Breaking the silence: helping men with erectile dysfunction
Breaking the silence: helping men with erectile dysfunction
Breaking the silence: helping men with erectile dysfunction

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
CARE OF THE OLDER PERSON<br />
<strong>Breaking</strong> <strong>the</strong> <strong>silence</strong>:<br />
<strong>helping</strong> <strong>men</strong> <strong>with</strong> <strong>erectile</strong> <strong>dysfunction</strong><br />
Ian Peate<br />
Ian Peate is Professor of Nursing and Independent Consultant<br />
Erectüe <strong>dysfunction</strong> does not discriminate and,<br />
while prevalence increases <strong>with</strong> advancing age,<br />
<strong>men</strong> of all ages, ethnic and socioeconomic groups<br />
may, at some point in <strong>the</strong>ir Uves, experience some form of<br />
<strong>erectile</strong> <strong>dysfunction</strong>.<br />
Erectile <strong>dysfunction</strong> is one aspect on a spectrum of sexual<br />
<strong>dysfunction</strong>s <strong>men</strong> may experience.The role and function of<br />
<strong>the</strong> community nurse is wide and varied, and, as such, it is<br />
Ukely that he or she will be required to care for <strong>men</strong> who<br />
have a problem <strong>with</strong> <strong>the</strong> ability to inidate and sustain an<br />
erection for sexual activity. The community nurse, working<br />
<strong>with</strong> various populations, can provide increased awareness<br />
and understanding of <strong>the</strong> condition to patients and partners,<br />
<strong>the</strong> media and o<strong>the</strong>r interested parties.<br />
Sexual health<br />
Sex is an important part of Hfe and relationships, and all people<br />
have a right to enjoy a fiilfilling sexual life; good sexual<br />
health (sexual health fi-ee fiom disease) is one way in which<br />
people achieve this right. Just as health means different things<br />
to different people, so too does sexual health. It is important<br />
to work towards a definidon of sexual health in order to<br />
provide care in a consistent and effecdve way to those who<br />
may have problems <strong>with</strong> <strong>the</strong>ir sexual health.<br />
Sexual health, according to <strong>the</strong>World Health Organization<br />
(WHO, 2002), can be described as:<br />
'A state of physical, <strong>men</strong>tal and social well-being<br />
in relation to sexuality. It requires a positive<br />
ABSTRACT<br />
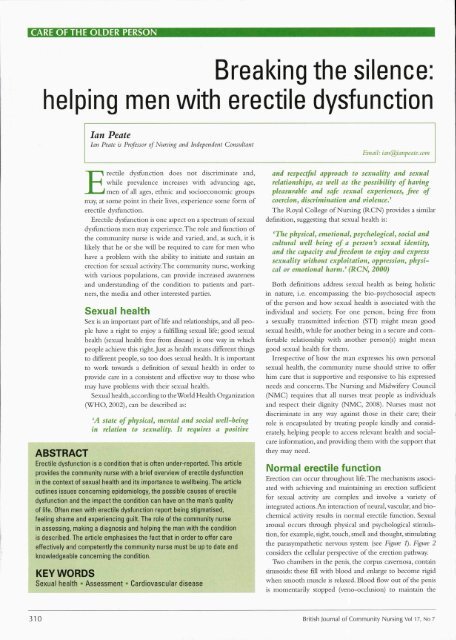
Erectile <strong>dysfunction</strong> is a condition that is often under-reported. This article<br />
provides <strong>the</strong> community nurse <strong>with</strong> a brief overview of <strong>erectile</strong> <strong>dysfunction</strong><br />
in <strong>the</strong> context of sexual health and its importance to wellbeing. The article<br />
outlines issues concerning epidemiology, <strong>the</strong> possible causes of <strong>erectile</strong><br />
<strong>dysfunction</strong> and <strong>the</strong> impact <strong>the</strong> condition can have on <strong>the</strong> man's quality<br />
of life. Often <strong>men</strong> <strong>with</strong> <strong>erectile</strong> <strong>dysfunction</strong> report being stigmatised,<br />
feeling shame and experiencing guilt. The role of <strong>the</strong> community nurse<br />
in assessing, making a diagnosis and <strong>helping</strong> <strong>the</strong> man <strong>with</strong> <strong>the</strong> condition<br />
is described. The article emphasises <strong>the</strong> fact that in order to offer care<br />
effectively and competently <strong>the</strong> community nurse must be up to date and<br />
knowledgeable concerning <strong>the</strong> condition.<br />
I<br />
KEYWORDS<br />
Sexual health • Assess<strong>men</strong>t •- Cardiovascular disease<br />
Email: iati@ianpeatc.com<br />
and respectful approach to sexuality and sexual<br />
relationships, as well as <strong>the</strong> possibility of having<br />
pleasurable and safe sexual experiences, free of<br />
coercion, discrimination and violence.'<br />
The Royal College of Nursing (RCN) provides a similar<br />
definition, suggesdng that sexual health is:<br />
'The physical, emotional, psychological, social and<br />
cultural well being of a person's sexual identity,<br />
and <strong>the</strong> capacity and freedom to enjoy and express<br />
sexuality <strong>with</strong>out exploitation, oppression, physical<br />
or emotional harm.' (RCN, 2000)<br />
Both definitions address sexual health as being holistic<br />
in nature, i.e. encompassing <strong>the</strong> bio-psychosocial aspects<br />
