TAY Living Plan (PDF) - Independent Living Program
TAY Living Plan (PDF) - Independent Living Program
TAY Living Plan (PDF) - Independent Living Program

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
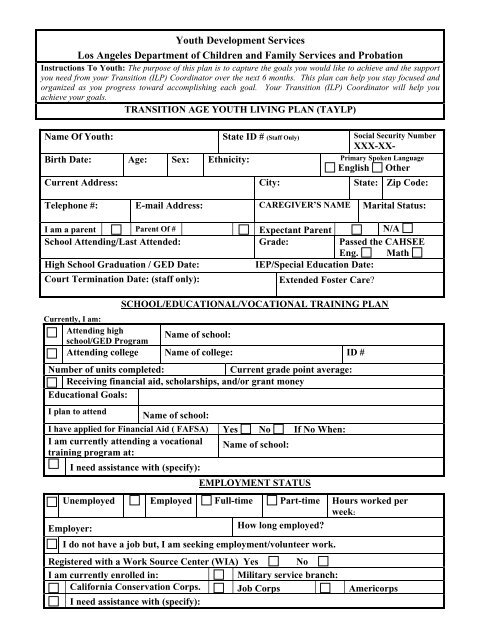
Youth Development Services<br />
Los Angeles Department of Children and Family Services and Probation<br />
Instructions To Youth: The purpose of this plan is to capture the goals you would like to achieve and the support<br />
you need from your Transition (ILP) Coordinator over the next 6 months. This plan can help you stay focused and<br />
organized as you progress toward accomplishing each goal. Your Transition (ILP) Coordinator will help you<br />
achieve your goals.<br />
TRANSITION AGE YOUTH LIVING PLAN (<strong>TAY</strong>LP)<br />
Name Of Youth: State ID # (Staff Only) Social Security Number<br />
XXX-XX-<br />
Birth Date: Age: Sex: Ethnicity: Primary Spoken Language<br />
English Other<br />
Current Address: City: State: Zip Code:<br />
Telephone #: E-mail Address: CAREGIVER’S NAME Marital Status:<br />
I am a parent Parent Of # Expectant Parent N/A<br />
School Attending/Last Attended: Grade: Passed the CAHSEE<br />
Eng. Math<br />
High School Graduation / GED Date:<br />
IEP/Special Education Date:<br />
Court Termination Date: (staff only):<br />
Extended Foster Care?<br />
SCHOOL/EDUCATIONAL/VOCATIONAL TRAINING PLAN<br />
Currently, I am:<br />
Attending high<br />
school/GED <strong>Program</strong><br />
Name of school:<br />
Attending college Name of college: ID #<br />
Number of units completed:<br />
Current grade point average:<br />
Receiving financial aid, scholarships, and/or grant money<br />
Educational Goals:<br />
I plan to attend<br />
Name of school:<br />
I have applied for Financial Aid ( FAFSA) Yes No If No When:<br />
I am currently attending a vocational Name of school:<br />
training program at:<br />
I need assistance with (specify):<br />
EMPLOYMENT STATUS<br />
Unemployed Employed Full-time Part-time Hours worked per<br />
week:<br />
Employer:<br />
How long employed?<br />
I do not have a job but, I am seeking employment/volunteer work.<br />
Registered with a Work Source Center (WIA) Yes No<br />
I am currently enrolled in:<br />
Military service branch:<br />
California Conservation Corps. Job Corps Americorps<br />
I need assistance with (specify):
CURRENT HOUSING STATUS/HOUSING PLAN<br />
My current living situation is:<br />
Rent/own housing Share rent with others Stay in college dorm<br />
Live with friends Live in board & care Live with relatives<br />
Live in county or other Name of <strong>Program</strong>:<br />
SILP<br />
transitional housing.<br />
Homeless Live w/care provider/guardian Live with parent(s)<br />
Housing plan<br />
I plan to live with:<br />
I am interested in/ or need<br />
assistance with:<br />
Health Insurance <strong>Plan</strong><br />
What is your health insurance plan?<br />
If you are not eligible for extended<br />
Medi-Cal, where do you plan to get<br />
health insurance from?<br />
Continuing Support Services (i.e.<br />
mental health, health services) <strong>Plan</strong>:<br />
Family, Other Permanent<br />
Connection, Mentor:<br />
I plan to stay connected to family<br />
and other adults (include names)<br />
Resource phone numbers and websites:<br />
ILP toll free number<br />
1 (877) MY ILP 411<br />
http://www.ilponline.org<br />
Medi-Cal Health Insurance Benefits<br />
application or to extend coverage<br />
626-569-2968 or 626-569-2948<br />
Youth Ombudsman<br />
Office:<br />
(213) 351-5720<br />
Other Resources<br />
Department of Public Social<br />
Services<br />
