척추관절통증증후군 - KoreaMed Synapse
척추관절통증증후군 - KoreaMed Synapse
척추관절통증증후군 - KoreaMed Synapse

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Korean J Pain Vol. 21, No. 1, 2008<br />
대한통증학회지 2008; 21: 1−10<br />
DOI:10.3344/kjp.2008.21.1.1 □ 종 설 □<br />
<strong>척추관절통증증후군</strong><br />
부산대학교 의학전문대학원 마취통증의학교실<br />
김 경 훈<br />
Spinal Joint Pain Syndrome<br />
Kyung Hoon Kim, M.D.<br />
Department of Anesthesia and Pain Medicine, School of Medicine, Pusan National University, Busan, Korea<br />
Spinal joint pain syndrome is composed of atlanto-occipital, atlanto-axial, facet, and sacro-iliac joints pain.<br />
The syndrome is characterized as referred pain which is originated from deep somatic tissues, which is quietly<br />
different from radicular pain with dermatomal distribution originated from nerve root ganglion. The prevalence<br />
of facet joint pain in patients with chronic spinal pain of cervical, thoracic, and lumbar regions has been known<br />
56%, 42%, and 31% as in order. It is generally accepted in clinical practice that diagnostic blocks are the<br />
most reliable means for diagnosing spinal joints as pain generators. The sacroiliac joint has been shown to<br />
be a source of 10% to 27% of suspected cases with chronic low back pain utilizing controlled comparative<br />
local anesthetic blocks. The treatment of spinal joints ideally consists of a multimodal approach comprising<br />
conservative therapy, medical management, procedural interventions, and if indicated. (Korean J Pain 2008;<br />
21: 1−10)<br />
Key Words:<br />
diagnosis, facet joint, pain, spine, treatment.<br />
서 론<br />
척추는 후두-환추 관절을 통해 두개골과 천장관절을<br />
통해 골반과 연결된다. 앞쪽 구조물인 경추 2−3번에서<br />
부터 요추 5−천추 1번 사이의 간의 추간판을 제외하고,<br />
후두-환추 관절, 환추-축추 관절, 경추 2−3번부터 요추<br />
5−천추 1번에 이르는 후관절 및 천장관절 등의 척추관<br />
절통증증후군에 관한 해부, 흔한 동반 질환, 진단 및 치<br />
료에 관해 소개하고자 한다.<br />
본 론<br />
척추 통증을 일으키는 해부학적 구조물은 다음과 같<br />
은 4가지 특징을 충족해야 한다. 1) 그 구조물은 신경분<br />
포를 가지고 있어야 하고(Fig. 1), 2) 정상 지원자들에서<br />
임상적으로 관찰할 수 있는 비슷한 통증을 유발할 수 있<br />
어야 하고, 3) 통증이 있는 질환과 손상에 감수성이 있어<br />
야 하며, 4) 신뢰성과 타당성이 있는 진단적 방법을 이용<br />
하여 그 구조물이 환자의 통증의 근원이 된다는 것을 규<br />
명해야 한다. 1) 척추 후관절의 경우 활액낭에 작은 C형<br />
통증 섬유가 둘러싸고 있다. 뿐만 아니라 단백유전자산<br />
물 9.5 (protein gene product 9.5), substance P 및 calcitonin<br />
gene-related peptide 등에 반응하는 신경섬유가 규명되어<br />
있고, 통증 유발이 가능하고, 후관절 증후군이 임상적으<br />
로 존재하며, 진단적 차단으로 통증을 차단할 수 있다. 2)<br />
1. 후두-환추 관절과 환추-축추 관절 통증<br />
1) 해부: 상부 경추의 운동 분절은 하부 경추와는 다른<br />
특수한 구조를 가지고 있다. 후두-환추 관절은 경추 1번<br />
접수일:2008년 3월 16일, 승인일:2008년 3월 28일<br />
책임저자:김경훈, (602-739) 부산시 서구 아미동 1-10<br />
부산대학교 의학전문대학원 마취통증의학교실<br />
Tel: 051-240-7394, Fax: 051-242-7394<br />
E-mail: pain@pusan.ac.kr<br />
Received March 16, 2008, Accepted March 28, 2008<br />
Correspondence to: Kyung Hoon Kim<br />
Department of Anesthesia and Pain Medicine, School of Medicine,<br />