of <strong>the</strong> person and how sexual health is associated <strong>with</strong> <strong>the</strong><br />
individual and society. For one person, being free from<br />
a sexually transmitted infection (STI) might mean good<br />
sexual health, while for ano<strong>the</strong>r being in a secure and comfortable<br />
relationship <strong>with</strong> ano<strong>the</strong>r person(s) might mean<br />
good sexual health for <strong>the</strong>m.<br />
Irrespective of how <strong>the</strong> man expresses his own personal<br />
sexual health, <strong>the</strong> community nurse should strive to offer<br />
him care that is supportive and responsive to his expressed<br />
needs and concerns. The Nursing and Midwifery Council<br />
(NMC) requires that all nurses treat people as individuals<br />
and respect <strong>the</strong>ir dignity (NMC, 2008). Nurses must not<br />
discriminate in any way against those in <strong>the</strong>ir care; <strong>the</strong>ir<br />
role is encapsulated by treating people kindly and considerately,<br />
<strong>helping</strong> people to access relevant health and socialcare<br />
information, and providing <strong>the</strong>m <strong>with</strong> <strong>the</strong> support that<br />
<strong>the</strong>y may need.<br />
Normal <strong>erectile</strong> function<br />
Erection can occur throughout Ufe. The mechanisms associated<br />
<strong>with</strong> achieving and maintaining an erecdon sufficient<br />
for sexual activity are complex and involve a variety of<br />
integrated actions. An interacdon of neural, vascular, and biochemical<br />
activity results in normal <strong>erectile</strong> function. Sexual<br />
arousal occurs through physical and psychological stimuladon,<br />
for example, sight, touch, smell and thought, sdmulating<br />
<strong>the</strong> parasympa<strong>the</strong>dc nervous system (see Figure 1). Figure 2<br />
considers <strong>the</strong> cellular perspective of <strong>the</strong> erection pathway.<br />
Two chambers in <strong>the</strong> penis, <strong>the</strong> corpus cavernosa, contain<br />
sinusoids: <strong>the</strong>se fiH <strong>with</strong> blood and enlarge to become rigid<br />
when smooth muscle is relaxed. Blood flow out of <strong>the</strong> penis<br />
is mo<strong>men</strong>tarily stopped (veno-occlusion) to maintain <strong>the</strong><br />
310 British Journal of Community Nursing Vol 17, No 7
CARE OFTHE OLDER PERSON<br />
4. Rigid erecdon<br />
5. Detumescent<br />
The significant biochemical event in erectue fiancdon is an<br />
increase in <strong>the</strong> amount of cyclic guanosine monophosphate;<br />
this causes smooth-muscle relaxation and permits an erection<br />
to occur. This process is mediated hy nitric oxide, produced<br />
by neurons and elsewhere, acting as a gaseous messenger<br />
molecule.<br />
Figure 7. The penis<br />
Corpus cavemosum<br />
erection. Neural control is complex; in general, <strong>the</strong> sympa<strong>the</strong>tic<br />
nervous system inhibits, and <strong>the</strong> parasympa<strong>the</strong>tic<br />
system excites erectue function. The central nervous system<br />
can induce erections <strong>with</strong>out peripheral stimuK, e.g. in nocturnal<br />
erections. There are five phases associated <strong>with</strong> <strong>erectile</strong><br />
response:<br />
1. Latent<br />
2. Tumescent<br />
3. FuU erection<br />
Erectile <strong>dysfunction</strong><br />
Erectile dysfuncdon is defined as 'inability to achieve or<br />
maintain a penile erection sufficient for sadsfactory sexual<br />
performance' (NIH Consensus Conference on Impotence,<br />
1993). Three events are required to take place for <strong>the</strong> erection<br />
to occur and to be maintained:<br />
• First is sexual arousal<br />
• Second is <strong>the</strong> brain's communication of<strong>the</strong> sexual arousal<br />
to <strong>the</strong> nervous system (activating blood flow)<br />
• Thirdly, relaxation of <strong>the</strong> blood vessels that supply blood<br />
to <strong>the</strong> penis must occur, allowing <strong>the</strong> erection.<br />
If anything occurs that affects any of <strong>the</strong> three events<br />
above — arousal, nervous system response or <strong>the</strong> vascular<br />
system response — or <strong>the</strong> interplay between <strong>the</strong>m, <strong>the</strong>n <strong>the</strong><br />
consequence can be <strong>erectile</strong> <strong>dysfunction</strong>. Erectile dysflinction<br />
should not he confused <strong>with</strong> o<strong>the</strong>r sexual <strong>dysfunction</strong><br />
