study; and e) a consensus-build<strong>in</strong>g workshop.<br />
a) Literature review<br />
<strong>The</strong> relevant <strong>in</strong>ternational and national literature was identified through library and<br />
<strong>in</strong>ternet searches. <strong>The</strong> literature was screened and relevant material was selected for <strong>in</strong>-depth<br />
review by the researcher. <strong>The</strong> documented <strong>arrangements</strong> and experiences <strong>in</strong> the countries<br />
were reviewed to identify key areas <strong>of</strong> <strong>in</strong>formation about various dimensions <strong>of</strong> <strong>contractual</strong><br />
<strong>arrangements</strong>. <strong>The</strong> guidel<strong>in</strong>es and schedule for focus group discussion and key <strong>in</strong>formant<br />
<strong>in</strong>terviews were developed, <strong>in</strong> the light <strong>of</strong> literature review.<br />
206
Pakistan<br />
<strong>The</strong> relevant documents were identified and collected from various national, prov<strong>in</strong>cial<br />
and district level stakeholders, <strong>in</strong>clud<strong>in</strong>g public and private <strong>sector</strong> partners. <strong>The</strong> documents<br />
<strong>in</strong>cluded organizational pr<strong>of</strong>iles, statement <strong>of</strong> operat<strong>in</strong>g procedures, contract documents,<br />
annual reports etc. <strong>The</strong> review <strong>of</strong> documents helped the researchers to learn about the<br />
environment, <strong>arrangements</strong> and experiences <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> <strong>health</strong> services.<br />
b) Focus group discussions<br />
<strong>The</strong> focus group discussion was designed (format attached as Annex 1)and held with<br />
representatives from national programmes, M<strong>in</strong>istry <strong>of</strong> Health, M<strong>in</strong>istry <strong>of</strong> Population<br />
Welfare, nongovernmental organizations, a postgraduate <strong>in</strong>stitute, district <strong>health</strong>, and a tertiary<br />
hospital. <strong>The</strong> focus group discussions helped the researcher to learn about various dimensions<br />
<strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong>, <strong>in</strong>clud<strong>in</strong>g perceptions, experiences, future vision and suggestions<br />
<strong>of</strong> the participants represent<strong>in</strong>g the key stakeholders. <strong>The</strong> discussion also helped <strong>in</strong> further<br />
ref<strong>in</strong><strong>in</strong>g the <strong>in</strong>terview schedule and <strong>in</strong> develop<strong>in</strong>g prelim<strong>in</strong>ary suggestions for further<br />
discussion with <strong>in</strong>dividual <strong>in</strong>terviewees.<br />
c) Key <strong>in</strong>formant <strong>in</strong>terviews<br />
A number <strong>of</strong> key <strong>in</strong>formants, represent<strong>in</strong>g various key stakeholders, were <strong>in</strong>terviewed to<br />
learn more about the structure, operations and relevant contract<strong>in</strong>g experiences <strong>of</strong> their<br />
respective organizations. In addition, key personnel from the M<strong>in</strong>istry <strong>of</strong> Health as well as<br />
from Plann<strong>in</strong>g and Development were <strong>in</strong>terviewed to discuss the f<strong>in</strong>d<strong>in</strong>gs and critically<br />
review and modify the prelim<strong>in</strong>ary recommendations.<br />
d) Case study<br />
A list <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> <strong>health</strong> services was prepared on the basis <strong>of</strong> formal<br />
and <strong>in</strong>formal <strong>in</strong>formation collected from governmental and the nongovernmental sources. <strong>The</strong><br />
governmental sources <strong>of</strong> <strong>in</strong>formation <strong>in</strong>cluded the M<strong>in</strong>istry <strong>of</strong> Health, prov<strong>in</strong>cial Department<br />
<strong>of</strong> Health, prov<strong>in</strong>cial Department <strong>of</strong> Social Welfare. <strong>The</strong> nongovernmental sources <strong>in</strong>cluded<br />
the World Bank, Department for International Development (United K<strong>in</strong>gdom), other<br />
<strong>in</strong>ternational and national nongovernmental organizations.<br />
<strong>The</strong> selection <strong>of</strong> project for detailed study <strong>of</strong> contract<strong>in</strong>g <strong>arrangements</strong> was done on the<br />
basis <strong>of</strong>: current geographical coverage; nature <strong>of</strong> services; duration <strong>of</strong> experience; and<br />
scal<strong>in</strong>g-up potential. <strong>The</strong> project selected for detailed study was the Punjab Rural Support<br />
Programme <strong>in</strong> Rahim Yar Khan district. <strong>The</strong> selected project was studied <strong>in</strong> detail for its<br />
<strong>contractual</strong> agreement, management <strong>arrangements</strong> and implementation experience.<br />
207
e) Consensus-build<strong>in</strong>g workshop<br />
Pakistan<br />
<strong>The</strong> researcher prepared a draft study report based on document review, focus group<br />
discussion and <strong>in</strong>terviews. <strong>The</strong> draft report was discussed with the representatives <strong>of</strong> key<br />
stakeholders, and <strong>in</strong> light <strong>of</strong> discussions the f<strong>in</strong>al draft <strong>of</strong> the study report was produced.<br />
FINDINGS [7–14]<br />
Overall f<strong>in</strong>d<strong>in</strong>gs<br />
Range <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong><br />
In <strong>health</strong> services, the <strong>contractual</strong> arrangement is be<strong>in</strong>g recognized as a potential way to<br />
optimize the use <strong>of</strong> available resources. <strong>The</strong> <strong>contractual</strong> <strong>arrangements</strong> between a public <strong>sector</strong><br />
purchaser and a private <strong>sector</strong> provider at various levels <strong>of</strong> hierarchy vary widely <strong>in</strong> the type <strong>of</strong><br />
contract and the set <strong>of</strong> services to be provided. <strong>The</strong> contracts are made at federal, prov<strong>in</strong>cial and<br />
district levels. <strong>The</strong> public <strong>sector</strong> purchasers <strong>in</strong>clude ma<strong>in</strong>ly the M<strong>in</strong>istry <strong>of</strong> Health, the prov<strong>in</strong>cial<br />
Departments <strong>of</strong> Health and Social Welfare, and the district governments. <strong>The</strong> private providers<br />
<strong>in</strong>clude ma<strong>in</strong>ly the <strong>in</strong>ternational and national nongovernmental organizations, <strong>in</strong>stitutions as well<br />
as private firms. <strong>The</strong> contract types <strong>in</strong>clude ma<strong>in</strong>ly contract<strong>in</strong>g out, cost shar<strong>in</strong>g agreements,<br />
grants and loans. <strong>The</strong> set <strong>of</strong> activities covered <strong>in</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong>clude ma<strong>in</strong>ly the<br />
primary <strong>health</strong> care services, research and development services, technical and management<br />
services. Table 1 lists several examples <strong>of</strong> the ongo<strong>in</strong>g <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> Pakistan.<br />
Rationale and <strong>in</strong>terest<br />
<strong>The</strong> government <strong>sector</strong> rationale for <strong>contractual</strong> <strong>arrangements</strong> generally varies with the<br />
size and nature <strong>of</strong> <strong>health</strong> problem, current coverage and capacity <strong>of</strong> public and private <strong>sector</strong><br />
<strong>health</strong> services, perceived need for service development and <strong>in</strong>novation, and consumer<br />
perceptions and expectations.<br />
<strong>The</strong> size and nature <strong>of</strong> <strong>health</strong> problem refers to issues <strong>of</strong> disease prevalence, diseaserelated<br />
stigma, high-risk population(s), and special social and technical requirements. <strong>The</strong><br />
coverage and capacity <strong>of</strong> services refers to the issues <strong>of</strong> limited geographical and social<br />
access, <strong>in</strong>adequate <strong>health</strong> <strong>in</strong>frastructure and resources, lack <strong>of</strong> competition lead<strong>in</strong>g to low<br />
efficiency, <strong>in</strong>adequate outreach services, poor staff motivation and support. <strong>The</strong> <strong>in</strong>novation<br />
refers to the issues <strong>of</strong> limited flexibility <strong>in</strong> operations, limited ability to respond to new<br />
situations/challenges, delayed decisions, and lack <strong>of</strong> market mechanisms. <strong>The</strong> consumer<br />
perspective refers to the issues <strong>of</strong> low perceived quality <strong>of</strong> care, social acceptability, and<br />
ability and will<strong>in</strong>gness to pay for a set <strong>of</strong> services.<br />
<strong>The</strong> private <strong>sector</strong> rationale for <strong>contractual</strong> <strong>arrangements</strong> generally <strong>in</strong>cludes enhanced size<br />
and scope <strong>of</strong> current activities, recognition and f<strong>in</strong>ancial support, and humanitarian concerns.<br />
208
Pakistan<br />
Table 1. Examples <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> the <strong>health</strong> <strong>sector</strong> <strong>in</strong> Pakistan<br />
Contract type Payment mode Purchaser Provider Focus area<br />
Contract<strong>in</strong>g<br />
out<br />
Service<br />
contract<br />
Contract<strong>in</strong>g-<strong>in</strong><br />
Social<br />
franchis<strong>in</strong>g<br />
Concession<br />
(Build-operate<br />
-transfer)<br />
Block payment National AIDS control<br />
programme<br />
Block payment M<strong>in</strong>istry <strong>of</strong> Population<br />
Welfare<br />
Block payment DoH Punjab<br />
(Rahim Yar Khan)<br />
Cost per case M<strong>in</strong>istry <strong>of</strong> Population<br />
Welfare<br />
Block payment National Programme for<br />
primary <strong>health</strong> care and<br />
Family Plann<strong>in</strong>g, lady<br />
<strong>health</strong> workers<br />
Programme<br />
Block payment Participatory<br />
Development<br />
Programme<br />
1994–2001<br />
Block payment National Trust for<br />
Population Welfare<br />
Block payment<br />
(Grant plus<br />
loan)<br />
Political environment<br />
Punjab Health<br />
Foundation<br />
Indemnification Malaria Control<br />
Programme<br />
Block payment Department <strong>of</strong> Health<br />
AJK/FANA<br />
Block payment Department <strong>of</strong> Health<br />
NWFP<br />
Block payment Department <strong>of</strong> Health<br />
S<strong>in</strong>dh<br />
209<br />
Private partners Management services,<br />
Third party evaluation<br />
Population Council Management and<br />
technical assistance<br />
services<br />
Punjab Rural<br />
Support<br />
Programme<br />
Family Plann<strong>in</strong>g<br />
Association <strong>of</strong><br />
Pakistan<br />
Management <strong>of</strong> PHC<br />
services<br />
Provision <strong>of</strong> family<br />
plann<strong>in</strong>g services<br />
UNICEF Delivery <strong>of</strong> certa<strong>in</strong> set <strong>of</strong><br />
services for programme<br />
(e.g. partial evaluation)<br />
Community-based<br />
organizations/<br />
nongovernmental<br />
organizations<br />
Nongovernmental<br />
organizations<br />
Nongovernmental<br />
organizations and<br />
private<br />
practitioners<br />
Institute <strong>of</strong> Public<br />
Health<br />
Marie Adelaide<br />
Leprosy Centre<br />
AIMS<br />
(nongovernmental<br />
organization)<br />
S<strong>in</strong>dh Graduates<br />
Association<br />
Service delivery<br />
Service delivery<br />
Service strengthen<strong>in</strong>g and<br />
delivery<br />
Technical services<br />
Tuberculosis service<br />
delivery<br />
Rural <strong>health</strong> care<br />
management and service<br />
delivery<br />
Management <strong>of</strong> basic<br />
<strong>health</strong> units<br />
Block payment M<strong>in</strong>istry <strong>of</strong> Health Greenstar Reproductive <strong>health</strong><br />
services<br />
Pre-payment Department <strong>of</strong> Health<br />
Punjab<br />
Munshi Trust<br />
(nongovernmental<br />
organization)<br />
Hospital services<br />
<strong>The</strong>re is <strong>in</strong>creas<strong>in</strong>g recognition and <strong>in</strong>terest <strong>in</strong> develop<strong>in</strong>g public–private partnerships<br />
for better coverage and quality <strong>of</strong> <strong>health</strong> services. <strong>The</strong>re is evidence <strong>of</strong> political commitment<br />
at the highest level, as shown by various statements by the Prime M<strong>in</strong>ister and the Federal<br />
M<strong>in</strong>ister <strong>of</strong> Health <strong>in</strong> which they have encouraged and projected public–private partnership as<br />
a major step <strong>in</strong> right direction. <strong>The</strong> <strong>in</strong>troduction <strong>of</strong> transparent <strong>arrangements</strong> for collective
Pakistan<br />
decision-mak<strong>in</strong>g, such as the Inter-Agency Coord<strong>in</strong>ation Committee and Country<br />
Coord<strong>in</strong>at<strong>in</strong>g Mechanism, has helped build understand<strong>in</strong>g and trust among public and private<br />
partners. <strong>The</strong> transparent decision-mak<strong>in</strong>g process has enabled the managers to avoid<br />
unnecessary political and other external <strong>in</strong>fluences. At prov<strong>in</strong>cial level there is an <strong>in</strong>creas<strong>in</strong>g<br />
number <strong>of</strong> <strong>health</strong> services delivery and research projects based on public–private partnership,<br />
e.g. a primary <strong>health</strong> care services project <strong>in</strong> Rahim Yar Khan district, followed by replication<br />
<strong>in</strong> other districts <strong>of</strong> Punjab. Global <strong>in</strong>itiatives such as Global Fund to Fight AIDS,<br />
Tuberculosis and Malaria (GFATM), Global Alliance for Vacc<strong>in</strong>es and Immunization (GAVI),<br />
and Global Alliance for Improved Nutrition (GAIN) have also contributed to br<strong>in</strong>g<strong>in</strong>g positive<br />
change <strong>in</strong> the environment for public–private partnership development.<br />
Bureaucratic setup support<br />
<strong>The</strong>re is a grow<strong>in</strong>g number <strong>of</strong> pro-contract<strong>in</strong>g bureaucrats at all levels. Some managers<br />
believe that the current set <strong>of</strong> government procedures can be used effectively <strong>in</strong> a <strong>contractual</strong><br />
environment, provided managers have the commitment and capacity to use the procedures.<br />
However, not all managers seem to be equally competent <strong>in</strong> manag<strong>in</strong>g public–private<br />
partnership <strong>in</strong> the current situation. <strong>The</strong> experiences at national and prov<strong>in</strong>cial level show that<br />
there have been process delays, primarily due to lack <strong>of</strong> precedence and guidel<strong>in</strong>es for<br />
manag<strong>in</strong>g <strong>contractual</strong> <strong>arrangements</strong>. At the same time, programme managers have expressed<br />
appreciation for the non-<strong>in</strong>terference <strong>of</strong> higher <strong>of</strong>ficials <strong>in</strong> the contract award<strong>in</strong>g process.<br />
<strong>The</strong> <strong>in</strong>stitutional <strong>arrangements</strong> for manag<strong>in</strong>g the public–private partnership are poorly<br />
developed. However, as an <strong>in</strong>creas<strong>in</strong>g number <strong>of</strong> contracts become operational, the tools and<br />
mechanisms for manag<strong>in</strong>g public–private partnership are be<strong>in</strong>g improved. <strong>The</strong> disease control<br />
programmes have started develop<strong>in</strong>g f<strong>in</strong>ancial and logistic management mechanisms for<br />
channell<strong>in</strong>g fund<strong>in</strong>g from the government as well as the GFATM and other sources, to support<br />
the activities carried out by private <strong>sector</strong> partners. An example is the AIDS control<br />
programme, <strong>in</strong> which about two-thirds <strong>of</strong> the allocated programme funds are be<strong>in</strong>g spent<br />
through private partners. <strong>The</strong>se developments still are <strong>in</strong> prelim<strong>in</strong>ary stages, and more<br />
concerted and susta<strong>in</strong>ed efforts are required at all bureaucratic levels.<br />
Private <strong>sector</strong> partners have expressed their satisfaction with the support received dur<strong>in</strong>g<br />
plann<strong>in</strong>g, implementation and monitor<strong>in</strong>g <strong>of</strong> the project activities. However, unexpected<br />
disturbances and delays have also been reported.<br />
Legal framework and mechanisms to recourse disputes<br />
A legal framework exists to guide the contractors and contractees as well as safeguard<br />
their <strong>in</strong>terests. <strong>The</strong> general legal framework is workable and adaptable for government <strong>sector</strong><br />
partners, <strong>in</strong>clud<strong>in</strong>g the <strong>health</strong> <strong>sector</strong>. <strong>The</strong> <strong>health</strong> <strong>sector</strong> contracts are reviewed by the f<strong>in</strong>ance<br />
as well as law and justice m<strong>in</strong>istries. An example is the contract<strong>in</strong>g out <strong>of</strong> a malaria control<br />
programme study, <strong>in</strong> which the proposed fiduciary management <strong>arrangements</strong> were reviewed<br />
by the m<strong>in</strong>istries <strong>of</strong> f<strong>in</strong>ance and law and justice.<br />
210
Pakistan<br />
Each contract generally spells out the agreed mechanisms for resolv<strong>in</strong>g any disputes, if<br />
they arise, between the partners. However, the description <strong>of</strong> the proposed <strong>arrangements</strong> is not<br />
always sufficiently comprehensive to cover all dimensions <strong>of</strong> potential dispute between the<br />
partners. <strong>The</strong>re is a need for strengthen<strong>in</strong>g the capacity <strong>of</strong> managers to make effective use <strong>of</strong><br />
the current legal framework for smooth operations under the <strong>contractual</strong> environment.<br />
Capacity: strengths and weaknesses<br />
Purchaser<br />
Many national programmes (such as the AIDS control programme, tuberculosis control<br />
programme, malaria control programme, lady <strong>health</strong> workers programme), through<br />
experience, have developed <strong>arrangements</strong> for prepar<strong>in</strong>g bid details, <strong>in</strong>vit<strong>in</strong>g bids through open<br />
as well as selective bidd<strong>in</strong>g process, evaluat<strong>in</strong>g the technical and f<strong>in</strong>ancial proposals,<br />
negotiat<strong>in</strong>g the terms, prepar<strong>in</strong>g the documents and award<strong>in</strong>g the contracts.<br />
<strong>The</strong> complexity <strong>of</strong> government f<strong>in</strong>ancial procedures sometimes delay the release <strong>of</strong><br />
funds accord<strong>in</strong>g to the agreed schedules. <strong>The</strong> fiduciary management <strong>arrangements</strong> do vary<br />
across contracts. This implies programme ability to manage the diversity <strong>of</strong> f<strong>in</strong>ancial flow<br />
mechanisms across projects. An example is the AIDS control programme effectively work<strong>in</strong>g<br />
with multiple sets <strong>of</strong> f<strong>in</strong>ancial flow mechanisms, accord<strong>in</strong>g to the source <strong>of</strong> funds, e.g.<br />
government, World Bank or GFATM.<br />
Some <strong>of</strong> the programmes have started strengthen<strong>in</strong>g their staff capacity and<br />
<strong>arrangements</strong> to supervise and monitor the implementation <strong>of</strong> contracted out projects,<br />
<strong>in</strong>clud<strong>in</strong>g the f<strong>in</strong>ancial performance <strong>of</strong> projects. <strong>The</strong> programmes have also developed<br />
<strong>arrangements</strong> for design<strong>in</strong>g and conduct<strong>in</strong>g third-party evaluation and evaluation through a<br />
team <strong>of</strong> experts from with<strong>in</strong> and outside the programme.<br />
Many <strong>of</strong> the programmes, especially at prov<strong>in</strong>cial level and below, are currently<br />
work<strong>in</strong>g with a sub-optimal mix <strong>of</strong> technical and adm<strong>in</strong>istrative expertise for manag<strong>in</strong>g the<br />
contract<strong>in</strong>g process, monitor<strong>in</strong>g and evaluat<strong>in</strong>g the performance, and manag<strong>in</strong>g f<strong>in</strong>ances <strong>in</strong> a<br />
<strong>contractual</strong> environment. <strong>The</strong> limited capacity is related ma<strong>in</strong>ly to <strong>in</strong>-adequate number and<br />
skills <strong>of</strong> the programme staff, but also <strong>in</strong>cludes sub-optimal resources and operational<br />
systems. However, these capacities do vary widely across the programmes. At present the<br />
organizational development plans seem <strong>in</strong>adequate to address the capacity challenges by<br />
mak<strong>in</strong>g optimal use <strong>of</strong> potential opportunities.<br />
Provider<br />