Pusan National University, 1-10, Ami-dong, Seo-gu, Busan 602-739,<br />
Korea<br />
Tel: +82-51-240-7394, Fax: +82-51-242-7394<br />
E-mail: pain@pusan.ac.kr
2 KH Kim / Korean J Pain Vol. 21, No. 1, 2008<br />
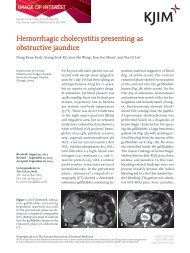
Fig. 1. Average number of receptors (and standard deviation) on<br />
the nine spots of the dorsal aspect of the facet joint capsule. The<br />
asterisks indicate a significantly higher number of receptors at a<br />
particular spot. S = Spot. More A-δ receptors were found around<br />
Spot 3, which was on the dorsolateral aspect of the facet joint<br />
at the joint gap, where muscles were attached. More C-fiber<br />
receptors were found at Spot 9, which was located at the<br />
dorsolateral part of the capsule, at the caudal marginal region.<br />
(From Chen C, Lu Y, Kallakuri S, Patwardhan A, Cavanaugh JM:<br />
Distribution of A-delta and C-fiber receptors in the cervical facet<br />
joint capsule and their response to stretch. J Bone Joint Surg Am<br />
2006; 88: 1807-16.)<br />
(환추)의 상관절면과 후두가 만나서 생기며, 변형된 후<br />
관절처럼 보인다. 환추(C1)는 추체가 없으며, 후두(C0)<br />
와 축추(C2) 사이를 연결해 주는 중심 역할(relay center)<br />
을 해 주고 있다(Fig. 2A). 3)<br />
축추(C2)의 가장 뚜렷한 특징은 치아돌기(odontoid<br />
process, dens)로서 축추의 골 분절의 앞쪽에서부터 나와<br />
아스파라거스와 같은 모양으로 돌출되어 있고, 환추와<br />
머리가 회전할 때 축의 역할을 한다(Fig. 2B).<br />
시상면에서 좌우의 양쪽으로 볼록한 외측의 환추-축<br />
추 관절은 1.4−3.2 mm 정도의 두꺼운 관절연골과 관절<br />
내의 반월연골에 의해 둘러싸여 있다. 이 관절을 통해<br />
굴곡, 신전, 회전 및 매우 작은 정도의 측면굴절(sidebending)이<br />
가능하다(Fig. 2C).<br />
인대의 통합성(ligament integrity)은 뇌줄기와 척수와<br />
인접하여 상부 경추의 골성 구조물 사이에 존재하므로<br />
필수적이다. 환추의 횡인대(transverse ligament of atlas)<br />
는 환추와 축추의 분리를 막기 위해 치아돌기의 뒤쪽에<br />
존재하는 lateral mass들 사이를 지난다. 이 횡인대는 경<br />
추의 굴곡 시에 치아돌기가 뇌줄기와 척수 방향으로 뒤<br />
쪽으로 끼이는 것을 막는다(Fig. 2D).<br />
환추의 횡인대는 치아돌기의 중심 위치를 유지하기<br />
위해 날개 인대들(alar ligaments)에 의해 보조를 받고 있<br />
다. 길이가 11−13 mm 정도인 좌우 후두날개인대의 가<br />
지들은 모두 각각 치아돌기의 뒤쪽 꼭대기에서 후두로<br />
달린다(Fig. 2E).<br />
환추-후두 관절과 환추-축추 관절의 해부학적 위치,<br />
가동범위 및 기능을 Table 1에 정리하였다.<br />
2) 경추인성 두통(cervicogenic headache): 목에서 유<br />
래한 통증이란 의미의 경추인성 두통은 1983년 Sjaastad<br />
가 “목에서 유래하는 재발이 잦고, 오래 지속되는 심한<br />
일측성 두통”으로 정의하였다(Table 2). 4) 그 이후 Sjaastad<br />
의 일부 수정된 내용, 세계두통학회(International Headache<br />
Society) 및 세계통증연구학회(International Association<br />
for the Study of Pain) 등에서 정의한 내용은 Table 3과<br />
같다. 5) 필수적인 증상들로 적어도 2−3시간 지속되는<br />
두통 이외에 어지럼증, 시각장애 및 현훈 등을 들 수 있<br />
다. 6)<br />
상부 경추 신경근들들로부터 감각 입력이 삼차신경핵<br />
(trigeminal nucleus)에 수렴되면서 경추인성 두통을 갖게<br />
되는 기전을 Fig. 2F에서 볼 수 있다. 7)<br />
3) 환추-후두 관절과 환추-축추 관절의 관절 내 주사:<br />
상기 시술에서 가장 주의할 사항은 척추동맥의 주행이<br />
다(Fig. 2G). 척추동맥은 환추-축추 관절의 외측과 환추-<br />
후두 관절의 내측으로 주행하므로, 환추-축추 관절은 관<br />
절의 내측부에 바늘을 자입한다는 느낌으로, 반면 환추-<br />
후두 관절은 관절의 외측부에 주입한다는 느낌을 가지<br />
면서 바늘이 작은 점으로 보일 수 있게 만든다 (through<br />
the eye of the needle technique) (Fig. 2H). 8) 환자로부터<br />
