Coagulation Factors in Controlling Traumatic Bleeds: FFP, PCC, or ...
Coagulation Factors in Controlling Traumatic Bleeds: FFP, PCC, or ...
Coagulation Factors in Controlling Traumatic Bleeds: FFP, PCC, or ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
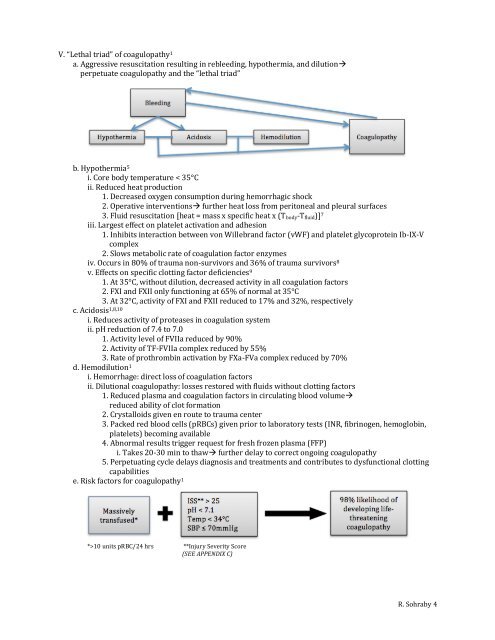
V. “Lethal triad” of coagulopathy 1<br />
a. Aggressive resuscitation result<strong>in</strong>g <strong>in</strong> rebleed<strong>in</strong>g, hypothermia, and dilution<br />
perpetuate coagulopathy and the “lethal triad”<br />
b. Hypothermia 5<br />
i. C<strong>or</strong>e body temperature < 35°C<br />
ii. Reduced heat production<br />
1. Decreased oxygen consumption dur<strong>in</strong>g hem<strong>or</strong>rhagic shock<br />
2. Operative <strong>in</strong>terventions further heat loss from peritoneal and pleural surfaces<br />
3. Fluid resuscitation [heat = mass x specific heat x (T body -T fluid )] 7<br />
iii. Largest effect on platelet activation and adhesion<br />
1. Inhibits <strong>in</strong>teraction between von Willebrand fact<strong>or</strong> (vWF) and platelet glycoprote<strong>in</strong> Ib-IX-V<br />
complex<br />
2. Slows metabolic rate of coagulation fact<strong>or</strong> enzymes<br />
iv. Occurs <strong>in</strong> 80% of trauma non-surviv<strong>or</strong>s and 36% of trauma surviv<strong>or</strong>s 8<br />
v. Effects on specific clott<strong>in</strong>g fact<strong>or</strong> deficiencies 9<br />
1. At 35°C, without dilution, decreased activity <strong>in</strong> all coagulation fact<strong>or</strong>s<br />
2. FXI and FXII only function<strong>in</strong>g at 65% of n<strong>or</strong>mal at 35°C<br />
3. At 32°C, activity of FXI and FXII reduced to 17% and 32%, respectively<br />
c. Acidosis 1,8,10<br />
i. Reduces activity of proteases <strong>in</strong> coagulation system<br />
ii. pH reduction of 7.4 to 7.0<br />
1. Activity level of FVIIa reduced by 90%<br />
2. Activity of TF-FVIIa complex reduced by 55%<br />
3. Rate of prothromb<strong>in</strong> activation by FXa-FVa complex reduced by 70%<br />
d. Hemodilution 1<br />
i. Hem<strong>or</strong>rhage: direct loss of coagulation fact<strong>or</strong>s<br />
ii. Dilutional coagulopathy: losses rest<strong>or</strong>ed with fluids without clott<strong>in</strong>g fact<strong>or</strong>s<br />
1. Reduced plasma and coagulation fact<strong>or</strong>s <strong>in</strong> circulat<strong>in</strong>g blood volume<br />
reduced ability of clot f<strong>or</strong>mation<br />
2. Crystalloids given en route to trauma center<br />
3. Packed red blood cells (pRBCs) given pri<strong>or</strong> to lab<strong>or</strong>at<strong>or</strong>y tests (INR, fibr<strong>in</strong>ogen, hemoglob<strong>in</strong>,<br />
platelets) becom<strong>in</strong>g available<br />
4. Abn<strong>or</strong>mal results trigger request f<strong>or</strong> fresh frozen plasma (<strong>FFP</strong>)<br />
i. Takes 20-30 m<strong>in</strong> to thaw further delay to c<strong>or</strong>rect ongo<strong>in</strong>g coagulopathy<br />
5. Perpetuat<strong>in</strong>g cycle delays diagnosis and treatments and contributes to dysfunctional clott<strong>in</strong>g<br />
capabilities<br />
e. Risk fact<strong>or</strong>s f<strong>or</strong> coagulopathy 1<br />
*>10 units pRBC/24 hrs **Injury Severity Sc<strong>or</strong>e<br />
(SEE APPENDIX C)<br />
R. Sohraby 4