Eyelid Reconstruction
Eyelid Reconstruction
Eyelid Reconstruction

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Eyelid</strong><br />
<strong>Reconstruction</strong><br />
Introduction<br />
Goal: restore normal anatomy and function<br />
Various reconstructive techniques<br />
Complex anatomy<br />
1
<strong>Eyelid</strong><br />
<strong>Eyelid</strong> functions<br />
– Protect eye (light, injury, desiccation)<br />
– Tear production and distribution<br />
Anterior/posterior lamella<br />
Extremely thin skin (upper > lower)<br />
Skin<br />
– Little subcutaneous fat<br />
– Adherent over the tarsus (levator aponeurosis)<br />
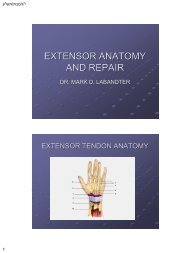
Anatomy<br />
Horizontal length – 28-30 mm<br />
Palpebral fissure – 10-12 mm<br />
Upper eyelid crease – 6-8 mm<br />
Lower eyelid crease – 3-4 mm<br />
2
Anatomy<br />
Tarsus<br />
– Dense, fibrous tissue<br />
– Contour and skeleton<br />
– Contain meibomian<br />
glands<br />
– Length – 25 mm<br />
– Thickness – 1 mm<br />
– Height<br />
• Upper plate – 10 mm<br />
• Lower plate – 4 mm<br />
Tarsus<br />
3
Orbicularis Oculi Muscle<br />
Orbicularis m.<br />
• PT - pretarsal<br />
• PS - preseptal<br />
• O - orbital portion<br />
4
Anatomy<br />
Orbital Septum<br />
– Fascial barrier<br />
– Underlies posterior<br />
orbicularis fascia<br />
– Origin<br />
• Arcus marginalis<br />
Anatomy<br />
Orbital Septum<br />
Insertion<br />
• Medial: post.<br />
lacrimal crest<br />
• Lateral:<br />
orbit tubercle<br />
• Superior:<br />
aponeurosis<br />
• Inferior:<br />
inferior tarsal border<br />
5
• - Arcus Marginalis<br />
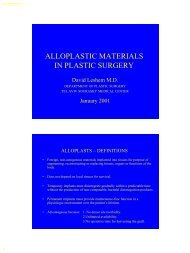
Upper Lid Anatomy<br />
6
• Lower - marginal artery<br />
• Upper - peripheral<br />
arterial arcade<br />
• L - levator aponeurosis<br />
• Blue - tarsus<br />
• M - muller’s muscle<br />
• C - conjuctival lining<br />
• O.S - orbital septum<br />
• W - transverse ligament<br />
of Whitnall<br />
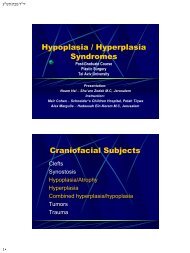
• M - muller’s m.<br />
• T - tarsal plate<br />
7
• LA - levator aponeurosis<br />
• L - palpebral portion of<br />
of the lacrimal gland<br />
• M - muller’s m.<br />
• T - tarsus<br />
• - Whitnall’s ligament<br />
• * - levator m.<br />
• T - trochlea<br />
• L - lacrimal<br />
gland stroma<br />
8
• V - median palpebral arterial vessels<br />
• * - superficial medial fat pad<br />
• CF - central fat pad<br />
Lower Lid Anatomy<br />
9
• OS - orbital septum<br />
• capsulopalpebral fascia<br />
• * - maxillary sinus mucosa<br />
• - infraorbital nerve<br />
10
Anatomy<br />
Anatomy<br />
11
Anatomy<br />
Canthal tendons<br />
– Extensions of preseptal & pretarsal orbicularis<br />
– Lateral slightly above medial<br />
– Lateral tendon attaches to Whitnall’s tubercle<br />
1.5 cm posterior to orbital rim<br />
– Medial tendon - for lacrimal pump function<br />
Canthal Tendons<br />
12
Anatomy<br />
Lateral canthal tendon<br />
- lateral retinaculum<br />
Anatomy<br />
Medial canthal tendon<br />
– Vertical fascial support<br />
13
Anatomy<br />
Lacrimal apparatus<br />
– Gland<br />
– Punctum<br />
– Canaliculus<br />
– Sac<br />
– Duct<br />
Anatomy<br />
Lacrimal System<br />
14
Anatomy<br />
Lacrimal Excretory Pump<br />
Lacrimal sys.<br />
• Lacrimal gland-->Collecting ducts-><br />
Upper & lower punctae--><br />
Ampullae--> Upper & lower lacrimal<br />
canaliculi--> Lacrimal sac--><br />
Nasolacrimal duct<br />
• ―Pump‖ mechanism forcing tears<br />
from canaliculi into the lacrimal sac<br />
15
Anatomy – Blood Supply<br />
Internal & external<br />
carotids anastomoses<br />
Marginal arcades –<br />
2-3 mm from lid<br />
margin<br />
Peripheral arcade –<br />
upper lid between<br />
levator aponeurosis<br />