<strong>The</strong>re is wide variation <strong>in</strong> the technical, managerial and f<strong>in</strong>ancial capacity <strong>of</strong> private<br />
<strong>sector</strong> providers. Technical capacity refers to the ability to analyse situation, develop<br />
strategies and <strong>in</strong>terventions, plan and implement activities etc. Managerial capacity refers to<br />
the ability to write proposals, negotiate contracts, manage resources <strong>in</strong>clud<strong>in</strong>g staff and<br />
materials, and prepare bus<strong>in</strong>ess plans and reports. F<strong>in</strong>ancial capacity refers to: f<strong>in</strong>ancial<br />
position <strong>in</strong>clud<strong>in</strong>g assets and <strong>in</strong>comes, f<strong>in</strong>ancial systems <strong>in</strong>clud<strong>in</strong>g account<strong>in</strong>g and audit<strong>in</strong>g,<br />
211
Pakistan<br />
f<strong>in</strong>ancial plans etc. Deficiencies <strong>in</strong> technical and managerial capacity are generally addressed,<br />
where feasible, through hir<strong>in</strong>g short-term and medium-term expert <strong>in</strong>puts. <strong>The</strong> majority <strong>of</strong><br />
private <strong>sector</strong> organizations rely ma<strong>in</strong>ly on project fund<strong>in</strong>g, which makes their long-term<br />
susta<strong>in</strong>ability less certa<strong>in</strong>. Some organizations receive supplementary <strong>in</strong>come from assets,<br />
endowment funds, and other <strong>in</strong>come-generation activities such as micro-credit and raffle<br />
schemes. <strong>The</strong> f<strong>in</strong>ancial systems generally vary accord<strong>in</strong>g to the size and scope <strong>of</strong> the<br />
organization’s work. All registered organizations are required to have their accounts audited<br />
by a qualified auditor on an annual basis.<br />
Risks and <strong>in</strong>centives<br />
Purchaser<br />
<strong>The</strong> contract<strong>in</strong>g process implies enhanced programme management capacity through<br />
staff and systems development, as well as availability <strong>of</strong> required material resources. <strong>The</strong>re is<br />
a risk that the purchaser may fail to enhance its organizational capacity for effectively<br />
manag<strong>in</strong>g the contract<strong>in</strong>g process. Weakness <strong>in</strong> the contract<strong>in</strong>g process may lead to the<br />
selection <strong>of</strong> <strong>in</strong>appropriate provider, delayed award <strong>of</strong> contract and <strong>in</strong>itiation <strong>of</strong> project<br />
activities, and conflict with the provider on size or scope <strong>of</strong> work.<br />
<strong>The</strong> complexity <strong>of</strong> fiduciary management <strong>arrangements</strong> may lead to decisions for which<br />
the purchaser can be held accountable <strong>in</strong> later stages. <strong>The</strong>re is a risk that the f<strong>in</strong>ancial<br />
procedures as agreed <strong>in</strong> the contract may conflict with government f<strong>in</strong>ancial procedures. <strong>The</strong><br />
auditors may not agree to the purchaser’s <strong>in</strong>terpretation <strong>of</strong> the f<strong>in</strong>ancial procedures followed<br />
<strong>in</strong> the <strong>contractual</strong> arrangement.<br />
<strong>The</strong> unavailability <strong>of</strong> an adequate number <strong>of</strong> potential providers may lead to a<br />
monopoly or a no-choice situation for the purchaser. As well, public <strong>sector</strong> providers may<br />
resist the idea <strong>of</strong> <strong>in</strong>volv<strong>in</strong>g private <strong>sector</strong> providers <strong>in</strong> the development and/or delivery <strong>of</strong><br />
services.<br />
Unforeseen constra<strong>in</strong>ts related to the purchaser or environment might result <strong>in</strong> the<br />
provider’s failure to deliver the agreed outputs. Purchaser-related constra<strong>in</strong>ts may <strong>in</strong>clude<br />
radical change <strong>in</strong> government priorities and policies, and delays <strong>in</strong> f<strong>in</strong>ancial flows.<br />
Environment-related constra<strong>in</strong>ts may <strong>in</strong>clude change <strong>in</strong> global, regional or country emphasis<br />
and support for <strong>contractual</strong> <strong>arrangements</strong>.<br />
<strong>The</strong> ma<strong>in</strong> <strong>in</strong>centives for the purchaser may <strong>in</strong>clude rapid expansion <strong>of</strong> services, shared<br />
load <strong>of</strong> service delivery, and improved quality <strong>of</strong> services. Expansion can refer to enhanced<br />
geographical or social access to services. An example <strong>of</strong> expanded services is the AIDS<br />
control programme contract<strong>in</strong>g out <strong>in</strong>terventions with high-risk groups. Shared load <strong>of</strong><br />
services refers to contract<strong>in</strong>g out a sub-set <strong>of</strong> services through private <strong>sector</strong> partners. An<br />
example is the Punjab Rural Support Programme shar<strong>in</strong>g the responsibility for primary<br />
<strong>health</strong> care delivery <strong>in</strong> Rahim Yar Khan district. Improved quality refers to a set <strong>of</strong> services<br />
meant to improve the quality <strong>of</strong> public <strong>sector</strong> services (e.g. microscopy quality control <strong>in</strong> a<br />
prov<strong>in</strong>ce contracted to a nongovernmental organization) as well as to avail the specialized<br />
212
Pakistan<br />
services. <strong>The</strong> specialized services may <strong>in</strong>clude communication and advocacy (e.g.<br />
communication strategy and material development for tuberculosis and malaria control<br />
programmes), systems analysis and development (e.g. tuberculosis control programme for<br />
microscopy quality control), development and conduct <strong>of</strong> tra<strong>in</strong><strong>in</strong>g (e.g. women’s <strong>health</strong><br />
project), third-party monitor<strong>in</strong>g and evaluation (e.g. rout<strong>in</strong>e immunization programme) etc.<br />
Provider<br />
Changes <strong>in</strong> the focus or management <strong>of</strong> purchasers over time may pose threats to the<br />
agreed set <strong>of</strong> provider’s activities. <strong>The</strong> purchaser may also fail to provide the agreed support,<br />
<strong>in</strong>clud<strong>in</strong>g timely release <strong>of</strong> payments, dur<strong>in</strong>g the project development and implementation.<br />
<strong>The</strong> purchaser may have a tendency to put the blame on the provider for delays <strong>in</strong> progress<br />
that are ma<strong>in</strong>ly due to purchaser-related factors.<br />
<strong>The</strong> non-availability <strong>of</strong> committed human <strong>in</strong>puts from outside the organization, due to<br />
delays <strong>in</strong> scheduled activities or other changed circumstances, may affect the provider’s<br />
ability to deliver the agreed outputs. Similarly, the non-availability <strong>of</strong> required material<br />
resources, due to changes <strong>in</strong> the market or <strong>in</strong> other circumstances <strong>in</strong>clud<strong>in</strong>g pric<strong>in</strong>g, may<br />
affect the provider’s ability to fulfil commitments <strong>in</strong> terms <strong>of</strong> quantity and quality <strong>of</strong> services.<br />
Exceptional changes <strong>in</strong> physical environment, such as those result<strong>in</strong>g from disasters and<br />
emergencies, may also affect the provider’s commitment.<br />
<strong>The</strong> providers’ failure to deliver the expected outputs, due to purchaser- or environment-<br />
related factors, may affect goodwill towards the organization which would <strong>in</strong> turn affect its<br />
prospects for future work. <strong>The</strong> client response deviation, i.e. difference from the anticipated or<br />
assumed response, may result <strong>in</strong> the provider’s failure to deliver the outputs.<br />
<strong>The</strong> ma<strong>in</strong> <strong>in</strong>centives for the provider <strong>in</strong>clude achievement <strong>of</strong> organizational goals and<br />
objectives, enhanced size and scope <strong>of</strong> work, enhanced recognition by public and private<br />
<strong>sector</strong> partners and communities, and enhanced capacity and susta<strong>in</strong>ability. An example <strong>of</strong><br />
enhanced size and scope <strong>of</strong> work is the National Rural Support Programme expand<strong>in</strong>g <strong>in</strong>to<br />
more communities and districts as well as new areas <strong>of</strong> work. An example <strong>of</strong> enhanced<br />
recognition and capacity is the Marie Adelaide Leprosy Centre, work<strong>in</strong>g with the government<br />
<strong>in</strong> AJK and the Northern Areas.<br />
Payment <strong>arrangements</strong><br />
Contract<strong>in</strong>g <strong>in</strong>, contract<strong>in</strong>g out and service contracts are the ma<strong>in</strong> types <strong>of</strong> <strong>contractual</strong><br />
<strong>arrangements</strong> used <strong>in</strong> the country. <strong>The</strong>re are occasional examples <strong>of</strong> social franchis<strong>in</strong>g and<br />
concession contract<strong>in</strong>g between the public <strong>sector</strong> purchaser and a private <strong>sector</strong> provider.<br />
<strong>The</strong> most common mode <strong>of</strong> payment <strong>in</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> Pakistan is block<br />
payment, made aga<strong>in</strong>st an agreed set <strong>of</strong> activities and outputs. However, there are examples <strong>of</strong><br />
payments to private <strong>sector</strong> providers on the basis <strong>of</strong> fee-for-service, <strong>in</strong>demnification and<br />
prepayment.<br />
213
Pakistan<br />
<strong>The</strong> block payment seems to be an appropriate payment mode under the current<br />
circumstances. In block payment, the data requirements and management efforts are relatively<br />
limited compared with other payment modes such as <strong>in</strong>demnification and fee-for-service.<br />
Block payment may be more suitable for ensur<strong>in</strong>g timely and un<strong>in</strong>terrupted availability <strong>of</strong><br />
required <strong>in</strong>puts, which <strong>in</strong> turn can affect the quality <strong>of</strong> services.<br />
Indemnification relies on the provider’s f<strong>in</strong>ancial <strong>in</strong>put for service delivery, which is<br />
then reimbursed. Organizations with a strong reserve <strong>of</strong> resources are likely to qualify;<br />
however organizations that are potentially able but have limited resources <strong>in</strong> reserve may opt<br />
not to compete for the contract. This has potential equity and quality implications.<br />
<strong>The</strong> fee-for-service payment made relies on more elaborate record-keep<strong>in</strong>g as well as<br />
advanced account<strong>in</strong>g and f<strong>in</strong>ancial management <strong>arrangements</strong>. <strong>The</strong>re are also potential<br />
difficulties <strong>in</strong> rationaliz<strong>in</strong>g the provision <strong>of</strong> services and limit<strong>in</strong>g its adm<strong>in</strong>istrative cost.<br />
Public <strong>sector</strong> managers are aware <strong>of</strong> but have a relatively limited ability to undertake<br />
cost and pric<strong>in</strong>g analysis. <strong>The</strong> national programmes have tried to carry out unit cost<strong>in</strong>g for<br />
various sub-components, and these unit costs have been used <strong>in</strong> the contract<strong>in</strong>g process. Only<br />
few larger private <strong>sector</strong> organizations have the capacity to conduct full cost and price<br />
analysis for contract<strong>in</strong>g purposes.<br />
Monitor<strong>in</strong>g and evaluation systems<br />
<strong>The</strong> Federal M<strong>in</strong>istry <strong>of</strong> Health has an <strong>in</strong>formation system <strong>in</strong> place for nationwide<br />
collection and analysis <strong>of</strong> <strong>health</strong> care delivery data from public <strong>sector</strong> facilities. This general<br />
system is also supplemented by disease-specific data collected by respective programmes, e.g.<br />
tuberculosis, malaria. <strong>The</strong> data are focused ma<strong>in</strong>ly on disease report<strong>in</strong>g and on service <strong>in</strong>put<br />
and output monitor<strong>in</strong>g. <strong>The</strong>se core data are supplemented by periodic community and <strong>health</strong><br />
surveys, e.g. <strong>in</strong>tegrated household survey. Some <strong>of</strong> the available <strong>in</strong>formation can be helpful<br />
dur<strong>in</strong>g the contract<strong>in</strong>g and implementation, <strong>in</strong> particular service delivery through government<br />
<strong>health</strong> facilities. Each contract also def<strong>in</strong>es specific <strong>in</strong>formation needs as well as <strong>arrangements</strong><br />
to monitor the performance and the outcomes by collect<strong>in</strong>g and extract<strong>in</strong>g the required<br />
<strong>in</strong>formation. However, the quality <strong>of</strong> performance <strong>in</strong>dicators and data vary across projects.<br />
<strong>The</strong>re are tools for record<strong>in</strong>g f<strong>in</strong>ancial data, and generally the records are adequate for<br />
periodic f<strong>in</strong>ancial audits.<br />
<strong>The</strong> M<strong>in</strong>istry does have <strong>arrangements</strong> to evaluate the ongo<strong>in</strong>g projects through peer<br />
review (i.e. <strong>in</strong>ternal), external review (i.e. third-party review and <strong>in</strong>ternational missions), and<br />
scientific research studies. A mix <strong>of</strong> these approaches is used <strong>in</strong> the projects, accord<strong>in</strong>g to the<br />
situation.<br />
<strong>The</strong> Federal M<strong>in</strong>istry <strong>of</strong> Health does not ma<strong>in</strong>ta<strong>in</strong> a database <strong>of</strong> private <strong>sector</strong> partners<br />
accord<strong>in</strong>g to their areas <strong>of</strong> expertise, <strong>in</strong>clud<strong>in</strong>g work<strong>in</strong>g experience. <strong>The</strong> M<strong>in</strong>istry also lacks<br />
reliable data on which to base the cost<strong>in</strong>g and pric<strong>in</strong>g analysis for contract<strong>in</strong>g. <strong>The</strong>re is no<br />
regular arrangement for collect<strong>in</strong>g data on care delivery activities or outputs <strong>of</strong> the private<br />
<strong>sector</strong> partners.<br />
214
Pakistan<br />
Case study: <strong>contractual</strong> <strong>arrangements</strong> for provision <strong>of</strong> PHC services<br />
Introduction<br />
In March 2003, a contract was signed between the Punjab Rural Support Programme<br />
(PRSP) and the District Government <strong>of</strong> Rahim Yar Khan for the efficient delivery <strong>of</strong> an<br />
agreed <strong>health</strong> services package at local basic <strong>health</strong> units (BHU). Accord<strong>in</strong>g to the agreement,<br />
104 BHUs <strong>of</strong> district Rahim Yar Khan are managed through public–private partnership with<br />
the support <strong>of</strong> the beneficiary local communities. <strong>The</strong> duration <strong>of</strong> the contract is five years.<br />
<strong>The</strong> agreement between two parties was reviewed by the <strong>health</strong>, f<strong>in</strong>ance, local government<br />
and law departments <strong>of</strong> Government <strong>of</strong> the Punjab.<br />
<strong>The</strong> 104 BHUs <strong>of</strong> district Rahim Yar Khan were taken over and assigned <strong>in</strong>to clusters <strong>in</strong><br />
July 2003. Each cluster <strong>of</strong> three BHUs has a Medical Officer In-charge. <strong>The</strong> Medical Officer<br />
was given a new contract with the PRSP with an enhanced compensatory package, along with<br />
agreement that the orig<strong>in</strong>al contract with the government is protected. <strong>The</strong> Medical Officer is<br />
required to reside at the “Focal BHU” and is not allowed to have a private practice. <strong>The</strong><br />
Medical Officer spends two days a week at each <strong>of</strong> the three BHUs <strong>in</strong> the cluster. <strong>The</strong><br />
availability and efficient management <strong>of</strong> medic<strong>in</strong>es complements the presence <strong>of</strong> a doctor.<br />
S<strong>in</strong>ce July 2003, the monthly outpatient attendance at BHUs has <strong>in</strong>creased significantly.<br />
Many collateral services are now be<strong>in</strong>g developed to supplement the grow<strong>in</strong>g outpatient<br />
service. School <strong>health</strong> programmes, immunizations and preventive <strong>in</strong>terventions are some <strong>of</strong><br />
the services that add value to the <strong>in</strong>itiative. With the <strong>in</strong>troduction <strong>of</strong> female doctors <strong>in</strong>to the<br />
service, many new vistas are expected to open. Prom<strong>in</strong>ent among these will be population<br />
plann<strong>in</strong>g services, mother and child <strong>health</strong> services and gynaecological services.<br />
Purchaser and provider<br />
<strong>The</strong> District Government <strong>of</strong> Rahim Yar Khan is a public <strong>sector</strong> organization under<br />
devolved <strong>arrangements</strong>. <strong>The</strong> elected District Assembly, led by a District Nazim, is the key<br />
decision-mak<strong>in</strong>g body <strong>in</strong> the district. <strong>The</strong> f<strong>in</strong>anc<strong>in</strong>g source is the direct government funds,<br />
without any donor <strong>in</strong>puts.<br />
<strong>The</strong> PRSP was <strong>in</strong>corporated <strong>in</strong> 1997 as a non-pr<strong>of</strong>it-mak<strong>in</strong>g organization. It is currently<br />
operat<strong>in</strong>g <strong>in</strong> 20 districts <strong>of</strong> Punjab through 8 regional <strong>of</strong>fices located at Lahore, Gujranwala,<br />
Sialkot, Faisalabad, Sargodha, Sahiwal, Multan and Muzzafargarh. <strong>The</strong> PRSP is a replication<br />
<strong>of</strong> the rural support programmes approach, proven successful <strong>in</strong> Pakistan through two decades<br />
<strong>of</strong> community organization, capacity build<strong>in</strong>g and empowerment. <strong>The</strong> process is designed<br />
around organization <strong>of</strong> poor village communities through rediscovery <strong>of</strong> community<br />
consciousness, common aspirations and ambitions before provid<strong>in</strong>g skill development,<br />
f<strong>in</strong>ancial and technical support. <strong>The</strong> purpose <strong>of</strong> such a support system is to <strong>in</strong>itiate and susta<strong>in</strong><br />
a process <strong>of</strong> diversified growth <strong>of</strong> economic, human and natural resources specifically for the<br />
poor. <strong>The</strong> ma<strong>in</strong> features <strong>of</strong> the PRSP package are:<br />
215
Pakistan<br />
Social organization<br />
Human resource development<br />
Natural resource management<br />
Physical <strong>in</strong>frastructure build<strong>in</strong>g<br />
Capital formation/sav<strong>in</strong>gs/credit<br />
L<strong>in</strong>kages (with government departments, private agencies, nongovernmental organizations).<br />
<strong>The</strong> programme acts as a support organization for whatever the community wishes to do<br />
for its own welfare. <strong>The</strong> PRSP, unlike most nongovernmental organizations, does not present<br />
any preconceived package to the community, and the delivery <strong>of</strong> support depends entirely on<br />
the identification <strong>of</strong> need by the communities themselves. Social organization is the lynchp<strong>in</strong><br />
<strong>of</strong> the PRSP approach and guarantees susta<strong>in</strong>able capacity build<strong>in</strong>g. <strong>The</strong>re are three levels at<br />
which need and <strong>in</strong>terventions are conceived: household, group and village level. <strong>The</strong><br />
communities are sensitized through “social guidance” to believe <strong>in</strong> themselves, and this<br />
process gradually leads to a po<strong>in</strong>t where the community is ready to take up responsibility for<br />
<strong>in</strong>dividual, group and village level <strong>in</strong>itiatives and become organized <strong>in</strong> the form <strong>of</strong><br />
homogenous solidarity groups or community organizations.<br />
<strong>The</strong> PRSP operates an endowment <strong>of</strong> PKR 500 million provided by the Government <strong>of</strong><br />
Punjab. With this money, PRSP secured a PKR 500 million credit l<strong>in</strong>e for delivery <strong>of</strong> microcredit<br />
to communities. Almost 100% <strong>of</strong> the PRSP fund<strong>in</strong>g comes from public sources. PRSP<br />
also <strong>in</strong>itiated a major partnership with the Pakistan Poverty Alleviation Fund (PPAF),<br />
f<strong>in</strong>anced jo<strong>in</strong>tly by the World Bank and Government <strong>of</strong> Pakistan. In the project under study,<br />
the BHU budget, other than the salaries <strong>of</strong> the permanent support and auxiliary staff, was<br />
transferred by the District Government <strong>of</strong> Rahim Yar Khan to the PRSP. In the first six years<br />
<strong>of</strong> its operations, the PRSP has generated, caused the creation <strong>of</strong> or applied significantly more<br />