conditions, such as loss of libido or premature ejaculation.<br />
Causes of <strong>erectile</strong> <strong>dysfunction</strong><br />
Given <strong>the</strong> complexities associated <strong>with</strong> erection, it is not<br />
surprising that a variety of diverse conditions can result in<br />
Smooth - muscle<br />
realaxation (erection)<br />
Figure 2. The<br />
erection at<br />
cellular level<br />
312 British Journal of Community Nursing Vol 17, No 7
CARE OF THE OLDER PERSON<br />
Psychogenic causes<br />
• Anxiety<br />
• Stress<br />
• Guilt about sex (arising<br />
from religion, family,<br />
culture)<br />
• Fatigue<br />
• Relationship problems<br />
(associated <strong>with</strong> power,<br />
trust, intimacy)<br />
• Feelings about partner<br />
(influences sexual<br />
response)<br />
• Depression<br />
• Sexual situation, where<br />
<strong>the</strong> act takes place, time,<br />
choice of person<br />
• Anxiety about performance,<br />
size<br />
uses of <strong>erectile</strong> <strong>dysfunction</strong><br />
' Physical and non-physical<br />
causes of <strong>erectile</strong> <strong>dysfunction</strong><br />
can and do interact<br />
'Too much alcohol,for<br />
example, may alter sexual<br />
response, resulting in<br />
anxiety about attaining an<br />
erection<br />
' Anxiety worsens <strong>erectile</strong><br />
<strong>dysfunction</strong><br />
Physical causes -<br />
•Vascular conditions<br />
• Neurological conditions<br />
•Alcohol<br />
• Medications (for example, major tranquillisers,<br />
antidepressants, endocrine drugs, antihypertensives,<br />
cimetidine, digoxin, metoclopramide,<br />
phenytoin, carbamazepine)<br />
• Diabetes mellitus<br />
• Abnormal nerve function<br />
• Hormone disorders<br />
• Prostatectomy<br />
• Pelvic/abdominal surgical procedures<br />
• Radio<strong>the</strong>rapy<br />
• Peyronie's disease<br />
• Recreational drug use<br />
• Smoking and diet (as contributing factors)<br />
Source: Adapted from Carson and Dean, 2007; Rané and Fraser, 2007; Carson and McMahon, 2008<br />
<strong>erectile</strong> disorders. Eardley (2002) suggests that <strong>the</strong>re are a<br />
number of ways of classifying <strong>the</strong> pathophysiological causes<br />
of <strong>erectile</strong> <strong>dysfunction</strong>:<br />
• Vascular<br />
• Neurogenic<br />
• Endocrinological<br />
• Psychogenic<br />
• Cellular<br />
• Iatriogenic.<br />
Table 1 outlines some of <strong>the</strong> causes of <strong>erectile</strong> <strong>dysfunction</strong>.<br />
Often <strong>the</strong>re may be more than one cause present<br />
at <strong>the</strong> same time. The role of <strong>the</strong> community nurse is to<br />
undertake a holistic assess<strong>men</strong>t <strong>with</strong> <strong>the</strong> aim of making a<br />
diagnosis and offering <strong>the</strong> man treat<strong>men</strong>t and support.<br />
Epidemiology<br />
There have been a number of large epidemiological studies<br />
carried out globally that demonstrate a high prevalence and<br />
incidence of <strong>erectile</strong> <strong>dysfunction</strong>. The Massachusetts Male<br />
Aging Study (MMAS) (<strong>the</strong> most often cited study) conducted<br />
in 1994 reveals <strong>the</strong> prevalence of <strong>erectile</strong> <strong>dysfunction</strong> to<br />
be 52% in non-institutionalised <strong>men</strong> aged 40—70 years, in <strong>the</strong><br />
Boston area; 17.2%, 25.2% and 9.6% for minimal, moderate<br />
and complete <strong>erectile</strong> dysñmction, respectively (Feldman et<br />
al, 1994). A study undertaken in <strong>the</strong> UK of <strong>men</strong> aged 18-75<br />
showed a rate of 39% for Hfetime <strong>erectile</strong> <strong>dysfunction</strong>, <strong>with</strong><br />
a current prevalence of 26% (Dunn et al, 1998). In <strong>the</strong>se<br />
studies <strong>the</strong>re is an age-related increase in <strong>erectile</strong> dysflmcdon.<br />
Making a diagnosis of <strong>erectile</strong><br />
<strong>dysfunction</strong><br />
The NMC (2004) requires all specialist community public<br />
health nurses to collect and structure data and information<br />
on <strong>the</strong> health and weUbeing and related needs of a defined<br />
population.The nurse has to be able to analyse, interpret and<br />
communicate data and information <strong>with</strong> <strong>the</strong> aim of improving<br />
health and social weUbeing: this also applies to <strong>the</strong> health<br />