and Müller’s muscle<br />
<strong>Eyelid</strong> <strong>Reconstruction</strong><br />
• Adjacent eyelid skin is the best color match<br />
• Cheek skin is a good match (texture & color)<br />
• Glabellar & nasolabial skin are useful flaps , but<br />
the color& texture match are not always best<br />
16
<strong>Eyelid</strong> <strong>Reconstruction</strong><br />
• Skin graft - if primary closure & local flap<br />
coverage are not feasible<br />
• STSG contract & give poor color match<br />
• Sup. Clavicle FTSG good color match<br />
• Upper inner arm FTSG are hairless and pliable,<br />
color match may not be good<br />
<strong>Eyelid</strong> <strong>Reconstruction</strong><br />
• There are numerous available local flaps:<br />
a- bipedicled Tripier flap<br />
b- Fricke flap<br />
c- midline forehead or glabellar flap<br />
d- medial & lateral skin-muscle flaps<br />
e- nasolabial flap, superiorly based<br />
f- cheek flap<br />
17
Lower <strong>Eyelid</strong> <strong>Reconstruction</strong><br />
Direct Closure<br />
Lateral Cantholysis<br />
Tenzel Rotational Flap<br />
Free Tarsal Grafts<br />
Hughes Procedure<br />
Mustarde (rotational cheek) Flap<br />
Lower <strong>Eyelid</strong> <strong>Reconstruction</strong><br />
PARTIAL THICKNESS DEFECTS<br />
• Tumor, trauma, or burns<br />
• It could involve skin loss only or skin & muscle<br />
• Enough skin in the adjacent area, primary<br />
closure be possible<br />
18
Lower <strong>Eyelid</strong> <strong>Reconstruction</strong><br />
PARTIAL THICKNESS DEFECTS<br />
• If the defect is horizontal, attempted closure<br />
of a large defect may result in ectropion<br />
• Small defects - skin from both upper lids<br />
• Orbicularis muscle loss - composite muscle and<br />
skin patch from the upper lid<br />
• FTSG from postauricular area<br />
• Excellent color match, heal with some<br />
stiffness - additional support to the lower lid<br />
19
• Relaxed lid margin furnishes poor support and<br />
allow lid eversion postoperatively<br />
• Wedge excision of tarsus and lid margin, the<br />
graft can be placed directly over the closure<br />
with good graft ―take‖<br />
Lower <strong>Eyelid</strong> <strong>Reconstruction</strong><br />
FULL THICKNESS DEFECTS<br />
• Frozen section<br />
• <strong>Reconstruction</strong> can be delayed<br />
20
Direct Closure<br />
30% defects in young patients<br />
Up to 45% in older patients (laxity)<br />
Lateral cantholysis - additional 5 mm<br />
Tarsal defect should be squared<br />
• The excision is vertically oriented in the tarsus:<br />
pentagon shape<br />
• Approximation of the pentagon:<br />
straight lid margin without notching<br />
• The knot must be tied<br />
away from the conjunctiva<br />
to prevent irritation<br />
• The wound is closed in<br />
three layers<br />
21
Direct Closure<br />
Lid Margin Repair<br />
22
The “extensile” approach:<br />
A: ―Tag‖ sutures can be placed in the tarsal margin<br />
under tension to see if closure is possible<br />
B: If direct closure is not possible, exposure and<br />
cantholysis of the lateral canthal tendon to relax<br />
the lateral eyelid<br />
23
Lateral Cantholysis<br />
Split upper and lower canthal tendons<br />
Detach lower limb (upper limb)<br />
Angle skin incision superiorly<br />
Anchor muscle layer to periosteum after<br />
closure of defect<br />
Lateral Cantholysis<br />
24
C: If lateral cantholysis is not adequate for closure,<br />
a skin flap can be designed with the incision<br />
extended onto the cheek or with a ―back-cut‖ of<br />
the flap as shown<br />
• Advancement of this<br />
flap along with rotation<br />
of the conjunctiva<br />
generally allows closure<br />
of defects, in some<br />
cases up to nearly onehalf<br />