than PKR 3 billion from the use <strong>of</strong> its endowment.<br />
Contract<strong>in</strong>g process and contract<br />
Basically, the PRSP has a special relationship with the government. It is more <strong>of</strong> a<br />
paragovernmental organization than a nongovernmental organization. It performs its functions<br />
<strong>in</strong> support <strong>of</strong> the government. <strong>The</strong> prov<strong>in</strong>cial government assisted <strong>in</strong> establish<strong>in</strong>g the PRSP<br />
through an endowment fund. <strong>The</strong>refore, the PRSP is a community mobilization arm <strong>of</strong> the<br />
prov<strong>in</strong>cial government.<br />
<strong>The</strong> project concept is based on the pilot experience <strong>of</strong> National Rural Support<br />
Programme (NRSP) <strong>in</strong> Lodhran district. <strong>The</strong> encourag<strong>in</strong>g results <strong>in</strong> Lodhran led the prov<strong>in</strong>cial<br />
and district government authorities to consider its replication <strong>in</strong> Rahim Yar Khan district. <strong>The</strong><br />
PRSP was the obvious choice for the Punjab government to test the rural support programme<br />
based model <strong>in</strong> a district.<br />
<strong>The</strong> agreement def<strong>in</strong>es the duties, and <strong>role</strong>s <strong>of</strong> parties, i.e. district government and<br />
PRSP. <strong>The</strong> set <strong>of</strong> services to be provided is described <strong>in</strong> broad terms, i.e. delivery <strong>of</strong> the<br />
services which are expected to be provided by the BHUs, as per national and prov<strong>in</strong>cial<br />
policies and strategies. As per agreement, the public <strong>sector</strong> monitor<strong>in</strong>g tools and systems are<br />
216
Pakistan<br />
used <strong>in</strong> the project to collect and regularly report the data on disease occurrence and service<br />
provision. Designated <strong>of</strong>ficials <strong>of</strong> the district government have the right to <strong>in</strong>spect the<br />
facilities, and the PRSP is obliged to respond to the written observations made. <strong>The</strong> agreement<br />
also requires an <strong>in</strong>dependent third party assessment <strong>of</strong> the BHU performance at the<br />
completion <strong>of</strong> first project year. <strong>The</strong> cont<strong>in</strong>uation <strong>of</strong> <strong>in</strong>terventions for the next four years is<br />
subject to improved BHU performance dur<strong>in</strong>g the first project year.<br />
As per agreement, the day-to-day operational difficulties are addressed by mutual<br />
agreement between the District Coord<strong>in</strong>ation Officer (district government) and an authorized<br />
representative <strong>of</strong> the PRSP. <strong>The</strong> resolution <strong>of</strong> disputes between the parties is addressed by<br />
referr<strong>in</strong>g the matter to a sole arbitrator, mutually acceptable to both parties. In case <strong>of</strong> failure<br />
to resolve the dispute or <strong>in</strong>ability to cont<strong>in</strong>ue, both parties have the right to term<strong>in</strong>ate the<br />
agreement through agreed <strong>arrangements</strong>.<br />
<strong>The</strong> agreement says that the BHU budget, other than the salaries <strong>of</strong> the permanent<br />
support and auxiliary staff, is transferred by the District Government to the PRSP. <strong>The</strong> annual<br />
budget <strong>in</strong>cludes the salary <strong>of</strong> doctors and other contract employees, medic<strong>in</strong>es, ma<strong>in</strong>tenance<br />
and repair <strong>of</strong> build<strong>in</strong>g and equipment, utilities, store and <strong>of</strong>fice supplies.<br />
<strong>The</strong> agreement covers the provider’s risk <strong>of</strong> <strong>in</strong>creased budget requirements for<br />
medic<strong>in</strong>es and supplies by provisions for readjustment <strong>of</strong> budget allocations by public <strong>sector</strong><br />
<strong>of</strong>ficials <strong>in</strong> light <strong>of</strong> requests or proposals by PRSP. <strong>The</strong> agreement forbids PRSP to charge a<br />
fee for the performance <strong>of</strong> the relevant management functions. However, PRSP has the right<br />
to claim reimbursement for actual costs <strong>in</strong>curred on management functions from the district<br />
government.<br />
Service package<br />
<strong>The</strong> preventive and curative <strong>health</strong> services, which the BHUs are already designated to<br />
provide, are <strong>in</strong>tended to address the local <strong>health</strong> needs. <strong>The</strong> <strong>in</strong>creased outpatient attendance<br />
reflects the relevance <strong>of</strong> services to the local <strong>health</strong> care needs. Many collateral services are<br />
now be<strong>in</strong>g developed to supplement the grow<strong>in</strong>g outpatient service. <strong>The</strong> addition <strong>of</strong> school<br />
<strong>health</strong> services (i.e. doctor’s regular visit to schools and schoolchildren’s monthly visit to<br />
BHU) and planned provision <strong>of</strong> female doctor services (for reproductive <strong>health</strong> as well as<br />
maternal and child <strong>health</strong>) are valuable additions to the set <strong>of</strong> core curative and preventive<br />
<strong>health</strong> care services at BHUs.<br />
<strong>The</strong> services are for the rural population <strong>of</strong> the entire district. <strong>The</strong> priority target group<br />
is poor women and children, for whom alternate sources <strong>of</strong> <strong>health</strong> care are <strong>in</strong>accessible. <strong>The</strong><br />
nature <strong>of</strong> the services be<strong>in</strong>g <strong>of</strong>fered is relatively more relevant to the <strong>health</strong> needs <strong>of</strong> the poor<br />
population.<br />
Monitor<strong>in</strong>g and evaluation<br />
<strong>The</strong> agreement broadly states the agreed approach to public <strong>sector</strong> monitor<strong>in</strong>g and<br />
evaluation <strong>of</strong> project performance. However, the public <strong>sector</strong> has not yet developed a set <strong>of</strong><br />
217
Pakistan<br />
specific <strong>in</strong>dicators and <strong>arrangements</strong> for monitor<strong>in</strong>g the performance <strong>of</strong> PRSP. So far the<br />
district <strong>of</strong>ficials rely on rout<strong>in</strong>e data provided by the programme, and district <strong>health</strong> <strong>of</strong>ficials<br />
have not been regular about visit<strong>in</strong>g the BHUs and provid<strong>in</strong>g written feedback, as agreed <strong>in</strong><br />
the contract. <strong>The</strong> evaluation <strong>of</strong> PRSP performance, to be conducted at the completion <strong>of</strong> the<br />
first year, was not yet due at the time <strong>of</strong> study.<br />
F<strong>in</strong>ancial management<br />
<strong>The</strong> adm<strong>in</strong>istrative and transaction cost is about one tenth <strong>of</strong> the project cost. <strong>The</strong> public<br />
<strong>sector</strong> reimburses the cost. <strong>The</strong> public <strong>sector</strong> provides the agreed f<strong>in</strong>ancial <strong>in</strong>puts as a block<br />
grant to PRSP. <strong>The</strong>re has been no delay reported <strong>in</strong> the release <strong>of</strong> funds.<br />
As a company, the PRSP is required to ma<strong>in</strong>ta<strong>in</strong> f<strong>in</strong>ancial records for audit purposes.<br />
<strong>The</strong> annual audit <strong>of</strong> accounts is conducted by a qualified audit<strong>in</strong>g firm, as required under the<br />
corporate law. <strong>The</strong> PRSP submits a copy <strong>of</strong> an annual audit report to the district government.<br />
<strong>The</strong>re has been no reported <strong>in</strong>cident <strong>of</strong> any fiduciary dispute between the PRSP and district<br />
government. However, the agreed process for dispute resolution is considered valid for<br />
fiduciary as well as other issues related to <strong>contractual</strong> <strong>arrangements</strong>.<br />
DISCUSSION<br />
<strong>The</strong> study is meant to focus on the contract<strong>in</strong>g process and experiences <strong>of</strong> the public<br />
<strong>sector</strong> purchasers and the private <strong>sector</strong> providers. <strong>The</strong> study is based ma<strong>in</strong>ly on qualitative<br />
<strong>in</strong>formation gathered from <strong>in</strong>terviews, discussions and document reviews. <strong>The</strong> scope does not<br />
<strong>in</strong>clude study <strong>of</strong> cost or quality comparisons between the services provided by the government<br />
and the private <strong>sector</strong>s, nor efficiency and equity ga<strong>in</strong>s over time.<br />
<strong>The</strong> rationale given by the public and private <strong>sector</strong> partners <strong>in</strong> Pakistan covers most <strong>of</strong><br />
the key dimensions observed <strong>in</strong> other countries. Not all the rationale cited is based on valid<br />
scientific evidence or programme experience. <strong>The</strong> issue <strong>of</strong> enhanced effectiveness and<br />
efficiency through the <strong>in</strong>troduction <strong>of</strong> market mechanisms has not emerged as an important<br />
justification for contract<strong>in</strong>g <strong>in</strong> <strong>health</strong>. Furthermore, the lack <strong>of</strong> resolution <strong>of</strong> potential equity<br />
issues and the preference for provid<strong>in</strong>g a certa<strong>in</strong> set <strong>of</strong> services require attention.<br />
In contrast to other develop<strong>in</strong>g countries, where the contract<strong>in</strong>g experience focuses<br />
more on non-cl<strong>in</strong>ical services, Pakistan has focused more on cl<strong>in</strong>ical and preventive services<br />
<strong>in</strong>clud<strong>in</strong>g primary <strong>health</strong> care.<br />
Political support seems to be reasonable at the higher level <strong>of</strong> government hierarchy.<br />
<strong>The</strong>re is a need to translate the political commitment <strong>in</strong>to a set <strong>of</strong> transparent <strong>in</strong>stitutional<br />
<strong>arrangements</strong> which can facilitate the plann<strong>in</strong>g, implementation and evaluation <strong>of</strong> <strong>health</strong><br />
<strong>in</strong>terventions through <strong>contractual</strong> <strong>arrangements</strong>. In absence <strong>of</strong> such transparent <strong>arrangements</strong>,<br />
there is a risk <strong>of</strong> <strong>in</strong>appropriate use <strong>of</strong> political <strong>in</strong>fluence <strong>in</strong> the contract<strong>in</strong>g process.<br />
Recogniz<strong>in</strong>g this, Pakistan has already started develop<strong>in</strong>g <strong>arrangements</strong> for optimiz<strong>in</strong>g these<br />
political, technical and bureaucratic <strong>in</strong>fluences. <strong>The</strong>se <strong>arrangements</strong> <strong>in</strong>clude an Inter-Agency-<br />
Coord<strong>in</strong>at<strong>in</strong>g Committee for tuberculosis and AIDS, Country Coord<strong>in</strong>at<strong>in</strong>g Mechanisms for<br />
218
Pakistan<br />
GFATM support, and a National Fortification Alliance for nutrition. <strong>The</strong> early experience with<br />
these multi-partner forums seems encourag<strong>in</strong>g.<br />
Bureaucratic support for the contract<strong>in</strong>g process has been <strong>in</strong>creas<strong>in</strong>g gradually dur<strong>in</strong>g<br />
the past few years. Multiple factors may have contributed to the change <strong>in</strong> bureaucrats’<br />
attitude <strong>in</strong>clud<strong>in</strong>g political commitment at the highest level, repeated failure <strong>of</strong> the<br />
government-only approach to <strong>health</strong> care delivery, enhanced abilities <strong>of</strong> private <strong>sector</strong>,<br />
<strong>in</strong>ternational <strong>in</strong>itiatives such as GFATM, GAIN, and GAVI. However, the bureaucratic<br />
commitment is more <strong>in</strong>dividual-based than <strong>in</strong>stitutionalized, which makes its future prospects<br />
uncerta<strong>in</strong>. <strong>The</strong>re is a need for expedit<strong>in</strong>g the development <strong>of</strong> standardized guidel<strong>in</strong>es and tools<br />
for transparent management <strong>of</strong> various <strong>health</strong> <strong>in</strong>terventions through contract<strong>in</strong>g <strong>arrangements</strong>.<br />
<strong>The</strong> general legal framework is workable and adaptable for guid<strong>in</strong>g and safeguard<strong>in</strong>g<br />
the private as well as the public <strong>sector</strong> contract<strong>in</strong>g partners <strong>in</strong> <strong>health</strong>. <strong>The</strong> f<strong>in</strong>ance as well as<br />
law and justice m<strong>in</strong>istries do assist the M<strong>in</strong>istry <strong>of</strong> Health <strong>in</strong> the contract<strong>in</strong>g process, by<br />
technically assess<strong>in</strong>g and vett<strong>in</strong>g their contracts. <strong>The</strong> agreed mechanisms for resolv<strong>in</strong>g any<br />
dispute, if arises, are generally documented <strong>in</strong> the contract. However, the description <strong>of</strong><br />
<strong>arrangements</strong> is not always detailed enough to cover all the important dimensions <strong>of</strong> potential<br />
dispute between the partners. Multiple factors that might contribute to <strong>in</strong>adequate description<br />
<strong>of</strong> dispute resolution <strong>arrangements</strong> <strong>in</strong>clude <strong>in</strong>adequate understand<strong>in</strong>g and experience <strong>of</strong><br />
partners, <strong>in</strong>fluence <strong>of</strong> private and public partners, and deficiencies <strong>in</strong> current legal and<br />
bureaucratic framework.<br />
Contract<strong>in</strong>g is meant to promote an optimal use <strong>of</strong> available resources by the private<br />
<strong>sector</strong> as a supplement, rather than a substitute, for public <strong>sector</strong> efforts. <strong>The</strong> contract<strong>in</strong>g<br />
implies enhanced capacity <strong>of</strong> the public <strong>sector</strong> to deliver its own set <strong>of</strong> services effectively as<br />
well as to support the private <strong>sector</strong> <strong>in</strong> supplement<strong>in</strong>g public <strong>sector</strong> efforts <strong>in</strong> certa<strong>in</strong> def<strong>in</strong>ed<br />
geographic or service areas. <strong>The</strong> success <strong>of</strong> contract<strong>in</strong>g and the efficiency ga<strong>in</strong>s depend on the<br />
government capacity to act as an efficient purchaser, and more specifically to decide on the<br />
need for contract<strong>in</strong>g, prepare contract related documents, support the implementation, and<br />
monitor the performance. <strong>The</strong> enabl<strong>in</strong>g process <strong>of</strong> public <strong>sector</strong> purchasers requires<br />
comprehensive analysis, plann<strong>in</strong>g, preparation and operationalization <strong>of</strong> efforts, which <strong>in</strong> turn<br />
means <strong>in</strong>vestment <strong>of</strong> time, energy and resources. Timely arrangement <strong>of</strong> the required <strong>in</strong>puts<br />
for build<strong>in</strong>g the purchaser capacity <strong>of</strong> public <strong>sector</strong> is a challenge with no simple answer. <strong>The</strong><br />
public <strong>sector</strong> organizational development plans need to address the purchaser capacity<br />
challenges at various levels by giv<strong>in</strong>g attention to areas such as plann<strong>in</strong>g, cost and price<br />
analysis, contract design and negotiation, regulatory capacity <strong>in</strong>clud<strong>in</strong>g licens<strong>in</strong>g and<br />
accreditation.<br />
<strong>The</strong>re is wide variation <strong>in</strong> the technical, managerial and f<strong>in</strong>ancial capacity <strong>of</strong> private<br />
<strong>sector</strong> providers. Based on the very limited <strong>in</strong>formation available, the number <strong>of</strong> capable<br />
private <strong>sector</strong> providers, i.e. with the right mix <strong>of</strong> strengths required for various types <strong>of</strong><br />
activities, seems relatively limited. <strong>The</strong> capacity limitation <strong>of</strong> providers can adversely affect<br />
the performance as well as the future prospects <strong>of</strong> the <strong>contractual</strong> <strong>arrangements</strong>. One key<br />
requisite for build<strong>in</strong>g private <strong>sector</strong> capacity is an “enabled public <strong>sector</strong>” for coord<strong>in</strong>at<strong>in</strong>g the<br />
219
Pakistan<br />
required support. <strong>The</strong> assessment and build<strong>in</strong>g <strong>of</strong> private <strong>sector</strong> capacity need to be <strong>in</strong>cluded<br />
and coord<strong>in</strong>ated with the public <strong>sector</strong> organizational development plans.<br />
Rapid expansion, shared load and improved quality <strong>of</strong> services are generally the stated<br />
<strong>in</strong>centives for the public <strong>sector</strong> purchasers to consider contract<strong>in</strong>g. However, the possibility <strong>of</strong><br />
important unstated motives such as personal <strong>in</strong>terest, political pressure, and technical and<br />
management <strong>in</strong>competence cannot be ruled out. Contractual <strong>arrangements</strong> do <strong>of</strong>fer certa<strong>in</strong><br />
potential <strong>in</strong>centives for the private <strong>sector</strong> providers such as enhanced size and scope <strong>of</strong> work,<br />
enhanced recognition and susta<strong>in</strong>ability. However, there are also some real risks, such as<br />
failure to achieve the targets due to purchaser <strong>in</strong>efficiencies or other environmental factors<br />
which <strong>in</strong> turn can adversely affect the prospects for future bus<strong>in</strong>ess. <strong>The</strong> availability <strong>of</strong><br />
alternate non-government purchasers <strong>of</strong> the provider’s services (i.e. donors) can alter the<br />
threshold for decid<strong>in</strong>g between the perceived <strong>in</strong>centives and the potential risks. In case <strong>of</strong><br />
purchaser competition, many competent providers may opt to stay away from the public<br />
contract<strong>in</strong>g, especially if the government <strong>arrangements</strong> are perceived as <strong>in</strong>efficient,<br />
<strong>in</strong>convenient or unreliable. Non-participation <strong>of</strong> more competent providers may adversely<br />
affect the quality <strong>of</strong> outputs achieved through <strong>contractual</strong> <strong>arrangements</strong>.<br />
<strong>The</strong> block payment, which is the usual mode <strong>of</strong> payment <strong>in</strong> <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong><br />
Pakistan, seems to be an appropriate payment mode for ensur<strong>in</strong>g timely and un<strong>in</strong>terrupted<br />
availability <strong>of</strong> required <strong>in</strong>puts. This is <strong>in</strong> contrast to the observations made <strong>in</strong> Bangladesh<br />
where a study found that contract management issues, <strong>in</strong>clud<strong>in</strong>g problems with prompt<br />
payment <strong>of</strong> contractors, procurement, and field supervision have been significant [15]. Both<br />
the public and private <strong>sector</strong>s have limited ability to carry out cost and price analysis. This<br />
limitation may lead to the purchaser purchas<strong>in</strong>g services at abnormally high rates or the<br />
provider committ<strong>in</strong>g services at very low prices. <strong>The</strong>re is evidence that under conditions <strong>of</strong><br />
<strong>in</strong>adequate f<strong>in</strong>ancial resources, contract<strong>in</strong>g may not lead to efficiency ga<strong>in</strong>s as government<br />
may focus on short term contract<strong>in</strong>g or prices may be set too low. Enhanced capacity <strong>of</strong> public<br />
and private <strong>sector</strong> partners to conduct cost and price analysis will lead to rationalized payment<br />
decisions for long-term benefits <strong>of</strong> the contract<strong>in</strong>g process.<br />
<strong>The</strong> availability and use <strong>of</strong> relevant <strong>in</strong>formation about <strong>health</strong> needs, quantity and quality<br />
<strong>of</strong> <strong>health</strong> services, cost and price <strong>of</strong> various care delivery strategies determ<strong>in</strong>es the efficiency<br />
<strong>of</strong> allocative as well as managerial decisions. <strong>The</strong> database available with the government is<br />
<strong>in</strong>adequate and needs enhancement to support the key decisions made <strong>in</strong> the contract<strong>in</strong>g<br />
process. <strong>The</strong> selection <strong>of</strong> <strong>in</strong>dicators, development and use <strong>of</strong> standardized monitor<strong>in</strong>g tools,<br />
periodic evaluation, and documentation as well as dissem<strong>in</strong>ation <strong>of</strong> early experiences with<br />
<strong>contractual</strong> <strong>arrangements</strong> will be important for further develop<strong>in</strong>g and expand<strong>in</strong>g the<br />