시술 직후 후부부의 두통이 없어지는 것은 물론 시력이<br />
갑자기 좋아진 느낌과 귀가 후 이전에 가졌던 어지럼증<br />
과 현훈이 없어지거나 현저히 줄었다는 말을 다음 추적<br />
관찰에서 들을 수 있다.<br />
시술 전 환추-후두 관절과 환추-축추 관절의 통증을<br />
연관통의 분포로 식별하기는 어렵지만, 환추-축추 관절
김경훈: <strong>척추관절통증증후군</strong> 3<br />
Fig. 2. (A) The atlas (C1): 1 facet for the dens; 2 anterior tubercle; 3 posterior tubercle; 4 transverse foramen; 5 groove for the vertebra<br />
artery; 6 cartilage over superior articular facet. (B) The axis (C2), cranial (a) and sagittal (b) view: 1 dens or odontoid process; 2 superior<br />
articular facet; 3 spinous process; 4 groove for transverse ligament of atlas; 5 facet for anterior arch of the atlas; 6 transverse foramen.<br />
(C) Lateral atlantoaxial joint (C1-C2). Biconvexity in the sagittal plane. (D) The ligaments of the upper cervical spine: 1 occiput; 2 posterior<br />
arch of the atlas; 3 anterior arch of the atlas; 4 dens of the axis; 5 posterior arch of C2; 6 vertebral body of C3; 7 posterior atlanto-occipital<br />
membrane; 8 ligamentum flavum, C1C2; 9 ligamentum flavum, C2C3; 10 anterior longitudinal ligament; 11 anterior atlanto-occipital<br />
membrane; 12 apical ligament of the atlas; 13 tectorial membrane; 14 posterior longitudinal ligament; 15 transverse ligament of atlas;<br />
16 Synovial compartment between the dens and the anterior arch of the atlas. (E) The alar ligaments (dorsal view): 1 left occipital alar<br />
ligament; 2 right occipital alar ligament; 3 left atlantal alar ligament; 4 right atlantal alar ligament; 5 occiput; 6 left C1; 7 right C1; 8<br />
dens; 9 left C2; 10 right C2. (F) Convergence of sensory input from the upper cervical nerve roots into the trigeminal nucleus<br />
(cervicotrigeminal interneuronal relay). (G) Diagram of the placement of 25-gauge spinal needle into the anterior axial joint on the left<br />
(atlanto-axial) and the anterior occipital joint on the right (atlanto-occipital) as seen by "through the eye of the needle" technique. The<br />
spatial relationships of the needles with the vertebral arteries, foramen magnum, and spinal cord are shown. The circled dot is equivalent<br />
to "through the eye of the needle."<br />
의 통증은 후두하부(suboccipital area)에 국한되지만 환<br />
추-후두 관절 통증은 후두 및 후두하부에 분산된 형태의<br />
통증분포를 보인다(Fig. 2I).<br />
병력으로 흔히 편타 손상(whiplash injury)과 같은 외<br />
상, 퇴행성 변화 및 류마티스 관절염 등을 들 수 있다.<br />
4) 제2경추신경의 후신경절 블록: 후두통(occipital<br />
headache)을 호소하는 환자에서 후두 신경통이 의심되면<br />
제2경추 신경의 후지인 대후두신경 혹은 Fig. 2J에서와<br />
같이 후신경절을 차단할 수 있다. 하지만 관절에서 유래<br />
한 통증이라면 그 관절을 목표로 하는 것이 옳다.
4 KH Kim / Korean J Pain Vol. 21, No. 1, 2008<br />
Fig. 2. Continued. (H) Atlantooccipital<br />
(a) and atlanto-axial (b)<br />
joint injections. (I) Referral zone<br />
of atlanto-occipital (a) and atlantoaxial<br />
(b) joint pain. (J) Right C2<br />
ganglion block: (a) anteroposterior<br />
view, (b) lateral view.