of the lower lid<br />
Tenzel Rotational Flap<br />
Semicircular musculocutaneous flap<br />
Defects up to 60%<br />
Flap must arch upward<br />
Fixation of muscle to periosteum<br />
superior to canthal attachment avoids<br />
droop of lid<br />
25
Tenzel Flap<br />
D: If a small cheek advancement is not adequate, a<br />
large cheek flap can be designed and used<br />
• Defects up to complete lower lid loss can be<br />
reconstructed by this technique<br />
• Mobilization of the<br />
cheek flap is<br />
accomplished by<br />
wide undermining.<br />
26
Mustarde Rotational Cheek Flap<br />
Good for very large defects<br />
Advantage – single stage procedure<br />
Preferable for patients with:<br />
– Monocular vision<br />
– Children with amblyopia<br />
– Active corneal disease<br />
– Glaucoma<br />
Disadvantages – lacks orbicularis,<br />
sagging<br />
Mustarde Technique<br />
27
Mustarde Technique<br />
• The size of the mucosal defect is estimated<br />
• Septal cartilage-mucosal composite graft to<br />
lend support to the newly reconstructed lateral<br />
canthal area<br />
• The cartilage thinned by splitting it (allows<br />
slight convex curvature of the cartilage )<br />
28
• Over correction in the vertical dimension<br />
allows good support<br />
• Anchoring of the cheek flap must be at the<br />
deep lateral canthal area with a permanent<br />
suture<br />
―<strong>Reconstruction</strong> of a large surgical defect<br />
involving the lower eyelid and infraorbital cheek‖<br />
Dermatol Surg;2003, California<br />
29
Combined side-to-side tissue advencement with<br />
―A dog ear ― full-thickness graft<br />
Free Tarsal Graft<br />
Free tarsocunjunctival flap<br />
Harvested from ipsi/contralateral lid<br />
Posterior lamellar replacement<br />
Cover with myocutaneous advancement<br />
30
Free Tarsal Graft<br />
Tripier bipedicled flap<br />
• If the defect involves the inferior lacrimal punctum, the<br />
lacrimal canaliculus can be mobilized and redirected<br />
31
Hughes Procedure<br />
Tarsoconjunctival Flap for posterior lamella<br />
Defects greater than 50%<br />
Vertical upper lid to lower lid sharing<br />
Anterior lamella reconstruction<br />
– Advancement musculocutaneous flap<br />
– Free skin graft<br />
Requires 2 nd stage procedure<br />
Hughes Procedure<br />
32
Hughes Procedure<br />
(continued)<br />
―Use of subcutaneously based naselabial flap<br />
in lower eyelid reconstruction‖<br />
Br J Plast Surg;2003, Demark<br />
33
Combined of Hughes procedure with<br />
nasolabial flap<br />
Small full-thickness defects of the medial<br />
canthal & lower lid:<br />
• medially based upper lid skin muscle flap with<br />
small composite mucosa-cartilage graft<br />
34
― Medial canthal reconstruction using a medialy<br />
based upper eyelid myocutaneous flap‖<br />
PRS;2002, N.Y&Philadelphia<br />
Laterally small horizontal defect:<br />
• Laterally based flap of skin and orbicularis muscle<br />
with small composite mucosal cartilage graft<br />
35
Upper <strong>Eyelid</strong> <strong>Reconstruction</strong><br />
Direct Closure +/- lateral cantholysis<br />
Tenzel Flap<br />
Sliding Tarsoconjunctival Flap<br />
Posterior Lamellar Graft with local<br />
myocutaneous flap<br />
Cutler-Beard (Bridge) Flap<br />
Upper <strong>Eyelid</strong> <strong>Reconstruction</strong><br />
• If a skin defect is present, direct closure,<br />
local flap, or skin graft may be indicated<br />
• Loss of the orbicularis muscle: should be<br />
replaced by moving adjacent muscle or by a<br />
composite muscle & skin graft from the opposite<br />
upper lid<br />
36
• An excellent flap for local coverage may come<br />
from adjacent lateral eyelid or temporal skin<br />