and weUbeing of <strong>men</strong>. One aspect of <strong>the</strong> community nurse's<br />
role is to undertake a range of screening activities (NMC,<br />
2004), for example, screening patients for undiagnosed<br />
cardiovascular disease. Part of this activity is to undertake a<br />
detailed health-care assess<strong>men</strong>t, which would also include an<br />
assess<strong>men</strong>t of <strong>the</strong> man's sexual function. An in-depth physical<br />
and psychological assess<strong>men</strong>t is required in order to make<br />
an accurate diagnosis. FuU physical, psychological and sexual<br />
health histories are prerequisites.<br />
The nurse should obtain a detailed description of <strong>the</strong><br />
problem, including <strong>the</strong> duration of symptoms as weU as <strong>the</strong><br />
original cause(s) of <strong>the</strong> problem (see Table 1). The British<br />
Society of Sexual Medicine (BSSM) (2008) suggests that<br />
o<strong>the</strong>r factors that should be identified and recorded will<br />
include: ' .•.'_;! _. f«ii?. ''h:<br />
• Any subsequent investigations<br />
• Treat<strong>men</strong>t interventions along <strong>with</strong> <strong>the</strong> response achieved<br />
• An expression of tumescence and rigidity <strong>with</strong> quality of<br />
morning awakening erections, and spontaneous, masturbatory<br />
or partner-related activity erections<br />
• Sexual desire, ejaculatory and orgasmic <strong>dysfunction</strong><br />
• Previous <strong>erectile</strong> capacity<br />
• Issues around any sexual aversion or sexual pain<br />
• Partner issues e.g. <strong>men</strong>opause or vaginal pain.<br />
The detailed assess<strong>men</strong>t requires <strong>the</strong> nurse to encourage<br />
<strong>the</strong> man, in a respectful and sensitive manner, to clarify any<br />
problems he may have related to his sexual function. O<strong>the</strong>r<br />
considerations that <strong>the</strong> nurse needs to think about when<br />
making a diagnosis are those factors related to precipitation,<br />
predisposing and maintenance factors (BSSM, 2008) (see<br />
Table 2).<br />
Any coexisting medical, psychiatric and surgical history<br />
should also be recorded, as well as <strong>the</strong> man's current rela-<br />
314 British Journal of Community Nursing Vol 17, No 7
CARE OFTHE OLDER PERSON<br />
Table 2. Some factors to consider when rnaking a diagnosis<br />
Precipitation<br />
• Lack of sexual knowledge<br />
• Negative previous sexual<br />
experience(s)<br />
• Relafionship problems<br />
• Religious or cultural beliefs<br />
• Restrictive upbringing<br />
^_____<br />
• Confusion concerning sexual or<br />
gender preference<br />
• Sexual abuse<br />
• Physical or <strong>men</strong>tal healfh problems<br />
• Ofher sexual problems in fhe man<br />
or his partner<br />
• Use of drugs<br />
Predisposing<br />
• New relationship<br />
• Acufe relafionship problems<br />
• Family or social pressures<br />
• Pregnancy and childbirth<br />
• O<strong>the</strong>r major life events<br />
• Partner's <strong>men</strong>opause<br />
• Acute physical or <strong>men</strong>tal health<br />
problems<br />
• Lack of knowledge concerning <strong>the</strong><br />
usual changes of ageing<br />
• Ofher sexual problems in <strong>the</strong> man<br />
or his partner<br />
• Use of drugs<br />
'ource: Adapted from Carson and Dean, 2007; : BSSM, 2008; Carson and McMahon, 2008<br />
Maintenance<br />
' Problems <strong>with</strong> relationship(s)<br />
• Poor communication between<br />
partners<br />
' Knowledge deficit concerning<br />
treat<strong>men</strong>t options<br />
• Long term physical or <strong>men</strong>tal<br />
health problems<br />
' Ofher sexual problems in <strong>the</strong> man<br />
or his partner<br />
• Use of drugs<br />
tionship status (single, married, in a long-term relationship);<br />
a history of previous sexual partners and relationships will<br />
also he required. Sexual orientation and gender identity<br />
should also be noted. The nurse must also ask <strong>the</strong> patient<br />
ahout alcohol, smoking and illicit drug use.<br />
Validated questionnaires are available that will help <strong>the</strong><br />
nurse to make <strong>the</strong> consultation more objective: for example,<br />
<strong>the</strong> International Index of Erectile Function (IIEF)<br />
(Rosen et al, 1997) or <strong>the</strong> validated shorter version of<strong>the</strong><br />
SHIM (Sexual Health Inventory for Men) (Cappelleri and<br />
Rosen, 2005) help to assess sexual function, and also <strong>the</strong><br />