김경훈: <strong>척추관절통증증후군</strong> 5<br />
Table 1. Anatomy, Range of Motion, and Function of the Atlanto-occipital and the Atlanto-axial Joint<br />
Joint Anatomic position Passive range of motion Function<br />
Atlanto-occipital joint<br />
Atlanto-axial joint<br />
The joint between the C1 vertebra<br />
or "Atlas" and the skull<br />
The joint between the C1 vertebra<br />
or "atlas" and the C2 vertebra or<br />
"Axis"<br />
Flexion passive range of<br />
motion of about 10 degrees<br />
Extension passive range of<br />
motion of about 25 degrees<br />
Lateral rotation of about 70<br />
degrees on either side with<br />
the movement occurring<br />
around the odontoid process<br />
Isolated flexion and extension<br />
of 5 degrees and 10 degrees,<br />
respectively, in and itself<br />
50% of the flexion and<br />
extension in the neck<br />
Nodding the head to indicate:<br />
"yes"<br />
50% of the side to side turning<br />
in the neck<br />
Shaking the head to indicate:<br />
"no"<br />
Table 2. Criteria to Include Cervicogenic Headache in Differential<br />
Diagnosis<br />
Typically, the headache:<br />
1. Is recurrent, long-lasting and severe<br />
2. Arises from the neck<br />
3. Has a unilateral dominance (but can bilateral)<br />
4. Is in the low occipital and temporal region (with possible<br />
radiation in the face, periorbital, frontal and parietal region<br />
and ipsilateral shoulder and arm)<br />
5. Is accompanied with a reduced cervical spine range of<br />
motion<br />
6. Can be precipitated<br />
2. 후관절 증후군<br />
정상적인 척추는 추체와 추간판과 같은 앞쪽 구조물이<br />
체중을 지탱하는 구조물들인 데 비해, 경추, 흉추 및 요<br />
추의 후관절은 체중 분배에서 보조해 주는 역할을 한다.<br />
그러나 앞쪽 구조물이 어떠한 이유로 그 구실을 하지 못<br />
할 경우 후관절에 무너지는 힘이 과다해지면 후관절 증<br />
후군의 전제 조건을 갖는다(Fig. 3A). 만성척추통증을 호<br />
소하는 환자의 56%, 42% 및 31%가 경추, 흉추 및 요추<br />
각 부위의 통증의 원인으로 후관절을 지목하고 있다<br />
(Table 4). 9)<br />
후관절은 척추 레벨에 따라 Fig 3B와 같이 시상면과<br />
횡단면으로 배열되어 있다. 10)<br />
1) 경추 후관절 증후군: 경추 후관절은 만성경추통증<br />
을 호소하는 환자들에서 가장 먼저 의심해 볼만 한 구조<br />
물이다. 흔한 경추 후관절로부터 발생하는 질환으로 근<br />
근막 증후군, 추간판 탈출증 및 편타 손상 등을 열거할<br />
수 있다(Table 5). 저자의 연구에서 근근막 증후군 환자<br />
군이 후관절 증후군으로 발전하여 통증치료실을 방문하<br />
는 때까지의 기간은 나머지 두 질환군보다 길고, 추간판<br />
탈출증에서 발전한 후관절 증상은 후관절 차단에 대해<br />
가장 효과가 길게 유지되었다. 2)<br />
가장 흔한 경추 후관절 증후군의 발병 부위는 경추 5−<br />
6과 6−7번 사이이다. 경추 5−6 사이의 후관절은 어깨<br />
의 상부, 견갑골의 spine 상부 때로 하부 경추부위 등에<br />
연관통을 보이는 반면, 견갑골 전체 특히 spine 하부로<br />
연관통을 보이므로 임상적으로 큰 차이를 보인다(Fig.<br />
3C). 환자는 언제나 무거운 것을 지고 있든지 무언가 올<br />
라타고 있다는 느낌을 호소한다. 치료로는 후관절 차단<br />
(Fig. 3D) 혹은 후내측지 차단을 시행하고 증상이 반복될<br />
경우 후내측지 파괴술을 시행한다.<br />
대부분 신경 및 관절차단의 경우 두 관절 이상을 침범<br />
하므로 제대로 들어간 바늘을 필요한 약물을 투여 후 조<br />
금만 뽑고 그 방향을 참조하여 반대편 혹은 상하 관절에<br />
시행하는 것이 시술 시간과 노력을 줄일 수 있다(Fig.<br />
3E).<br />
관절차단과 후관절 분지 신경인 후내측지 차단은 각<br />
각의 장단점이 존재한다. 간접적인 방법으로 관절에 분<br />
포하는 신경인 후내측지의 신경차단으로 통증을 완화하<br />
는 방법보다 관절차단의 경우 통증을 일으키는 물질의<br />
직접적인 염증 경로의 차단을 볼 수 있는 장점이 있지만,<br />
단점으로 증상 재발이 되는 경우 후내측지 차단 이후 파<br />
괴술이 시행되어야 하고 관절낭의 의인성 파괴가 일어<br />
날 수 있다.<br />
2) 흉추 후관절 증후군: 흉추 후관절 증후군은 경흉추<br />
이행부를 제외하면 대부분 악성 혹은 양성 추체압박골<br />
절이 발생할 경우 발생한다. 경흉추 이행부는 경추의 원<br />
인과 큰 차이가 없으며, 중간 흉추는 갑상선암, 폐암 및<br />