• Midline forehead & glabellar areas:color &<br />
texture match are not good<br />
• The best donor source for color & texture<br />
match: same/opposite upper lid skin<br />
• If there is significant loss of muscle, an adjacent<br />
reinnervated muscle flap/graft can be utilized<br />
• Full-thickness defects of the upper lid can be<br />
treated in the same way as the lower lid defects<br />
37
Direct Closure<br />
Tenzel Flap<br />
38
Sliding Tarsoconjunctival Flap<br />
Isolated medial or lateral lid defects<br />
Borrows a sliding portion of remaining lid<br />
segment for posterior lamella<br />
Anterior lamella repaired with skin graft or<br />
local myocutaneous advancement flap<br />
Sliding Tarsoconjunctival Flap<br />
39
• If closure does not appear to be feasible, a<br />
composite septal mucosal graft and a local pedicle<br />
flap can be used<br />
Posterior Lamellar Graft with<br />
Local Myocutaneous Flap<br />
Patients with skin laxity / redundancy<br />
Posterior lamella defect<br />
– Conjunctival advancement<br />
– Supplement with ear cartilage<br />
Anterior lamella<br />
– Myocutaneous flap for blood supply<br />
40
Posterior Lamellar Graft with<br />
Local Myocutaneous Flap<br />
Cutler-Beard (Bridge) Flap<br />
Used for 60% to entire lid defects<br />
Borrows skin, muscle and conjunctiva<br />
from lower eyelid<br />
Autogeneous cartilage to provide support<br />
Requires 2 nd stage procedure<br />
41
Cutler-Beard (Bridge) Flap<br />
Cutler-Beard (Bridge) Flap –<br />
2 nd Stage Procedure<br />
42
Pedicle Flap From Lower Lid<br />
Full-thickness upper lid defects:<br />
Mustarde - rotation of pedicle flaps of fullthickness<br />
lower lid tissue (similar to an Abbe flap)<br />
―A technique for reconstruction of upper lid<br />
marginal defects‖<br />
Br J Ophtalmol;2003, Melbourne<br />
A one stage technique:<br />
Local posterior (tarsoconjuctival) & anterior<br />
lamella (outlined with redundent Burrow’s triangles)<br />
advancement flaps<br />
43
Conclusion<br />
Thorough understanding of eyelid anatomy<br />
Understand basic techniques of repair<br />
Challenging problem do to complex nature<br />
of eyelid anatomy<br />
Careful attention to detail with delicate<br />
surgical technique required<br />
44
Lateral Canthal <strong>Reconstruction</strong><br />
Lateral Canthal <strong>Reconstruction</strong><br />
45
Medial Canthal <strong>Reconstruction</strong><br />
Medial Canthal <strong>Reconstruction</strong><br />
46
Medial Canthal <strong>Reconstruction</strong><br />
Related Vocabulary<br />
Ptosis – upper eyelid margin abnormally<br />
inferiorly displaced<br />
Entropion – inward rotation of eyelid margin<br />
Ectropion – eversion of eyelid margin<br />
Trichiasis – misdirected eyelashes<br />
47
Related Vocabulary<br />
Distichiasis – aberrant eyelashes from<br />
metaplastic meibomian glands<br />
Epiblepharon – normal eyelashes pushed<br />
toward the eye by redundant folds of skin<br />
Epicanthal folds – vertical folds of skin over<br />
the medial canthus<br />
CORRECTION OF PTOSIS<br />
• Ptosis is defined as an abnormal drooping of<br />
the eyelid<br />
• The normal level of the eyelid is that position<br />
where it covers 1 - 2 mm of the upper limbus<br />
of the cornea<br />
48
CORRECTION OF PTOSIS<br />
• When dealing with ptosis patients, factors<br />
other than lid level must be considered,<br />
including the amount of levator function, the<br />
level of the ptotic lid, and the level of the<br />
opposite lid<br />
CORRECTION OF PTOSIS<br />
• The levator is skeletal muscle under<br />
voluntary control<br />
• Muller’s muscle is smooth muscle innervated<br />
by the sympathetic part of the autonomic<br />
nervous system<br />
49
CLASSIFICATION OF PTOSIS<br />