impact of treat<strong>men</strong>ts and interventions. These tools are only<br />
an adjunct to a detailed history and physical examination,<br />
however, <strong>the</strong>y do not replace <strong>the</strong>m.<br />
According to <strong>the</strong> BSSM (2008), <strong>erectile</strong> dysfuncdon and<br />
coronary heart disease have <strong>the</strong> same risk factors. It is important<br />
to note that coronary artery disease is frequently only<br />
one of <strong>the</strong> affected sites in a generalised arteriopathy that<br />
has <strong>the</strong> ability to impact on arterial blood inflow to <strong>the</strong> corpora<br />
cavernosum.The penile arteries are substantially smaller<br />
than <strong>the</strong> main coronary arteries, and <strong>erectile</strong> <strong>dysfunction</strong><br />
frequently pre-dates coronary artery disease (Montorsi et al,<br />
2004), hence <strong>the</strong> need for <strong>the</strong> nurse to approach <strong>the</strong> assess<strong>men</strong>t<br />
of <strong>the</strong> patient fi-om a hoUsdc perspective.<br />
Physical examination<br />
There is controversy concerning <strong>the</strong> need to perform a<br />
physical examination of<strong>the</strong> genitalia. The physical examination<br />
should focus on secondary sexual characteristics, an<br />
abdominal examination, major pulse examination, S2—4<br />
neurological assess<strong>men</strong>t and external genitalia examination.<br />
This type of examination should be undertaken by a specialist<br />
skilled practitioner. The history gained from <strong>the</strong> man<br />
will direct <strong>the</strong> nurse to determine if a physical examination<br />
is required (see Table 3).<br />
The BSSM (2008) suggests that all patients should have a<br />
focused physical examination and a genital examination is<br />
recom<strong>men</strong>ded; this is essential if <strong>the</strong>re is a history of rapid<br />
onset of pain, deviation of<strong>the</strong> penis during tumescence, <strong>the</strong><br />
symptoms of hypogonadism or o<strong>the</strong>r current or past urological<br />
symptoms. If <strong>the</strong> nurse suspects Peyronie's disease<br />
this would merit assess<strong>men</strong>t of <strong>the</strong> peripheral vasculature<br />
(Rané and Fraser, 2007). It is not obligatory to perform a<br />
digital rectal examination; however, this should be considered<br />
if <strong>the</strong>re is evidence of genito-urinary or protracted<br />
secondary ejaculatory symptoms (Carson and McMahon,<br />
2008). Blood pressure, heart rate, waist circumference and<br />
weight should be measured.<br />
O<strong>the</strong>r investigations may be indicated and are tailored<br />
to <strong>the</strong> needs of <strong>the</strong> patient after an in-depth assess<strong>men</strong>t<br />
Table 3. Individual examination and assess<strong>men</strong>t<br />
Assess general appearance.<br />
Are <strong>the</strong>re signs of<br />
o<strong>the</strong>r illnesses:<br />
Assess secondary sexual<br />
characteristics:<br />
Assess genitalia:<br />
Assess physical parameters.<br />
Measure:<br />
• Depression<br />
•Thyroid problems<br />
• Parkinson's disease<br />
• Distribution of body hair (facial, pubic,<br />
body)<br />
• Muscle develop<strong>men</strong>t<br />
• Distribution of body fat<br />
• Observe, palpate and examine penile<br />
shaft, foreskin (if present)<br />
• Any evidence of swelling, lumps, tenderness<br />
• Any evidence of sexually transmitted<br />
infection<br />
• Inspect and palpate scrotal sac and<br />
contents (what size are <strong>the</strong> testes develop<strong>men</strong>tally)<br />
• Blood pressure<br />
• Heart rate<br />
•Waist circumference<br />
•Weight<br />
Source: Adapted from Carson and Dean, 2007; BSSM, 2008<br />
British Journal of Community Nursing Vol 17, No 7 315
CARE OF THE OLDER PERSON<br />
has taken place, as weU as in response to <strong>the</strong> wishes of <strong>the</strong><br />
patient. Carson and Dean (2007) have suggested that <strong>the</strong><br />
foUowing should be performed for all <strong>men</strong> <strong>with</strong> erectue<br />
<strong>dysfunction</strong>, accompanied by a detailed cardiovascular<br />
assess<strong>men</strong>t that includes:<br />
• Fasting glucose<br />
• Urinalysis for glucose<br />
• Total HDL and cholesterol and triglycérides<br />
• Total testosterone, sex hormone binding globulin and<br />
albu<strong>men</strong><br />
• Prolactin<br />
• Prostate specific antigen<br />
Carson and McMahon (2008) suggest that in addition to<br />