contract<strong>in</strong>g processes <strong>in</strong> Pakistan. To conclude, as <strong>in</strong> other countries contract<strong>in</strong>g us<strong>in</strong>g a<br />
competitive bidd<strong>in</strong>g approach is feasible <strong>in</strong> Pakistan and the experience <strong>of</strong> PRSP <strong>of</strong> manag<strong>in</strong>g<br />
primary <strong>health</strong> care, as experienced <strong>in</strong> Romania, can be scaled up to other parts <strong>of</strong> the country<br />
provided the f<strong>in</strong>al evaluation confirms the efficiency and equity ga<strong>in</strong>s [16,17].<br />
220
RECOMMENDATIONS<br />
Pakistan<br />
1. Conduct a further study cover<strong>in</strong>g the quality, effectiveness, cost-analysis, efficiency and<br />
equity aspects <strong>of</strong> the services provided through <strong>contractual</strong> <strong>arrangements</strong>.<br />
2. Assess the needs and plan for build<strong>in</strong>g capacity <strong>of</strong> public and private <strong>sector</strong> partners for<br />
effective work<strong>in</strong>g under <strong>contractual</strong> <strong>arrangements</strong>.<br />
3. Develop transparent processes and tools for award<strong>in</strong>g and manag<strong>in</strong>g contracts.<br />
4. Encourage documentation and dissem<strong>in</strong>ation <strong>of</strong> experiences with <strong>contractual</strong><br />
<strong>arrangements</strong> <strong>in</strong> the country and region.<br />
REFERENCES<br />
1. Economic survey <strong>of</strong> Pakistan 2003–2004. M<strong>in</strong>istry <strong>of</strong> F<strong>in</strong>ance, Government <strong>of</strong> Pakistan.<br />
2. Jean Perrol et al. <strong>The</strong> <strong>contractual</strong> approach: new partnerships for <strong>health</strong> <strong>in</strong> develop<strong>in</strong>g<br />
countries. Geneva, WHO, 1997. Macroeconomics, Health and Development series<br />
number 24.<br />
3. Rosen JE. Contract<strong>in</strong>g for reproductive <strong>health</strong> care: a guide. Reproductive Health<br />
<strong>The</strong>matic Group <strong>of</strong> <strong>The</strong> World Bank, December 2000)<br />
4. Mills A, Broombergs. Experiences <strong>of</strong> contract<strong>in</strong>g: an overview <strong>of</strong> literature. Geneva,<br />
World Health Organization, 1998. Macroeconomics, Health And Development series<br />
number 33.<br />
5. Hard<strong>in</strong>g A, Preker A, eds. Private participation <strong>in</strong> <strong>health</strong> services. Wash<strong>in</strong>gton DC,<br />
World Bank, 2003.<br />
6. England R. DFID, Health Systems Resource Centre, Contract<strong>in</strong>g and performance<br />
management <strong>in</strong> the <strong>health</strong> <strong>sector</strong>. April 2000.<br />
7. Punjab Health Foundation, Govt. <strong>of</strong> the Punjab, Lahore- Pakistan<br />
8. Social Welfare, Women Development and Bait-ul-Mal Punjab, Govt. <strong>of</strong> the Punjab,<br />
Lahore- Pakistan<br />
9. Northern Health Project, Memorandum <strong>of</strong> Understand<strong>in</strong>g, 1996–2000.<br />
10. Shakil S. Analysis <strong>of</strong> experience <strong>of</strong> government partnerships with non government<br />
organizations. Mutilateral Donor Support Unit for SAP/World Bank, 2002.<br />
11. Research Protocol To Evaluate <strong>The</strong> Effectiveness Of PPPs In Enhanc<strong>in</strong>g Health And<br />
Welfare Systems Development)<br />
221
Pakistan<br />
12. Report on the proceed<strong>in</strong>gs <strong>of</strong> the consultation on public private partnership <strong>in</strong> the <strong>health</strong><br />
<strong>sector</strong>, Bhurban, 10–11 October 2003. Sponsored By DFID). Available at<br />
www.idd.bham.ac.uk/serviceproviders/downloads/literature/<strong>health</strong>/pakistanppp%20<strong>health</strong>.doc<br />
13. Introduction – Punjab Rural Support Programme, Lahore-Pakistan<br />
14. Primary <strong>health</strong> care service <strong>in</strong> the rural Punjab. Lahore, PRSP (RYK), March 2004.<br />
15. Loev<strong>in</strong>sohn B. Practical issues <strong>in</strong> contract<strong>in</strong>g for primary <strong>health</strong> care delivery: lessons<br />
from two large projects <strong>in</strong> Bangladesh. Wash<strong>in</strong>gton DC, World Bank, 2002.<br />
16. Loev<strong>in</strong>sohn B. Contract<strong>in</strong>g for the delivery <strong>of</strong> primary <strong>health</strong> care <strong>in</strong> Cambodia: design<br />
and <strong>in</strong>itial experience <strong>of</strong> a large pilot-test. Wash<strong>in</strong>gton DC, World Bank, 2000.<br />
17. Vladescu C, Radulescu S. Primary <strong>health</strong> services: output-based contract<strong>in</strong>g to lift<br />
performance <strong>in</strong> Romania. Public Policy for the Private Sector, Note no. 239 Wash<strong>in</strong>gton<br />
DC, <strong>The</strong> World Bank, September 2001.<br />
222
Pakistan<br />
Annex 1<br />
GUIDELINES FOR DISCUSSION<br />
Question Discussion po<strong>in</strong>ts Source<br />
1. What is the rationale for<br />
M<strong>in</strong>istries <strong>of</strong> Health to enter<br />
<strong>in</strong>to <strong>health</strong> services contracts<br />
with nongovernmental<br />
organizations or the private<br />
<strong>sector</strong>?<br />
2. What is the <strong>in</strong>terest <strong>of</strong> the<br />
nongovernmental<br />
organizations/private <strong>sector</strong> <strong>in</strong><br />
receiv<strong>in</strong>g public <strong>sector</strong><br />
f<strong>in</strong>anc<strong>in</strong>g?<br />
3. Is the political environment<br />
enabl<strong>in</strong>g/disabl<strong>in</strong>g for the<br />
execution <strong>of</strong> <strong>contractual</strong><br />
<strong>arrangements</strong> <strong>in</strong> <strong>health</strong> <strong>sector</strong>?<br />
Does the political environment<br />
<strong>in</strong>fluence the negotiation and<br />
execution <strong>of</strong> contracts?<br />
Does the bureaucratic set-up<br />
support contract<strong>in</strong>g out <strong>of</strong><br />
services to the private <strong>sector</strong>?<br />
Is the legal framework robust<br />
enough to facilitate<br />
contract<strong>in</strong>g between the<br />
public and private <strong>sector</strong>s:<br />
Extend basic services to underserved areas<br />
Inability <strong>of</strong> to provide specific service by the public<br />
<strong>sector</strong><br />
Efficiency and effectiveness <strong>in</strong> delivery <strong>of</strong> services<br />
Why?<br />
Ownership<br />
Incentives<br />
Flexibility <strong>in</strong> decision mak<strong>in</strong>g<br />
Use <strong>of</strong> market mechanisms<br />
Weaken<strong>in</strong>g <strong>of</strong> wested <strong>in</strong>terest <strong>in</strong>fluence<br />
Functional specialization rather hierarchical tall<br />
organizational structures<br />
Role <strong>of</strong> state enabl<strong>in</strong>g rather service delivery<br />
Transparency<br />
Decentralization<br />
Distanc<strong>in</strong>g from political process<br />
Increased competition result<strong>in</strong>g <strong>in</strong> quality<br />
Challenge to established power <strong>of</strong> organized labour<br />
Dangers<br />
Equity<br />
Increased staff turnover<br />
Fulfil social mission/Enhance size and scope <strong>of</strong><br />
activities<br />
Other sources not available/accessible<br />
F<strong>in</strong>ancial susta<strong>in</strong>ability<br />
Recognition from government<br />
Enabl<strong>in</strong>g<br />
Political commitment<br />
Disabl<strong>in</strong>g<br />
Influence<br />
Explicit procedures; Comprehensiveness and<br />
transparency<br />
Process<strong>in</strong>g time<br />
Standard contract<strong>in</strong>g tool<br />
Responsibility <strong>of</strong> decision mak<strong>in</strong>g<br />
Statutes/ord<strong>in</strong>ance<br />
Frameworks developed by autonomous organizations<br />
Legal mechanisms/status <strong>of</strong> nongovernmental<br />
organizations<br />
Jo<strong>in</strong>t community contract<strong>in</strong>g<br />
Accreditation<br />
National standards<br />
223<br />
Federal<br />
Secretary<br />
DG<br />
Programme Managers<br />
DFA<br />
Law and Justice<br />
Senior Jo<strong>in</strong>t Secretary<br />
Chief Plann<strong>in</strong>g Health<br />
Registration Authorities<br />
Prov<strong>in</strong>cial<br />
DGs<br />
Plann<strong>in</strong>g Officers<br />
Organizations<br />
NRSP<br />
PRSP<br />
IPH<br />
Punjab Health Foundation<br />
Others<br />
Selected nongovernmental<br />
organizations<br />
Private hospitals?<br />
Federal and prov<strong>in</strong>cial<br />
Planners and managers/<br />
Experts <strong>in</strong> the field<br />
Federal and prov<strong>in</strong>cial<br />
Planners and managers/<br />
Experts <strong>in</strong> the field<br />
EDOs<br />
Federal and prov<strong>in</strong>cial<br />
Planers and managers/<br />
Experts <strong>in</strong> the field<br />
Federal and prov<strong>in</strong>cial<br />
Planners and managers/<br />
Experts <strong>in</strong> the field<br />
Federal Law and Justice Dept.<br />
Prov<strong>in</strong>cial Regulation Dept.<br />
Are there efficient Availability <strong>of</strong> guidel<strong>in</strong>es for arbitration <strong>of</strong> disputes Federal and prov<strong>in</strong>cial
Pakistan<br />
Question Discussion po<strong>in</strong>ts Source<br />
mechanisms to recourse <strong>in</strong> the<br />
event <strong>of</strong> a dispute between the<br />
two contract<strong>in</strong>g partners?<br />
What are the capabilities <strong>of</strong><br />
the purchaser (M<strong>in</strong>istry <strong>of</strong><br />
Health) <strong>in</strong> order to<br />
successfully enter <strong>in</strong>to a<br />
contract <strong>in</strong> terms <strong>of</strong>: (i)<br />
competitive bidd<strong>in</strong>g;<br />
(ii)award<strong>in</strong>g contracts; (iii)<br />
monitor<strong>in</strong>g and supervision;<br />
(iv) regulation; (v) payment<br />
mechanisms; (vi)performance<br />
evaluation; (vii) other<br />
aspects?<br />
What are the capabilities and<br />
experiences <strong>of</strong> the providers<br />
(private <strong>sector</strong> organizations)<br />
<strong>in</strong> terms <strong>of</strong>: (i) develop<strong>in</strong>g a<br />
proposal; (ii) technical<br />
capacity to implement; (iii)<br />
f<strong>in</strong>ancial management<br />
capacity <strong>in</strong> order to fulfil the<br />
terms <strong>of</strong> the contracts?<br />
What are the strengths and<br />
weaknesses <strong>of</strong> the purchaser<br />
(public <strong>sector</strong>) that should be<br />
taken <strong>in</strong>to consideration when<br />
enter<strong>in</strong>g <strong>in</strong>to a <strong>contractual</strong><br />
agreement?<br />
What are the strengths and<br />
weaknesses <strong>of</strong> the provider<br />
(nongovernmental<br />
organizations/private <strong>sector</strong>)<br />
that should be taken <strong>in</strong>to<br />
consideration when enter<strong>in</strong>g<br />
<strong>in</strong>to a <strong>contractual</strong> agreement?<br />
What risks and <strong>in</strong>centives<br />
does each party <strong>in</strong>cur when<br />
How def<strong>in</strong>ed, agreed Planners and managers/<br />
Experts <strong>in</strong> the field<br />
Federal Law and Justice Dept.<br />
Prov<strong>in</strong>cial Regulation Dept.<br />
Capabilities <strong>of</strong> the purchaser <strong>in</strong> terms <strong>of</strong> tra<strong>in</strong>ed<br />
human resource for project<br />
preparation/analysis/cost<strong>in</strong>g and performance <strong>of</strong><br />
follow<strong>in</strong>g activities:<br />
(i) competitive bidd<strong>in</strong>g; Development <strong>of</strong> bidd<strong>in</strong>g<br />
documents<br />
(ii)award<strong>in</strong>g contracts; project proposal assessment<br />
<strong>in</strong> terms <strong>of</strong> service-cost-quality comparability and<br />
negotiations<br />
(iii) monitor<strong>in</strong>g and supervision; resources, logistics<br />
and Information systems<br />
(iv) regulation; guidel<strong>in</strong>es, procedures<br />
(v) payment mechanisms; disbursement procedures,<br />
account<strong>in</strong>g and audit<strong>in</strong>g systems and promptness and<br />
flexibilities.<br />
(vi) performance evaluation; methods and<br />
procedures, quality assurance system development<br />
(viii) other aspects?<br />
Capabilities and experiences <strong>of</strong> the providers<br />
(i) develop<strong>in</strong>g a proposal;<br />
(ii) technical capacity<br />
Organizational structure and human resources,<br />
Operational systems, culture to adjust to public<br />
<strong>sector</strong> norms<br />
Strategic purchas<strong>in</strong>g plan<br />
Annual bus<strong>in</strong>ess plan<br />
L<strong>in</strong>k<strong>in</strong>g plans to budget<strong>in</strong>g<br />
Performance evaluation<br />
Specifications<br />
(iii) f<strong>in</strong>ancial management<br />
Strengths and weaknesses <strong>of</strong> the purchaser <strong>in</strong> terms <strong>of</strong>;<br />
Managerial<br />
Organizational/structural<br />
Human<br />
Material<br />
F<strong>in</strong>ancial /transaction costs<br />
Functional/service shar<strong>in</strong>g<br />
Credibility<br />
Level <strong>of</strong> purchaser autonomy<br />
Provider competition<br />
Incentive<br />
Strengths and weaknesses <strong>of</strong> the provider <strong>in</strong> terms <strong>of</strong>;<br />
Managerial<br />
Organizational/Structural<br />
Human<br />
Material<br />
F<strong>in</strong>ancial<br />
Functional/service provision<br />
Credibility and acceptance<br />
Timely payments/releases<br />
Bureaucratic Attitudes<br />
224<br />
Federal and prov<strong>in</strong>cial<br />
Planners and managers/<br />
Experts <strong>in</strong> the field<br />
Federal and prov<strong>in</strong>cial<br />
Planners and managers/<br />
Experts <strong>in</strong> the field<br />
Providers <strong>of</strong> Services<br />
Federal and prov<strong>in</strong>cial<br />
Planners and managers/<br />
Experts <strong>in</strong> the field<br />
Federal and prov<strong>in</strong>cial<br />
Planners and managers/<br />
Experts <strong>in</strong> the field<br />
Providers<br />
Federal and prov<strong>in</strong>cial<br />
Planners and managers/
Pakistan<br />
Question Discussion po<strong>in</strong>ts Source<br />
enter<strong>in</strong>g <strong>in</strong>to a contract? Adherence to schedules<br />
Quantity <strong>of</strong> Services<br />
Quality <strong>of</strong> Services<br />
What are the prevalent<br />
payment mechanisms <strong>of</strong> each<br />
contract? To what extent do<br />
they promote efficiency,<br />
equity, and quality? How<br />
transparent are these?<br />
Is there capacity among the<br />
public and private <strong>sector</strong> to<br />
undertake a cost and price<br />
analysis prior to negotiations?<br />
What <strong>in</strong>formation systems/<br />
sources exist <strong>in</strong> the M<strong>in</strong>istries<br />
<strong>of</strong> Health <strong>in</strong> order to<br />
successfully carry out the<br />
contract and assess<br />
performance <strong>of</strong> the contract<strong>in</strong>g<br />
private <strong>sector</strong> agency?<br />
What monitor<strong>in</strong>g mechanisms<br />
and evaluation systems are <strong>in</strong><br />
place <strong>in</strong> the public <strong>sector</strong> and<br />
what challenges exist <strong>in</strong> this<br />
area?<br />
Capitation<br />
Fee-for-service<br />
Block contracts<br />
Labour and materials<br />
Cost-and-volume contracts<br />
Cost-per-case contracts<br />
Set price<br />
Prepayment<br />
Indemnification<br />
Awareness<br />
Skilled human resource<br />
Availability <strong>of</strong> f<strong>in</strong>ances for the analysis<br />
Availability <strong>of</strong> a system/mechanism, tools and<br />
procedures<br />
Human resources<br />
F<strong>in</strong>ances<br />
Availability <strong>of</strong> a system/mechanism, tools and<br />
procedures<br />
Human resources<br />
F<strong>in</strong>ances<br />
225<br />
Experts <strong>in</strong> the field<br />
Providers<br />
Federal and prov<strong>in</strong>cial<br />
Planners and managers/<br />
Experts <strong>in</strong> the field<br />
Providers<br />
Federal and prov<strong>in</strong>cial<br />
Planners and managers/<br />
Experts <strong>in</strong> the field<br />
Providers<br />
Federal and prov<strong>in</strong>cial<br />
Planners and managers/<br />
Experts <strong>in</strong> the field<br />
Federal and Prov<strong>in</strong>cial<br />
Planers & Managers/<br />
Experts <strong>in</strong> the field
Tunisia<br />
TUNISIA
INTRODUCTION<br />
Tunisia<br />
<strong>The</strong> <strong>health</strong> <strong>in</strong>surance system <strong>in</strong> Tunisia <strong>in</strong>cludes a multitude <strong>of</strong> schemes. <strong>The</strong> legal schemes<br />
managed by social security funds cover about 2 200 000 socially <strong>in</strong>sured people and their<br />
dependents (spouses ascendants and children). Health coverage varies from one year to another,<br />
with an average rate <strong>of</strong> 5.14% (2002).<br />
With the constant aim <strong>of</strong> improv<strong>in</strong>g <strong>health</strong> care provided to the socially <strong>in</strong>sured, the social<br />
security funds have reached agreements with public, parapublic and private <strong>health</strong> care providers.<br />
Through these agreements, the socially <strong>in</strong>sured can benefit from the services provided <strong>in</strong> public or<br />
private facilities. Grow<strong>in</strong>g openness towards the private <strong>sector</strong> is reflected <strong>in</strong> the agreements<br />
between the social security funds and private hospitals.<br />
Concern to improve the quality <strong>of</strong> <strong>health</strong> coverage has driven the funds to develop a system <strong>of</strong><br />
<strong>health</strong> service contract based on lump sum settlement <strong>of</strong> fixed-cost packages cover<strong>in</strong>g the costs <strong>of</strong><br />
thermal (spa) treatment, scans, laser treatment and lithotripsy.<br />
<strong>The</strong>se agreements also cover the f<strong>in</strong>anc<strong>in</strong>g <strong>of</strong> some other, more extensive <strong>health</strong> care<br />
treatments or <strong>in</strong>vestigations:<br />
Cardiovascular surgery (<strong>in</strong> the public <strong>sector</strong>, and then extended to the private <strong>sector</strong>)<br />
Transplants (kidney, bone marrow)<br />
Magnetic Resonance Imag<strong>in</strong>g (MRI) and other medical imag<strong>in</strong>g procedures<br />
Severe burns (Military Hospital <strong>of</strong> Tunis)<br />
In this report, we describe the major agreements signed by the social security funds and the<br />
<strong>health</strong> care providers <strong>in</strong> Tunisia (public and private facilities). <strong>The</strong>se agreements make it possible<br />
for those covered by the funds to benefit from extensive <strong>health</strong> care that was not <strong>in</strong>cluded <strong>in</strong> earlier<br />
agreements. Of course, the agreements are based on the evolv<strong>in</strong>g demand for <strong>health</strong> care result<strong>in</strong>g<br />
from demographic, epidemiological and technological changes.<br />
<strong>The</strong> report provides a description <strong>of</strong> the terms <strong>of</strong> reference <strong>of</strong> these agreements as well as the<br />
expenditure <strong>of</strong> the funds <strong>in</strong> this area. It starts with a description <strong>of</strong> the Tunisian <strong>health</strong> system, then<br />
presents an evaluation <strong>of</strong> these agreements along with comments on the process.<br />
OVERVIEW OF THE TUNISIAN HEALTH SYSTEM<br />
Institutional and legal framework <strong>of</strong> the Tunisian <strong>health</strong> system<br />
<strong>The</strong> system <strong>of</strong> <strong>health</strong> care provision<br />
<strong>The</strong> current framework was def<strong>in</strong>ed by the Health Organization Law <strong>of</strong> 29 June 1991. This<br />
law set the general pr<strong>in</strong>ciples concern<strong>in</strong>g the function<strong>in</strong>g <strong>of</strong> the <strong>health</strong> system, the architecture <strong>of</strong><br />
the public and private <strong>health</strong> care facilities and their objectives and the fundamental conditions <strong>of</strong><br />
orientation <strong>of</strong> the <strong>health</strong> system by the authorities <strong>in</strong> charge and the advisory bodies that have been<br />
set up.<br />
227
Tunisia<br />
Health care is provided by public, parapublic and private <strong>health</strong> care facilities. <strong>The</strong> public<br />
<strong>health</strong> facilities are usually classified accord<strong>in</strong>g to three levels: primary, secondary and tertiary.<br />
Primary level comprises basic <strong>health</strong> centres and district hospitals. Basic <strong>health</strong> centres provide<br />
preventive care and curative <strong>health</strong> care services as well as <strong>health</strong> education for:<br />
Treatment <strong>of</strong> common diseases<br />
Mother and child care, <strong>in</strong>clud<strong>in</strong>g family plann<strong>in</strong>g<br />
Prevention and control <strong>of</strong> communicable and <strong>in</strong>fectious diseases, particularly through immunization<br />
Pre-school, school and university medical services<br />
Dissem<strong>in</strong>ation <strong>of</strong> hygiene pr<strong>in</strong>ciples and practices and rules relat<strong>in</strong>g to environmental protection<br />
through <strong>health</strong> education<br />
Collection and use <strong>of</strong> epidemiological and statistical <strong>health</strong> data.<br />
At the end <strong>of</strong> 2000, there were 1981 basic <strong>health</strong> care centres throughout the country with a<br />