Congenital ptosis<br />
1. Simple<br />
2. With lid anomalies<br />
3. With ophthalmoplegias<br />
4. Synkinetic (Marcus-Gunn)<br />
Acquired ptosis<br />
1. Neurogenic<br />
2. Myogenic<br />
3. Traumatic<br />
4. Mechanical<br />
5. Pseudoptosis<br />
• Congenital ptosis is associated with myogenic<br />
dystrophic changes of the levator muscle<br />
resulting in poor levator function<br />
• A small percentage of these changes include<br />
two types: misdirected third cranial nerve<br />
(CN III) ptosis of the Marcus-Gunn type &<br />
blepharophimosis<br />
50
• Neurogenic ptosis includes CN III palsy,<br />
congenital or acquired, and Horner’s cervical<br />
sympathetic nerve palsy<br />
• Myogenic ptosis includes ―involutional‖ or<br />
senile ptosis; acquired muscular dystrophy;<br />
progressive external ophthalmoplegia; and<br />
myasthenia gravis<br />
• Traumatic ptosis varies according to the<br />
location of the injury to the levator muscle or<br />
lid mechanism<br />
• Mechanical ptosis is due to a tumor, cyst, or<br />
enlarged lacrimal gland pushing down the eyelid<br />
• Pseudoptosis refers to the drooping lid skin of<br />
blepharochalasis and to the apparent ptosis seen<br />
in the postenucleation eyelid<br />
• Before proceeding with surgery in the ptosis<br />
patient, it is wise to make a detailed evaluation of<br />
the history and development of the problem<br />
51
Useful guide to the workup of ptosis<br />
1. Obtain the patient’s history<br />
2. Perform a careful gross eyes examination<br />
3. Measure the supratarsal fold and symmetry<br />
4. Evaluate the lid contour<br />
5. Measure the ptosis (in millimeters)<br />
6. Measure the difference between the two<br />
eyelids (width of the palpebral fissure)<br />
Useful guide to the workup of ptosis<br />
7. Measure levator function<br />
(lid excursion with the brow static)<br />
8. Check the visual acuity of each eye<br />
9. Check the extra-ocular muscle movements<br />
10. Check for Bell’s phenomenon<br />
11. Check for jaw-winking motion<br />
12. Check for lagophthalmos and lid lag<br />
52
• Previous problems:excessive tearing or dryness,<br />
allergy, or irritation<br />
• Photographs<br />
• Tensilon test<br />
• Horner’s syndrome can be tested by stimulation<br />
with 10% phenylephrine hydrochloride solution,<br />
which corrects the ptosis<br />
Classification of Ptosis Severity:<br />
Mild 1–2 mm<br />
Moderate 3 mm<br />
Severe 4+ mm<br />
Classification of Levator Function<br />
Excellent 12–15 mm<br />
Good 8–12 mm<br />
Fair 5–7 mm<br />
Poor 2–4 mm<br />
53
Margin reflex distance<br />
– Number of millimeters<br />
from the corneal light<br />
reflex to the lid margin<br />
– Upper lid – 4 to 5 mm<br />
(rests slightly below<br />
limbus)<br />
– Lower lid – 5 mm (rests at<br />
the lower limbus(<br />
– Reflex to limbus – 2.5 mm<br />
Absent function of the levator<br />
• For patients with absent function and severe ptosis, a<br />
frontalis sling is the procedure of choice<br />
Fascia sling<br />
A:<br />
Incisions at the lid margin<br />
54
B: Fascia is inserted between the orbicularis<br />
muscle and the tarsus at the lid margin<br />
C: pulling fascia to the upper brow level<br />
55
D,E: Crossover of the fascia<br />
sling pulls the lid to the<br />
desired level. Simple suture<br />
ties are used for fixation<br />
F: <strong>Eyelid</strong> is at the desired level<br />
• The principle of this operation is direct<br />
attachment of the frontalis muscle at the<br />
brow to the lid margin by means of a fascia<br />
lata sling or strip<br />
56
Mild/Moderate ptosis with fair to good<br />
levator function:<br />
• To correct mild ptosis, separate or combined<br />
