Saliva Alcohol - California Association of Toxicologists
Saliva Alcohol - California Association of Toxicologists
Saliva Alcohol - California Association of Toxicologists

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Saliva</strong> <strong>Alcohol</strong><br />
Vina Spiehler Ph.D., DABFT<br />
Newport Beach, CA
Physiology <strong>of</strong> <strong>Saliva</strong><br />
Excreted by Parotid, SM, and SL Glands<br />
0.5 - 1.5 L/day<br />
serous and mucous alveoli<br />
99% water w 0.3% protein and 0.3% mucins<br />
ave pH 6.4 range 5.6-7 unstimulated<br />
ave pH 7.0 max 8.0 stimulated<br />
Submandibular gland 65%<br />
Parotid gland 23%<br />
Sublingual 4%
<strong>Alcohol</strong> <strong>Saliva</strong>/Blood Ratio<br />
• Friedemann et al 1938<br />
• Newman Abramson 1942<br />
• McColl 1979<br />
• Jones 1979<br />
• Haeckel 1987<br />
• Jones 1993<br />
• Bendtsen et al 1999<br />
• close correlation<br />
• close agreement<br />
• 1.05 parotid,<br />
0.95 mixed saliva<br />
• 1.082 (s.e.m<br />
0.0059)<br />
• S/P = 0.85<br />
• 1.094 (range 0.88-<br />
1.36)<br />
•
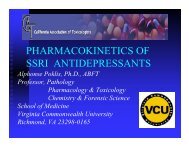
orrelation <strong>Saliva</strong> and Blood EtOH Conc
Ethanol Conc-Time Pr<strong>of</strong>ile<br />
Jones 1993
Before <strong>Saliva</strong> EtOH Test
DOT Conforming Products List<br />
<strong>Saliva</strong> <strong>Alcohol</strong> Screening Tests<br />
www.nhtsa.dot.gov/people/injury/alcohol/blood<br />
• Roche Diagnostics<br />
• OraSure<br />
Technologies, Inc.<br />
(formerly STC )<br />
• Chematics, Inc.<br />
• On-Site <strong>Alcohol</strong> R<br />
• Q.E.D. A150<br />
<strong>Saliva</strong> <strong>Alcohol</strong><br />
Test<br />
• ALCO-SCREEN<br />
02 TM
Q.E.D. <strong>Saliva</strong> <strong>Alcohol</strong> Test
• Advantages<br />
Conclusions<br />
– Non-invasive collection<br />
– Difficult to adulterate<br />
– On site testing<br />
– Correlates with BAC and impairment<br />
• Disadvantages<br />
– Dry mouth may not produce sufficient sample<br />
– Small sample <strong>of</strong> sticky fluid<br />
– Second sample or test needed for confirmation
<strong>Saliva</strong> <strong>Alcohol</strong><br />
Vina Spiehler, Ph.D., DABFT<br />
Spiehler and Associates, Newport Beach, CA 92663<br />
Introduction<br />
<strong>Saliva</strong> is the secretion product <strong>of</strong> the saliva glands <strong>of</strong> the head and mouth. However, the<br />
fluids found in the oral cavity are a mixture <strong>of</strong> predominately saliva, with lesser amounts<br />
<strong>of</strong> gingival crevicular fluid, cellular debris and blood. For this reason the New York<br />
Academy <strong>of</strong> Sciences meeting on saliva testing in 1993 agreed to use the word saliva for<br />
glandular secretions which are collected directly from the saliva glands (most <strong>of</strong>ten the<br />
parotid glands), and oral fluid for fluid collected by placing absorbants in the oral cavity<br />
or by expectoration (Malamud 1993).<br />
The advantages <strong>of</strong> saliva drug testing are mainly tw<strong>of</strong>old. First, saliva alcohol<br />
concentrations can be related to blood alcohol concentrations and pharmacological<br />
effects. Second, saliva or oral fluid collection is non-invasive, simple and can be done<br />
on-site under observation.<br />
Oral fluid collection can be carried out by having the specimen donor himself or herself<br />
place a cotton swab or absorptive material attached to a stick into his/her mouth for a few<br />
minutes. The oral fluid absorbed on the material is then processed for testing. <strong>Saliva</strong> can<br />
be collected at the site <strong>of</strong> the incident in accident or crime investigation. If necessary,<br />
saliva flow can be stimulated with citrate hard candy or citrate salts or by chewing on<br />