national average <strong>of</strong> 1 centre per 4826 population.<br />
District hospitals, beside the services similar to those <strong>of</strong> the basic <strong>health</strong> centres, also provide<br />
general, maternity and emergency services, and have hospital beds. At the end <strong>of</strong> 2002, there were<br />
106 district and maternity hospitals with a total capacity <strong>of</strong> 2711 beds.<br />
<strong>The</strong> secondary level comprises regional hospitals that provide specialized medical and<br />
surgical care, <strong>in</strong> addition to those services mentioned for primary, or first-l<strong>in</strong>e, facilities. Every<br />
county town has one or two regional hospitals, which makes a total number <strong>of</strong> 32 hospitals and<br />
5126 beds for Tunisia as a whole.<br />
<strong>The</strong> tertiary level comprises the university-oriented <strong>health</strong> facilities which, while shar<strong>in</strong>g<br />
some attributes with first-l<strong>in</strong>e and second-l<strong>in</strong>e facilities, have as their primary objective to provide<br />
high specialized care, graduate and post-graduate education <strong>of</strong> <strong>health</strong> personnel as well as to<br />
develop research <strong>in</strong> the medical, pharmaceutical and dental areas.<br />
Almost all <strong>of</strong> these third-l<strong>in</strong>e <strong>in</strong>stitutions have the legal status <strong>of</strong> public <strong>health</strong> <strong>in</strong>stitutions, as<br />
specified <strong>in</strong> the Health Organization Law and def<strong>in</strong>ed <strong>in</strong> detail <strong>in</strong> a specific decree issued on<br />
2 December 1991, grant<strong>in</strong>g autonomy to these facilities <strong>in</strong> their adm<strong>in</strong>istrative and f<strong>in</strong>ancial<br />
management, as with public facilities. <strong>The</strong>y are 20 such <strong>in</strong>stitutions. <strong>The</strong> number <strong>of</strong> departments <strong>in</strong><br />
these teach<strong>in</strong>g hospitals is 177 with 40 specialties totall<strong>in</strong>g 8305 beds (2002).<br />
In total, there are 167 public <strong>health</strong> facilities under the supervision <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Public<br />
Health with a capacity <strong>of</strong> 16 142 beds (1.69 beds per 1000 population).<br />
Another component <strong>of</strong> the public <strong>sector</strong>, although <strong>of</strong>ten called parapublic, comprises<br />
ambulatory care centres that are under the supervision <strong>of</strong> public bodies for their affiliated members<br />
or salaried employees. <strong>The</strong>se are ma<strong>in</strong>ly the private general hospitals <strong>of</strong> the National Social<br />
Security Fund (six private general hospitals).<br />
<strong>The</strong> development <strong>of</strong> the public <strong>health</strong> care provision system is guided by the “<strong>health</strong> map”<br />
established by the M<strong>in</strong>istry <strong>of</strong> Public Health. This map, which is updated at the beg<strong>in</strong>n<strong>in</strong>g <strong>of</strong> every<br />
national development plan, determ<strong>in</strong>es the territorial areas and <strong>health</strong> <strong>sector</strong>s where <strong>health</strong> care and<br />
228
Tunisia<br />
hospital facilities may be established. <strong>The</strong>se directions are usually based on the trend <strong>of</strong> the demand<br />
for care, result<strong>in</strong>g from demographic, epidemiological and technological changes.<br />
<strong>The</strong> private <strong>health</strong> facilities are classified accord<strong>in</strong>g to the Health Organization Law <strong>in</strong>to four<br />
categories:<br />
multidiscipl<strong>in</strong>ary private hospitals (polycl<strong>in</strong>ics) (43 private hospitals with a capacity <strong>of</strong> 1835 beds <strong>in</strong><br />
2002)<br />
s<strong>in</strong>gle-discipl<strong>in</strong>ary private hospitals (cl<strong>in</strong>ics) (27 private hospitals with a capacity <strong>of</strong> 184 beds <strong>in</strong><br />
2002)<br />
private practice <strong>of</strong>fices (3293 <strong>of</strong>fices with a ratio <strong>of</strong> 2903 population per <strong>of</strong>fice <strong>in</strong> 2002).<br />
Health coverage system<br />
In Tunisia, the structure <strong>of</strong> <strong>health</strong> coverage theoretically allows the <strong>in</strong>clusion <strong>of</strong> the entire<br />
population, regardless <strong>of</strong> <strong>in</strong>come, social category or place <strong>of</strong> residence. This is a fundamental<br />
pr<strong>in</strong>ciple <strong>of</strong> the Tunisian <strong>health</strong> policy, the effective implementation <strong>of</strong> which is the driv<strong>in</strong>g force<br />
beh<strong>in</strong>d the reforms regularly undertaken <strong>in</strong> this area.<br />
Currently, the <strong>health</strong> care coverage is managed by three major categories <strong>of</strong> facilities: a) social<br />
security funds; b) the State; and c) the mutual <strong>in</strong>surance companies and group or private <strong>in</strong>surance.<br />
a) <strong>The</strong> social security funds<br />
<strong>The</strong> National Pension and Social Security Fund (CNRPS) covers all public <strong>sector</strong> employees<br />
(state and public bodies), <strong>in</strong>clud<strong>in</strong>g retired employees. It provides a compulsory legal scheme and<br />
an optional scheme. <strong>The</strong> compulsory legal scheme provides two exclusive options for <strong>health</strong><br />
coverage:<br />
Option 1: reimbursement limited to long illness and surgical operations, for which or private <strong>health</strong><br />
care providers can be used.<br />
Option 2: <strong>health</strong> card scheme provid<strong>in</strong>g full coverage (long illness, surgery and common diseases) <strong>in</strong><br />
M<strong>in</strong>istry <strong>of</strong> Public facilities.<br />
<strong>The</strong> additional, optional scheme is f<strong>in</strong>anced by additional contributions made by the affiliated<br />
members (3%) and their employ<strong>in</strong>g <strong>in</strong>stitutions (1.5%). This scheme allows those hav<strong>in</strong>g opted for<br />
the reimbursement system to be reimbursed for expenses <strong>in</strong>curred for common diseases.<br />
<strong>The</strong> National Social Security Fund (CNSS) covers, <strong>in</strong> addition to employees <strong>of</strong> the private<br />
<strong>sector</strong>, other categories <strong>of</strong> the population such as students, workers abroad and, recently, selfemployed<br />
workers.<br />
Its compulsory scheme is based on the <strong>health</strong> card system, and allows its affiliates to have<br />
access to public <strong>health</strong> facilities and to benefit from the services provided <strong>in</strong> the private general<br />
hospitals <strong>of</strong> the Fund itself.<br />
In return for the services provided to its affiliates <strong>in</strong> the <strong>health</strong> facilities under the supervision<br />
<strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Public Health, the Fund makes lump sum payments to the Treasury, participates<br />
229
Tunisia<br />
<strong>in</strong> the <strong>in</strong>vestment <strong>of</strong> these facilities and, s<strong>in</strong>ce 1996, has made bill payments. This last mode <strong>of</strong><br />
payment was <strong>in</strong>troduced first <strong>in</strong> the university teach<strong>in</strong>g hospitals. S<strong>in</strong>ce 1999, it has been gradually<br />
extended to regional hospitals.<br />
<strong>The</strong> cont<strong>in</strong>ued growth <strong>of</strong> <strong>health</strong> care needs has pushed the social security funds to diversify<br />
their <strong>in</strong>terventions and coverage for some specialized services, under agreements with public or<br />
private <strong>in</strong>stitutions: cardiology and cardiovascular surgery, kidney transplants, CAT scan, magnetic<br />
resonance imag<strong>in</strong>g, lithotripsy, bone marrow transplant, heart transplant, haemodialysis procedures,<br />
spa treatment and functional rehabilitation, medical devices, prostheses, medic<strong>in</strong>es and care abroad.<br />
b) <strong>The</strong> State’s contribution to <strong>health</strong> coverage<br />
Some segments <strong>of</strong> the population benefit either from free <strong>health</strong> care and hospitalization <strong>in</strong><br />
public facilities or from reduced fees. This is stipulated <strong>in</strong> the Health Organization Law and detailed<br />
<strong>in</strong> decrees, orders and specific circulars for implementation. Ambulatory care and hospitalization<br />
are entirely free <strong>of</strong> charge for any citizen considered destitute and for his/her family.<br />
It concerns ma<strong>in</strong>ly <strong>in</strong>dividuals and families <strong>in</strong> need who benefit from permanent assistance<br />
under the follow<strong>in</strong>g programmes:<br />
National Programme <strong>of</strong> Assistance to families <strong>in</strong> need, def<strong>in</strong>ed as those families with <strong>in</strong>come below<br />
the poverty l<strong>in</strong>e, equivalent to 8.3% <strong>of</strong> the population <strong>in</strong> 2002 (162 650 families).<br />
Programme <strong>of</strong> assistance for deprived elderly people liv<strong>in</strong>g <strong>in</strong> their families, which <strong>in</strong>volves 3225<br />
elderly people (2002).<br />
Programme <strong>of</strong> assistance for disabled people, unable to work, which <strong>in</strong>volves 3456 people.<br />
<strong>The</strong> free <strong>health</strong> care scheme also concerns children without family support, <strong>in</strong>clud<strong>in</strong>g:<br />
Children resid<strong>in</strong>g at the National Institute for the Protection <strong>of</strong> Childhood<br />
Children liv<strong>in</strong>g <strong>in</strong> units managed by other associations for the protection <strong>of</strong> children under agreement<br />
with National Institute<br />
Children liv<strong>in</strong>g <strong>in</strong> foster families that cannot afford to provide them with <strong>health</strong> coverage.<br />
<strong>The</strong> benefit <strong>of</strong> reduced costs for <strong>health</strong> care and hospitalization <strong>in</strong> public facilities is granted<br />
to some categories <strong>of</strong> households with limited <strong>in</strong>come. <strong>The</strong> criteria take <strong>in</strong>to consideration both the<br />
<strong>in</strong>come level and the size <strong>of</strong> the family. Other categories <strong>of</strong> the population benefit from <strong>health</strong> care<br />
and hospitalization <strong>in</strong> public facilities entirely free <strong>of</strong> charge. <strong>The</strong>y are ma<strong>in</strong>ly:<br />
persons covered with<strong>in</strong> the framework <strong>of</strong> scientific research and prevention campaigns or those<br />
suffer<strong>in</strong>g from epidemic diseases.<br />
certa<strong>in</strong> pr<strong>of</strong>essional categories who benefit from the full <strong>health</strong> coverage <strong>in</strong> the <strong>in</strong>stitutions under the<br />
supervision <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Public Health or <strong>in</strong> facilities specific to them; they are the<br />
personnel <strong>of</strong> the army, national security forces, customs, and <strong>health</strong> personnel and veterans.<br />
c) Mutual <strong>in</strong>surance companies and group <strong>in</strong>surance<br />
<strong>The</strong> mutual <strong>in</strong>surance companies provide optional <strong>health</strong> coverage and accompanies the legal<br />
obligation <strong>of</strong> affiliation with the Social Security Fund. Mutual <strong>in</strong>surance companies are governed by<br />
230
Tunisia<br />
the regulations <strong>of</strong> the mutual benefit associations go<strong>in</strong>g back to 1954, and are <strong>in</strong> conformity with a<br />
standard statute set up <strong>in</strong> 1961. Currently, there are 50 mutual <strong>in</strong>surance companies and 130 000<br />
affiliated members. <strong>The</strong> resources <strong>of</strong> the mutual <strong>in</strong>surance companies come from contributions <strong>of</strong><br />
the affiliated members, which usually range from 1% to 7% <strong>of</strong> their gross salaries, and subsidies<br />
from adm<strong>in</strong>istrations and enterprises that vary accord<strong>in</strong>g to cases.<br />
Group <strong>in</strong>surance covers the personnel <strong>of</strong> enterprises <strong>in</strong> the public and private <strong>sector</strong>s on a<br />
<strong>contractual</strong> basis. <strong>The</strong>se companies are governed by the <strong>in</strong>surance code, and the resources also<br />
come from the salaried employees and the employers’ contributions.<br />
<strong>The</strong> contribution rate ranges from 6% to 15% accord<strong>in</strong>g to the contracts. This rate is shared<br />
between the employer and the employee. <strong>The</strong> employer’s share varies between 67% and 80% and<br />
the employee’s share ranges from 20% to 33%. <strong>The</strong> number <strong>of</strong> affiliates reached 200 000 <strong>in</strong> 2001.<br />
<strong>The</strong> extent <strong>of</strong> <strong>health</strong> coverage by mutual <strong>in</strong>surance and group <strong>in</strong>surance companies varies; it<br />
depends on <strong>in</strong>ternal regulations for the mutual <strong>in</strong>surance companies and on the clauses <strong>of</strong> the policy<br />
for group <strong>in</strong>surance.<br />
Support to the <strong>health</strong> system<br />
In order to ensure the proper function<strong>in</strong>g <strong>of</strong> the <strong>health</strong> care system and its susta<strong>in</strong>ability,<br />
Tunisia regards the development <strong>of</strong> support <strong>sector</strong>s considered to be strategic, particularly, the<br />
<strong>sector</strong>s <strong>of</strong> education and <strong>of</strong> the pharmaceutical <strong>in</strong>dustry.<br />
<strong>The</strong> medical education <strong>sector</strong><br />
At present, Tunisia has:<br />
4 medical faculties, which provide basic medical and specialty education <strong>in</strong> more than 40 medical<br />
specialties.<br />
3 schools <strong>of</strong> science and technology which tra<strong>in</strong> senior <strong>health</strong> technicians <strong>in</strong> more than 10 specialties.<br />
19 nurs<strong>in</strong>g schools, distributed throughout the country.<br />
<strong>The</strong> pharmaceutical <strong>sector</strong><br />
This <strong>sector</strong>, which is considered to be strategic <strong>in</strong> terms <strong>of</strong> secur<strong>in</strong>g medic<strong>in</strong>e supply and<br />
reduc<strong>in</strong>g its cost, has greatly developed over the past 10 years. <strong>The</strong> number <strong>of</strong> units produc<strong>in</strong>g<br />
medic<strong>in</strong>es <strong>in</strong>creased from 3 <strong>in</strong> 1987 to 27 <strong>in</strong> 1999; this resulted <strong>in</strong> an <strong>in</strong>crease <strong>in</strong> the rate <strong>of</strong><br />
coverage <strong>of</strong> needs by local production from 7.6% <strong>in</strong> 1987 to 43.7% <strong>in</strong> 1999. Accompany<strong>in</strong>g the<br />
development <strong>of</strong> the pharmaceutical <strong>in</strong>dustry, was the establishment <strong>of</strong> <strong>in</strong>frastructure for quality<br />
control, particularly the national laboratory for control <strong>of</strong> drugs and the drug monitor<strong>in</strong>g centre,<br />
which performs test<strong>in</strong>g before licens<strong>in</strong>g and at the market<strong>in</strong>g (systematic control <strong>of</strong> batches) and<br />
post-market<strong>in</strong>g stages.<br />
Other support actions<br />
Apart from the education and pharmaceutical <strong>in</strong>dustry, several actions were carried out or are<br />
be<strong>in</strong>g implemented as essential support to the system. <strong>The</strong>se <strong>in</strong>clude establish<strong>in</strong>g a computer centre<br />
231
Tunisia<br />
<strong>in</strong> the M<strong>in</strong>istry <strong>of</strong> Health, which is an important element for structur<strong>in</strong>g the <strong>health</strong> <strong>in</strong>formation<br />
system, and re-structur<strong>in</strong>g the National Centre for Biomedical Ma<strong>in</strong>tenance which is now an expert<br />
unit serv<strong>in</strong>g the M<strong>in</strong>istry <strong>of</strong> Health.<br />
2.4 Resources allocated to the <strong>health</strong> system<br />
F<strong>in</strong>ancial resources<br />
<strong>The</strong> trend <strong>in</strong> overall <strong>health</strong> expenditures is characterized by a steady <strong>in</strong>crease, from about 574<br />
million Tunisian d<strong>in</strong>ars (TND) <strong>in</strong> 1990 to approximately 1670 <strong>in</strong> 2002 and 1821 <strong>in</strong> 2003.<br />
In the early 1990s, overall <strong>health</strong> expenditures represented about 4.5% <strong>of</strong> the GDP, and then<br />
start<strong>in</strong>g from 1994, a markedly more rapid progression than that <strong>of</strong> the GDP brought it to an<br />
average level <strong>of</strong> about 5.6% (2002). Per capita expenditure <strong>in</strong> current d<strong>in</strong>ars rose from about 70 <strong>in</strong><br />
1990 to about 105.5 <strong>in</strong> 1995, 150.5 <strong>in</strong> 2000 and 180.0 <strong>in</strong> 2003.<br />
With<strong>in</strong> this overall trend, important changes have affected the structure <strong>of</strong> <strong>health</strong> care<br />
f<strong>in</strong>anc<strong>in</strong>g. <strong>The</strong>y concern ma<strong>in</strong>ly the respective <strong>role</strong>s <strong>of</strong> out-<strong>of</strong>-pocket payment by the state’s<br />
beneficiaries and the social security funds. As from 1990, there has been a steady decl<strong>in</strong>e <strong>in</strong> the<br />
share f<strong>in</strong>anced by the state to reach about 23.9 <strong>in</strong> 2003, result<strong>in</strong>g <strong>in</strong> an average annual growth rate<br />
<strong>of</strong> 8.2% (1995–2000), lower than that <strong>of</strong> the total expenditure.<br />
<strong>The</strong> share <strong>of</strong> the social security funds has steadily <strong>in</strong>creased from about 15% <strong>in</strong> 1990 up to<br />
about 20% <strong>in</strong> 2000 (22.5% <strong>in</strong> 2003), <strong>in</strong>creas<strong>in</strong>g at an average annual rate <strong>of</strong> 12.5%.<br />
<strong>The</strong> gradual adjustment <strong>of</strong> the contributions <strong>of</strong> these two major funds has started from the<br />
beg<strong>in</strong>n<strong>in</strong>g <strong>of</strong> 2000 with the revaluation <strong>of</strong> the lump sum contribution made by the funds to the<br />
public <strong>health</strong> budget for <strong>health</strong> care provided to their affiliates <strong>in</strong> public facilities, along with the<br />
reform <strong>of</strong> hospital management. However, a much more substantial change has taken place with the<br />
<strong>in</strong>troduction <strong>of</strong> s<strong>in</strong>gle-act bill<strong>in</strong>g <strong>in</strong> public <strong>health</strong> facilities. This will expand with the extension <strong>of</strong><br />
this mechanism to regional hospitals.<br />
Other approaches <strong>of</strong> the social security funds have also contributed to <strong>in</strong>creas<strong>in</strong>g their share <strong>in</strong><br />
the <strong>health</strong> care f<strong>in</strong>anc<strong>in</strong>g:<br />
Specific agreements for the coverage <strong>of</strong> some diseases <strong>in</strong>creased from about TND 2 million <strong>in</strong> 1990 to<br />
TND 19 million <strong>in</strong> 2000.<br />
<strong>The</strong> coverage <strong>of</strong> some <strong>health</strong> care categories (haemodialysis, devices, care abroad, spa treatment)<br />
<strong>in</strong>creased dur<strong>in</strong>g the same period from TND 23 to 61 million.<br />
Other direct actions, notably <strong>health</strong> care <strong>in</strong> the CNSS private general hospitals and reimbursements<br />
made by the CNRPS, <strong>in</strong>creased from TND 12 to 32 million and from TND 9 to 24 million,<br />
respectively, between 1990 and 2000.<br />
<strong>The</strong> contributions <strong>of</strong> mutual <strong>in</strong>surance companies, private <strong>in</strong>surance companies and enterprise<br />
services have also <strong>in</strong>creased rapidly, at an average annual rate <strong>of</strong> 13%. However, they rema<strong>in</strong><br />
marg<strong>in</strong>al compared with total expenditure.<br />
Out-<strong>of</strong>-pocket household expenditure has <strong>in</strong>creased at a rate that is slightly more rapid than<br />
total expenditure, estimated at an average <strong>of</strong> 10.3% per annum. However, the <strong>in</strong>crease <strong>of</strong> out-<strong>of</strong>-<br />
232
Tunisia<br />
pocket household expenditure <strong>in</strong> <strong>health</strong> care has been relatively more susta<strong>in</strong>ed throughout the<br />
second half <strong>of</strong> the 1990s, br<strong>in</strong>g<strong>in</strong>g this share to about 49.1% <strong>in</strong> 2000 and 52.3% <strong>in</strong> 2003.<br />
<strong>The</strong> regular <strong>in</strong>crease <strong>of</strong> f<strong>in</strong>ancial resources allocated to <strong>health</strong> care reflects a larger<br />