resection of the tarsal plate, Muller’s muscleconjunctiva,<br />
aponeurosis, levator muscle or<br />
Aponeurosis plication has been used effectively<br />
Mild/Moderate ptosis with fair to good<br />
levator function:<br />
• To correct moderate ptosis some form of<br />
levator shortening threw aponeurosis approach<br />
procedure is used by most surgeons<br />
• Levator resection, levator “tucking”<br />
procedures, levator advancement, and<br />
aponeurosis shortening procedures are the<br />
treatment of moderate ptosis<br />
57
Fasanella-Servat procedure: posterior conjunctival<br />
approach (Combination of tarsal plate resection with<br />
mullerectomy & aponeurosectomy)<br />
A: Ptotic eyelid<br />
B: Eversion of the lid, clamping the<br />
combined edge of the upper tarsus,<br />
conjunctiva, and Muller’s muscle<br />
C: Running crossover<br />
pull-out suture<br />
above the clamped<br />
area<br />
D: Excision of tissue included in the clamped specimen<br />
E: Tissue is excised, and the lid is shortened by excision<br />
of the tarsus, conjunctiva, and Muller’s muscle, with<br />
tying of crossover stitches.<br />
F: Final position of eyelid<br />
58
Mustarde’s “split-level” tarsectomy<br />
A: Planned resection of skin, muscle, and tarsus<br />
B: Resected areas shown<br />
C: ―Split-level‖ closure of<br />
the eyelid for the<br />
desired level<br />
Aponeurosectomy (Anterior view)<br />
A: Exposure of the aponeurosis<br />
B: Excision of the<br />
ellipse of the<br />
aponeurosis, Muller’s<br />
muscle, and<br />
conjunctiva<br />
C, D: Closure defect<br />
E: Defect closed<br />
59
Aponeurosectomy (Lateral view)<br />
A: Exposure of the<br />
aponeurosis<br />
B: Excision of the<br />
ellipse of the<br />
aponeurosis,<br />
Muller’s muscle,<br />
and conjunctiva<br />
C, D: Closure defect<br />
E: Defect closed<br />
Aponeurosis plication<br />
A: Incision to expose aponeurosis<br />
B: Exposed<br />
aponeurosis with<br />
plication sutures<br />
C: Plication sutures<br />
tied to desired<br />
level<br />
D: Lateral view of<br />
plicated<br />
aponeurosis<br />
60
• The usual amount of plication is approximately 3<br />
mm to each 1 mm of ptosis<br />
• This procedure is not effective for patients who have<br />
progressive aponeurosis dehiscence (the aponeurosis<br />
will continue to dehisce)<br />
• The plication technique is an excellent noninvasive way<br />
to repair minimal long-standing eyelid asymmetry<br />
Levator advancement procedure<br />
moderate ptosis, fair to good levator function<br />
A: Incision in tarsal crease<br />
B: Exposure of<br />
aponeurosis and<br />
Whitnall’s ligament<br />
C, D: Isolation of<br />
levator muscle<br />
after Whitnall’s<br />
ligament has been<br />
dissected away<br />
E: Marking points on<br />
levator muscle &<br />
tarsus<br />
61
F: Cross-clamping of levator muscle at level of insertion<br />
into aponeurosis<br />
G: Advancement of levator muscle to tarsal plate, with<br />
fixation by permanent sutures<br />
H, I: Desired lid<br />
level achieved by<br />
advancement of 4<br />
mm of levator<br />
muscle to the<br />
tarsus for each 1<br />
mm of ptosis<br />
• It is usually best in a unilateral ptosis to have the lid<br />
level approximately 1.0 - 1.5 mm higher than the<br />
contralateral eye<br />
• Most surgeons prefer to use levator shortening as the<br />
first procedure, hoping to get a reasonably good<br />
result without having to resort to a fascia sling<br />
• If correction utilizing the patient’s levator muscle<br />
function is possible, it can potentially give a more<br />
natural result<br />
62
― Aesthetic eyelid ptosis correction: a review<br />
of technique and cases‖<br />
PRS;2003,Alabama<br />