gum or rubber to ensure adequate sample volume. Unlike breath testing saliva collection<br />
does not require a cooperative effort on the part <strong>of</strong> the donor. <strong>Saliva</strong> collection may be<br />
an alternative when the person is unable to blow into an alcohol breath instrument for<br />
sufficient time or volume. Because saliva collection is non-invasive and can be done by<br />
the donor themselves in most situations, it is more acceptable to most persons than<br />
providing urine, blood or hair and can be done while the donor is under observation by<br />
the collector. An exception may be when the donor is unconscious or so sedated to be<br />
unable to follow instructions. Finally, it is difficult to adulterate or substitute oral fluid<br />
specimens in an attempt to avoid detection as any adulterating substances held in the<br />
mouth will dissipate, be swallowed or spit out during the ten to twenty minute<br />
observation period before collection <strong>of</strong> the specimen.<br />
Like any bi<strong>of</strong>luid from human subjects, oral fluid may transmit infectious agents and<br />
should be handled with the appropriate universal precautions for human biological fluids.<br />
<strong>Saliva</strong> contains mucopolysaccharides and mucoproteins which make it less fluid and less<br />
easily poured or pipetted than urine. Some drugs, medical conditions or anxiety can<br />
inhibit saliva secretion and cause dry mouth.<br />
Anatomy and Physiology <strong>of</strong> <strong>Saliva</strong>: The <strong>Saliva</strong> Glands<br />
1
The human saliva glands produce between 0.5 and 1.5 liters <strong>of</strong> saliva daily. During<br />
resting conditions most mixed saliva is supplied by the submandibular glands (70%) with<br />
lesser amount (25%) from the parotid glands and the remaining (5%) from the sublingual<br />
and other minor glands. During stimulation the parotid saliva output increases to about<br />
half <strong>of</strong> the total. <strong>Saliva</strong> is composed <strong>of</strong> 99% water 0.3% protein (largely amylase) and<br />
0.3% mucins. The parotid gland produces mostly serous fluid. The submandibular and<br />
sublingual glands excrete both serous fluid and mucins. The saliva glands like the liver,<br />
kidney and brain, are well supplied with arterial blood.<br />
<strong>Saliva</strong>ry glands are composed <strong>of</strong> two regions, the acinar region which contains the cells<br />
which are capable <strong>of</strong> secretion and the ductal region lined with water-impermeable cells<br />
which carry the secretions to the outlets in the mouth. Similarly, saliva formation occurs<br />
in two steps. Water and exocrine proteins are secreted by the secretory cells in the acinar<br />
region. The fluid which collected in the acinar lumen is isotonic with plasma. As the<br />
fluid travels down the saliva ducts, sodium and chloride are reabsorbed while potassium<br />
and bicarbonate are secreted. Therefore, when saliva moves rapidly through the ducts,<br />
less time is available for sodium reabsorption and the pH <strong>of</strong> the saliva is higher (Dawes<br />
1964). When the fluid reaches the mouth it is hypotonic to plasma.<br />
<strong>Saliva</strong>ry glands are activated by the autonomic nerves. Generally sympathetic<br />
stimulation via norepinephrine causes low levels <strong>of</strong> fluid and high concentrations <strong>of</strong><br />
protein while parasympathetic stimulation via acetylcholine induces large amounts <strong>of</strong><br />
fluid secretion.<br />
<strong>Saliva</strong> <strong>Alcohol</strong> Pharmacology<br />
Ethanol is a low molecular weight compound which passes through cell membranes, does<br />
not ionize nor bind to plasma proteins. Ethanol distributes to all body fluids in<br />