consideration <strong>of</strong> the demand for <strong>health</strong> care and the efforts to meet this demand <strong>in</strong> the best<br />
conditions. However, it also leads to concern over br<strong>in</strong>g<strong>in</strong>g expenditure under control and manag<strong>in</strong>g<br />
<strong>health</strong> care with a maximum <strong>of</strong> efficiency while safeguard<strong>in</strong>g equity <strong>of</strong> access to <strong>health</strong> care. As<br />
mentioned earlier, this is a major objective <strong>of</strong> <strong>health</strong> and social policies, present <strong>in</strong> all the reforms <strong>of</strong><br />
<strong>health</strong> care and <strong>health</strong> <strong>in</strong>surance systems.<br />
Health facilities<br />
<strong>The</strong> <strong>health</strong> <strong>in</strong>frastructure has steadily developed throughout the past decade for the different<br />
categories <strong>of</strong> <strong>health</strong> centres: first-l<strong>in</strong>e, second-l<strong>in</strong>e or highly specialized <strong>health</strong> care provided <strong>in</strong><br />
specialized centres and university teach<strong>in</strong>g hospitals. This represents an important prerequisite for<br />
improv<strong>in</strong>g the citizens’ access to <strong>health</strong> care throughout the country and for all the segments <strong>of</strong> the<br />
population.<br />
This development <strong>of</strong> <strong>health</strong> facilities was accompanied by structural adjustments with<strong>in</strong> the<br />
system <strong>of</strong> <strong>health</strong> care provision, reflect<strong>in</strong>g the objectives <strong>of</strong> the reforms be<strong>in</strong>g implemented dur<strong>in</strong>g<br />
the past ten years. This <strong>in</strong>volved readjust<strong>in</strong>g the respective <strong>role</strong>s <strong>of</strong> the public and private <strong>sector</strong>s<br />
and target<strong>in</strong>g their efforts and their <strong>in</strong>terventions. Thus, whereas the public <strong>sector</strong> hospitalization<br />
capacity has <strong>in</strong>creased very little (especially <strong>in</strong> the specialized centres and the university teach<strong>in</strong>g<br />
hospitals), from about 15 400 beds <strong>in</strong> 1989 to about 16 142 beds <strong>in</strong> 2002, the private <strong>sector</strong> capacity<br />
more than doubled dur<strong>in</strong>g the same period, from 950 to 2040 beds.<br />
On the whole, the comb<strong>in</strong>ed actions <strong>of</strong> both <strong>sector</strong>s have stabilized the average overall<br />
<strong>in</strong>dicator <strong>of</strong> the number <strong>of</strong> beds per 1000 <strong>in</strong>habitants at 1.9, with a total number <strong>of</strong> 18 182 beds<br />
(2002).<br />
At the same time, it is clear that public efforts have substantially extended the regional and<br />
basic coverage. <strong>The</strong> number <strong>of</strong> regional and district hospitals <strong>in</strong>creased from 24 and 98 <strong>in</strong> 1989 to<br />
32 and 106 <strong>in</strong> 2002, respectively, and the network <strong>of</strong> basic <strong>health</strong> centres expanded from about 1300<br />
centres <strong>in</strong> 1987 to 1981 <strong>in</strong> 2002 (4826 people per centre <strong>in</strong> 2002).<br />
This <strong>in</strong>crease <strong>in</strong> the number <strong>of</strong> places provid<strong>in</strong>g basic and specialized services is also clear <strong>in</strong><br />
the private <strong>sector</strong>. <strong>The</strong> number <strong>of</strong> private s<strong>in</strong>gle and multidiscipl<strong>in</strong>ary private hospitals grew from<br />
28 <strong>in</strong> 1989 to 70 <strong>in</strong> 2002, as well as the number <strong>of</strong> dialysis centres, <strong>health</strong> laboratories, and<br />
radiology units. <strong>The</strong> total number <strong>of</strong> private practice <strong>of</strong>fices <strong>in</strong>creased from about 2800 <strong>in</strong> 1992 to<br />
more than 3293 <strong>in</strong> 2002, and pharmacy dispensaries <strong>in</strong>creased from 1087 <strong>in</strong> 1992 to 1392 <strong>in</strong> 2002.<br />
Human resources<br />
Along with the <strong>health</strong> <strong>in</strong>frastructure and the facilities and technical resources related to it,<br />
human resources are a major component <strong>of</strong> the <strong>health</strong> system. Ultimately, the performance <strong>of</strong> the<br />
system depends largely on the knowledge, skills and motivations <strong>of</strong> those <strong>in</strong> charge <strong>of</strong> <strong>health</strong> care<br />
provision. Given the <strong>health</strong> needs, the social priorities and the expectations <strong>of</strong> care seekers, all the<br />
know-how <strong>in</strong> the management <strong>of</strong> human potential lies <strong>in</strong> achiev<strong>in</strong>g and ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g several<br />
233
Tunisia<br />
balances: proper specialty mix; consistency <strong>of</strong> the structure <strong>of</strong> the personnel (medical, paramedical,<br />
technical and adm<strong>in</strong>istrative); balance <strong>in</strong> the geographical distribution; and match<strong>in</strong>g competencies<br />
and functions. <strong>The</strong> system <strong>of</strong> basic and cont<strong>in</strong>u<strong>in</strong>g education makes a crucial contribution towards<br />
reach<strong>in</strong>g these balances; the same holds for the organization <strong>of</strong> remunerations and <strong>in</strong>centives.<br />
<strong>The</strong>se concerns for appropriate education and efficient management <strong>of</strong> human resources<br />
(Table 1) are strongly emphasized, as mentioned earlier, <strong>in</strong> the national programmes for the <strong>health</strong><br />
<strong>sector</strong> reform. <strong>The</strong>y contribute, along with the relevant quantitative <strong>in</strong>dicators, to reflect the efforts<br />
made and actions undertaken for strengthen<strong>in</strong>g and promot<strong>in</strong>g <strong>health</strong> personnel.<br />
Table 1. Human resources <strong>in</strong> the Tunisian <strong>health</strong> system, 2002<br />
Category Private <strong>sector</strong> Public <strong>sector</strong> Total<br />
Physicians 3297 4147 7444<br />
Dentists 940 375 1315<br />
Pharmacists 1614 337 1951<br />
Paramedical personnel 726 27 392 28 118<br />
<strong>The</strong> overall <strong>in</strong>dicators underl<strong>in</strong>e the steady and substantial improvement <strong>of</strong> medical<br />
∗<br />
supervision. <strong>The</strong> population per physicianTP PT decreased steadily from about 1900 <strong>in</strong> 1990 to 1100 <strong>in</strong><br />
2000; so, for 1000 population, we had 0.5 physicians <strong>in</strong> 1990 and 0.9 physicians <strong>in</strong> 2000. This<br />
improvement is found both <strong>in</strong> the public and private <strong>sector</strong>s. <strong>The</strong> population per public <strong>sector</strong><br />
physician decreased from about 3100 <strong>in</strong> 1990 to approximately 2100 <strong>in</strong> 2000. For private practice<br />
physicians, this ratio decreased from about 4750 to approximately 2300 dur<strong>in</strong>g the same period.<br />
Paramedical supervision rema<strong>in</strong>s exclusively limited to the public <strong>sector</strong>, with a population per<br />
paramedic <strong>of</strong> about 340. Indeed, the private <strong>sector</strong> has only 726 staff belong<strong>in</strong>g to this category <strong>of</strong><br />
human resources, compared with 27 147 <strong>in</strong> the public <strong>sector</strong> (June 2000). Conversely, the number<br />
<strong>of</strong> dentists and pharmacists has substantially <strong>in</strong>creased <strong>in</strong> the private <strong>sector</strong>, from 684 and 1087 <strong>in</strong><br />
1992 to 928 and 1508 <strong>in</strong> 2000, respectively, i.e. an average annual growth <strong>of</strong> 3.9% and 4.2%<br />
respectively.<br />
2.5 Performance <strong>in</strong>dicators <strong>of</strong> the <strong>health</strong> system<br />
<strong>The</strong> assessment <strong>of</strong> the performance <strong>of</strong> a <strong>health</strong> system aims at evaluat<strong>in</strong>g the actions<br />
undertaken with<strong>in</strong> the framework <strong>of</strong> <strong>health</strong> policies, i.e. to which extent the objectives set <strong>in</strong> these<br />
policies have been achieved.<br />
This concerns ma<strong>in</strong>ly the degree <strong>of</strong> improvement <strong>in</strong> the population’s <strong>health</strong> status and the<br />
conditions <strong>of</strong> such improvement, particularly <strong>in</strong> organizational and f<strong>in</strong>ancial terms. It <strong>in</strong>volves<br />
address<strong>in</strong>g not only the costs <strong>of</strong> <strong>health</strong> care services, but also the responsiveness <strong>of</strong> the <strong>health</strong><br />
system and its capacity to meet patient demands, and to anticipate changes <strong>in</strong> demand result<strong>in</strong>g<br />
from demographic and socioeconomic factors or even those caused by major unexpected events. It<br />
also <strong>in</strong>volves assess<strong>in</strong>g the accessibility <strong>of</strong> <strong>health</strong> care by all the segments <strong>of</strong> the population, i.e. the<br />
equity <strong>of</strong> the <strong>health</strong> system.<br />
∗ Includ<strong>in</strong>g dentists; if dentists are excluded, the population/physician ratio is 1284 (Source DEP/MSP)<br />
234
Tunisia<br />
<strong>The</strong> Tunisian <strong>health</strong> strategy, as expressed <strong>in</strong> the programmes carried out and reforms under<br />
way, follows this approach and aims at develop<strong>in</strong>g ways for its comprehensive implementation.<br />
With<strong>in</strong> this framework, certa<strong>in</strong> data are regularly produced on the ma<strong>in</strong> to assess results <strong>of</strong> the<br />
<strong>health</strong> policy.<br />
<strong>The</strong> basic demographic <strong>in</strong>dicators highlight a steady improvement <strong>of</strong> the overall <strong>health</strong> status<br />
and the decrease <strong>in</strong> the disease burden.<br />
Life expectancy at birth has <strong>in</strong>creased from an average <strong>of</strong> 67.4 years <strong>in</strong> 1984 to 72.9 years <strong>in</strong> 2002.<br />
This <strong>in</strong>crease is greater for women, who ga<strong>in</strong>ed about 6 years dur<strong>in</strong>g the period 1984–1999,<br />
than for men who ga<strong>in</strong>ed 4 years. It is true that the <strong>in</strong>crease has levelled <strong>of</strong>f <strong>in</strong> the past few<br />
years, most probably call<strong>in</strong>g for expansion <strong>of</strong> <strong>health</strong> care coverage. <strong>The</strong> probabilities <strong>of</strong> death<br />
before 60 and 40 years <strong>of</strong> age also illustrate this tendency and gender differences.<br />
After a cont<strong>in</strong>ued decl<strong>in</strong>e dur<strong>in</strong>g the 1960s, 1970s and 1980s, the overall mortality rate has stabilized<br />
around 5.6%. Accord<strong>in</strong>g to demographic projections, it should rema<strong>in</strong> at this level until 2015,<br />
when age<strong>in</strong>g <strong>of</strong> the population will start to show substantially and lead to an <strong>in</strong>crease <strong>in</strong> overall<br />
mortality rates.<br />
<strong>The</strong> targeted programmes on reproductive <strong>health</strong>, mother and child <strong>health</strong> and family plann<strong>in</strong>g<br />
that are <strong>in</strong>tegrated with<strong>in</strong> basic <strong>health</strong> centres have achieved very tangible and quite outstand<strong>in</strong>g<br />
results.<br />
<strong>The</strong> <strong>in</strong>fant mortality rate (per 1000 live births) was reduced from 60.5 <strong>in</strong> 1995 to 26 <strong>in</strong> 1998 (23.4%<br />
for girls and 29% for boys).<br />
For children under 5 years, the mortality rate is 31.5 (28.4 for girls and 34.6 for boys).<br />
<strong>The</strong> percentage <strong>of</strong> one-year-old children immunized is 96%–97%. Immunization programmes have<br />
been strengthened, with a view to elim<strong>in</strong>at<strong>in</strong>g measles and susta<strong>in</strong><strong>in</strong>g poliomyelitis eradication.<br />
In addition to the 6 target diseases identified by WHO, the national Expanded Programme on<br />
Immunization also <strong>in</strong>cludes the rout<strong>in</strong>e immunization <strong>of</strong> children aga<strong>in</strong>st viral hepatitis.<br />
<strong>The</strong> rate <strong>of</strong> low birth weight for neonates was 5.4% <strong>in</strong> 1999; the rate <strong>of</strong> oral rehydration therapy use<br />
reached nearly 95% at the same period.<br />
Care <strong>of</strong> pregnant women has improved: the number <strong>of</strong> those hav<strong>in</strong>g at least one antenatal visit<br />
exceeded 85% <strong>of</strong> the total <strong>in</strong> 1999; the proportion <strong>of</strong> attended deliveries <strong>in</strong> hospitals and private<br />
hospitals also <strong>in</strong>creased, reach<strong>in</strong>g over 90%. <strong>The</strong> proportion <strong>of</strong> pregnant women with anaemia<br />
was about 32% <strong>in</strong> 1999.<br />
<strong>The</strong> impact <strong>of</strong> the family plann<strong>in</strong>g policy is apparent through several key <strong>in</strong>dicators. <strong>The</strong><br />
contraceptive prevalence rate, which was about 59.7% <strong>in</strong> 1994 <strong>in</strong>creased to 65.5% <strong>in</strong> 1999. <strong>The</strong><br />
total fertility rate decreased to 2.09 <strong>in</strong> 1999 compared with 2.7% <strong>in</strong> 1995. <strong>The</strong> crude birth rate<br />
decreased from 25.2% <strong>in</strong> 1990 to 16.9% <strong>in</strong> 1999. Stabilization <strong>of</strong> the mortality rate has resulted <strong>in</strong> a<br />
slow<strong>in</strong>g down <strong>of</strong> population growth, with the growth rate decreas<strong>in</strong>g from 1.96% <strong>in</strong> 1990 to 1.12%<br />
<strong>in</strong> 1999. Accord<strong>in</strong>g to demographic projections, this rate will range from 0.8% to 1.05% <strong>in</strong> 2004<br />
and from 0.6 to 1.03% <strong>in</strong> 2009, depend<strong>in</strong>g on the tempo <strong>of</strong> fertility changes.<br />
<strong>The</strong> communicable disease report<strong>in</strong>g system confirms the eradication <strong>of</strong> several diseases<br />
caus<strong>in</strong>g major <strong>health</strong> problems <strong>in</strong> the past, such as malaria, schistosomiasis and cholera. <strong>The</strong><br />
surveillance system has been strengthened so as to ma<strong>in</strong>ta<strong>in</strong> these achievements and prevent the<br />
<strong>in</strong>troduction <strong>of</strong> emerg<strong>in</strong>g or re-emerg<strong>in</strong>g diseases. <strong>The</strong> national programmes and prevention and<br />
235
Tunisia<br />
control <strong>in</strong>terventions are provided with specific systems for permanent data collection to allow for<br />
epidemiological surveillance <strong>of</strong> diseases such as malaria, schistosomiasis, HIV/AIDS, rabies,<br />
tuberculosis, leishmaniasis and leprosy.<br />
CONTRACTUAL ARRANGEMENTS<br />
History<br />
<strong>The</strong> Tunisian <strong>health</strong> system has made extensive use <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> s<strong>in</strong>ce 1970,<br />
when the social security funds and the public <strong>health</strong> care providers agreed upon the payment <strong>of</strong> a<br />
lump sum to the Treasury for <strong>health</strong> care provided to their affiliate members and their dependents.<br />
This process <strong>of</strong> contract<strong>in</strong>g has greatly developed <strong>in</strong> the past decade, with the objective <strong>of</strong> manag<strong>in</strong>g<br />
the relationships between the <strong>health</strong> <strong>in</strong>surance (social security) and the <strong>health</strong> care providers (both<br />
public and private) and to br<strong>in</strong>g together the <strong>of</strong>ten conflict<strong>in</strong>g <strong>in</strong>terests <strong>of</strong> these two actors.<br />
Several extensive <strong>health</strong> care and specialized services are not provided for <strong>in</strong> the <strong>in</strong>itial<br />
agreements made between the social security funds and the M<strong>in</strong>istry <strong>of</strong> Public Health. Most <strong>of</strong> these<br />
services are the subject <strong>of</strong> later agreements and memoranda <strong>of</strong> understand<strong>in</strong>g with the M<strong>in</strong>istry <strong>of</strong><br />
Public Health and are adhered to by some private specialized care <strong>in</strong>stitutions and the Military<br />
Hospital. <strong>The</strong>se agreements are useful as there is no act or decree allow<strong>in</strong>g the socially <strong>in</strong>sured to<br />
receive <strong>health</strong> care <strong>in</strong> private <strong>health</strong> facilities.<br />
Legal foundations<br />
Generally, the M<strong>in</strong>istry <strong>of</strong> Social Affairs and Solidarity (MASS) establishes the agreement<br />
with the M<strong>in</strong>istry <strong>of</strong> Public Health or the Military Hospital attached to the M<strong>in</strong>istry <strong>of</strong> Defence. <strong>The</strong><br />
private facilities are only adherents to the agreement. <strong>The</strong> legal foundations <strong>of</strong> these agreements are<br />
shown <strong>in</strong> Table 2.<br />
Table 2. Distribution <strong>of</strong> agreements<br />
Subject <strong>of</strong> the agreement Service providers concerned by the agreement Year <strong>of</strong> signature<br />
Cardiovascular <strong>in</strong>tervention 1- MASS, MSP (2002) and the Military Hospital <strong>of</strong> Tunis 1995<br />
- Taoufik Private Hospital 1991<br />
- Bergé du Lac Private Hospital 2000<br />
- Cardiovascular Surgery Private Hospital 1995<br />
- Social Security Private Hospital, Sousse 1997<br />
- El Basat<strong>in</strong>e Private Hospital 2000<br />
- El Manar Private Hospital 1997<br />
- Chams Private Hospital, Sfax 2000<br />
- Ibn El Neffis Private Hospital, Sfax 2000<br />
- El Korniche Private Hospital, Sousse 2003<br />
2- MASS, MSP : Public Facilities only 2001<br />
Heart transplant MASS and Tunis Military Hospital 1998<br />
Services <strong>of</strong> myocardial<br />
MASS and Tunis Military Hospital 2000<br />
sc<strong>in</strong>tigraphy Mejdi El Mahrsi Radiology and Nuclear Medic<strong>in</strong>e Centre 2002<br />
Kidney transplant MASS, MSP and the Tunis Military Hospital 2002<br />
236
Table 2. Distribution <strong>of</strong> agreements<br />
Tunisia<br />
Subject <strong>of</strong> the agreement Service providers concerned by the agreement Year <strong>of</strong> signature<br />
Lithotripsy<br />
Scanner<br />
MASS and MSP 1995<br />
- El Manar Private Hospital 1998<br />
- El Menzah Private Hospital 1998<br />
- Abou Libaba El Ansari Private Hospital, Gabès 2000<br />
- Social Security Private Hospital, Sfax 2002<br />
- Hamouda El Aouani Private Hospital, Kairouan 2003<br />
MASS, MSP and Tunis Military Hospital 1995<br />
- El Kef Centre <strong>of</strong> Radiology 2001<br />
- Dr Anis Chebbi Radiology and scanner Centre 2002<br />
- El Nakhil private Hospital, Gafsa 2003<br />
- Ceres Centre, Bizerte 2001<br />
- Jendouba Radiology Centre 2002<br />
- Beja Radiology Centre 2003<br />
Bone marrow ransplant MASS and MSP (Bone marrow Transplant Centre) 1998<br />
MRI<br />
MASS and MSP 1996<br />
- El Manar Private Hospital (IMS company) 2003<br />
- Tunis Centre, Soukra 2003<br />
- Tunis Military Hospital 2001<br />
Major burns Social Security Funds and Military Hospital 1993<br />
<strong>The</strong>rmal cures<br />
Social Security Funds and the M<strong>in</strong>eral Waters Agency 1997<br />
- Djebel Oust Centre<br />
- Korbous Centre<br />
- Hammam Bourguiba <strong>The</strong>rmal Centre<br />
Functional rehabilitation<br />
- Djerbal <strong>The</strong>rmal Centre<br />
CSS and the Djebel Oust Pr<strong>of</strong>essional Rehabilitation Centre 1993 and 1997<br />
Haemodialysis MASS and MSP 2001<br />
Details <strong>of</strong> implementation <strong>of</strong> the agreements<br />
Every agreement covers specific <strong>health</strong> care services, whether for the CNSS or the CNRPS.<br />
<strong>The</strong> affiliate members <strong>of</strong> both funds are eligible for coverage for all <strong>health</strong> care services provided <strong>in</strong><br />
the terms <strong>of</strong> the agreements. <strong>The</strong> conditions for benefits vary accord<strong>in</strong>g to several criteria, as<br />
detailed below.<br />
<strong>The</strong> CNRPS agreements<br />
Whatever the scheme <strong>of</strong> the <strong>health</strong> care coverage (<strong>health</strong> cards or reimbursement), the affiliate<br />
is entitled to direct coverage for certa<strong>in</strong> services such as lithotripsy, scann<strong>in</strong>g, bone marrow<br />
transplant, kidney transplant, cardiovascular <strong>in</strong>terventions, thermal treatments, Magnetic Resonance<br />
Imag<strong>in</strong>g, heart transplant and haemodialysis. Most <strong>of</strong> these services have been the subject <strong>of</strong><br />
memoranda <strong>of</strong> agreement with the M<strong>in</strong>istry <strong>of</strong> Public Health, to which some private specialized<br />
<strong>health</strong> care facilities have been party. Except where otherwise noted,coverage for the procedures<br />