유방암 등의 척추 전이에 흔하고, 흉요추 이행부는 골다<br />
공증에 의한 흔하다.<br />
흉추는 해부학적으로 흉곽으로 잘 고정되어 가동성보
6 KH Kim / Korean J Pain Vol. 21, No. 1, 2008<br />
Table 3. Comparison of Diagnostic Criteria for Cervicogenic Headache<br />
Sjaastad et al. (1990) International Headache Society (1988)<br />
International Association for the Study of Pain<br />
(1994)<br />
1. Unilateral headache<br />
triggered by head/neck<br />
movements or posture<br />
2. Unilateral headache<br />
triggered by pressure on the<br />
neck<br />
3. Unilateral headache<br />
spreading to the neck and<br />
homolateral shoulder/arm<br />
4. Pain improvement after<br />
greater occipital nerve<br />
(GON)/C2 block<br />
1. Pain localized to neck and occipital region. It<br />
may project to forehead, orbital region, temples,<br />
vertex or ears.<br />
2. Pain is precipitated or aggravated by special<br />
neck movement or sustained neck pressure<br />
3. At least one of the following: (1) Resistance<br />
to or limitation of passive neck movement<br />
(2) Changes in neck muscles contour, texture,<br />
tone or response to active and passive<br />
stretching and contraction<br />
(3) Abnormal tenderness of neck muscles<br />
4. Radiological examination reveals at least one<br />
of the following:<br />
(1) Movement abnormalities in flexion/extension<br />
(2) Abnormal posture<br />
(3) Fractures, congenital abnormalities, bone<br />
tumors, rheumatoid arthritis or other distinct<br />
pathology (not spondylosis or osteochondrosis)<br />
Attacks of moderately severe unilateral head pain<br />
without change in side, ordinarily involving the<br />
whole hemicranium, usually starting in the neck<br />
or occipital area, and eventually involving the<br />
forehead and temporal areas, where the maximal<br />
pain is frequently located.<br />
The headache usually appears in episodes of<br />
varying duration in the early phase, but with time<br />
the headache frequently becomes more<br />
continuous, with exacerbation and remissions.<br />
Symptoms and signs such as mechanical<br />
precipitation of attacks imply involvement of the<br />
neck.<br />
A blockade of the greater occipital nerve, the<br />
minor occipital nerve, the so-called third occipital<br />
nerve, or the cervical roots on the symptomatic<br />
side 1/4 represents a diagnostic test.<br />
다 중요 장기의 보호 역할을 주로 하고 있기 때문에 경<br />
추와 요추의 연결 부위의 전만(cervical and lumbar<br />
lordosis)들과 만나는 부위에 흔히 역학적인 요소에 의한<br />
병변이 흔히 발생하기 마련이다. 추체압박골절에 따른<br />
체중 부하로 인한 후관절 증후군의 동반은 저자의 연구<br />
에 따르면 88% 정도이며, 11) 차단을 시행하지 않을 경우<br />
추체성형술 혹은 후만성형술 이후에도 갈비뼈를 따라<br />
경계가 불분명한 무거운 느낌의 통증과 아침 처음 동작<br />
에서 누워 있다가 일어날 때 큰 불편을 호소한다. 이학적<br />
검사에서도 후관절 부위에 대부분 심한 압통을 호소하<br />
면서 갈비뼈를 따라 통증이 재현되는 경우가 흔하다<br />
(Fig. 3F).<br />
후관절 차단은 반드시 추체성형술 혹은 후만성형술<br />
이전에 시행하는 것이 옳다. 그 이유로 첫째, 복와위에서<br />
참을 수 없는 통증을 호소하는 환자에서 후관절 차단 후<br />
추체성형술을 시행할 때 후관절 통증의 제거로 시술 중<br />
자세에 대한 환자의 협조를 받을 수 있다. 둘째, 외래에<br />
서 척추압박골절과 후관절 통증을 감별하기 힘들 정도<br />
의 심한 통증으로 복와위에서 이학적 검사를 할 수 없을<br />
경우 fluoroscope하에서 추체성형술 전 후관절 차단만으<br />
로도 전체 통증이 없어지고 가시돌기 부위의 압통이 발<br />
견되지 않을 경우 형태적으로 압박골절이 있지만 통증<br />