proportion to their water content. The measured saliva plasma ratio for alcohol, 1.10, is<br />
slightly higher than the calculated value, perhaps because <strong>of</strong> the high blood flow to the<br />
salivary glands, saliva ethanol is in equilibrium with arterial blood rather than venous<br />
blood collected for analysis. <strong>Saliva</strong> equilibrates rapidly with blood ethanol.<br />
The passage <strong>of</strong> ethanol into saliva and the close correlation between saliva and blood<br />
alcohol concentrations was reported in the 1930's (Friedemann et al 1938). Jones (1979)<br />
reported ethanol saliva/plasma ratio <strong>of</strong> 1.077 with a range <strong>of</strong> 0.84 to 1.36 in 48 male<br />
subjects between one and three hours after ingestion <strong>of</strong> 0.72 g/kg ethanol in a fasting<br />
condition. Variation was determined by analysis to be equally due to inter- and intraindividual<br />
components. Individual variation in saliva/plasma ratios showed no<br />
systematic variation through absorption, distribution and elimination phases <strong>of</strong> ethanol<br />
metabolism. Jones 1993 confirmed this value with a measured saliva/plasma ratio <strong>of</strong><br />
1.094 (range 0.88 to 1.36) in twenty-one male volunteers. McColl et al 1979 found a<br />
highly significant linear correlation between blood ethanol concentrations and those in<br />
mixed saliva obtained before and after rinsing and drying the mouth and parotid saliva.<br />
McColl pointed out that this only applies if the saliva ethanol is determined in saliva<br />
obtained more than 20 minutes after ingestion <strong>of</strong> ethanol.<br />
2
Haeckel (1987) reported that ethanol concentrations reached higher peak concentrations<br />
in saliva than in peripheral blood. They noted that saliva ethanol concentrations like<br />
breath ethanol concentrations more closely correlate with capillary blood than venous<br />
blood. Haeckel (1992) reported a saliva/plasma ratio <strong>of</strong> 0.85 (if related to the aqueous<br />
compartment <strong>of</strong> blood) in saliva and breath samples taken from traffic drivers retained by<br />
the police.<br />
Newman and Abramson 1942 correlated saliva alcohol concentrations with ethanol<br />
effects on performance. Jones 1993 compared saliva, breath and blood concentrationtime<br />
pr<strong>of</strong>iles with subjective feelings <strong>of</strong> intoxication, body sway, hand tremor, positional<br />
nystagmus and roving ocular movement after 0.68 g/kg ethanol ingestion by fasting male<br />
subjects. <strong>Saliva</strong> concentrations were higher than blood and breath concentrations. All<br />
three correlated equally well with measures <strong>of</strong> alcohol effects. Maximum impairment<br />
was reached at the same time as peak saliva, blood and breath levels. The mean<br />
elimination rate <strong>of</strong> ethanol from saliva <strong>of</strong> 130 ± 25 mg/L/hr was not significantly<br />
different from that from blood, 120 ± 11 mg/L/hr and paralleled the recovery <strong>of</strong> baseline<br />
function in the physiological tests.<br />
Analysis<br />
Ethanol can be analyzed in saliva by the same headspace chromatographic (Jones 1978)<br />
or enzymatic methods (Jones 1979) as used for blood. Dipstick or reagent strip tests for<br />
alcohol have been reported (Tu et al 1992, Pate 1993) but were found to be too unreliable<br />
for use in determining blood alcohol content (Lutz et al 1993, Pate et al 1993, Wong<br />
2002). Current enzymatic tests have proven more reliable as quantitative tests<br />
(Christopher 1992, Jones 1995, Smolle et al 1999, Bendtsen et al 1999) and several<br />
commercial tests for on-site or point <strong>of</strong> collection testing <strong>of</strong> saliva alcohol are available.<br />
