Coagulation Factors in Controlling Traumatic Bleeds: FFP, PCC, or ...
Coagulation Factors in Controlling Traumatic Bleeds: FFP, PCC, or ...
Coagulation Factors in Controlling Traumatic Bleeds: FFP, PCC, or ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
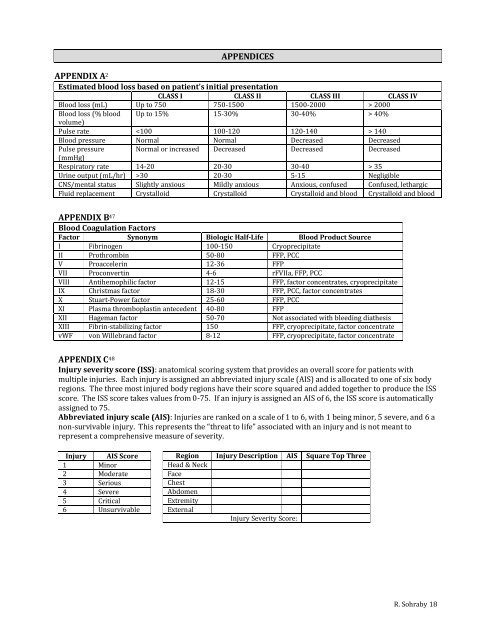
APPENDICES<br />
APPENDIX A 2<br />
Estimated blood loss based on patient’s <strong>in</strong>itial presentation<br />
CLASS I CLASS II CLASS III CLASS IV<br />
Blood loss (mL) Up to 750 750-1500 1500-2000 > 2000<br />
Blood loss (% blood Up to 15% 15-30% 30-40% > 40%<br />
volume)<br />
Pulse rate 140<br />
Blood pressure N<strong>or</strong>mal N<strong>or</strong>mal Decreased Decreased<br />
Pulse pressure N<strong>or</strong>mal <strong>or</strong> <strong>in</strong>creased Decreased Decreased Decreased<br />
(mmHg)<br />
Respirat<strong>or</strong>y rate 14-20 20-30 30-40 > 35<br />
Ur<strong>in</strong>e output (mL/hr) >30 20-30 5-15 Negligible<br />
CNS/mental status Slightly anxious Mildly anxious Anxious, confused Confused, lethargic<br />
Fluid replacement Crystalloid Crystalloid Crystalloid and blood Crystalloid and blood<br />
APPENDIX B 47<br />
Blood <strong>Coagulation</strong> <strong>Fact<strong>or</strong>s</strong><br />
Fact<strong>or</strong> Synonym Biologic Half-Life Blood Product Source<br />
I Fibr<strong>in</strong>ogen 100-150 Cryoprecipitate<br />
II Prothromb<strong>in</strong> 50-80 <strong>FFP</strong>, <strong>PCC</strong><br />
V Proacceler<strong>in</strong> 12-36 <strong>FFP</strong><br />
VII Proconvert<strong>in</strong> 4-6 rFVIIa, <strong>FFP</strong>, <strong>PCC</strong><br />
VIII Antihemophilic fact<strong>or</strong> 12-15 <strong>FFP</strong>, fact<strong>or</strong> concentrates, cryoprecipitate<br />
IX Christmas fact<strong>or</strong> 18-30 <strong>FFP</strong>, <strong>PCC</strong>, fact<strong>or</strong> concentrates<br />
X Stuart-Power fact<strong>or</strong> 25-60 <strong>FFP</strong>, <strong>PCC</strong><br />
XI Plasma thromboplast<strong>in</strong> antecedent 40-80 <strong>FFP</strong><br />
XII Hageman fact<strong>or</strong> 50-70 Not associated with bleed<strong>in</strong>g diathesis<br />
XIII Fibr<strong>in</strong>-stabiliz<strong>in</strong>g fact<strong>or</strong> 150 <strong>FFP</strong>, cryoprecipitate, fact<strong>or</strong> concentrate<br />
vWF von Willebrand fact<strong>or</strong> 8-12 <strong>FFP</strong>, cryoprecipitate, fact<strong>or</strong> concentrate<br />
APPENDIX C 48<br />
Injury severity sc<strong>or</strong>e (ISS): anatomical sc<strong>or</strong><strong>in</strong>g system that provides an overall sc<strong>or</strong>e f<strong>or</strong> patients with<br />
multiple <strong>in</strong>juries. Each <strong>in</strong>jury is assigned an abbreviated <strong>in</strong>jury scale (AIS) and is allocated to one of six body<br />
regions. The three most <strong>in</strong>jured body regions have their sc<strong>or</strong>e squared and added together to produce the ISS<br />
sc<strong>or</strong>e. The ISS sc<strong>or</strong>e takes values from 0-75. If an <strong>in</strong>jury is assigned an AIS of 6, the ISS sc<strong>or</strong>e is automatically<br />
assigned to 75.<br />
Abbreviated <strong>in</strong>jury scale (AIS): Injuries are ranked on a scale of 1 to 6, with 1 be<strong>in</strong>g m<strong>in</strong><strong>or</strong>, 5 severe, and 6 a<br />
non-survivable <strong>in</strong>jury. This represents the “threat to life” associated with an <strong>in</strong>jury and is not meant to<br />
represent a comprehensive measure of severity.<br />
Injury AIS Sc<strong>or</strong>e<br />
1 M<strong>in</strong><strong>or</strong><br />
2 Moderate<br />
3 Serious<br />
4 Severe<br />
5 Critical<br />
6 Unsurvivable<br />
Region Injury Description AIS Square Top Three<br />
Head & Neck<br />
Face<br />
Chest<br />
Abdomen<br />
Extremity<br />
External<br />
Injury Severity Sc<strong>or</strong>e:<br />
R. Sohraby 18