<strong>the</strong> above, <strong>the</strong> foUowing specialist clinical investigations may<br />
be required:<br />
• Nocturnal penile tumescence rigidity testing<br />
• Colour Doppler imaging<br />
• Pharmacocavernosography<br />
• Pharmacoarteriography<br />
• Psychiatric evaluation<br />
• Vascular evaluation<br />
• Cardiac evaluation.<br />
Treat<strong>men</strong>t and nursing care<br />
Eardley (2002) noted that, in <strong>the</strong> general population, <strong>the</strong><br />
most common causes of erectUe <strong>dysfunction</strong> are vascular,<br />
<strong>with</strong> increasing evidence that <strong>the</strong> risk factors for a<strong>the</strong>rosclerosis,<br />
specificaUy hypertension, smoking, hyperlipidaemia and<br />
diabetes, are aU associated <strong>with</strong> erectue <strong>dysfunction</strong>.There are<br />
two key consequences:<br />
Figure 3. Intercavernosal injection <strong>the</strong>rapy<br />
1. Control of <strong>the</strong>se risk factors would help to reduce <strong>the</strong><br />
risk of <strong>erectile</strong> <strong>dysfunction</strong><br />
2. When a man presents <strong>with</strong> <strong>erectile</strong> <strong>dysfunction</strong> <strong>the</strong><br />
nurse must identify <strong>the</strong>se risk factors, not only <strong>with</strong> <strong>the</strong><br />
intention of improving <strong>the</strong> <strong>erectile</strong> <strong>dysfunction</strong>, but to also<br />
aim to prevent future cardiovascular sequelae.<br />
As weU as <strong>helping</strong> <strong>men</strong> <strong>with</strong> problems associated <strong>with</strong> <strong>the</strong><br />
physical and psychological impact of <strong>erectile</strong> <strong>dysfunction</strong>, <strong>the</strong><br />
nurse must also ensure that measures are put in place to deal<br />
<strong>with</strong> <strong>the</strong> potential cardiovascular consequences.<br />
Erectile <strong>dysfunction</strong> can have a significant impact on a<br />
man, his partner(s) and <strong>the</strong>ir relationships, ofi:en resulting<br />
in a reduction in self-esteem and poor quality of life. Men<br />
report feeling guilty and experiencing a sense of shame<br />
Table 4. Treat<strong>men</strong>t ODtions<br />
^ Treat<strong>men</strong>t option<br />
First line<br />
Second line<br />
Third line<br />
Description<br />
• Provision of education that reinforces sexual function, sexual responsiveness, sexual<br />
satisfaction and sexuality<br />
• Debunking of myths<br />
• Promotion of sex and <strong>the</strong> older person and intimacy<br />
• Consider referral to sexual and relationship <strong>the</strong>rapist (psychosexual <strong>the</strong>rapy)<br />
• Advice should be provided about lifestyle issues such as <strong>the</strong> harmful effects of cigarette<br />
smoking, use of alcohol and illicit drugs and <strong>the</strong> benefits of exercise<br />
• Depression and dyslipldemias if present should be addressed and corrected<br />
• Review and revision of current medications may be needed<br />
• O<strong>the</strong>r <strong>the</strong>rapeutic options may be indicated if <strong>the</strong>re is evidence of o<strong>the</strong>r underlying<br />
pathology such as hypertension and coronary heart disease or poorly controlled diabetes<br />
• Administration of oral <strong>the</strong>rapies such as sildenafil, tadalafil, vardenafil and sublingual<br />
apomorphine as required<br />
• Use of a vacuum tumescence device <strong>with</strong> a constriction ring<br />
• Administration of oral <strong>the</strong>rapies such as sildenafil, tadalafil, vardenafil and sublingual<br />
apomorphine on a daily basis<br />
• Administration of intracavernosal injections such as alprostadil (see Figure 5)<br />
•Administration oftransurethral pellets, such as alprostadil<br />
• Penile implant surgery<br />
Source: BSSM, 2008; Carson and McMahon, 2008<br />
•Vascular reconstructive surgery<br />
316 British Journal of Community Nursing Vol 17, No 7
CARE OFTHE OLDER PERSON<br />
(Engender Health, 2003), and <strong>the</strong> stigma associated <strong>with</strong><br />
<strong>erectile</strong> <strong>dysfunction</strong> can cause <strong>the</strong> man to <strong>with</strong>draw from<br />
intimacy. In some cases all forms of physical contact can<br />
become non-existent, resulting in emotional distress, causing<br />
stress and adding to <strong>the</strong> psychogenic component associated<br />
<strong>with</strong> <strong>erectile</strong> <strong>dysfunction</strong>. Treat<strong>men</strong>t has <strong>the</strong> potential<br />