Levator aponeurosis plication<br />
blepharoplasty approach<br />
COMPLICATIONS<br />
• The best results are obtained in those patients who have<br />
the least severe ptosis with the greatest amount of<br />
levator muscle function<br />
• Selection of the proper operation for the patient is<br />
the most important part of the process<br />
• Under correction: the most common complication<br />
63
• Over correction: often leads to corneal exposure<br />
(especially during sleep), drying, and possible corneal<br />
erosion<br />
• If the over correction is mild, massage of the lid with<br />
gentle intermittent traction may be effective<br />
• If the procedure performed was tarsectomy or a similar<br />
operation, gentle separation of the suture line under topical<br />
anesthesia often corrects the problem by forcing the lid<br />
level down<br />
• If the over correction is severe, opening the defect in the<br />
aponeurosis and placing a scleral graft as a spacer may be<br />
necessary<br />
• This technique may allow the lid level to drop down to<br />
normal and overcome the corneal problems<br />
• Lagophthalmos: may result from removing a large amount<br />
of aponeurosis with subsequent adhesions preventing the<br />
downward motion of the eyelid<br />
• Usually time and massage take care of this problem, but in<br />
the interim the cornea must be protected from drying,<br />
especially at night, by artificial tears or ointment<br />
• If lagophthalmos persists and the lid level is normal,<br />
surgical exploration and lysis of adhesions may be<br />
indicated if severity of symptoms indicates it<br />
• Hematoma, excessive swelling: may occur and may<br />
compromise the result by causing excessive fibrosis,<br />
chronic edema, loss of lid fold, or loss of the surgical<br />
correction<br />
64
• Loss of eyelashes: may occur, probably due to<br />
dissecting too close to the lid margin during exposure of<br />
the tarsal plate<br />
• Once the loss occurs, there is no good procedure to<br />
correct it<br />
• Entropion: sometimes occurs as a result of removing<br />
too much tarsal plate or poor placement of the<br />
sutures, which reattach the levator muscle to it<br />
In summary: great care must be exerted to<br />
avoid the complications of ptosis surgery, as<br />
these problems may give rise to severe corneal<br />
symptoms or an unhappy patient. Moreover, they<br />
often require another operative procedure for<br />
correction<br />
65
Entropion<br />
Congenital<br />
– Hypertrophy of pretarsal orbicularis<br />
– Deficiency or absence of tarsal plate<br />
– Dehiscence of eyelid retractors<br />
Involutional (senile)<br />
– Loss of orbital volume—enopthalmos<br />
– Upward migration of preseptal orbicularis<br />
– Laxity or dehiscence of eyelid retractors<br />
– Thinning of tarsal plate<br />
Cicatricial<br />
– Shortening of internal lamella<br />
Entropion<br />
Congenital Entropion<br />
– Extremely rare<br />
– Inversion of entire tarsus and<br />
lid margin<br />
– Horizontal tarsal kink<br />
Epiblepharon<br />
– In-rolling of lid margin and<br />
lashes over superior tarsal edge<br />
– More common; bilateral<br />
– Lack of adhesion between lid<br />
retractors and anterior lamella<br />
66
Entropion<br />
Correction of congenital<br />
entropion / epiblepharon<br />
– Observation<br />
– <strong>Eyelid</strong> taping<br />
– Suture correction--Snellen<br />
– Excision of redundant tissue<br />
Entropion<br />
Correction of involutional entropion<br />
– Temporary taping<br />
– Suture correction—Snellen<br />
– Surgical techniques<br />
• Horizontal laxity—enopthalmos,<br />
tarsal thinning<br />
• Laxity of eyelid retractors<br />
• Vertical mobility preseptal<br />