An example <strong>of</strong> a point <strong>of</strong> collection quantitative test is the Q.E.D. <strong>Saliva</strong> <strong>Alcohol</strong> Test<br />
(OraSure, Bethlehem, PA, USA). The saliva or oral fluid is collected by the donor with a<br />
cotton swab which is applied to the test pad. As the saliva moves along the reagent bar<br />
by capillary action any ethanol present is oxidized by alcohol dehydrogenase to<br />
acetaldehyde with simultaneous reduction <strong>of</strong> nicotinamide-adenine dinucleotide (NAD).<br />
This results in a cascade <strong>of</strong> electron donor-acceptor reactions catalyzed by diaphorase,<br />
involving FeCN and a tetrazolium salt which proceed to production <strong>of</strong> a purple-colored<br />
endpoint. The length <strong>of</strong> the resulting purple-colored bar on the Q.E.D. device is directly<br />
proportional to the concentration <strong>of</strong> ethanol in the specimen. The alcohol concentration<br />
can be read directly from the height <strong>of</strong> the colored reaction bar from a printed scale in<br />
mg/dL or mg% ethanol just as in reading a thermometer. To get an accurate reading the<br />
capillary must draw saliva all the way to the top <strong>of</strong> the device. This is signaled by<br />
development <strong>of</strong> a purple color within five minutes at the QA Spot at the top <strong>of</strong> the<br />
"thermometer."<br />
Since the saliva moves along the reagent bar and reacts directly with the indicator<br />
chemicals, any oxidant in the saliva can cause a false positive. The most common<br />
3
oxidant found in saliva is ascorbic acid commonly added to fruit juices, sodas and s<strong>of</strong>t<br />
drinks as a preservative. Ascorbic acid is absorbed in the gums and is still found in the<br />
mouth in amounts sufficient to give a false positive with the Q.E.D. <strong>Saliva</strong> <strong>Alcohol</strong> test<br />
for up to ten minutes after drinking some s<strong>of</strong>t drinks and sodas. For this reason a 15<br />
minute waiting period before testing after taking anything by mouth is doubly<br />
recommended for saliva alcohol testing with the Q.E.D.<br />
The Q.E.D. <strong>Saliva</strong> <strong>Alcohol</strong> test comes in two ranges, 0 to 150 which can be read from<br />
0.01 to 0.15 g/dL, and 0 to 350 which can be read from 0.02 to 0.35 g/dL. The first,<br />
lower, range is for DOT and DUI applications, the second is for hospital and overdose<br />
applications.<br />
An example <strong>of</strong> a headspace enzymatic assay is the On-Site <strong>Alcohol</strong> Assay for qualitative<br />
detection <strong>of</strong> alcohol in urine and saliva (Roche Diagnostics, Nutley, NJ, USA; Varian<br />
Inc. Consumable Products, Lake Forest, CA, USA). The On-Site <strong>Saliva</strong> <strong>Alcohol</strong> test is<br />
similar to the Q.E.D. <strong>Saliva</strong> <strong>Alcohol</strong> test in that saliva is collected by the donor from<br />
his/her own mouth with a cotton swab and then the swab is applied to the specimen well.<br />
Since alcohols are volatile, alcohol vapors will diffuse from the sample pad to the<br />
reaction pad where they react with alcohol dehydrogenase and diaphorase. The hydrogen<br />
released is transferred to tetrazolium salt to produce a highly colored formazen dye. The<br />
presence <strong>of</strong> alcohol is indicated by the appearance <strong>of</strong> a purple plus sign (+) in the result<br />
pad. The On-Site <strong>Saliva</strong> <strong>Alcohol</strong> test does not have a control spot so an external control<br />
must be run in each testing session on an additional test unit. Since the test detects<br />
alcohol vapors from the saliva, the saliva sample does not come into contact with the<br />