(DPSS)<br />
1 (877) 597-4777<br />
Edelman's Children's Court<br />
(323) 526-6646<br />
FINANCIAL RESOURCES<br />
My sources of income include:<br />
Work CalWORKs Cooperative for Assistance and<br />
Relief Everywhere (CARE)<br />
Department of Vocational EOP&S<br />
Financial Aid/Scholarship<br />
Rehab<br />
General Relief Payments SSI/SSDI Temporary Assistance for Needy<br />
Families (TANF)<br />
Trust Account EFC (SILP) Other (Specify):<br />
Revised 1/31/2013<br />
Contact: Youth Development Services Division (ILP) Headquarters at (213) 351-0100<br />
Toll Free Number: 1(877) MY ILP 411 or http://www.ilponline.org<br />
2
PERSONAL DOCUMENTATION<br />
Do you have the following Have<br />
important documents?<br />
Birth Certificate<br />
Financial Aid Award<br />
Letter<br />
High School Diploma Or<br />
GED/School Records<br />
Immigration Record/Green<br />
Card/ Naturalization<br />
Need<br />
help<br />
N/A<br />
Do you have the<br />
following important<br />
documents?<br />
Social Security<br />
Card/Number<br />
California Drivers<br />
License/ID<br />
Medi-Cal Card<br />
Last two minute<br />
orders from<br />
Children’s Court<br />
For Probation Youth Only<br />
Have<br />
Need<br />
help<br />
Juvenile Probation - Terminated Yes No<br />
Youth on adult Probation Yes No<br />
Need assistance with expunging my juvenile record Yes No<br />
Need assistance with sealing my juvenile record Yes No<br />
Need assistance with credit report or identity theft related issues Yes No<br />
Other Specify):<br />
Additional information if necessary:<br />
_______________________________________________________________________________________<br />
_______________________________________________________________________________________<br />
Please note: Youth leaving the Kinship Guardian Assistance Payment (Kin-GAP) or Adoption Assistance<br />
Payment (AAP) <strong>Program</strong>s receive Medi-Cal benefits through their next annual redetermination date, which<br />
could be up to 11 months. Prior to the month of expiration, the youth will receive a redetermination packet<br />
to be completed and returned for an eligibility evaluation to any other Medi-Cal benefits program. This is<br />
why it’s important that we have your current address.<br />
Please check with Transition (ILP) Coordinator for a complete list of required documents to receive ILP funds and to<br />
verify eligibility. Youth might be eligible for ILP Services if he/she is or was a court dependent and placed in foster<br />
care/probation placement at any time between the age of 16 and 18 or if under a Kin-GAP guardianship or if under a<br />
non-related legal guardianship granted by Dependency Court after age 8 .<br />
I understand that any requested funds are subject to availability and that failure to submit receipts<br />
could jeopardize continued financial assistance from the ILP program.<br />
Date your next <strong>TAY</strong>LP update is to be completed (six months): ________________<br />
N/A<br />
______________________________________________<br />
Youth Signature<br />
______________________________________________<br />
Caregiver Signature (if applicable)<br />
______________________________________________<br />
Transition (ILP) Coordinator/Probation Officer Signature<br />
_________________________________<br />
Date<br />
_________________________________<br />
Date<br />
_________________________________<br />
Date<br />
Revised 1/31/2013<br />
Contact: Youth Development Services Division (ILP) Headquarters at (213) 351-0100<br />
Toll Free Number: 1(877) MY ILP 411 or http://www.ilponline.org<br />
3