listed below requires a file <strong>in</strong>clud<strong>in</strong>g an application for prior approval filled by the affiliate member<br />
237
Tunisia<br />
and the attend<strong>in</strong>g physician, and the adm<strong>in</strong>istrative documents <strong>of</strong> the beneficiary concern<strong>in</strong>g the<br />
coverage. <strong>The</strong> latter must not be affiliated with another social security or social welfare scheme.<br />
This application should be submitted to the regional centre that is nearest to the affiliate member’s<br />
residence. <strong>The</strong> coverage can only be granted upon the advice <strong>of</strong> the CNRPS medical committee.<br />
• Lithotripsy. Coverage is provided for any treatment for kidney stones that does not require a<br />
surgical procedure.<br />
• Computerized axial tomography. <strong>The</strong> CNRPS covers the expenses <strong>of</strong> computerized axial<br />
tomography (CT) scan procedures performed for the socially <strong>in</strong>sured <strong>in</strong> public <strong>health</strong> facilities<br />
on a lump sum basis cover<strong>in</strong>g all the operations related to this procedure. Coverage <strong>in</strong>cludes<br />
expenses for CT scans <strong>of</strong> the skull and <strong>of</strong> other parts <strong>of</strong> the body.<br />
• Bone marrow transplant. Coverage by the CNRPS is provided for bone marrow transplant<br />
performed at the National Centre for Bone Marrow Transplant <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Public Health.<br />
Coverage for bone marrow transplant requires the constitution <strong>of</strong> a file <strong>in</strong>clud<strong>in</strong>g: an application<br />
for prior approval on a special form provided by the National Centre for Bone Marrow<br />
Transplant, filled by the affiliate member and the attend<strong>in</strong>g physician.<br />
• Kidney transplant <strong>in</strong>terventions. Coverage <strong>in</strong>cludes the medical procedures related to the<br />
cl<strong>in</strong>ical, biological and radiological preparations <strong>of</strong> the donor and the recipient, the surgical<br />
procedures <strong>of</strong> removal and transplant as well as the cl<strong>in</strong>ical, biological and radiological followup,<br />
length <strong>of</strong> stay and post-surgical care. Coverage can only be granted upon the advice <strong>of</strong> the<br />
CNRPS medical committee.<br />
• Cardiovascular surgical <strong>in</strong>terventions. Coverage <strong>in</strong>cludes cardiovascular surgical procedures<br />
performed <strong>in</strong> public <strong>health</strong> facilities and hospitals, <strong>in</strong> Tunis Military Hospital as well as <strong>in</strong> the<br />
private facilities that adhere to the memorandum <strong>of</strong> agreement made between the M<strong>in</strong>istry <strong>of</strong><br />
Social Affairs and the M<strong>in</strong>istry <strong>of</strong> Public Health. Specific procedures covered are:<br />
Open-heart <strong>in</strong>terventions<br />
Vascular <strong>in</strong>terventions <strong>of</strong> arterial restoration with or without prosthesis<br />
Open-heart <strong>in</strong>terventions requir<strong>in</strong>g cardiopulmonary bypass, <strong>in</strong>strumental dilatation, arterial<br />
dilatation, <strong>in</strong>sertion <strong>of</strong> <strong>in</strong>tracardiac or <strong>in</strong>travascular material, costs <strong>of</strong> pre-surgical<br />
<strong>in</strong>vestigations and post-surgical care, upon the advice <strong>of</strong> the CNRPS medical<br />
committee.<br />
• <strong>The</strong>rmal (spa) treatment. Coverage <strong>in</strong>cludes medical procedures relat<strong>in</strong>g to thermal cures<br />
(rheumatology and otorh<strong>in</strong>olaryngology), medical visits and accommodation expenses <strong>in</strong> hotels.<br />
Coverage is provided to a limit <strong>of</strong> 85% <strong>of</strong> care expenses, plus a ceil<strong>in</strong>g <strong>of</strong> TND 8.5 per<br />
overnight stay. <strong>The</strong> thermal treatment centres are:<br />
thermal centre <strong>of</strong> Hamman Bourguiba<br />
thermal centre <strong>of</strong> Korbous<br />
<strong>health</strong> complex <strong>of</strong> Djebel Oust<br />
thermal centre <strong>of</strong> Djerba<br />
Coverage for thermal care requires the submission <strong>of</strong> an application made on a special “ST”<br />
form, filled by the affiliate member and the attend<strong>in</strong>g physician.<br />
• Magnetic Resonance Imag<strong>in</strong>g (MRI). Coverage is provided for MRI procedures performed <strong>in</strong><br />
the follow<strong>in</strong>g facilities:<br />
Centre <strong>of</strong> Bab Sâadoun (Tunis)<br />
Tunis Military Hospital<br />
Habib Bourguiba Hospital (Sfax)<br />
Sahloul Hospital ( Sousse)<br />
238
Tunisia<br />
Coverage <strong>of</strong> MRI procedures requires the submission <strong>of</strong> an application made on a special<br />
form available <strong>in</strong> the above-mentioned facilities.<br />
• Heart transplant. Coverage <strong>of</strong> heart transplant expenses is provided to the socially <strong>in</strong>sured<br />
undergo<strong>in</strong>g treatment <strong>in</strong> Tunis Military Hospital. This coverage <strong>in</strong>cludes: the cost <strong>of</strong> cl<strong>in</strong>ical,<br />
biological and radiological preparations <strong>of</strong> the donor and recipient; the surgical procedures<br />
(removal and transplant); and the cl<strong>in</strong>ical, biological and radiological follow-up as well as the<br />
treatment <strong>of</strong> possible complications dur<strong>in</strong>g the first year and the immunosuppressive treatment<br />
dur<strong>in</strong>g the first year. Coverage <strong>of</strong> heart transplant requires: an application for prior approval<br />
submitted on a special form provided by Tunis Military Hospital.<br />
• Haemodialysis. In order to get coverage for haemodialysis sessions, the affiliate member hould<br />
submit to the CNRPS. An application for prior approval made on a special form available <strong>in</strong> one<br />
<strong>of</strong> the follow<strong>in</strong>g hospitals:<br />
Charles Nicole Hospital<br />
<strong>The</strong> Military Hospital (Tunis)<br />
Fattouma Bourguiba Hospital (Monastir)<br />
Hédi Chaker Hospital ( Sfax)<br />
Also necessary are a written request specify<strong>in</strong>g the haemodialysis centre selected by the<br />
patient, and an application for coverage <strong>of</strong> long illness made on a special form provided by the<br />
CNRPS.<br />
2<br />
<strong>The</strong> CNSSTP PT agreements<br />
Except where otherwise specified, coverage requires a file consist<strong>in</strong>g <strong>of</strong> an application made<br />
on a CNSS form, and a medical report. Prior approval is usually required before the procedure is<br />
provided.<br />
<strong>The</strong> conditions to be eligible for coverage vary accord<strong>in</strong>g to the socio-pr<strong>of</strong>essional status <strong>of</strong><br />
the person <strong>in</strong>sured; <strong>in</strong> general the requirements for prior approval areas follows:<br />
Retirees: must be a recipient <strong>of</strong> a pension from the CNSS.<br />
Salaried employees from the non-farm <strong>sector</strong>: must have accrued 50 days <strong>of</strong> work dur<strong>in</strong>g the past two<br />
terms or 80 days <strong>of</strong> work dur<strong>in</strong>g the past 4 terms preced<strong>in</strong>g submission <strong>of</strong> the application.<br />
Salaried employees from the farm <strong>sector</strong>: must have paid contributions for at least one term dur<strong>in</strong>g the<br />
2 terms preced<strong>in</strong>g the submission <strong>of</strong> application or contributions for at least two terms dur<strong>in</strong>g<br />
the 4 terms preced<strong>in</strong>g submission <strong>of</strong> the application.<br />
Non wage-earn<strong>in</strong>g workers: must have paid contributions for at least 2 terms dur<strong>in</strong>g the 4 terms<br />
preced<strong>in</strong>g submission <strong>of</strong> the application.<br />
Workers abroad: (not covered by a social security bilateral agreement) must have paid contributions<br />
for at least 2 terms dur<strong>in</strong>g the 4 terms preced<strong>in</strong>g submission <strong>of</strong> the application.<br />
Students under 28 years: must hold a valid student card dur<strong>in</strong>g the current academic year.<br />
Students over 28 years or married: must be registered at the CNSS.<br />
Some categories <strong>of</strong> workers with low <strong>in</strong>come must have paid contributions for at least 3 months <strong>in</strong> the<br />
2 months preced<strong>in</strong>g submission <strong>of</strong> the application.<br />
A socially <strong>in</strong>sured person’s spouse: must not have a pr<strong>of</strong>essional activity or social coverage.<br />
2 For the two social security funds, the agreements relate to the same services for the different conditions/diseases covered.<br />
239
Tunisia<br />
A dependent child: must be a m<strong>in</strong>or or an orphan under 20 years <strong>of</strong> age or disabled without any paid<br />
activity (without age limit) or a girl without any <strong>in</strong>come and unmarried (without age limit).<br />
A socially <strong>in</strong>sured person’s ascendant beneficiary: must be dependent upon the socially <strong>in</strong>sured<br />
person.<br />
Conditions <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong><br />
<strong>The</strong> agreements are governed by criteria for coverage required to be fulfilled by the recipient<br />
(beneficiary) and by conditions to be met by the signatory <strong>health</strong> facilities, particularly private ones.<br />
<strong>The</strong> criteria for coverage vary accord<strong>in</strong>g to the CNSS or the CNRPS.<br />
In order to conclude an agreement with the M<strong>in</strong>istry <strong>of</strong> Social Affairs and Solidarity, private<br />
<strong>in</strong>stitutions are obliged to accept the follow<strong>in</strong>g conditions.<br />
Reimbursement is made on the basis <strong>of</strong> a flat rate determ<strong>in</strong>ed at the level <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Public<br />
Health.<br />
Private facilities are committed not to <strong>in</strong>crease these rates and to require no payment from the patient<br />
covered under the agreements.<br />
For cardiovascular <strong>in</strong>terventions, a def<strong>in</strong>ition <strong>of</strong> requirements has recently been established<br />
concern<strong>in</strong>g only private <strong>in</strong>stitutions.<br />
<strong>The</strong> public or private facilities are subject to a medical <strong>in</strong>spection, provided for <strong>in</strong> the agreements. <strong>The</strong><br />
<strong>in</strong>spection concerns the hospitalization and treatment conditions <strong>of</strong> the CNSS <strong>in</strong>sured patients.<br />
In order for an affiliate who applies for coverage to receive <strong>health</strong> care under the <strong>contractual</strong><br />
<strong>arrangements</strong>, the follow<strong>in</strong>g conditions should be met.<br />
Prior approval <strong>of</strong> the social security fund medical committee is mandatory, except for emergencies.<br />
A request from the hospital is required and should be <strong>in</strong> accordance with the form developed by the<br />
social security funds. It should be accompanied by a medical report describ<strong>in</strong>g the patient’s<br />
<strong>health</strong> condition and his/her need for care. For every agreement, the social security funds have<br />
devised an application form for prior approval.<br />
Resources <strong>in</strong>volved <strong>in</strong> implementation<br />
Contributions <strong>of</strong> the social security funds<br />
<strong>The</strong> agreements are divided <strong>in</strong>to two categories: the first category concerns the funds’<br />
contribution to the f<strong>in</strong>anc<strong>in</strong>g <strong>of</strong> the public <strong>in</strong>stitutions provid<strong>in</strong>g <strong>health</strong> care to their affiliate<br />
members. Three forms <strong>of</strong> f<strong>in</strong>anc<strong>in</strong>g are currently applied: strengthen<strong>in</strong>g <strong>of</strong> public <strong>health</strong> <strong>in</strong>stitutions,<br />
contribution to the budgets <strong>of</strong> the regional hospitals and the system <strong>of</strong> bill<strong>in</strong>g.<br />
<strong>The</strong> second category concerns the coverage <strong>of</strong> <strong>health</strong> care services provided by parties under<br />
contract with the social security funds, the M<strong>in</strong>istry <strong>of</strong> Public Health, the Military Hospital and the<br />
private <strong>health</strong> <strong>in</strong>stitutions.<br />
Tables 3 and 4 show the trend <strong>of</strong> social security fund contributions to the M<strong>in</strong>istry <strong>of</strong> Public<br />
Health dur<strong>in</strong>g the period 1995–2004.<br />
Table 3. Trend <strong>of</strong> social security fund contributions to the f<strong>in</strong>anc<strong>in</strong>g <strong>of</strong> public <strong>health</strong> facilities<br />
240
under the agreements, 1995–2004<br />
Tunisia<br />
Scheme 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004<br />
Contribution to CNSS 43.5 43.5 43.5 43.5 43.5 43.5 43.5 43.5 43.5 43.5<br />
the State budget CNRPS 11.0 11.0 11.0 11.0 11.0 11.00 11.0 11.0 11.0 11.0<br />
Direct<br />
contribution to<br />
the budgets <strong>of</strong><br />
Regional<br />
Hospitals<br />
Bill<strong>in</strong>g system<br />
Total 54.5 54.5 54.5 54.5 54.5 54.5 54.5 54.5 54.5 54.5<br />
CNSS 0.5 0.5 0.5 0.5 3.6 8.3 21.1 30.1 41.6 47.660<br />
CNRPS 0.3 0.3 0.3 0.3 1.2 2.7 6.9 9.9 12.4 14.340<br />
Total 0.8 0.8 0.8 0.8 4.8 11.0 28.0 40.0 54.0 62.000<br />
CNSS 2.6 10.7 18.8 26.5 33.3 37.3 48.5 62.3 75.0 81.200<br />
CNRPS 1.7 3.6 5.4 7.8 9.0 10.7 13.5 17.7 21.0 21.800<br />
Total 4.3 14.3 24.3 34.3 42.3 48.0 62.0 80.0 96.0 103.0<br />
Table 4. Trend <strong>of</strong> social security fund total contributions, 1995-2004<br />
Year 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004<br />
CNSS 46.5 54.6 62.8 70.4 103.9 102.4 113.1 135.9 160.1 172.3<br />
CNRPS 13.0 14.9 16.7 19.1 27.1 27.7 31.4 38.6 44.4 47.1<br />
Total 59.5 69.5 79.5 89.5 130.9 130.1 144.5 174.5 204.5 219.4<br />
<strong>The</strong> strengthen<strong>in</strong>g <strong>of</strong> public <strong>health</strong> <strong>in</strong>stitutions has taken place s<strong>in</strong>ce 1990, follow<strong>in</strong>g an<br />
agreement made between the M<strong>in</strong>istry <strong>of</strong> Social Affairs and Solidarity and the M<strong>in</strong>istry <strong>of</strong> Public<br />
Health. This agreement aims at improv<strong>in</strong>g hospital care and reduc<strong>in</strong>g the need for <strong>health</strong> care<br />
abroad.<br />
Two types <strong>of</strong> <strong>in</strong>terventions have been implemented. <strong>The</strong>y help ensure f<strong>in</strong>anc<strong>in</strong>g <strong>of</strong> the<br />
<strong>in</strong>frastructure and purchase <strong>of</strong> medical equipment and new technology. <strong>The</strong> first <strong>in</strong>tervention is a<br />
contribution <strong>of</strong> 55 million d<strong>in</strong>ars for the period 1990–1994, distributed annually: 20 million for<br />
1990–1991, 24 million for 1992–1993 and 11 million for 1993–1994. <strong>The</strong> second <strong>in</strong>tervention<br />
co<strong>in</strong>cided with the N<strong>in</strong>th Development Plan. <strong>The</strong> two funds have contributed 50 million d<strong>in</strong>ars, 40<br />
million <strong>of</strong> which are supported by the CNSS for strengthen<strong>in</strong>g public <strong>health</strong> <strong>in</strong>stitutions.<br />
In total, the contribution <strong>of</strong> the social security funds has <strong>in</strong>creased at an average annual rate <strong>of</strong><br />
30%.<br />
<strong>The</strong> National Social Security Fund (CNSS)<br />
For the period 1987–2001, the CNSS spent 345.8 million d<strong>in</strong>ars for all the <strong>health</strong> care<br />
provided under agreements; 72% <strong>of</strong> this expenditure was for coverage <strong>of</strong> haemodialysis sessions.<br />
Haemodialysis expenses <strong>in</strong>creased at an average annual rate <strong>of</strong> 21%.<br />
Cardiovascular <strong>in</strong>terventions have accounted for 18% <strong>of</strong> total expenditure by the CNSS on<br />
<strong>health</strong> care provided under the agreements. Dur<strong>in</strong>g the period 1988–2001, cardiovascular surgery<br />
expenses <strong>in</strong>creased at an average annual rate <strong>of</strong> 43.3%.<br />
241
Tunisia<br />
<strong>The</strong>re has been a significant <strong>in</strong>crease <strong>in</strong> the number <strong>of</strong> persons benefit<strong>in</strong>g from <strong>health</strong> care<br />
provided under the agreements. <strong>The</strong> number <strong>of</strong> beneficiaries for cardiovascular <strong>in</strong>terventions has<br />
<strong>in</strong>creased from 24 to 14 016 (1988–2001). For the scanner, this number reached 58 100 <strong>in</strong> 2001<br />
compared with 171 <strong>in</strong> 1988.<br />
Accord<strong>in</strong>g to Table 5, the policy <strong>of</strong> reduc<strong>in</strong>g the need for care abroad, which was the reason<br />
for adopt<strong>in</strong>g <strong>contractual</strong> <strong>arrangements</strong>, has been successful. In 15 years, the number <strong>of</strong> beneficiaries<br />
receiv<strong>in</strong>g <strong>health</strong> care abroad has been reduced about n<strong>in</strong>efold. <strong>The</strong> CNSS expenses have been<br />
reduced by 3.5 million d<strong>in</strong>ars, without adjust<strong>in</strong>g for <strong>in</strong>ternational <strong>in</strong>flation but with coverage<br />
ma<strong>in</strong>ta<strong>in</strong>ed at a high level.<br />
S<strong>in</strong>ce 1987 the largest share <strong>of</strong> expenses for <strong>health</strong> care provided under agreements for<br />
haemodialysis sessions. Haemodialysis expenses exceed 60% <strong>of</strong> total expenditure dur<strong>in</strong>g the period<br />
1987–2001. <strong>The</strong> gradual <strong>in</strong>crease <strong>of</strong> cardiovascular surgery expenses, from 2.7% <strong>in</strong> 1988 to 20.7%<br />
<strong>in</strong> 2001, is also noted.<br />
242
Tunisia<br />
Table 5. Beneficiaries (BEN) and expenses (EXP) under CNSS agreements, 1987–2001T (million d<strong>in</strong>ars)<br />
Agreements Year 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001<br />
Cardiovascular BEN 24 35 35 62 513 735 819 966 1396 1331 1585 1930 2057 2528<br />
surgery EXP 0.100 0.250 0.422 1.012 2.009 3.054 3.224 3.929 6.022 6.147 7.132 8.732 9.296 10.793<br />
Kidney transplant BEN 13 5 12 4 9 15 9 21 27 9 25 46 20 8<br />
EXP 0.060 0.084 0.060 0.152 0.126 0.210 0.126 0.323 0.491 0.164 0.455 0.649 0.534 0.316<br />
Bone marrow<br />
transplant<br />
BEN 15 34 25 30<br />
EXP 0.720 1.913 1.595 1.815<br />
Scanner BEN 171 113 388 2067 2176 3470 3927 3009 3255 4731 6744 6935 8931 12183<br />
EXP 0.013 0.009 0.01 0.061 0.13 0.208 0.236 0.215 0.234 0.342 0.483 0.493 0.635 0.882<br />
Lithotripsy BEN 709 571 695 824 971 1118<br />
EXP 0.280 0.221 0.267 0.317 0.375 0.432<br />
MRI BEN 1418 2042 2870 3376 3923 4570<br />
EXP 0.425 0.613 0.861 1.013 1.177 1.371<br />
Haemodialysis BEN 268 361 385 492 717 891 1047 1258 1369 1552 1747 2081 2224 2385 2703<br />
EXP 2.338 3.334 3.866 6.183 7.422 9.640 13.993 16.681 18.935 18.793 22.132 26.850 29.408 33.951 35.035<br />
<strong>The</strong>rmal cure BEN 968 1210 1465 1650 1958 2702 3635 3295 3795 2820 2046 1640 1634 1776 1699<br />
EXP 0.151 0.249 0.223 0.368 0.494 0.741 0.988 0.857 0.948 0.675 0.474 0.374 0.390 0.434 0.716<br />
Military Hospital EXP 0 0 0.178 0.889 0.804 0.926 0.815 0.600 0.000 0.026 0.028 0.079 0.031 0.746 0.834
Tunisia<br />
Figure 1 shows the distribution <strong>of</strong> expenses for <strong>health</strong> care provided under CNSS agreements.<br />
In 2001, 66% <strong>of</strong> the CNSS expenses under agreements were for haemodialysis sessions, 21% for<br />
cardiovascular <strong>in</strong>terventions and 13% for rema<strong>in</strong><strong>in</strong>g items or procedures covered by the agreements<br />
(thermal treatment, bone marrow transplant, kidney transplant, scann<strong>in</strong>g, MRI, lithotripsy and the<br />
Military Hospital).<br />
CTH<br />
1%<br />
HEM<br />
66%<br />
HMI<br />
2%<br />
CCV<br />
21%<br />
HEM: Haemodialysis; CTM: <strong>The</strong>rmal Cure; HMI: Military Hospital; CCV: Cardiovascular <strong>in</strong>terventions;<br />
GR: Kidney transplant; GMO: Bone marrow transplant; SCA: Scanner; LIT: Lithotripsy; IRM: MRI<br />
Figure 2. Distribution <strong>of</strong> <strong>health</strong> care expenses under the CNSS agreements (2001)<br />
<strong>The</strong> resources <strong>of</strong> all the schemes managed by the CNSS are steadily <strong>in</strong>creas<strong>in</strong>g, they <strong>in</strong>creased<br />
threefold between 1990 and 2000 alone. <strong>The</strong> Fund resources have <strong>in</strong>creased by 10.8%, from 383.5<br />
million d<strong>in</strong>ars <strong>in</strong> 1990 to 1075.2 million d<strong>in</strong>ars <strong>in</strong> 2000. <strong>The</strong> Fund expenditures on medical care<br />
under <strong>health</strong> <strong>in</strong>surance (<strong>health</strong> and social actions), <strong>in</strong> comparison with the global expenditures,<br />
represented 20% <strong>in</strong> 1991 and 31% <strong>in</strong> 2000.<br />
Table 6 shows an <strong>in</strong>crease <strong>in</strong> the CNSS <strong>contractual</strong> <strong>arrangements</strong>. Indeed, the CNSS devoted<br />