이 없어진 추체에 굳이 추체성형술을 시행할 필요가 없<br />
다. 셋째, 추체성형술 시행 후 후관절 차단을 시행할 경<br />
우 먼저 주입 된 추체의 골 시멘트에 의해 후관절을 제<br />
대로 관찰할 수 없어서 후관절 차단에 어려움을 겪게 된<br />
다. 11)<br />
관절 내 주사는 전후상에서 추경의 9시부터 12시 사이<br />
의 내상방에 존재하는 우측 후관절 혹은 12시에서 3시<br />
사이의 좌측 후관절을 향하게 된다(Fig. 3G). 반대로 후<br />
내측지 차단 및 파괴술은 사면상에서 추경의 추체의 9시<br />
부터 12시 사이의 내상방에 존재하는 좌측 후관절 혹은<br />
12시에서 3시 사이의 우측 후관절을 향하게 된다.<br />
3) 요추 후관절 증후군: 요추 후관절 증후군은 요추 전<br />
방전위증, 척추 측만증, 척추 유합술 후 상하, 상부 요추<br />
의 골다공증성 압박골절 및 하부 요추의 암 전이 골분해<br />
성 압박골절 등에서 흔히 동반한다. 환자는 아침에 첫<br />
움직임이 어렵고 오후가 되면 다소 완화된다는 점에서<br />
흉추와 차이가 없으며, 엉치와 다리 쪽으로 연관통을 보<br />
이지만 무릎 이하로는 통증이 뻗치지는 않는다. 이학적<br />
검사에서 후관절 주위의 압통과 함께 옆구리와 엉치 쪽<br />
으로 무겁고 때로 시린 증상을 재현할 수 있다.
김경훈: <strong>척추관절통증증후군</strong> 7<br />
Fig. 3. (A) Illustration of spinal loads and articular surface area across the lumbar spinal column. (B) Orientation of cervical, thoracic,<br />
and lumbar facet joint from the view of the sagittal and transverse plane. (C) The referral zone of cervical facet joint pain from C2-3<br />
to C6-7. (D) Cervical facet joint injection on the right C6-7: (a) anteroposterior view, (b) lateral view. (E) The first lower needle is just<br />
removed from C6-7 facet joint. The second needle is approaching to the C5-6 facet joint with the guidance of the first one. (F) The<br />
referral zone of thoracic facet joint pain from the C7-T1 and T11-12. (G) The needle is placed at the superiomedial aspect of the left<br />
thoracic pedicle on the anteroposterior view. (H) The needle is placed at the superiomedial aspect of the lumbar pedicle on the oblique<br />
view.<br />
관절 차단을 위해 사면상에서 관절을 잘 볼 수 있는<br />
방향으로 맞추고 가능하면 후관절의 하부 함몰(inferior<br />
recess) 쪽으로 바늘을 삽입한다. 관절 내 조영제 투입은<br />
0.5 ml 이하로 하여 관절의 의인성 파괴의 기회를 줄인<br />
다(Fig. 3H). 후내측지 차단 및 파괴술 역시 흉추와 마찬<br />
가지로 추경의 외상방을 목표로 하고 감각과 운동신경
8 KH Kim / Korean J Pain Vol. 21, No. 1, 2008<br />
Fig. 4. (A) Sacroiliac joint: (a) posterior view of the articulations and associated ligaments of the sacroiliac joint and surrounding structures<br />
and (b) anterior view of the articulations and associated ligaments of the sacroiliac joint and surrounding structures. (B) Commonly used<br />
physical test for sacroiliac joint pain. (C) Referral pain pattern of sacroiliac joints. (D) Sacroiliac joint block. (E) Direction of the needle<br />
for sacroiliac joint block.<br />
자극을 통해 자극의 수치가 3배 이상 차이가 나면 이상<br />
적이다.<br />
3. 천장관절 증후군<br />
1) 해부와 기능: 천장관절은 평균 표면적이 17.5 cm 2<br />
이나 되는 체내의 가장 큰 축 관절이며 활액낭으로 구성<br />
되어 있다. 그러나 실제로 천골과 장골 사이의 앞쪽 1/3<br />
만 접해있고, 나머지는 뒤쪽 2/3는 인대로 연결되어 있다<br />
(Fig. 4A). 12) 일부 근육들 특히 대둔근, 이상근 및 대퇴이<br />
두근 등이 천장관절의 인대와 함께 관절의 유동성에 조<br />
절한다.<br />
뒤쪽 천장관절의 신경분포는 요추 3번−천추 4번 간
김경훈: <strong>척추관절통증증후군</strong> 9<br />
Table 4. The Prevalence of Facet joint Pain in Patients with<br />
Chronic Spinal Pain<br />
Cervical Thoracic Lumbar<br />
spine spine spine<br />
Prevalence 56 (49−61) 42 (30−53) 31 (27−36)<br />
The false positive rate<br />
with single blocks 63 (54−72) 55 (39−78) 27 (22−32)<br />
with lidocaine<br />
Values are % values of mean (95% confidence interval).<br />