reagents, so there is no possibility <strong>of</strong> false positives from oxidizing agents such as<br />
ascorbic acid in the saliva. However the result is qualitative only. The cut<strong>of</strong>f is 0.02 g%,<br />
so a purple plus sign (+) indicates the presence <strong>of</strong> alcohol at greater than 0.02 g%.<br />
Interpretation<br />
<strong>Saliva</strong> ethanol concentrations are an accurate reflection <strong>of</strong> blood alcohol concentrations<br />
Jones (1979, 1993). <strong>Saliva</strong> alcohol can be used to estimate blood alcohol concentrations,<br />
to estimate pharmacokinetics <strong>of</strong> ethanol in an individual, as evidence <strong>of</strong> impairment and<br />
to determine fitness for duty in the workplace.<br />
In the USA workplace testing, the Department <strong>of</strong> Transportation has codified saliva<br />
ethanol testing (DOT 1994). The screening cut<strong>of</strong>f is 0.02 g% saliva or 0.02 g/210 L <strong>of</strong><br />
breath. Because the saliva alcohol tests are non-specific chemical screening tests which<br />
may react with oxidizing agents other than alcohol and with ketones and alcohols other<br />
than ethanol, it is necessary to confirm any positive results greater than 0.02 g% with an<br />
independent test based on a different chemical principle. Breath alcohol tests are usually<br />
either fuel cells or infrared spectrophotometers with optical filters and computer s<strong>of</strong>tware<br />
safeguards for specificity and sensitivity. Specifically they must be able to distinguish<br />
acetone from ethanol at the 0.02 g% alcohol level. A time limit is put on confirmation <strong>of</strong><br />
saliva ethanol results since ethanol is rapidly metabolized by the liver. Initially the<br />
4
confirmation breath test had to be performed within 20 minutes. DOT now requires the<br />
confirmation test to be done within 30 minutes.<br />
DOT 1994 requires a 15 minute waiting period before saliva or breath alcohol tests.<br />
DOT describes this as a safeguard against false high readings due to accumulation <strong>of</strong><br />
mouth alcohol, but the 15 waiting period will also protect against false positive readings<br />
from food or drink components such as ascorbic acid which might cause false positive<br />
readings in saliva tests. To obtain a correct test, the most important factor is that a<br />
waiting period be observed in which the donor does not eat, drink, smoke or belch (that<br />
is, nothing by mouth).<br />
References<br />
Bates M E, Brick J, and White H R. The correspondence between saliva and breath<br />
estimates <strong>of</strong> blood alcohol concentration: advantages and limitation <strong>of</strong> the saliva method.<br />
J. Stud. <strong>Alcohol</strong> 54:17-22, 1993.<br />
Baum B J. Principles <strong>of</strong> saliva secretion. Ann. New York Acad. Sci. 694:17-23.<br />
Caplan YH and Goldberger BA (2001). Alternative specimens for workplace drug<br />
testing. J. Anal Toxicol. 25(5):396-399, 1993.<br />
Bendtsen P, Hultberg J, Carlsson M and Jones A W, Monitoring ethanol exposure in a<br />
clinical setting by analysis <strong>of</strong> blood, breath, saliva and urine. <strong>Alcohol</strong> Clin. Exp. Res.<br />
23:1446-1451, 1999.<br />
Christopher T A and Zeccardi J A. Evaluation <strong>of</strong> the QED saliva alcohol test: a new,<br />
rapid, accurate device for measuring ethanol in saliva. Ann. Emerg. Med. 21:1135-1137.<br />
1992.<br />
Dawes C and Jenkins G N. The effects <strong>of</strong> different stimuli on the composition <strong>of</strong> saliva<br />
in man,” J. Physiol., 170:86-100, 1964.<br />
Department <strong>of</strong> Transportation (1994). 49 CFR Part 40 Procedures for Transportation<br />
Workplace Drug and <strong>Alcohol</strong> Testing Programs. Final Rule. Federal Register 59:7340-<br />