orbicularis<br />
67
Entropion<br />
Correction of<br />
involutional entropion<br />
– Horizontal tightening<br />
Entropion<br />
Correction of<br />
involutional entropion<br />
– Horizontal shortening<br />
modified Bick procedure<br />
68
Entropion<br />
Correction of<br />
involutional entropion<br />
– Weis procedure<br />
• Full-thickness horizontal<br />
lid incision<br />
Entropion<br />
Correction of involutional entropion<br />
– Quickert procedure<br />
• Combination of horizontal tightening and Weis procedure<br />
69
Entropion<br />
Correction of<br />
involutional entropion<br />
– Inferior retractor<br />
plication<br />
Entropion<br />
Correction of<br />
involutional entropion<br />
– Orbicularis fixation<br />
• Beyer modification of<br />
Hill procedure<br />
• Wheeler orbicularis<br />
transplantation<br />
70
Entropion<br />
Correction of<br />
cicatricial entropion<br />
– Wedge excision of<br />
tarsal plate<br />
Entropion<br />
Correction of<br />
cicatricial entropion<br />
– Marginal incision and<br />
grafting<br />
71
Entropion<br />
Correction of<br />
cicatricial entropion<br />
– Tarsal fracture and<br />
margin rotation—Tenzel<br />
procedure<br />
Entropion<br />
Correction of<br />
cicatricial entropion<br />
– Posterior lamella grafting<br />
• Conchal cartilage<br />
• Nasal chondromucosa<br />
• Palatal mucoperichondrium<br />
• Buccal mucosa<br />
• Tarsoconjunctival<br />
composite graft<br />
72
Ectropion<br />
Congenital<br />
– Insufficient anterior lamella<br />
– Decreased tarsal rigidity<br />
– Poor development of canthal tendons<br />
Paralytic<br />
– Orbicularis denervation<br />
• Widened palpebral fissure<br />
• Lagopthalmos<br />
Ectropion<br />
Cicatricial<br />
– Contraction of anterior lamella<br />
Involutional<br />
– Laxity of tarsoligamentous sling<br />
– Generalized loss of elastin<br />
– Orbicularis atrophy<br />
73
Ectropion<br />
Congenital<br />
– Rare<br />
– Association with other<br />
anomalies<br />
– Euryblepharon<br />
– Blepharophimosis<br />
Correction of congenital<br />
ectropion<br />
– Horizontal lid<br />
tightening/shortening<br />
– Grafting of anterior lamella<br />
Ectropion<br />
Paralytic ectropion<br />
Correction of<br />
paralytic ectropion<br />
– Tarsorrhaphy<br />
74
Ectropion<br />
Correction of<br />
paralytic ectropion<br />
– Horizontal lid<br />
tightening<br />
Ectropion<br />
Correction of<br />
paralytic ectropion<br />
– Fascial sling<br />
75
Ectropion<br />
Correction of<br />
cicatricial ectropion<br />
– Horizontal tightening<br />
– Fascial sling<br />
– Full thickness skin<br />
graft<br />
Ectropion<br />
Correction of<br />
cicatricial ectropion<br />
– Horizontal tightening<br />
– Fascial sling<br />
– Full thickness skin<br />
graft<br />
– Transposition graft<br />
76
Ectropion<br />
Correction of<br />
cicatricial ectropion<br />
– Horizontal tightening<br />
– Fascial sling<br />
– Full thickness skin<br />
graft<br />
– Transposition graft<br />
– Split level graft<br />
Ectropion<br />
Correction of<br />
involutional ectropion<br />
– Transverse<br />
blepharotomy and<br />
rotational sutures<br />
77
Ectropion<br />
Correction of<br />
involutional ectropion<br />
– Cathopexy<br />
Ectropion<br />
Correction of<br />
involutional ectropion<br />
– Lateral Tarsal Strip<br />
78
Ectropion<br />
Correction of<br />
involutional ectropion<br />
– Horizontal lid<br />
tightening/shortening<br />
• Medial<br />
Ectropion<br />
Correction of<br />
involutional ectropion<br />
– Horizontal lid<br />
tightening/shortening<br />
• Lateral<br />
79
Ectropion<br />
Correction of<br />
involutional ectropion<br />
– Horizontal lid<br />
tightening/shortening<br />
• Both<br />
SOF<br />
80