Table 5. Comparison of Myofascial Pain Syndrome (MPS),<br />
Herniated Nucleus Pulposus (HNP), and Whiplash Associated<br />
Disorder (WAD)<br />
Group<br />
History of<br />
Trauma radicular pain Imaging<br />
history on the shoulder diagnosis<br />
and arm<br />
MPS (−) (−) (−)<br />
HNP (−) (+) (+)<br />
WAD, grade II (+) (−) (±)<br />
Table 6. Common Tests Utilized in Evaluation of Sacroiliac Joint Dysfunction<br />
Patrick's (FABERE) test<br />
With the patient supine on a level surface, the thigh is flexed<br />
and the ankle is placed above the patella of the opposite<br />
extended leg. With the knee depressed and the ankle<br />
maintaining its position above the opposite knee, the patient<br />
will complain of pain before the knee reaches the level<br />
obtained in normal persons.<br />
Gaenslen's (Pelvis torsion) test<br />
The patient lies supine, flexes the ipsilateral knee and hip with<br />
the thigh crowded against the abdomen with the aid of both<br />
the patient's hands clasped about the flexed knee. This brings<br />
the lumbar spine firmly in contact with the table and fixes both<br />
the pelvis and lumbar spine. The patient is then brought well<br />
to the side of the table, and the opposite thigh is slowly<br />
hyperextended with gradually increasing force by pressure of<br />
the examiner's hand on the top of the knee. With the opposite<br />
hand, the examiner assists the patient in fixing the lumbar<br />
spine and pelvis by pressure over the patient's clasped hands.<br />
The hyperextension of the hip exerts a rotating force on the<br />
corresponding half of the pelvis in the sagittal plane through<br />
the transverse axis of the sacroiliac joint. The rotating force<br />
causes abnormal mobility accompanied by pain, either local or<br />
referred on the side of the lesion.<br />
후외측지가 관여하고, 반면 앞쪽 천장관절은 요추 2번−<br />
천추 2번 간 전지가 관여한다고 알려져 있다. 고양이에<br />
서 규명된 신경생리검사에서 대부분의 기계적 자극에<br />
민감한 구심성 신경들이 관절낭에서 발견되었고 일부만<br />
근처 근육에서 발견되었다. 또 대부분이 침해성 자극을<br />
받아들이는 신경이며 일부만 고유감각에 관여하였다.<br />
이들 신경들은 뒤쪽 천장관절 근위부 1/3과 중간 1/3에<br />
분포하고 있다. 침해수용을 하는 신경의 기계적 역치는<br />
70 g으로 요추 후관절의 6 g과 앞쪽 구조물인 추간판의<br />
241 g의 중간 정도로 알려져 있다.<br />
기능적으로 천장관절의 기능은 안정적으로 하지에 체<br />
간의 무게를 전달하고 분산하며, x축 회전을 제한하고,<br />
출산 시 도움을 준다. 요추와 비교하여 내측으로 주어지<br />
는 힘에 6배 잘 견디지만, 반대로 꼬임에 대해서 1/2 정<br />
도와 축 방향의 힘에 대해서는 1/20 정도 견디는 힘이<br />
약하다.<br />
손상기전으로 축 방향의 부하와 갑작스런 회전을 들<br />
고 있다. 해부학적으로 관절낭 혹은 활액의 파괴, 관절낭<br />
과 인대의 긴장, 과다 혹은 과소운동, 외부 압박 혹은 전<br />
단력(shearing force), 골절 및 연골연화, 연조직 손상 및<br />
염증 등에서 발생할 수 있다. 그 외 위험인자로서 양쪽<br />
다리의 길이가 다른 경우, 걸음의 이상, 지속되는 심한<br />
운동, 척추 측만증 및 천공과의 유합술 등을 들 수 있다.<br />
그 외 임신 시에도 체중의 증가, 과다한 척추 전만, 분만<br />
시 기계적인 손상 및 호르몬에 기인한 인대의 느슨해짐<br />
등이 천장관절의 통증을 일으키는 위험요소가 된다.<br />
만성 축 방향의 요통을 호소하는 환자의 15−25%의 환<br />
자가 천장관절 증후군을 동반하고 있음을 알려져 있다.<br />
2) 진단: 가장 흔히 이용되는 이학적 검사로는 Patrick's<br />
test와 Gaenslen's test가 있다(Table 6)(Fig. 4B). 핵의학<br />
검사는 13−44% 정도의 민감성과 89.5−100%의 특이<br />
성을 갖는다고 알려져 있다. 12)<br />
연관통의 분포는 엉치(94%), 하부 요추부(72%), 하지<br />
(50%), 사타구니(14%), 상부 요추부(6%) 및 복부(2%) 정<br />
도로 알려져 있어, 대부분 요추 5번 극돌기 이하에서 무<br />
릎 위쪽 허벅지까지로 생각하는 것이 옳다(Fig. 4C).