to resolve depression and improve <strong>the</strong> man's self esteem and<br />
overall quality of life and sense of weDbeing (Carson and<br />
McMahon, 2008).<br />
Currently, practitioners working in <strong>the</strong> primary care<br />
setting imple<strong>men</strong>t <strong>the</strong> guidance issued by <strong>the</strong> Depart<strong>men</strong>t<br />
of Health (DH), in a number of Health Service Circulars<br />
(DH, 1999a; 1999b; 1999c), to determine <strong>the</strong> manage<strong>men</strong>t<br />
and treat<strong>men</strong>t of <strong>men</strong> <strong>with</strong> <strong>erectile</strong> dysfiinction.The circulars<br />
provide <strong>the</strong> community nurse <strong>with</strong> guidance on good<br />
practice for those <strong>men</strong> who qualify for treat<strong>men</strong>t <strong>with</strong>in<br />
<strong>the</strong> NHS. Fur<strong>the</strong>r guidelines have heen produced hy <strong>the</strong><br />
BSSM (2008); this guidance, while still adhering to <strong>the</strong><br />
current DH circulars, is underpinned hy a more up-to-date<br />
evidence base.<br />
Regardless of <strong>the</strong> treat<strong>men</strong>t plan chosen, <strong>the</strong> nurse has<br />
a duty to provide <strong>the</strong> man and (if appropriate) his partner<br />
<strong>with</strong> appropriate and adequate informadon to help<br />
him understand <strong>the</strong> reasons why <strong>erectile</strong> dysfiinction has<br />
occurred. Explaining to <strong>the</strong> man how his problem compares<br />
<strong>with</strong> <strong>the</strong> general population may help him feel less<br />
stigmatised, and debunking any myths associated <strong>with</strong><br />
<strong>erectile</strong> <strong>dysfunction</strong> can provide an opportunity for him<br />
and his partner to understand each o<strong>the</strong>r's sexual needs and<br />
<strong>the</strong>ir sexuality and to chose <strong>the</strong> most appropriate treat<strong>men</strong>t.<br />
There are a number of treat<strong>men</strong>t options available for<br />
<strong>erectile</strong> <strong>dysfunction</strong>, and inany of <strong>the</strong>se have been developed<br />
and revised over time, becoming more effective.<br />
Carson and McMahon (2008) consider treat<strong>men</strong>t options<br />
from psychogenic and organic perspectives. The choice of<br />
treat<strong>men</strong>t will depend on several factors, such as patient<br />
(and, if appropriate, partner) preference, severity of <strong>erectile</strong><br />
<strong>dysfunction</strong> and <strong>the</strong> underlying cause. Rané and Fraser<br />
(2007) recom<strong>men</strong>d a 'step ladder' approach to treat<strong>men</strong>t,<br />
progressing from non-invasive talking <strong>the</strong>rapies and drug<br />
<strong>the</strong>rapies, to minimally invasive injection <strong>the</strong>rapy {Figure 3)<br />
and vacuum devices, to invasive pros<strong>the</strong>tic surgery. Table 4<br />
provides an overview of treat<strong>men</strong>t options.<br />
In order to help <strong>the</strong> patient chose <strong>the</strong> right treat<strong>men</strong>t<br />
option, <strong>the</strong> nurse must have an up-to-date and in-depth<br />
knowledge base. Not all treat<strong>men</strong>t opdons will suit all <strong>men</strong>,<br />
and <strong>the</strong>y all have side-effects and contraindications. There<br />
is no 'one size fits all' approach: each man must be assessed<br />
and treated as an individual. The information and advice<br />
that <strong>the</strong> nurse offers should he provided in such a way that<br />
<strong>the</strong> man understands <strong>the</strong> options, <strong>the</strong> advantages and drawhacks,<br />
<strong>with</strong> <strong>the</strong> intention of making an informed choice.<br />
Conclusion<br />
Erectile <strong>dysfunction</strong> can have devastating effects on individuals.<br />
Men report feelings of guilt and shame, and experience<br />
stigma associated <strong>with</strong> this condition that can lower<br />
self esteem and impact negatively on <strong>the</strong> person's sense of<br />
wellbeing. Community nurses are ideally placed to help<br />
<strong>men</strong> and, if appropriate, <strong>the</strong>ir partner(s) to come to terms<br />
<strong>with</strong> <strong>the</strong> condition and to select <strong>the</strong> most appropriate<br />
treat<strong>men</strong>t option. In order to provide this information it<br />
is essential that <strong>the</strong> nurse is knowledgeable and up-to-date<br />