7360 and 42996-43019.<br />
Friedemann, T E, Motel W G and Necheles H. The excretion <strong>of</strong> ingested ethyl alcohol in<br />
saliva. J. Lab. Clin. Med. 23:1007-10014, 1938.<br />
Haeckel R and Bucklitsch I. The comparability <strong>of</strong> ethanol concentrations in peripheral<br />
blood and saliva: The phenomemon <strong>of</strong> variation in saliva to blood concentrations ratios.<br />
J. Clin. Chem. Clin. Biochem. 25:199-204, 1987.<br />
Haeckel R and Peiffer U. Comparison <strong>of</strong> ethanol concentration in saliva and blood from<br />
police controlled persons. Blutalkohol 29:342-349, 1992.<br />
5
Haeckel R and Hanecke P. Application <strong>of</strong> saliva for drug monitoring an in vivo model for<br />
transmembrane transport,” Eur. J. Clin. Chem. Biochem. 34:171-191, 1996.<br />
Jones A W. A rapid head-space method for ethyl alcohol determination in saliva<br />
samples. Anal. Biochem. 86:589-596, 1978.<br />
Jones A W. Distribution <strong>of</strong> ethanol between saliva and blood in man. Clin. Exp.<br />
Pharmacol. Physiol. 6:53-59, 1979.<br />
Jones A W. Assessment <strong>of</strong> an automated enzymatic method for ethanol determination in<br />
microsamples <strong>of</strong> saliva. Scand. J. Clin. Lab. Invest. 39:199-203, 1979.<br />
Jones A W. Inter- and intra-individual variations in the saliva/blood alcohol ratio during<br />
ethanol metabolism in man. Clin. Chem. 25:1394-1398, 1979.<br />
Jones A W. Pharmacokinetics <strong>of</strong> ethanol in saliva: Comparison with blood and breath<br />
alcohol pr<strong>of</strong>iles, subjective feeling <strong>of</strong> intoxication and diminished performance. Clin.<br />
Chem. 39:1837-1844, 1993.<br />
Jones A W. Measuring ethanol in saliva with the QED Enzymatic test device:<br />
Comparison <strong>of</strong> results with blood and breath alcohol concentrations. J. Anal. Toxicol.<br />
19:169-174, 1995.<br />
Lutz F U, Frohlich S, Reuhl J. Alco Screen-a reliable method for determining blood<br />
alcohol concentration by saliva alcohol concentration? Blutalkohol 30:240-243, 1993.<br />
McColl K E, Whiting B, Moore M R and Goldberg A. Correlation <strong>of</strong> ethanol<br />
concentrations in blood and saliva. Clin. Sci. (Colch) 56:283-286, 1979.<br />
Malamud D. Guidelines for saliva nomenclature and collection. Ann. New York Acad.<br />
Sci. 694:xi-xii, 1993.<br />
Newman H W and Abramson M. Some factors influencing the intoxicating effect <strong>of</strong><br />
alcoholic breverages. J. Stud. <strong>Alcohol</strong>. 42:351-370, 1942.<br />
Pate L A, Hamilton J D, Park R S and Strobel R M. Evaluation <strong>of</strong> a saliva alcohol test<br />
stick as a therapeutic adjunct in an alcoholism treatment program. J. Stud. <strong>Alcohol</strong><br />
54:520-521, 1993.<br />
Peel H W, Perrigo B J and Mikhael N Z (1984). Detection <strong>of</strong> drugs in saliva <strong>of</strong> impaired<br />
drivers. J. For. Sci., 29(1):185-189.<br />
Smolle K H, H<strong>of</strong>mann G, Kaufmann P et al. QED alcohol test: a simple and quick<br />
method to detect ethanol in saliva <strong>of</strong> patients in emergency departments. Comparison<br />
with the conventional determination in blood. Intensive Care Med. 25:492-495, 1999.<br />
6
Tu G C, Kapur B, and Israel Y. Characteristics <strong>of</strong> a new urine, serum and saliva alcohol<br />
reagent strip. <strong>Alcohol</strong> Clin. Exp. Res. 16:222-227, 1992.<br />
Turner R J. Mechanisms <strong>of</strong> fluid secretion by salivary glands. Ann. New York Acad. Sci.<br />
694:24-35, 1993.<br />
Wong KS Over-the-counter preliminary alcohol screening devices. The <strong>California</strong><br />
<strong>Association</strong> <strong>of</strong> <strong>Toxicologists</strong> Proceedings 30(3): 14-16, 2002.<br />
7