10 KH Kim / Korean J Pain Vol. 21, No. 1, 2008<br />
3) 치료: 관절 내 주사와 고주파 열응고술에 의한 신경<br />
파괴를 시행할 수 있다. 관절 내 주사는 불행히도 하부<br />
끝 부위에만 바늘이 주입되는 경우가 흔해, 조영제가 관<br />
절의 양면 및 위쪽까지 잘 묻었는지 관찰을 요한다(Fig.<br />
4D). 주입되는 바늘의 방향은 CT의 영상에서 추측할 수<br />
있다(Fig. 4E). 파괴술 역시 분포하는 신경인 요추 3번−<br />
천추 4번 간 후외측지를 모두 찾아 파괴하는 것은 현실<br />
적으로 불가능하며 대안으로 관절 내 들어와 있는 신경<br />
이라도 모두 파괴하는 노출(denudation) 방법(Fig. 4D)을<br />
사용하기도 한다.<br />
결<br />
만성 척추통증의 가장 흔한 원인이 되는 후관절 통증<br />
이 임상적으로 영상학적 검사에서 자주 무시될 수 있으<br />
므로 쉽게 간과될 수 있으며 가장 좋은 진단 방법이자<br />
치료 방법인 작용 기간이 다른 두 가지 국소마취제를 사<br />
용하여 이중 차단법을 시행하는 것이 유용하다. 임상적<br />
으로 척추 후관절의 연관통 그림과 같은 통증의 재현보<br />
다 그 통증의 감소가 의미가 있기 때문이기도 하다. 수많<br />
은 관절로 구성된 척추의 뒤쪽 구조물인 후관절에 대한<br />
정확한 진단은 환자와 의사의 신뢰에도 큰 몫을 할 것으<br />
로 생각한다.<br />
론<br />
참 고 문 헌<br />
1. Bogduk N: Clinical anatomy of the lumbar spine and<br />
sacrum. 3rd ed. New York, Churchill Livingstone. 1997, pp<br />
187-214.<br />
2. Kim KH, Choi SH, Kim TK, Shin SW, Kim CH, Kim JI:<br />
Cervical facet joint injections in the neck and shoulder pain.<br />
J Korean Med Sci 2005; 20: 659-62.<br />
3. Sizer PS Jr, Phelps V, Azevedo E, Haye A, Vaught M:<br />
Diagnosis and management of cervicogenic headache. Pain<br />
Pract 2005; 5: 255-74.<br />
4. Chou LH, Lenrow DA: Cervicogenic headache. Pain<br />
Physician 2002; 5: 215-25.<br />
5. Leone M, D'Amico D, Grazzi L, Attanasio A, Bussone G:<br />
Cervicogenic headache: a critical review of the current<br />
diagnostic criteria. Pain 1998; 78: 1-5.<br />
6. Antonaci F, Bono G, Mauri M, Drottning M, Buscone S:<br />
Concepts leading to the definition of the term cervicogenic<br />
headache: a historical overview. J Headache Pain 2005; 6:<br />
462-6.<br />
7. Haldeman S, Dagenais S: Cervicogenic headaches: a critical<br />
review. Spine J 2001; 1: 31-46.<br />
8. Waldman SD: Interventional pain management. 2nd ed.<br />
Philadelphia, Saunders. 2008, p 301.<br />
9. Manchikanti L, Boswell MV, Singh V, Pampati V, Damron<br />
KS, Beyer CD: Prevalence of facet joint pain in chronic<br />
spinal pain of cervical, thoracic, and lumbar regions. BMC<br />
Musculoskelet Disord 2004; 5: 15.<br />
10. Czerniecki JM, Goldstein B: General considerations of pain<br />
in the low back, hips, and lower extremities. In: Bonica's<br />
management of pain. 3rd ed. Edited by Loeser JD:<br />
Philadelphia, Lippincott Williams & Wilkins. 2001, p 1482.<br />
11. Kim TK, Kim KH, Kim CH, Shin SW, Kwon JY, Kim HK,<br />
et al: Percutaneous vertebroplasty and facet joint block. J<br />
Korean Med Sci 2005; 20: 1023-8.<br />
12. Cohen SP: Sacroiliac joint pain: a comprehensive review of<br />
anatomy, diagnosis, and treatment. Anesth Analg 2005; 101:<br />
1440-53.