only 2.7% <strong>in</strong> 1990 and then 5.4% <strong>in</strong> 2001 <strong>of</strong> its total expenditures to agreements. <strong>The</strong> share <strong>of</strong> the<br />
expenditures under <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> comparison with <strong>health</strong> <strong>in</strong>surance expenditures<br />
<strong>in</strong>creased tw<strong>of</strong>old dur<strong>in</strong>g the 1990s, from 15.4% to 30.0%.<br />
Table 6. Share <strong>of</strong> CNSS expenditure allocated to <strong>health</strong> care provided under <strong>contractual</strong><br />
agreements (parties under contract) <strong>in</strong> comparison with <strong>health</strong> <strong>in</strong>surance expenditure (<strong>health</strong><br />
and social actions)<br />
Expenditure 1990 2001<br />
Health <strong>in</strong>surance expenditures(1) 51.7 173.0<br />
Expenditures under contractural<br />
agreements(2)<br />
7.9 52.2<br />
Ratio: (2)/(1) 15.4% 30.0%<br />
GR<br />
1%<br />
IRM<br />
3%<br />
GM<br />
3%<br />
SCA<br />
2%<br />
LIT<br />
1%
Tunisia<br />
<strong>The</strong> National Pension and Social Security Fund (CNRPS)<br />
<strong>The</strong> social security scheme managed by the CNRPS is based on two mutually exclusive<br />
schemes, the direct <strong>health</strong> care provision scheme (<strong>health</strong> card) and the reimbursement scheme.<br />
Regardless <strong>of</strong> scheme, the affiliate member is entitled to direct care services mentioned <strong>in</strong> the<br />
<strong>in</strong>troduction. Most <strong>of</strong> these services have been the subject <strong>of</strong> memoranda <strong>of</strong> agreement with the<br />
M<strong>in</strong>istry <strong>of</strong> Public Health, to which some specialized <strong>health</strong> care facilities adhere.<br />
For the period 1987–2001, the CNRPS spent 169.5 million d<strong>in</strong>ars for all the <strong>health</strong> care<br />
provided by parties under contract: 68% was for coverage <strong>of</strong> haemodialysis sessions.<br />
Haemodialysis expenses <strong>in</strong>creased at an average annual rate <strong>of</strong> 15.9% (Table 7).<br />
Cardiovascular surgery <strong>in</strong>terventions accounted for 18.7% <strong>of</strong> the total expenditures by the<br />
CRPS on <strong>health</strong> care provided under agreements. Dur<strong>in</strong>g the period 1988–2001, cardiovascular<br />
surgery expenses <strong>in</strong>creased at an average annual rate <strong>of</strong> 28.8%.<br />
Moreover, there has been a significant <strong>in</strong>crease <strong>in</strong> the number <strong>of</strong> persons benefit<strong>in</strong>g from the<br />
<strong>health</strong> care provided under the agreements. <strong>The</strong> number <strong>of</strong> beneficiaries for cardiovascular<br />
<strong>in</strong>terventions has <strong>in</strong>creased from 75 to 1373 (1988–2001). For the scanner, this number has reached<br />
7034 <strong>in</strong> 2001 compared to 141 <strong>in</strong> 1990.<br />
Accord<strong>in</strong>g to Table 7, the policy <strong>of</strong> reduc<strong>in</strong>g the need for <strong>health</strong> care abroad, which was the<br />
reason for CNSS adopt<strong>in</strong>g <strong>contractual</strong> <strong>arrangements</strong>, has been successful. In 14 years, the number<br />
<strong>of</strong> beneficiaries receiv<strong>in</strong>g <strong>health</strong> care abroad had been reduced about sixfold. CNRPS expenditures<br />
have been reduced by 3.1 million d<strong>in</strong>ars, without adjust<strong>in</strong>g for <strong>in</strong>ternational <strong>in</strong>flation and with<br />
coverage ma<strong>in</strong>ta<strong>in</strong>ed at a high level.<br />
S<strong>in</strong>ce 1987, the largest share <strong>of</strong> expenditures on <strong>health</strong> care has been for haemodialysis<br />
sessions. Haemodialysis expenditures exceed 60% <strong>of</strong> total expenditures for the period 1987–2001.<br />
In 1987, the share haemoialysis expenditures 83%, decreas<strong>in</strong>g to 62% <strong>in</strong> 2001 (Figure 2).<br />
In 2001, 62% <strong>of</strong> CNRPS expenditures under agreements were for haemodialysis sessions,<br />
21% for cardiovascular <strong>in</strong>terventions and 13% for rema<strong>in</strong><strong>in</strong>g items and procedures (thermal<br />
treatment, bone marrow and kidney transplants, scanner, MRI, lithotripsy and the Military<br />
Hospital).<br />
245
Tunisia<br />
Table 7. Trend <strong>in</strong> number <strong>of</strong> beneficiaries (BEN) and expenses (EXP) under CNRPS agreements, 1987–2001T (million d<strong>in</strong>ars)<br />
Cardiovascular<br />
surgery<br />
Year 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001<br />
BEN 75 110 100 248 368 475 486 584 793 754 890 989 1231 1373<br />
EXP 0.188 0.306 0.253 0.445 1.477 1.380 1.455 2.035 2.969 3.394 4.0084.335 4.352 5.035<br />
Kidney transplant BEN 2 5 4 3 7 3 8 6 7 12 15 9 7 9 11<br />
EXP 0.024 0.0060 0.048 0.036 0.094 0.042 0.112 0.084 0.098 0.165 0.273 0.164 0.187 0.164 0.200<br />
Bone marrow transplant BEN 9 7 15 11<br />
EXP 0.370 0.187 0.6650.590<br />
Scanner BEN 141 1173 1365 2173 2453 2695 2962 3357 4145<br />
EXP 0.009 0.031 0.061 0.096 0.111 0.165 0.211 0.235 0.3 0.282 0.385<br />
Lithotripsy BEN 2 192 190 546 536 462 464 447 444<br />
EXP 0.002 0.048 0.149 0.168 0.099 0.140 0.163 0.17 0.169<br />
MRI BEN 885 1177 1755<br />
EXP 0.279 0.353 0.527<br />
Haemodialysis BEN 138 142 199 256 314 393 492 593 715 784 798 966 1043<br />
EXP 1.931 2.045 2.440 3.058 4.016 5.154 6.341 7.639 8.856 9.497 10.966 11.257<br />
<strong>The</strong>rmal cure BEN 1936 2440 2670 2799 3557 2049 3379 3610 3690 3668 2536 2050<br />
EXP 0.361 0.429 0.461 0.482 0.741 0.467 0.759 0.820 0.846 0.686 0.522 0.412<br />
Military Hospital EXP 0.242 0.455 0.273 0.170 0.016 0.114 0.070<br />
:[<br />
1h]<br />
Comment
Tunisia<br />
Table 8 shows an <strong>in</strong>crease <strong>in</strong> CNRPS expenditures under <strong>contractual</strong> <strong>arrangements</strong>.<br />
Indeed, the CNRPS devoted only 3.1% <strong>in</strong> 1992, and 3.4% <strong>in</strong> 2001, <strong>of</strong> its total expenditures to<br />
agreements. <strong>The</strong> share <strong>of</strong> expenditures under <strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> comparison with<br />
<strong>health</strong> <strong>in</strong>surance expenditures <strong>in</strong>creased by 1.6% dur<strong>in</strong>g the 1990s, from 25.7% to 27.3%.<br />
Table 8. Share <strong>of</strong> CNRPS expenditures allocated to <strong>health</strong> care provided under<br />
<strong>contractual</strong> <strong>arrangements</strong> <strong>in</strong> comparison with <strong>health</strong> <strong>in</strong>surance expenditures<br />
(compulsory scheme)<br />
Year 1992 2001<br />
Health <strong>in</strong>surance expenditures (1) 29.7 89.2<br />
Expenditures under agreements (2) 7.6 24.4<br />
Ratio: (2)/(1) 25.7% 27.3%<br />
Importance <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> for the CNSS and CNRPS<br />
Dur<strong>in</strong>g the period 1990–2001, the agreements have gradually taken a major place <strong>in</strong> the<br />
coverage activity <strong>of</strong> the two Funds. <strong>The</strong> number <strong>of</strong> beneficiaries <strong>in</strong>creased from 5878 to<br />
39 791, i.e. an <strong>in</strong>crease <strong>of</strong> 6.7%. Expenditures also <strong>in</strong>creased significantly, from 12. to<br />
MD 71.9 million d<strong>in</strong>ars, equivalent to an average annual <strong>in</strong>crease rate <strong>of</strong> 17.7%.<br />
Figure 2 shows the trend <strong>of</strong> expenditures <strong>of</strong> the two Funds under agreements. <strong>The</strong><br />
CNSS spends more than the CNRPS. <strong>The</strong> share <strong>of</strong> the CNSS expenditure represented 66% <strong>of</strong><br />
the total expenditure <strong>of</strong> the two Funds <strong>in</strong> 1990 and 72.6% <strong>in</strong> 2001.<br />
EXP (<strong>in</strong> million d<strong>in</strong>ars)<br />
60<br />
50<br />
40<br />
30<br />
20<br />
10<br />
0<br />
CNSS CNRPS<br />
1987 1989 1991 1993 1995 1997 1999 2001<br />
Year<br />
Figure 2. Trend <strong>of</strong> expenditures on <strong>health</strong> care provided<br />
under agreements, 1987–2001
Tunisia<br />
Haemodialysis accounts for more than 70% <strong>of</strong> the expenditures under agreements made<br />
by the two Funds. In 1987, it accounted for 83%. Cardiovascular surgical <strong>in</strong>terventions are<br />
ga<strong>in</strong><strong>in</strong>g <strong>in</strong>creas<strong>in</strong>g importance under the agreements both <strong>in</strong> terms <strong>of</strong> beneficiaries and<br />
expenditures.<br />
Resort<strong>in</strong>g to <strong>health</strong> care abroad for the <strong>in</strong>sured is gradually decreas<strong>in</strong>g <strong>in</strong> both Funds.<br />
<strong>The</strong> expenditures <strong>of</strong> the two Funds for <strong>health</strong> care abroad have been reduced by more than<br />
half, as measured <strong>in</strong> current d<strong>in</strong>ars (Table 9).<br />
Table 9. Coverage <strong>of</strong> beneficiaries resort<strong>in</strong>g to <strong>health</strong> care abroad <strong>in</strong> the two Funds, 1987–2001<br />
Year 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001<br />
CNRPS BEN 395 292 230 259 171 206 207 160 125 89 74 72 52 34 63<br />
EXP 4.88 2.523 3.205 3.306 2.046 3.565 2.751 2.698 2.840 2.514 2.405 2.095 1.672 1.235 1.760<br />
CNSS BEN 692 598 495 314 198 222 224 259 141 113 123 138 81 48 66<br />
EXP 5.904 5.890 5.526 6.784 3.957 4.2054.169 6.174 3.173 3.500 3.397 3.780 2.737 1.238 3.042<br />
CSS BEN 1087 890 725 273 369 428 431 419 266 202 197 210 133 82 129<br />
EXP 10.784 8.413 8.731 10.09 6 7.77 6.92 8.87 6.01 6.014 5.8 5.88 4.409 2.473 4.802<br />
EVALUATION OF CONTRACTUAL ARRANGEMENTS<br />
Advantages <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong><br />
<strong>The</strong> agreements have contributed to:<br />
• <strong>The</strong> reduction <strong>of</strong> <strong>health</strong> care abroad, which represents a very high cost for the social<br />
security funds and for the economy <strong>of</strong> the country.<br />
• <strong>The</strong> development <strong>of</strong> public and private facilities which have become well-equipped<br />
medical centres with advanced technology (Table 10). <strong>The</strong> expansion <strong>of</strong> the private <strong>sector</strong><br />
is also remarkable as it attracts a large number <strong>of</strong> patients from neighbour<strong>in</strong>g countries.<br />
• Contribut<strong>in</strong>g to improve <strong>health</strong> care provision throughout the country. Equipment such as<br />
scanners and lithotripters are now more available <strong>in</strong> the private <strong>sector</strong> <strong>in</strong> most<br />
governorates <strong>of</strong> the country and have become accessible to the <strong>in</strong>sured.<br />
• <strong>The</strong> creation <strong>of</strong> new jobs <strong>in</strong> the medical field, <strong>contractual</strong> <strong>arrangements</strong> guarantee<br />
potential clients and solvent demand for the private <strong>health</strong> facilities.<br />
• De facto regulation <strong>of</strong> the private <strong>sector</strong>. <strong>The</strong> social security funds <strong>in</strong>tervene through<br />
agreements so as to ensure the best treatment conditions (<strong>role</strong> <strong>of</strong> medical <strong>in</strong>spection <strong>of</strong> the<br />
CSS) on the basis <strong>of</strong> flat rates.<br />
• A fundamental change <strong>in</strong> public hospital management (management <strong>of</strong> the system <strong>of</strong><br />
bill<strong>in</strong>g) and <strong>in</strong> budget preparation procedures, which have developed from procedures<br />
based on a systematic annual <strong>in</strong>crease to procedures l<strong>in</strong>ked to hospital activity.<br />
Disadvantages <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong><br />
With regard to <strong>in</strong>dividual behaviour, <strong>health</strong> pr<strong>of</strong>essionals from the public <strong>sector</strong> who are<br />
allowed to practice privately, may f<strong>in</strong>d it to their own advantage to refer the <strong>in</strong>sured patients<br />
248
Tunisia<br />
to the private <strong>sector</strong>. <strong>The</strong> <strong>in</strong>sured also f<strong>in</strong>d it to their best <strong>in</strong>terest to go to the private <strong>sector</strong><br />
known for better quality services. Under the agreements, the patients can choose between the<br />
public and the private <strong>sector</strong>s.<br />
With regard to the behaviour <strong>of</strong> private hospitals the private hospitals charge: a fee per<br />
hospital day which is supposed to cover accommodation and <strong>in</strong>termediate care; a fee for<br />
service to be paid to medical practitioners, as doctors’ fees are not <strong>in</strong>cluded <strong>in</strong> the private<br />
hospital budget; and lump sums for expensive procedures such as scans.<br />
This comb<strong>in</strong>ed formula may lead to <strong>in</strong>creas<strong>in</strong>g the number <strong>of</strong> stays and reduc<strong>in</strong>g their<br />
average duration so as to accelerate bed rotation and maximize the output <strong>of</strong> the technical<br />
equipment and the volume <strong>of</strong> surgeon fees. It can prompt private hospitals to specialize <strong>in</strong><br />
rout<strong>in</strong>e surgery, maternity, medic<strong>in</strong>e, or <strong>in</strong> dialyses and cancer treatment, all <strong>of</strong> which are costeffective<br />
activities, tak<strong>in</strong>g <strong>in</strong>to account the fee structure.<br />
Private hospitals have also found it <strong>in</strong> their <strong>in</strong>terest to acquire technical equipment, for<br />
the purposes enter<strong>in</strong>g <strong>in</strong>to an agreement. Table 10 shows the higher number <strong>of</strong> equipment <strong>in</strong><br />
the private <strong>sector</strong> compared with the public <strong>sector</strong>.<br />
<strong>The</strong> <strong>in</strong>fluence <strong>of</strong> the fee structure appears, for example, <strong>in</strong> the choice <strong>of</strong> the treatment<br />
formula <strong>in</strong> the case <strong>of</strong> a private hospital.<br />
Table 10. Advanced technical equipment <strong>in</strong> hospital facilities, 2003<br />
Equipment Public Private Total Density<br />
Population per piece <strong>of</strong> equipment<br />
MRI 3 5 8 1 236 000<br />
Scanner 15 54 69 143 000<br />
Lithotripter 3 12 15 660 000<br />
Tele-cobalt 4 5 9 1 100 000<br />
Digital vascular imag<strong>in</strong>g mach<strong>in</strong>es 6 10 16 618 000<br />
Catheter 9 10 19 520 000<br />
CEC 6 12 18 550 000<br />
249
Tunisia<br />
With regard to the Funds, current trends <strong>in</strong>dicate that the agreements are responsible for<br />
higher costs, which is likely to create a fiscal imbalance <strong>of</strong> the Funds. <strong>The</strong> cost <strong>of</strong> <strong>contractual</strong><br />
<strong>arrangements</strong> may become unbearable for the follow<strong>in</strong>g reasons:<br />
Patients benefitt<strong>in</strong>g from two or three different types <strong>of</strong> coverage.<br />
<strong>The</strong> extension <strong>of</strong> private facilities that are jo<strong>in</strong><strong>in</strong>g <strong>in</strong> the agreements.<br />
Table 11 shows the upward trend <strong>in</strong> the agreement costs for the two Funds over five<br />
years (1996–2001).<br />
Table 11. Trend <strong>of</strong> CNSS and CNRPS expenditures on <strong>health</strong> care provided under<br />
agreements between 1996 and 2001T (<strong>in</strong> million d<strong>in</strong>ars)<br />
CNSS CNRPS<br />
1996 2001 1996 2001<br />
Ben Exp Ben Exp Ben Exp Ben Exp<br />
Lithotripsy 709 0.280 1118 0.432 464 0.163 706 0.268<br />
Scann<strong>in</strong>g 3255 0.234 12183 0.882 2962 0.211 7034 0.508<br />
MRI 2042 0.613 4570 1.377 885 0.279 2995 0.889<br />
For lithotripsy, the CNSS and CNRPS expenditures have <strong>in</strong>creased by 50%. For<br />
scann<strong>in</strong>g procedures, they have <strong>in</strong>creased by 3.8 and 2.4, respectively.<br />
On their part, the Funds will have to ask for an <strong>in</strong>crease <strong>in</strong> the contribution rate, which<br />
is likely to further <strong>in</strong>crease the households’ contributions to <strong>health</strong> f<strong>in</strong>anc<strong>in</strong>g and to cause<br />
problems for private employers (<strong>in</strong>crease <strong>in</strong> production costs). Indeed, <strong>in</strong> 1987 the Funds<br />
contributed to 13.5% <strong>in</strong> 1987 <strong>of</strong> the total expenditure before the agreements, and about 21.1%<br />
<strong>in</strong> 2002.<br />
<strong>The</strong> <strong>in</strong>crease <strong>in</strong> the costs <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> stems from the fact that they are<br />
<strong>in</strong>volved only <strong>in</strong> care requir<strong>in</strong>g advanced technological equipment. Such equipment enables<br />
rapid and effective diagnosis <strong>of</strong> disease, hence the significant <strong>in</strong>crease <strong>in</strong> the number <strong>of</strong><br />
beneficiaries.<br />
It has been observed that the agreement system, based on flat rates, has prompted the<br />
actors––<strong>health</strong> care providers––to adopt the pr<strong>in</strong>ciple <strong>of</strong> cost<strong>in</strong>g so as to be able to adjust<br />
themselves to the new context <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> aim<strong>in</strong>g at payment <strong>of</strong> the true costs<br />
<strong>of</strong> <strong>health</strong> care. <strong>The</strong> M<strong>in</strong>istry <strong>of</strong> Public Health has adopted, s<strong>in</strong>ce 1999, the pr<strong>in</strong>ciple <strong>of</strong> <strong>health</strong><br />
care cost<strong>in</strong>g which is conducted yearly by the directorate responsible for supervis<strong>in</strong>g<br />
hospitals. <strong>The</strong> objectives <strong>of</strong> the rout<strong>in</strong>e cost<strong>in</strong>g exercise are to:<br />
measure the performance <strong>of</strong> the various activities.<br />
establish the basis for charg<strong>in</strong>g the services provided.<br />
expla<strong>in</strong> and account for the results <strong>of</strong> each exercise.<br />
facilitate budget<strong>in</strong>g and budget control.<br />
250
CONCLUSIONS<br />
Tunisia<br />
Three closely <strong>in</strong>tertw<strong>in</strong>ed factors have contributed to the emergence <strong>of</strong> <strong>contractual</strong><br />
agreements <strong>in</strong> the Tunisian <strong>health</strong> system:<br />
epidemiological and demographical transition<br />
over dependence on <strong>health</strong> care abroad<br />
development <strong>of</strong> the complementary <strong>role</strong> <strong>of</strong> the private <strong>sector</strong> <strong>in</strong> the management <strong>of</strong> emerg<strong>in</strong>g<br />
diseases and <strong>in</strong> <strong>in</strong>vestment <strong>in</strong> <strong>health</strong>.<br />
modernization <strong>of</strong> management procedures <strong>of</strong> the public <strong>health</strong> facilities.<br />
On the whole, the private <strong>in</strong>itiative <strong>in</strong>centive policy has also encouraged to undertake<br />
this type <strong>of</strong> <strong>contractual</strong> <strong>arrangements</strong> so as to ensure the cont<strong>in</strong>uity <strong>of</strong> private <strong>in</strong>vestment.<br />
<strong>The</strong> social security funds play a very important <strong>role</strong> <strong>in</strong> the f<strong>in</strong>anc<strong>in</strong>g <strong>of</strong> the <strong>health</strong> <strong>sector</strong>.<br />
<strong>The</strong> Funds aim at ensur<strong>in</strong>g the quality <strong>of</strong> <strong>health</strong> care and improvement <strong>of</strong> the <strong>health</strong> status <strong>of</strong><br />
the <strong>in</strong>sured who are provided <strong>health</strong> care <strong>in</strong> public and private <strong>health</strong> <strong>in</strong>stitutions. In order to<br />
ensure the cont<strong>in</strong>uity <strong>of</strong> this <strong>role</strong>, the Funds have concluded special agreements. <strong>The</strong> Funds<br />
have also adopted modes <strong>of</strong> f<strong>in</strong>anc<strong>in</strong>g the public <strong>health</strong> <strong>in</strong>stitutions that are essentially based<br />
on lump sum payment, users charges (s<strong>in</strong>gle-act bill<strong>in</strong>g) and strengthen<strong>in</strong>g <strong>of</strong> hospitals.<br />
In this perspective, the charg<strong>in</strong>g procedure has become more and more important,<br />
generat<strong>in</strong>g the practice <strong>of</strong> unit cost calculation that forms the basis for sett<strong>in</strong>g lump sum tariffs<br />
which are <strong>in</strong>creas<strong>in</strong>gly ref<strong>in</strong>ed.<br />
It is to be noted that, apart from the procedures specific to the public <strong>sector</strong>, the<br />
expenses <strong>in</strong>curred <strong>in</strong> the special agreements for coverage are absorbed by the <strong>health</strong><br />
<strong>in</strong>stitutions <strong>of</strong> the private <strong>sector</strong>. <strong>The</strong> managers <strong>in</strong> charge <strong>of</strong> the Funds estimate the proportion<br />
<strong>of</strong> these expenditures made <strong>in</strong> the private <strong>sector</strong> to be about 80%.<br />
251