<strong>with</strong> contemporary approaches to <strong>the</strong> care and manage<strong>men</strong>t<br />
of <strong>men</strong> <strong>with</strong> <strong>erectile</strong> <strong>dysfunction</strong>.<br />
BJCN<br />
Acknowledge<strong>men</strong>ts: I would like to thank Mrs Frances Cohen for<br />
her help and support.<br />
British Society for Sexual Medicine (2008) British Society for Sexual Medicine<br />
Guidelines on <strong>the</strong> Manage<strong>men</strong>t of Erectue Dysfuncdon. J Sex Med 5(8):<br />
1841-^5<br />
Cappelleri JC, Rosen RC (2005) The Sexual Health Inventory for Men (SHIM):<br />
A 5-year Review of Research and Clinical Experience. Ini j hnpoc Res 17:<br />
307-19<br />
Carson CC, Dean JD (2007) Manage<strong>men</strong>t of Erectile Dysfunction in Clinical Practice.<br />
Springer, London<br />
Carson CC, McMahon CG (2008) Erectile Dysfunction. 4th Edn. Health Press,<br />
Abingdon<br />
Depart<strong>men</strong>t of Health (1999a) Health Service Circular/115. DH, London<br />
Depart<strong>men</strong>t of Health (1999b) Health Service Circular/148. DH, London<br />
Depart<strong>men</strong>t of Health (1999c) Heahh Service Circular HSC/U?. DH, London<br />
Dunn KM, Croft PR, Hackett GI (1998) Sexual Problems: A Study of <strong>the</strong><br />
Prevalence and Need for Health Care in <strong>the</strong> General Population. Fam Pract<br />
15(6): 519-24<br />
Eardley I (2002) Pathophysiology of <strong>erectile</strong> <strong>dysfunction</strong>. BrJ Diabetes Vase Dis<br />
2(4): 272-6<br />
Engender Health (2003) Men's Reproductive Health Curriculum. 3:<br />
Manage<strong>men</strong>t of Men's Reproductive Health Problems. http://tinyurl.coni/<br />
dxx7x37 (Accessed 27 June 2012)<br />
Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ, McKinlay JB (1994)<br />
Impotence and its medical and psychosocial correlates: results of <strong>the</strong><br />
Massachusetts Male Aging Study.J tjrol 151(1): 54-61<br />
Montorsi P, Ravagnani PM, Galli S et al (2004) Common grounds for <strong>erectile</strong><br />
<strong>dysfunction</strong> and coronary artery disease. Curr Opin Urot 14(6): 361-5<br />
NIH Consensus Conference on Impotence (1993) NIH Consensus Develop<strong>men</strong>t<br />
Panel on Impotence.J^Ai/1 270(1): 83-90<br />
Nursing and Midwifery Council (2004) Standards of Proficiency for Specialist<br />
Community Public Health Nurses. NMC, London<br />
Nursing and Midwifery Council (2008) The Code: Standards of Conduct,<br />
Performance and Ethics for Nurses and Midwives. NMC, London<br />
Rané A, Fraser M (2007) Erectile Dysfunction Digest. Merit Publishing<br />
International, West Palm Beach, Florida<br />
Rosen RC.Riley A, Wagner G, Osterloh IH, KirkpatnckJ, Mishra A (1997) The<br />
International Index of Erectile Function (IIEF):A multidi<strong>men</strong>sional scale for<br />
assess<strong>men</strong>t of <strong>erectile</strong> <strong>dysfunction</strong>. Urology 49(6): 822-30<br />
Royal College of Nursing (2000) Sexuality and Sexual Health in Nursing Practice.<br />
RCN, London<br />
World Health Organisation (2002) Gender and Human Rights - Sexual Heahh.<br />
WHO. Geneva<br />
LEARNING POINTS<br />
• Sex is an important aspect of many people's lives<br />
• Our understanding of <strong>erectile</strong> <strong>dysfunction</strong> continues to develop<br />
• The community nurse is ideally placed to help <strong>men</strong> (and <strong>the</strong>ir partners)<br />
who experience <strong>the</strong> physical and psychological impact <strong>erectile</strong><br />
<strong>dysfunction</strong> can have on <strong>the</strong>ir lives and wellbeing<br />
• Any condition that damages endo<strong>the</strong>lial function can result in <strong>erectile</strong><br />
<strong>dysfunction</strong><br />
• Some <strong>men</strong> <strong>with</strong> <strong>erectile</strong> <strong>dysfunction</strong> will also have coexisting conditions<br />
such as hypertension, hyperlipidaemia, diabetes and depression<br />
British Journal of Community Nursing Vol 17, No 7 317
Copyright of British Journal of Community Nursing is <strong>the</strong> property of Mark Allen Publishing Ltd and its<br />
content may not be copied or emailed to multiple sites or posted to a listserv <strong>with</strong>out <strong>the</strong> copyright holder's<br />
express written permission. However, users may print, download, or email articles for individual use.




![The Rink - Cyril Dabydeen[1].pdf](https://img.yumpu.com/21946808/1/155x260/the-rink-cyril-dabydeen1pdf.jpg?quality=85)